Embed Size (px)
Citation preview

This is the author’s version of a work that was submitted/accepted for pub-lication in the following source:
Gwinner, Karleen & Ward, Louise (2013) P.I.C.U., H.D.U., A.O.A. Whattreatment do we provide?: Current descriptions of the function of intensivecare for inpatient Psychiatric Health Care. Mental Health Review Journal,18(3), pp. 128-143.
This file was downloaded from: http://eprints.qut.edu.au/60951/
c© Copyright 2013 Emerald Group Publishing Limited
Notice: Changes introduced as a result of publishing processes such ascopy-editing and formatting may not be reflected in this document. For adefinitive version of this work, please refer to the published source:
http://dx.doi.org/10.1108/MHRJ-02-2013-0008
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by Queensland University of Technology ePrints Archive

For Peer Review
P.I.C.U., H.D.U., A.O.A. What treatment do we provide?
Current descriptions of the function of intensive care for
inpatient Psychiatric Health Care.
Journal: Mental Health Review Journal
Manuscript ID: MHRJ-02-2013-0008.R1
Manuscript Type: Research Paper
Keywords: psychiatric intensive care, recovery-oriented, Nurses, mental health
services, organisation, PICU
Mental Health Review Journal

For Peer Review
(Author) Year Journal
Title Aim Context Research Method/ Approach
data base Search terms
Alexander, J., & Bowers, L. (2004) Journal of Psychiatric and Mental Health Nursing
Acute psychiatric ward rules: a review of the literature
To ascertain the flexibility/inflexibility of ward nursing regimes and patient outcomes.
psychiatric wards Literature review Blackwell Science
'Acute psychiatric ward' rules
Bjorkdahl, A., Palmstierna, T., & Hansebo, G. (2010) Journal of Psychiatric and Mental Health Nursing
The bulldozer and the ballet dancer: aspects of nurses' caring approaches in acute psychiatric intensive care
To describe nurses' caring approaches
Acute psychiatric wards
Qualitative Blackwell Science
Psychiatric intensive care mental OR illness not pediatric 2009<
Bowers, Crowhurst, Alexander, Eales, Guy, & McCann, (2003) International Journal of Nursing Studies,
Psychiatric nurses' views on criteria for psychiatric intensive care: acute and intensive care staff compared
To explore and investigate differences between the views of qualified nurses working in PICUs and acute care wards on which patients are appropriate for PICU care.
PICU UK
Qualitative, Structured interviews
Wiley Online Library
nurse perspective acute mental health
Bowers, L. (2005) Journal of Psychiatric and Mental Health Nursing
Reasons for admission and their implications for the nature of acute inpatient psychiatric nursing
To define the function of acute inpatient psychiatry, and the role of psychiatric nurses
acute inpatient psychiatry Literature review Blackwell Science
psychiatric intensive care unit in acute psychosis
Bowers, L., Jeffery, D., Bilgin, H., Jarrett, M., Simpson, A., & Jones, J. (2008) International Journal of Social Psychiatry,
Psychiatric intensive care units: a literature review
To conduct a systematic literature review to assess the current state of knowledge about PICU services.
PICU- UK Literature review Sage Journals
Therapeutic role of a psychiatric intensive care unit in acute psychosis
Bowers, L., Stewart, D., Papadopoulos, C., Dack, C., Ross, J., Khanom, H., et al. (2011)
Inpatient violence and aggression: a literature review
To describe the available research literature on the prevalence, antecedents, consequences and circumstances of violence and aggression in psychiatric hospitals
Report from the Conflict and Containment Reduction Research Programme UK
Literature review
Institute of Psychiatry Kings College London
conflict and containment on acute wards
Brennan, G., Flood, C., & Bowers, L. (2006) Journal of Psychiatric & Mental Health Nursing
Constraints and blocks to change and improvement on acute psychiatric wards – lessons from the City Nurses project
To reduce levels of conflict and containment on acute wards through the placement of expert nurses on wards
2 generic acute admission wards with 18 beds UK
Intervention incorporating elements of action research
CINHAL
management acute inpatient psychiatric city nurse
Brown, S., & Bass, N. (2004)
The psychiatric intensive care unit (PICU): patient
To compare the characteristics, treatment and
Psychiatric Intensive Care
Case controlled retrospective case
Intensive Care Units, treatment
Page 1 of 24 Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
Journal of Mental Health, characteristics, treatment and outcome
outcome of a series of patients
Units, Acute unit
note analysis. outcomes, provision of care
Caldwell, B. A., Gill, K. J., Fitzgerald, E., Sclafani, M., & Grandison, P. (2006) American Journal of Psychiatric Rehabilitation
The Association of Ward Atmosphere with Burnout and Attitudes of Treatment Team Members in a State Psychiatric Hospital.
To examine hospital characteristics as they relate to the strategies necessary to transform an approach of custodial care to a culture of recovery.
5 Major state psychiatric facility
Quanitative Maslach Burnout Inventory (Maslach & Jackson, 1986) Nursing Work Index (Aiken & Hage, 1968; Kramer & Hafner, 1989)
Informa Health Care
Psychiatric intensive care unit /acute care / recovery organizational culture
Chalmers, A., Harrison, S., Mollison, K., Molloy, N., & Gray, K. (2012) Australasian Psychiatry
Establishing sensory-based approaches in mental health inpatient care: a multidisciplinary approach
To reflect upon the implementation of sensory-based approaches within the environment of a psychiatric inpatient unit.
29-bed acute adult psychiatric inpatient unit in Victoria. Australia
Intervention Ebsco
Acute psychiatry, multidisciplinary Australia 2009<
Cleary, M. (2004) Journal of Mental Health Nursing
The realities of mental health nursing in acute inpatient environments.
To understand how nurses construct their practice in an acute inpatient psychiatric unit in light of the current challenges, demands and influences brought about by service reform.
22-bed acute inpatient mental health facility in New South Wales, Australia
Ethnographic study Blackwell Science
interaction and arrangements provisions of (intensive psychiatric inpatient care)
Cleary, M., Horsfall, J., O'Hara-Aarons, M., & Hunt, G. E. (2012). International Journal of Mental Health Nursing
Mental health nurses’ views of recovery within an acute setting
to ask acute inpatient MHN about their understanding of recovery and how they are incorporating a recovery paradigm in their dayto- day nursing practice.
Four acute inpatient mental health units in a large area health service in New South Wales, Australia
Qualitative interpretive approach
Wiley Online Library
recovery Mental health nurse acute setting Australia 2009<
Cleary, M., Hunt, G. E., Walter, G., & Robertson, M. (2009) Journal Of Medical Ethics
Locked inpatient units in modern mental health care: values and practice issues.
To examine briefly some of the issues pertaining to the use of locked units in modernmental health care
Locked inpatient units Literature review Medline Complete
Psychiatric intensive acute procedures nursing patient outcomes
Cleary, M., Hunt, G., & Walter, G. (2009) Australasian Psychiatry,
A comparison of patient and staff satisfaction with services after relocating to a new purpose-built mental health facility.
Measure patient satisfaction levels and staff views regarding their expectations and workplace and other opinions after relocation to a new purpose-built mental health facility.
Australia’s oldest and largest psychiatric hospital, Sydney’s Australia & purpose built mental health facility
Inpatient Evaluation of Services Questionnaire (Meehan, Bergen and Stedman, 2002)
Informa Healthcare
purpose-built mental health acute facility Australia 2009<
Page 2 of 24Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
Cresswell, J., Beavon, M., & Glover, N. (2009). London: Royal College of Psychiatrists Centre for Quality Improvement.
Accreditation for Inpatient Mental Health Services (AIMS) Standards for Psychiatric Intensive Care Units (PICUs)
To provide clear standards which are monitored and externally accredited.
Department of Health London UK
Report Royal College of Psychiatrists
Referenced elsewhere
Crowhurst, N., & Bowers, L. (2002) Journal of Psychiatric and Mental Health Nursing,
Philosophy, care and treatment on the psychiatric intensive care unit: themes, trends and future practice
Examine the infrastructure of PICU, the treatment provided to patients on the PICU, the efficacy of PICU care
PICU provision Literature review Blackwell Science
Therapeutic role of a psychiatric intensive care unit in acute psychosis
Crowther, A., & Ragusa, A. (2011) Issues in Mental Health Nursing
Realities of Mental Health Nursing Practice in Rural Australia
To investigate the contemporary relevance and existence of key challenges facing mental health nursing
mental health nursing in rural areas, NSW Australia
Qualitative Informa Healthcare mental health nursing practice in rural areas
Curtis, S., Gesler, W., Fabian, K., Francis, S., & Priebe, S. (2007). Environment and Planning
Therapeutic landscapes in hospital design: a qualitative assessment by staff and service users of the design of a new mental health inpatient unit.
To provide a post-occupancy assessment of a new mental health inpatient unit in London
Mental health unit UK Qualitative Google scholar
environments mental health inpatient hospital design
Daffern, M., Mayer, M. M., & Martin, T. (2004) International Journal of Forensic Mental Health
Environment Contributors to Aggression in Two Forensic Psychiatric Hospitals
To examine the role of environment and ward routine on aggression in a secure forensic psychiatric hospital.
Rosanna Forensic Psychiatry Centre and the Thomas Embling Hospital
Comparative review of incident forms relating to aggressive behaviors
Taylor and Francis
environment aggression in psychiatric hospitals
Dix and Page, (2008) In M. D. Beer, Pereira, S. M., & Paton, C. (Ed.), Psychiatric intensive care
Physical Environmnets To provide the clinical context within which PICU/LSU design should be considered
UK
Experienced-based principles for effective PICU design
Cambridge University Press
Referenced elsewhere in literature
Fiddler, M., Borglin, G., Galloway, A., Jackson, C., McGowan, L., & Lovell, K. (2010) International Journal of Mental Health Nursing
Once-a-week psychiatric ward round or daily inpatient team meeting? A multidisciplinary mental health team's experience of new ways of working.
Highlight staff view of the once-a-week psychiatric ward round compared to a reformed ward round taking place every weekday.
1 acute psychiatric ward in north-west England
Qualitative Wiley Online 'Acute psychiatric ward' rules
Fourie, W. J., McDonald, S., Connor, J., & Bartlett, S.
(2005). International Journal of Mental Health Nursing
The role of the registered nurse in an acute mental health inpatient setting in
New Zealand: Perceptions versus reality.
To establish from registered nurses what they perceived
their roles to be
3 Acute inpatient facilities
Qualitative descriptive
exploratory study Blackwell Science
nurses psychiatry
standards of the environment safety acute
care
Page 3 of 24 Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
Georgieva, I., de Haan, G., Smith, W., & Mulder, C. L.
(2010) Journal of Psychiatric
Intensive Care,
Successful reduction of seclusion in a newly
developed psychiatric intensive care unit.
To investigate whether patients transferred to a newly developed PICU,
focused on the effective and non-coercive management of
disruptive behavior, are secluded and restrained less than during earlier stays in a
psychiatric unit.
eight patients in Mental
Health Care Centre in
Netherlands
Retrospective study evaluating the effect
of a PICU on reducing seclusion
Cambridge Online Library
Mental health nursing practice
in acute psychiatric
close-observation
areas
Glick, I.R.A.D., G., Carter, W. G., & Tandon, R.
(2003) Journal of Psychiatric
Practice
A paradigm for treatment of inpatient psychiatric
disorders: from asylum to intensive care
Detail a workable model of inpatient psychiatric
treatment based on current, drastically changed realities.
Inpatient psychiatric
care, academic
inpatient units, Veterans
Affairs inpatient unit.
Literature review Wolters Kluwer Health
Psychiatric intensive care units recovery-
oriented
Hopkins, J. E., Loeb, S. J., & Fick, D. M. (2009)
Journal of Psychiatric and Mental Health Nursing
Beyond satisfaction, what service users expect of inpatient mental health
care: a literature review.
Ascertain if service users are satisfied with the care
received from nurses, but also the degree to which
initial expectations are being met.
Inpatient psychiatric unit
or mental health unit.
Systematic literature review
Blackwell Publishing
responsibility treatment
mental illness (intensive psychiatric
inpatient care) 2000<
Lee, S. J., Cox, A., Whitecross, F., Williams, P.,
& Hollander, Y. (2010)
Journal of Psychiatric Intensive Care
Sensory assessment and therapy to help reduce
seclusion use with service users needing psychiatric
intensive care
To test sensory modulation as a method to help reduce seclusion use with service users needing psychiatric
intensive care
30-bed acute psychiatric unit
Six-month pilot of the use of sensory
modulation strategies and a brief sensory
and risk assessment tool (Safety Tool)
Cambridge Journals Online
Psychiatry sensory
stimulation
Meehan, T., Fjeldsoe, K., Stedman, T., & Duraiappah,
V. (2006) Australian Health Review
Reducing aggressive behaviour and staff injuries: a multi-strategy approach
To evaluate the impact of a multi-strategy approach on the management of patient aggression and staff injury
rates
Stand alone psychiatric facility Qld, Australia
Longtidual (7year) Intervention- pre-
test/post-test
O'Brien, L., & Cole, R. (2003)
International Journal of Mental Health Nursing
Close-observation areas in acute psychiatric units: A
literature review
To address the processes or goals of containing patients, the role of nurses, and the
skills Involved.
Australian inpatient
psychiatric units
Literature Review
acute psychiatric units
close observation
Page 4 of 24Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
O'Brien, L., & Cole, R. (2004)
Journal of Mental Health Nursing,
Mental health nursing practice in acute psychiatric close-
observation areas.
To reveal the experience of patients, relatives, and
nurses in a close-observation area
Nursing care in close-
observation units or
psychiatric intensive care
units
Participatory action research framework to identify qualitative
and quantitative measures of activity
in the area
Wiley Online Library
Therapeutic role of a psychiatric intensive care unit in acute psychosis
Pereira, S., Dawson, P., & Sarsam, M.
(2006) Journal of Psychiatric
Intensive Care
The national survey of PICU and low secure services: 1. Patient
characteristics.
To perform the first UK wide survey developing a national
data set of low secure services
307 units comprised 170
Psychiatric Intensive Care
Unit (PICU) housing 1,242 patients and
137 Low Secure Units
(LSUs) treating 1,583
patients
Cross-sectional census day postal
survey design
Cambridge Journals Online
operational characteristics PICU intensive psychiatric care
Pereira, S., Chaudhry, K., Pietromartire, S., Dale C.and
Halliwell J. (2005)
Journal of Psychiatric Intensive Care
Design in Psychiatric Intensive Care Units: problems and issues
To determine whether current physical environment of
PICUs and LSUs are adequate to meet the
therapeutic needs of patients in England.
(PICU) (LSU) An inventory was sent to all NHS
PICUs and LSUs
Cambridge Journals Online
Design PICU
Pereira, S. M., Sarsam, M., Bhui, K., & Paton, C.
(2005) Journal of Psychiatric
Intensive Care
The London Survey of Psychiatric Intensive Care
Units: service provision and operational characteristics of National Health Service
units.
To offer the first large-scale systematic survey describing
service structure and functioning of PICU and LSU.
(PICUs) (LSUs)
Quantitative- Questionnaire was
sent to ward managers of every PICU and LSU in
London
Cambridge Journals Online
hot beds intensive acute inpatient wards
Queensland Health, (2012) Report
Guideline for the operation of High Dependency Units
(HDUs) in Mental Health Services
Recommendations regarding best
practice around the management and operation
of High Dependency Units (HDUs) in
mental health services.
HDU- Queensland
Australia
Procedures, Guidelines, Protocols Google web search
Qld Mental Health
Guidelines
Salzmann-Erikson, M., Lützén, K., Ivarsson, A.-B., &
Eriksson, H. (2008)
International Journal of Mental Health Nursing
The core characteristics and nursing care activities
in psychiatric intensive care units in Sweden.
To describe the core characteristics of a PICU in Sweden and to describe the care activities provided for
patients admitted to the PICUs
PICU Qualitative- Critical incident technique
Blackwell Publishing caring in PICU
Page 5 of 24 Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
Salzmann-Erikson, M., Lutzen, K., Ivarsson, A. B., &
Eriksson, H. (2011)
Issues in Mental Health Nursing
Achieving Equilibrium within a Culture of Stability-
Cultural Knowing in Nursing Care on
Psychiatric Intensive Care Units.
To describe the cultural knowing expressed in nursing
care in PICU
14 PICUs (approximately
120 beds) Sweden
Ethnographic fieldwork Informa healthcare
Psychiatric intensive care
mental OR illness –not
paediatric 2009<
Seed, M. S., Torkelson, D. J., & Alnatour, R.
(2010) Issues in Mental Health
Nursing
The Role of the Inpatient Psychiatric Nurse and Its Effect on Job Satisfaction
To describe the role (tasks and functions) and job
satisfaction levels of inpatient psychiatric nurses.
Inpatient psychiatric
units specific
functions during a
nursing shift
Observational correlational design Informa healthcare
Role of the Inpatient
Psychiatric Nurse
Singh, N. N., Singh, S. D., Sabaawi, M., Myers, R. E., &
Wahler, R. G. (2006)
Behavior Modification
Enhancing Treatment Team Process Through
Mindfulness-Based Mentoring in an Inpatient
Psychiatric Hospital.
To evaluate the effects of mindfulness-based mentoring
on treatment team functioning.
Treatment teams in adult
inpatient psychiatric
hospital
Intervention using Kennedy (1992) model- treatment planning process
Sage Publications
multi discipline Inpatient
Psychiatric Team
Vaaler, A. E., Morken, G., & Linaker, O. M.
(2005) Nordic Journal Of Psychiatry
Effects of different interior decorations in the seclusion area of a
psychiatric acute ward
To compare, treatment and patient satisfaction of a
traditional interior and an interior furnished like an
ordinary home .
Seclusion area of a psychiatric
acute ward
Intervention- comparison Taylor and Francis
design furnishing acute
wards Psychiatry, Seclusion
Van Der Merwe, M., Muir-Cochrane, E., Jones, J., Tziggili, M., & Bowers, L.
(2012) Journal of Psychiatric and
Mental Health Nursing
Improving seclusion practice: implications of a review of staff and patient
views.
Explores patient and staff perceptions and improvement
suggestions regarding seclusion in psychiatric
inpatient settings.
inpatient seclusion
Review of empirical literature
Wiley Online Library
acute psychiatric ward
nursing
Wynaden, D., McGowan, S., Chapman, R., Castle, D.,
Lau, P., Headford, C., et al. (2001)
Australian & New Zealand Journal of Psychiatry
Types of patients in a psychiatric intensive care
unit
To provide insight and measurements relating to
patient diagnosis, treatment interventions, and patient
care.
Eight bed psychiatric
intensive care unit (PICU) in
Western Australia
Descriptive study of a patient population over a three-month
period
Inpatient seclusion
Intensive Care Units
Australia Treatment
Page 6 of 24Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
Inclusion Criteria Exclusion Criteria International research
English language 2000 onwards,
Adult PICU Youth
Meets operational definition in acute psychiatric wards Empirical literature
Reviews Allied Health
Evaluations of services
Nursing context
Dissertations
Non-‐English Language Pre 2000
Community Mental Health General intensive care
Pediatrics
Dual diagnosis Alcohol & Drug recovery
Abstracts, conference proceedings Editorials
Page 7 of 24 Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
P.I.C.U., H.D.U., A.O.A. What treatment do we provide?: Current descriptions of the function of intensive care for inpatient Psychiatric Health Care.
Abstract
Purpose: This paper adds to growing research of Psychiatric Intensive Care Units (PICU) by recounting descriptions of psychiatric intensive care settings and discusses the perceptions held by Nurses of the organisational interfaces, arrangements and provisions of care in these settings.
Method: Data gathered from focus groups held with Nurses from two PICUs was used to establish terminology, defining attributes, related concepts, antecedents, values, processes, and concepts related to current practices. A literature search was conducted to permit a review of the conceptual arrangements and contemporary understanding of intensive care for people experiencing acute psychiatric illness based on the perspectives held by the nurses from the focus groups.
Findings: Dissonance between service needs and the needs and management of individual patients overshadows strategies to implement comprehensive recovery-oriented approaches. Three factors are reported in this article that influence standards and procedural practice in PICU; Organisational structures; Physical structures; and Subtype nomenclature.
Originality/value: Current descriptions from nurses substantiate wide variations in the provisions, design and classifications of psychiatric intensive care. Idiosyncratic and localized conceptions of psychiatric intensive care are not adequately entailing effective treatment and methods in support of recovery principles for improved and comprehensive outcomes. The authors suggest that more concrete descriptions, guidelines, training and policies for provision of intensive psychiatric health care encompassing the perspective of nursing professionals, would reinforce conceptual construction and thus optimum treatments within a comprehensive, recovery-oriented approach to mental health services.
Keywords; Psychiatric intensive care, nurses, recovery-oriented, mental health services, organisation, PICU
Page 8 of 24Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
Introduction
“We had so many chronic patients walking around, cause they are dependent on a
service and then the PICU is a mish mash of everybody requiring treatment but
what treatment do we provide?”
This statement illustrates the frustration involved in meeting the needs of people experiencing acute psychiatric distress. While much has been written about the need to minimise the impact of mental illness through a comprehensive approach to health services based on consumer driven recovery principles (Geraghty et al., 2011, Migdole et al., 2011, Ramon et al., 2007, Bertolote and McGorry, 2005, Olmos-Gallo et al., 2012), limited inquiry has focused on how acute intensive care units deliver a recovery-oriented approach as part of a comprehensive mental health service.
Intensive care of patients experiencing acute psychiatric distress is an essential, yet complex part of mental health services as a whole system. Commonly intensive care is delivered in specialized wards or units co-located with Acute Mental Health Inpatient Units mostly known as Psychiatric Intensive Care Units (PICU). PICUs are staffed by specialised nurses and equipped to provide observation, care and treatment to individuals with actual or potential life-threatening illness, or complications from which recovery is possible (Australasian Health Infrastructure Alliance, 2010). In many other countries, as in Australia standards of care are mandated by relevant guidelines such as the National standards for mental health services (Australian Health Ministers, 2009). However standards can be translated into different ideas and objectives, functionalities and according to varying context of use (Beer et al., 2001, Cleary et al., 2009a).
Despite promising developments, the arrangements for provisions of intensive psychiatric inpatient care have been described as a neglected area of thinking and research (Glick et al., 2011, Cox et al., 2010). Evidence of the effectiveness of care and treatment remain scarce (Pereira et al., 2005b, Paul and Menditto, 1993, Walsh and Boyle, 2009). The purpose of acute admission has also been insufficiently defined (Bowers et al., 2009). Audits and surveys of PICUs demonstrate conceptual discrepancies about the nature and purpose of PICU (Cleary et al., 2009a p.231, Glick et al., 2011). Additionally narratives from patient and carer experiences are too often impoverished, indicating insufficient conditions for care, treatment and engagement of a recovery-oriented approach in PICU (Geraghty et al., 2011, Horsfall et al., 2010, Cleary and Dowling, 2009).
It is timely to establish greater clarification of the complex and changing mixture involved in meeting the needs of people experiencing acute psychiatric distress. This paper draws on data from focus groups with nurses and an integrated study of current literature to depiction of the concepts and issues in PICU. The aim of this paper is to provide a critical reading of the perceptions and descriptions understood by nurses, as the vanguard of providing intensive care to patients experiencing acute psychiatric distress. The lack of specific paradigms in this area has significantly influenced the organisational and physical structures and subtype nomenclature, leading to discrepancies and less than optimum recovery-oriented approaches for nursing in PICU.
Page 9 of 24 Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
“What sort of recovery practice would you say you practice?”
The discourse of recovery and comprehensive recovery-oriented systems, infrequently incorporate the practice of recovery principles by health professionals, which also conceive the complexities involved in meeting the needs of people with acute psychiatric distress (Amering and Schmolke, 2009). The rhetoric for a comprehensive, recovery-oriented mental health system determines recovery as a central strategy to reduce the prevalence and impact of mental health problems and mental illness (Caldas, 2011). Recovery is defined as a person’s improved capacity to lead a fulfilled life that is not dominated by illness
and treatment; and a journey toward a new and valued sense of identity, role and
purpose outside the boundaries of mental illness (The State of Queensland, 2008 p.2). For the purposes of this paper, the authors hold a key principle of recovery as valuing the expertise and needs of the individual with lived experience of mental illness in defining knowledge about their own experiences of illness and wellness, and individually negotiated approaches for support and interventions (Gwinner et al., 2012). The Study
Four focus groups were held to ascertain concepts of recovery held by Nurses working in two Psychiatric Intensive Care Units in Queensland, Australia. The focus of the study was to identify the concepts and connected expressions of recovery in relation to PICU, held by nursing professionals. Expressions identified in the focus groups were used to examine current literature for congruency with existing concepts, properties and dimensions. The analysis explicated practical and epistemic basis for nursing practice within PICU environments.
Participants and Ethics
Ethical approval was granted by the University and Health care service Human Research Ethics Committee for an investigation into the Psychiatric Intensive Care with health staff. The participants in the focus groups were nurses who operated within locked wards attached to two metropolitan district hospitals. Nurses were invited to participate in two focus groups, one at the start of the project and one following an integrative review to member check the emerging findings. Participation was voluntary and participants signed a consent form at commencement of the focus groups. The nurse informants identified many nursing practices as fundamental to appropriate and effective intensive care delivery, while also providing insight into the complexities and congruency they face.
Design
The study incorporated a qualitative approach to an integrative review and analysis of the overall data. Other studies have used and advocated an integrative review approach as important to nursing to present the varied
Page 10 of 24Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
perspectives on issues of concern (Dix, 1995, Vinokur-Kaplan, 1995). Integrative reviews can encompass a wide range of purposes: to define concepts, to review theories and evidence, and to analyse procedure from a number of sources (Dix, 1995). Data Collection
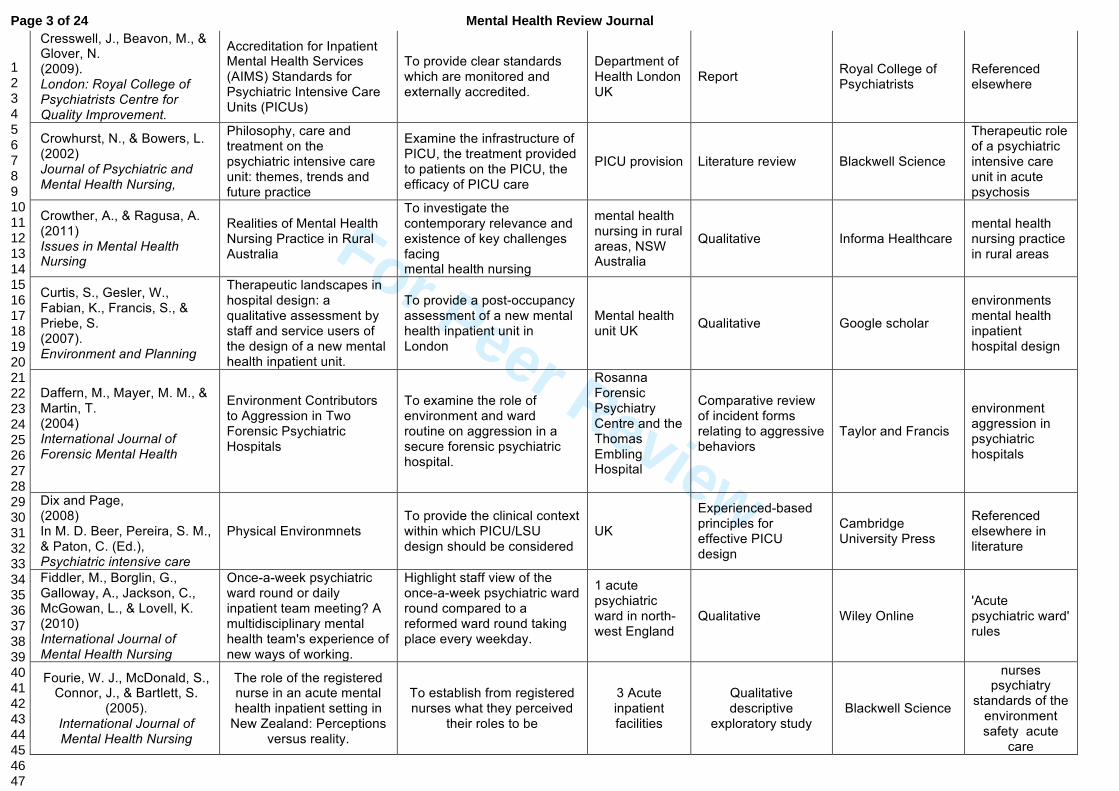
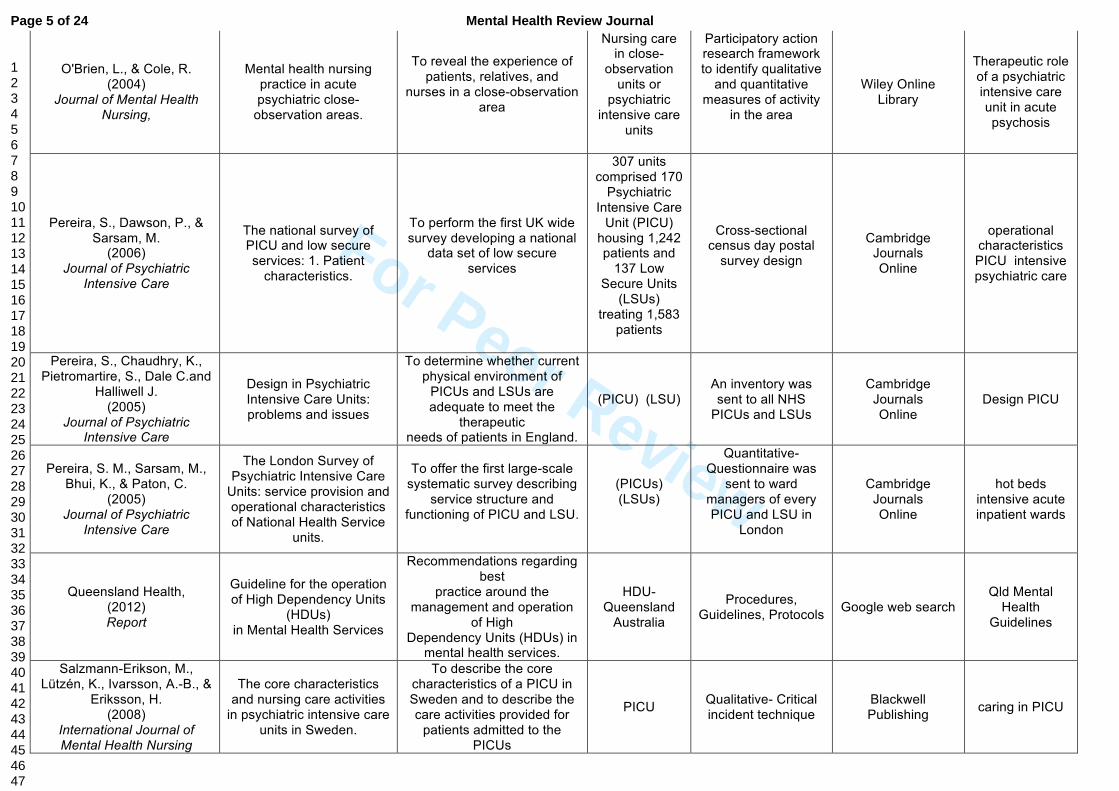
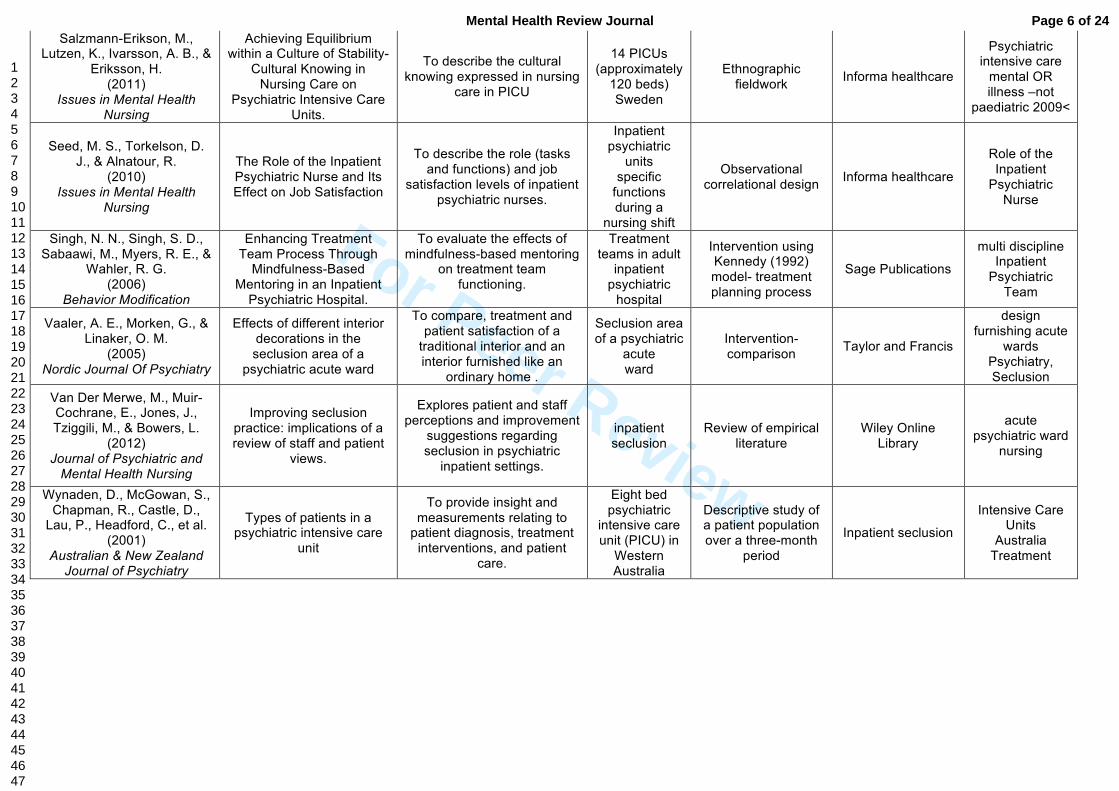
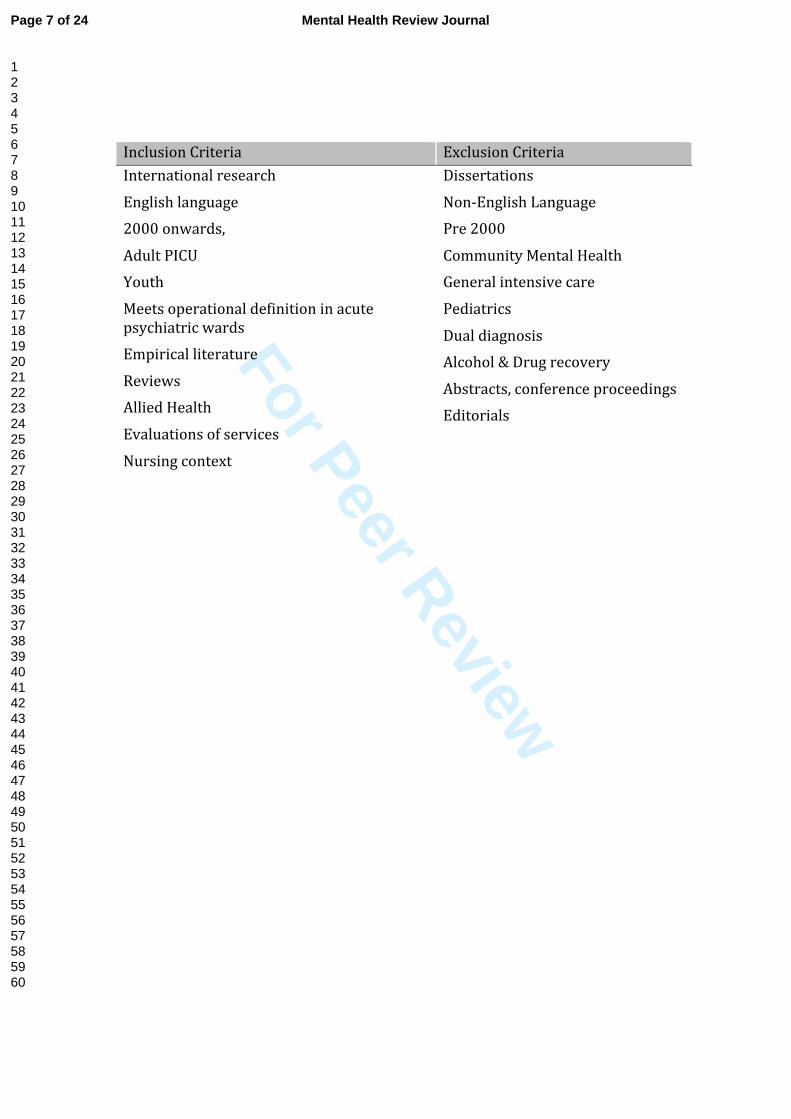
Four focus groups were used to elicit informants’ perspectives on various aspects of nursing and recovery-oriented practices. The data emergent from focus groups was used to identify concerns related to the complexity of psychiatric intensive nursing in PICU and establish the review framework. This approach was essential to provide explicit attention on key purpose, concepts, terms and importantly the boundaries for the literature review process. Review of the literature was done through Google scholar to allow boarder search of databases such as CINAHL, Informa Healthcare Medline, PubMed, PsycARTICLES, and Wiley. Purposive sampling of literature was combined, to enhance variables and expand explanation of the perspectives and definitions expressed in the focus groups. 40 items that met the inclusion criteria (Table 1) and augmented the focus group concerns of psychiatric intensive nursing in PICU are reported on in this article (Table 2).
Table 1. Inclusion and Exclusion criteria
Table 2. Description of the Literature
Data Analysis
A thematic analysis involved a process of examining, comparing and conceptualising, firstly the focus group data to enable recognition of emerging patterns to identify sub-themes and major themes; and secondly dividing the literature into themes related to the perspectives and definitions of the focus group. Theme identification was based on repeated occurrences of dialogue with similar content, both within and across the textual data. The most important and recurring themes in our findings and their corresponding explanatory data were cross-checked among researchers to ensure consensus. In labelling the themes, thick description was used to indicate the context from which they were drawn. The congruencies among informants’ experiences were examined and taken back to informants to corroborate the authenticity and reliability of the interpretation of these understandings. Several sources of data captured the depth and range of issues to be cross-checked, achieving convergent validity of the data (Shih, 1998).
FINDINGS
From the analysis of the data generated through the focus groups, and the literature review, three factors that significantly influenced the function and treatment provided by nursing professionals in PICU were identified; Organisational structures; Physical structures; and Subtype nomenclature. The remainder of this paper provides an interpretative account of each factor with supporting verbatim from the focus groups and the review of literature.
Organisational Structures
Page 11 of 24 Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
The first factor, ‘organisational structures’ encapsulated contradictory
configurations in standards and procedural practice to provide intensive care of patients experiencing acute psychiatric distress. Nurses discussed issues such as different staffing ratios and skill requirements for the treating team, varied necessities for paper work, reporting and developing recovery plans and divergent values in the type of treatment and therapies provided to the patient while in PICU. One nurse proclaimed,
There is no perfect infrastructure but it is about how many clientele you are
going to have in each unit. How many beds you going to have and how that
is really going to be managed. And then of course staffing becomes an issue.
The provision of a balanced approach in PICU pivoted on the logistics of staffing. One informant stated,
PICU can be such a time bomb at times. And then it comes back to shifts and
depending on staff who are coming on shifts. You might lose your regular
staff, you’ve got casuals coming in the whole equation can change very, very
quickly.
Emergent themes were supported and extended in the literature. Studies around intensive and acute settings cited structural and organisational impediments such as understaffing, rapid patient turnover, insufficient beds numbers, and inadequate hospital–community coordination as reasons why recovery is not achieved as an embedded process within hospital settings (Crowther and Ragusa, 2011, Wynaden et al., 2001, Fourie et al., 2005, Cleary et al., 2012). Overall care is delivered through regulators that are often conflicting, with constraints on resources and funding (Bowers et al., 2008, Glick et al., 2003, Fourie et al., 2005).
Unsatisfactory admission of patients whose needs are not adequately met in other services can drive arrangements in PICU (Brown and Bass, 2004, Bowers et al., 2003). An informant from the focus groups perceived PICU as a ‘dumb off
zone’ for people who don’t ‘fit’ criteria for other services models. Other studies have identified patient admissions were more likely to come from court or prison rather than directly from the community, overtly influencing the approach to care (Bowers et al., 2008, Pereira et al., 2005b).
Meanings attached to the idea of care were assumed to prompt the types of treatment available for patients. Rather than providing short-term intensive care in PICU’s data suggests some patient groups remain ‘locked in’ for long periods of time (Bowers et al., 2008 p.62). Brown and Bass (2004) found the length of stay in PICU could range from 1-502+ days. One Nurse in the focus groups talked about the complications of dealing with patients coming through the court system.
…the biggest issue is that we then have to take classified patients. Take
them from the watch house or prison and they are very unwell and
sometimes they stay for long periods of time because of their classification
and the risk they impose and they end up staying and locked in.
Page 12 of 24Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
Poor communication, and a lack of adequate patient/family focused recovery information were evident (Cleary, 2004). When describing admission processes one nurse reflected on the problems associated with gaining appropriate information and knowledge of the patient, their history and their personal choices to initiate recovery processes.
We might have frequent flyers coming from the A&E (Accident and
Emergency department) or wherever, or we might have first timers. So
generally we have frequent flyers we’ve got (information) on what we need
to do, or what’s expected. But when you’ve got first timers that becomes a
different ballpark. That transition of coming … from A&E getting escorted
by a couple of big burley security guards to a PICU area and go ‘oh my god’.
If you have got the relevant information…hopefully they have gathered
enough information that’s going to give us a good grounding on what’s
going to happen and how we are going to start that recovery model, or
process (for the patient).
The literature stipulates the risk involved to supervise acutely disturbed patients in PICU which can threaten the safety of other patients and staff, whilst also being un-conducive to the overall treatment milieu (Bowers et al., 2011, Meehan et al., 2006). O’Brien and Cole (2004), suggest that patients and families consider predictable routine and therapeutic interventions are useful to alleviate acute distress. Furthermore, they found scarce incorporation of the individual needs of patients in care plans and in the overall organisation and treatment of patients. An informant from the focus groups also lamented problems with providing pre-emptive treatment options.
Psychiatric intensive care unit…these people should be intensively cared for,
and it’s a high dependency unit, these people are dependent. So…there
needs to be proactive treatment. You shouldn’t be locked into PICU and
have no… only medication even if they are considered to have improved and
that’s…. I think people haven’t got the idea of what it is. They just see it
(care) as containment.
Despite promotion of multidisciplinary care teams for recovery-oriented approaches (Beer, 2008), and also as a way to improve communication between health care providers (Hopkins et al., 2009), the data indicated implementation of routine multidisciplinary interaction was far from adequate. Informants stated,
We have a full range of 18 psychologists a range of social workers welfare
workers and artists. We've got access to an artist, access to recreational
therapist… But not in PICU!
Their social workers their OTs were meant to visit the patients in PICU. I
never saw any. Surprisingly there is little data in the literature evaluating the delivery, pattern of interactions or effectiveness of multidisciplinary teamwork in PICU (Fiddler et al., 2010). The paucity of research on effective training models in the context of multidisciplinary treatment teams and planning for inpatient mental health care
Page 13 of 24 Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
has been identified elsewhere (Amering and Schmolke, 2009, Singh et al., 2006). However, studies of burnout in nursing have linked; weak nurse-physician relationships; and problems with roles, leadership, clinical accountability, and understanding between professionals to the quality of work life for nurses (Caldwell et al., 2006). The frustrations PICU nurses feel with inadequate collaboration by treatment teams, and to appropriately support patients in a vacuum of information was evident in the other research (Cleary, 2004, Seed et al., 2010) and in the focus group data. One nurse said,
Quite often we are waiting all day for a treating team… for instance one
patient didn't get reviewed by his treatment team last Friday1. I was
completely damming of the fact that treating teams are not seeing people
every day. Well, we are totally pissed off with it. Patient expectancies, requirements and organisational necessities often result in high levels of anxiety for nursing professionals. One informant allegorised,
I think it is just the fact of containment and of course you are the thing that
is keeping them in there… It’s like getting a bad burger at MacDonald’s; it’s
the poor girl that served it that cops it.
Physical Structures
The significance of the environment is summarised in this second theme, ‘physical structures’. Dialogue of layout, security, clinical facilities, recreational facilities, staff and patient safety, fixtures and fittings, garden areas, and private confidential staff areas were raised as concerns to adequately provide care for people experiencing acute psychiatric distress. The data indicated lack of consideration for the design of the physical environments of PICU. One informant stated,
It was never built as a specific… I mean there have been modifications over
the years but it is not ideal. Another informant protested the lack of a ‘standard’ or purpose in the design and
layout of PICU wards.
None of them are purpose built. The closest to purpose built…was forced. My
understanding was it was a very late last minute decision to make that area
a PICU…so what they did was cram in a PICU to a footprint that wasn’t
designed for it. So you have got an inadequate facility. Because in a PICU,
when they are extremely unwell you need space. You need choices for people
to be able to get away from each other.
1 In this instance ‘not being reviewed’ meant it was over 3 days before the psychiatrist assessed the patient, and a treatment/recovery plan initiated.
Page 14 of 24Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
Congruency about the lack of purposefulness in the design of PICU’s was found in literature. Terms like “critical issue impossible to resolve in the current building”
(Pereira et al., 2005b p.75) and “dissatisfaction with the physical environment as a
major issue” (Dix and Mathew, 2008 p. 303), indicated failure to meet acceptable requirements for intensive care (Brennan et al., 2006). Concern was raised of the preoccupation on a risk aversive environment over other important requirements in PICU (Curtis et al., 2007, Cleary et al., 2009b, Daffern et al., 2004). Informants from the focus groups discerned the physical requirements often focused on controlled and locked environments. The environment was described as, more of locked down approach.
A survey cited in Crowhurst and Bowers, (2002 p. 692) determined that patients in PICU are generally dissatisfied with restrictions placed upon their environment. Other studies convey modification of the physical structures and objects through specific rules and routines ‘which could not be questioned by the
patients’ (Salzmann-Erikson et al., 2011 p.8). Informants’ described the setting of PICU as sparse and difficult to reorganise for individual or varied treatment/therapy interventions and lacking simple resources to help orient the patient.
Even simple things like orientation …It wasn’t until I was looking for a clock
in the unit to help a person who didn’t know what day it was and where,
when they were; amongst a range of other things, that I realize we were
bereft of basic things, clocks, the date and the time ...so that I can remember
that today is Wednesday.
An audit of PICU facilities in the UK found that only 35% had en-suite amenities for patients; 25% had no enclosed gardens; 90% of units had separate smoking areas; only half the units had good quality day lighting; 70% of units had an air lock entry to the unit and over half have electronic locking systems; and 35% had no gender specific facilities (Pereira et al., 2005a p. 72). Worryingly dialogue around room configuration raised serious concern for the physical and emotional necessities of female patients, who are evidently at risk as a result of insufficient bedroom arrangements.
There is one double room, which is not really good. I don’t think there
should be double rooms in Acute Observation Areas. …cause, the patients
are so acutely unwell, they don’t want to be in there they don’t want to be
sharing a room. They don’t want to be in there. I had a patient say to me
yesterday. “ You know, why am I ... there is a stranger inside, he is going to
rape me in the middle of the night.” And there is only one toilet, one shower.
A recurrent theme was the need to curtail stimulation for patients in PICUs (Van Der Merwe et al., 2012, Alexander and Bowers, 2004, Lee et al., 2010). One study reported this was achieved through a practice of allowing ‘no stuff’, effectively governing patients’ personal possessions with rules such as, no pictures in the patients’ room (Salzmann-Erikson et al., 2011 p. 262). Informants in the focus groups discussed the rational of establishing low stimulation milieu, as opposed
Page 15 of 24 Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
to establishing routine and providing activity as substantiated methods for reduction to aggression and dormancy. One informant noted,
You use to do your training and you were told about these areas, these non-
stimulating environments, but it has changed with the clientele that are in
there now and they need their stimulation.
These perceptions were also documented in literature (Curtis et al., 2007, Georgieva et al., 2010). Findings from a study in Norway did not support theories that a sparse environment is useful as a method to reduce symptoms of psychopathology and dangerous behaviours (Vaaler et al., 2005). Issues were raised of the confined physical space of PICU and access to appropriate resources that can be used for distraction.
When they are so agitated and so worked up you have to go and confront
these people and try and diffuse the whole situation. You have a metre by
metre to try and diffuse the whole situation. Where as if you had a bit more
area out there where they could kick the ball or punch a bag or what ever
they needed to do that would honestly take away at least 60-70% of your
incidents.’
The physical environment is reported to influence ward practice and affect staff recruitment, retention and confidence (Curtis et al., 2007, Pereira et al., 2006). One informant in the focus groups commented on the impersonal setting of PICU and empathised with patients’ desire to leave.
There is two showers and what they are is a little thing that comes out of
the wall … I don’t think I would even use the shower if I was staying
there…(I) use to think how would I get out if I was a patient in here.
Insight was gained of the lack of consideration, respect and insufficient resources to meet administration requirements in the working environment of the nursing staff in PICU.
The office is actually, has supposedly been an airlock. But it is our office.
For staff to actually have some quarantine time to actually sit without being
distracted to be able to do what they need to complete a recovery plan…you
know actually sit there for 10-15 min in front of the computer and getting
something done.
Lack of respect and provision of sufficient resources to support nurses to deal with complex needs has been highlighted by others (Crowther and Ragusa, 2011, Brennan et al., 2006, Cleary, 2004, Seed et al., 2010). Crowther and Ragusa (2011) distinguished consensus amongst nurses that Commonwealth and State governments had shirked their responsibilities for provision of mental health care for decades. Subtype Nomenclature
The final theme ‘subtype nomenclature’ illustrated the properties and
Page 16 of 24Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
coordination that govern the formation and use of terms assigned to PICU. The relationship between the terms their referents, meanings and the structure of language around intensive acute psychiatric care reflect the context-specific understandings of individuals, resources, experiences and practices. Of particular interest were the differences discussed by the nurse informants in the focus groups, describing contextual boundaries within the larger context of the mental health system. One informant stated,
We call it AOA because we are not allowed to call it HDU (High Dependency Unit). We went to call it HDU and they said that no that was a medical term.
So we call it AOA. Acute Observation Area.
O’Brien and Cole (2003) describe close-observation units as small 8-10 bed units, similar to PICU, indicating the variance between close-observation units and PICU is a higher than usual observation and safety regime. Close-observation units are normally locked where as PICUs have been reported as being not locked (p. 166). Conversely, suggesting that HDUs maintain tighter security than the AOA, the informants communicated,
We don’t meet the guidelines for HDU in the sense of, for the psych unit,
because….oh our AOA area doesn’t meet the criteria because the HDU has to
be more an enclosed thing with the fencing and stuff like that. Which ours
doesn’t.
Other literature refers to the classification of HDU and low-dependency units (LDU). The terms are differentiated by nurse to-patient staffing ratios of 1:5 within the LDU and 1:3 within the HDU. The configuration of HDU also included two seclusion rooms (Chalmers et al., 2012). Attention to the nomenclature of PICU that reflects the underlying bases of care is essential. Meanings of particular terms have significant implications for the delivery of high quality intensive care. The term PICU is recognised internationally and legitimatised in the UK with the establishment of a manual of standards written primarily for Psychiatric Intensive Care Units (Cresswell et al., 2009). While, Queensland Health’s current guidelines for practice in HDUs are meagre. Additionally the guidelines discourage the use of the term PICU, stating it causes confusion with Paediatric Intensive Care Units (Queensland Health, 2012). In a study to more clearly define the concept of PICU in Sweden, Salzmann-Erikson, Lutz, Ivarsson and Eriksson (2008) found no clear differentiation between acute and intensive psychiatric care according to the Swedish National Board of Health. The elaboration of similarities and differences in the idea of care in PICU can have diverse influences on the manner in which treatment is conceived. Bjorkdahl and Pamestierna (2010) defined a caring continuum in PICU on which nurses adapted two understandings related to the context-specific frameworks of care in PICU. The ballet dancer and the bulldozer:
Page 17 of 24 Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
“One approach involved sensitive and perceptive behaviour on the part
of the nurse, with the intention of generating trust and signalling a
desire to provide care. The other approach was used by the same nurses,
who would then become guardians of the safety and structure in the
ward – sometimes by using force and coercion” (p.512). Classifications systems anchor experience and phenomena into shared understandings. How recovery-oriented care is delivered in PICU is influenced by the terminology that describes the contextual framework. While the term PICU is used more frequently in the literature, to date there is no widely accepted international terminology that defines and guides practice in PICU. The need for new, sophisticated and specialist terms related to intensive psychiatric health care, far beyond traditional notions of containment and pharmacological treatments are urgent. As, in the words of a nurse informant from the focus groups,
It really is a specialist area.
Discussion
A critical reading has been offered of the perceptions understood by nurses, as the vanguard of providing intensive care to patients experiencing acute psychiatric distress. Adopting a recovery-oriented approach for patients experiencing acute psychiatric distress construes the function of PICU as the specialised provision of intensive and efficient treatment. However rudiments, principles and practices shared in the perceptions and descriptions from nurses
demonstrate discrepancies in the provisions, design and classifications of psychiatric intensive care. More often the data assessed for this article denoted the primary function of PICU as the suppression of aggressive and violent behaviour, or ‘a punishment block’ (Dix, 2012 p. 60)
It is timely to review the consequences of engaging in a variety of practices that share only some standards and ideologies that only inadvertently relate to goals of achieving a recovery-oriented approach for people experiencing acute psychiatric distress. Review of the literature based on the nurses’ perceptions exposed the significant need for development, formation, use and application of simple, stable and internationally accepted systems in the conceptual arrangements and contemporary understanding of PICUs.
Findings show that ‘organisational structures’ place considerable demands on nurses to meet configurations that are often contradictory and conflicting (Seed et al., 2010). Staff need consistent support and clearly articulated principles to provide optimum psychiatric intensive care (Macpherson et al., 2005). Staffing issues, insufficient beds numbers and room configurations, and poor multi-discipline team engagement and communication all impacted on the provision of intensive care to patients experiencing acute psychiatric distress. The lack of a clear and coherent ideology for acute psychiatric care is worrying (Bowers, 2005 p. 232). Organisational configurations rarely reported standards or direction beyond recovery rhetoric to encapsulate the meanings individual patients
Page 18 of 24Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
attribute to wellness and illness and the ability to negotiate these. Notwithstanding there is significant indication of beneficial treatment interventions for people experiencing acute psychiatric distress, which can support recovery-oriented approaches (Bowers et al., 2005, Brimblecombe et al., 2007, Lakeman, 2008, Chambers et al., 2012, Janner, 2007, Seed and Torkelson, 2012, Olmos-Gallo et al., 2012).
Positive therapeutic treatment in PICU requires leadership and further research to transform the traditional focus of care on a crisis orientated model in which nurses react to situations, to being proactive in planning individualised nursing interventions (Bowers, 2012). A balanced approach to care and treatment must constructively evaluate the logistics of staffing and clearly identify admission criteria to tackle perception of PICU as a ‘dumb off zone’. There is a critical need for research into the function of multidisciplinary care teams in PICU. Principles of a recovery-oriented approach emphasise a comprehensive service approach (The State of Queensland, 2008) and therefore requires a multidisciplinary approach to care with good communication and information sharing and clear lines of responsibilities and accountability (Cleary and Dowling, 2009). Yet there is very limited literature considering the delivery, pattern of interactions or effectiveness of multidisciplinary teamwork in PICU. Emerging evidence suggests that a security ‘containment’ approach in PICU is no more useful or helpful for recovery than if the person remained in corrective services (Bowers et al., 2012), while evidence suggests that sparse and restrictive environments do not reduce symptoms of psychopathology and dangerous behaviours (Vaaler et al., 2005). The physical structures of PICU also come under criticism in light of the substantial affect on moral and capacity of nursing staff to provide routine activities and therapeutic practices (Gilbody et al., 2006, Anthony, 1993). The lack of universality in the function and paradigms related to PICU demand critical dialogue concerning preferred terms, clarity of procedures and principles of care between nurse and health professionals, governing bodies and people with lived experience of mental illness and treatment in PICU. It is critical to develop globally agreed and shared names, definitions, principles, rules and recommendations to enrich treatment and govern the purpose of PICU as a highly specialised environment. There is need for further research with subsequent research questions and designs aimed at resolving the conflicting function of PICU as the specialised provision of intensive and efficient treatment and as a space for containment.
References
ALEXANDER, J. and BOWERS, L. 2004. Acute psychiatric ward rules: a review of the literature. Journal of Psychiatric and Mental Health Nursing, 11, 623-631.
Page 19 of 24 Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
AMERING, M. and SCHMOLKE, M. 2009. Recovery in mental health: reshaping scientific and clinical responsibilities.
ANTHONY, W. A. 1993. Recovery from mental illness: The guiding vision of the mental health service system in the 1990s. Psychosocial Rehabilitation
Journal, 16, 11-11. AUSTRALASIAN HEALTH INFRASTRUCTURE ALLIANCE 2010. Australasian
Health Facility Guidelines Manual v1.2. In: (AHIA), A. H. I. A. (ed.). NSW. AUSTRALIAN HEALTH MINISTERS 2009. Fourth National Mental Health Plan: An
Agenda for Collaborative Government Action in Mental Health 2009-2014. Commonwealth of Australia Canberra.
BEER, M. D. 2008. Psychiatric intensive care and low secure units: where are we now? Psychiatric Bulletin, 32, 441-443.
BEER, M. D., PEREIRA, S. M., PATON, C., BEER, M. and PEREIRA, S. 2001. Psychiatric intensive care–development and definition. Psychiatric
intensive care, 1-11. BERTOLOTE, J. and MCGORRY, P. 2005. Early intervention and recovery for
young people with early psychosis: consensus statement. The British
Journal of Psychiatry, 187, s116-s119. BJORKDAHL, A., PALMSTIERNA, T. and HANSEBO, G. 2010. The bulldozer and the
ballet dancer: aspects of nurses' caring approaches in acute psychiatric intensive care. Journal of Psychiatric and Mental Health Nursing, 17, 510-518.
BOWERS, L. 2005. Reasons for admission and their implications for the nature of acute inpatient psychiatric nursing. Journal of Psychiatric and Mental
Health Nursing, 12, 231-236. BOWERS, L. 2012. What are PICUs for? Journal of Psychiatric Intensive Care, 1, 1-4. BOWERS, L., CHAPLIN, R., QUIRK, A. and LELLIOTT, P. 2009. A conceptual model
of the aims and functions of acute inpatient psychiatry. Journal of mental
Health, 18, 316-325. BOWERS, L., CROWHURST, N., ALEXANDER, J., EALES, S., GUY, S. and MCCANN, E.
2003. Psychiatric nurses' views on criteria for psychiatric intensive care: acute and intensive care staff compared. International Journal of Nursing
Studies, 40, 145-152. BOWERS, L., HAMMOND, N., JAMES, K., QUIRK, A., ROBSON, D. and STEWART, D.
2012. Characteristics of acute wards associated with the presence of a psychiatric intensive care unit, and transfers of patients to it. Journal of
Psychiatric Intensive Care, 8, 66-77. BOWERS, L., JEFFERY, D., BILGIN, H., JARRETT, M., SIMPSON, A. and JONES, J.
2008. Psychiatric Intensive Care Units: a Literature Review. International
Journal of Social Psychiatry, 54, 56-68. BOWERS, L., SIMPSON, A. and ALEXANDER, J. 2005. Real world application of an
intervention to reduce absconding. Journal of Psychiatric and Mental
Health Nursing, 12, 598-602. BOWERS, L., STEWART, D., PAPADOPOULOS, C., DACK, C., ROSS, J., KHANOM, H.
and JEFFERY, D. 2011. Inpatient violence and aggression: a literature. BRENNAN, G., FLOOD, C. and BOWERS, L. 2006. Constraints and blocks to change
and improvement on acute psychiatric wards -- lessons from the City Nurses project. Journal of Psychiatric and Mental Health Nursing, 13, 475-482.
Page 20 of 24Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
BRIMBLECOMBE, N., TINGLE, A. and MURRELLS, T. 2007. How mental health nursing can best improve service users' experiences and outcomes in inpatient settings: responses to a national consultation. Journal of
Psychiatric and Mental Health Nursing, 14, 503-509. BROWN, S. and BASS, N. 2004. The psychiatric intensive care unit (PICU): patient
characteristics, treatment and outcome. Journal of mental Health, 13, 601-609.
CALDAS, J. M. 2011. Long-Term Mental Health Care For People With Severe Mental Disorders.
CALDWELL, B. A., GILL, K. J., FITZGERALD, E., SCLAFANI, M. and GRANDISON, P. 2006. The Association of Ward Atmosphere with Burnout and Attitudes of Treatment Team Members in a State Psychiatric Hospital. American
Journal of Psychiatric Rehabilitation, 9, 111-129. CHALMERS, A., HARRISON, S., MOLLISON, K., MOLLOY, N. and GRAY, K. 2012.
Establishing sensory-based approaches in mental health inpatient care: a multidisciplinary approach. Australasian Psychiatry, 20, 35-39.
CHAMBERS, M., GILLARD, S., TURNER, K. and BORSCHMANN, R. 2012. Evaluation of an educational practice development programme for staff working in mental health inpatient environments. Journal of Psychiatric and Mental
Health Nursing, no-no. CLEARY, A. and DOWLING, M. 2009. Knowledge and attitudes of mental health
professionals in Ireland to the concept of recovery in mental health: a questionnaire survey. Journal of Psychiatric and Mental Health Nursing, 16, 539-545.
CLEARY, M. 2004. The realities of mental health nursing in acute inpatient environments. International Journal of Mental Health Nursing, 13, 53-60.
CLEARY, M., HORSFALL, J., O'HARA-AARONS, M. and HUNT, G. E. 2012. Mental health nurses’ views of recovery within an acute setting. International
Journal of Mental Health Nursing, n/a-n/a. CLEARY, M., HUNT, G. and WALTER, G. 2009a. A comparison of patient and staff
satisfaction with services after relocating to a new purpose-built mental health facility. Australasian Psychiatry, 17, 212-217.
CLEARY, M., HUNT, G. E., WALTER, G. and ROBERTSON, M. 2009b. Locked inpatient units in modern mental health care: values and practice issues. Journal Of Medical Ethics, 35, 644-646.
COX, A., HAYTER, M. and RUANE, J. 2010. Alternative approaches to ‚"enhanced observations‚" in acute inpatient mental health care: a review of the literature. Journal of Psychiatric and Mental Health Nursing, 17, 162-171.
CRESSWELL, J., BEAVON, M. and GLOVER, N. 2009. Accreditation for Inpatient Mental Health Services (AIMS) Standards for Psychiatric Intensive Care Units (PICUs).
CROWHURST, N. and BOWERS, L. 2002. Philosophy, care and treatment on the psychiatric intensive care unit: themes, trends and future practice. Journal
of Psychiatric and Mental Health Nursing, 9, 689-695. CROWTHER, A. and RAGUSA, A. 2011. Realities of Mental Health Nursing Practice
in Rural Australia. Issues in Mental Health Nursing, 32, 512-518. CURTIS, S., GESLER, W., FABIAN, K., FRANCIS, S. and PRIEBE, S. 2007.
Therapeutic landscapes in hospital design: a qualitative assessment by
Page 21 of 24 Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
staff and service users of the design of a new mental health inpatient unit. Environment and Planning C, 25, 591.
DAFFERN, M., MAYER, M. M. and MARTIN, T. 2004. Environment Contributors to Aggression in Two Forensic Psychiatric Hospitals. International Journal of
Forensic Mental Health, 3, 105-114. DIX, R. 1995. A nurse-led psychiatric intensive care unit. Psychiatric Bulletin, 19,
285-287. DIX, R. 2012. Responding to acute crisis: ways and means. Journal of Psychiatric
Intensive Care, 8, 59-61. DIX, R. and MATHEW, J. P. 2008. Physical enviornment. In: BEER, M. D., PEREIRA,
S. M., and PATON, C. (ed.) Psychiatric intensive care. 2 ed. Cambridge: Cambridge University Press.
FIDDLER, M., BORGLIN, G., GALLOWAY, A., JACKSON, C., MCGOWAN, L. and LOVELL, K. 2010. Once-a-week psychiatric ward round or daily inpatient team meeting? A multidisciplinary mental health team's experience of new ways of working. International Journal of Mental Health Nursing, 19, 119-127.
FOURIE, W. J., MCDONALD, S., CONNOR, J. and BARTLETT, S. 2005. The role of the registered nurse in an acute mental health inpatient setting in New Zealand: Perceptions versus reality. International Journal of Mental Health
Nursing, 14, 134-141. GEORGIEVA, I., DE HAAN, G., SMITH, W. and MULDER, C. L. 2010. Successful
reduction of seclusion in a newly developed psychiatric intensive care unit. Journal of Psychiatric Intensive Care, 6, 31-38.
GERAGHTY, K., MCCANN, K., KING, R. and EICHMANN, K. 2011. Sharing the load: Parents and carers talk to consumer consultants at a child and youth mental health inpatient unit. International Journal of Mental Health
Nursing, 20, 253-262. GILBODY, S., CAHILL, J., BARKHAM, M., RICHARDS, D., BEE, P. and GLANVILLE, J.
2006. Can we improve the morale of staff working in psychiatric units? A systematic review. Journal of mental Health, 15, 7-17.
GLICK, I. D., SHARFSTEIN, S. S. and SCHWARTZ, H. I. 2011. Inpatient Psychiatric Care in the 21st Century: The Need for Reform. Psychiatric Services, 62, 206.
GLICK, I. R., CARTER, W. G. and TANDON, R. 2003. A paradigm for treatment of inpatient psychiatric disorders: from asylum to intensive care. Journal of
Psychiatric Practice®, 9, 395-402. GWINNER, K., KNOX, M. and BROUGH, M. 2012. Making Sense Of Mental Illness
As A Full Human Experience: Perspective of illness and recovery held by people with a mental illness living in the community. Social Work in
Mental Health, null-null. HOPKINS, J. E., LOEB, S. J. and FICK, D. M. 2009. Beyond satisfaction, what service
users expect of inpatient mental health care: a literature review. Journal of
Psychiatric and Mental Health Nursing, 16, 927-937. HORSFALL, J., CLEARY, M. and HUNT, G. E. 2010. Acute Inpatient Units in a
Comprehensive (Integrated) Mental Health System: A Review of the Literature. Issues in Mental Health Nursing, 31, 273-278.
JANNER, M. 2007. From the inside out: Star Wards' lessons from within acute in-patient wards. Journal of Psychiatric Intensive Care, 3, 75-78.
Page 22 of 24Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
LAKEMAN, R. 2008. Practice standards to improve the quality of family and carer participation in adult mental health care: an overview and evaluation. International Journal of Mental Health Nursing, 17, 44-56.
LEE, S. J., COX, A., WHITECROSS, F., WILLIAMS, P. and HOLLANDER, Y. 2010. Sensory assessment and therapy to help reduce seclusion use with service users needing psychiatric intensive care. Journal of Psychiatric Intensive
Care, 6, 83-90. MACPHERSON, R., DIX, R. and MORGAN, S. 2005. A growing evidence base for
management guidelines: Revisiting... Guidelines for the management of acutely disturbed psychiatric patients. Advances in Psychiatric Treatment, 11, 404-415.
MEEHAN, T., FJELDSOE, K., STEDMAN, T. and DURAIAPPAH, V. 2006. Reducing aggressive behaviour and staff injuries: a multi-strategy approach. Australian Health Review, 30, 203-210.
MIGDOLE, S., TONDORA, J., SILVA, M. A., BARRY, A. D., MILLIGAN, J. C., MATTISON, E., RUTLEDGE, W. and POWSNER, S. 2011. Exploring New Frontiers: Recovery-Oriented Peer Support Programming in a Psychiatric ED. American Journal of Psychiatric Rehabilitation, 14, 1-12.
O'BRIEN, L. and COLE, R. 2003. Close-observation areas in acute psychiatric units: A literature review. International Journal of Mental Health Nursing, 12, 165-176.
O'BRIEN, L. and COLE, R. 2004. Mental health nursing practice in acute psychiatric close-observation areas. International Journal of Mental Health
Nursing, 13, 89-99. OLMOS-GALLO, P. A., STARKS, R., LUSCZAKOSKI, K. D. R., HUFF, S. and MOCK, K.
2012. Seven Key Strategies that Work Together to Create Recovery Based Transformation. Community mental health journal, 1-8.
QUEENSLAND HEALTH, Q. 2012. Guideline for the operation of High Dependency Units (HDUs) in Mental Health Services
PAUL, G. L. and MENDITTO, A. A. 1993. Effectiveness of inpatient treatment programs for mentally ill adults in public psychiatric facilities. Applied and
Preventive Psychology, 1, 41-63. PEREIRA, S., DAWSON, P. and SARSAM, M. 2006. The national survey of PICU and
low secure services: 1. Patient characteristics. Journal of Psychiatric
Intensive Care, 2, 7-12. PEREIRA, S. M., CHAUDHRY, K., PIETROMARTIRE, S., DALE, C. and HALLIWELL, J.
2005a. Design in Psychiatric Intensive Care Units: problems and issues. Journal of Psychiatric Intensive Care, 1, 70-76.
PEREIRA, S. M., SARSAM, M., BHUI, K. and PATON, C. 2005b. The London Survey of Psychiatric Intensive Care Units: service provision and operational characteristics of National Health Service units. Journal of Psychiatric
Intensive Care, 1, 7-15. RAMON, S., HEALY, B. and RENOUF, N. 2007. Recovery from mental illness as an
emergent concept and practice in Australia and the UK. International
Journal of Social Psychiatry, 53, 108-122. SALZMANN-ERIKSON, M., LUTZ, K., IVARSSON, A.-B. and ERIKSSON, H. 2011a.
Achieving Equilibrium within a Culture of Stability—Cultural Knowing in Nursing Care on Psychiatric Intensive Care Units. Issues in Mental Health
Nursing, 32, 255-265.
Page 23 of 24 Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
SALZMANN-ERIKSON, M., LÜTZÉN, K., IVARSSON, A.-B. and ERIKSSON, H. 2008. The core characteristics and nursing care activities in psychiatric intensive care units in Sweden. International Journal of Mental Health
Nursing, 17, 98-107. SALZMANN-ERIKSON, M., LUTZEN, K., IVARSSON, A. B. and ERIKSSON, H. 2011.
Achieving Equilibrium within a Culture of Stability-Cultural Knowing in Nursing Care on Psychiatric Intensive Care Units. Issues in Mental Health
Nursing, 32, 255-265. SEED, M. S. and TORKELSON, D. J. 2012. Beginning the Recovery Journey in Acute
Psychiatric Care: Using Concepts from Orem's Self-Care Deficit Nursing Theory. Issues in Mental Health Nursing, 33, 394-398.
SEED, M. S., TORKELSON, D. J. and ALNATOUR, R. 2010. The Role of the Inpatient Psychiatric Nurse and Its Effect on Job Satisfaction. Issues in Mental Health
Nursing, 31, 160-170. SHIH, F.-J. 1998. Triangulation in nursing research: issues of conceptual clarity
and purpose. Journal of Advanced Nursing, 28, 631-641. SINGH, N. N., SINGH, S. D., SABAAWI, M., MYERS, R. E. and WAHLER, R. G. 2006.
Enhancing Treatment Team Process Through Mindfulness-Based Mentoring in an Inpatient Psychiatric Hospital. Behavior Modification, 30, 423-441.
THE STATE OF QUEENSLAND 2008. The Queensland Plan for Mental Health 2007-2017. In: HEALTH, Q. (ed.). Brisbane: Mental Health Branch, Queensland Health, Queensland Government.
VAALER, A. E., MORKEN, G. and LINAKER, O. M. 2005. Effects of different interior decorations in the seclusion area of a psychiatric acute ward. Nordic
Journal Of Psychiatry, 59, 19-24. VAN DER MERWE, M., MUIR-COCHRANE, E., JONES, J., TZIGGILI, M. and BOWERS,
L. 2012. Improving seclusion practice: implications of a review of staff and patient views. Journal of Psychiatric and Mental Health Nursing, no-no.
VINOKUR-KAPLAN, D. 1995. Treatment Teams that Work (and those that don't): An Application of Hackman's Group Effectiveness Model to Interdisciplinary Teams in Psychiatric Hospitals. The Journal of Applied
Behavioral Science, 31, 303-327. WALSH, J. and BOYLE, J. 2009. Improving acute psychiatric hospital services
according to inpatient experiences. A user-led piece of research as a means to empowerment. Issues in Mental Health Nursing, 30, 31-38.
WYNADEN, D., MCGOWAN, S., CHAPMAN, R., CASTLE, D., LAU, P., HEADFORD, C. and FINN, M. 2001. Types of patients in a psychiatric intensive care unit. Australian and New Zealand Journal of Psychiatry, 35, 841-841.
Page 24 of 24Mental Health Review Journal
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960





























