Embed Size (px)
Citation preview

Contents lists available at ScienceDirect
J Ped Surg Case Reports 2 (2014) 85e88
Journal of Pediatric Surgery CASE REPORTS
journal homepage: www.jpscasereports .com
c-KIT positive malignant gastrointestinal stromal tumor in a malechild: A rare case
Sandesh V. Parelkar*, Natasha L. Vageriya, Beejal V. Sanghvi, Devdas S. Samala,Bhupesh A. Paradkar, Sanjay N. OakDepartment of Pediatric Surgery, King Edward Memorial Hospital, E. Borges road, Parel, Mumbai 400012, India
a r t i c l e i n f o
Article history:Received 28 November 2013Received in revised form24 January 2014Accepted 25 January 2014
Key words:Pediatric GISTsEpithelioid varietyImatinib
* Corresponding author. Tel.: þ91 9869039091 (mobE-mail address: [email protected] (S.V. Pa
2213-5766� 2014 The Authors. Published by Elsevierhttp://dx.doi.org/10.1016/j.epsc.2014.01.009
a b s t r a c t
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumors of the gastroin-testinal tract, representing 1e3% of gastrointestinal malignancies. The majority of GISTs present at age50e70 years. Pediatric GISTs are considered to be biologically distinct from adult GISTs. The incidence ofmalignant GISTs is less in children than in adults. Significant clinical and genetic differences are alsonoted between the two. A pediatric case typically affects females; is multifocal; is sited more commonlyin the stomach and follows an indolent course. Histologically, epithelioid morphology is common andgenetically most tumors lack mutations in the KIT or PDGFRA genes. We report a 12 year old male childpresenting with a highly vascular stomach GIST for whom we did a pylorus-preserving wide localexcision. On histopathology it was a malignant variety of GIST of epithelioid type; positive for c-KIT &CD34. The boy is now on Imatinib Mesylate chemotherapy and is asymptomatic.
� 2014 The Authors. Published by Elsevier Inc. Open access under CC BY-NC-ND license.
Gastrointestinal stromal tumors (GISTs) are nonepithelialtumors of connective tissue of the gastrointestinal tract. About60% occur in the stomach, 30% in the small intestine and lessthan 1% in the esophagus. Very rarely do they occur in otherabdominal organs. Smaller tumors are usually benign, especiallywhen cell division rate is slow, but large tumors tend todisseminate to the liver, omentum and peritoneal cavity. Theincidence of GISTs is estimated to be approximately 10e20 permillion people per year, of which 20e30% are malignant. Over90% of GISTs occur in adults over 40 years, with a median ageof 63 years [1e3]. GISTs occurring in the pediatric age groupare extremely rare and form a distinct clinical and molecularsubset from the adult tumors (Table 1). Almost all GISTs diag-nosed in children occur in girls, have multifocal gastric locationand lack oncogenic mutations in KIT or PDGFRA genes [1e3].Infrequently, boys are affected; and in this setting their tumorsusually do not resemble the typical pediatric GISTs phenotype,showing variability in extra-gastric location and/or KIT/PDGFRAmutations [1e3]. We report a rare case of a c-KIT positive
ile).relkar).
Inc. Open access under CC BY-NC-ND
malignant GIST of epithelioid variety occurring in a 12 year oldmale child.
1. Case report
A 12-year old boy presented to uswith complaints of dull-achingcontinuous epigastric pain, nausea and generalized weakness forsix months. He had significant weight loss (4 kg in one month) andalso had a single episode of melena 3 months before. He had sig-nificant pallor and a soft abdomen with no palpable lump. Per-rectal examination was normal. Ultrasound of the abdomenshowed a 6 cm � 6.5 cm heterogenous mass in the lesser saccontinuous with the stomach but free from surrounding structures.Contrast enhanced computerized tomography (CECT) showedextensive breakdown within the mass which was continuous withstomach but free from surrounding structures, without lymph-adenopathy or liver metastases (Fig. 1). An ultrasound guided bi-opsy showed only fibrocollagenous tissue with inflammatory cells.Blood transfusion was given to correct anemia and the child wasexplored through a vertical midline incision. We found a large8� 8 cm vascular and friable mass arising from the lesser curvatureof the stomach with well defined margins. As the mass was veryvascular and friable, and USG guided biopsy was inconclusive formalignancy, only an incisional biopsy was taken. Histopathologyshowed epithelioid cells highly suggestive of GIST with rare
license.

Table 1Typical differences between adult and pediatric GIST.
Adults Pediatrics
Males > female Females > malesCan start anywhere in the GI tract Usually starts in the stomachStarts at a single tumor site May present with multiple stomach
tumors (“multifocal” or“multinodular”)
Rarely metastasizes to the lymphnodes
Lymph node metastases are morecommon
Faster growing Slower growingTumor cells usually have a spindle
shapeTumor cells usually have anepitheloid shape
Has a high response rate to the currentfirst-line drug treatment, ImatinibMesylate
Has an undefined; but generallylower response rate to ImatinibMesylate
Typically has mutations in either KITor PDGFRA genes
Typically does not have KIT orPDGFRA mutations
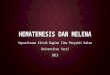
Fig. 2. Intraoperative picture with tumor.
S.V. Parelkar et al. / J Ped Surg Case Reports 2 (2014) 85e8886
possibility of epithelioid hemangioendothelioma. The child was re-explored after 8 days, once the definitive diagnosis of GIST wasmade, and wedge resection of the tumor was done along the lessercurvature with 2 cm normal margin, saving the pylorus (Figs. 2e4).Postoperative course was uneventful. Final histopathology report ofthe mass proved it to be GIST of high malignant potential. Onimmunohistochemistry, the tumor was positive for CD34 & c-KITbut negative for DOG-1, EMA and CK. He was started on ImatinibMesylate chemotherapy (200 mg twice daily) and is continuing thesame without any side effects. Follow up after 1.5 year shows noevidence of recurrence on computed tomography scan (Fig. 5) (notmandatory). Child is growing well, has continued his education.
2. Discussion
GISTs are rare tumors arising from interstitial cells of Cajal,which are normally part of the autonomic nervous system of theintestine. They serve a pacemaker function in controlling motility.The diagnosis of GISTs might have often been missed in the past. Amore stringent definition of the disease and the introduction of aspecific molecular targeted therapy drew attention to it and itsdifferential diagnosis. Thus, the annual incidence which earlier wasthought to be 0.5/100,000, is now almost 1.5/100,000 new cases peryear [4]. These tumors were initially thought to belong to the
Fig. 1. Picture of preoperative computerized tomography scan.
smooth muscle cell family [5]. Later on, cases with nerve sheathdifferentiation were described (gastrointestinal autonomic nervetumors, or GANT, now considered a variant of GISTs), along withcases lacking characteristics of either [6,7]. A relationship to theinterstitial cells of Cajal has now been established on the basis ofsome common phenotypical features of GISTs [4]. The differentialdiagnosis is conventional leiomyosarcomas; however both havedifferent natural history and drug sensitivity [8,9]. Physiologically,the system of interstitial cells of Cajal is involved in the control ofgut motility. In fact, interstitial cells of Cajal are known as thegastrointestinal pacemaker cells, hence the alternative termGIPACT(gastrointestinal pacemaker cell tumors) has been proposed forGISTs.
There are important differences between pediatric GISTs andadult GISTs (Table 1). Pediatric GISTs can be further divided intosubgroups. The most familiar and commonest type is simply called“Pediatric GISTs.” It most commonly affects girls aged 6e18 yearsand almost always starts in the stomach. However, it can occur afterthe age of 18 years [10e12]. The secondwell-known type of GISTs inchildren is called “Carney’s Triad” named after Dr. J. Aidan Carneywho first described it in 1977. Patients with Carney’s triad must
Fig. 3. Intraoperative picture post excision of tumor.

Fig. 4. Picture of specimen.
S.V. Parelkar et al. / J Ped Surg Case Reports 2 (2014) 85e88 87
have two of these different types of tumors; GISTs, pulmonarychondroma, and/or functioning extra-adrenal paraganglioma,particularly if age and sex factors are supportive [10e12].
Two additional subtypes of pediatric GIST which are even rarer;Carney-Stratakis Syndrome (familial paraganglioma and gastricstromal sarcoma) which is familial, and “Neonatal GIST” whichoccurs in newborns.
Emerging evidence suggests that the various forms of pediatricGISTs are related by deficiencies of a protein called succinate de-hydrogenase [10e12]. All female patients and about two-thirds ofmale patients lack activating mutations in KIT/PDGFRA [13,14].Morphologically the tumors have either a predominantly epithe-lioid or mixed epithelioid e spindle cell appearance [13,14].
Pediatric GISTs have indolent clinical behavior, even in thepresence of loco-regional or distant metastatic disease. Long term
Fig. 5. Picture of computerized tomography scan at 1 year follow up.
follow-up of these patients in the pre-Imatinib era showed a pro-longed survival with slow growth and tumor progression even inthe absence of targeted kinase inhibition. These findings suggestdistinct tumor biology of GISTs affecting children, with possiblyalternative molecular mechanisms and signaling pathways down-stream of the KIT receptor.
The clinical findings vary depending on the location and size ofthe tumor at presentation. If the tumor is small, it may be only anincidental finding during radiological imaging or surgery for someother cause, whereas a large exophytic lesion may present as anabdominal mass due to its large size. Lesions in the stomach, smallbowel, or colon may present with gastrointestinal bleed in the formof hematemesis, melena, or occult blood in stools; alternatively,there may be abdominal pain, nausea, and vomiting. An esophagealGIST most commonly presents with dysphagia [15].
As is evident from the case being reported, a pediatric gastricGIST can pose a diagnostic dilemma even after an USG guided bi-opsy and should be considered a differential diagnosis in lesser sactumors despite atypical presentation and in cases of inconclusivebiopsies.
GISTs can occur anywhere along the GI tract, but most often arefound in the stomach or small intestine. The American Joint Com-mittee on Cancer (AJCC) Staging Manual lists the distributions inthis order; stomach (60%), small intestine (30%), rectum (3%), colon(1e2%), esophagus (<1%), omentum/mesentery (rare) [16]. A singlecase has been reported of GISTs occurring in appendix [17].
Because most of these tumors in pediatric as well as adult pa-tients are submucosal in location, they usually attain a large sizewithout causing bowel obstruction by the time of diagnosis [18].Many of these tumors have an exophytic component as they arisefrom the muscularis propria (Marla et al. [19]). Lee et al. [20,21]found GIST to be well-defined tumors with homogenousenhancement, while Levy et al. found large heterogeneouslyenhancing masses due to areas of necrosis or cystic degeneration.They described ulceration as a common feature of GISTs.
Metastases from GISTs in pediatric as well as adult patientscommonly occur to the liver and peritoneal cavity and occasionallysoft tissues, lungs, and pleura. Marla et al. also found that tumorsthat enhanced homogenously (nine out of 53 cases in their series)showed no metastases when they were followed for a mean periodof 2.6 years as compared with those that enhanced heteroge-neously. According to Nilsson et al. [22], at least 50% of these tumorshave metastasis at presentation.
Surgery is the definitive therapy for patients with GISTs. Radicaland complete surgical extirpation offers the only chance for cure.For localized primary GISTs, surgical resection is the mainstay oftherapy with the 5-year survival rate after complete resectionaveraging approximately 50e65%. Surgery is also indicated insymptomatic patients with locally advanced or metastatic disease.Debulking large lesions is helpful when adjuvant therapy withImatinib Mesylate is contemplated.
Preoperative Imatinib should be considered if surgical morbiditywould be improved by cytoreducing the size of the tumor.
Postoperative Imatinib has been shown to increase recurrence-free survival after complete resection of localized GISTs. In 2012,Joensuu et al. showed that 36 months of Imatinib improvedrecurrence free survival and overall survival of GISTs patients with ahigh risk of GIST recurrence, compared with 12 months of adjuvantImatinib.
The optimal follow-up schedules are not known. High-risk pa-tients undergo a routine follow-up with CT scan or MRI every 3e6months for 3 years during adjuvant therapy (with tighter clinicalfollow-up due to the need to manage the side effects of adjuvanttherapy), unless contraindicated, then on cessation of adjuvanttherapy every 3 months for 2 years, then every 6 months until 5

S.V. Parelkar et al. / J Ped Surg Case Reports 2 (2014) 85e8888
years from stopping adjuvant therapy and annually for an addi-tional 5 years. For low-risk tumors, the usefulness of a routinefollow-up is not known; if selected, this is carried out with a CT scanorMRI every 6e12months for 5 years. Very low-risk GISTs probablydo not deserve routine follow-up, although one must be aware thatthe risk is not nil. X-ray exposure is a factor to take into account,with abdominal MRI being an option as an alternative option to a CTscan [23].
Factors such as tumor size, mitotic rate, tumor location, kinasemutational status and occurrence of tumor rupture have beenproposed as predictors of outcome. Adjuvant Imatinib is proposedas an option for those patients with a substantial risk of relapse.Unresectable metastatic or recurrent GISTs can be treated withImatinib, with a remarkable response rate (50e70%) and prolongedsurvival (median progression-free survival: 18e20 months; medianoverall survival: 51e57 months). Sunitinib is licensed as a second-line therapy following progression on Imatinib. Other promisingsystemic therapies include Regorafenib and agents targeting thePI3K/mTOR pathway [24].
3. Conclusion
Gastrointestinal stromal tumors are very rare in pediatric agegroup more so in males, when they are usually c-KIT negative andhave doubtful response to Imatinib. However as is evident in theindexed case, boys may be c-KIT positive and have a better prog-nosis and good response to Imatinib.
References
[1] Kim KM, Kang DW, MoonWS, Park JB, Park CK, Sohn JH, et al, , GastrointestinalStromal Tumor Committee; The Korean Gastrointestinal Pathology StudyGroup. Gastrointestinal stromal tumors in Koreans: incidence and the clinical,pathologic and immunohistochemical findings. J Korean Med Sci 2005;20:977e84.
[2] Tryggvason G, Gislason HG, Magnusson MK, Jónasson JG. Gastrointestinalstromal tumors in Iceland, 1990-2003: the Icelandic GIST study, a population-based incidence and pathologic risk stratification study. Int J Cancer 2005;117:289e93.
[3] Goettsch WG, Bos SD, Breekveldt-Postma N, Casparie M, Herings RM,Hogendoorn PC. Incidence of gastrointestinal stromal tumors is under-estimated: results of a nation-wide study. Eur J Cancer 2005;41:2868e72.
[4] Kindblom L-G, Meis-Kindblom J, Bumming P, Dimitrijevic S, Miret M, Dortok A,et al. Incidence, prevalence, phenotype and biologic spectrum of gastrointes-tinal stromal cell tumors (GIST). A population-based study of 600 cases. AnnOncol 2002;13(Suppl. 5):157.
[5] Kindblom LG, Remotti HE, Aldenborg F, Meis-Kindblom JM. Gastrointestinalpacemaker cell tumor (GIPACT): gastrointestinal stromal tumors show
phenotypic characteristics of the interstitial cells of Cajal. Am J Pathol 1998;152:1259e69.
[6] Lauwers GY, Erlandson RA, Casper ES, Brennan MF, Woodruff JM. Gastroin-testinal autonomic nerve tumors: a clinicopathologic, immunohistochemicaland ultrastructural study of 12 cases. Am J Surg Pathol 1993;17:887e97.
[7] Mazur MT, Clark HB. Gastric stromal tumors. Reappraisal of histogenesis. Am JSurg Pathol 1983;7:507e19.
[8] Plaat BE, Hollema H, Molenaar WM, Torn Broers GH, Pijpe J, Mastik MF, et al.Soft tissue leiomyosarcomas and malignant gastrointestinal stromal tumors:differences in clinical outcome and expression of multidrug resistance pro-teins. J Clin Oncol 2000;18:3211e20.
[9] Clary BM, DeMatteo RP, Lewis JJ, Leung D, Brennan MF. Gastrointestinalstromal tumors and leiomyosarcoma of the abdomen and retroperitoneum: aclinical comparison. Ann Surg Oncol 2001;8:290e9.
[10] Carney JA, Sheps SG, Go VL, Gordon H. The triad of gastric leiomyosarcoma,functioning extra-adrenal paraganglioma and pulmonary chondroma. N Engl JMed 1977;296:1517e8.
[11] Carney JA. Gastric stromal sarcoma, pulmonary chondroma, and extraadrenalparaganglioma (Carney Triad): natural history, adrenocortical component, andpossible familial occurrence. Mayo Clin Proc 1999;74:543e52.
[12] Carney JA, Stratakis CA. Familial paraganglioma and gastric stromal sarcoma: anew syndrome distinct from the Carney triad. Am J Med Genet 2002;108:132e9.
[13] Prakash S, Sarran L, Socci N, DeMatteo RP, Eisenstat J, Greco AM, et al.Gastrointestinal stromal tumors in children and young adults: a clinicopath-ologic, molecular, and genomic study of 15 cases and review of the literature.J Pediatr Hematol Oncol 2005;27:179e87.
[14] Miettinen M, Lasota J, Sobin LH. Gastrointestinal stromal tumors of thestomach in children and young adults: a clinicopathologic, immunohisto-chemical, and molecular genetic study of 44 cases with long-term follow-upand review of the literature. Am J Surg Pathol 2005;29:1373e81.
[15] Miettinen M, Sarlomo-Rikala M, Sobin LH, Lasota J. Esophageal stromal tu-mors: a clinicopathologic, immunohistochemical, and molecular genetic studyof 17 cases and comparison with esophageal leiomyomas and leiomyosarco-mas. Am J Surg Pathol 2000;24:211e22.
[16] Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, editors.Gastrointestinal stromal tumor. AJCC cancer staging manual. 7th ed. NewYork, NY: Springer; 2010. p. 175e80.
[17] Tran S, Dingeldein M, Mengshol SC, Kay S, Chin AC. Incidental GIST after ap-pendectomy in a pediatric patient: a first instance and review of pediatricpatients with CD117 confirmed GISTs. Pediatr Surg Int November 2013.
[18] King M. The radiology of gastrointestinal stromal tumors (GIST). Cancer Im-aging 2005;5:150e6.
[19] Hersh MR, Choi J, Garsett C, Clark R. Imaging gastrointestinal stromal tumors.Cancer Control 2005;12:111e5.
[20] Lee CM, Chen HC, Leung TK, Chen YY. Gastrointestinal stromal tumor:computed tomographic features. World J Gastroenterol 2004;10:2417e8.
[21] Levy AD, Remotti HE, Thompson WM, Sobin LH, Miettinen M. Gastrointestinalstromal tumors: radiologic features with pathologic correlation. Radiographics2003;23:283e304.
[22] Nilsson B, Bümming P, Meis-Kindblom JM, Odén A, Dortok A, Gustavsson B,et al. Gastrointestinal stromal tumors: the incidence, prevalence, clinicalcourse, and prognostication in the preimatinib mesylate era: a population-based study in western Sweden. Cancer 2005;103:821e9.
[23] Gastrointestinal stromal tumors: ESMO Clinical Practice Guidelines for diag-nosis, treatment and follow-up. Ann Oncol 2012;23(Suppl. 7):vii49e55.
[24] Rajendra R, Pollack SM, Jones RL. Management of gastrointestinal stromaltumors. Future Oncol 2013;9:193e206.