Embed Size (px)
Citation preview

C L.,
Enrique Criado, MD, FACS, and Cynthia B. Burnham, BSN, RN, RVT, Chapel Hill, N.c.
Background. The widespread use of ultrasonography for the diagnosis of deep vein thrombosis (DVT)has led to the overuse of ultrasonograPhy with low diagnostic yield. We conducted this study to investi-gate the predictive value of clinical features in the diagnosis of DW and their potential value as clini-cal guidelines for the use of ultrasonograPhic testing in the diagnosis of DVI:Methods. The results of lower-extremity duplex ultrasonograPhic studies and clinical surveys prospec-tively obtained in 1526 patients suspected of having DVT were analyzed.Results. There were 916 inpatients and 610 outpatients. Acute DWwasfound in 16% ofthe inpa-tient duplex scans, and in 12 % of the outpatient studies (P < 0.05). The incidente of acute DVT wasnot different between men and women in inpatient or outpatient populations. Acute DW was found inthe left leg in 60% ofthe outpatient studies, significantly more ojeen (P < 0.001) than in the inpatients(35%). BilateralDW was more common (P < 0.05) in the inpatient population (35%) compared withthe outpatient population (20 %). No difference in the anatomic distribution of thrombosis was foundbetween inpatients and outpatients. The presente of leg symptoms was associated with a significantlyhigher Tale (P < 0.05) of positive studies compared with those patients without leg symptoms in both theinpatient and the outpatient populations. Individual symptoms, risk factors, and Physical findings hadlow positive predictive value and sensitivity for the presente of acute DW on duplex scan. A calf cir-cumference discrepancy of less than 2 cm predicted the absence of DW in 93 % of inpatients and 85 %of outpatients. The combination of a calf circumference discrepancy of less than 2 cm with the absence ofrecent operation, trauma, malignancy, previous history of D~ ar hypercoagulable state predicted theabsence ofDW in 92% ofthe inpatients and 97% ofthe outpatients.Conclusions. Clinical symptoms, risk factors, and Physical findings are poor predictors of the presenteof acute DW on duplex scan. Howeve¡; the absence of a combination of objective clinical factors has
high predictive value for the absence of acute DVT on duplex scan. These criteria may be used to estab-lish clinical guidelines to reduce the use of duplex scanning far the diagnosis of DVI: (Surgery1997;122:578-83.)
From the Division oi Vascular Surge1'Y, University oi North Carolina School oi Medicine, and the PeriPheralVascular Laboratory, University oi North Carolina HosPitals, Chapel HiU, N. C.
increase in fue demand forits use for fue screen-ing and diagnosis of DVT. The indiscriminate useof duplex scanning for the diagnosis of DVT bur-dens noninvasive vascular laboratories with a largenumber of negative tests and decreases its cost-effectiveness.3 In fue current cost-conscious healthcare environment it is important for peripheralvascular laboratories to minimize unnecessary test-ing. We conducted this study to investigate thecharacteristics of patients referred to fue noninva-sive vascular laboratory and to determine whetherobjective clinical criteria could be established toreduce fue number of negative duplex scans per-formed for fue diagnosis ofDVI' among both inpa-tient and outpatient populations.
.
THE LIMITATIONS IN THE clinical diagnosis of deepvein thrombosis (DVf) have be en apparent formore than three decades.l For that reason, physi-cians have relied on the liberal use of differenttests for the diagnosis of DVf, and it has be comecommon practice to obtain noninvasive studies forthe diagnosis of DVf without considering anyobjective clinical criteria to justify such tests.During the last decade fue diagnosis of DVf withduplex scanning has reached high levels of accu-racy.2 The reliability and widespread availability of ,"duplex scanning have produced an explosive
MATERIAL AND METHODSFrom January 1994 to January 1995, 1526
patients undergoing lower-extremity duplex ultra-
Accepted for publicaüon March 16, 1997.
Reprint requests: Enrique Criado, MD, UNC Department ofSurgery, 212 Burnett-Womack Building, CB# 7212, Chapel Hill,NC 27599-7212.
Copyright @ 1997 by Mosby-Year Book, Inc.
0039-6060/97/$5.00 + O 1.1/56/81934
578 SURqERY
Criado and Burnham 579SurgeryVolume 122, Number 3
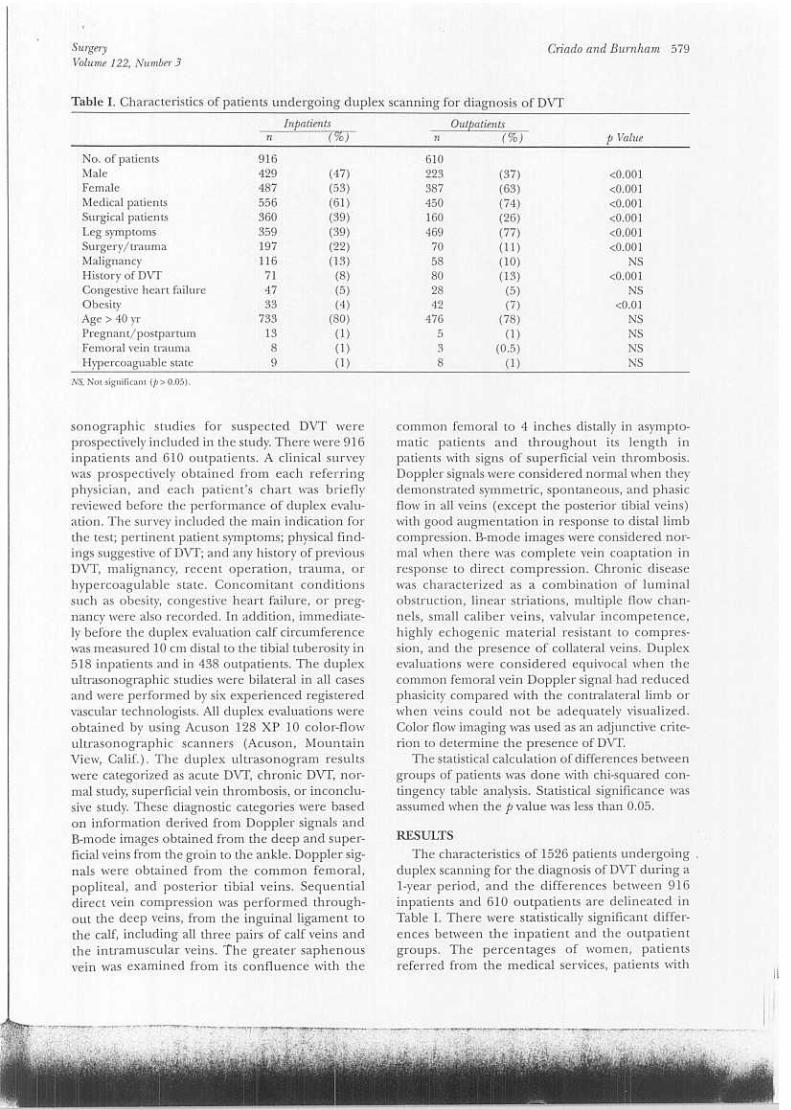
Table l. Characteristics of patients undergoing duplex scanning for diagnosis of OvT
Outf>atientsn (%)
Inpatientsn (%) p Value
No. ofpatients 916 610Male 429 (47) 223 (37) <0.001Female 487 (53) 387 (63) <0.001Medical patients 556 (61) 450 (74) <0.001Surgical patients 360 (39) 160 (26) <0.001Leg symptoms 359 (39) 469 (77) <0.001Surgery/trauma 197 (22) 70 (11) <0.001Malignancy 116 (13) 58 (10) NSHistory of DVf 71 (8) 80 (13) <0.001Congestive heart failure 47 (5) 28 (5) NSObesity 33 (4) 42 (7) <0.01Age > 40 yr 733 (80) 476 (78) NSPregnant/postpartum 13 (1) 5 (1) NSFemoral vein trauma 8 (1) 3 (0.5) NSHypercoaguablestate., 9 (1) 8 (1) NS
NS. Not significant (p> 0.05).
sonographic studies for suspected DVT wereprospectively included in the study. There were 916inpatients and 610 outpatients. A clinical surveywas prospectively obtained from each referringphysician, and each patient's chart was brieflyreviewed before the performance of duplex evalu-ation. The survey included fue main indication forthe test; pertinent patient symptoms; physical find-ings suggestive of DVf; and any history of previousDVT, malignancy, recent operation, trauma, orhypercoagulable state. Concomitant conditionssuch as obesity, congestive heart failure, or preg-nancy were also recorded. In addition, immediate-ly before fue duplex evaluation calf circumferencewas measured 10 cm distal to the tibial tuberosity in518 inpatients and in 438 outpatients. The duplexultrasonographic studies were bilateral in all casesand were performed by six experienced registeredvascular technologists. AlI duplex evaluations wereobtained by using Acuson 128 XP 10 color-flowultrasonographic scanners (Acuson, MountainView, Calif.). The duplex ultrasonogram resultswere categorized as acute DVf, chronic DVT, nor-mal study, superficial vein thrombosis, or inconclu-sive study. These diagnostic categories were basedon information derived from Doppler signals andB-mode images obtained from fue deep and super-ficial veins from the groin to the ankle. Doppler sig-nals were obtained from the common femoral,popliteal, and posterior tibial veins. Sequentialdirect vein compression was performed through-out fue deep veins, from the inguinalligament tofue calf, including all three pairs of calf veins andthe intramuscular veins. The greater saphenousvein was examined from its confluence with the
common femoral to 4 inches distally in asympto-matic patients and throughout its length inpatients with signs of superficial vein thrombosis.Doppler signals were considered normal when theydemonstrated symmetric, spontaneous, and phasicflow in all veins (except the posterior tibial veins)with good augmentation in response to distallimbcompression. B-mode images were considered nor-mal when there was complete vein coaptation inresponse to direct compression. Chronic diseasewas characterized as a combination of luminal.obstruction, linear striations, multiple flow chan-nels, small caliber veins, valvular incompetence,highly echogenic material resistant to compres-sion, and the presence of collateral veins. Duplexevaluations were considered equivocal when thecommon femoral vein Doppler signal had reducedphasicity compared with the contralaterallimb orwhen veins could not be adequately visualized.Color flow imaging was used as an adjunctive crite-rion to determine fue presence of DVf.
The statistical calculation of differences betweengroups of patients was done with chi-squared con-tingency table analysis. Statistical significance wasassumed when fue p value was less than 0.05.
RESULTSThe characteristics of 1526 patients undergoing
duplex scanning for the diagnosis of DVT during a1-year period, and the differences between 916inpatients and 610 outpatients are delineated inTable l. There were statistically significant differ-ences between the inpatient and the outpatientgroups. The percentages of women, patientsreferred from the medical services, patients with
580 Criado and Bumham SurgerySeptember 1997
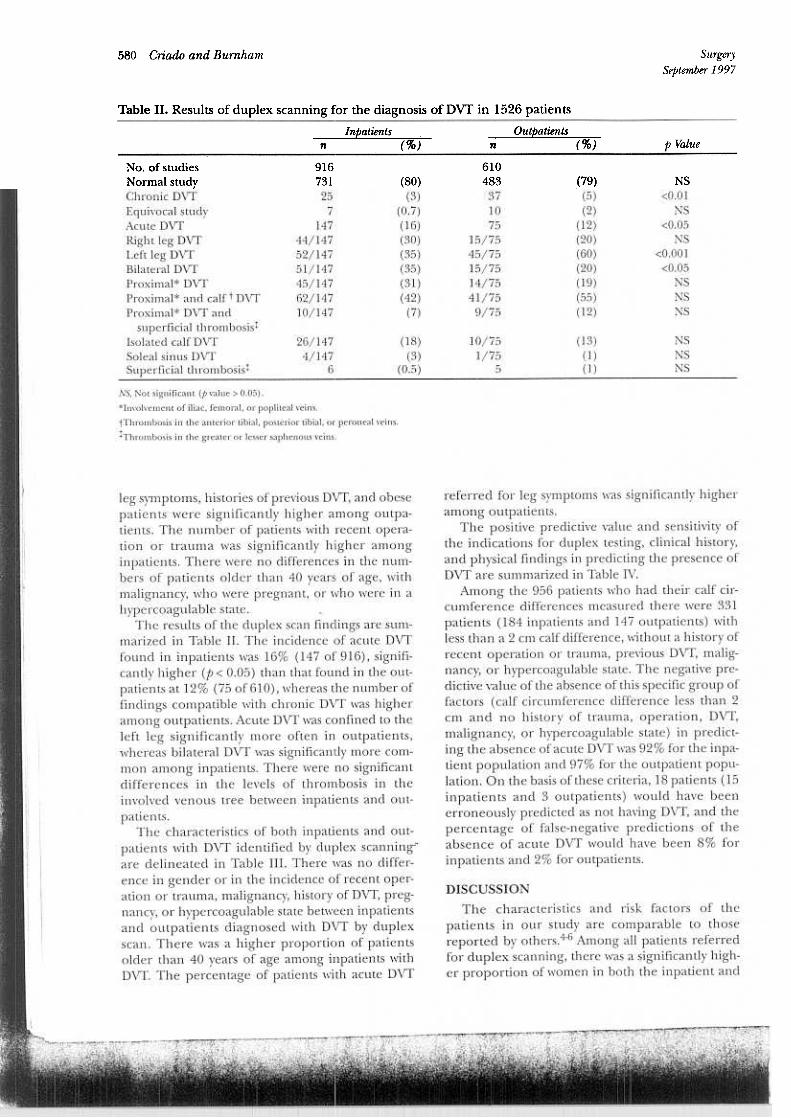
Table 11. Results of duplex scanning for the diagnosis of DVT in 1526 patients
lnpatientsn (%)
Outpatientsn (%) p Value
44/52/51/45/62/10/
610483
371075
15/7545/7515/7514/7541/759/75
(79)(5)(2)
(12)(20)(60)(20)(19)(55)(12)
NS<0.01
NS<0.05
NS<0.001
<0.05NSNSNS
(80)(3)
(0.7)(16)(30)(35)(35)(31)(42)
(7)
(13)(1)(1)
NSNSNS
26/1474/147
6
(18)(3)
(0.5)
10/751/75
5
No. of studiesNormal studyChronic DVf
Equivocal studyAcute DVfRight leg DVfLeft leg DVfBilateral DVfProximal* DVfProximal* and calf t DVfProximal* DVf and
superficial thrombosistIsolated calf DVfSoleal sinus DVfSuperficial thrombosist
NS, Not significant (frvalue > 0.05).
*Involvement of iliac, femoral, or popliteal veins.
tThrombosis in Ihe anterior tibia!, posterior tibial, or peroneal veins.
1:Thrombosis in Ihe greater or lesser saphenous veins.
referred for leg symptoms was significantIy higher
among outpatients.The positive predictive value and sensitivity of
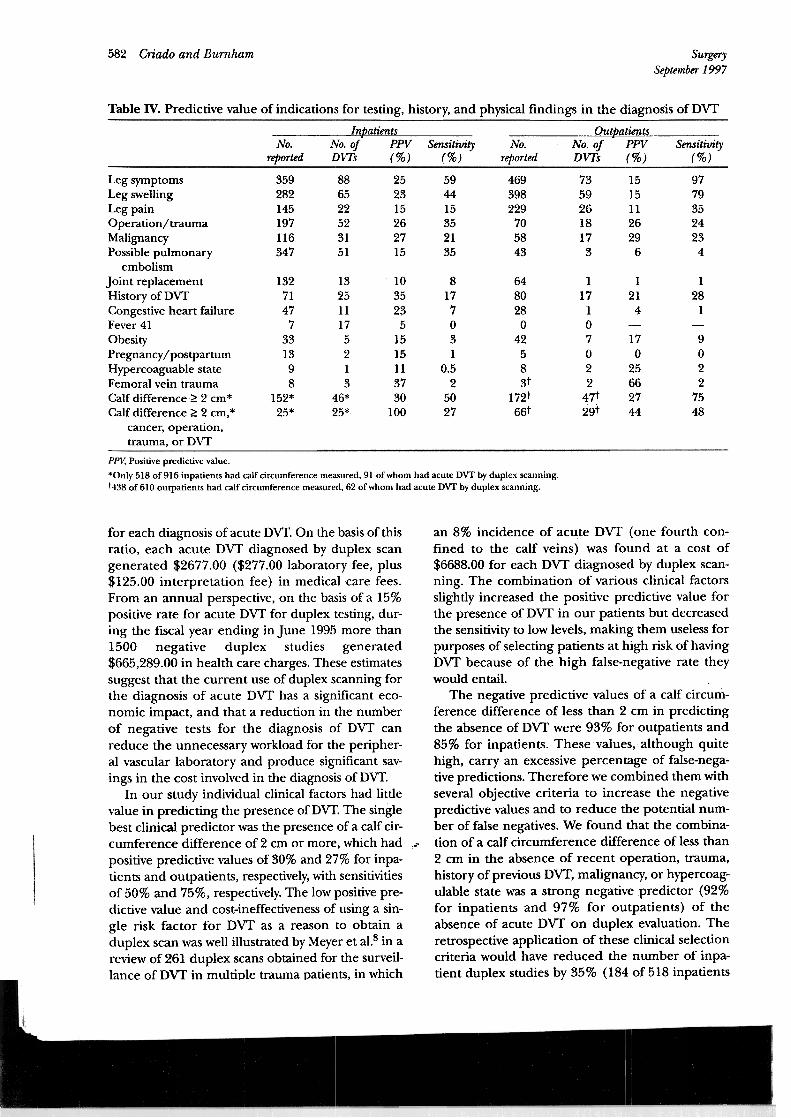
the indications for duplex testing, clinical history,and physical findings in predicting the presence ofDVT are summarized in Table IV.
Among fue 956 patients who had their calf cir-cumference differences measured there were 331patients (184 inpatients and 147 outpatients) withless than a 2 cm calf difference, without a history ofrecent operation or trauma, previous DVT, malig-nancy, or hypercoagulable state. The negative pre-dictive value of fue absence of this specific group offactors (calf circumference difference less than 2cm and no history of trauma, operation, DVT,malignancy, or hypercoagulable state) in predict-ing fue absence of acute DVT was 92% for the inpa-tient population and 97% for the outpatient popu-lation. On fue basis ofthese criteria, 18 patients (15inpatients and 3 outpatients) would have beenerroneously predicted as not having DVT, and fuepercentage of false-negative predictions of theabsence of acute DVT would have been 8% forinpatients and 2% for outpatients.
leg symptoms, histories of previous DVT, and obesepatients were significantly higher among outpa-tients. The number of patients with recent opera-tion or trauma was significantly higher amonginpatients. There were no differences in the num-bers of patients older than 40 years of age, withmalignancy, who were pregnant, or who were in ahypercoagulable state.
The results of the duplex scan findings are sum-marized in Table 11. The incidence of acute DVTfound in inpatients was 16% (147 of 916), signifi-cantly higher (p < 0.05) than that found in fue out-patients at 12% (75 of610), whereas the number offindings compatible with chronic DVT was higheramong outpatients. Acute DVT was confined to theleft leg significantly more often in outpatients,whereas bilateral DVT was significantly more com-mon among inpatients. There were no significantdifferences in the levels of thrombosis in theinvolved venous tree between inpatients and out-
patients.The characteristics of both inpatients and out-
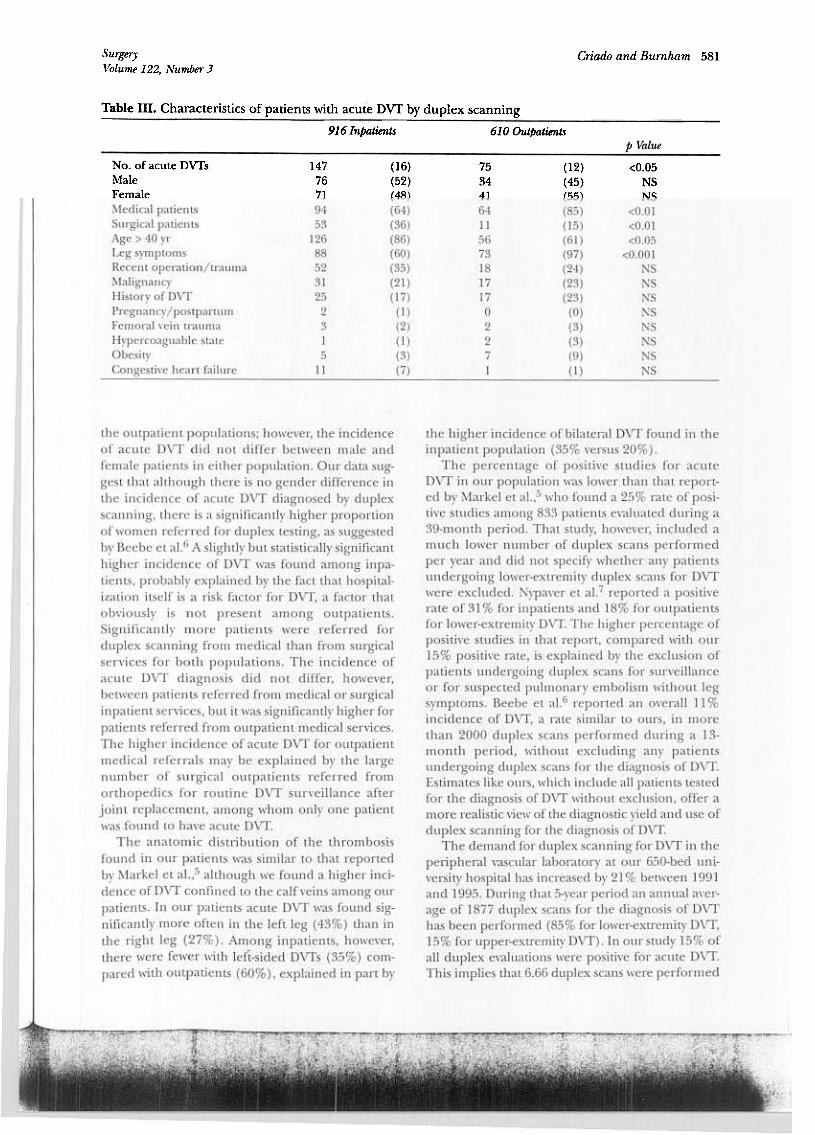
patients with DVT identified by duplex scannin~are delineated in Table III. There was no differ-ence in gender or in the incidence of recent oper-ation or trauma, malignancy, history of DVT, preg-nancy, or hypercoagulable state between inpatientsand outpatients diagnosed with DVT by duplexscan. There was a higher proportion of patientsolder than 40 years of age among inpatients withDVT. The percentage of patients with acute DVT
DISCUSSIONThe characteristics and risk factors of the
patients in our study are comparable to thosereported by others.4-6 Among all patients referredfor duplex scanning, there was a significantly high-er proportion ofwomen in both fue inpatient and
916731
257
147147147147147147147
Criado and Bumham 581SurgeryVolume 122, Number 3
Table 111. Characteristics of patients with acute Dvr by duplex scanning
916 lnpatientsn (%)
610 Out/Jatientsn (%)
No. ofacute DVI's 147 (16) 75 (12) <0.05Male 76 (52) 34 (45) NSFemale 71 (48) 41 (55) NSMedical patients 94 (64) 64 (85) <0.01Surgical patients 53 (36) 11 (15) <0.01Age > 40 yr 126 (86) 56 (61) <0.05Leg syrnptoms 88 (60) 73 (97) <0.001Recent operation/trauma 52 (35) 18 (24) NSMalignancy 31 (21) 17 (23) NSHistoryofDVI' 25 (17) 17 (23) NSPregnancy/postpartum 2 (1) O (O) NSFemoral vein trauma 3 (2) 2 (3) NSHypercoaguable state 1 (1) 2 (3) NSObesity 5 (3) 7 (9) NSCongestive heart failure 11 (7) 1 (1) NS
fue outpatient populations; however, the incidenceof acute DVT did not differ between male andfemale patients in either population. OUT data sug-gest that although there is no gender difference inthe incidence of acute DVT diagnosed by duplexscanning, there is a significantly higher proportionofwomen referred for duplex testing, as suggestedby Beebe et al.6 A slightly but statistically significanthigher incidence of DVT was found among inpa-tients, probably explained by the fact that hospital-ization itself is a risk factor for DVT, a factor thatobviously is not present among outpatients.Significantly more patients were referred forduplex scanning from medical than from surgicalservices for both populations. The incidence ofacute DVT diagnosis did not differ, however,between patients referred from medical or surgicalinpatient services, but it was significantly higher forpatients referred from outpatient medical services.The higher incidence of acute DVT for outpatientmedical referrals mar be explained by the largenumber of surgical outpatients referred fromorthopedics for routine DVT surveillance afterjoint replacement, among whom only one patientwas found to have acute DVT.
The anatomic distribution of the thrombosisfound in OUT patients was similar to that reportedby Markel et al.,5 although we found a higher inci-dence of DVT confined to the calf veins among OUTpatients. In our patients acute DVT was found sig-nificantly more often in fue left leg (43%) than inthe right leg (27%). Among inpatients, however,fueTe were fewer with left-sided DVTs (35%) com-pared with outpatients (60%), explained in part by
the higher incidence of bilateral DVf found in theinpatient population (35% versus 20%).
The percentage of positive studies for acuteDVf in our population was lower than that report-ed by Markel et al.,5 who found a 25% rate of posi-tive studies among 833 patients evaluated during a39-month periodo That study, however, included amuch lower number of duplex scans performedper year and did not specify whether any patientsundergoing lower-extremity duplex scans for DVfwere excluded. Nypaver et al.7 reported a positiverate of 31 % for inpatients and 18% for outpatientsfor lower-extremity DVf. The higher percentage ofpositive studies in that report, compared with our15% positive rate, is explained by the exclusion ofpatients undergoing duplex scans for surveillanceor for suspected pulmonary embolism without legsymptoms. Beebe et al.6 reported an overall 11 %incidence of DVf, a rate similar to ours, in morethan 2000 duplex scans performed during a 13-month period, \vithout excluding any patientsundergoing duplex scans for the diagnosis of DVf.Estimates like ours, which include all patients testedfor the diagnosis of DVT without exclusion, offer amore realistic view of the diagnostic yield and use ofduplex scanning for the diagnosis of DVT.
The demand for duplex scanning for DVf in theperipheral vascular laboratory at our 650-bed un\-versity hospital has increased by 21 % between 1991and 1995. During that 5-year period an annual aver-age of 1877 duplex scans for the diagnosis of DVfhas been performed (85% for lower-extremity DVf,15% for upper-extremity DVf). In our study 15% ofall duplex evaluations were positive for acute DVf.This implies that 6.66 duplex scans were performed
582 Criado and Bumham SurgerySeptember 1997
Table IV. Predictive value of indications for testing, history, and physical findings in fue diagnosis of DVT
OutpatientsNo. No. o/ PPV Smsitivity
reported DVTs (%) (%)
lnpatientsNo. No. oi PPV Sensitivity
rtported DWs (%) (%)
359282145197116347
886522523151
252315262715
594415352135
469398229705843
73592618173
9779352423
4
1515112629
6
13271477
331398
152*25*
132511175213
46*25*
103523
51515113730
100
8177O31
0.52
5027
648028
O
42583t
172t66t
1171O7O2247t29t
121
4
17O
25662744
128
1
9O
22
7548
Leg symptomsLeg swellingLeg painOperation/traumaMalignancyPossible pulmonary
embolismJoint replacementHistory of nVfCongestive heart failureFever 41
ObesityPregnancy IpostpartumHypercoaguable stateFemoral vein traumaCalf difference~ 2 cm*Calf difference ~ 2 cm,*
cancer, operation,trauma, or nVf
PPV; Positive predictive value.
*Olliy 518 of916 inpatients had calf circurnference rneasured, 91 ofwhorn had acute DVf by duplex scanning.t438 of 610 outpatients had calf circurnference rneasured, 62 ofwhorn had acute DVf by duplex scanning.
for each diagnosis of acute DVT. On the basis of thisratio, each acute DVT diagnosed by duplex scangenerated $2677.00 ($277.00 laboratory fee, plus$125.00 interpretation fee) in medical care fees.From an annual perspective, on the basis of a 15%positive rate for acute DVT for duplex testing, dur-ing the fiscal year ending in June 1995 more than1500 negative duplex studies generated$665,289.00 in health care charges. These estimatessuggest that the current use of duplex scanning forthe diagnosis of acute DVT has a significant eco-nomic impact, and that a reduction in the numberof negative tests for the diagnosis of DVT canreduce the unnecessary workload for fue peripher-al vascular laboratory and produce significant sav-ings in the cost involved in fue diagnosis of DVT.
In our study individual clinical factors had littlevalue in predicting the presence of DVT. The singlebest clinical predictor was fue presence of a calf cir-cumference difference of 2 cm or more, which had ...positive predictive values of 30% and 27% for inpa-tients and outpatients, respectively, with sensitivitiesof 50% and 75%, respectively. The low positive pre-dictive value and cost-ineffectiveness of using a sin-gle risk factor for DVT as a reason lo obtain aduplex scan was well illustrated by Meyer et al.8 in areview of 261 duplex scans obtained for the surveil-lance of DVT in multiple trauma patients, in which
an 8% incidence of acure DVT (one fourth con-fined to the calf veins) was found at a cost of$6688.00 for each DVT diagnosed by duplex scan-ning. The combination of various clinical factorsslightly increased the positive predictive value forthe presence of DVT in our patients but decreasedthe sensitivity to low levels, making them useless forpurposes of selecting patients at high risk of havingDVT because of the high false-negative rate theywould entail.
The negative predictive values of a calf circum-ference difference of less than 2 cm in predictingfue absence of DVT were 93% for outpatients and85% for inpatients. Thesevalues, although quitehigh, carry an excessive percentage of false-nega-tive predictions. Therefore we combined them withseveral objective criteria to increase the negativepredictive values and to reduce fue potential nUffi-ber of false negatives. We found that fue combina-tion of a calf circumference difference of less than2 cm in fue absence of recent operation, trauma,history of previous DVT, malignancy, or hypercoag-ulable state was a strong negative predictor (92%for inpatients and 97% for outpatients) of theabsence of acure DVT on duplex evaluation. Theretrospective application of these clinical selectioncriteria would have reduced fue number of inpa-tient duplex studies by 35% (184 of 518 inpatients

~
Criado and Bumham 583SurgeryVolume 122, Number 3
Dosis of DVT remains elusive, our data support thenotion that clinical guidelines can be developed todetermine which patients should not undergoduplex scanning for DVT because of fue very lowlikelihood of positive diagnoses. The safety of clin-ical guidelines established to identify patients inwhom duplex scanning would be unnecessaryshould be prospectively evaluated before beingimplemented.
with calf measurements) and fue number of outpa-tient studies by 34% (147 of 438 outpatients withcalf measurements), albeit at fue risk of missing thediagnosis of DVT in 18 patients (15 inpatients and3 outpatients). Among the 15 DVTs potentiallymissed among inpatients, four had thrombosis con-fined to the calf without popliteal involvement;among the three potential miss es in outpatients,one thrombosis was confined to fue calf, one was acombination of acute and chronic thrombosis, andfue third occurred in a patient being treated withmethotrexate and prednisone for severe rheuma-toid arthritis with limited mobility and who was athigh risk for DVT. Disregarding fue DVTs confinedto the calf veins would reduce the false-negativerates of these clinical criteria from 8% to 6% forinpatients and from 2% to 1.4% for outpatients.The application of these criteria would havedecreased the number of duplex scans by morethan one third, with 527 fewer duplex scans per-formed in 1 year and a reduction of charges ofmore than $210,000, and would have increased theyield of duplex scanning for DVT from 15% to23%. In a similar study Nypaver et al.7 found a96.7% negative predictive value in the diagnosis ofDVT, using more than 7 days' duration of symp-toms, a thigh circumference discrepancy of lessthan 3 cm, and no history of neoplasia as criteria topredict the absence of DVT in a smaller, selectedoutpatient population.
From our data it appears difficult, if not impos-sible, to establish any clinical criteria with high sen-sitivity and high positive predictive value to identifypatients with a high likelihood of having DVT. Onthe other hand, although the positive clinical diag-
REFERENCESl. McLachlinJ, Richards T, PatersonJC. An evaluation of clin-
ical signs in the diagnosis of deep vein thrombosis. ArchSurg 1962;85:738-44.
2. Sumner DS, Mattos MA. Diagnosis of deep vein thrombosiswith real time color and duplex scanning. In: Berstein EF,editor. Vascular diagnosis. 4th ed. Sto Louis: Mosby; 1993. p785-800.
3. Fowl RJ, Strothman GB, BlebeaJ, Rosenthal GJ, KempczinskiRF. Inappropriate use ofvenous duplex scans: an analysis ofindications and results.J Vasc Surg 1996;23:881-6.
4. Anderson FA, Wheeler HB, Goldberg RJ, Straudness DEJr.A population-based perspective of the hospital incidenteand case fatality rates of deep vein thrombosis and pul-monary embolism. Arch Intern Med 1991;151:933-8.
5. Markel A, Manzo RA, Bergelin RO, Hosmer DW,Partwardhan NA, Tovanovic B, et al. Pattern and distribu-tion of thrombi in acute deep vein thrombosis. Arch Surg1992;127:305-9.
6. Beebe HG, Scissons RP, Salles-Cunha SX, Dosick SM,Whalen RC, Gale SS, et al. Gender bias in use of venousultrasonography for diagnosis of deep vein thrombosis. JVasc Surg 1995;22:538-42.
7. Nypaver TJ, Shepard AD, Kiell CS, McPnarlin M, Fenn N,Ernst CB. Outpatient duplex scanning for deep veinthrQmbosis: parameters predictive of a negative study. JVasc Surg 1993;18:821-6.
8. Meyer CS, BlebeaJ, Davis KJr, Fowl RJ, Kempczinski RF.Surveillance venous scans for deep venous thrombosis inmultiple trauma patients. Ann Vasc Surg 1995;9:109-14.