Embed Size (px)
Citation preview
April 1995 SSAT A1221
O FAMILIAL SEGREGATION IN THE OCCURRENCE AND SEVERITY OF
PERIAMPULLARY NEOPLASMS IN FAMILIAL ADENOMATOUS
POLYPOSIS. S. Gallin¢er, L R. Sanabria. R. Croxford. T.C. Berk. Z. Cohen,
and B. Bapat. Departments of Surgery and Pathology, Mount Sinai
Hospital, Steve Atanas Stavro Familial GI Cancer Registry, Department
of Statistics, University of Toronto, Toronto, Ontario, Canada.
Familial Adenomatous Polyposis (FAP) patients often develop
periampullary adenomas which may progress to periampullary cancer.
However, variables that predict the occurrence and severity of
periampullary neoplasms are not we!l understood. The specific a im of this
study was to determine whether the risk of periampullary neoplasia
segregates in PAP families. A total of 144 FAP patients from 74 families
were either screened by gastroduodenoscopy (n=f32) or information was
obtained from surgical or autopsy reports (n=12). The severity of
periampullary neoplasia was recorded for each patient and graded based
on polyp size and histology. A blood sample from at least one member of 50
unrelated families was used to detect germline mutations in codons 686-1693
of the APC gene. Statistically significant familial segregation was found
for the incidence and severity of periampullary neoplasia (p<0.02, linear
regression). Age was also a statistically significant variable (p<0.01). No
correlation was observed between specific APC germline mutations and
periampullary polyp frequency and severity. The occurrence and severity of
periampullary neoplasms in patients with PAP segregates in families. This
familial association may be related to as yet unidentified modifier genes
or perhaps common environmental factors. These results may be useful in
the development of more effective screening protocols for upper endoscopy
in PAP.
R O U T I N E BILE C U L T U R E D U R I N G L A P A R O S C O P I C CHOLECYSTECTOMY IS NOT INDICATED L. Gellman. M. Edye~B. Salky, Division of Laparoscopic Surgery, Mount Sinai Medical Center, New York, New York
Cholecystectomy is the most common intra-abdominal surgical procedure performed numbering over 500,000 cases per year. It has been reported that a positive bile culture may be a significant factor in predicting post-operative complications in patients undergoing biliary surgery. Recommendations for performing bile cultures range from routine use in all patients, to a selective approach. It was the aim of this study to evaluate clinical usefulness and cost effectiveness of routine bile cultures in the era of laparoscopic cholecystectomy.
A da tabase of 1,305 pat ients who u n d e r w e n t laparoscopic cholecysfectomy from March, 1990 to December, 1994 was retrospectively reviewed. There were 1176 elective and 129 acute cases performed. Bile cultures were performed routinely as per hospital protocol at an average patient cost of $51.
The most common isolate from routine culture was a staphylococcal species. There were twelve septic complications (0.9%), including nine wound infections and three bile leaks. Positive bile cultures were not predictive of a septic complication. There were no mortalities in the series. In all nine patients with wound infections, primary treatment was drainage and in no case did a positive culture result influence treatment. In each patient with a bile leak, initial culture was negative. Pr imary treatment was percutaneous or laparoscopic drainage with at tempted endoscopic placement of a biliary stent. At no time were the results of bile cultures used to alter the management of these patients. There were no mortalities in this series.
In patients undergoing laparoscopic cholecystectomy the routine use of intraoperative bile cultures is neither clinically useful nor cost effective. Assuming 90% of cholecysteeomies are performed laparoscopically in the United States, if routine bile culture is eliminated, the potential annual savings is $23 million dollars.
O Ca2+-CALMODULIN DOWNREGULAT1ON ALTERS CHLORIDE SECRETION DURING GALLSTONE FORMATION. D. [. Giursiu. M. Z. Abedia. J. A. Karam. L J. Roslvn. Research and Surgical Services, The Medical College of Pemasylvania and DVAMC. Philadelphia, Permsylvania.
Gallbladder (GB) absorption and biliary Ca 2+ are both increased during gallstone (GS) formation. Recent studies show that Ca2+-CaImodulta (CAM), a mediator of intracelinlar calcium ( [ Ca2+]i ) signal, regulates GB basal Na + and CI transport, with pronounced effects on C1- secretion. However, the role of CAM during GS formation is unknown. We hypothesize that CaM activity is altered during GS formation. Prairie dogs were fed either control chow (n=4) or 1.2% cholesterol diet (n=8) for I to 6 weeks. After overnight fast, animals were anesthetized with ketamine (100mg/kg) and xylazine (1.5mg/kg) and cholecystectomy performed. Gallbladders were examined for the presence of gallstones then designated as either Pre-GS (n=4), or GS (n=4). Tissues were mounted in Ussthg chambers and
unidirectional Ct fluxes (J, geq.cm'2.hr -t) were measured before and after treatment with trifluoperazine (TFP), a potent CaM antagonist. Tissues pre-treated with TFP were then exposed to Ca 2+ ionophore, A23187(A), and fluxes continued.
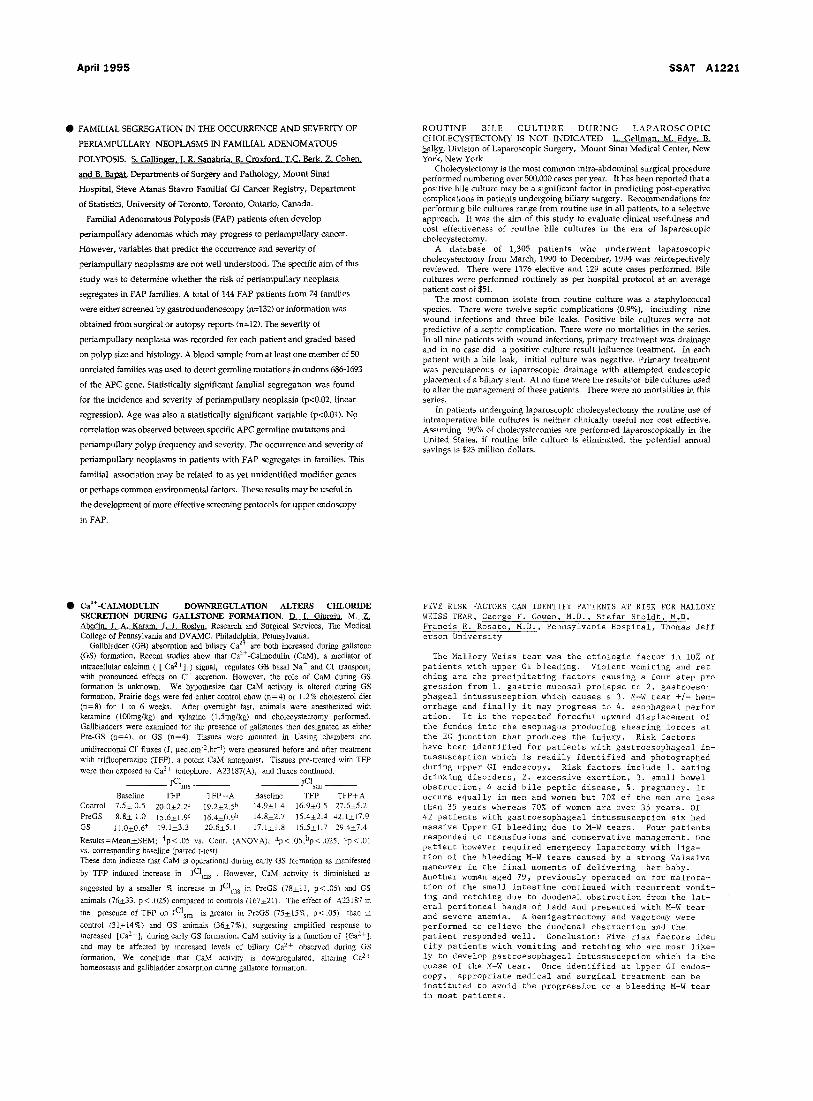
jClms _ _ IClsm _ _
Baseline TFP TFP÷A Baseline TFP TFP+A Control 7.5--+ 0.5 20.0+2.2 c i9.2--2.5 b 14.9--+1.4 16.9-+0.5 27.6+5.2 PreGS 8.8+ 1.0 15.6±1.9 c 16.4+0.9 b i4.8±2.7 15.4--+2.4 42A-+17.9 GS 1t.0-+0.6* i9.1--+3.3 20.6-+5.t 17.1_+I.8 [6.5-+1.7 29.4-+7.4
Results=Mean_+SEM; tp<.05 vs. Cont. (ANOVA); ap<.05,bp<.025, cp<.01 vs. corresponding baseline (paired t-test). These data indicate that CaM is operational during early GS formation as manifested
by TFP induced increase in fCIms . However, CaM activity is diminished as
suggested by a smaller % increase in jCIms in PreGS (78-+11, p<.05) and GS
animals (76__+33, p< .025) compared to controls (I67-+21). The effect of A23187 ha
the presence of TFP on jClsm is greater in PreGg (75-+15%, p<.05) than in
control (31+_14%) and GS animals (36-+7%), suggesting amplified response to increased [Ca2+]i during early GS formation. CaM activity is a functinn of [Ca2+]~ and may be affected by increased levels of biliary Ca 2+ observed during GS formation. We conclude that CaM activity is downregulated, altering Ca 2+ homeostasis and gallbladder absorption during gallstone formation.
FIVE RISK FACTORS CAN IDENTIFY PATIENTS AT RISK FOR MALLORY WEISS TEAR, George F. Gowen, M.D., Stefan Stoldt, M,D. Francis E. Rosato M.D., Pennsylvania Hospital, Thomas Jeff erson University
The Mallory Weiss tear was the etiologic factor in 10% of patients with upper GI bleeding. Violent vomiting and ret ching are the precipitating factors causing a four step pro gression from i. gastric mucosal prolapse to 2. gastroeso- phageal intussusception which causes a 3. M-W tear +/- hem- orrhage and finally it may progress to 4. esophageal perfor ation. It is the repeated forceful upward displacement of the fundus into the esophagus producing shearing forces at the EG junction that produces the injury. Risk factors have been identified for patients with gastroesophageal in- tussusception which is readily identified and photographed during upper GI endoscopy. Risk factors include i. eating drinking disorders, 2. excessive exertion, 3. small bowel obstruction, 4 acid bile peptic disease, 5. pregnancy. It occurs equally in men and women but 70% of the men are less than 35 years whereas 70% of women are over 35 years. Of 42 patients with gastroesophageal intussusception six had massive Upper GI bleeding due to M-W tears. Four patients responded to transfusions and conservative management. One patient however required emergency laparotomy with liga- tion of the bleeding M-W tears caused by a strong Valsalva maneuver in the final moments of delivering her baby. Another woman aged 79, previously operated on for malrota- tion of the small intestine continued with recurrent vomit- ing and retching due to duodenal obstruction from the lat- eral peritoneal bands of Ladd and presented with M-W tear and severe anemia. A hemigastrectomy and vagotomy were performed to relieve the duodenal obstruction and the patient responded well. Conclusion: Five risk factors iden tify patients with vomiting and retching who are most like- ly to develop gastroesophageal intussusception which is the cuase of the M-W tear. Once identified at Upper GI endos- copy, appropriate medical and surgical treatment can be instituted to avoid the progression to a bleeding M-W tear in most patients.