Embed Size (px)
Citation preview

Caesarea, April 2008Caesarea, April 2008
D.Hoelzer D.Hoelzer J.W.Goethe UniversityJ.W.Goethe University
FrankfurtFrankfurt
for the GMALL Study GroupGerman Multicenter Studies for Adult Acute Lymphoblastic Leukemia
Adult ALL – therapeutic strategies, Adult ALL – therapeutic strategies, including Burkitt including Burkitt
and Lymphoblastic Lymphomasand Lymphoblastic Lymphomas
Comprehensive Therapeutic Strategy in Comprehensive Therapeutic Strategy in Acute Lymphoblastic LeukemiaAcute Lymphoblastic Leukemia
1.1. MRD evaluationMRD evaluation
2. New „targeted“ therapies 2. New „targeted“ therapies e.g. Ph+ ALLe.g. Ph+ ALL
33. . Antibody Therapy Antibody Therapy e.g.e.g. B-ALL/Burkitt NHLB-ALL/Burkitt NHL
4. Stem cell transplantation4. Stem cell transplantation
5. New cytostatic drugs5. New cytostatic drugs
6. Treatment of subentities and related 6. Treatment of subentities and related diseasesdiseases e.g. Elderly, Adolescents, T-LBLe.g. Elderly, Adolescents, T-LBL
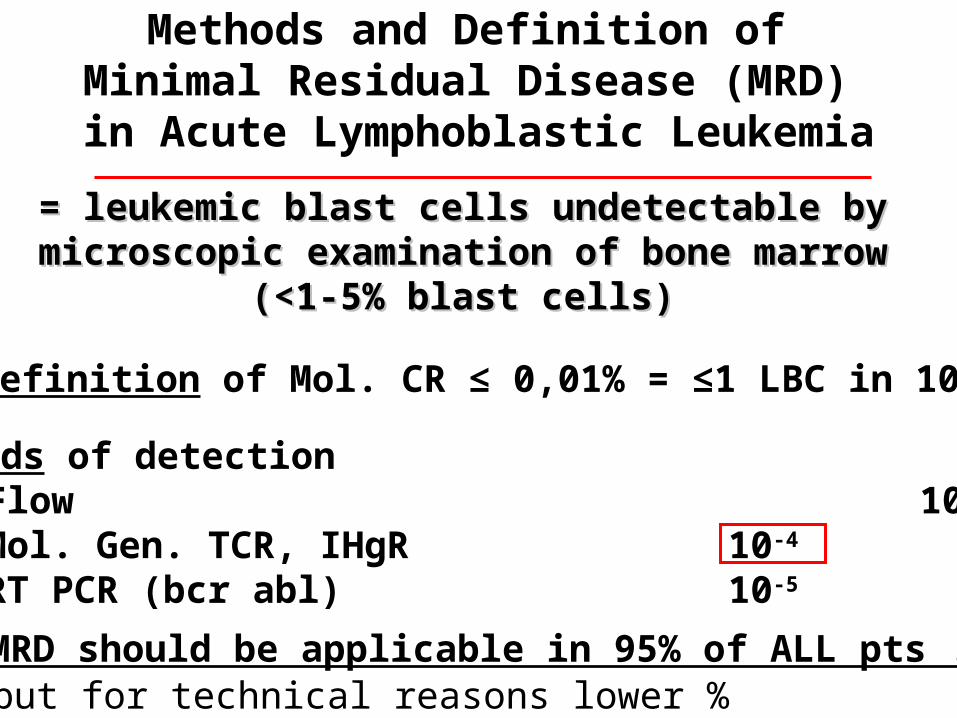
Methods and Definition of Minimal Residual Disease (MRD) in Acute Lymphoblastic Leukemia
= leukemic blast cells undetectable by = leukemic blast cells undetectable by microscopic examination of bone marrowmicroscopic examination of bone marrow
(<1-5% blast cells)(<1-5% blast cells)
• Methods of detection• Flow 10-2 – 10-3
• Mol. Gen. TCR, IHgR 10-4
• RT PCR (bcr abl) 10-5
• MRD should be applicable in 95% of ALL pts !
• Definition of Mol. CR ≤ 0,01% = ≤1 LBC in 10.000
but for technical reasons lower %

Value of MRD for Adult ALL
Induction therapy

1 4 5 7 9 11 13 16 19 22 25 27 30 33 36 39 41 43 46 49 weeks 51 53
Phase I
Induction
Phase II
Cons. I
CNS 24 Gy
i.th. MTX
i.th. Triple prophylaxis
SC-collection
V
(HR/VHR)
Stratification IAccording to Risk Factors
SR
MolecularFailure
HD-MTXASP
I II
ReInduction VM 26ARAC
HD-MTXASP
CYCLOARAC
HD-MTXASP
6 MP 6 MP 6 MP
HRVHR
Med 24 Gy
MRD based German Multicenter Study for Adult ALL – GMALL 07/2003Overview Plan
SCT
Stratification IIaccording to MRD
(6 TPs)
Intens.Maint.
MRDSR
MRD HR
Stop
SZT
MRDIMR

Patientenrekrutierung in laufende GMALL-Studien
de novo N 1921GMALL 07/2003 1135
GMALL für ph+ Pat. < 55 J. 118 GMALL mit Rituximab (SR) 51
GMALL Elderly 1/2003 257GMALL T-LBL 1/2004 58GMALL B-ALL/NHL 2002 471
Rezidivstudien N 171Compound 506U78 (AraG) 140Depocyte für ZNS-Rezidive 19Campath 12
10/07

GroupGroup YearYear NN AgeAge DrugsDrugs Early DeathEarly Death CRCR
CALGB 9111CALGB 9111 19981998 198198 35 35 V,P,D,A,CV,P,D,A,C 8%8% 85%85%
LALA 87LALA 87 20002000 572572 33 (<60)33 (<60) V,P,D/Z,C,[AM/HDAC]V,P,D/Z,C,[AM/HDAC] 9%9% 76%76%
NILG 08/96NILG 08/96 20012001 121121 3535 V,P,I,A,[C]V,P,I,A,[C] 8%8% 84%84%
GMALL 05/93GMALL 05/93 20012001 11631163 35 (<65)35 (<65) V,P,D,A,C,AC,MPV,P,D,A,C,AC,MP 7%7% 83%83%
JALSG-ALL93JALSG-ALL93 20022002 263263 31 (<60)31 (<60) V,P,AD,A,CV,P,AD,A,C 6%6% 78%78%
UCLAUCLA 20022002 8484 27 (<60)27 (<60) V,P,D,AV,P,D,A 1%1% 93%93%
SwedenSweden 20022002 153153 4242 V,BX,D,C,HDACV,BX,D,C,HDAC n.r.n.r. 75%75%
GIMEMA 0288GIMEMA 0288 20022002 767767 28 (<60)28 (<60) V,P,D,A,C, [HDAC,Mi]V,P,D,A,C, [HDAC,Mi] 11%11% 82%82%
MD AndersonMD Anderson 20042004 288288 4040 V,DX,AD,C,HDM,HDACV,DX,AD,C,HDM,HDAC 5%5% 92%92%
EORTC ALL-3EORTC ALL-3 20042004 340340 3333 V,P,D,C,[AM/HDAC]V,P,D,C,[AM/HDAC] n.r.n.r. 74%74%
LALA94LALA94 20042004 922 922 33 (<55)33 (<55) V,P,I/D,CV,P,I/D,C 5%5% 84%84%
GOELAL02*GOELAL02* 20042004 198198 33 (<60)33 (<60) V,P,I,AV,P,I,A 2%2% 86%86%
MRC/ECOGMRC/ECOG 20052005 15211521 (<60) (<60) V,P,D,A,C,AC,MPV,P,D,A,C,AC,MP n.r.n.r. 91%91%
GIMEMA 0496GIMEMA 0496 20052005 450450 (<60) (<60) V,P,D,AV,P,D,A n.r.n.r. 80%80%
Pethema ALL-93*Pethema ALL-93* 20052005 222222 27 (<50)27 (<50) V,D,P,A,CV,D,P,A,C 6%6% 82%82%
NetherlandsNetherlands 20072007 5656 39 (<67)39 (<67) AC,VP,M - V,DX,ADAC,VP,M - V,DX,AD 9%9% 88%88%
JCOG-9004JCOG-9004 20072007 143143 41 (<64)41 (<64) V,C,P,AD,AV,C,P,AD,A 10%10% 83%83%
Results of Recent Trials in Adult ALLResults of Recent Trials in Adult ALLINDUCTION THERAPYINDUCTION THERAPY
N:N: 72627262ED: ED: 7% 7% (2-11%)(2-11%)CR:CR: 84% 84% (74%-93%)(74%-93%)
* HR only

CYTOLOGIC CR Rate after inductionCYTOLOGIC CR Rate after induction GMALL Study 07/2003GMALL Study 07/2003
TotalTotal
EvalEval 713713
CRCR 91%91%
PR/FailPR/Fail 6% 6%
EDED 5% 5%
StandardStandard HighHigh
353353 236 236
92%92% 88%88%
4%4% 9% 9%
4%4% 4% 4%
Very High (Ph+)
119
85% (CH + IMat)
8%
8%
high CR rate for all risk groups !
achievement of hematol. CR important
but no prognostic value for ALL subgroups
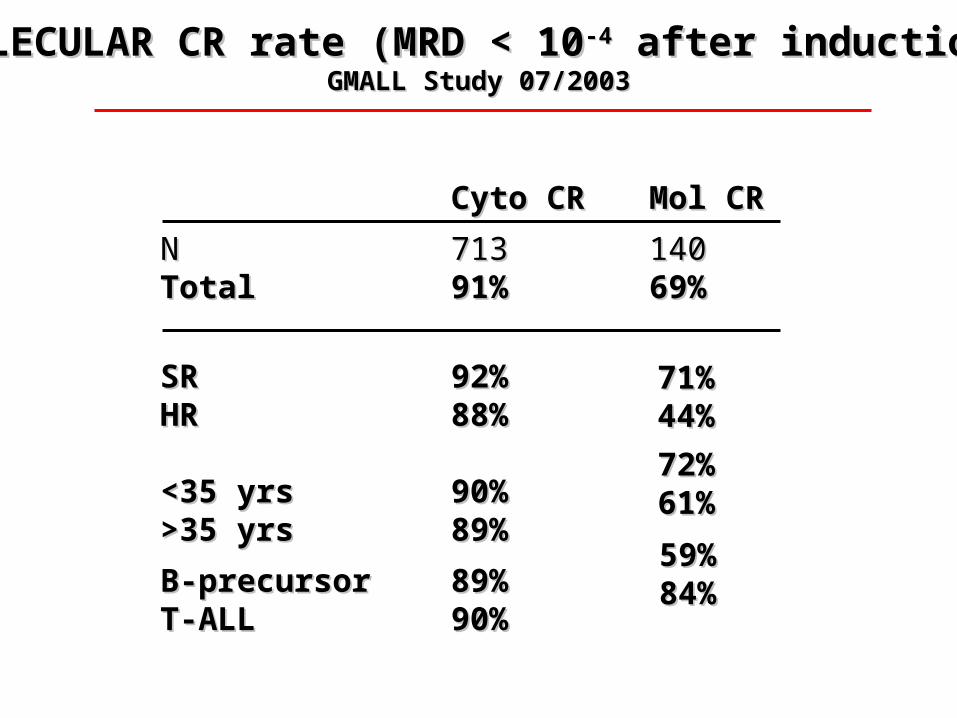
MOLECULAR CR rate (MRD < 10MOLECULAR CR rate (MRD < 10-4-4 after induction) after induction)GMALL Study 07/2003GMALL Study 07/2003
Cyto CRCyto CR Mol CRMol CR
NN 713713 140140TotalTotal 91%91% 69%69%
SRSR 92%92%HRHR 88%88%
<35 yrs<35 yrs 90%90%>35 yrs>35 yrs 89%89%
B-precursorB-precursor 89%89%T-ALLT-ALL 90%90%
71%71%44%44%
72%72%61%61%
59%59%84%84%

Cytologic and Molecular CRSubtype: B vs T
B-Lin N=525 50%T-Lin N=202 60%
Survival of CR Survival of CR
B Mol CR N=82 79%No Mol CR N=48 37%
T Mol CR N=52 68%No Mol CR N=14 28%
B- and T-lineage: need for improvement of Molecular Cr rate

Molecular CR after induction therapy
Conclusion
New endpoint for effectivity ?
Therapeutic consequences ?
Molecular failure Immediate SCT New targeted drugs ?
Molecular CR SCT still in HR/VHR (Ph+) pts ? Proof in randomized studies !

Why do we need MRD evaluation in addition to
„conventional“ risk factors ?
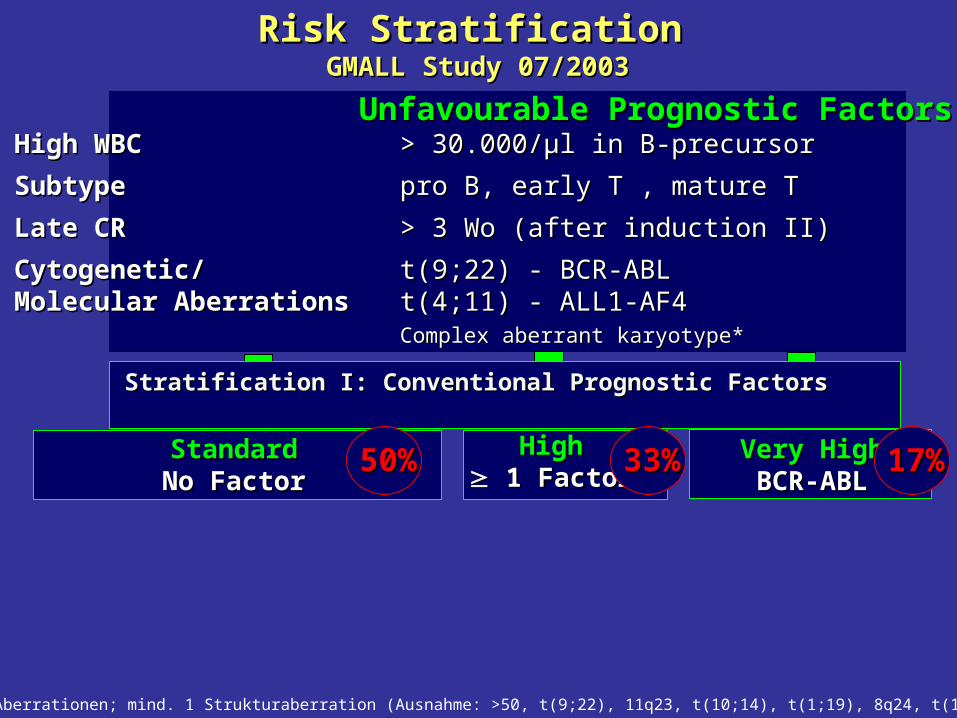
Unfavourable Prognostic FactorsUnfavourable Prognostic FactorsHigh WBC High WBC > 30.000/µl in B-precursor> 30.000/µl in B-precursor
SubtypeSubtype pro B, early T , mature Tpro B, early T , mature T
Late CRLate CR > 3 Wo (after induction II)> 3 Wo (after induction II)
Cytogenetic/Cytogenetic/ t(9;22) - BCR-ABLt(9;22) - BCR-ABLMolecular AberrationsMolecular Aberrations t(4;11) - ALL1-AF4t(4;11) - ALL1-AF4
Complex aberrant karyotype*Complex aberrant karyotype*
Risk StratificationRisk Stratification GMALL Study 07/2003GMALL Study 07/2003
Stratification I: Conventional Prognostic Factors Stratification I: Conventional Prognostic Factors
StandardStandardNo FactorNo Factor
Very HighVery HighBCR-ABLBCR-ABL
HighHigh 1 Factor1 Factor
>=3 Aberrationen; mind. 1 Strukturaberration (Ausnahme: >50, t(9;22), 11q23, t(10;14), t(1;19), 8q24, t(14;18), t(11;14)
50%50% 33%33% 17%17%
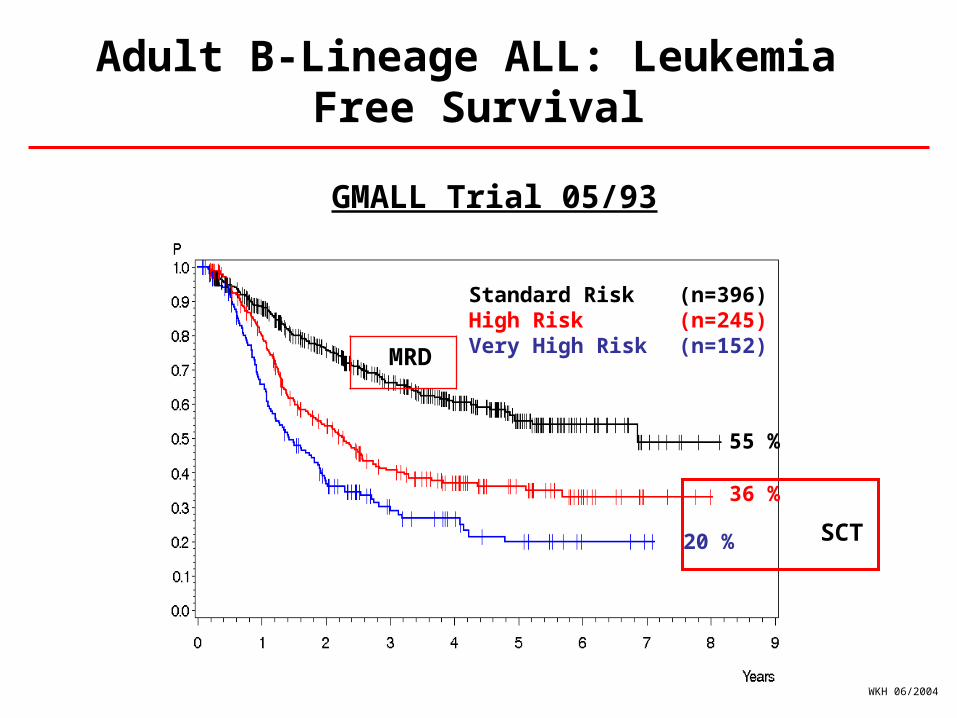
Adult B-Lineage ALL: Leukemia Free Survival
Standard Risk (n=396)High Risk (n=245)Very High Risk (n=152)
55 %
36 %
20 %
GMALL Trial 05/93
WKH 06/2004
SCT
MRD
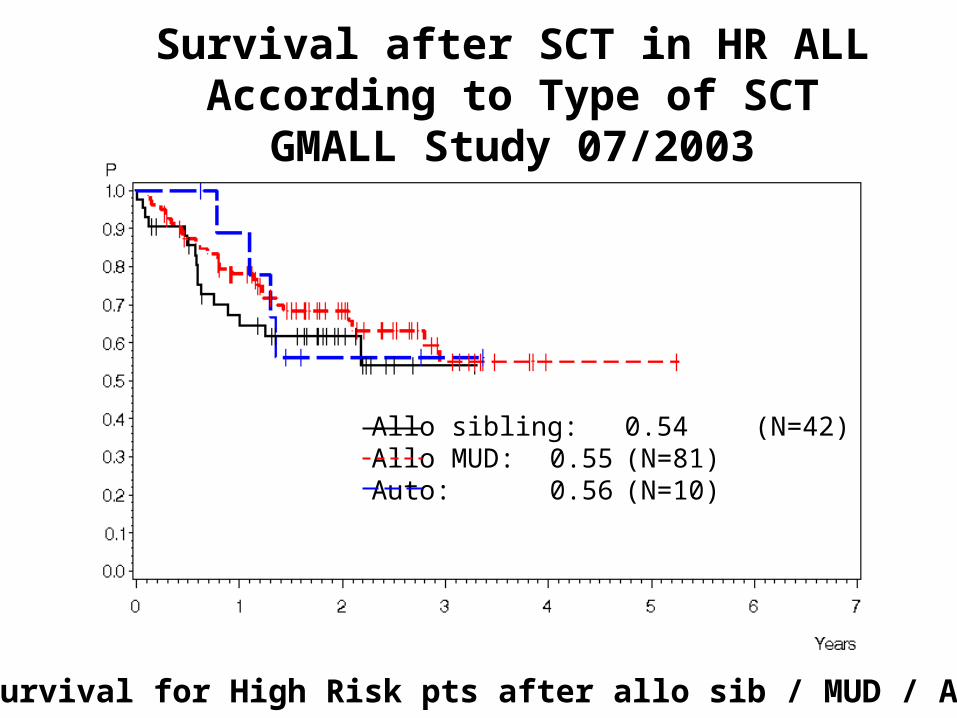
Survival after SCT in HR ALLAccording to Type of SCT
GMALL Study 07/2003
Allo sibling: 0.54 (N=42)Allo MUD: 0.55 (N=81)Auto: 0.56 (N=10)
~ 50% survival for High Risk pts after allo sib / MUD / Auto SCT

Time to achieve Molecular Remission in Standard Risk ALL
Kinetics of Mol.CR in B- and T-Lin.ALLGMALL Studies 06/99 – 07/03
No increase of Mol CR > d 71Lowest MRD level = best time point for SCT
Conclusion MRD in Adult ALL I
Statements mainly based on GMALL 07/2003 experience
1) Molecular CR after induction therapy of greater prognostic impact than cytol. CR
2) „Slow“ decrease / dissapearance of MRD in adult B/T-lin. ALL compared to children
3) Best time point for MRD decision week 16 = after ind.+cond.
• Treatment results before the Imatinib era
• Imatinib / Chemo / SCT in younger patients
• Value of MRD
• Imatinib Mono in Elderly
• Mutations and resistance
• New TK Inhibitors• Dasatinib, Nilotinib, Aurora, others
Ph+ ALL
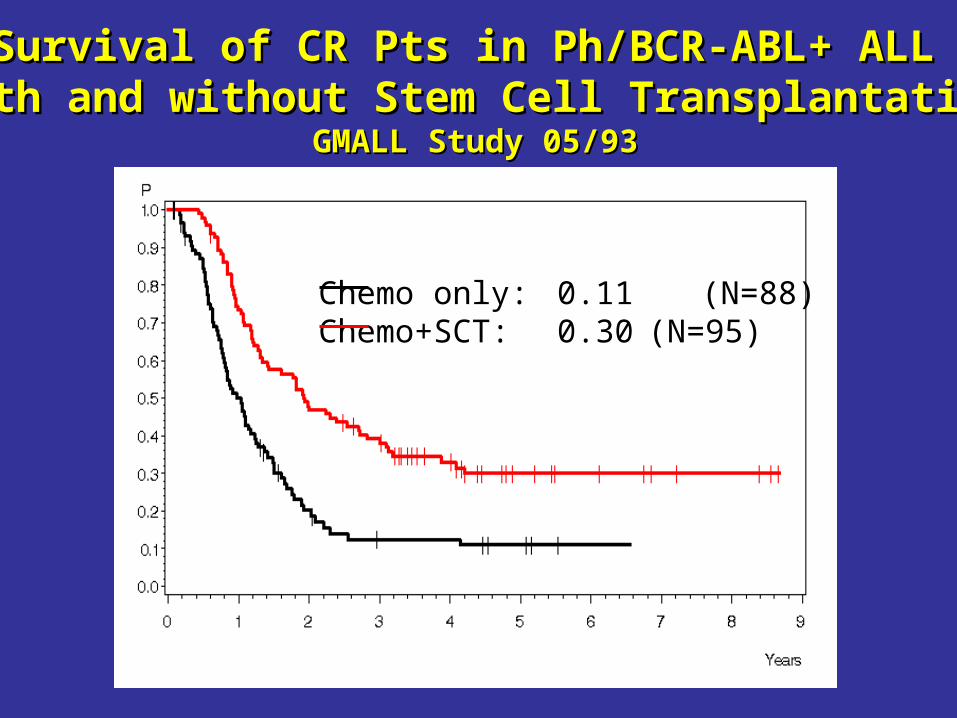
Survival of CR Pts in Ph/BCR-ABL+ ALL Survival of CR Pts in Ph/BCR-ABL+ ALL with and without Stem Cell Transplantationwith and without Stem Cell Transplantation
GMALL Study 05/93GMALL Study 05/93
Chemo only: 0.11 (N=88)Chemo+SCT: 0.30 (N=95)
Imatinib in the Treatment ofAdult Ph+ ALL
Questions• Concomitant with intensive induction therapy ?• Increase in (hemato) toxicity ?
• Other toxicities ?
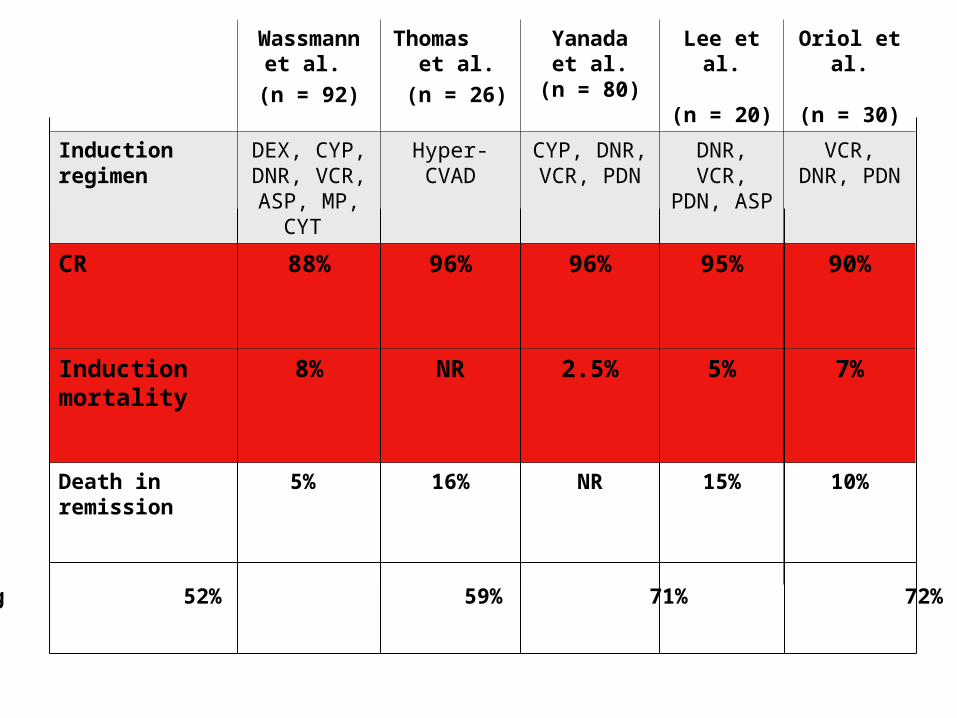
Wassmann et al.
(n = 92)
Thomas et al.
(n = 26)
Yanadaet al.
(n = 80)
Lee et al.
(n = 20)
Oriol et al.
(n = 30)
Induction regimen
DEX, CYP, DNR, VCR,
ASP, MP, CYT
Hyper-CVAD CYP, DNR, VCR, PDN
DNR, VCR, PDN, ASP
VCR, DNR, PDN
CR 88% 96% 96% 95% 90%
Induction mortality
8% NR 2.5% 5% 7%
Death in remission
5% 16% NR 15% 10%
PCR neg 52% 59% 71% 72% n.a.

EFS OS
49%57%
Yanada et al. J Clin Oncol 2006
(+IM)
(-IM)
(+IM)
(-IM)
Event-free and Overall Survival of PH+ ALLComparison of ALL202 (+IM) and ALL93 (-IM)
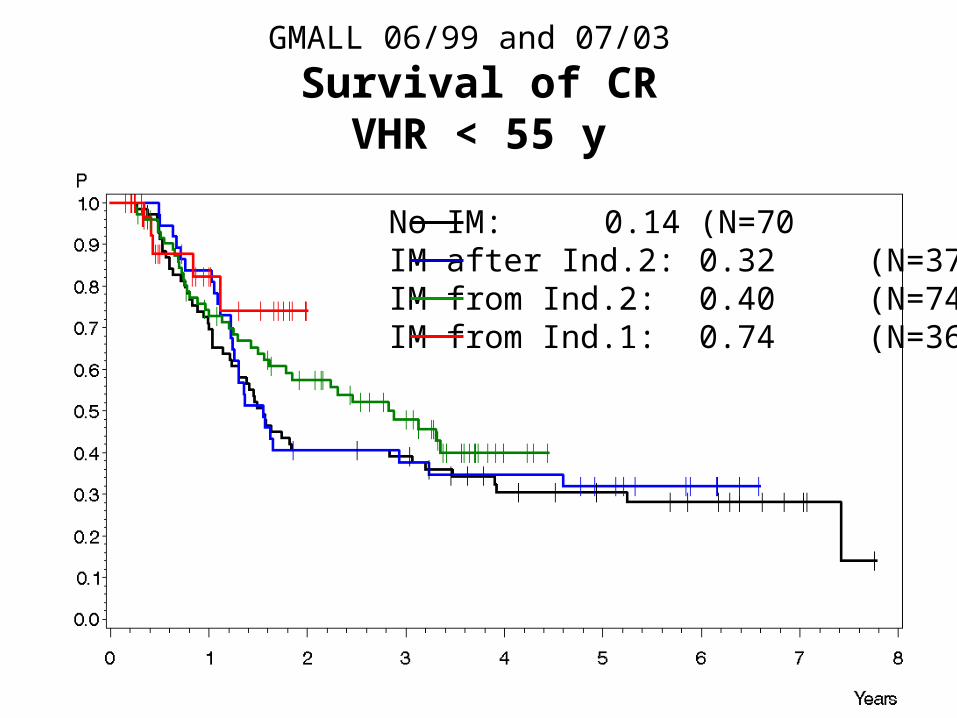
No IM: 0.14 (N=70 IM after Ind.2: 0.32 (N=37)IM from Ind.2: 0.40 (N=74)IM from Ind.1: 0.74 (N=36)
GMALL 06/99 and 07/03
Survival of CRVHR < 55 y
Imatinib in Adult Ph+ ALL (pts 15 – 55 y)Imatinib in Adult Ph+ ALL (pts 15 – 55 y)CONCLUSIONSCONCLUSIONS
• Increase in CR rate from 65-75% to 95%Increase in CR rate from 65-75% to 95%
• Increase in Mol. CR rates from <5% to Increase in Mol. CR rates from <5% to ~~50%50%
• Induction mortality low, but death in CRInduction mortality low, but death in CR
• Improvement in long-term outcome ?Improvement in long-term outcome ?
• Effect on SCT?Effect on SCT?
Treatment of Elderly
Ph+ ALL Patients

Imatinib
Consolidation
Pre-phase R
Randomizedinduction
C1 C2 Reind. C3 C4 [C5]*
weeks 1-4 1 year
Chemo-therapy
Imatinib
Imatinib Versus Chemotherapy Induction
GMALL Trial in Elderly de novo Ph+ ALLN = 55; median age 68 years (58-79)
* Imatinib Mono 400 mg/d for 4 weeks
*CR rate
Induction- 50%Chemo-tx
Imatinib 96%alone
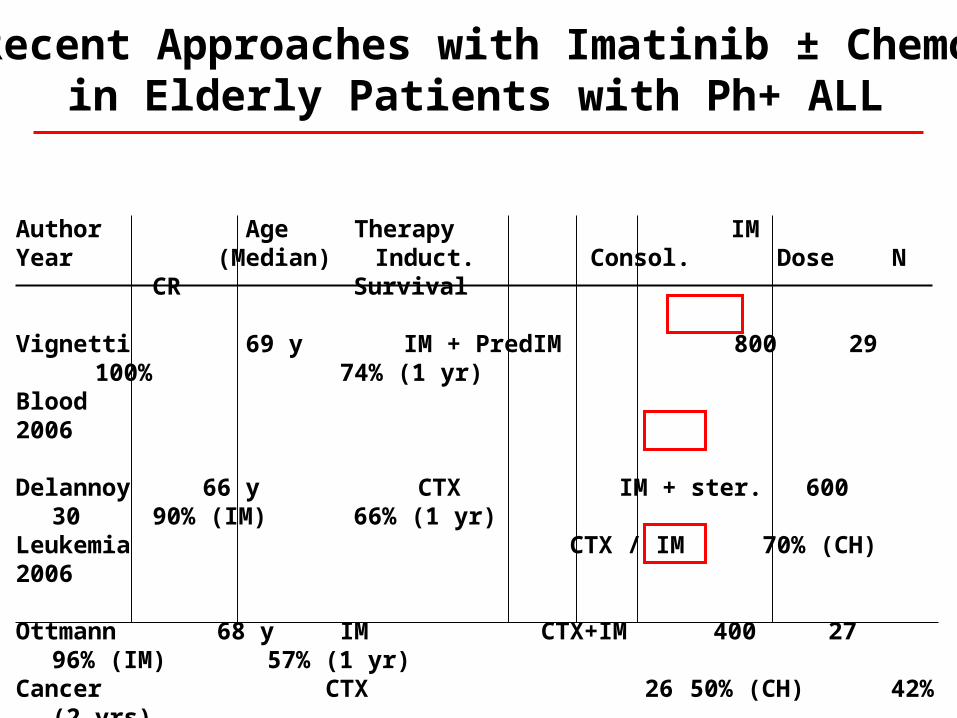
Recent Approaches with Imatinib ± Chemoin Elderly Patients with Ph+ ALL
Author Age Therapy IMYear (Median) Induct. Consol. Dose N CR Survival
Vignetti 69 y IM + Pred IM 800 29 100% 74% (1 yr)Blood 2006
Delannoy 66 y CTX IM + ster. 600 30 90% (IM) 66% (1 yr)Leukemia CTX / IM 70% (CH)2006
Ottmann 68 y IM CTX+IM 400 27 96% (IM) 57% (1 yr)Cancer CTX 26 50% (CH) 42% (2
yrs)2007

0 100 200 300 400 500 600 700 800 900 1000 11000
25
50
75
100 EFS%
GMALLGMALL11
Proba
bility
of dis
ease
-free
survi
val
months
Proba
bility
of dis
ease
-free
survi
val
months
DFS
GIMEMAGIMEMA22
Days Months Months
GRAALLGRAALL33
AFR09(+ IM)
hist. control(no IM)
DFS
1Ottman et al, Cancer 2007;109:2068-76; 2 Vignetti et al. Blood. 2007;109(9):3676-8; 3Delannoy et al., Leukemia. 2006; 20:1526-32.
Imatinib-Based Therapy in Elderly Ph(+) ALL:Comparison of Outcome
High rate of mutations !
Monotherapy with Imatinib in Elderly Ph+ ALLMonotherapy with Imatinib in Elderly Ph+ ALLConclusionsConclusions
Increase of CR rate to >90%,Increase of CR rate to >90%,no induction deathno induction death
Molecular CR rate ~ 40 %Molecular CR rate ~ 40 %
Improvement of median survival from 6 Improvement of median survival from 6 to 12 moto 12 mo
Improvement of quality of life Improvement of quality of life - very low toxicity and- very low toxicity and- partly outpatient treatment- partly outpatient treatment
Outcome impaired due to development Outcome impaired due to development of of resistanceresistance

BCR-ABL Mutations BCR-ABL Mutations
in Ph+ ALLin Ph+ ALL
(GMALL - Elderly)(GMALL - Elderly)
Mechanism of Resistance in Ph+ ALLMechanism of Resistance in Ph+ ALLHofmann et al, Blood & Lancet 2002Hofmann et al, Blood & Lancet 2002
Single point mutation in ATP binding site (e.g. T315I), P-loop or activation loop
Amplification of bcr-abl fusion gene
Up-regulation of bcr-abl transcription
Increase of imatinib efflux / decreased cellular bioavailability
BCR-ABL independence (SRC)

01020304050
60708090
100
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31
01020304050
60708090100
CR CRmol
REL
Time
IMATINIBIMATINIB
% unmutated% unmutatedBCR-ABLBCR-ABL
% mutated% mutatedBCR-ABLBCR-ABL
ChemotherapyChemotherapy
Proportion of Mutant BCR-ABL Alleles in Relation to Treatment Response of de novo Ph+ALL
H.Pfeifer,O.G.Ottmann
Novel Bcr-Abl inhibitors
• AMN107 Novartis• Dasatinib BMS
• VX-680 (L-00128) MSD (T315i)Aurorakinase-Inh.
• SGX70393 Novartis (T315i)
• LBH589 NovartisHDAC-Inhibitor

Experience with Dasatinib in Experience with Dasatinib in front-line Therapy of Ph+ ALLfront-line Therapy of Ph+ ALL
Author N Age Dose CR MolCRChemo
Ravandi 14 55 50 mg bid 93% 46%ASH 2007, #2814 (23-79) HyperCVAD
Foa 23 57 70 mg bid 100% 70%ASH 2007, #7 (30-74) Pred <10-2
Tolerable in combination with chemo Effectivity comparable to Imatinib Long-term results pending
New Drugs in ALL
1.1. NelarabineNelarabine
2.2. ClofarabineClofarabine
3.3. Forodesine HCLForodesine HCL
4.4. BanoxantroneBanoxantrone
5.5. Liposomal ARAC for i.th. use Liposomal ARAC for i.th. use
6.6. Liposomal VCRLiposomal VCR
7.7. Liposomal DNRLiposomal DNR
8.8. Anti CD20Anti CD20
9.9. AntiCD52AntiCD52
10.10. AntiCD33AntiCD33
11.11. AntiCD19 / Tcell engagerAntiCD19 / Tcell engager
12.12. ImatinibImatinib
13.13. NilotinibNilotinib
14.14. DasatinibDasatinib
15.15. Aurorakinase Inhibitors + othersAurorakinase Inhibitors + others
CytostaticsCytostatics
LiposomalLiposomal
AntibodiesAntibodies
Kinase inhibitorsKinase inhibitors
Explored in GMALL studies
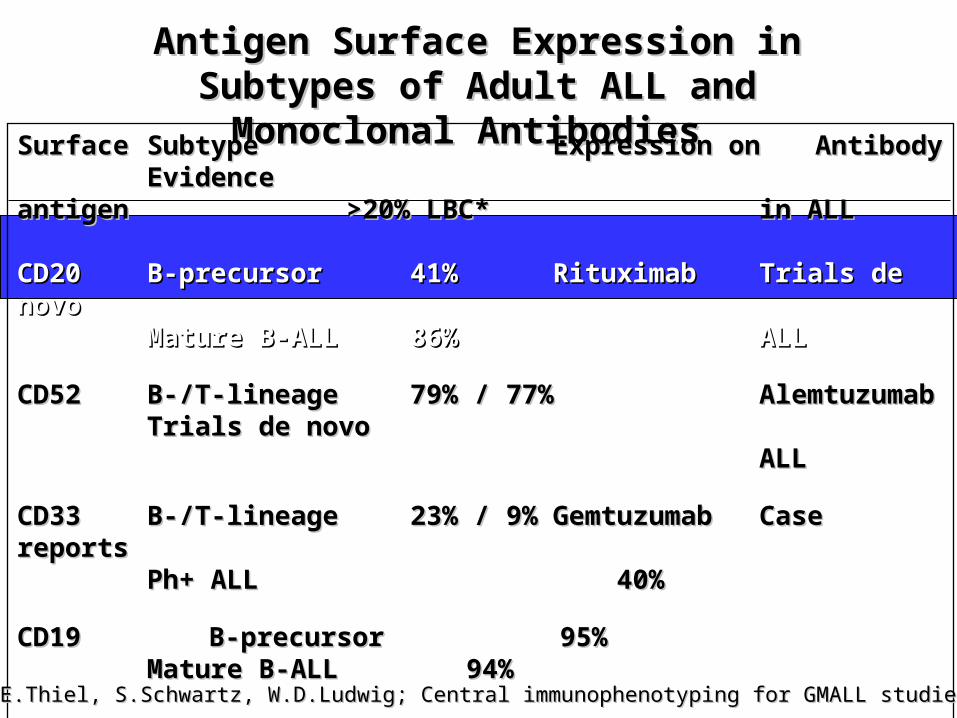
Antigen Surface Expression in Antigen Surface Expression in Subtypes of Adult ALL and Subtypes of Adult ALL and
Monoclonal Antibodies Monoclonal Antibodies Surface Surface SubtypeSubtype Expression onExpression on AntibodyAntibody EvidenceEvidence antigenantigen >20% LBC*>20% LBC* in ALLin ALL
CD20CD20 B-precursorB-precursor 41% 41% RituximabRituximab Trials de novoTrials de novoMature B-ALLMature B-ALL 86% 86% ALLALL
CD52CD52 B-/T-lineageB-/T-lineage 79% / 77% 79% / 77% AlemtuzumabAlemtuzumab Trials de novoTrials de novoALLALL
CD33CD33 B-/T-lineageB-/T-lineage 23% / 9% 23% / 9% GemtuzumabGemtuzumab Case reportsCase reportsPh+ ALLPh+ ALL 40% 40%
CD19 B-precursor 95%CD19 B-precursor 95% Mature B-ALL 94%Mature B-ALL 94%
CD22CD22 B-lineageB-lineage 17% 17% EpratuzumabEpratuzumab
*E.Thiel, S.Schwartz, W.D.Ludwig; Central immunophenotyping for GMALL studies*E.Thiel, S.Schwartz, W.D.Ludwig; Central immunophenotyping for GMALL studies

Rituximab in Different Subentities of Adult ALLRituximab in Different Subentities of Adult ALL
Mature B-ALL / Burkitt‘s NHLMature B-ALL / Burkitt‘s NHL
B-precursor ALLB-precursor ALL-- ElderlyElderly-- YoungerYounger
-- standard riskstandard risk-- high riskhigh risk
Relapsed ALLRelapsed ALL
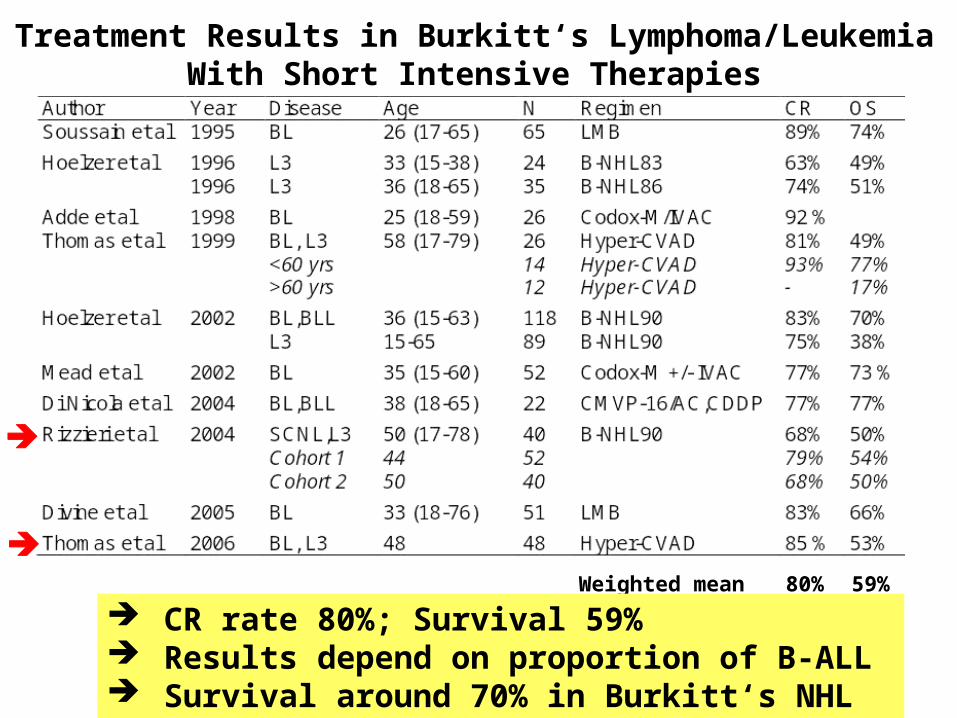
Treatment Results in Burkitt‘s Lymphoma/LeukemiaWith Short Intensive Therapies
Weighted mean 80% 59%
CR rate 80%; Survival 59% Results depend on proportion of B-ALL Survival around 70% in Burkitt‘s NHL
GMALL B-ALL/NHL 2002 Trial
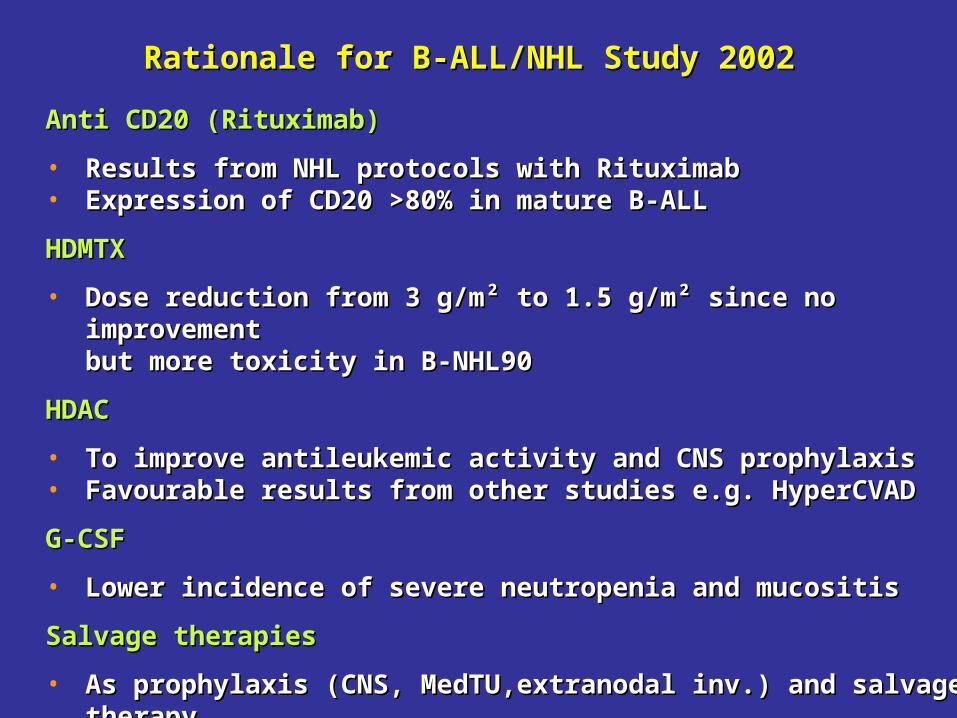
Rationale for B-ALL/NHL Study 2002Rationale for B-ALL/NHL Study 2002
Anti CD20 (Rituximab)Anti CD20 (Rituximab)
• Results from NHL protocols with RituximabResults from NHL protocols with Rituximab• Expression of CD20 >80% in mature B-ALLExpression of CD20 >80% in mature B-ALL
HDMTXHDMTX
• Dose reduction from 3 g/m² to 1.5 g/m² since no improvement Dose reduction from 3 g/m² to 1.5 g/m² since no improvement but more toxicity in B-NHL90but more toxicity in B-NHL90
HDACHDAC
• To improve antileukemic activity and CNS prophylaxisTo improve antileukemic activity and CNS prophylaxis• Favourable results from other studies e.g. HyperCVADFavourable results from other studies e.g. HyperCVAD
G-CSFG-CSF
• Lower incidence of severe neutropenia and mucositisLower incidence of severe neutropenia and mucositis
Salvage therapiesSalvage therapies
• As prophylaxis (CNS, MedTU,extranodal inv.) and salvage therapyAs prophylaxis (CNS, MedTU,extranodal inv.) and salvage therapy• SC apheresis in HR pts for potential auto SCTSC apheresis in HR pts for potential auto SCT
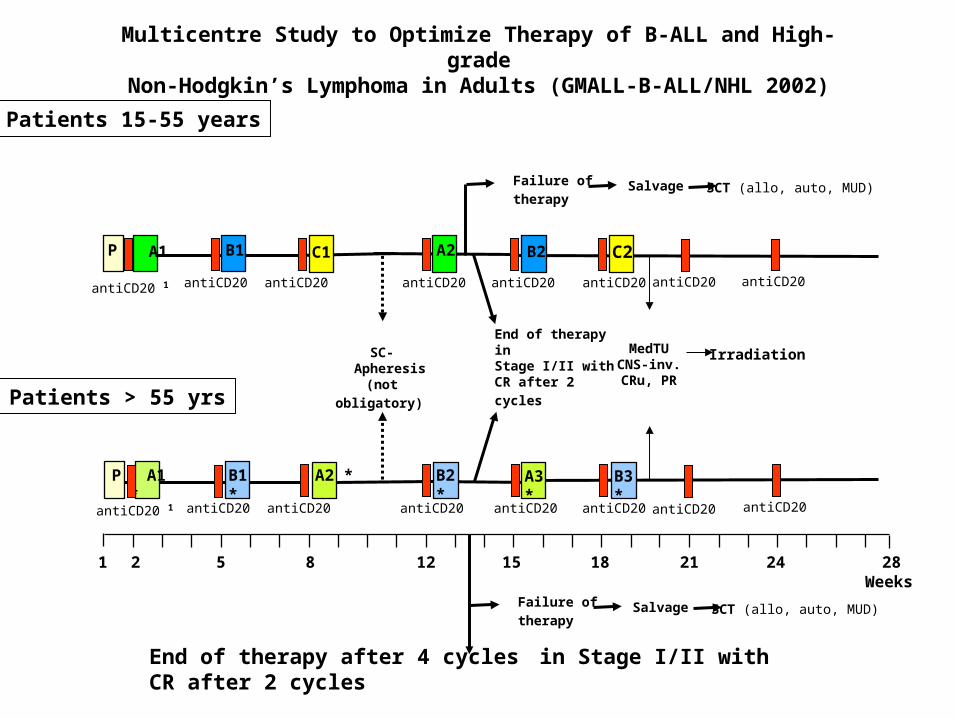
A1 B1P C1 A2 B2 C2
SC- Apheresis
(not obligatory)
antiCD20 antiCD20 antiCD20 antiCD20 antiCD20antiCD20 1
Multicentre Study to Optimize Therapy of B-ALL and High-gradeNon-Hodgkin’s Lymphoma in Adults (GMALL-B-ALL/NHL 2002)
Patients 15-55 years
Failure of
therapy Salvage SCT (allo, auto, MUD)
antiCD20 antiCD20
End of therapy inStage I/II with
CR after 2 cycles
MedTUCNS-inv.CRu, PR
Irradiation
1 2 5 8 12 15 18Weeks
21 24 28
A1 * B1 *P A2 * B2 * A3 * B3 *
antiCD20 antiCD20 antiCD20 antiCD20 antiCD20antiCD20 1 antiCD20 antiCD20
Patients > 55 yrs
Failure of
therapy Salvage SCT (allo, auto, MUD)
End of therapy after 4 cycles in Stage I/II with CR after 2 cycles
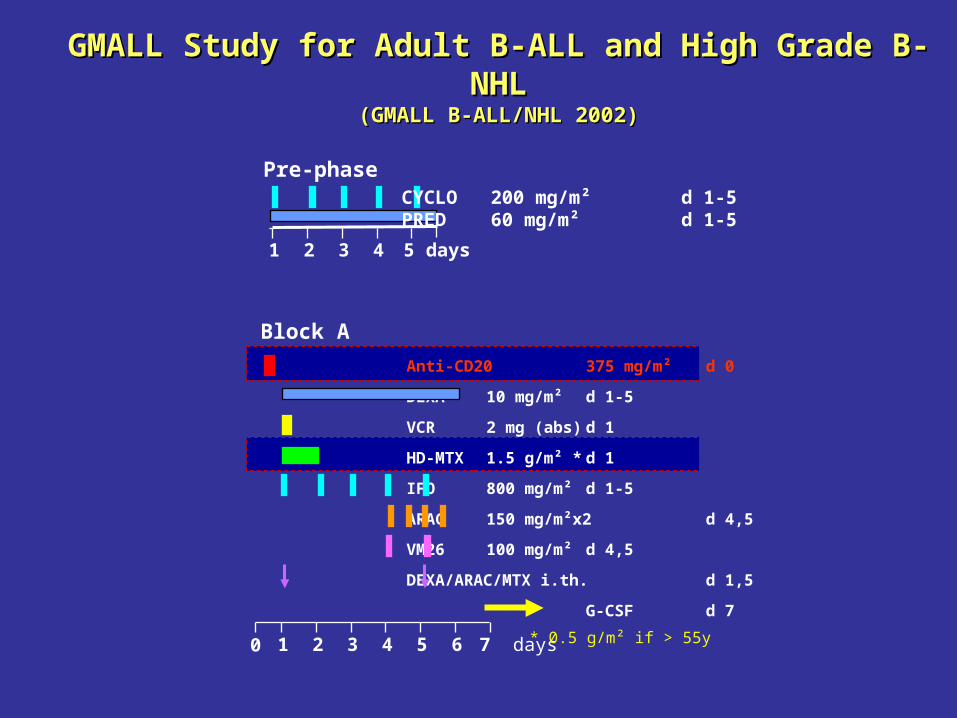
GMALL Study for Adult B-ALL and High Grade B-NHLGMALL Study for Adult B-ALL and High Grade B-NHL
(GMALL B-ALL/NHL 2002)(GMALL B-ALL/NHL 2002)
1 2 3 4 5 days
CYCLO 200 mg/m² d 1-5PRED 60 mg/m² d 1-5
Pre-phase
Block A
Anti-CD20 375 mg/m² d 0
DEXA 10 mg/m² d 1-5
VCR 2 mg (abs) d 1
HD-MTX 1.5 g/m² * d 1
IFO 800 mg/m² d 1-5
ARAC 150 mg/m²x2 d 4,5
VM26 100 mg/m² d 4,5
DEXA/ARAC/MTX i.th. d 1,5
G-CSF d 7
1 2 3 4 5 6 7 days0 * 0.5 g/m² if > 55y
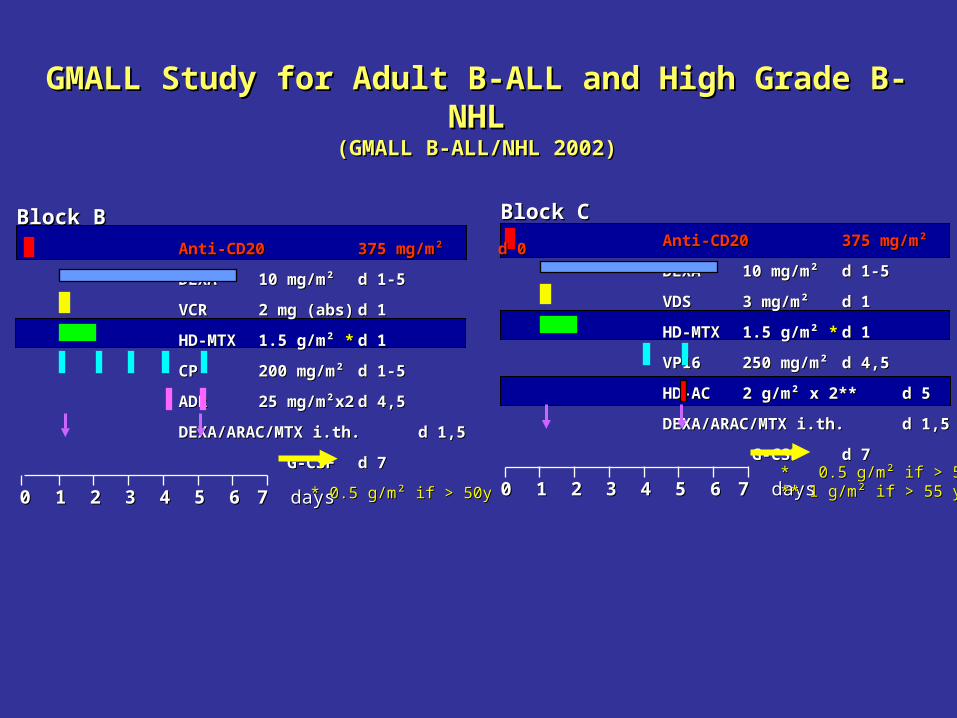
Block CBlock CAnti-CD20Anti-CD20 375 mg/m²375 mg/m² d 0d 0
DEXADEXA 10 mg/m² 10 mg/m² d 1-5d 1-5
VDSVDS 3 mg/m²3 mg/m² d 1d 1
HD-MTXHD-MTX 1.5 g/m² 1.5 g/m² ** d 1d 1
VP16VP16 250 mg/m²250 mg/m² d 4,5d 4,5
HD-ACHD-AC 2 g/m² x 2**2 g/m² x 2** d 5d 5
DEXA/ARAC/MTX i.th.DEXA/ARAC/MTX i.th. d 1,5d 1,5
G-CSFG-CSF d 7d 7
11 22 33 44 55 66 7 7 days days* 0.5 g/m² if > 55y* 0.5 g/m² if > 55y** 1 g/m² if > 55 y** 1 g/m² if > 55 y00
Block BBlock B
Anti-CD20Anti-CD20 375 mg/m²375 mg/m² d 0d 0
DEXADEXA 10 mg/m² 10 mg/m² d 1-5d 1-5
VCRVCR 2 mg (abs)2 mg (abs) d 1d 1
HD-MTXHD-MTX 1.5 g/m² 1.5 g/m² ** d 1d 1
CPCP 200 mg/m²200 mg/m² d 1-5d 1-5
ADRADR 25 mg/m²x225 mg/m²x2 d 4,5d 4,5
DEXA/ARAC/MTX i.th.DEXA/ARAC/MTX i.th. d 1,5d 1,5
G-CSFG-CSF d 7d 7
11 22 33 44 55 66 7 7 days days * 0.5 g/m² if > 50y* 0.5 g/m² if > 50y00
GMALL Study for Adult B-ALL and High Grade B-NHLGMALL Study for Adult B-ALL and High Grade B-NHL(GMALL B-ALL/NHL 2002)(GMALL B-ALL/NHL 2002)

Accrual period:Accrual period: 9/2002 - 10/2007 9/2002 - 10/2007
N evaluable:N evaluable: 381 381 (minimum 2 cycles(minimum 2 cycles completed)completed)
Diagnoses:Diagnoses: B-ALLB-ALL 84 (22%) 84 (22%)
BurkittBurkitt 146 (38%) 146 (38%) 32 32 atyp./B-likeatyp./B-like
DLBCLDLBCL 102 (27%) 102 (27%)70 70 mediastinalmediastinal
B-LBLB-LBL 22 (6%) 22 (6%)
LCALLCAL 25 (7%) 25 (7%)
GMALL B-ALL/NHL 2002GMALL B-ALL/NHL 2002 Evaluable PatientsEvaluable Patients
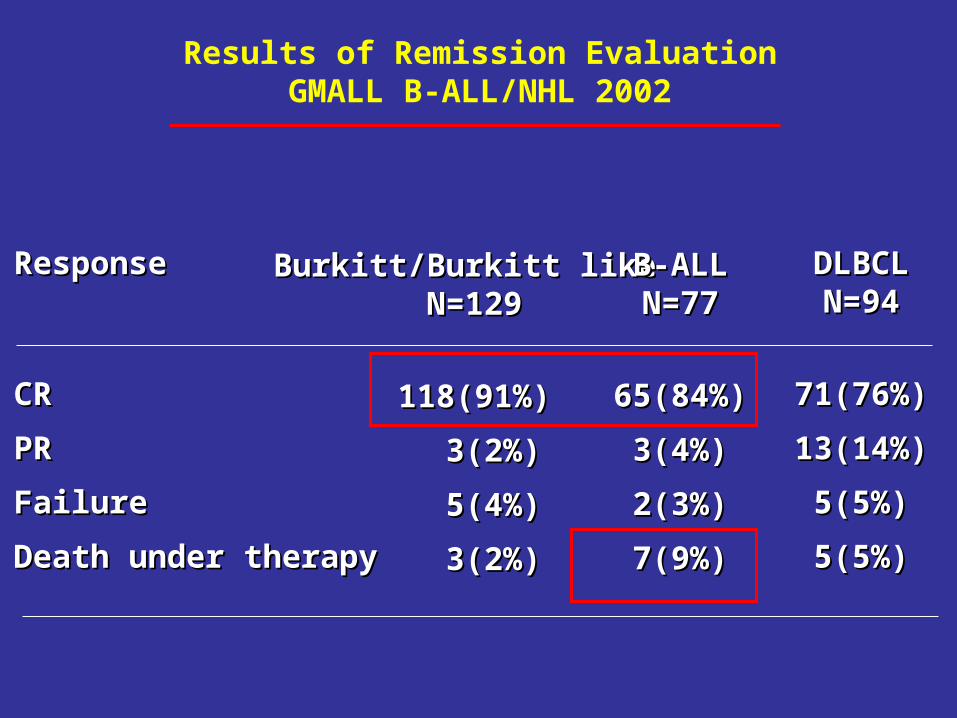
Results of Remission EvaluationGMALL B-ALL/NHL 2002
ResponseResponse
CRCR
PRPR
FailureFailure
Death under therapyDeath under therapy
Burkitt/Burkitt like Burkitt/Burkitt like N=129N=129
118(91%)118(91%)
3(2%)3(2%)
5(4%)5(4%)
3(2%)3(2%)
B-ALLB-ALLN=77N=77
65(84%)65(84%)
3(4%)3(4%)
2(3%)2(3%)
7(9%)7(9%)
DLBCLDLBCLN=94N=94
71(76%)71(76%)
13(14%)13(14%)
5(5%)5(5%)
5(5%)5(5%)

Burkitt 0.93 (N=101)B-ALL 0.76 (N=49)DLBCL 0.84 (N=74)
Overall Survival (<55 yrs)GMALL B-ALL/NHL 2002
Majority of events < 1 y

Overall Survival Burkitt / Burkitt‘s-like LymphomaGMALL B-ALL/NHL 2002
Burkitt 0.93 (N=101)Burkitt-like 0.91 (N=28)

Rituximab in Combination with Hyper-CVADRituximab in Combination with Hyper-CVADin Mature B-ALL/Burkitt‘s NHLin Mature B-ALL/Burkitt‘s NHL
Thomas et al , Cancer 2006Thomas et al , Cancer 2006
Hyper-CVAD+R Hyper-CVAD
Evaluable 31 (14 B-ALL) 48
CR 86% 85%
OS (3y) 89% 53%> 60 89% 19%
Relapses 7% 34%> 60 yrs 0% 50%
Toxicity ± R comparable
HDMTXHDMTX ARACARAC
00 22 44 66 88 1010 1212 1414 1616 1818 2020 2222
weeksweeks
Hyper-Hyper-CVADCVAD
HDMTXHDMTX ARACARAC
Hyper-Hyper-CVADCVAD
HDMTXHDMTX ARACARAC
Hyper-Hyper-CVADCVAD
HDMTXHDMTX ARACARAC
Hyper-Hyper-CVADCVAD
26262424
Rituximab 375 mg/m²Rituximab 375 mg/m²
Burkitt‘s NHL in HIV+ pts

Short Intensive Chemotherapy in HIV+ Adult Burkitt‘s NHLShort Intensive Chemotherapy in HIV+ Adult Burkitt‘s NHL
AuthorAuthor YearYear AgeAge Stage III/IVStage III/IV L3-ALLL3-ALL HAARTHAART ProtocolProtocol NN CRCR OSOS
Horst et alHorst et al 20032003 n.r. n.r. 70%* 70%* 8%* 8%* 60%60% GMALL B-ALLGMALL B-ALL 1616 87%87% 72%72%0.5-3 g/m² MTX0.5-3 g/m² MTX
Wang et alWang et al 20032003 40 (19-61)* 40 (19-61)* 88%88% 29%* 29%* n.r.n.r. CODOX-MCODOX-M 88 63%63% 60%60% 7 g/m² MTX7 g/m² MTX
Astrow et al Astrow et al 20032003 45 (27-59) 45 (27-59) 83%83% 76%76% n.r.n.r. McMastersMcMasters 2323 39%39% 39%39% 200 mg/m²200 mg/m²
Oriol et alOriol et al 20032003 45 (23-65)45 (23-65) 57%57% 43%43% 36%36% GMALL B-ALLGMALL B-ALL 1414 71%71% 55%55%3 g/m² MTX3 g/m² MTX
Costello et alCostello et al 20042004 18-65 18-65 81%81% n.r.n.r. n.r.n.r. CHOP augm.CHOP augm. 1313 n.r.n.r. 60%60%8 g/m² MTX8 g/m² MTX
Cortes et alCortes et al 20022002 43 (32-55)43 (32-55) 29%29% 50%50% 64%64% HyperCVADHyperCVAD 1414 92%92% 48%48%1 g/m² MTX1 g/m² MTX
Weighted meanWeighted mean 8888 68%68% 54%54%
* Whole cohort including arm with less intensive chemotherapy* Whole cohort including arm with less intensive chemotherapy
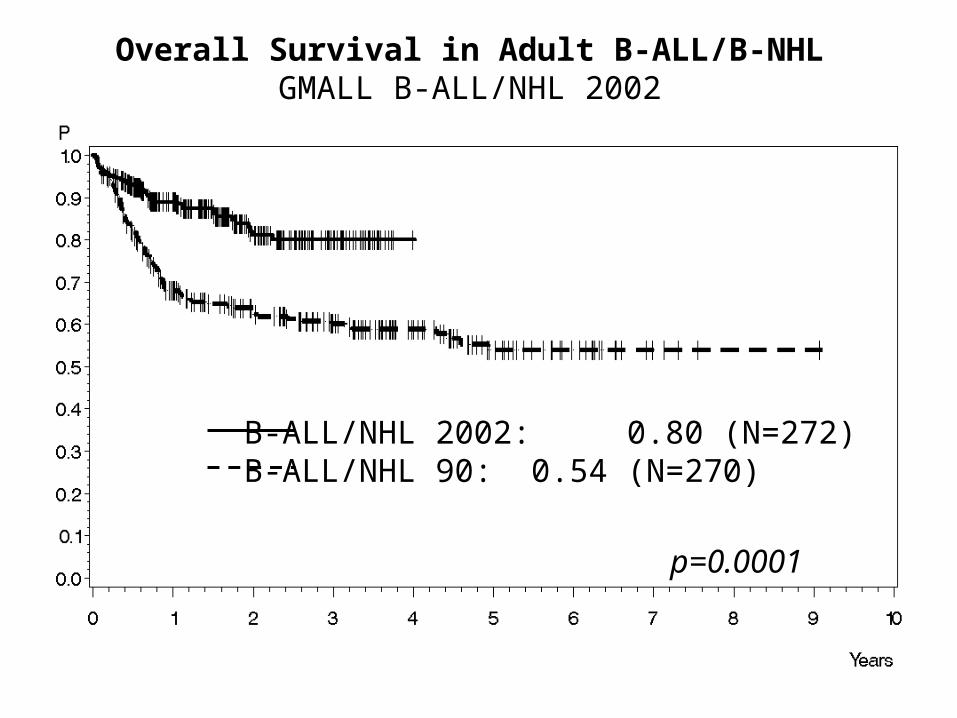
B-ALL/NHL 2002: 0.80 (N=272)B-ALL/NHL 90: 0.54 (N=270)
Overall Survival in Adult B-ALL/B-NHLGMALL B-ALL/NHL 2002
p=0.0001

Mature B-ALL/Burkitt‘s NHLMature B-ALL/Burkitt‘s NHL
Summary and ConclusionsSummary and Conclusions
• Combination of Rituximab and intensive chemo feasibleCombination of Rituximab and intensive chemo feasible
• Response rate 80-90% in Burkitt / DLBCL,Response rate 80-90% in Burkitt / DLBCL,
overall survival ~ 90%overall survival ~ 90%
• Improvement in mature B-ALL, less for pts > 55 yImprovement in mature B-ALL, less for pts > 55 y
• Irradiation of residual tumors effective salvage therapyIrradiation of residual tumors effective salvage therapy
• SCT: No prognostic factors SCT: No prognostic factors no indication for SCT in CR1 no indication for SCT in CR1
No stem cell apheresis any more No stem cell apheresis any more
• Major toxicity: mucositisMajor toxicity: mucositis
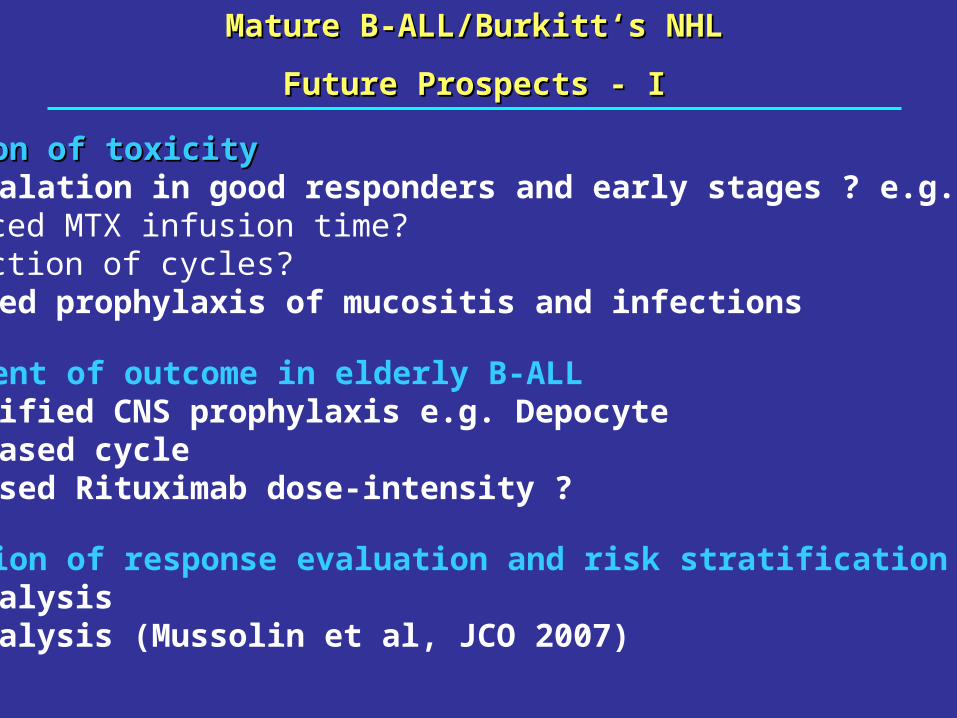
Mature B-ALL/Burkitt‘s NHLMature B-ALL/Burkitt‘s NHL
Future Prospects - IFuture Prospects - I
Reduction of toxicityReduction of toxicity• De-escalation in good responders and early stages ? e.g.- Reduced MTX infusion time?- Reduction of cycles?• Improved prophylaxis of mucositis and infections
Improvment of outcome in elderly B-ALL• Intensified CNS prophylaxis e.g. Depocyte• HDAC based cycle• Increased Rituximab dose-intensity ?
Refinition of response evaluation and risk stratification e.g.• PET analysis• MRD analysis (Mussolin et al, JCO 2007)

Study CenterStudy Center Head Head D.Hoelzer, FrankfurtD.Hoelzer, FrankfurtCoordinatorCoordinator N.Gökbuget, FrankfurtN.Gökbuget, FrankfurtData ManagerData Manager R.Reutzel, FrankfurtR.Reutzel, Frankfurt
Central DiagnosisCentral Diagnosis Morphology/CytochemistyMorphology/Cytochemisty H.Horst, KielH.Horst, KielImmunphenotypingImmunphenotyping E.Thiel, S.Schwartz,E.Thiel, S.Schwartz,Molecular geneticsMolecular genetics T.Burmeister, BerlinT.Burmeister, BerlinGene expression analysisGene expression analysis W.K.Hofmann, BerlinW.K.Hofmann, BerlinCytogeneticsCytogenetics H.Rieder, DüsseldorfH.Rieder, Düsseldorf
C.Schoch, MünchenC.Schoch, München
MinimalMinimal M.Kneba, M.Brüggemann,T. Raff, KielM.Kneba, M.Brüggemann,T. Raff, KielResidual DiseaseResidual Disease H. Pfeifer, FrankfurtH. Pfeifer, Frankfurt
Molecular therapiesMolecular therapies O. Ottmann, FrankfurtO. Ottmann, Frankfurt
SCT coordinatorSCT coordinator R.Arnold, BerlinR.Arnold, Berlin
Irradiation therapyIrradiation therapy R.Fietkau, RostockR.Fietkau, Rostock
StatisticsStatistics GMALL Study Center GMALL Study Center
+ ~126 participating centers+ ~126 participating centers
GMALL- Study GroupGMALL- Study Group





























