Embed Size (px)
Citation preview

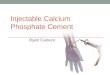
The electrolytes calcium and phosphate have many roles in:•the structure and function of bones, •the function of membranes,•the activation of hundreds of enzymes involved in genetic regulation, muscles contraction, blood coagulation, and energy use.The clinical importance: Ca² and PO4 are used for diagnosing:•parathyroid dysfunction,•hypercalcemia of malignancies,•monitoring surgery, critical care and neonate.

ECF 22,5mmol
Bone 99%25000mmol
Skin 0,3mmol/24h
Plasma9 mmol
Exchange500mmol/24h
Formation7,5mmol/24h
Resorption7,5mmol/24h
Absorption12mmol/24h
Secretion6mmol/24h
Faeces19mmol/24h
Food25mmol/24h
Urine 6mmol/24h
Reabsorption234mmol/24h
GlomerularFiltration240mmol/24h
GUT
Distributionof calcium

BONE CALCIUMBone consists of osteoid, on which is deposited
inorganic hydrated calcium salts (hydroxyapatite). (Ca10(PO4)6(OH)2)
Osteoid synthesis by osteoblasts requires adequate calcium, phosphate, ALP and this process is controlled by hormones (GH and Cytokines).
Bone provides an important reservoir of calcium and phosphate.
The amount of intracellular calcium is relatively low, (5000 -10000) lower than blood.

PLASMA CALCIUM
Total calcium2.3 – 2.6mmol/l
Diffusible54%
Nondiffusible(bound to protein)
46%
Free ions(physiologically active)
47%
Complexed(bicarbonate, citrate, phosphate)
7%

Plasma calciumIn alkalosis, there is increase in calcium binding to
albumin and calcium complex formation. As a result, the concentration of ionized calcium falls, and this may produces clinical signs of hypocalcaemia although total plasma calcium concentration is unchanged.
In an acute acidosis, the reverse effect is observed, the ionized calcium concentration is increased.
Measurement of total plasma calcium is satisfactory for most clinical purposes because of speed with which results are available. (blood transfusion, surgery with extracorporeal bypass.

Plasma calcium
Changes in plasma albumin concentration will affect total calcium concentration, leading to misinterpretation of results in both hypoproteinaemic and hyperproteinaemic cases.
A common cause of apparent hyperproteinaemia, and hence hypercalcaemia, is venous stasis during blood sampling.
The increase in ץ-globulin in patient with myeloma can also increase the total calcium, however, hypercalcaemia is due to secretion of calcium-mobilizing substances by the tumour cells.

Plasma calciumFor albumin < 40 g/l :
Corrected calcium =Ca + 0.02 X (40 – alb) mmol/l
For albumin > 40 g/l :
Corrected calcium =Ca – 0.02 X (alb – 45) mmol/l

Reference ranges for calciummmol/l mg/dl
Total calcium
Child
adult
2.2-2.7
2.1-2.6
8.8-10.7
8.4-10.2
Ionized calcium
At birth
Neonate
Child
adult
1.3-1.6
1.2-1.5
1.2-1.4
1.2-1.3
5.2-6.4
4.8-5.9
4.8-5.5
4.6-5.3

Physiologic functions of calcium ions
The flow of calcium ions into the myocardial cells, helps control cardiac contraction and rhythm by binding to contractile proteins (troponin, calmodulin).
Calcium ions also serve as second messengers in controlling the secretion of many enzymes (insulin, aldosterne, vasopressin, renin).

Parathyroid gland
PTH SECRETION
Bone kidney
Stimulate:Osteoclastic activity(release Ca²,HPO4)
Promotes:Ca² absorptionHPO4 excretion1-α-hydrolase activation
hypercalcemia hypocalcaemia– +
PTH:

Calcium homeostasisCalictriol: Circulating 25-OH vit D
(INACTIVE)
+
1,25(OH)2 vit D
Kidney
vitD promotes:renal reabsorptionof Ca² and HPO4
intestine
vitD promotes:intestinal absorptionof Ca² and PO4
1-α- hydroxylase

Calcium homeostasisCalcitonin: This polypeptide hormone, produced by C-
cells of the thyroid gland in response to a marked hypercalcemia.
Calcitonin reduces calcium by inhibiting osteoclast activity and inhibiting the action of both PTH and vitamin D.

Hypocalcaemia:
Artefactual: blood collected into EDTA or oxalate.
Associated with low PTH: •Hypoparathyroidism.•Hypomagnesaemia.•Hungry bone syndrome.•Neonatal hypocalcaemia.
Associated with high PTH:•Deficiency and disorders of vitamin D.•Acute pancreatitis.•High PO4 intake.•Massive transfusion with citrated blood.•Acute rhabdomyolysis.
Causes
• Behavioural disturbance.
• Numbness and paraesthesae.
• Muscle cramps and spasms.
• Laryngeal stridor.• Convulsions.• Cataracts chronic.• Basal ganglia
calcification.• Papilloedema.• Prolonged QT on ECG.
Clinical features

Hypercalcemia:
COMMON:
Malignant disease.
Primary hyperthyroidism.
LESS COMMON:
Thyrotoxicosis.
VitD intoxication.
Sarcoidosis.
Renal transplantation.
UNCOMMON:
Milk-alkali syndrome.
tuberculosis.
Acute adrenal failure.
Weakness, tiredness, weight loss.
Mental changes.Abdominal pain.Anorexia, nausea and
vomiting.Polyuria, dehydration and
renal failure.Short QT on ECG.Cardiac arrhythmias and
hypertension.Corneal calcification,
vascular calcification.
CAUSES Clinical features

Laboratory testing of calcium
Methods:
1. Atomic absorption spectroscopy.2. Ion selective electrode (ionized calcium).3. Titrimetric method.4. Colorimetric methods : I. Precipitation method. II. Ortho-cresolphthalein complexone,
Arsenazo III. 5. Turbidometric method ( for urine).

Laboratory testing of calcium1. Atomic absorption spectroscopy: This method involves introducing a dilute sample
into an air-acetylene flame and measuring the absorption of light at 422.5nm.
2. Ion selective electrode (ionized calcium):
These electrodes use membranes impregnated with molecules (ionophores) that selectively bind calcium ions. An electric potential develops across the membrane that is related to ionized calcium concentration.

Laboratory testing of calcium3. Titrimetric method: A diluted specimen is titrated against
EDTA which removes calcium from the titrating fluid and changes the colour of an indicator (calcon dye from purple to blue) as response to the presence or absence of calcium.
Calculations: Serum calcium conc. = Tt / Tstd X conc. Of stdTt: volume of titrant EDTA needed for the test
serum. Tstd: volume of titrant EDTA needed for the
standard.

Laboratory testing of calcium4. Colorimetric methods:I. Precipitation method: Calcium is precipitated from the
specimen as calcium chloranilate by adding a saturated solution of sodium chloranilate.
The precipitate is washed (with isopropyl alcohol) and then treated with EDTA, which binds the calcium and releases the cholranilic acid (purple in colour) which can be read at 520nm against an EDTA blank .

Laboratory testing of calcium4. Colorimetric methods:II. Ortho-cresolphthalein complexone,
Arsenazo III: This method is based on the
complexometric reaction between calcium and the dye ortho-cresolphthalein complexone. Another method uses the dye Arsenazo III.
CALCIUM + Arsenazo III ALK calcium-Arsenazo complex (purple)
The colored complex is absorbed at 650nm.

Laboratory testing of calcium5. Turbidometric method ( for urine): When Sulkowitch reagent (oxalate
buffered with acetate) is added to urine, it will produce a white precipitate of calcium oxalate without co-precipitation of other urinary constituents.
This semiquantitative test should only be used for quick screening.

Laboratory testing of calciumDecreased ionized Ca
Measure serum Mg
Measure serum PTH
If acute, is the patient:• Receiving citrated blood?• A neonate (1-3day)?• Recovering from surgery?• Having pancreatitis? • Having drugs?
Mg high:Parathyroid glandare suppressed
Mg normal Mg low:PTH release is inhibited
PTH elevated:CRF (PO4 high)Vit D defect (PO4 low)
PTH low/normal:Primary or post surgicalhypoparathyroidism

Laboratory testing of calcium
Increased ionized Ca
Measure serum PO4 and PTH
Is there is:• Renal failure?• Drugs (vita D, Li, thiazides)?• Hyperthyroidism?• Low cortisol?
• PTH high;PO4 normal or high: possible renal failure.• PTH normal or high; PO4low: hyperthyroidism.• PTH normal or low: malignancy, Sarcoidosis.• PTH low; PO4 low: dietary excess of Ca.

Phosphate Distribution:About 80% of the(700-800) gm of body phosphate
is contained in bone, in the form of hydroxyapatite.
Blood phosphate is either absorbed from dietary sources or reabsorbed from bone.
Most phosphate is found within cells, and the transport of glucose into cells is accompanied by an influx of phosphate, which is used in the synthesis of phosphorlyted compounds.

Plasma phosphate
Plasma phosphate12mg/dl
Inorganic (phosphorus)
25%Organic
75%
Free ions22.5%
Bound to anions2.5%

Biochemical functionsCompounds of phosphorus are in all
cells participating many processes:As component of: nucleotides(DNA,RNA),
phospholipids and most enzymes.
As biochemical energy reservoirs: ATP, creatine phosphate and phosphoenol pyruvate.

Homeostasis:The kidney plays an important role in the
regulation of phosphate concentration by several factors including:
acid –base status (normally by reabsorb 90% of phosphate filtered at the glomerulus),
Vitamin D (promotes renal reabsorption, and intestinal absorption, of phosphate),
PTH inhibit renal reabsorption of phosphate.

Reference rangesmmol/l mg/dl
S.Phosphate:Newborn
Infant
Child
Adult male
Adult female
1.8-3.1
1.5-2.1
1.5-1.8
0.7-1.2
0.9-1.3
5.5-9.5
4.5-6.5
4.5-5.5
2.3-3.7
2.8-4.1

Hypophosatemia:
Causes:Vitamin D deficiency,Primary
hyperparathyroidism,Nutrition with
inadequate phosphate,Diabetic ketoacidosis
(recovery phase),Renal tubular disease,Respiratory alkalosis.
Clinical features:Muscles weakness,Respiratory and
myocardial insufficiency,
Hepatocellular damage.
Convulsions.

Hyperphosphatemia:Causes:Renal failure,Hypoparathyroidism,Acromegaly,Excessive phosphate intake,Vitamin D intoxication,

Laboratory testing of phosphate
1. Colorimetric method:Determinations are usually made only of
inorganic phosphorus after removing the protein by precipitation with trichloroacetic acid (TCA).
Phosphate has been measured by methods in which molybdate react with phosphate to form complex molecules of phosphomolybdate. Several reducing agents have been developed:

Laboratory testing of phosphateFiske and Subbarow used1-amino-2-
naphthol-4-sulfonic acid (ANS), to form molybdenum blue with high absorptivity at 660 nm.
Stannous chloride and ferrous ammonium sulfate are also been used.
Garber and Miller selected a method uses semidine HCl as a reducing agent.

Laboratory testing of phosphate2. Spectrophotometeric method:(without protein precipitation)
Inorganicphosphorus
H2SO4Ammoniummolybdate+ +
Phosphomolybdatecomplex
The absorbance at 340 nm is directly proportional tothe amount of inorganic phosphorus concentration.

Low serum PO4
Urinary PO4 excretionlow high
maldistribution GI losses Renal losses
Serum Ca²
increased
hyperparathyroidism
Low ornormal
Diuretics;Renal tubular defects;Recovery from burns;Inadequate vit D.

High serum PO4
GFR<25 ml/min >30-40 ml/min
Renal failure(acute or chronic)
Urinary PO4
Normal(<1500mg/day)
Increased(>1500mg/day)
Hypoparathyroidism;Other endocrine disorders
Increased PO4 intake;Cell destruction;Cellular redistribution.