Embed Size (px)
Citation preview

Calcium oxalate stones
Lama Nazzal

Case 66 yo Male seen for the first time in VA urology clinic in 2005 after he was found to have bilat stones on back Xray. Pt with stone passage 3 years ptp, did not see urologist. He complained of intermittent L flank pain, and occasional R flank pain. He passed another stone 1 week ptp after he felt nauseated and had back pain. ROS: multiple loose BMs PAST MEDICAL HISTORY: •Anxiety •Chronic Back Problems •hx partial colectomy '76, & abd hernia repair '79 •hx psorasis per patient FH: no hx of stones in family; 3 bro and 2 sis, 4 children.
meds: none. no vitamins or supplements.
SH: no tobacco, past EtOH; retired on disability due to back pain.

Labs

CT from 7/2005 shows B/L small stones. > 2 cm L renal pelvic stone. L distal ureteral stone 8 mm, and B/l slight cortical thinning. So sig L hydro ureter or hydro.

• Dec 2005: Left ureteroscopy/laser lithotripsy/left ureteral stent placement • Stone composition: 60% CA.OXALATE MONOHYDRATE 20% CA.OXALATE
DIHYDRATE 20% CA. PHOSPHATE
Started K citrate bid


New 1.1 cm obstructing right ureteral calculus in the proximal ureter with mild upstream hydroureteronephrosis and perinephric stranding consistent with obstructive uropathy. Passage of left ureteral stones with resolution of hydroureteronephrosis.
8/19/2011: cystoscopy, R stent placement
Stone composition: 100% CaOx stone, both mono- and dihydrate.


Calcium Oxalate Stones
• In the US, the lifetime risk for developing a stone is 5 to 15%
• 5-yr risk for a recurrence is ~ 30 to 50%.
• 60–80% of the stones are calcium oxalate
• Calcium oxalate stones incidence is increasing.

Oxalate
• Oxalate is the salt-forming ion of oxalic acid • Oxalic acid may form oxalate salts with various cations, such as
sodium, potassium, magnesium, and calcium. • Sodium oxalate, potassium oxalate, and magnesium oxalate
are water soluble but calcium oxalate (CaOx) is nearly insoluble.
• Urinary oxalate is derived from both exogenous and endogenous sources.
• Oxalate is an ubiquitous component of plants and plant-derived foods
• Depending on dietary intake, daily urinary oxalate excretion varies between 10 and 40 mg per 24 h (0.1–0.45 mmol per 24 h).
• Concn > 40-45 mg per 24 h are considered as clinical hyperoxaluria

Endogenous oxalate synthesis

OXALATE TRANSPORT
• In the gut: Paracellular vs. transcellular. In the small intestine where junctional resistance is low and luminal oxalate concentration is expected to be high, it is expected that the paracellular route is the major contributor to absorption as compared to more distal segments.
• Solute-linked carrier 26 (SLC26) anion exchangers: 11 members capable of transporting several anions, including sulfate, chloride, hydroxyl, iodide, bicarbonate, formate, and oxalate.
• Role of CFTR (Cystic fibrosis transmembrane conductance regulator) in reciprocal regulatory activity with several SLC26 anion exchangers, including SCL26A6
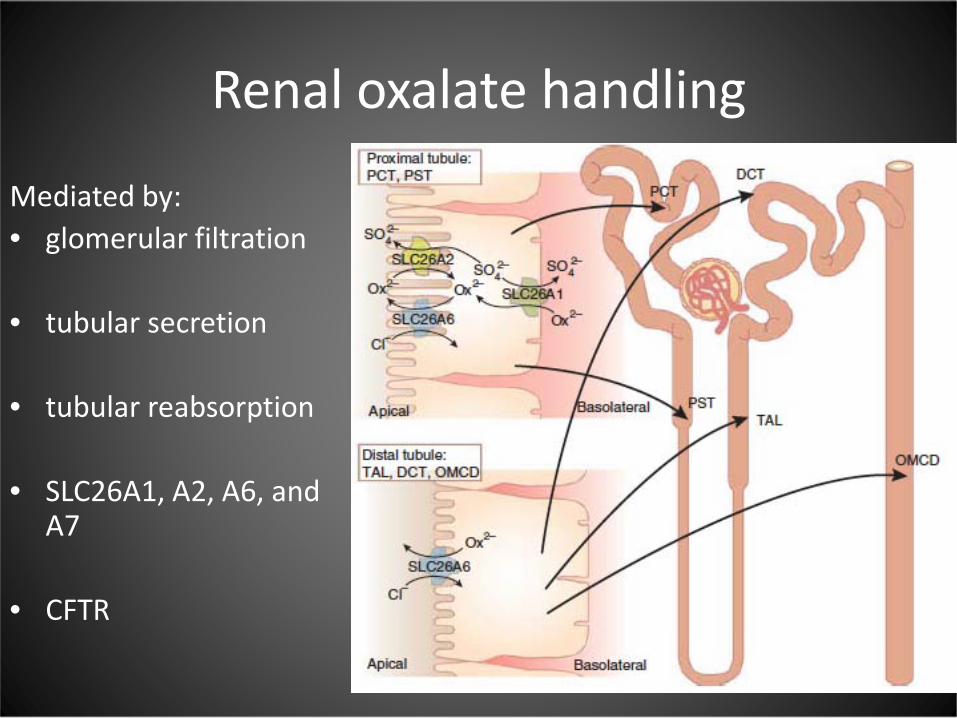
Renal oxalate handling
Mediated by: • glomerular filtration • tubular secretion
• tubular reabsorption
• SLC26A1, A2, A6, and
A7 • CFTR

Oxalate handling across the intestine has been shown to be segment specific in animals with net oxalate secretion in the small intestine and proximal colon and net oxalate absorption in the distal colon

Jiang Z et al.Nat Genet 2006; 38: 474–478.

Jiang Z et al.Nat Genet 2006; 38: 474–478.

Primary hyperoxaluria
• Autosomal recessive hepatic enzyme deficiencies causing d/o of glyoxylate metabolism
• Increased endogenous oxalate synthesis.
• Severe hyperoxaluria
• Reported values of oxaluria ranging between 88 and 352 mg per 24 h for PH I and 88 and 176 mg per 24 h for PH II
• progressive nephrocalcinosis and/or nephrolithiasis
• Often leading to early end-stage renal disease.

Secondary hyperoxaluria
• High-oxalate diet.
• Fat malabsorption (enteric hyperoxaluria).
• Alterations in intestinal oxalate-degrading microorganisms.
• Genetic variations of intestinal oxalate transporters.

High oxalate diet
• Daily average oxalate intake is variable, ranging between 44 and 351 mg/day (0.5–4.0 mmol/day)
• Ingestion of calcium (or magnesium) with oxalate can reduce oxaluria by forming insoluble oxalate complexes in the gut
• Intestinal oxalate absorption in healthy individuals was reported to be between 2.2 and 18.5% of an administered load, with values 15% considered as oxalate hyperabsorption
• Hyperabsorption is a risk factor for idiopathic CaOx nephrolithiasis.
• Idiopathic CaOx stone formers absorb more oxalate than normal individuals.

Holmes RP et al.Kidney Int 2001; 59: 270–276.
Oxalate free diet

Taylor EN, Clin J Am Soc Nephrol 2008; 3: 1453–1460.
• cross-sectional study of 3348 individuals with and without a history of kidney stones from three cohorts: the Health Professionals Follow-up Study (HPFS) and the Nurses’ Health Studies I and II (NHS I and NHS II).
• To examine the relations between specific demographic, dietary, and urinary factors and the 24-h urinary excretion of oxalate, and to determine whether these associations varied by kidney stone history

Taylor EN, Clin J Am Soc Nephrol 2008; 3: 1453–1460.

Secondary hyperoxaluria:Fat malabsorption (enteric hyperoxaluria).
• Dihydroxy bile acids and fatty acids increase the permeability of the intestinal mucosa to oxalate
• Complexation of fatty acids with calcium in intestinal lumen increases the amount of soluble oxalate that is available for absorption as insoluble CaOx complexes are no longer formed
Typically in patients with:
• inflammatory bowel disorders
• after bariatric surgery
• after the use of gastrointestinal lipase inhibitors.
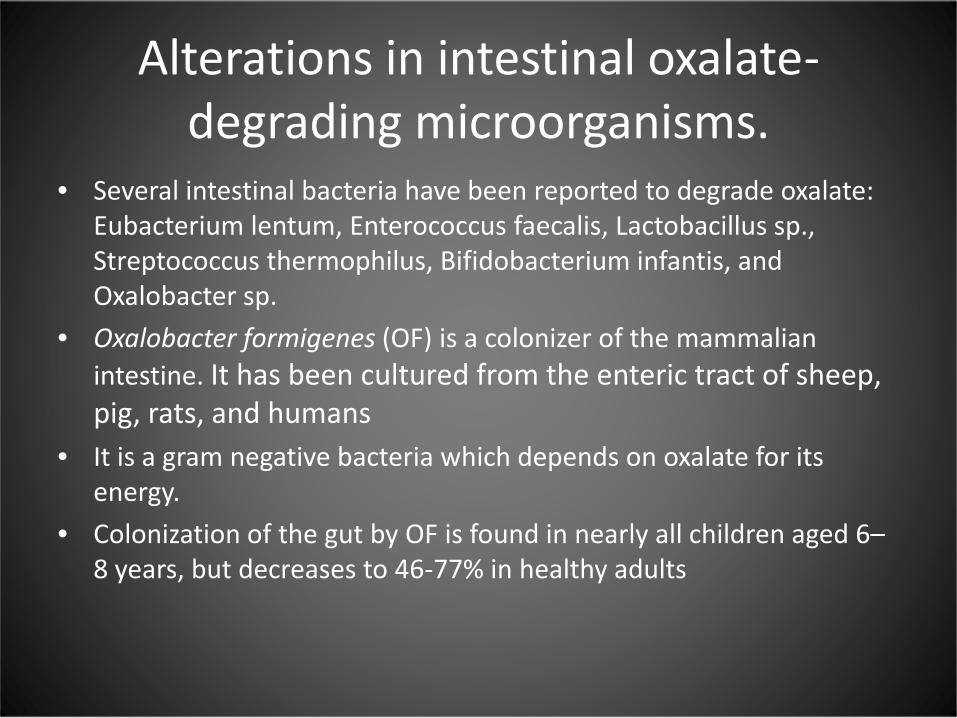
Alterations in intestinal oxalate-degrading microorganisms.
• Several intestinal bacteria have been reported to degrade oxalate: Eubacterium lentum, Enterococcus faecalis, Lactobacillus sp., Streptococcus thermophilus, Bifidobacterium infantis, and Oxalobacter sp.
• Oxalobacter formigenes (OF) is a colonizer of the mammalian intestine. It has been cultured from the enteric tract of sheep, pig, rats, and humans
• It is a gram negative bacteria which depends on oxalate for its energy.
• Colonization of the gut by OF is found in nearly all children aged 6–8 years, but decreases to 46-77% in healthy adults


Lange JN et al. Urology. 2012 Jun;79(6):1286-9.

Lange JN et al. Urology. 2012 Jun;79(6):1286-9.

• case-control study of 247 adult patients with recurrent calcium oxalate stones and 259 age-, gender-, and region-matched control.

Kaufman DW et al. J Am Soc Nephrol 19:1197–1203

OF in primary hyperoxaluria
• Randomized, double-blind, placebo controlled multicenter study to evaluate OF effect and safety.
• eligible subjects enrolled into the study were randomized (1:1) to receive orally either NLT 107 CFU of Oxabact or placebo twice daily with meals.
Hoppe B et al. Nephrol Dial Transplant 26:3609–3615

Hoppe B et al. Nephrol Dial Transplant 26:3609–3615
P 0.616

• 11 O. formigenes colonized and 11 noncolonized subjects were administered diets controlled in calcium and oxalate contents.
• 24-hour urine collections and stool samples obtained on the last 4 days of each 1-week diet.
• For the first phase dietary oxalate intake was varied, including 50 mg daily for week 1, 250 mg for week 2 and 750 mg for week 3. Calcium consumption was fixed at 1,000 mg daily.
• For the second phase dietary calcium intake was varied, including 400 mg daily for week 1, 1,000 mg for week 2 and 2,000 mg for week 3. Oxalate consumption was fixed at 250 mg daily.
Jiang J et al. J Urol. 2011 Jul;186(1):135-9
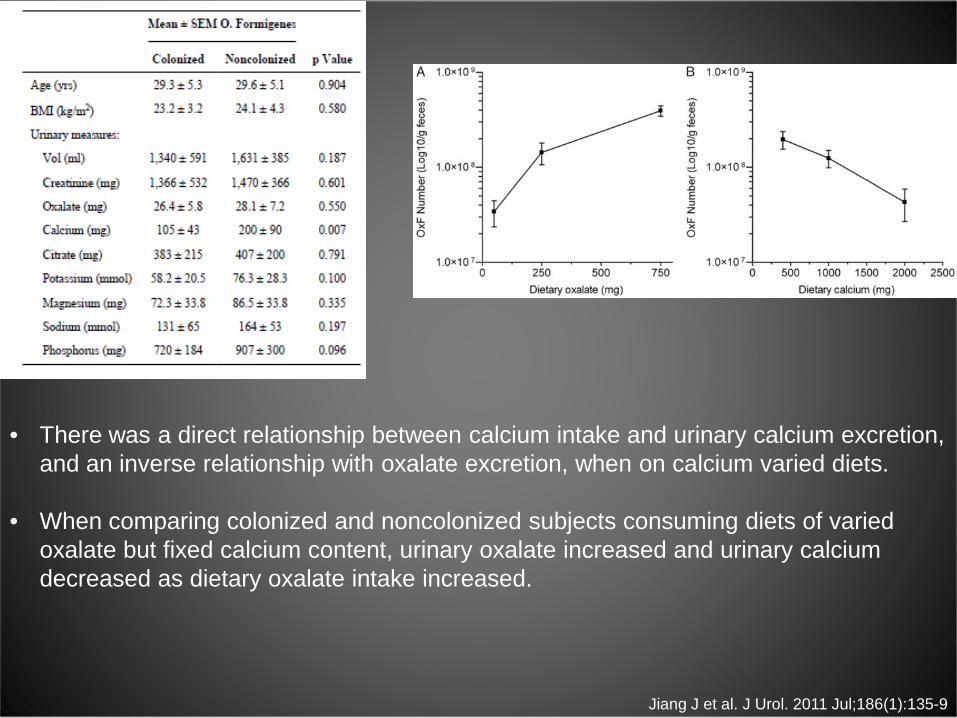
Jiang J et al. J Urol. 2011 Jul;186(1):135-9
• There was a direct relationship between calcium intake and urinary calcium excretion, and an inverse relationship with oxalate excretion, when on calcium varied diets.
• When comparing colonized and noncolonized subjects consuming diets of varied oxalate but fixed calcium content, urinary oxalate increased and urinary calcium decreased as dietary oxalate intake increased.

Proposed study:1
• Male or female individuals between the ages of 18 and 40 years presenting for general primary care evaluation at the Bellevue Internal Medicine outpatient clinics
• Hypothesis: is the loss of OF colonization in the GI tract associated with increase in urinary oxalate excretion in patients colonized with H. pylori and OF?
• Primary outcome variable: change in urine calcium oxalate supersaturation. Will consider increase of 30% a significant outcome.
• Study Design: cohort with patient serving as their own control. They will be followed for a total of 6 months with serial urine and stool analysis.
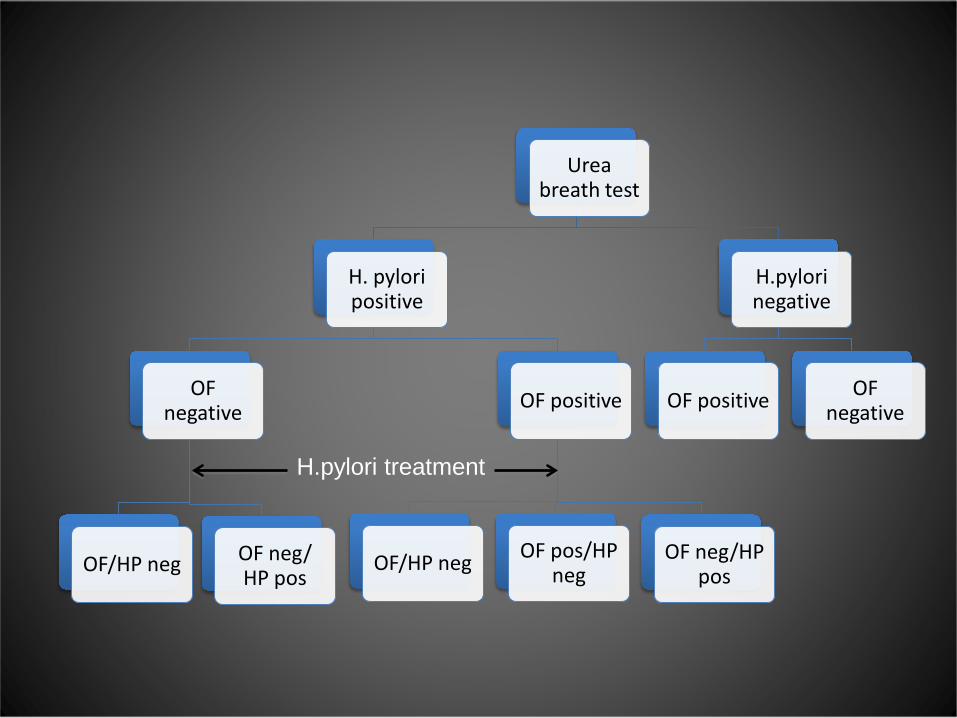
Urea breath test
H. pylori positive
OF negative
OF/HP neg OF neg/ HP pos
OF positive
OF/HP neg OF pos/HP neg
OF neg/HP pos
H.pylori negative
OF positive OF negative
H.pylori treatment

Proposed study 2:
• Hypothesis: to detect the rate of Oxalobacter formigenes (OF) recolonization 2 years after OF eradication.
• Descriptive prospective unblinded study
• Subjects included in the prior study by Kharlamb et al. will be contacted for participation.
• Stool testing for OF colonization will be performed.

THANK YOU