Embed Size (px)
Citation preview
2016, 63 (12), 1065-1080
THE GUIDELINES for the diagnosis and treatment of primary aldosteronism (PA) have been established
Calibration and evaluation of routine methods by serum certified reference material for aldosterone measurement in blood
Tetsuo Nishikawa1), Masao Omura1), Migaku Kawaguchi2), Akiko Takatsu2), Fumitoshi Satoh3), Sadayoshi Ito4), Isao Kurihara5), Hiroshi Itoh5), Toshihiko Yanase6), Hirotaka Shibata7), Yutaka Oki8), Mitsuhide Naruse9), Keiko Sakurai10), Hidehiko Sasamoto11) and Katsuhiko Kuwa2)
1) Endocrinology and Diabetes Center, Yokohama Rosai Hospital, Yokohama, Japan2) National Metrology Institute of Japan, National Institute of Advanced Industrial Science and Technology, Tsukuba, Japan3) Division of Clinical Hypertension, Endocrinology & Metabolism, Tohoku University Graduate School of Medicine,
Sendai, Japan4) Division of Nephrology, Endocrinology and Vascular Medicine, Department of Medicine, Tohoku University School of
Medicine, Sendai, Japan5) Department of Endocrinology, Metabolism and Nephrology, School of Medicine Keio University, Tokyo, Japan6) Department of Endocrinology and Diabetes Mellitus, School of Medicine, Fukuoka University, Fukuoka, Japan7) Department of Endocrinology and Metabolism, Rheumatology and Nephrology, Faculty of Medicine, Oita University,
Yufu, Japan8) Department of Community and Family Medicine, Hamamatsu University School of Medicine, Hamamatsu, Japan9) Department of Endocrinology, Metabolism and Hypertension, National Hospital Organization Kyoto Medical Center,
Kyoto, Japan10) Reference Material Institute for Clinical Chemistry Standards, Kawasaki, Japan11) Aska Pharma Medical Co., Ltd., Kawasaki, Japan
Abstract. We attempted to study the standardization of aldosterone measurement in blood. The serum certified reference material (serum CRM) was established by spiking healthy human serum with pure aldosterone. ID-LC/MS/MS as a reference measurement procedure was performed by using the serum CRM. LC-MS/MS as a comparison method (CM) was routinely used for clinical samples, and the values with and without calibration by the serum CRM were compared. The serum CRM demonstrated similar reactivity with peripheral blood plasma as clinical samples in routine methods (RM) of RIA, ELISA, and CLEIA. In comparison between RM and CM, the results in regression analysis indicated that the range of the correlation coefficient (r) was 0.913 – 0.991, the range of y intercept was 0.9 – 67.3 pg/mL and the range of slope was 0.869 – 1.174. The values by RM in 100 – 150 pg/mL for the diagnostic level, had a significant calibration effect, and the relative difference between calibrated value in RM and result by CM was within ±20%. Furthermore, the calibrated value using the serum CRM was 10,187 pg/mL, which corresponds to measured value of 14,000 pg/mL using RIA for the adrenal venous sampling. Measured values between plasma and serum as a sample for the aldosterone measurement from clinical samples showed no significant differences. In conclusion, we succeeded to prepare the certified reference material of aldosterone for RM. Then, we can accurately calculate corrected values by using our equation for four RMs of determination of aldosterone.
Key words: Standardization, Serum certified reference material, Traceability, Calibration
by the Japan Endocrine Society[1, 2]. Furthermore, the procedure for adrenal venous sampling (AVS), which is required to determine PA treatment strategies after a definite diagnosis of PA, and the localized diagnostic criteria are described in the guidelines [1, 2] or in the textbook [3].
As screening for the PA diagnosis, plasma aldoste-rone concentration (PAC) and plasma renin activity
Original
©The Japan Endocrine Society
Submitted Jun. 14, 2016; Accepted Jul. 28, 2016 as EJ16-0304Released online in J-STAGE as advance publication Sep. 2, 2016Correspondence to: Tetsuo Nishikawa, M.D., Ph.D., Endocrinology and Diabetes Center, Yokohama Rosai Hospital, 3211 Kozukue-cho, Kohoku-ku, Yokohama City, Kanagawa 222-0036, Japan. E-mail: [email protected]
1066 Nishikawa et al.
samples and 4) collaboration study using comparison method and routine methods.
The Reference Material Institute for Clinical Chemistry Standards (ReCCS) was responsible for preparation of serum reference material. ReCCS mainly performed the following tasks: preparation of serum raw materials, property tests and infection tests on the raw material, concentration preparation and concentration confirmation. The National Metrology Institute of Japan (NMIJ) was responsible for deter-mining the certified value of the serum reference mate-rial. The concentration of the certified value of the serum certified reference material (serum CRM) was determined by ID-LC/MS/MS, which is isotope dilu-tion-mass spectrometry for reference measurement procedure. In clinical group, peripheral blood and adrenal venous samplings (AVS) were collected as clinical samples in each of the collaborating clinical institutions, after obtaining informed consent from the patient and with the approval of the respective ethical review boards.
The manufacturer’s group was responsible for col-laboration study of the calibration effect using com-parison method and routine methods. The calibration effect using serum CRM was investigated for these measured values.
(PRA) are used. In the PAC measurements routine methods by RIA are mainly used in Japan. However, considering the rapid measurements needed in rou-tine medical care, routine methods using nonRIA are more useful. In clinically, standardization of aldoste-rone measurement has been needed to ensure com-parability of measured values of the current RIA and nonRIA.
The aim of this study is to establish a serum certified reference material (serum CRM) by reference mea-surement procedure for standardization of aldosterone measurement in blood and to evaluate the calibration effect for routine methods with the serum CRM using comparison method. Comparison between plasma and serum as a sample for the aldosterone measurement from clinical samples was also examined.
Materials and Methods
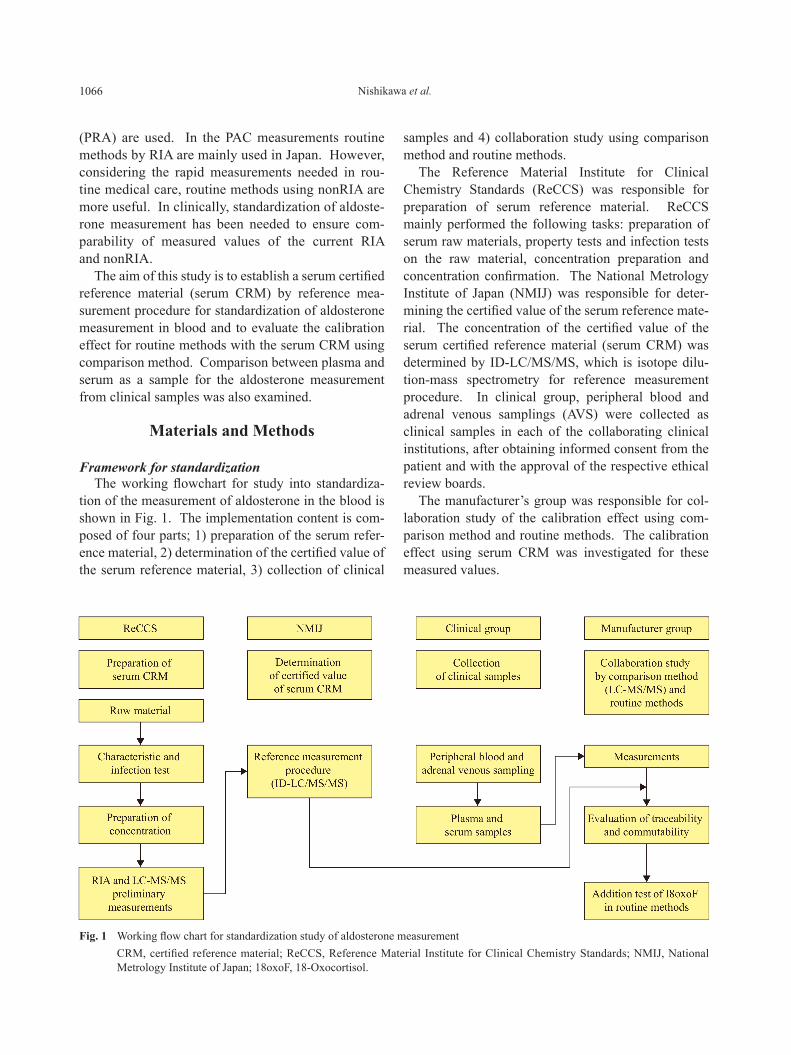
Framework for standardizationThe working flowchart for study into standardiza-
tion of the measurement of aldosterone in the blood is shown in Fig. 1. The implementation content is com-posed of four parts; 1) preparation of the serum refer-ence material, 2) determination of the certified value of the serum reference material, 3) collection of clinical
Fig. 1 Working flow chart for standardization study of aldosterone measurement CRM, certified reference material; ReCCS, Reference Material Institute for Clinical Chemistry Standards; NMIJ, National
Metrology Institute of Japan; 18oxoF, 18-Oxocortisol.

1067Reference of aldosterone measurement
Participated proceduresThe list of participated procedures is shown in Table
1. ID-LC/MS/MS was used as the reference measure-ment procedure, and LC-MS/MS was used as the com-parison method. Two types of RIA (same kit) and three types of nonRIA were used as the routine methods. The nonRIA routine method included a candidate rou-tine method. These RIA and nonRIA routine methods have become direct measurement procedure.
Metrological traceability of aldosterone measurement in blood
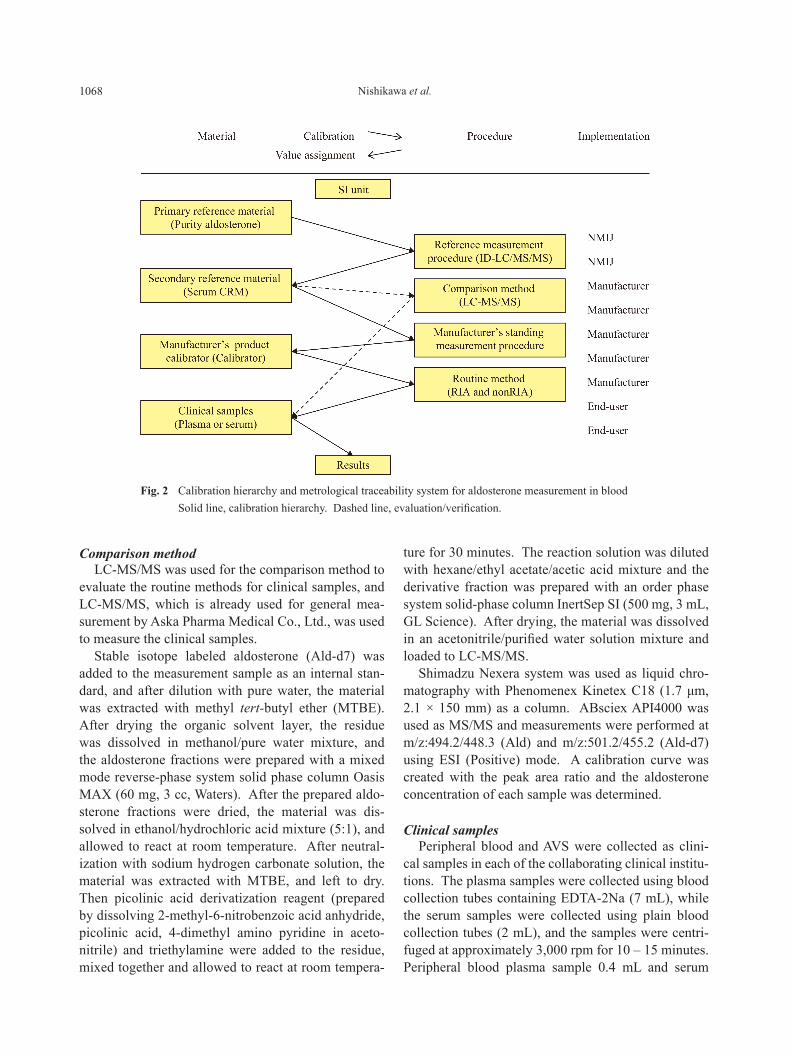
The scheme to transfer the accuracy (accuracy of measurement is related to both trueness of measure-ment and precision of measurement) required for stan-dardized operations has assembled the measurement system shown in Fig. 2 in accordance with the metro-logical traceability chain based on ISO17511 [4], which is applied to standardization in clinical laboratory.
Therefore, transferability of accuracy runs in the order from top to bottom: purity reference mate-rial, isotopic dilution -mass spectrometry (ID-LC/MS/MS), serum certified reference material (serum CRM), manufacturer’s standing measurement proce-dure (same as a kit), calibrator (exclusively used for the kit), routine measurement procedures (kit) and clinical samples.
The types of patient samples used for measurement aldosterone with the routine method are plasma and/or serum. At present, cases using both plasma and serum, or plasma alone exist for the routine meth-
ods, so the calibration standard for the routine meth-ods is the reference standard (serum certified refer-ence material).
Preparation of serum reference materialThe base serum of reference material for aldoste-
rone measurement was prepared with healthy human serum by mixing together 20 or more samples in accor-dance with the CLSI CA37-A guideline [5]. Adding a pure aldosterone (manufactured by Sigma-Aldrich) to the base serum, samples at three concentrations as 200 pg/mL, 400 pg/mL and 800 pg/mL were prepared. These serum reference materials satisfied the raw material specifications for the reference standard [6]. Dispensed the homogeneous samples of the prepared three concentrations, and frozen the dispensed sam-ples in a cryostat at -75°C, and appropriately stored the samples at the same temperature until delivery.
Value assignment and validation of serum certified reference material
For value assignment to the serum certified refer-ence material, aldosterone (Lot SLBF 3506V, purity 95 ± 1 (%), Sigma-Aldrich) for which the purity has been determined by NMIJ was used to create a cali-bration curve, and isotope dilution-mass spectrome-try (ID-MS) [7, 8] was performed. ID-MS used the isotope dilution-liquid chromatography tandem mass spectrometry (ID-LC/MS/MS).
The serum density was measured using a mechani-cal oscillator densitometer.
Table 1 Participated procedures
Procedure PrincipleAutomated
chemiluminescencesystem
Implementation
Reference measurement procedure ID-LC/MS/MS ― National Metrology Institute of Japan
Comparison method LC-MS/MS ― Aska Pharma Medical Co., Ltd., Japan
Routine method
ELISA * ― Cosmic Corporation, Japan
RIA ** ― Fujirebio Inc., Japan
CLEIA * CL-JACK®NX Kyowa Medex Co., Ltd., Japan
RIA *** ― LSI Medience Corporation, Japan
CLEIA * ― Wako Pure Chemical Industries, Ltd., Japan
ID-LC/MS/MS, isotope dilution-liquid chromatography/mass spectrometry/mass spectrometry; LC-MS/MS, liquid chromatography-mass spectrometry/mass spectrometry; RIA, radioimmunoassay; CLEIA, chemiluminescent enzyme immunoassay; ELISA, enzyme-linked immuno-sorbent assay; * candidate routine method, ** Spac S Aldosterone kit, *** measurement of clinical serum samples using Spac S Aldosterone kit.
1068 Nishikawa et al.
Comparison method LC-MS/MS was used for the comparison method to
evaluate the routine methods for clinical samples, and LC-MS/MS, which is already used for general mea-surement by Aska Pharma Medical Co., Ltd., was used to measure the clinical samples.
Stable isotope labeled aldosterone (Ald-d7) was added to the measurement sample as an internal stan-dard, and after dilution with pure water, the material was extracted with methyl tert-butyl ether (MTBE). After drying the organic solvent layer, the residue was dissolved in methanol/pure water mixture, and the aldosterone fractions were prepared with a mixed mode reverse-phase system solid phase column Oasis MAX (60 mg, 3 cc, Waters). After the prepared aldo-sterone fractions were dried, the material was dis-solved in ethanol/hydrochloric acid mixture (5:1), and allowed to react at room temperature. After neutral-ization with sodium hydrogen carbonate solution, the material was extracted with MTBE, and left to dry. Then picolinic acid derivatization reagent (prepared by dissolving 2-methyl-6-nitrobenzoic acid anhydride, picolinic acid, 4-dimethyl amino pyridine in aceto-nitrile) and triethylamine were added to the residue, mixed together and allowed to react at room tempera-
ture for 30 minutes. The reaction solution was diluted with hexane/ethyl acetate/acetic acid mixture and the derivative fraction was prepared with an order phase system solid-phase column InertSep SI (500 mg, 3 mL, GL Science). After drying, the material was dissolved in an acetonitrile/purified water solution mixture and loaded to LC-MS/MS.
Shimadzu Nexera system was used as liquid chro-matography with Phenomenex Kinetex C18 (1.7 μm, 2.1 × 150 mm) as a column. ABsciex API4000 was used as MS/MS and measurements were performed at m/z:494.2/448.3 (Ald) and m/z:501.2/455.2 (Ald-d7) using ESI (Positive) mode. A calibration curve was created with the peak area ratio and the aldosterone concentration of each sample was determined.
Clinical samplesPeripheral blood and AVS were collected as clini-
cal samples in each of the collaborating clinical institu-tions. The plasma samples were collected using blood collection tubes containing EDTA-2Na (7 mL), while the serum samples were collected using plain blood collection tubes (2 mL), and the samples were centri-fuged at approximately 3,000 rpm for 10 – 15 minutes. Peripheral blood plasma sample 0.4 mL and serum
Fig. 2 Calibration hierarchy and metrological traceability system for aldosterone measurement in blood Solid line, calibration hierarchy. Dashed line, evaluation/verification.

1069Reference of aldosterone measurement
sample 0.5 mL, AVS plasma sample 0.1 mL and serum sample 0.2 mL were dispensed as measurement sam-ples, and all the samples were used for measurement after freezing. Furthermore, sample collection was implemented after obtaining informed consent from the patient and with the approval of the ethical review boards in the applicable facility.
Measurement by comparison method and routine methods
Measurements by comparison method and rou-tine methods were performed in accordance with the respective standard operating procedures (SOP).
Measurement of serum certified reference materialMeasurements of serum CRM by comparison
method and routine methods were performed by taking two measurements for each level of serum CRM and using the mean value for data analysis.
Measurement of clinical samplesMeasurement of clinical samples by the compari-
son method and routine methods were performed by taking one measurement for the comparison method and duplicate measurements for each of the routine methods, and the mean value of each was used for data analysis.
Measurement of high concentration serumHigh concentration serum was prepared by add-
ing aldosterone to the serum to make the concentra-tion value approximately 14,000 pg/mL, each of these samples were measured duplicate with ID-LC/MS/MS, LC-MS/MS and the routine method (A–D) and the mean values were used for data analysis.
Influence of 18-Oxocortisol in serumTo confirm the influence of 18-Oxocortisol
with the routine methods, various quantities of 18-Oxocortisol (Aska Pharma Medical Co., Ltd.) were added to the serum to make the final concen-trations as 0, 100, 200, 300, 400, 500 pg/mL, each of these were measured duplicate measurements and the mean values were used for analysis. The measure-ment samples were prepared by manufacturer of the routine methods.
Comparison of plasma and serumNormally plasma is used as samples for measure-
ment of aldosterone in the blood. The CRM matrix is serum. Then sets of plasma and serum were measured using RIA and the measurement results were compared.
Results
Measurement performance of participated proce-dures
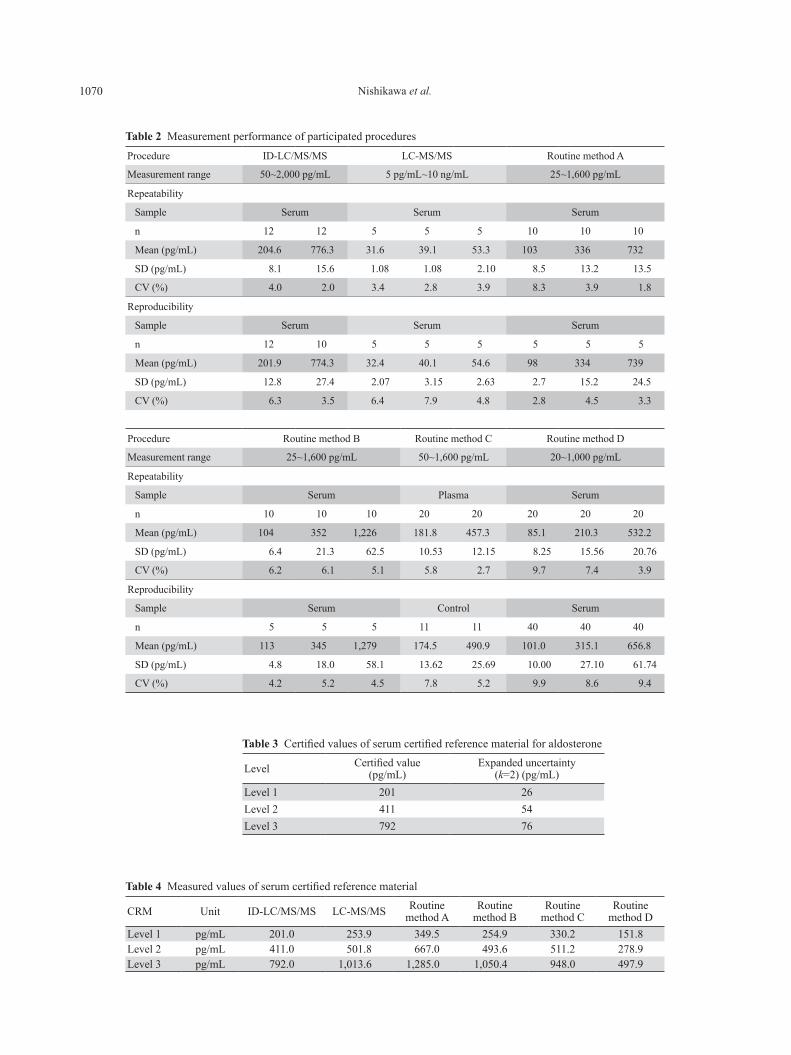
Measurement performance of measurement proce-dures is shown in Table 2. Measurement performance was evaluated by measurement range, intra-assay pre-cision (repeatability) and inter-assay precision (repro-ducibility). ID-LC/MS/MS was the measurement results of serum CRM, while LC-MS/MS and routine methods (A–D) were each reported from the respec-tive manufacturers. The precision performances of all measurement procedures were within 10 % in the CV values.
Certified value of serum certified reference materialThe certified values and their uncertainties of serum
CRM for aldosterone measurement are shown in Table 3. The mass concentration was calculated using the 25°C density (1.0235 g/cm3) obtained with the mechanical oscillator densitometer.
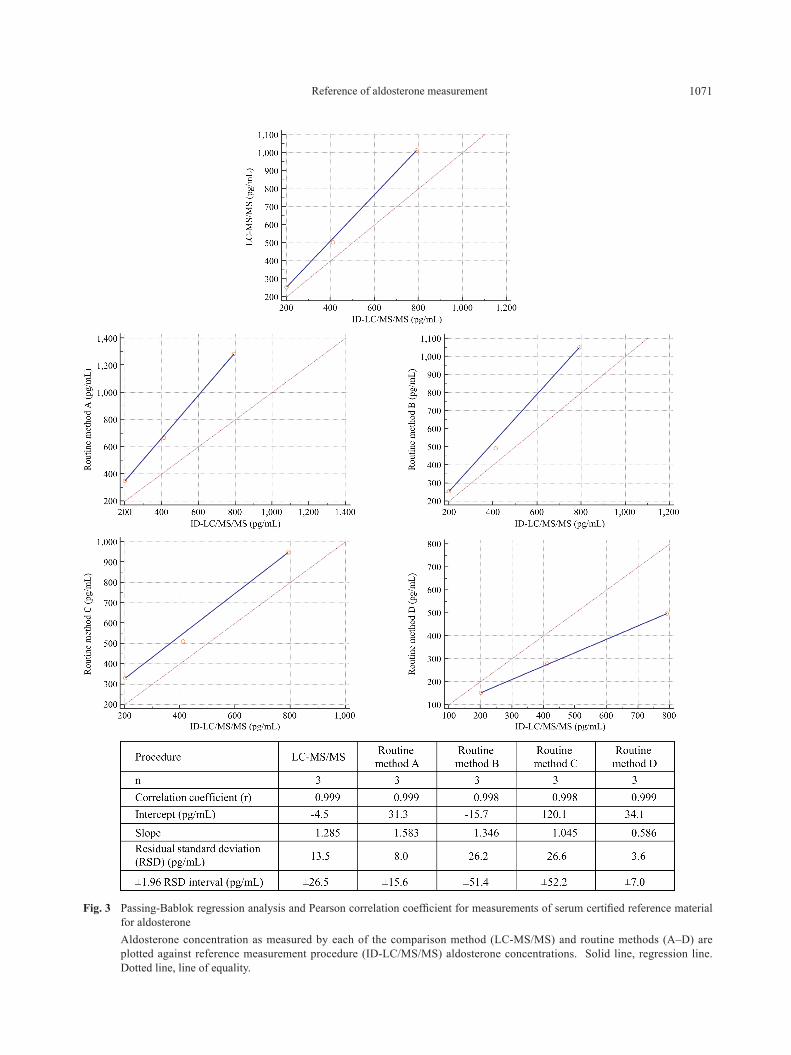
Uncertainties from preparation of the reference material, standard solution, weighing of the sam-ple solution and the calibration curve were also taken into consideration to estimate the standard uncertainty of the quantitative value. Furthermore, uncertainties derived from homogeneity and stability were added, and finally the coverage factor was set as k=2 and set as the expanded uncertainty. The measurement results of serum CRM are shown in Table 4. The certified values were obtained by ID-LC/MS/MS, while the mean val-ues were obtained from LC-MS/MS and routine meth-ods (A–D) in the duplicate measurements. The results of the Passing-Bablok regression analysis and Pearson correlation coefficient plotted against ID-LC/MS/MS value are shown in Fig. 3 for each comparison method and routine method. The results indicate that the r range was 0.998 – 0.999, the y intercept range was -4.5 – 120.1 pg/mL, the slope was 0.586 – 1.583 and the residual standard deviation (RSD) range was 3.6 – 26.6 pg/mL. Also, based on the Passing-Bablok regression analysis for serum CRM, the calibration equation (Yi= -(a/b) + (1/b) Xi) was calculated for serum CRM for each of the LC-MS/MS and routine methods (A–D).
1070 Nishikawa et al.
Table 3 Certified values of serum certified reference material for aldosterone
Level Certified value (pg/mL)
Expanded uncertainty (k=2) (pg/mL)
Level 1 201 26Level 2 411 54Level 3 792 76
Table 4 Measured values of serum certified reference material
CRM Unit ID-LC/MS/MS LC-MS/MS Routine method A
Routine method B
Routine method C
Routine method D
Level 1 pg/mL 201.0 253.9 349.5 254.9 330.2 151.8Level 2 pg/mL 411.0 501.8 667.0 493.6 511.2 278.9Level 3 pg/mL 792.0 1,013.6 1,285.0 1,050.4 948.0 497.9
Table 2 Measurement performance of participated procedures
Procedure ID-LC/MS/MS LC-MS/MS Routine method A
Measurement range 50~2,000 pg/mL 5 pg/mL~10 ng/mL 25~1,600 pg/mL
Repeatability
Sample Serum Serum Serum
n 12 12 5 5 5 10 10 10
Mean (pg/mL) 204.6 776.3 31.6 39.1 53.3 103 336 732
SD (pg/mL) 8.1 15.6 1.08 1.08 2.10 8.5 13.2 13.5
CV (%) 4.0 2.0 3.4 2.8 3.9 8.3 3.9 1.8
Reproducibility
Sample Serum Serum Serum
n 12 10 5 5 5 5 5 5
Mean (pg/mL) 201.9 774.3 32.4 40.1 54.6 98 334 739
SD (pg/mL) 12.8 27.4 2.07 3.15 2.63 2.7 15.2 24.5
CV (%) 6.3 3.5 6.4 7.9 4.8 2.8 4.5 3.3
Procedure Routine method B Routine method C Routine method D
Measurement range 25~1,600 pg/mL 50~1,600 pg/mL 20~1,000 pg/mL
Repeatability
Sample Serum Plasma Serum
n 10 10 10 20 20 20 20 20
Mean (pg/mL) 104 352 1,226 181.8 457.3 85.1 210.3 532.2
SD (pg/mL) 6.4 21.3 62.5 10.53 12.15 8.25 15.56 20.76
CV (%) 6.2 6.1 5.1 5.8 2.7 9.7 7.4 3.9
Reproducibility
Sample Serum Control Serum
n 5 5 5 11 11 40 40 40
Mean (pg/mL) 113 345 1,279 174.5 490.9 101.0 315.1 656.8
SD (pg/mL) 4.8 18.0 58.1 13.62 25.69 10.00 27.10 61.74
CV (%) 4.2 5.2 4.5 7.8 5.2 9.9 8.6 9.4
1071Reference of aldosterone measurement
Fig. 3 Passing-Bablok regression analysis and Pearson correlation coefficient for measurements of serum certified reference material for aldosterone
Aldosterone concentration as measured by each of the comparison method (LC-MS/MS) and routine methods (A–D) are plotted against reference measurement procedure (ID-LC/MS/MS) aldosterone concentrations. Solid line, regression line. Dotted line, line of equality.
1072 Nishikawa et al.
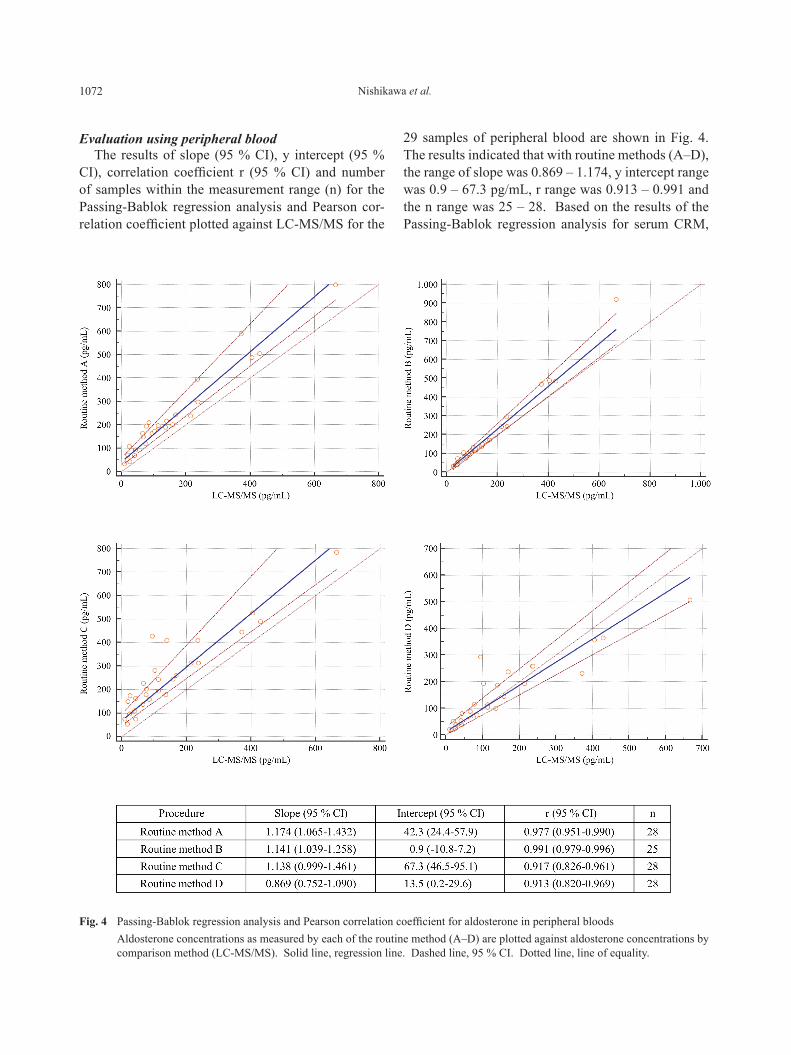
Evaluation using peripheral bloodThe results of slope (95 % CI), y intercept (95 %
CI), correlation coefficient r (95 % CI) and number of samples within the measurement range (n) for the Passing-Bablok regression analysis and Pearson cor-relation coefficient plotted against LC-MS/MS for the
29 samples of peripheral blood are shown in Fig. 4. The results indicated that with routine methods (A–D), the range of slope was 0.869 – 1.174, y intercept range was 0.9 – 67.3 pg/mL, r range was 0.913 – 0.991 and the n range was 25 – 28. Based on the results of the Passing-Bablok regression analysis for serum CRM,
Fig. 4 Passing-Bablok regression analysis and Pearson correlation coefficient for aldosterone in peripheral bloods Aldosterone concentrations as measured by each of the routine method (A–D) are plotted against aldosterone concentrations by
comparison method (LC-MS/MS). Solid line, regression line. Dashed line, 95 % CI. Dotted line, line of equality.
1073Reference of aldosterone measurement
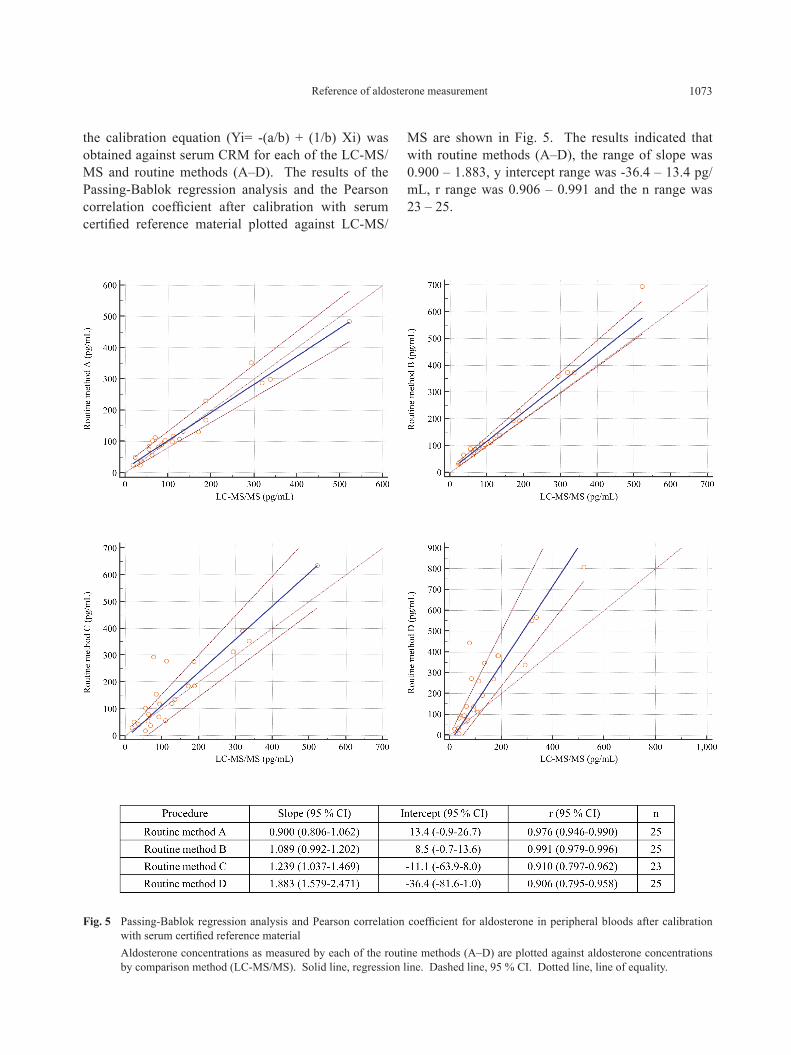
the calibration equation (Yi= -(a/b) + (1/b) Xi) was obtained against serum CRM for each of the LC-MS/MS and routine methods (A–D). The results of the Passing-Bablok regression analysis and the Pearson correlation coefficient after calibration with serum certified reference material plotted against LC-MS/
MS are shown in Fig. 5. The results indicated that with routine methods (A–D), the range of slope was 0.900 – 1.883, y intercept range was -36.4 – 13.4 pg/mL, r range was 0.906 – 0.991 and the n range was 23 – 25.
Fig. 5 Passing-Bablok regression analysis and Pearson correlation coefficient for aldosterone in peripheral bloods after calibration with serum certified reference material
Aldosterone concentrations as measured by each of the routine methods (A–D) are plotted against aldosterone concentrations by comparison method (LC-MS/MS). Solid line, regression line. Dashed line, 95 % CI. Dotted line, line of equality.
1074 Nishikawa et al.
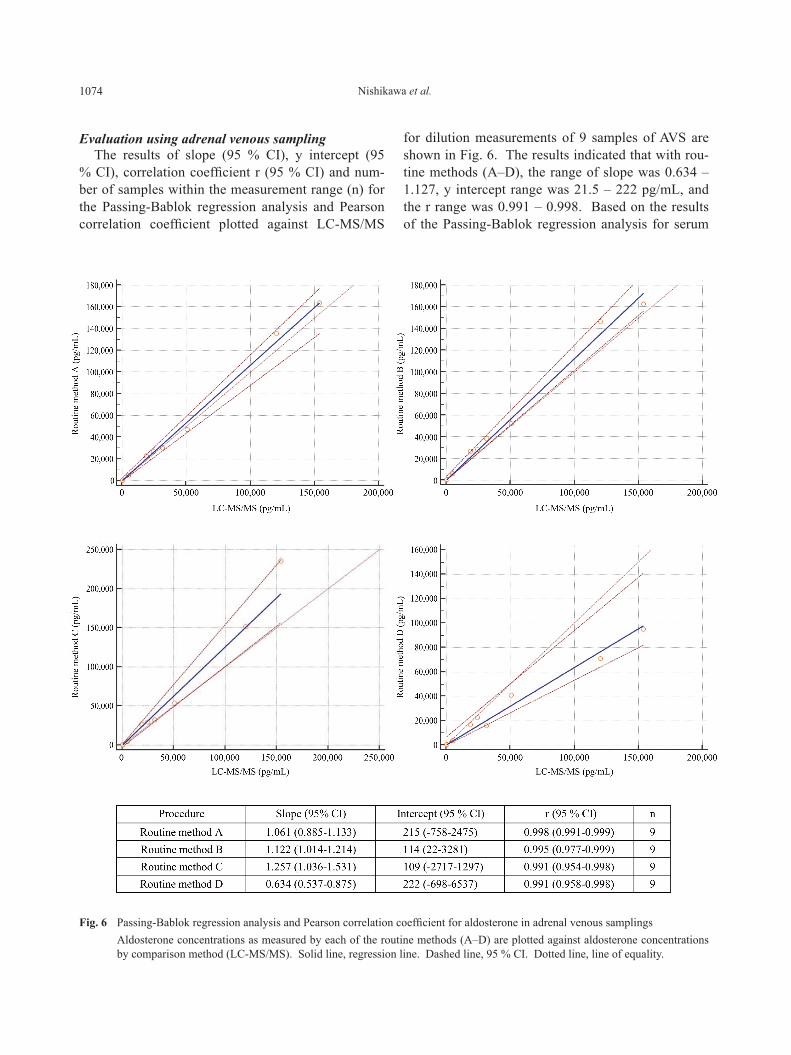
Evaluation using adrenal venous samplingThe results of slope (95 % CI), y intercept (95
% CI), correlation coefficient r (95 % CI) and num-ber of samples within the measurement range (n) for the Passing-Bablok regression analysis and Pearson correlation coefficient plotted against LC-MS/MS
for dilution measurements of 9 samples of AVS are shown in Fig. 6. The results indicated that with rou-tine methods (A–D), the range of slope was 0.634 – 1.127, y intercept range was 21.5 – 222 pg/mL, and the r range was 0.991 – 0.998. Based on the results of the Passing-Bablok regression analysis for serum
Fig. 6 Passing-Bablok regression analysis and Pearson correlation coefficient for aldosterone in adrenal venous samplings Aldosterone concentrations as measured by each of the routine methods (A–D) are plotted against aldosterone concentrations
by comparison method (LC-MS/MS). Solid line, regression line. Dashed line, 95 % CI. Dotted line, line of equality.
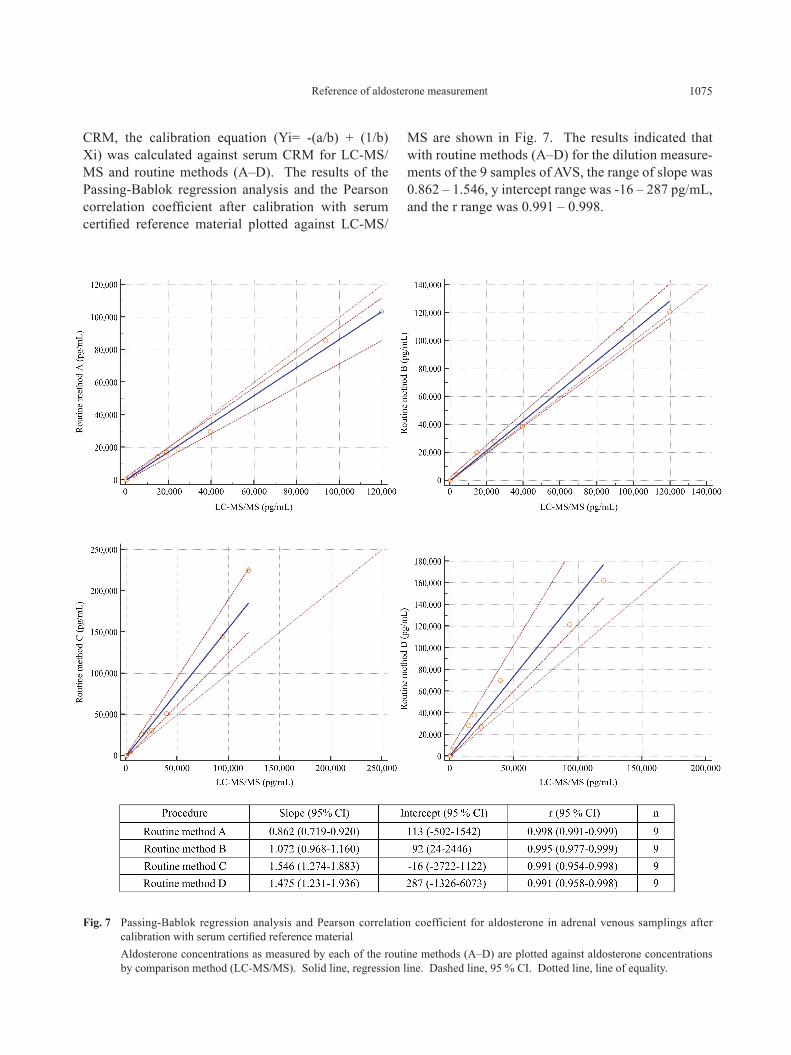
1075Reference of aldosterone measurement
CRM, the calibration equation (Yi= -(a/b) + (1/b) Xi) was calculated against serum CRM for LC-MS/MS and routine methods (A–D). The results of the Passing-Bablok regression analysis and the Pearson correlation coefficient after calibration with serum certified reference material plotted against LC-MS/
MS are shown in Fig. 7. The results indicated that with routine methods (A–D) for the dilution measure-ments of the 9 samples of AVS, the range of slope was 0.862 – 1.546, y intercept range was -16 – 287 pg/mL, and the r range was 0.991 – 0.998.
Fig. 7 Passing-Bablok regression analysis and Pearson correlation coefficient for aldosterone in adrenal venous samplings after calibration with serum certified reference material
Aldosterone concentrations as measured by each of the routine methods (A–D) are plotted against aldosterone concentrations by comparison method (LC-MS/MS). Solid line, regression line. Dashed line, 95 % CI. Dotted line, line of equality.
1076 Nishikawa et al.
Measurement of clinical samples under 400 pg/mL level
The results of comparability evaluation using Passing-Bablok regression analysis for routine meth-ods (A–D) before and after calibration with serum CRM for measurement values less than 400 pg/mL are shown in Table 5. The results indicated that the resid-ual standard deviation (RSD) calibrated with serum CRM reduced from 22.0 pg/mL to 17.6 pg/mL with routine method (A), from 14.3 pg/mL to 10.9 pg/mL with routine method (B), from 49.6 pg/mL to 42.4 pg/mL with routine method (C) and from 40.9 pg/mL to 43.3 pg/mL with routine method (D).
Measurement of high concentration serumThe measurement results of high concentration
serum samples are shown in Table 6. The results indi-cated that range of difference in the relative values plotted against ID-LC/MS/MS was -24.8 – 62.0 %. The ID-LC/MS/MS value corresponding to 14,000 pg/
mL by RIA was 10,780 pg/mL. For the 14,000 pg/L by RIA the calibrated value using serum CRM was 10,187 pg/mL.
Influence of 18-Oxocortisol in serumThe results of the influence of 18-Oxocortisol are
shown in Table 7. The results indicated that with the reported routine methods (A–C) the degree of influ-ence of 18-Oxocortisol was 0 – 65 % in 1,200 pg/mL, 0 – 16 % in 300 pg/mL, 0 – 14 % in 400 pg/mL and 2 – 24 % in 500 pg/mL.
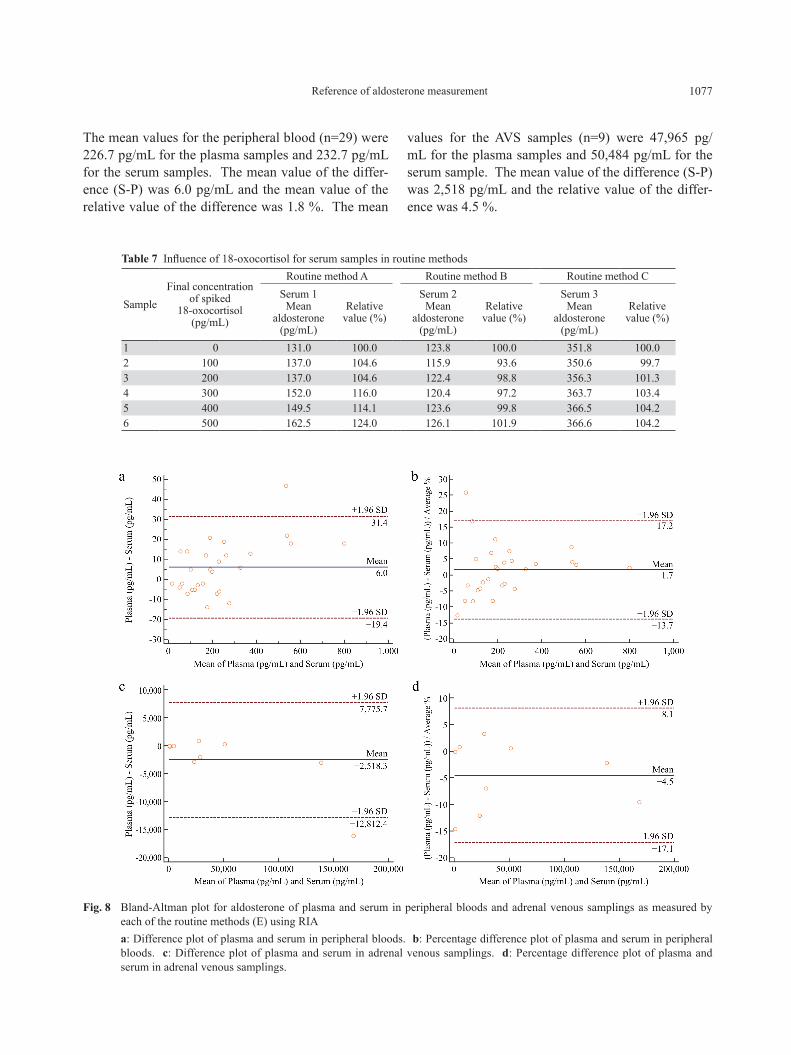
Comparison between plasma samples and serum samples
We compared measurement values of 38 sets of plasma and serum samples collected at the same time with routine methods (E) of RIA. The results are shown as a Bland-Altman Plot in Fig. 8 showing the mean value of plasma (P) and serum (S) with 29 sam-ples of peripheral blood and with 9 samples of AVS.
Table 5 Comparison study by using under 400 pg/mL aldosterone with comparison method (LC-MS/MS) in peripheral bloodsRoutine method A Routine method B Routine method C Routine method D
CRM * CRM * CRM * CRM *Before
calibrationAfter
calibrationBefore
calibrationAfter
calibrationBefore
calibrationAfter
calibrationBefore
calibrationAfter
calibrationn 25 22 22 22 25 20 25 22Lowest value (pg/mL) 33.6 24.0 29.1 33.2 53.9 16.7 20.2 8.1Highest value (pg/mL) 587.5 351.5 468.0 359.4 445.6 311.5 293.8 443.0Arithmetic mean 179.2 105.3 138.1 114.2 220.8 129.5 123.5 176.1Median (pg/mL) 172.0 100.0 111.1 94.2 193.1 109.3 99.9 127.9Standard deviation (pg/mL) 119.7 72.9 101.1 75.1 114.0 95.7 84.1 136.5Standard error of the mean (pg/mL) 23.9 15.5 21.6 16.0 22.8 21.4 16.8 29.1
Residual standard deviation (RSD) (pg/mL) 22.0 17.6 14.3 10.9 49.6 42.4 40.9 43.3
±1.96 RSD interval (pg/mL) ±43.1 ±34.5 ±28.1 ±21.3 ±97.3 ±83.2 ±80.1 ±84.9* CRM, serum certified reference material.
Table 6 Aldosterone spiked high concentration serum sample
Procedure ID-LC/MS/MS LC-MS/MS Routine method A
Routine method B
Routine method C
Routine method D
Mean (pg/mL) 12,437 14,482 16,150 20,143 17,578 9,349Relative value against ID-LC/MS/MS (%) 100.0 116.4 129.9 162.0 141.3 75.2
Relative value of difference agaist ID-LC/MS/MS (%) 0.0 16.4 29.9 62.0 41.3 -24.8
Corrected value with serum certified reference material (pg/mL) ― 11,270 10,187 14,978 16,707 15,891
Relative value of corrected value (%) 100.0 90.6 81.9 120.4 134.3 127.8
1077Reference of aldosterone measurement
The mean values for the peripheral blood (n=29) were 226.7 pg/mL for the plasma samples and 232.7 pg/mL for the serum samples. The mean value of the differ-ence (S-P) was 6.0 pg/mL and the mean value of the relative value of the difference was 1.8 %. The mean
values for the AVS samples (n=9) were 47,965 pg/mL for the plasma samples and 50,484 pg/mL for the serum sample. The mean value of the difference (S-P) was 2,518 pg/mL and the relative value of the differ-ence was 4.5 %.
Table 7 Influence of 18-oxocortisol for serum samples in routine methods
SampleFinal concentration
of spiked 18-oxocortisol
(pg/mL)
Routine method A Routine method B Routine method CSerum 1
Meanaldosterone
(pg/mL)
Relative value (%)
Serum 2Mean
aldosterone (pg/mL)
Relative value (%)
Serum 3Mean
aldosterone (pg/mL)
Relativevalue (%)
1 0 131.0 100.0 123.8 100.0 351.8 100.02 100 137.0 104.6 115.9 93.6 350.6 99.73 200 137.0 104.6 122.4 98.8 356.3 101.34 300 152.0 116.0 120.4 97.2 363.7 103.45 400 149.5 114.1 123.6 99.8 366.5 104.26 500 162.5 124.0 126.1 101.9 366.6 104.2
Fig. 8 Bland-Altman plot for aldosterone of plasma and serum in peripheral bloods and adrenal venous samplings as measured by each of the routine methods (E) using RIA
a: Difference plot of plasma and serum in peripheral bloods. b: Percentage difference plot of plasma and serum in peripheral bloods. c: Difference plot of plasma and serum in adrenal venous samplings. d: Percentage difference plot of plasma and serum in adrenal venous samplings.

1078 Nishikawa et al.
Discussion
Fresh sera obtained from healthy individuals are used generally as the base for serum CRM. The serum samples in which antigens and antibodies for specific infections have not been detected, and the biochemi-cal components are within the prescribed concentra-tion range [5, 6] were used in this study. When healthy human serum is used for fundamental analysis, pure aldosterone was spiked to obtain a target high concen-tration. In this study, the serum CRM was prepared by spiking with Sigma-Aldrich aldosterone. Generally plasma samples are measured in routine method. However, matrix reference materials are generally pre-pared using serum as a base for ensuring the stabil-ity and other reasons. Therefore, in this standardiza-tion study of aldosterone measurement in blood, it was required that serum CRM was used for calibration of routine methods. The comparison method as a con-trol for evaluation testing can apply a large number of samples, where the comparison method has commut-ability with the reference measurement procedure. We chose LC-MS/MS as a comparison method. LC-MS/MS applied for measurement of clinical samples is rou-tinely implemented in the respective facilities, so this was not particularly set as a condition to be imple-mented as a comparison method. Therefore, the tol-erance range for quality control (QC) was compara-tively broad. As a result, particularly when assessing the comparability with reference measurement proce-dures, there were cases where there was a maximum difference of 25 %. Fortunately, LC-MS/MS has been operated routinely for measurement of clinical samples as a comparison method for aldosterone measurement in blood. Then, we performed to ensure the accuracy of this method by using serum CRM (Figs. 5 – 7).
When establishing the serum CRM, it is necessary to demonstrate a similar reactivity of the serum CRM with the patient sample with the routine method. We evaluated comparability for 38 patient samples, includ-ing AVS samples. In the measurement values of the patient sample and serum CRM, each of the regres-sion formulae had a 95 % CI for each of the regres-sion analyses for the reference measurement proce-dure and between the comparison method and routine method. We could confirm that the serum CRM reac-tivity demonstrated a similar level of reactivity to that of the patient samples (Figs. 3 and 4). In the compari-son of the calibration values against 5 samples at 100
– 150 pg/mL, which were close to the diagnosis value, we confirmed that there was a marked calibration effect in routine methods as RIA and CLEIA, and the rela-tive difference against comparison method was within ±20 % (Table 5). In one of CLEIA and ELISAwhich did not obtained sufficient calibration effect, it is nec-essary to revise for reactivity to the clinical samples for enhancement of more specificity and reliability.
Furthermore, another consideration is the inclu-sion of 18-Hydroxycortisol (18OHF), 18-Oxocortisol (18oxoF) and 18-Hydroxycorticosterone (18OHB) as so-called hybrid steroids (steroidogenic intermediates) in PA patients’ AVS high level samples. These samples demonstrated cross reaction using the current RIA. These samples may show cross reaction even with nonRIA with polyclonal antibodies. With the current routine methods, while it may be difficult to ascertain an accurate measurement value for specimens around AVS 14,000 pg/mL, a hybrid steroid mix is not prob-lematic for specimens less than 200 pg/mL, apart from the technical issues of specimen dilution [9].
In reports that compared the correlation of aldoste-rone using PA and 18OHB, 18OHF, and 18oxoF for the subtype diagnosis flowchart patient samples and routine methods regarding the correlation between LC-MS/MS and RIA, when comparing patient samples with GRA (glucocorticoid-remediable aldosteronism), APA (aldosterone-producing adenoma), BAH (bilat-eral adrenal hyperplasia) and EH (low-renin essential hypertension), a reaction was noted with cortisol sub-stances in APA and BAH samples [9, 10].
Also, in reports that investigated the effectiveness of 18oxoF and 18OHF in plasma for identification of PA and BHA (bilateral hyperaldosteronism), in the correlation between LC-MS/MS and RIA for plasma aldosterone (PAC), the results of regression analysis of 90 patient samples indicated that the slope was high at approximately 25 %. In particular, with low range PAC, the possibility of measuring 18oxoF and 18OHF, etc. is not zero, but cases of 330 pg/mL using RIA were PA, where tumors were found on CT scans [10]. The mix of 18OHF, 18oxoF and 18OHB is thought to not pose diagnostic problems when differentiating dif-ferences in the left and right adrenals using AVS, how-ever, it is essential to give adequate consideration to peripheral blood. In the future, after the serum refer-ence material has been officially set, and when it has been set to function as a comparison method, operat-ing procedures, such as confirmation processes using

1079Reference of aldosterone measurement
the serum reference material, are to be reset, and if the measurements are out of alignment, then it is essen-tial to create standard operating procedures (SOP) for measurement of the serum reference material in a traceable condition by conducting calibration, etc. Furthermore, It is necessary to perform periodically for evaluation and calibration with the serum CRM.
In conclusion, we could establish the serum CRM and comparison method in this study on standardiza-tion of measurement of aldosterone. In standardiza-tion operations, which are being proactively driven forward, the first priority is to assemble a traceability chain for the measurements, and finally to establish an actual sample reference material (serum CRM) based on serum. This serum CRM will become the latest high order calibrator for the routine methods. Calibrating routine methods using this serum CRM will enable comparability between routine methods. In the future, to standardize the routine methods and to meet them to the demands of clinical practice, firstly, a reactivity evaluation testing should be conducted using clinical samples, and then if the reaction profile of the routine method is satisfied, the methods can be used in clinical care by conducting calibration testing on the accuracy of the method. Immunoassay is used as a measuring principle for routine methods for measurement aldo-sterone in the blood. The basic concepts for measure-ment performance with these types of routine methods are rapidity in promptly delivering the measurement results to clinical practice, and precision of the mea-surements. However, if we demand the accuracy, the
rapidity will not be satisfied. To further improve the methods to ensure a high degree of reaction specific-ity should be required and, we consider that it is nec-essary to undertake work including an improvement in specificity of antibody and assay systems. It would be particularly desirable to have kits with higher order of reaction specificity readily available in the future.
Acknowledgments
This work was partly supported by the Grant for Research on Intractable Diseases provided by the Japanese Ministry of Health, Labour and Welfare, and also the Japanese Endocrine Society supported the present studies.
Disclosure Statement
The authors declare that they have no conflicts of interest, while Cosmic Corporation, Fujirebio Inc., Kyowa Medex Co., Ltd., LSI Medience Corporation, Wako Pure Chemical Industries, Ltd., and Aska Pharma Medical Co., Ltd., Japan supported the present studies.
Author Contributions
MO, MK, AT, FS, SI, IK, HI, TY, HS TO and MN conducted the research, MO, MK, AT, KS, HS and KK reviewed and edited the manuscript, and TN, MO and KK reviewed the manuscript.
References
1. Nishikawa T, Omura M, Satoh F, Shibata H, Takahashi K, et al. (2009) Guidelines for the diagnosis and treat-ment of primary aldosteronism. Folia Endocrinol Japonica 86 Supplement-2: 1-19 (In Japanese).
2. Nishikawa T, Omura M, Satoh F, Shibata H, Takahashi K, et al. (2011) Guidelines for the diagnosis and treat-ment of primary aldosteronism ― The Japan Endocrine Society 2009. Endocr J 58: 711-721.
3. Omura M, Makita K, Matsui A, Nishikawa T (2012) Diagnosis and criteria. In Ito S and Nishikawa T (ed) Point of hypertension care, know-how and evaluation of adrenal venous sampling (AVS) for primary aldo-steronism diagnosis. Medical Review, Tokyo: 11-19 (In Japanese).
4. ISO17511 (2003) : In vitro diagnostic medical devices – Measurement of quantities in biological samples –
Metrological traceability of values assigned to calibra-tors and control materials.
5. CLSI C37-A (1999) : Preparation and validation of commutable frozen human serum pools an secondary reference materials for cholesterol measurement pro-cedures; Approved Guideline. Clinical and Laboratory Standards Institute, Wayne, Pennsylvania, USA.
6. Committee on Quality Management, Japan Society of Clinical Chemistry (2003) : Standard of matrix refer-ence material for quantitative analysis. Jpn J Clin Chem 32: 180-185 (In Japanese).
7. Yamashita K, Okuyama M, Nakagawa R, Honma S, Satoh F, et al. (2008) Development of sensitive derivatization method for aldosterone in liquid chromatography-elec-trospray ionization tandem mass spectrometry of cortico-steroids. J Chromatogr A 1200: 114-121.

1080 Nishikawa et al.
8. Kawaguchi M, Eyama S, Takatsu A (2016) Development of serum certified reference material for aldosterone measurement in blood. Anal Sci (In press).
9. Mulatero P, Mdi Cella SM, Monticone S, Schiavone D, Manzo M, et al. (2012) 18-Hydroxycorticosterone, 18-fydroxycortisol, and 18-oxocortisol in the diagno-sis of primary aldosteronism and its subtypes. J Clin
Endocrinol Metab 97: 881-889.10. Satoh F, Morimoto R, Ono Y, Iwakura Y, Omata K, et
al. (2015) : Measurement of peripheral plasma 18-oxo-cortisol can discriminate unilateral adenoma from bilat-eral diseases in patients with primary aldosteronism. Hypertension 65: 1096-1102.





























