Embed Size (px)
DESCRIPTION
Can This Fall Be Prevented?. Demi Haffenreffer, RN, MBA Email: [email protected]. OUTLINE. Risk Factors Creating a Culture of Safety Components of a good fall management program Requirements and Common Citations Assessment and Care Planning Resident Centered Care - PowerPoint PPT Presentation
Citation preview

OUTLINE Risk Factors Creating a Culture of Safety
Components of a good fall management program Requirements and Common Citations Assessment and Care Planning Resident Centered Care
When an accident happens What constitutes a fall? Conducting thorough investigations & assessments Implementing measures & updating the care plan
Quality Improvement

RISK FACTORS Anticipated vs. Unanticipated risk factors
Anticipated risk factors are those factors we should address before the resident falls
Measures are implemented after an unanticipated risk factor becomes known
Unanticipated risk factors Seizures, resident to resident behaviors, arrhythmias, CVA,
TIA, a pure accident Anticipated risk factors
Fall History Confused or possible lethargy related to med Unsteady gait or weak transfer Syncope or orthostatic hypotension Other Internal or external risk factors

RISK FACTORS
Anticipated Internal Risk factors: Cardiovascular Neuromuscular/functional Orthopedic Perceptual/Sensory Overall poor health Psychiatric or cognitive

RISK FACTORS
Anticipated External Risk Factors: Medications Appliances or devices Environmental Equipment issues Environment overall or situational hazards Poor assessment and care planning Poor communication Lack of staff knowledge

Components of a good Fall Prevention Program
Goal Driven Prevent avoidable accidents Prevent repeat falls Prevent major injuries Provide quality person-centered care Prevent citations Prevent legal actions Good communication systems Satisfied customers – residents and employees

Components
System is consistent Become a learning organization and
acknowledge high risk and error prone nature of the work we do & the people we work with
Good, consistent investigation/assessment procedures when a resident falls
Simple documentation system Blame free error reporting system but
individuals accept responsibility

Components
Assessments of risks on admission, quarterly & with condition changes
Many prevention strategies (including equipment) available to staff – including restraints as a last resort (however the program is based on a restraint free environment)
Education & orientation Multidisciplinary
Continuous Quality Improvement activities to identify problem/strength areas and improve

Common citations
Investigation/assessment not thorough and does not identify all risk factors.
Investigation/assessment not timely – resulting in another incident/fall before interventions put in place.
Investigation/assessment and interventions not based on facts or incident.

Citations continued:
Interventions not followed. Lack of supervision No investigation/assessment of accident
occurred – no new preventive plan.

Assessment and Care Planning
Upon Admission: Preliminary assessment with immediate measures
discussed with the resident & implemented Orientation of the room with an observation of how the
resident interacts with the environment Increased supervision/observation during the first few
days/evenings/nights Obtain a general history of past falls – establish trends Develop an initial care plan

Assessment and Care Planning
A comprehensive assessment within 14 days Assess and proactively implement person and
environmentally centered measures to prevent accidents
Person-centered care plan approaches What does the resident want?

Person-centered care
Begins with the investigation Resident involved &
informed of data collected, options, risks and benefits of each option
Resident decision Documentation of
assessment/cause & resident choices
Care planning Reevaluation & cp updates

What Constitutes a Fall?
Alleged fall, unwitnessed Fall Lowering to the floor Preventing a fall Rolling off a low mattress

When to complete an investigation / assessment? Alleged fall, unwitnessed Fall Resident found in a
dangerous or risky situation: Climbing out of bed Other

Culture of Safety Old Approach
Resident falls Minimal investigation
w/ much paperwork Incident report Implement an
intervention 24-hour report Move on
New Perspective Resident falls Investigative process is
thorough & consistent w/ as little paper as possible
Incident report & stepped investigative process
24-hour report Evaluation of
interventions / CQI

Conducting thorough investigations Initial step – often
performed by Charge Nurse Immediate protection of
resident as indicated Begin data collection per
guidelines Examine area and
equipment Conduct staff interviews Determine if care plan was
followed as written Gather first impressions Implement initial action &
communicate

Conducting an investigation continued: Second step – often completed by the RN Care
Manager Clinical assessment of possible causes
Medications Medical Cognitive or sensory Environment Psychosocial Physical functioning

Conducting an investigation continued: Third step - Ongoing data gathering by RN Care
Manager and/or a department head Incident trending based on prior incident information or
log Has this happened before? Similarities/differences? What was implemented in the past? Initial identification of root cause Staff assignments Other more complex environmental issues

Conducting an investigation.
Fourth Step - Analyze data What is the data telling you?
Report suspected abuse/neglect How can this be prevented from happening again? Utilize CAA guidelines to assist with assessment and
investigation. Use Interdisciplinary team Summarize findings Communicate

Conducting an investigation continued:
Fifth step – CQI and the 5 Why’s Analyze all incidents monthly in order to identify
trends and implement action plans (education, policy changes, etc.) for the safety of the entire facility and facility population (residents, staff & families)

Trending and Root Cause Analysis Possible system issues:
Physician orders not followed Care plan not followed Failure to assess risk and care plan Standards of practice not followed Resident preference not honored Illness, diagnosis related

Trending and Root Cause Analysis System issues continued:
Staff orientation Staff on break Staff training Equipment mal-function Environment/maintenance/housekeeping hazard

Trending and Root Cause Analysis Action plans for root cause(s) trends
Staff education Staff counseling Resident education Family education Change in system e.g. orientation program Environmental changes QA surveillance change Process improvement team

What to for? Falls What was resident doing?
Rising? Sitting? In bed or out of bed? During assisted transfer? To chair or from chair?
Indicate type of chair Brakes on w/c/bed Chair too low Foot rests appropriate
Self ambulating?

What to for? Falls continued: What was resident doing?
Reaching Assisted ambulation Sliding/leaning forward out of chair
Location & time of fall? Side rails?
Up, down, per care plan? Malfunctioned
Time since last voided/toileted? Call light within reach? Call light on? Time since last meal?

What to for? Falls continued: Environment/equipment a factor?
Failed or misused adaptive device? Device out of reach? Faulty equipment? Furniture? Clutter? Lighting/glare? Water on floor? Uneven floor or if outside uneven pavement?

What to for? Falls continued: Mobility alarm on? Functioning? Removed by
resident? Type of footwear?
Non-skid shoes Slippers Socks only Shoes Barefoot

What to for? Falls continued: Care Plan followed as written? Assigned staff on break? Staff in orientation? Medical factors e.g. Parkinson’s Vital signs – BP lying and sitting Diabetic? Check blood sugar

What to for? Falls continued:
Medications Any new medications? Meds in last two hours? Psychoactive Hypertension Sedative/hypnotic Narcotic
If unknown origin Interview all staff and visitors going backwards in time to
determine possible time frame for event

What to for? Falls continued: Physical functioning
Gait Upper torso weakness
Vision/sensory – glasses/hearing aide on? Need for contrasting colors?
Pain? Sitting too long? Seating Assessment done? Tired?

Falls Investigation Guides
Overview Guide Environmental Guide

Falls investigation Guides
Medication Guide Communication Guide

Case Example # 1
Background: A woman fell at home after getting caught in her small dog’s leash resulting in a fractured right hip. Following a surgical Open Reduction Internal Fixation (ORIF, hip pinning), she was admitted for skilled rehabilitative services secondary to the ground level fall. She is alert and oriented and has not experienced any memory loss.
In the skilled rehab facility, the resident had a fall at bedside after attempting to self transfer from bed while attempting to go to the bathroom due to urinary urgency. The resident was found with a skin tear to her left hand and abrasion to her left knee. The resident was immediately evaluated/assessed for injury, treatment needs and to assure comfort and safety.
Resident has a history of Congestive Heart Failure and is on diuretic therapy.
She has Hypertension and is on two different anti-hypertensive medications.
She is also on Coumadin as a preventative post surgery measure.
The physician was notified and a treatment to left hand skin tear was ordered as well as an x-ray to her left knee and her right
Begin Falls Investigation Guide
Gather 1st impressions Indentify Possible Causes
Use Communication Guide
Ensure necessary communication of information (i.e., to staff/management, family, physician, etc.)
Use Environment and Equipment Investigation Guide
Review factors related to environment and equipment
Use the Medication Investigation Guide
Review factors related to medication use
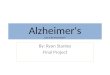
Resident Falls
The resident was witnessed resting in her bed at 1030.
The staff heard her call out at 1115. The fall was not witnessed by staff. The aide who found the resident stated that she was on her
left knee, that her left hand was bleeding, and that her right leg was extended straight and in alignment with her body.
The resident does not complain of any increase in right hip pain and her recent surgical incision is intact to her right hip. Does state she has pain to her left knee, which was found to have an abrasion, and her left hand, where a 3 cm skin tear was found and was bleeding.
The resident does not use side rails. The resident’s wheel chair was beside her bed but tipped
forward. The resident stated that she went to sit in her wheel chair
because she became dizzy on standing. Her wheel chair was tipped forward behind her and the brakes were not locked.

Figure 3: RCA/Causal Tree Diagram

Some Interventions
Non-slip surfaces Lights are automatic Raised toilet seats Half rails- arc rails – transfer poles Lower beds – Hi/low beds better Automatic bed controls Trapezes – merry walkers, etc

Some Interventions
Bedside commodes Easy to use call lights Infant monitors Pressure pads Non-slip socks/shoes Night lights Assistive devices/Equipment close by Increased supervision during time likely to fall

Some Interventions
Toilet schedules Let them sleep Familiarity Concave mattresses or bolsters Eliminate clutter Drug reductions Locks on movable equipment that work Assess them for pain & treat

Some Interventions
Benches so residents can rest Level surfaces Chair cushions and other non-slip
surfaces/wedges Move them closer Keep things in reach on their dominant side Eliminate the shine

Some Interventions
Activities Physician consults (including psych;
audiology, visual & medical) Hip protectors, helmets, knee and elbow
protectors Therapy or restorative care Restraints & alarms - consideration as a last
resort

MAY ALL YOUR SURVEYS BE SUCCESSFUL & ALL
YOUR RESIDENTS & STAFF WELL CARED FOR!