Embed Size (px)
Citation preview

Can we measure structured chronic care ?
• Michel Wensing
• Jochen Gensichen
• John Tooker

Contents the workshop
• Why measurement is important
• Patient and provider reports on chronic care
• Examples from U.S.A, and Europe
• Discussion on desired research and implications for practice and policy

Why measure chronic care ?
• To be able to optimize it (formative evaluation and internal improvement)
• To show its value (summative evaluation for transparancy, contracts, public reporting, P4P)
• But: is it measurable? Some say that structured chronic care is too complex to be measured

Specific challenges for measurement
• Chronic care often includes a range of health professionals - certainly from a patient or system perspective
• Chronic care implies things that may be absent and unknown to patients (and perhaps providers)
• Measure disease specific or generic aspects of chronic care?

Netherlands: PACIC questionnaire in general practice
Validation study in 165 patients from 4 practices
Wensing
Van Lieshout
Jung
Hermsen
Rosemann

Methods
• Diabetes patients and COPD patients, randomly sampled from practice registers
• PACIC (20 items): forward and backward translation, interviews with 15 patients, and adaptations
• Postal survey with reminders (70% response rate)

Description of the patients (n=165)
Mean age (SD) 68.0 (10.3)
Percentage women 47%
Percentage medium/high education 36%
Percentage good/excellent health status 55%
Percentage who rated GP care as excellent 57%

Floor and ceiling effects (examples)
% in lowest category % in highest category
PA: given choices about treatment to think about
25% 20%
DS: given a written list of thinkgs I should do to improve my health
39% 24%
GS Encouraged to go to a specific group or class to help me copy with my chronic illness
76% 10%
FU: Encouraged to attend programmes in the community that could help me
78% 10%

PACIC domains metrics
Overall PA DS GS PS FU
Nr items 20 3 3 5 4 5
Mean 2.9 3.2 3.5 2.5 3.3 3.1
Missing 31% 21% 20% 25% 28% 25%
Alpha 0.93 0.85 0.75 0.81 0.87 0.71
ICC 0.91 0.85 0.66 0.76 0.86 0.66
Europep effect + + + + + +
PEI effect - NS - - - -

Diabetes versus COPD patients
• Diabetes patients scored higher than COPD patients on 14 of the 20 PACIC items
• This might be explained by better structured chronic care for diabetes patients, or by patient characteristics

Conclusions
• A translated and validated Dutch version of PACIC is available
• Reasonably good measurement characteristics, but some problems:
- About 25% non responders
- Floor and ceiling effects
- Unexpected assocation with PEI

Chronic care and physician workload
Secondary analysis of EPA data from 140 practices in 10 countries
Wensing
Van den Hombergh
Van Doremalen
Grol
Szescenyi

Chronic care and physician workload in European primary care
• Secondary analysis of data from the EPA project

Background
• Delivery of chronic care is an important task of primary care
• Primary care practices are relatively small
• A higher volume of chronic patients may be associated with better performance and higher efficiency
• Many factors could influence such associations: international research needed

Methods
• Data from 140 practices in 10 countries (convenience samples)
• Physician workload = working hours per 1000 yearly attending patients
• Post-hoc measures based on EPA to measure aspects of the chronic care model
• Practice size: number of yearly attending patients
• Non-physician staff: total units of full time equivalance staff in the practice
• Mixed linear regression analysis models
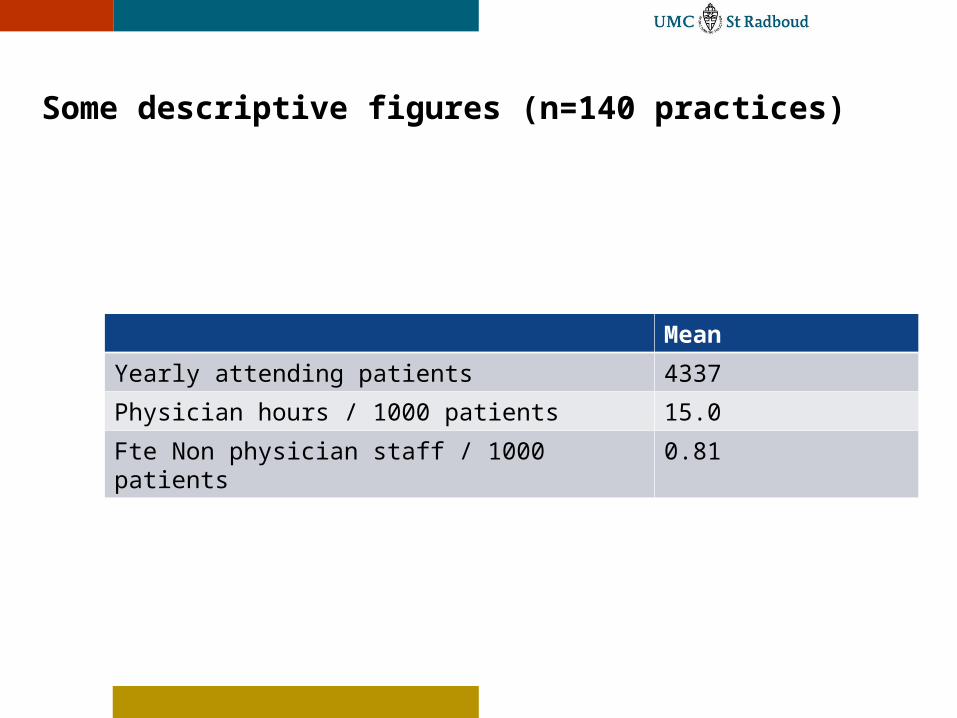
Some descriptive figures (n=140 practices)
Mean
Yearly attending patients 4337
Physician hours / 1000 patients 15.0
Fte Non physician staff / 1000 patients 0.81

Structured chronic care (n=140 practices)
Theoretical range
Mean
Presence of staff in team meetings 0 – 6 1.5
Procedures for preventive services 0 – 5 3.0
Use of disease classification 0 – 6 3.0
Use of email and internet 0 - 3 2.2
Computerized medical records 0 – 3 2.9
Use of advanced sotfware 0 – 3 2.4
Access to sources of evidence 0 – 4 2.3
Use of patiëet education materials 0 - 4 2.8

Main findings
• Practice size was the single most important predictor of physician workload per 1000 patients: each additional 1000 patients was associated with 1.29 fewer working hours per week per 1000 patients
• More non-physician staff was associated with higher physician workload: each additional 0.1 fte led to an additional 1.6 physician hours per week per 1000 patients

Conclusions
• Practice size, not chronic care delivery, was the most important determinant of physician worklload
• Warning: observational research
• Physician workload per 1000 patients is a proxy measure for physician efficiency; larger practices are more efficient
• Involving more nurses in primary does not imply reduced physician workload, and may in fact imply higher workload

www.topaseurope.eu

Discussion
• Further research and development
• Implementation in policy and practice





























