Embed Size (px)
Citation preview
Frank CobelensEuropean Advanced Course in Clinical TBRotterdam11-13 November 2019
C A N W E P R E D I C T T U B E RC U LOS I S C U R E?
C U R RE NT TO O L S AVA I L A BL E
www.aighd.org
Conflict of interest
I have the following, real or perceived direct or indirect conflicts of interest that relate to this presentation:
I have been awarded a grant by EDCTP (RIA-2018D-2509) for evaluating prediction tests for TB.
www.aighd.org
Content
Treatment monitoring
Establishing cure
Predicting cure
Individualized treatment
www.aighd.org
Establishing cure
WHY?
To establish that a patient has been cured of TB disease
→ no residual disease/pathology
→ no relapse expected
Idenify patients who need:
→ prolonged treatment
→ posttreatment vaccination
WHEN?
At end of treatment
→ ≈ 6 months post-initiation for first-line treatment
→ depending on cure definition for second-line treatment
www.aighd.org
Predicting cure
WHY?
To predict that a patient will (not) relapse after having completed treatment (relapse-free cure)
→ for the full treatment duration
→ for shortened treatment
Identify patients who:
→ need additional treatment (e.g. adjunct host-directed therapy)
→ can be cured with a shortened treatment regimen
WHEN
At treatment initiation or within the first 2 months of treatment
www.aighd.org
Establishing cure
www.aighd.org
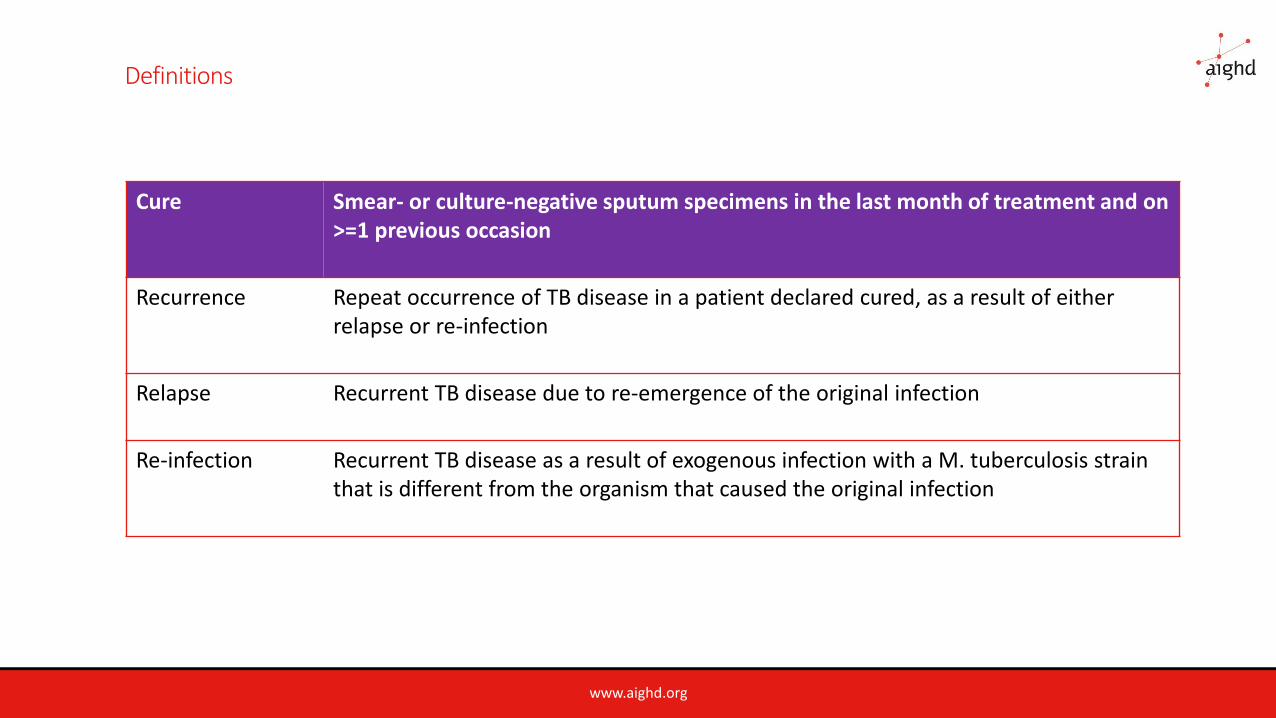
Definitions
Cure Smear- or culture-negative sputum specimens in the last month of treatment and on >=1 previous occasion
Recurrence Repeat occurrence of TB disease in a patient declared cured, as a result of eitherrelapse or re-infection
Relapse Recurrent TB disease due to re-emergence of the original infection
Re-infection Recurrent TB disease as a result of exogenous infection with a M. tuberculosis strainthat is different from the organism that caused the original infection
www.aighd.org
Methods for establishing cure
Sputum culture – limitations (turnaround times, logistics, false-negative rates, BSL requirements )
Sputum smear microscopy (non-viable bacilli) - improve by viability staining?
? Xpert MTB/RIF, Xpert Ultra
Bacterial rRNA (MBLA)
www.aighd.org
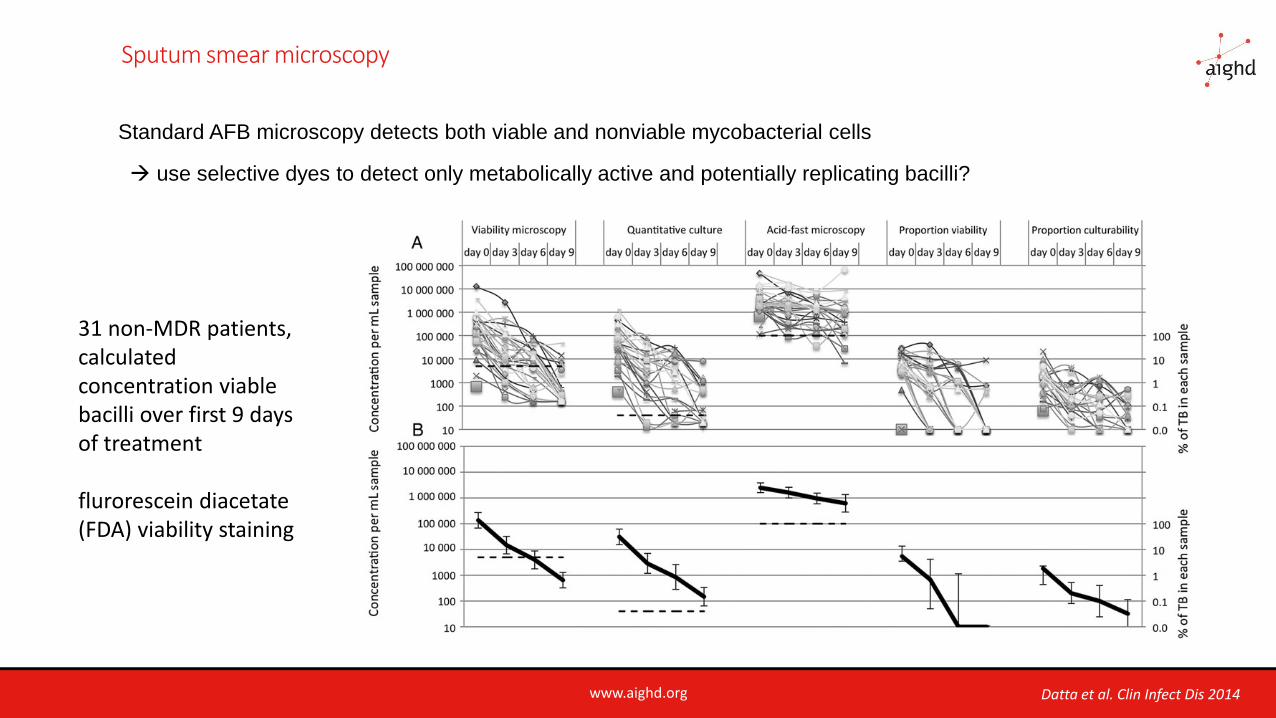
Sputum smear microscopy
Standard AFB microscopy detects both viable and nonviable mycobacterial cells
→ use selective dyes to detect only metabolically active and potentially replicating bacilli?
31 non-MDR patients, calculated concentration viable bacilli over first 9 days of treatment
flurorescein diacetate (FDA) viability staining
Datta et al. Clin Infect Dis 2014
www.aighd.org
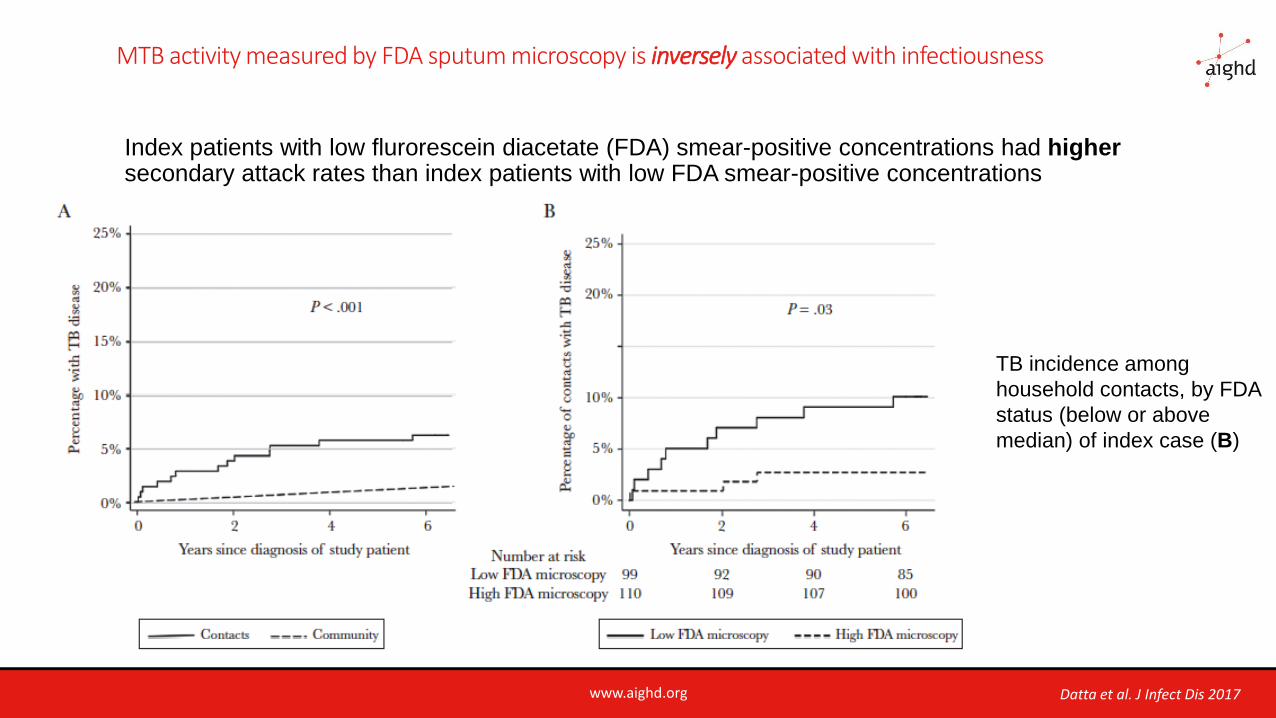
MTB activity measured by FDA sputum microscopy is inversely associated with infectiousness
Index patients with low flurorescein diacetate (FDA) smear-positive concentrations had highersecondary attack rates than index patients with low FDA smear-positive concentrations
TB incidence among
household contacts, by FDA
status (below or above
median) of index case (B)
Datta et al. J Infect Dis 2017
www.aighd.org
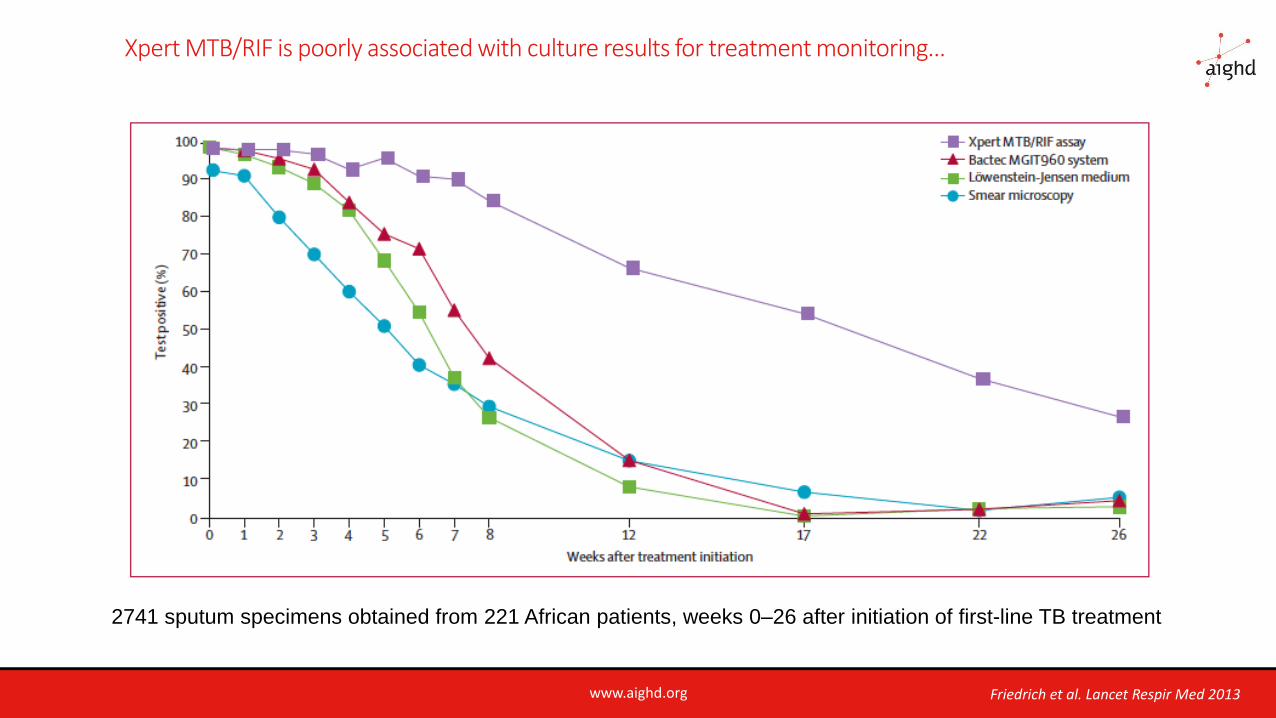
Xpert MTB/RIF is poorly associated with culture results for treatment monitoring…
Friedrich et al. Lancet Respir Med 2013
2741 sputum specimens obtained from 221 African patients, weeks 0–26 after initiation of first-line TB treatment
www.aighd.org
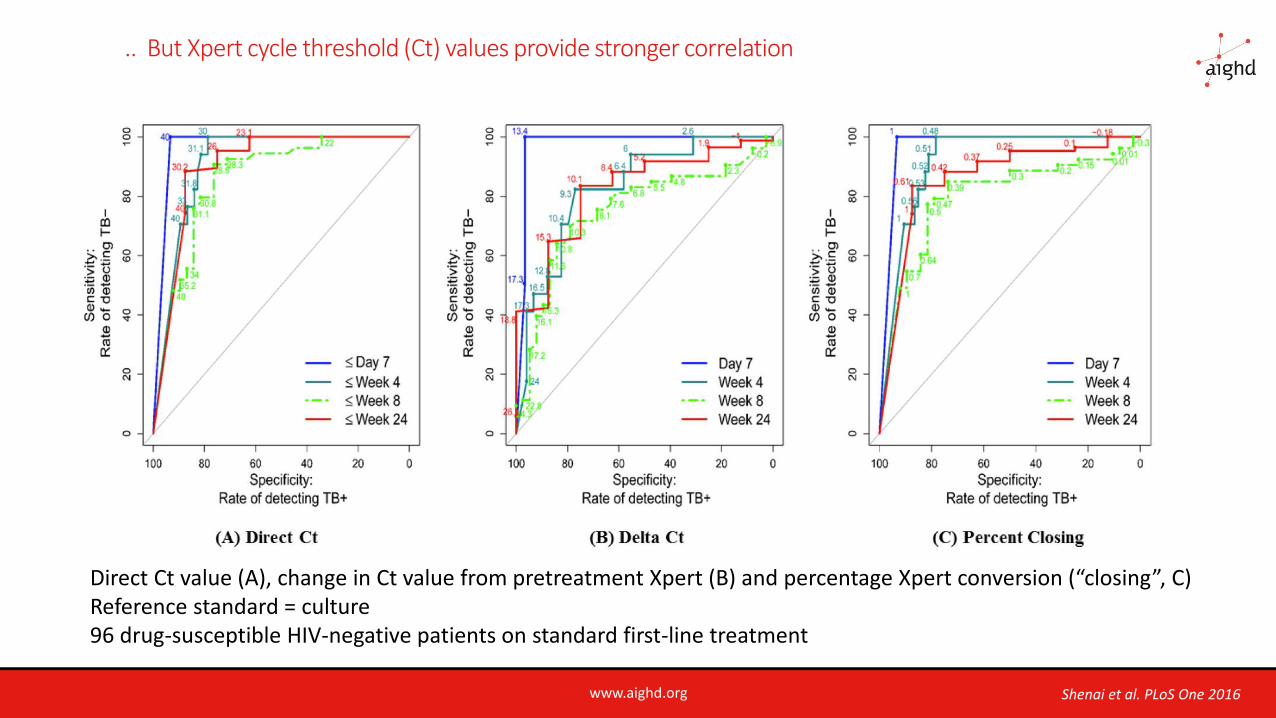
.. But Xpert cycle threshold (Ct) values provide stronger correlation
Shenai et al. PLoS One 2016
Direct Ct value (A), change in Ct value from pretreatment Xpert (B) and percentage Xpert conversion (“closing”, C)Reference standard = culture 96 drug-susceptible HIV-negative patients on standard first-line treatment
www.aighd.org
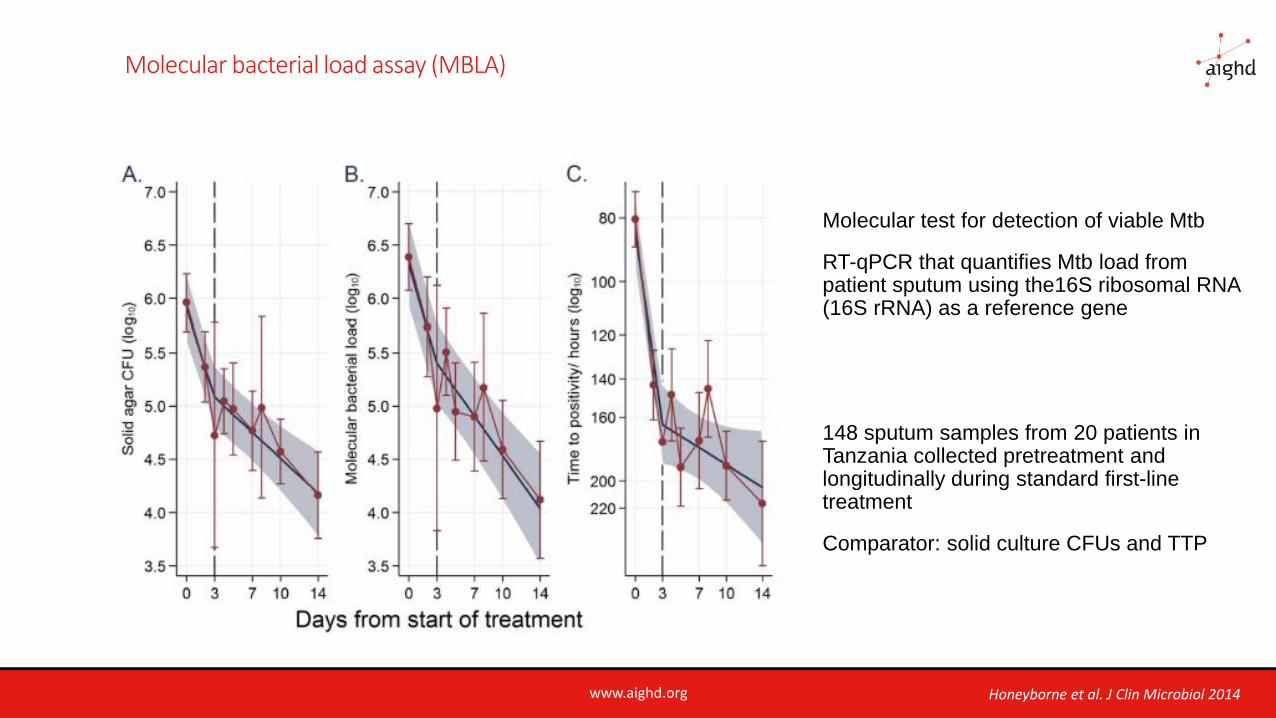
Molecular bacterial load assay (MBLA)
Molecular test for detection of viable Mtb
RT-qPCR that quantifies Mtb load frompatient sputum using the16S ribosomal RNA (16S rRNA) as a reference gene
148 sputum samples from 20 patients in Tanzania collected pretreatment andlongitudinally during standard first-line treatment
Comparator: solid culture CFUs and TTP
Honeyborne et al. J Clin Microbiol 2014
www.aighd.org
Issues with current definition of cure
1. Does it adequately reflect that there is no residual disease/pathology?
2. Is it relevant with regard to relapse – i.e. does it reflect relapse-free cure?
Are 1 and 2 different?
More specifically:
Does 2 imply that the test must exclude the presence of residual persistent/latent infection?
Or is relapse “flare up” of residual active disease?
www.aighd.org
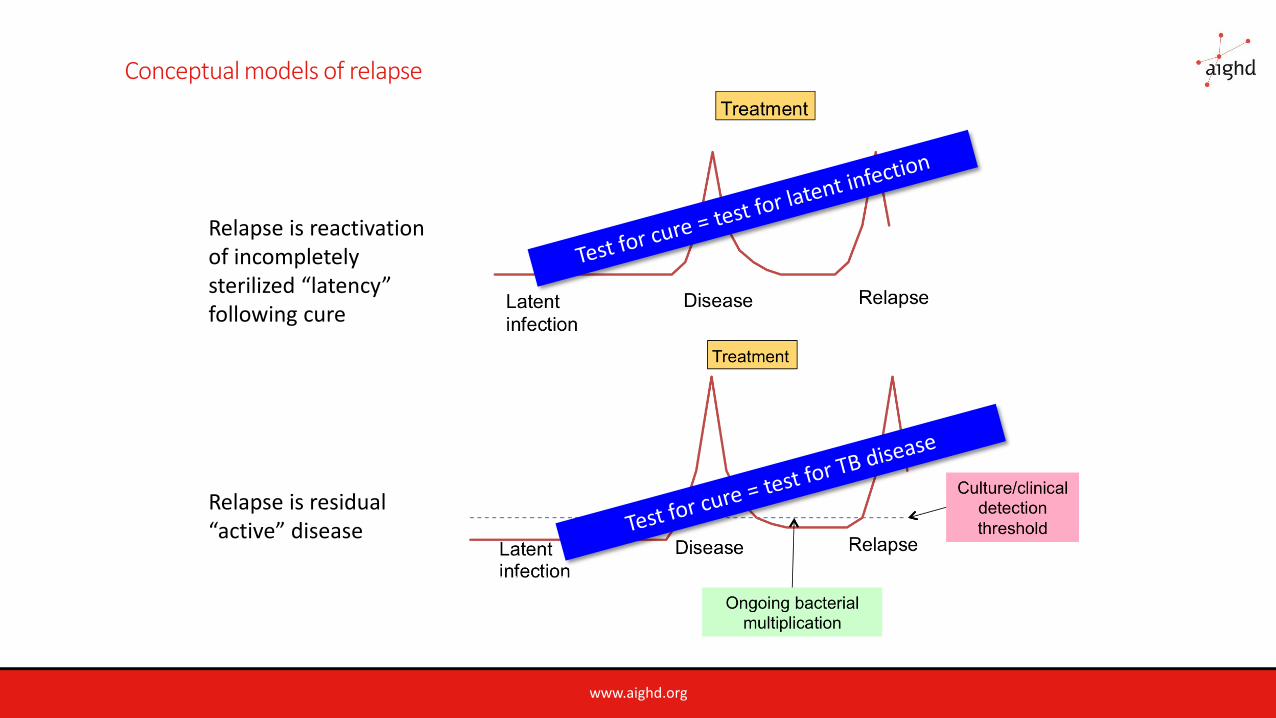
Conceptual models of relapse
15
Relapse is reactivation of incompletely sterilized “latency” following cure
Relapse is residual “active” disease
www.aighd.org
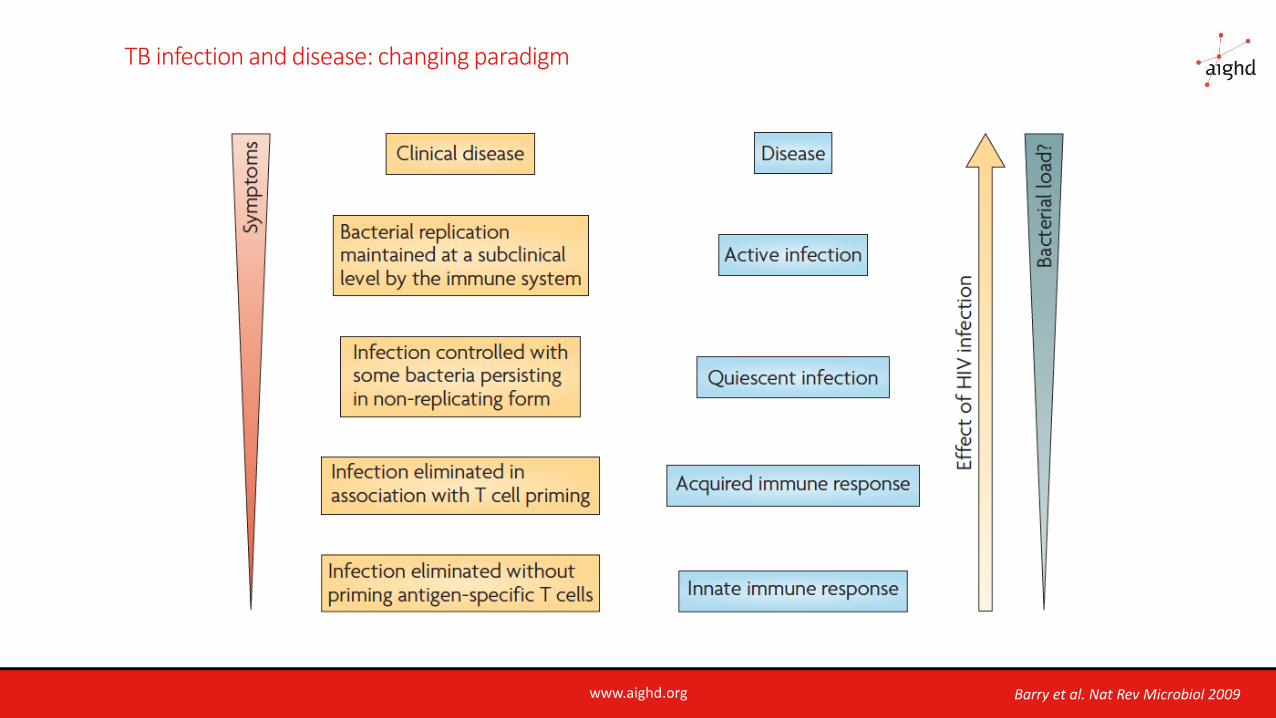
TB infection and disease: changing paradigm
Barry et al. Nat Rev Microbiol 2009
www.aighd.org
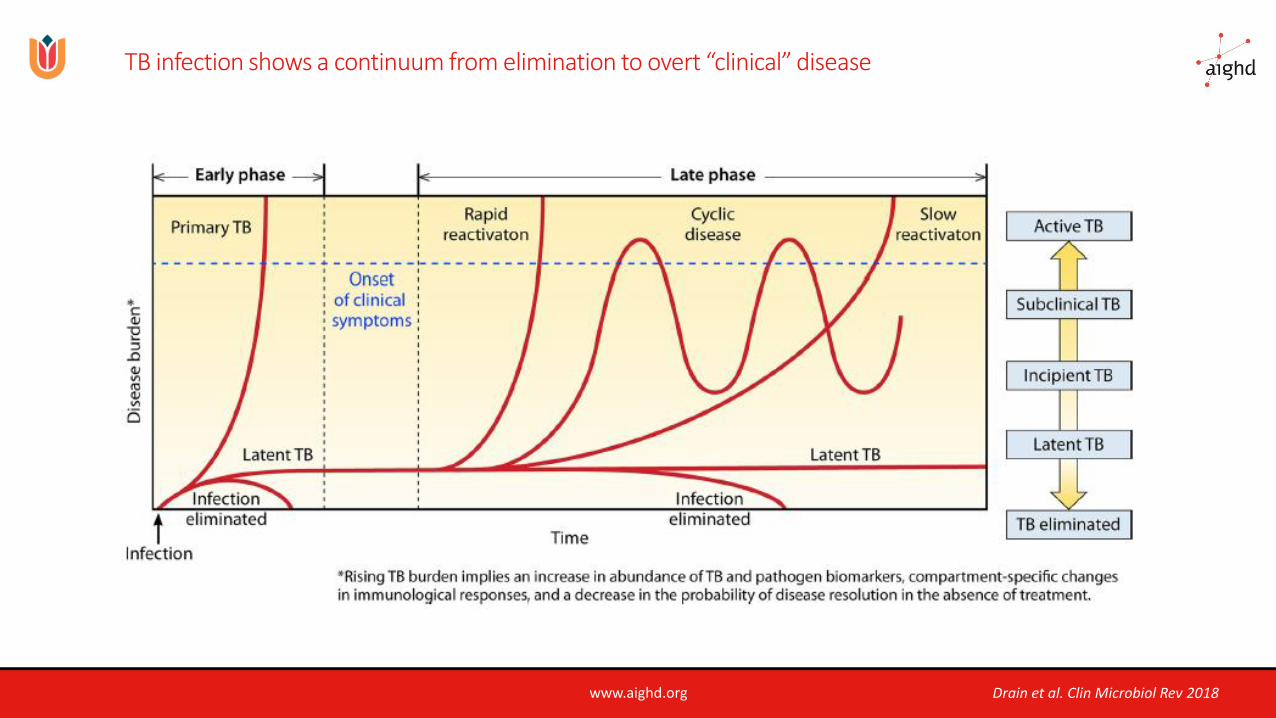
TB infection shows a continuum from elimination to overt “clinical” disease
Drain et al. Clin Microbiol Rev 2018
www.aighd.org
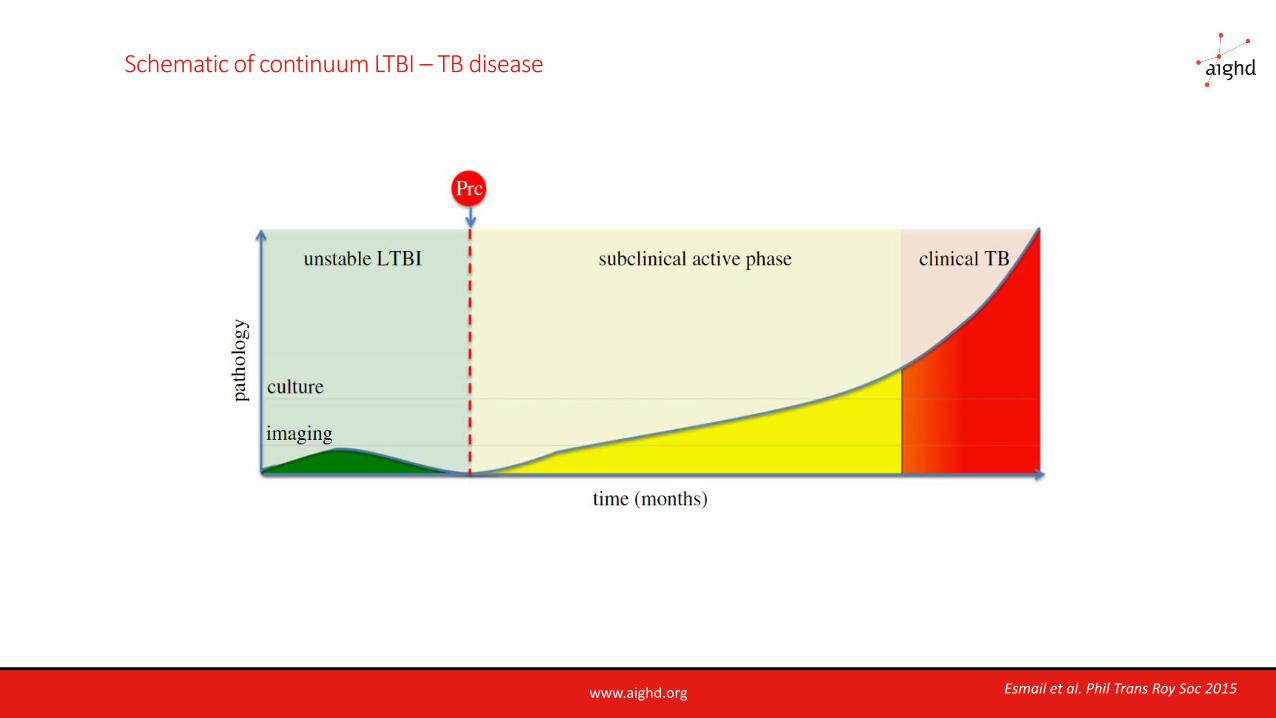
Schematic of continuum LTBI – TB disease
Esmail et al. Phil Trans Roy Soc 2015
www.aighd.org
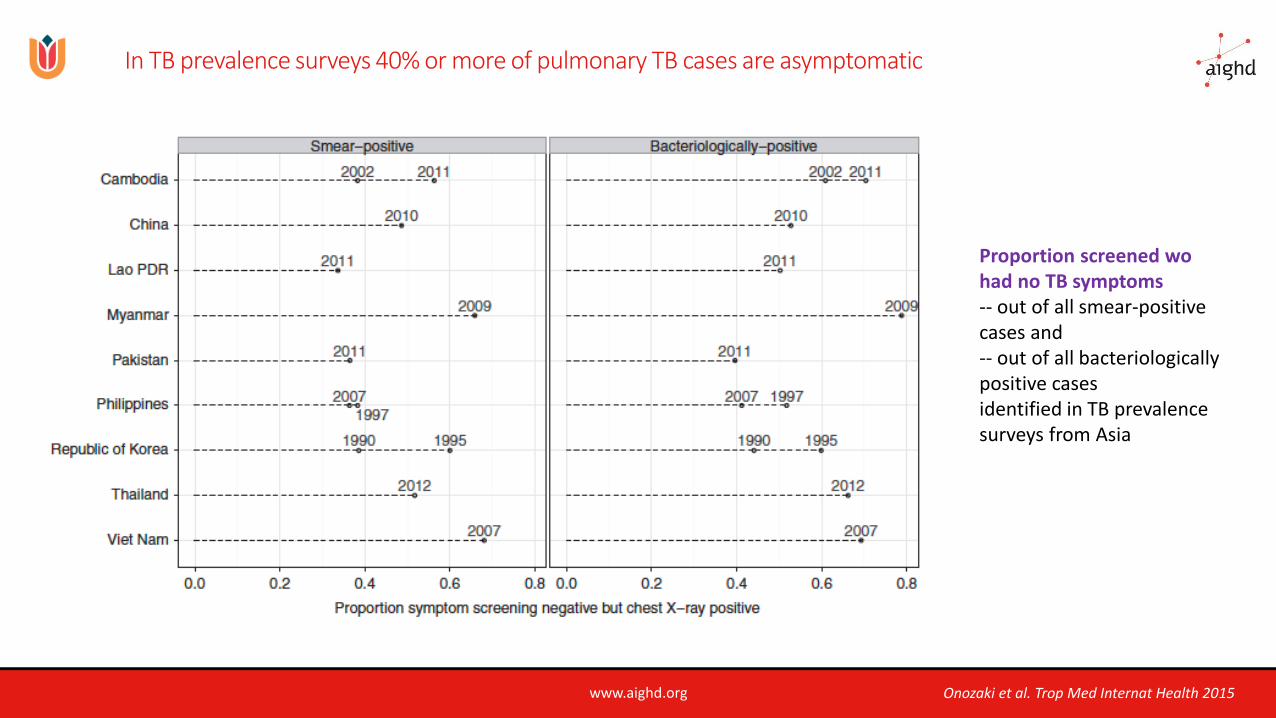
In TB prevalence surveys 40% or more of pulmonary TB cases are asymptomatic
Proportion screened wo had no TB symptoms -- out of all smear-positive cases and -- out of all bacteriologically positive cases identified in TB prevalence surveys from Asia
Onozaki et al. Trop Med Internat Health 2015
www.aighd.org
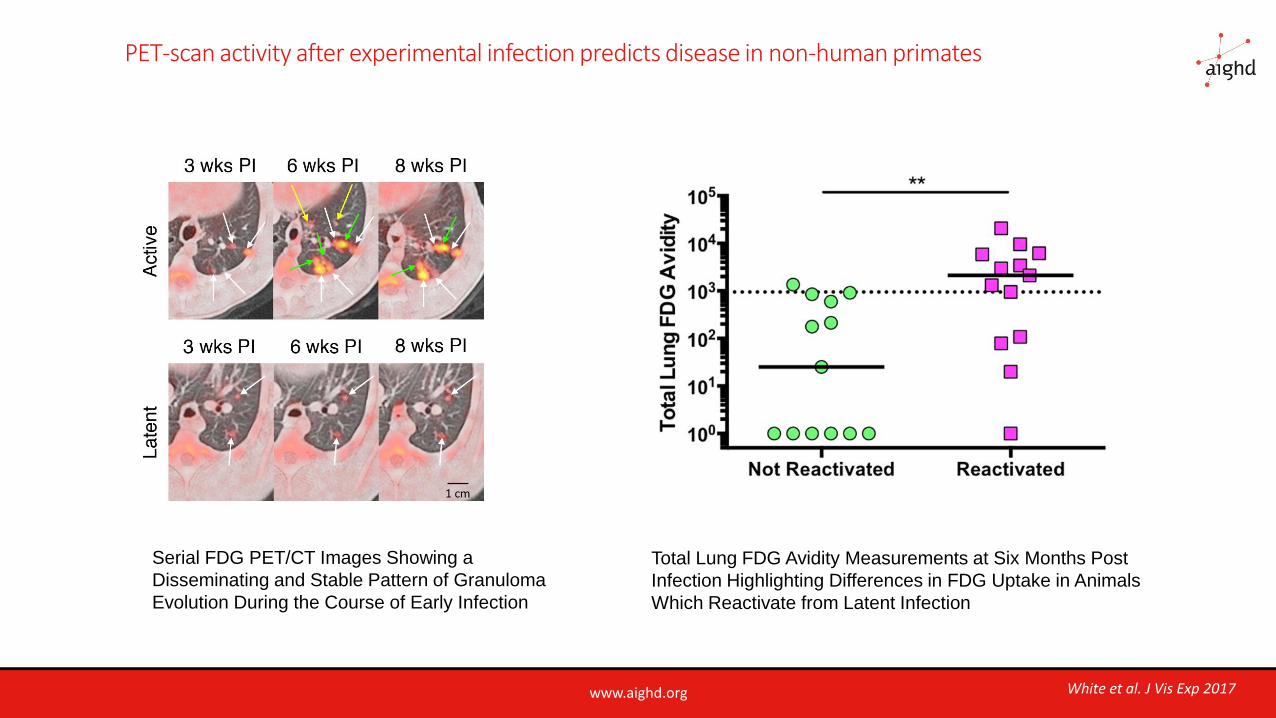
PET-scan activity after experimental infection predicts disease in non-human primates
Total Lung FDG Avidity Measurements at Six Months Post
Infection Highlighting Differences in FDG Uptake in Animals
Which Reactivate from Latent Infection
Serial FDG PET/CT Images Showing a
Disseminating and Stable Pattern of Granuloma
Evolution During the Course of Early Infection
White et al. J Vis Exp 2017
www.aighd.org
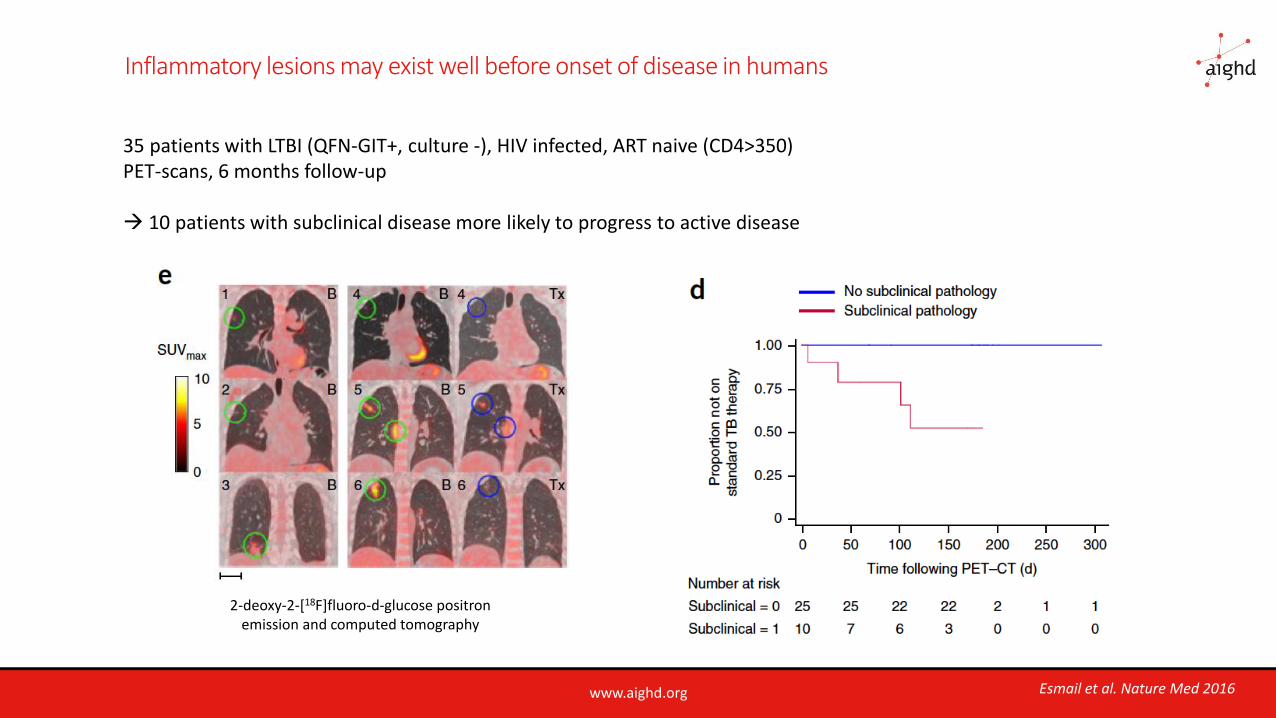
Inflammatory lesions may exist well before onset of disease in humans
35 patients with LTBI (QFN-GIT+, culture -), HIV infected, ART naive (CD4>350)PET-scans, 6 months follow-up
→ 10 patients with subclinical disease more likely to progress to active disease
2-deoxy-2-[18F]fluoro-d-glucose positron emission and computed tomography
Esmail et al. Nature Med 2016
www.aighd.org
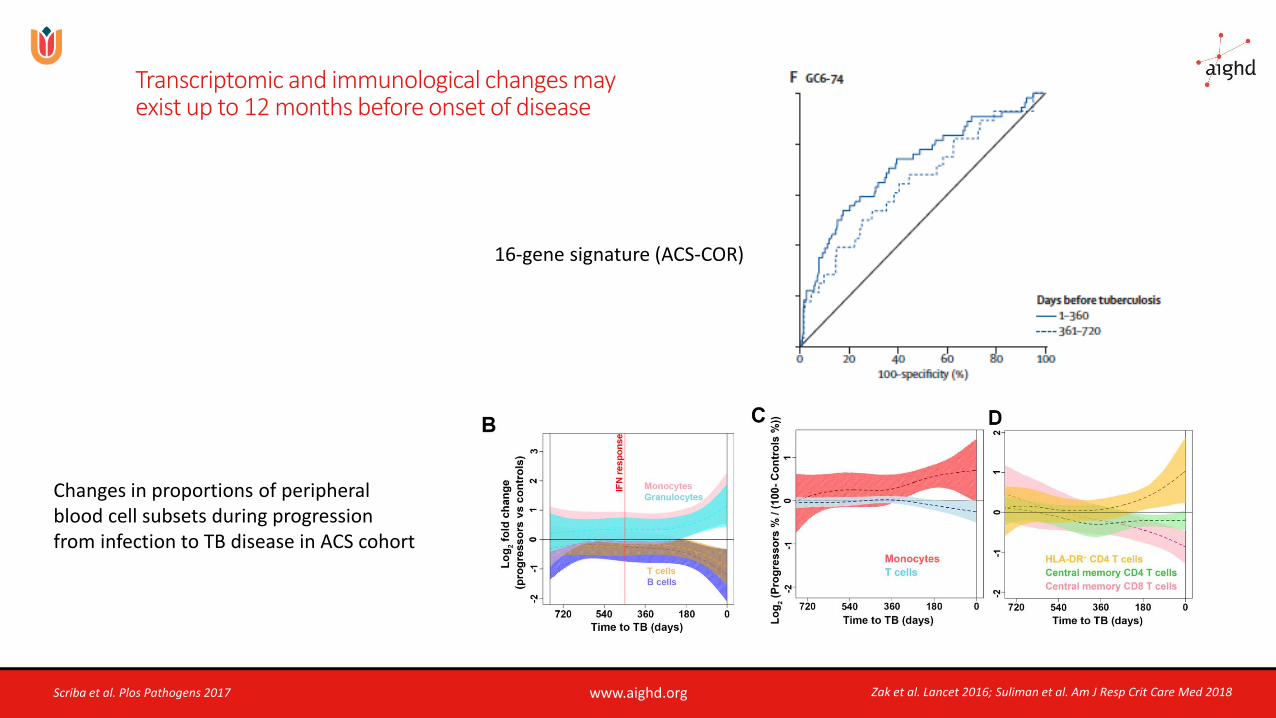
Transcriptomic and immunological changes mayexist up to 12 months before onset of disease
16-gene signature (ACS-COR)
Zak et al. Lancet 2016; Suliman et al. Am J Resp Crit Care Med 2018Scriba et al. Plos Pathogens 2017
Changes in proportions of peripheralblood cell subsets during progressionfrom infection to TB disease in ACS cohort
www.aighd.org
So…
❑ Overt clinical TB disease may be preceded by a prolonged subclinical period of “incipient” TB in which there
are no/few symptoms and sputum cultures may be positive
❑ This subclinical phase may last several months
❑ Progression of subclinical to clinical disease may be halted spontaneously
Would this also apply to relapse?
www.aighd.org
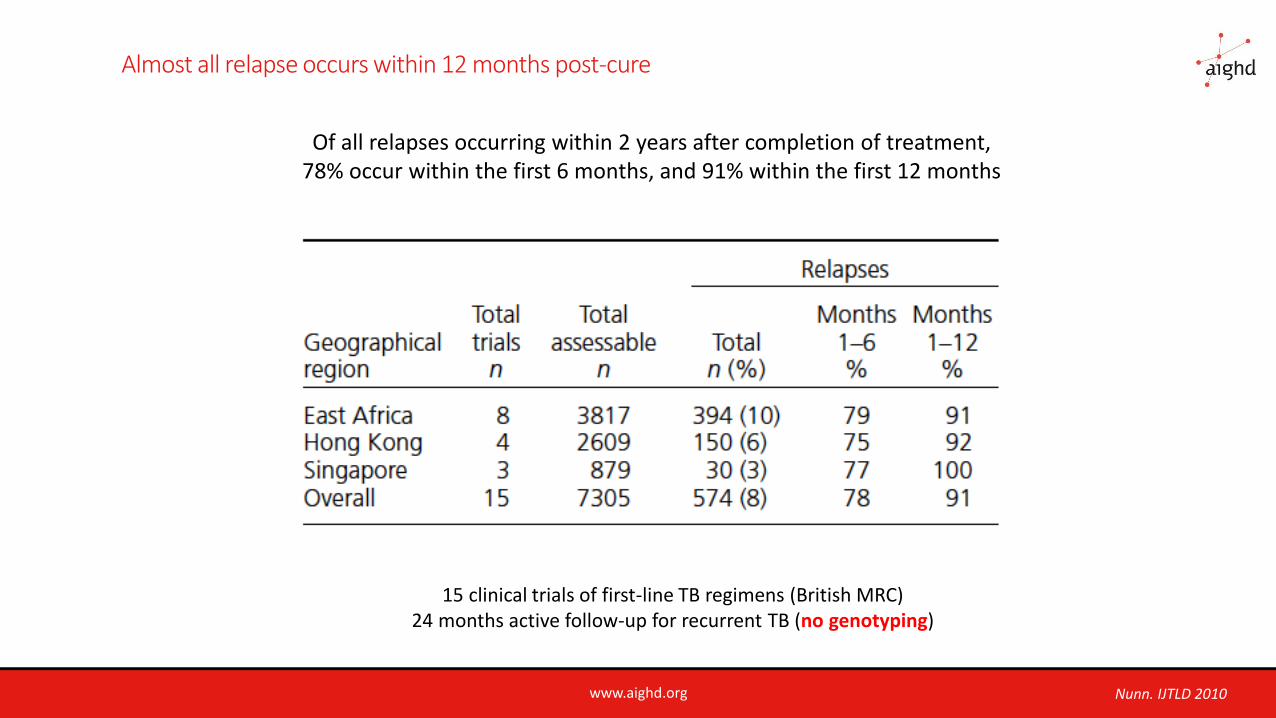
Almost all relapse occurs within 12 months post-cure
Of all relapses occurring within 2 years after completion of treatment, 78% occur within the first 6 months, and 91% within the first 12 months
15 clinical trials of first-line TB regimens (British MRC)24 months active follow-up for recurrent TB (no genotyping)
Nunn. IJTLD 2010
www.aighd.org
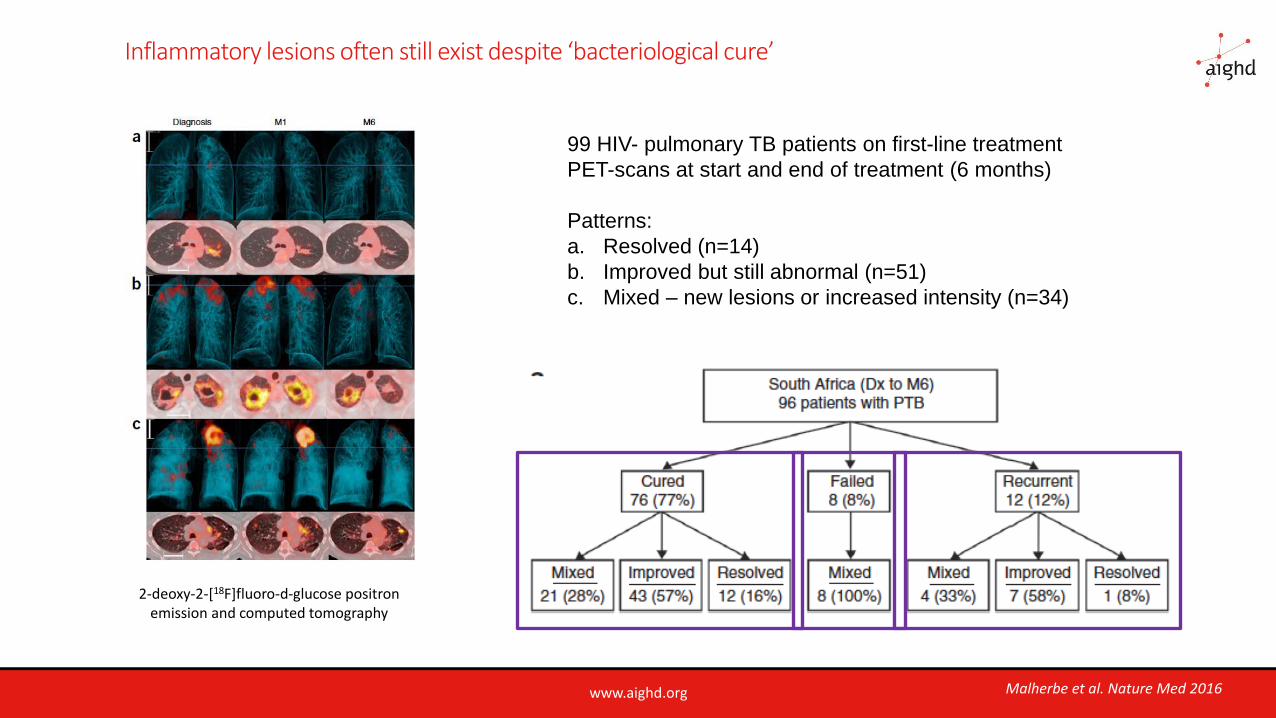
Inflammatory lesions often still exist despite ‘bacteriological cure’
99 HIV- pulmonary TB patients on first-line treatment
PET-scans at start and end of treatment (6 months)
Patterns:
a. Resolved (n=14)
b. Improved but still abnormal (n=51)
c. Mixed – new lesions or increased intensity (n=34)
2-deoxy-2-[18F]fluoro-d-glucose positron emission and computed tomography
Malherbe et al. Nature Med 2016
www.aighd.org
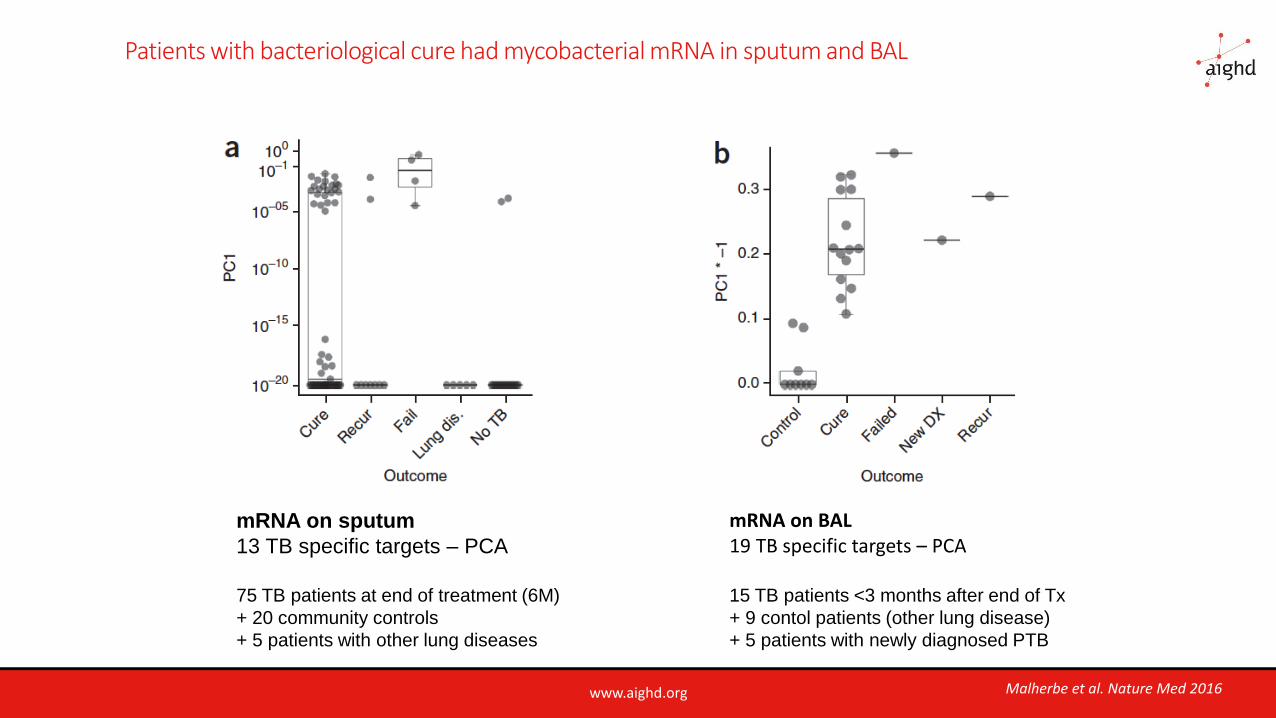
Patients with bacteriological cure had mycobacterial mRNA in sputum and BAL
mRNA on BAL 19 TB specific targets – PCA
15 TB patients <3 months after end of Tx
+ 9 contol patients (other lung disease)
+ 5 patients with newly diagnosed PTB
mRNA on sputum
13 TB specific targets – PCA
75 TB patients at end of treatment (6M)
+ 20 community controls
+ 5 patients with other lung diseases
Malherbe et al. Nature Med 2016
www.aighd.org
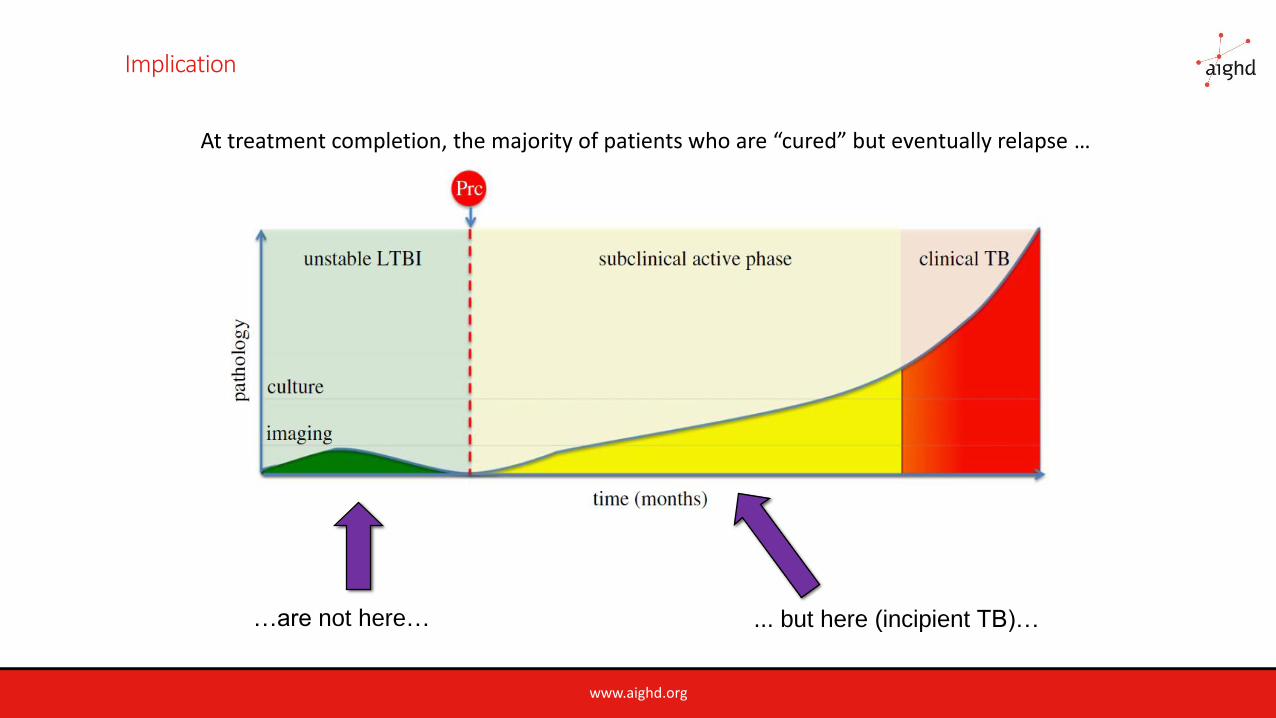
Implication
... but here (incipient TB)……are not here…
At treatment completion, the majority of patients who are “cured” but eventually relapse …
www.aighd.org
Predicting cure
www.aighd.org
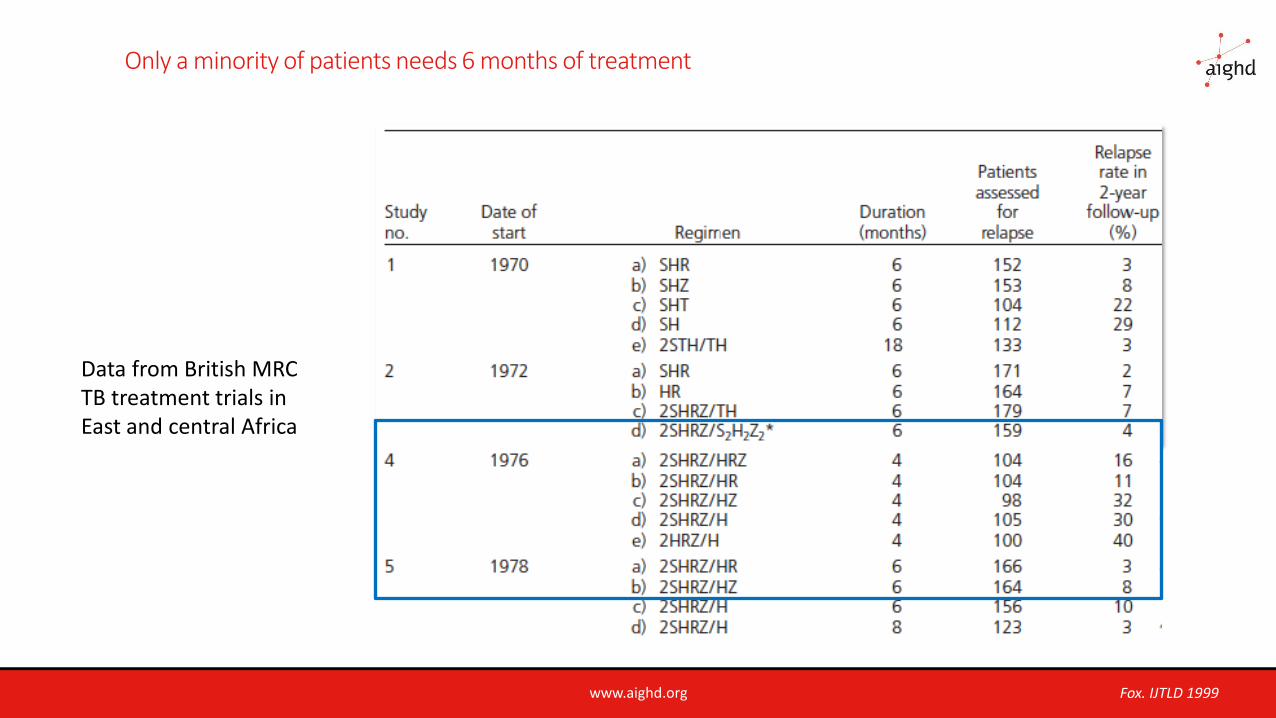
Only a minority of patients needs 6 months of treatment
Data from British MRC TB treatment trials in East and central Africa
Fox. IJTLD 1999
www.aighd.org
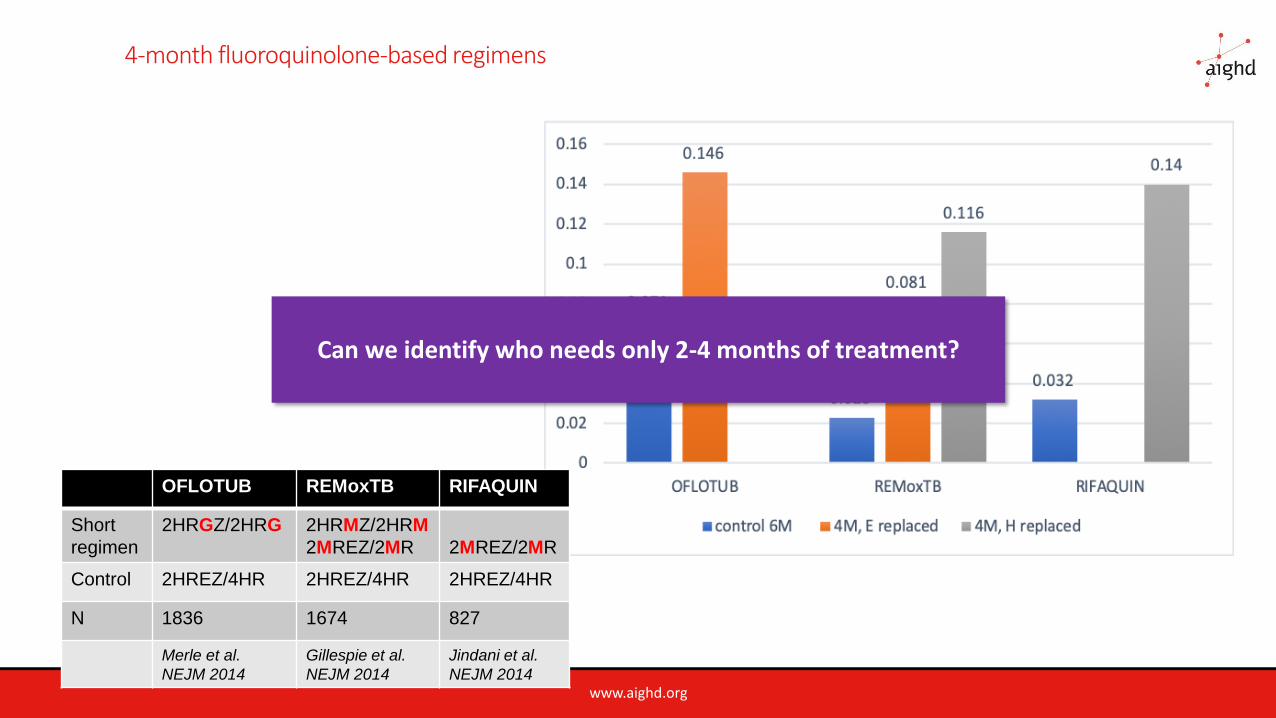
4-month fluoroquinolone-based regimens
OFLOTUB REMoxTB RIFAQUIN
Short
regimen
2HRGZ/2HRG 2HRMZ/2HRM
2MREZ/2MR 2MREZ/2MR
Control 2HREZ/4HR 2HREZ/4HR 2HREZ/4HR
N 1836 1674 827
Merle et al.
NEJM 2014
Gillespie et al.
NEJM 2014
Jindani et al.
NEJM 2014
Can we identify who needs only 2-4 months of treatment?
www.aighd.org
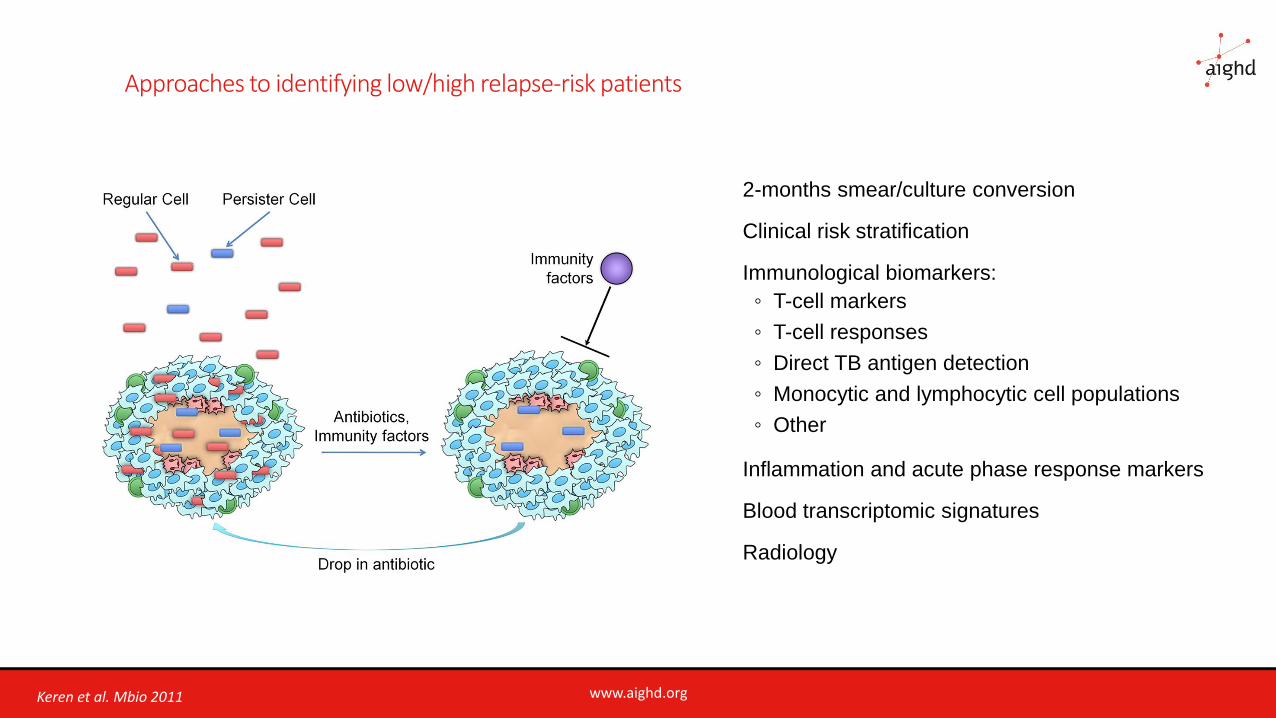
Approaches to identifying low/high relapse-risk patients
2-months smear/culture conversion
Clinical risk stratification
Immunological biomarkers:
◦ T-cell markers
◦ T-cell responses
◦ Direct TB antigen detection
◦ Monocytic and lymphocytic cell populations
◦ Other
Inflammation and acute phase response markers
Blood transcriptomic signatures
Radiology
Keren et al. Mbio 2011
www.aighd.org
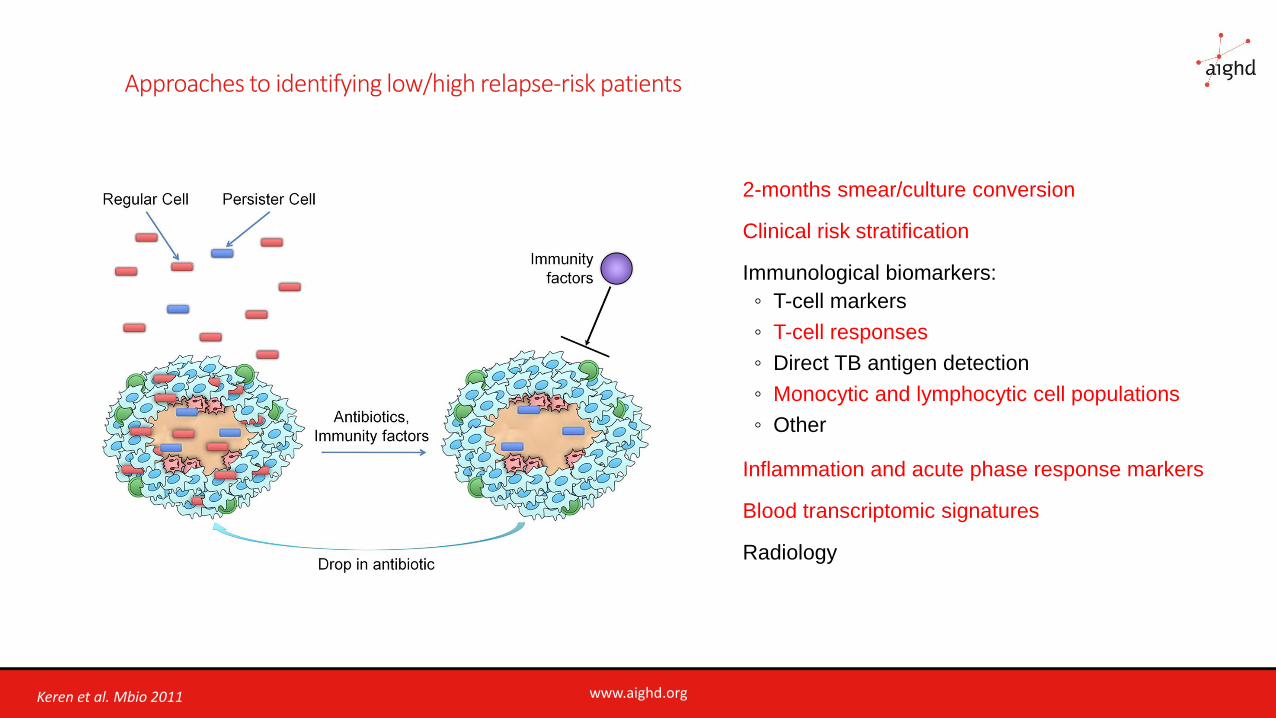
Approaches to identifying low/high relapse-risk patients
2-months smear/culture conversion
Clinical risk stratification
Immunological biomarkers:
◦ T-cell markers
◦ T-cell responses
◦ Direct TB antigen detection
◦ Monocytic and lymphocytic cell populations
◦ Other
Inflammation and acute phase response markers
Blood transcriptomic signatures
Radiology
Keren et al. Mbio 2011
www.aighd.org
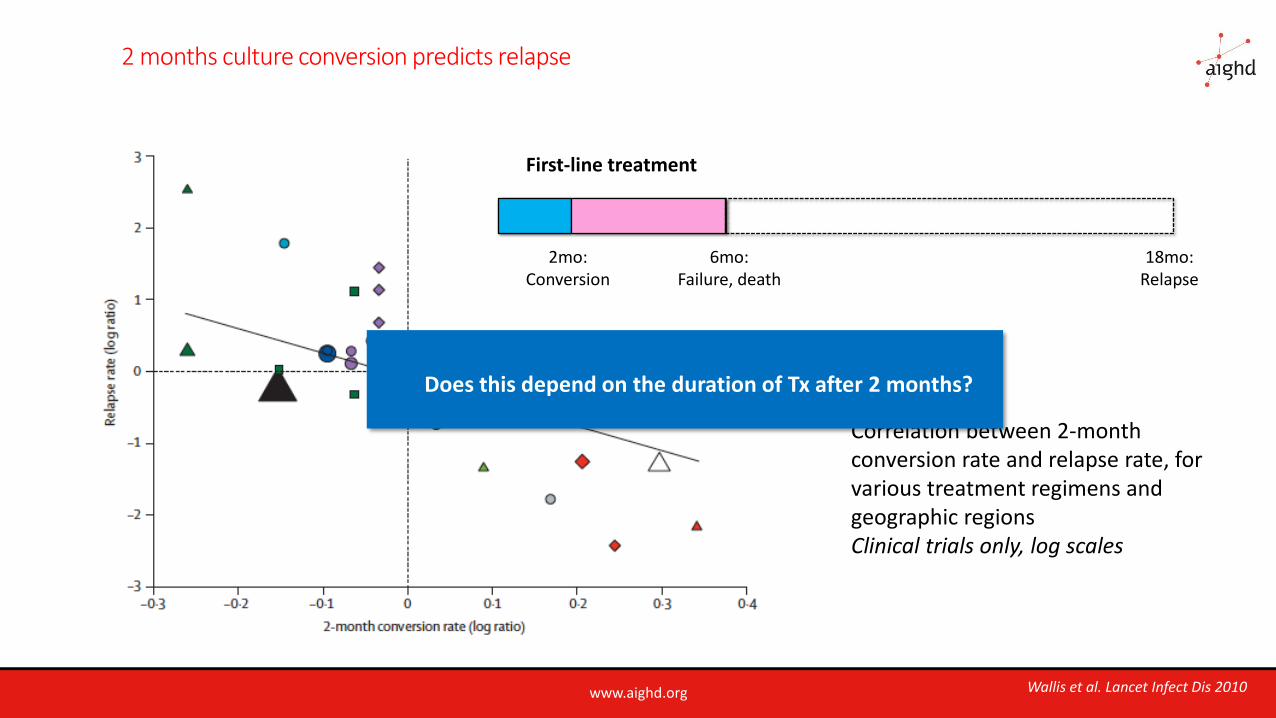
2 months culture conversion predicts relapse
2mo:Conversion
6mo:Failure, death
First-line treatment
18mo:Relapse
Correlation between 2-month conversion rate and relapse rate, forvarious treatment regimens and geographic regionsClinical trials only, log scales
Wallis et al. Lancet Infect Dis 2010
Does this depend on the duration of Tx after 2 months?
www.aighd.org
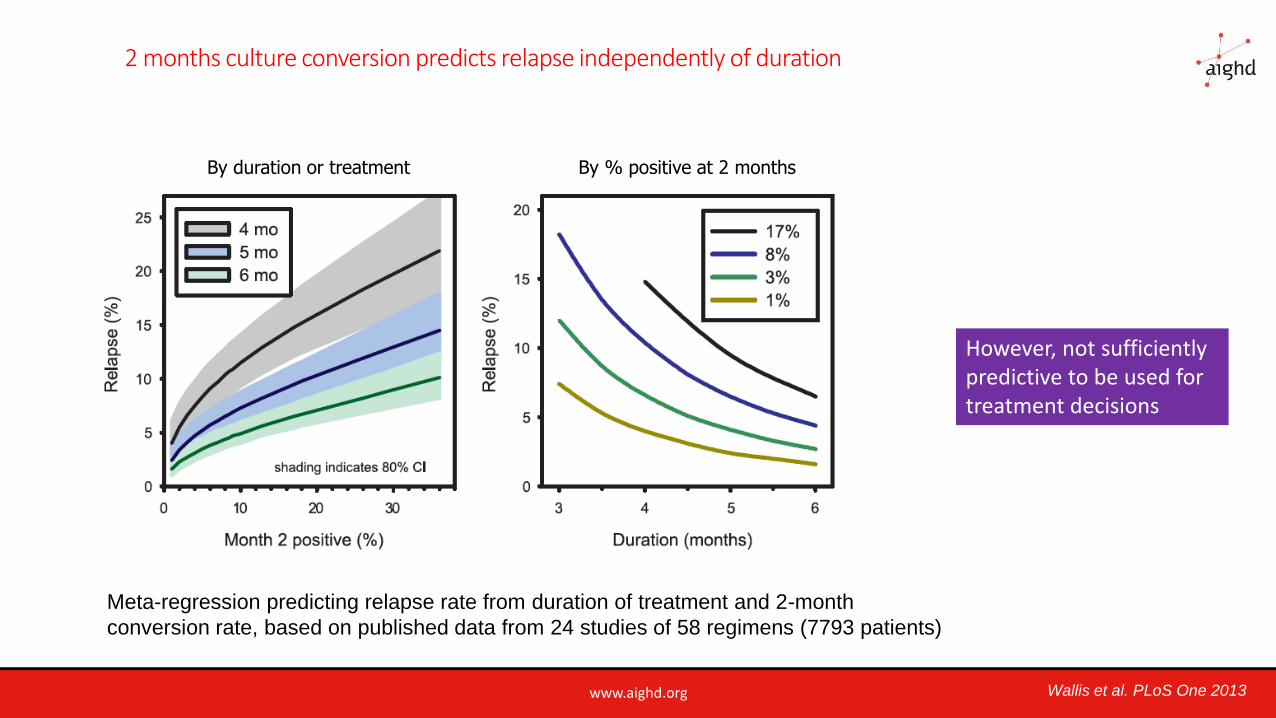
2 months culture conversion predicts relapse independently of duration
By duration or treatment By % positive at 2 months
Meta-regression predicting relapse rate from duration of treatment and 2-month
conversion rate, based on published data from 24 studies of 58 regimens (7793 patients)
Wallis et al. PLoS One 2013
However, not sufficiently predictive to be used for treatment decisions
www.aighd.org
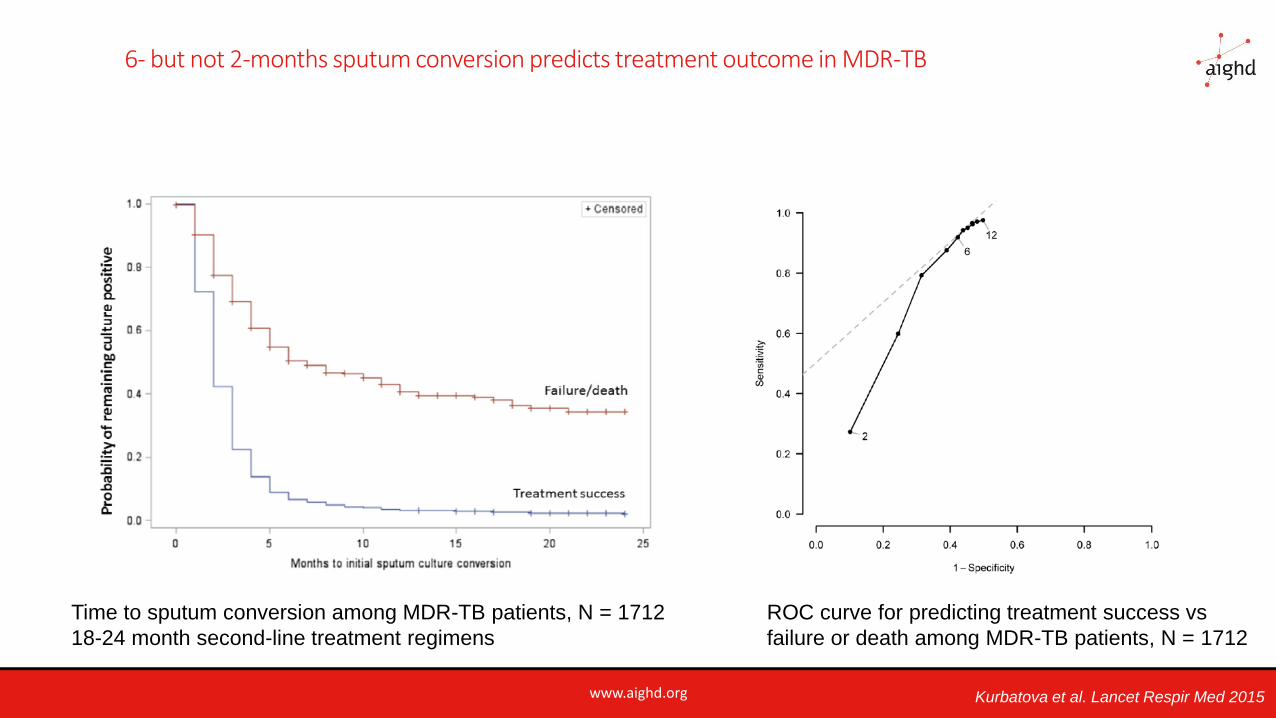
6- but not 2-months sputum conversion predicts treatment outcome in MDR-TB
Time to sputum conversion among MDR-TB patients, N = 1712
18-24 month second-line treatment regimens
ROC curve for predicting treatment success vs
failure or death among MDR-TB patients, N = 1712
Kurbatova et al. Lancet Respir Med 2015
www.aighd.org
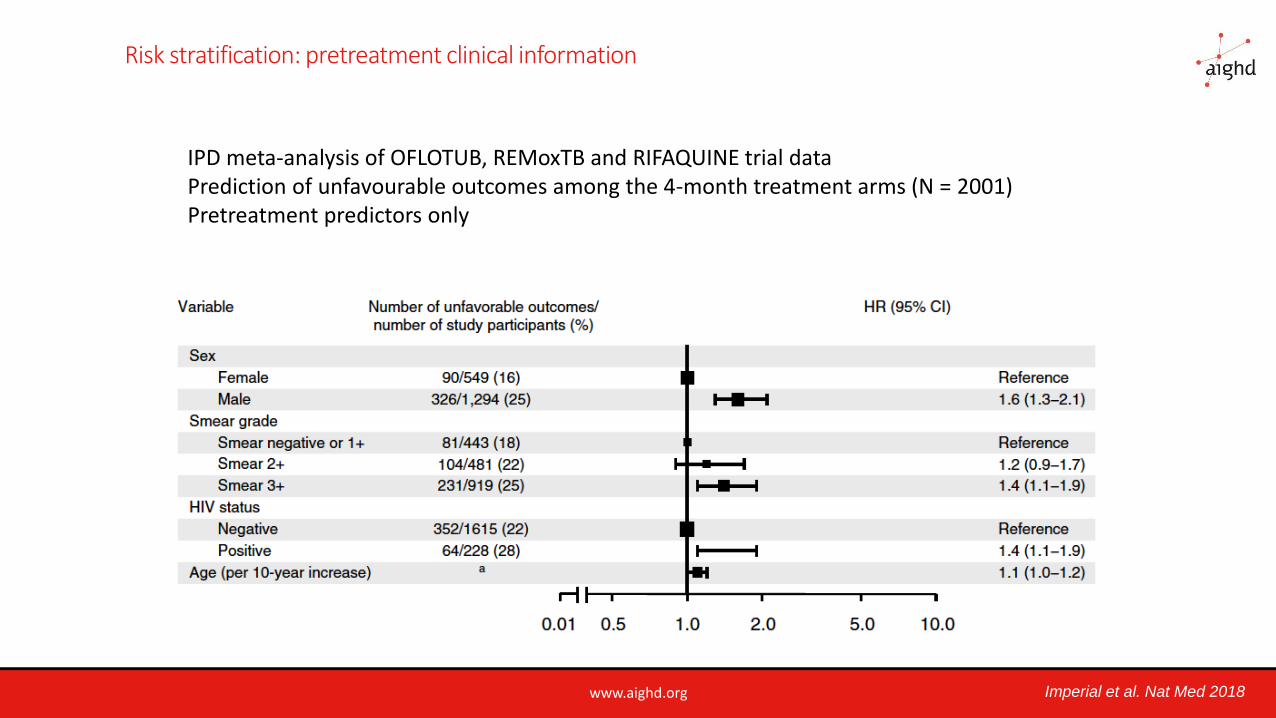
Risk stratification: pretreatment clinical information
IPD meta-analysis of OFLOTUB, REMoxTB and RIFAQUINE trial dataPrediction of unfavourable outcomes among the 4-month treatment arms (N = 2001) Pretreatment predictors only
Imperial et al. Nat Med 2018
www.aighd.org
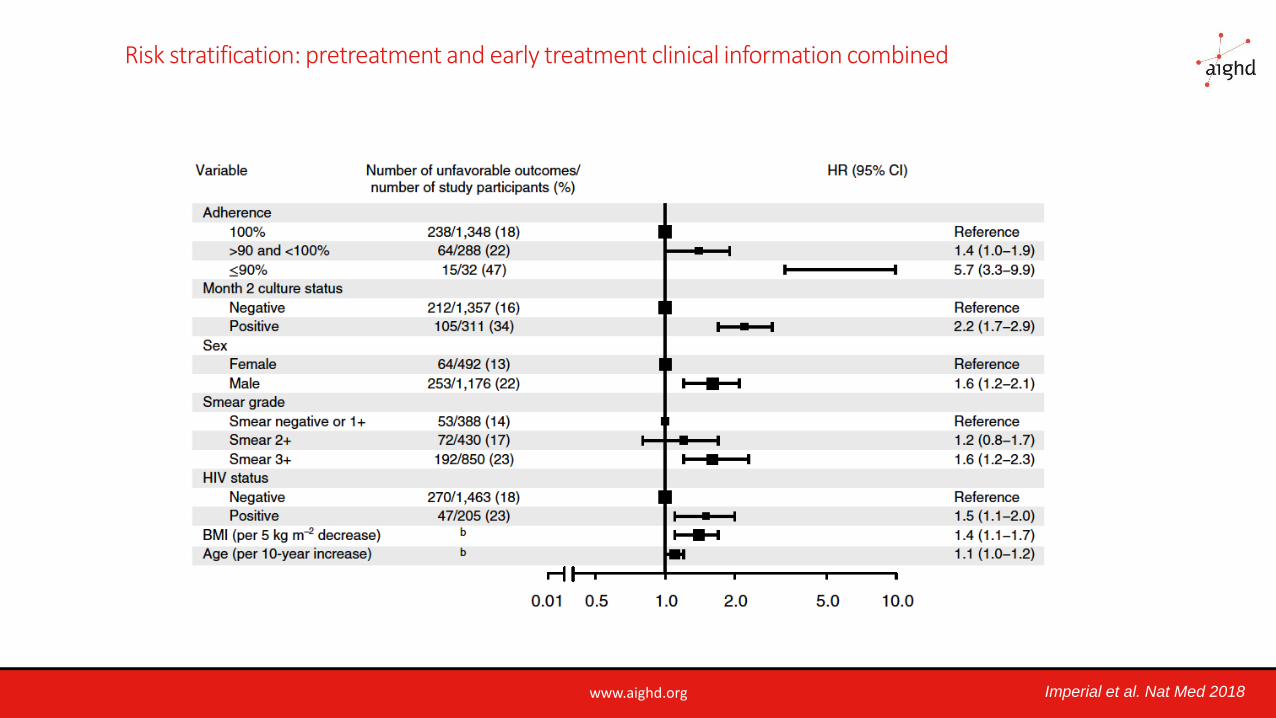
Risk stratification: pretreatment and early treatment clinical information combined
Imperial et al. Nat Med 2018
www.aighd.org
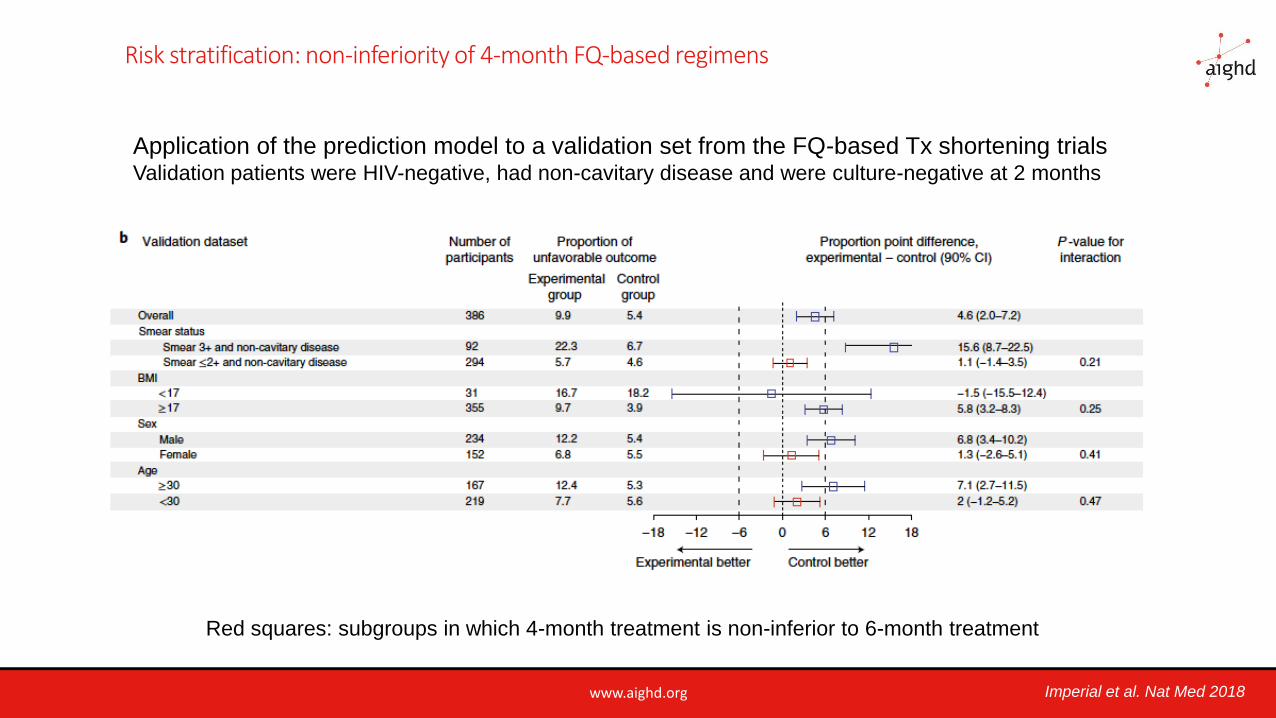
Risk stratification: non-inferiority of 4-month FQ-based regimens
Imperial et al. Nat Med 2018
Application of the prediction model to a validation set from the FQ-based Tx shortening trialsValidation patients were HIV-negative, had non-cavitary disease and were culture-negative at 2 months
Red squares: subgroups in which 4-month treatment is non-inferior to 6-month treatment
www.aighd.org
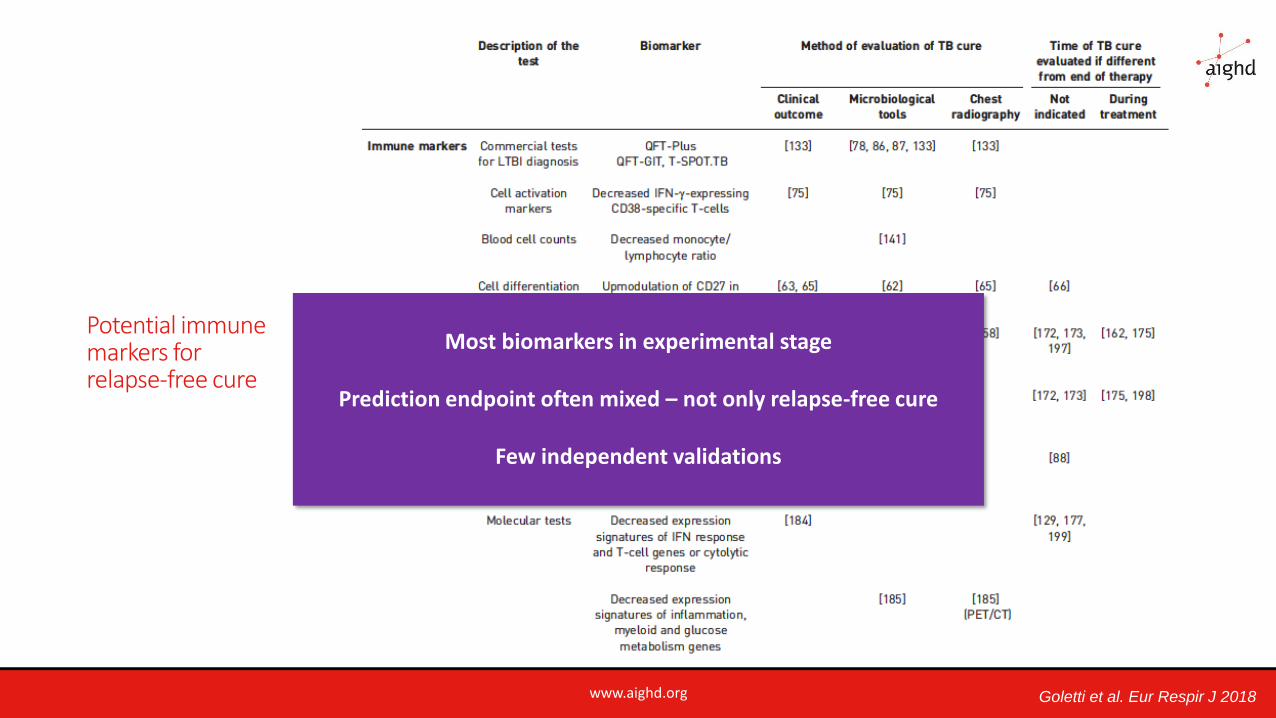
Potential immune markers for relapse-free cure
Goletti et al. Eur Respir J 2018
Most biomarkers in experimental stage
Prediction endpoint often mixed – not only relapse-free cure
Few independent validations
www.aighd.org
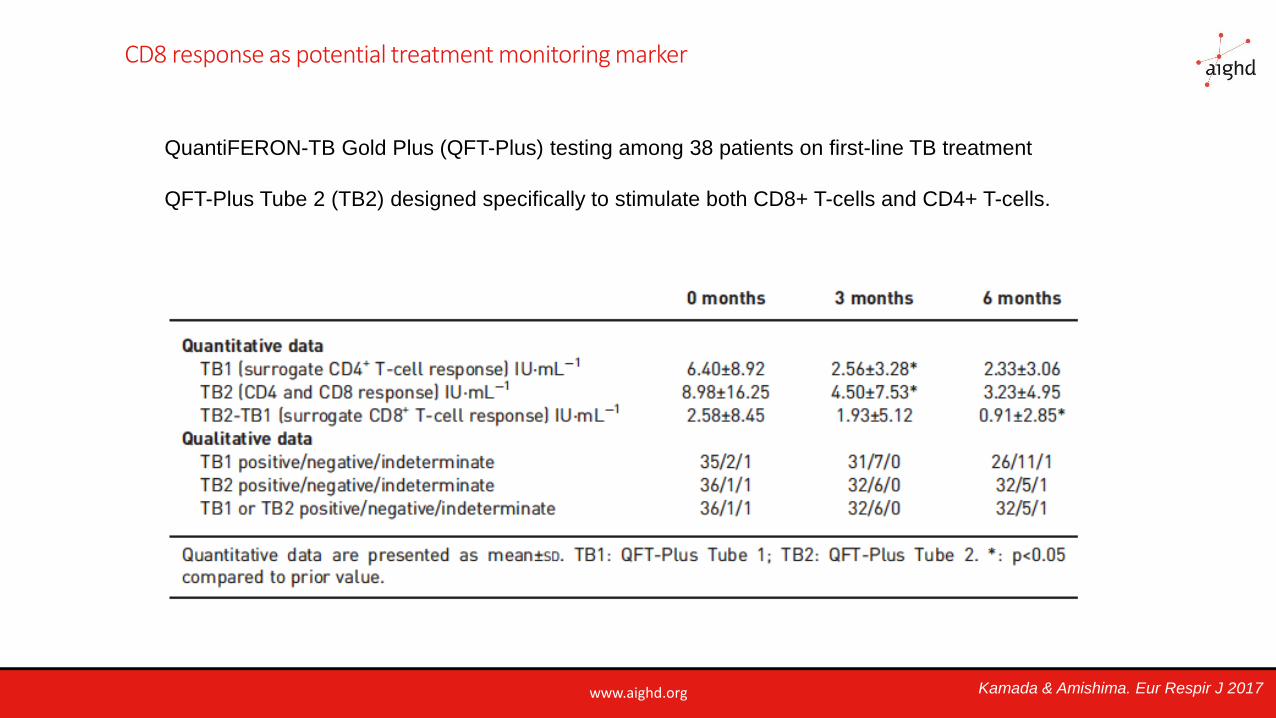
CD8 response as potential treatment monitoring marker
QuantiFERON-TB Gold Plus (QFT-Plus) testing among 38 patients on first-line TB treatment
QFT-Plus Tube 2 (TB2) designed specifically to stimulate both CD8+ T-cells and CD4+ T-cells.
Kamada & Amishima. Eur Respir J 2017
www.aighd.org
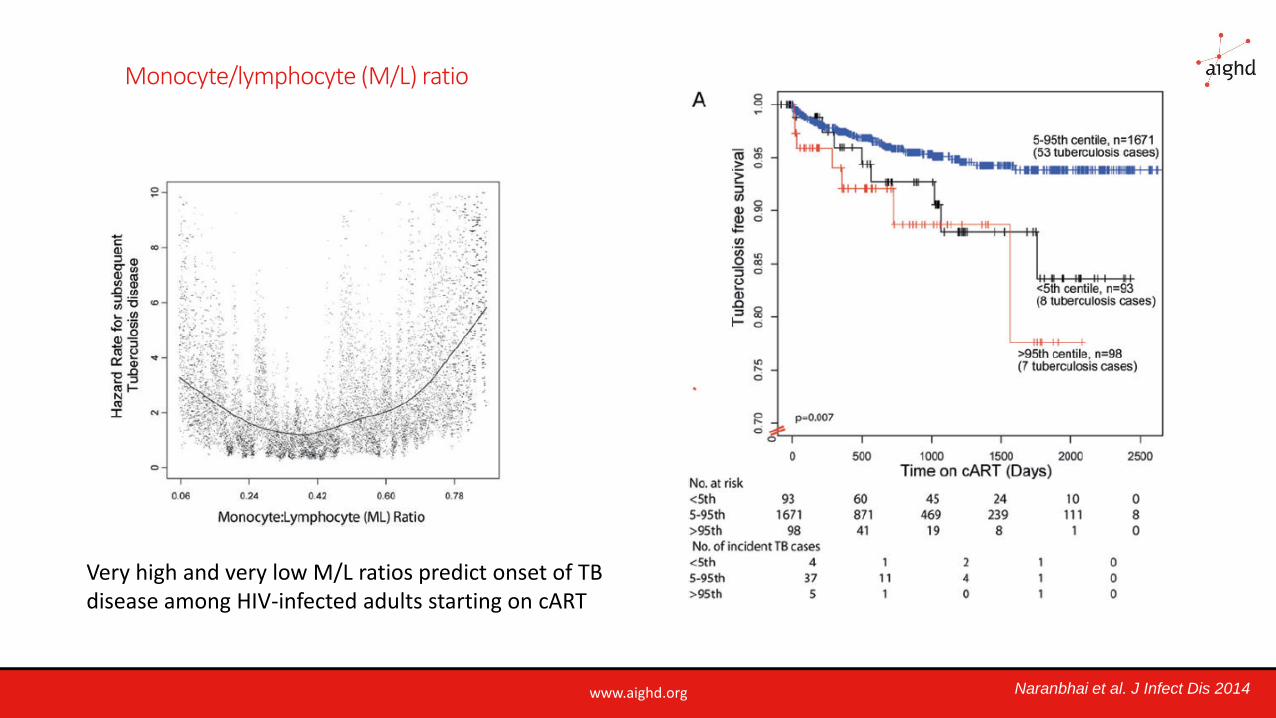
Monocyte/lymphocyte (M/L) ratio
Very high and very low M/L ratios predict onset of TB disease among HIV-infected adults starting on cART
Naranbhai et al. J Infect Dis 2014
www.aighd.org
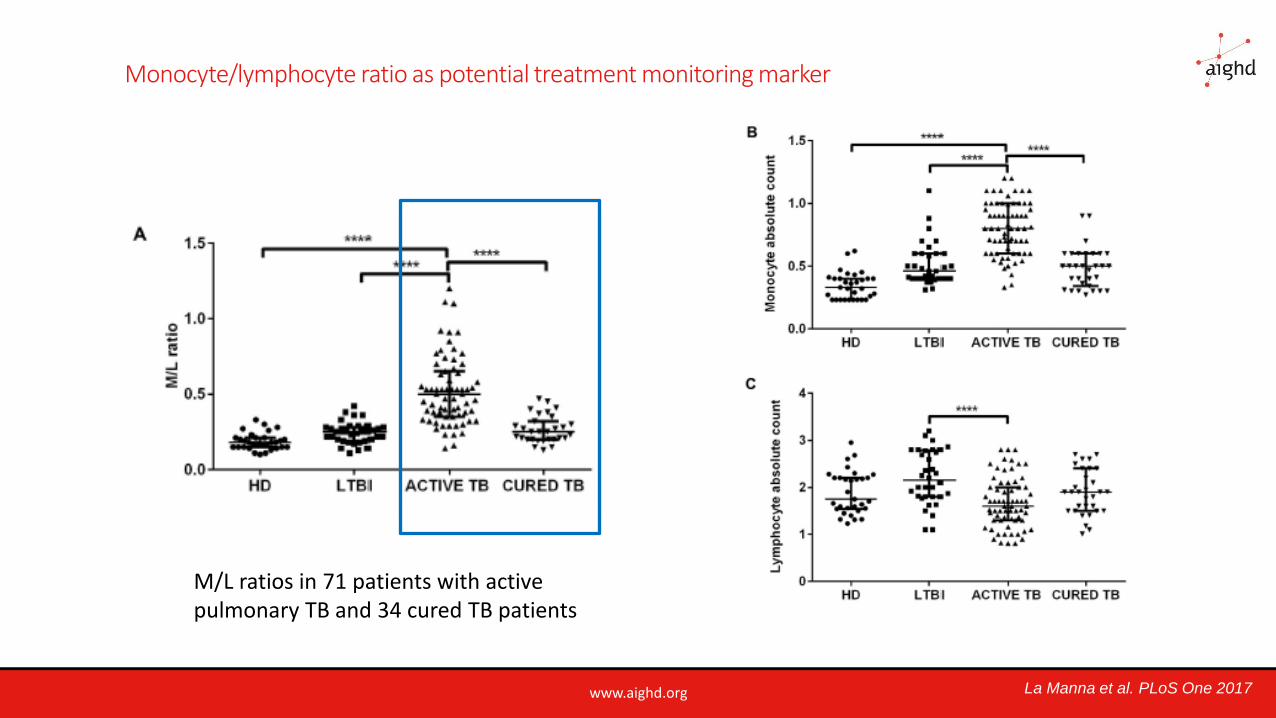
Monocyte/lymphocyte ratio as potential treatment monitoring marker
La Manna et al. PLoS One 2017
M/L ratios in 71 patients with activepulmonary TB and 34 cured TB patients
www.aighd.org
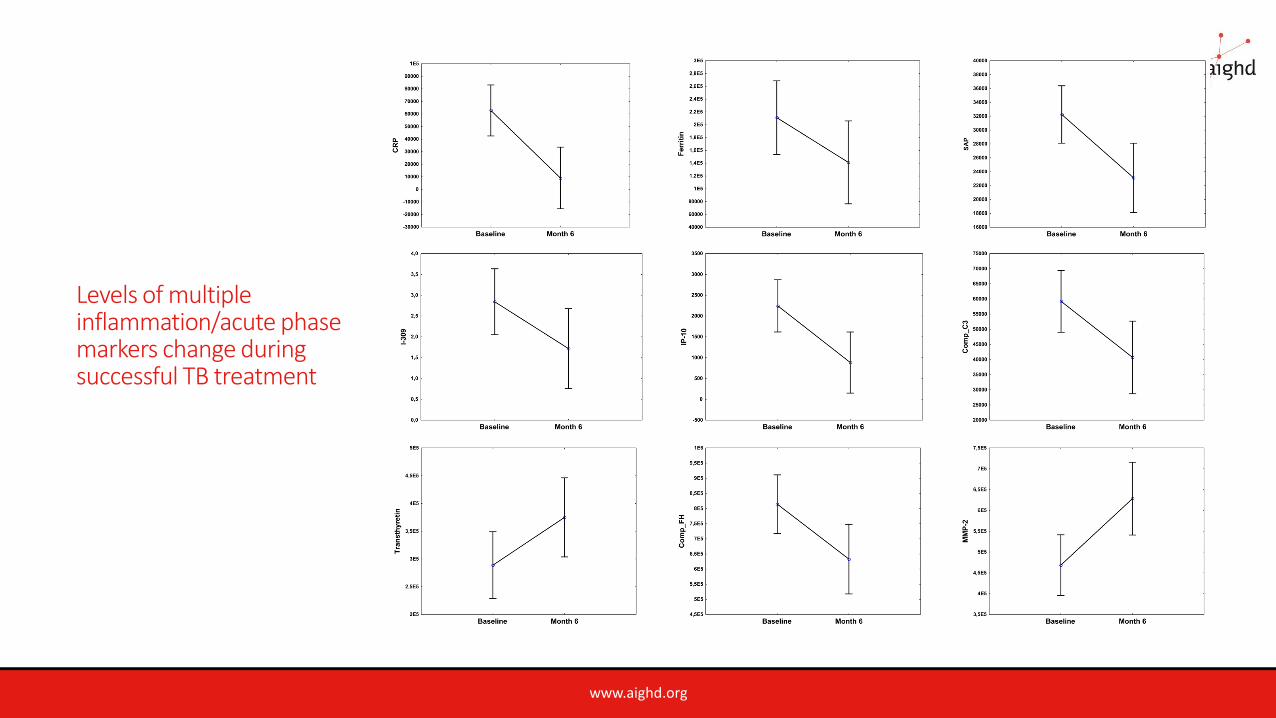
Levels of multiple inflammation/acute phase markers change during successful TB treatment
www.aighd.org
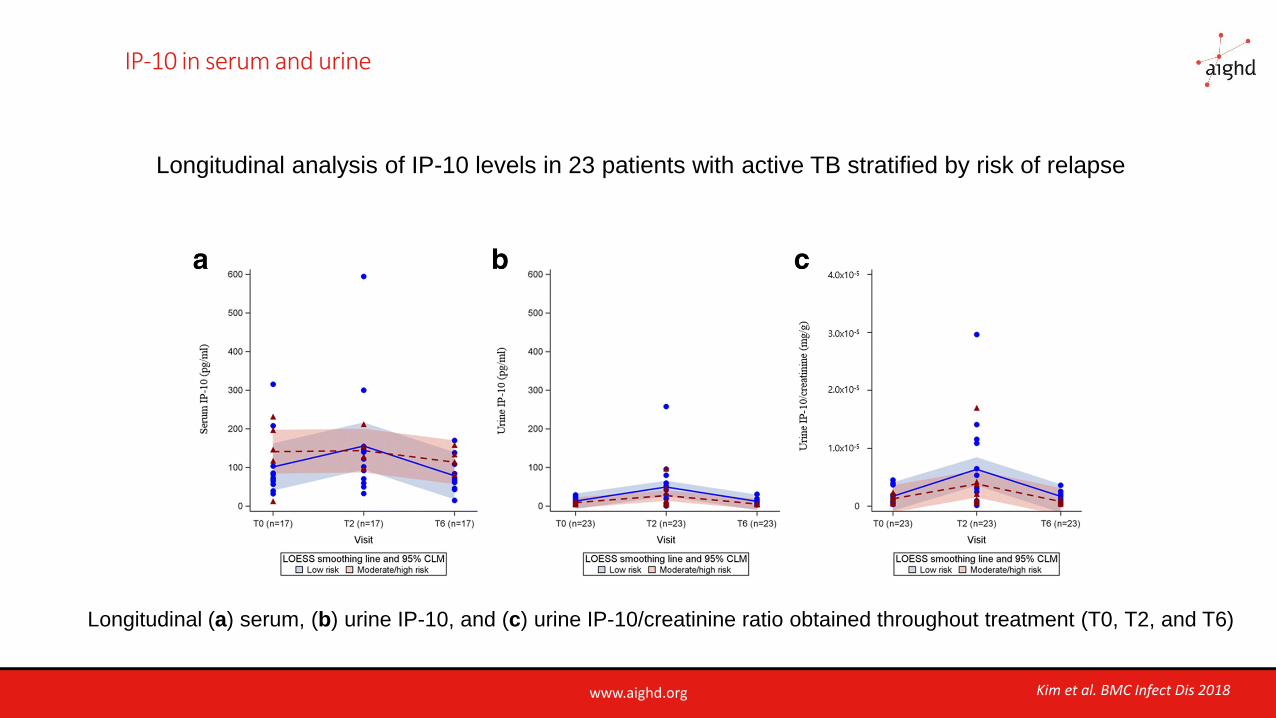
IP-10 in serum and urine
Longitudinal analysis of IP-10 levels in 23 patients with active TB stratified by risk of relapse
Longitudinal (a) serum, (b) urine IP-10, and (c) urine IP-10/creatinine ratio obtained throughout treatment (T0, T2, and T6)
Kim et al. BMC Infect Dis 2018
www.aighd.org
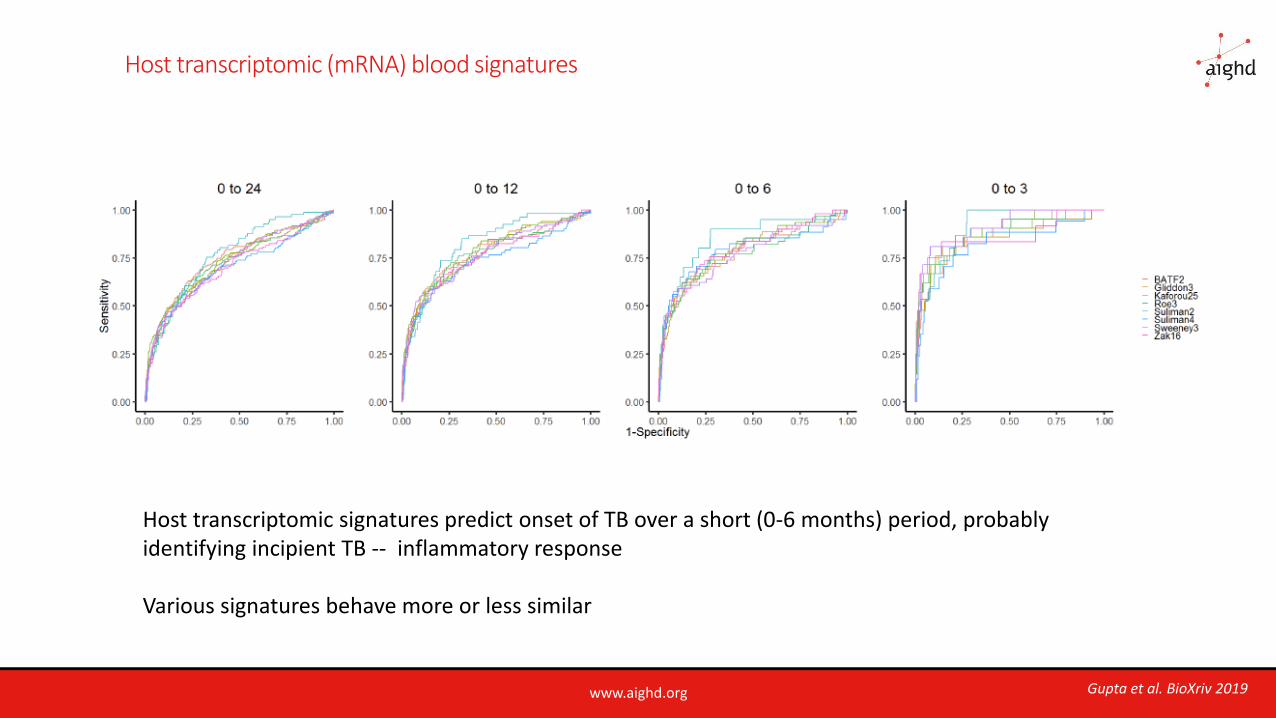
Host transcriptomic (mRNA) blood signatures
Host transcriptomic signatures predict onset of TB over a short (0-6 months) period, probably identifying incipient TB -- inflammatory response
Various signatures behave more or less similar
Gupta et al. BioXriv 2019
www.aighd.org
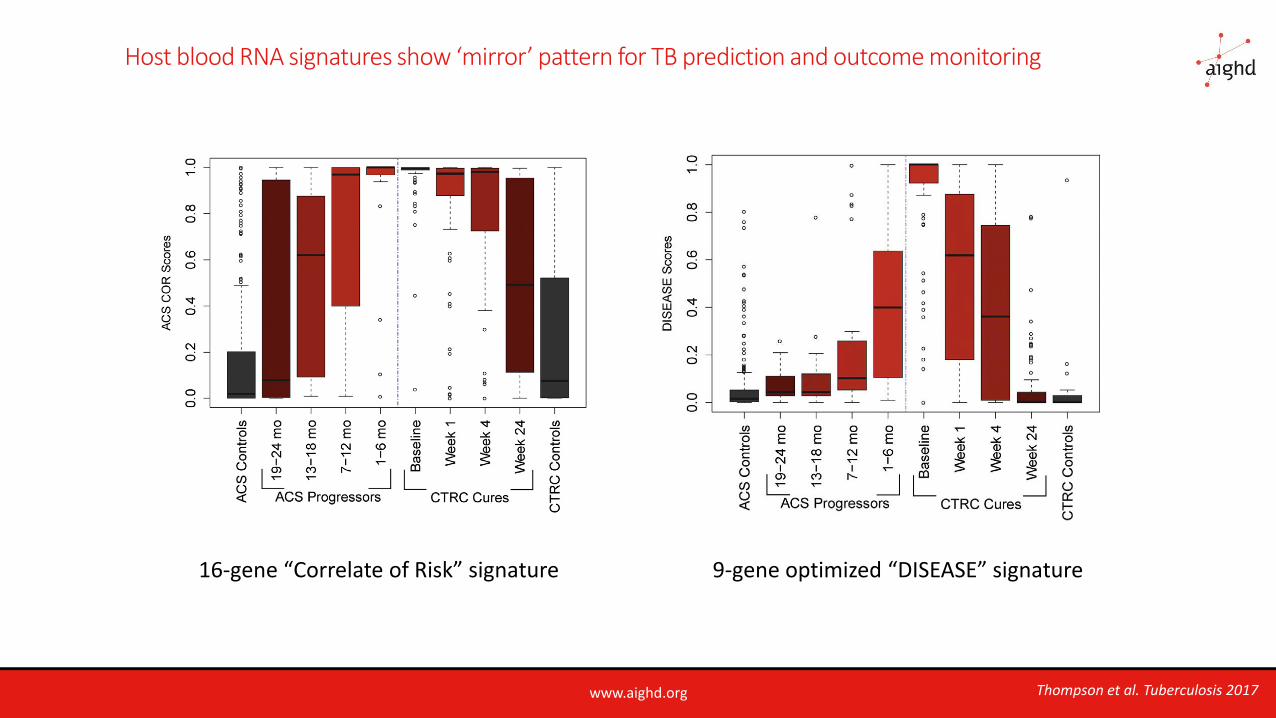
Host blood RNA signatures show ‘mirror’ pattern for TB prediction and outcome monitoring
16-gene “Correlate of Risk” signature 9-gene optimized “DISEASE” signature
Thompson et al. Tuberculosis 2017
www.aighd.org
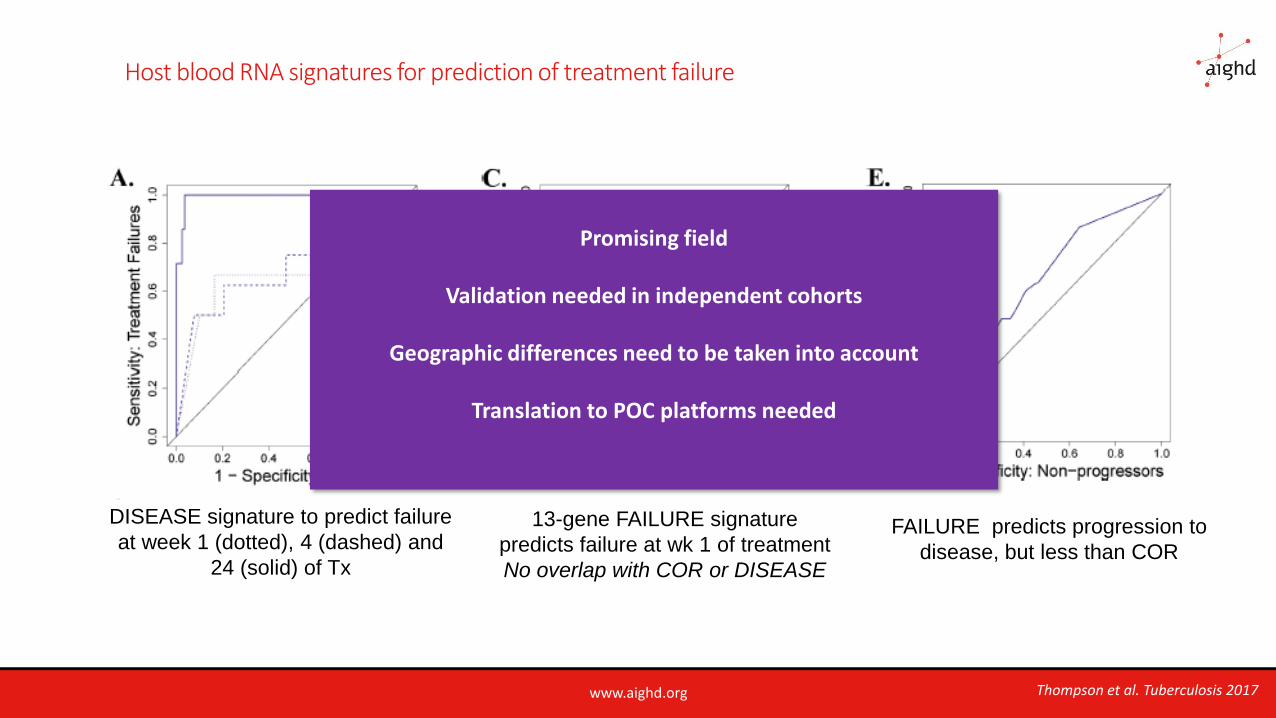
Host blood RNA signatures for prediction of treatment failure
DISEASE signature to predict failure
at week 1 (dotted), 4 (dashed) and
24 (solid) of Tx
13-gene FAILURE signature
predicts failure at wk 1 of treatment
No overlap with COR or DISEASE
FAILURE predicts progression to
disease, but less than COR
Thompson et al. Tuberculosis 2017
Promising field
Validation needed in independent cohorts
Geographic differences need to be taken into account
Translation to POC platforms needed
www.aighd.org
Conclusion
Current tools for establishing cure (smear, culture) do not exclude ongoing pathology that may result in relapse
Predicting relapse-free cure in early stages of treatment is important for stratifying patients:
-- those who need less than 6 months treatment
-- those who need more than 6 months treatment or adjunct treatment
Promising options for predicting relapse-free cure include:
◦ Risk-stratification based on pretreatment and early-treatment clinical information
◦ Immunological response marker signatures
◦ Inflammation/acute phase marker signatures
◦ Transcriptional signatures
Validation studies in various patient populations are needed prior to clinical application
Individualized treatment

www.aighd.org
Acknowledgements
Delia Goletti, Tonino Alonzi National Institute for Infectious Diseases “L. Spallanzani”, Rome , Italy
Cecilia Lindestam Arlehamn La Jolla Institute for Allergy and Immunology (LJI), La Jolla CA, USA
Tom Scriba South African Tuberculosis Vaccine Initiative, University of Cape Town, Cape Town, South Africa
Richard Anthony National Institute for Public Health and the Environment (RIVM), Utrecht, The Netherlands
Daniela Cirillo San Raffaele Scientific Institute, HSR, Milan, Italy
Claudia Denkinger FIND, currently University of Heidelberg, Heidelberg, Germany

THANK YOU