Embed Size (px)
Citation preview

Ta u s s i g C a n c e r I n s t i t u t e | A S T R O 2 0 0 9 E d i t i o n
Cancer ConsultHigHligHts from the 2009
American Society for Radiation Oncology Meeting

Dear Colleagues and Friends:
The Department of Radiation Oncology is pleased to be highlighted in
this issue of Cancer Consult. As you will see in the following pages,
2009 was a very productive year in the department. Our participation
in the 51st annual American Society for Radiation Oncology
(ASTRO) meeting in Chicago in November provides a glimpse into
the breakthrough research in which we are involved. We were very
well-represented at this meeting, with more than 20 oral and poster
presentations. In addition, Ping Xia, PhD, our new head of medical
physics, led an education session on the transition from 3D IMRT to
4D IMRT. And for the first time, each of our residents who attended
ASTRO had a poster or oral presentation, which speaks very highly of
the dedication and caliber of our residents.
This newsletter also highlights our extensive database of more than
11,000 prostate cancer patients who have undergone surgery, external
beam radiation therapy or brachytherapy at Cleveland Clinic. This
database, which is one of the largest in the world, is meticulously
maintained by Chandana Reddy, our biostatistician, and has been the
source for more than 100 papers.
In October, we were fortunate to welcome executives from major
radiation oncology corporations to our campus as part of the Medical
Innovations Summit on “Improving the Prognosis: Cancer Cures through
Innovation.” It was a chance for experts from throughout the world to
wrestle with the challenges in developing new approaches to cancer
care and to discuss future trends and opportunities. This newsletter
includes an overview of the summit on pages 6-7.
We hope you find this edition of Cancer Consult valuable, as it high-
lights new directions in our field and some of our newer programs
within the Taussig Cancer Institute. Our most important mission is to
deliver outstanding care to our patients and ultimately to win the war
on cancer. On behalf of the department, I would like to thank all of you
for your ongoing support and I look forward to continued collaboration
with you. Please feel free to contact me with any questions, concerns
or suggestions on how we can improve our service to you and your
patients, at [email protected].
Sincerely,
John Suh, MD
Chairman, Department of Radiation Oncology
Cleveland Clnic to Launch Pilot
Study to Compare Calypso with other
Therapy Modalities...1
Resident Wins 2009 American
Medical Association Award...4
Trial Paves Way for Multicenter
Study of External Beam
Radioimmunotherapy in Low-Grade
Lymphoma Management...5
Summit Showcases Improving
Prognosis in C2ancer Through
Innovation ...6
Prostate Cancer Database Is Valuable
Research Tool…8
Changing Patient Population Prompts
Study of Androgen Deprivation
Therapy in Prostate Cancer…9
Cleveland Clinic Leads RTOG
Randomized Study for Patients
with Inoperable Early-Stage Lung
Cancer…10
Radiation Oncology Welcomes New
Head of Medical Physics…13
CLINICAL TRIALS…14
PUBLICATIONS….16

Tumor motion during radiation therapy has always presented difficult
challenges for radiation oncologists. New medical technology, however,
is helping radiation oncologists address this challenge.
T E C h n O l O g y A D v A n C E S
Cleveland Clinic to Launch Pilot Study to Compare Calypso with other Therapy Modalities

In 2005, Cleveland Clinic was one of five medical
centers in the nation that participated in a prostate
cancer research study involving unique and in-
novative technology, the Calypso 4D Localization
System. Developed by Calypso Medical Technolo-
gies Inc., the external beam radiation system pre-
cisely tracks the movement of the prostate during
therapy, optimizing radiation targeting and mini-
mizing its side effects. The purpose of the clinical
study was to evaluate a nonionizing electromag-
netic method to align the prostate treatment site
for therapy and to monitor its position throughout
therapy delivery.
“During the preliminary research phase of the
Calypso System, we demonstrated that there is
fairly substantial motion of the prostate while
the patient is lying on the treatment table,” says
Rahul Tendulkar, MD, Cleveland Clinic radiation
oncologist. “One of the benefits of the Calypso
System is its ability to track the position of the
prostate in real time by emitting radio-frequency
signals from miniature Beacon wireless electro-
magnetic transponders about 8 mm in length.
The transponders are implanted transrectally
into the prostate in an outpatient procedure.
The transponders transmit the information at a
frequency of every one-tenth of a second, which
enables the real time information.”
The clinical study compared the electromagnetic
positioning to setup using skin marks and to
stereoscopic X-ray localization of the transpon-
ders. Study results published in the International
Journal of Radiation Oncology, Biology and Physics in
2007 determined that the difference between skin
marks versus the Calypso System alignment was
found to be > 5 mm in vector length in more than
T E C h n O l O gy A D vA n C E S
( c o n t i n u e d )

CLeveLAnd CLiniC | TAuSSig CAnCeR inSTiTuTe | CAnCeR COnSuLT
75 percent of fractions. Comparisons between
the Calypso System and X-ray localization showed
good agreement.
Qualitatively, the continuous motion was un-
predictable and varied from persistent drift to
transient rapid movements. Displacement > 3 mm
and > 5 mm for cumulative durations of at least 30
seconds were observed during 41 percent and 15
percent of sessions, respectively.
For individual patients, the number of fractions
with displacement >3 mm ranged from 3 percent
to 87 percent, whereas the number of fractions
with displacements >5 mm ranged from 0 percent
to 56 percent. What’s more, the Calypso System’s
transponders were typically stable four days post
implant (all by 14 days) and <1 mm standard devia-
tion for inter-transponder distances over time. All
of the transponders remained functional through-
out therapy.
“The Calypso System is a clinically efficient and
objective localization method for positioning
prostate patients undergoing radiotherapy,” the
study concluded. “Initial treatment setup can
be performed rapidly, accurately and objectively
before radiation delivery. The extent and frequency
of prostate motion during radiotherapy delivery
can be easily monitored and used for motion
management.”
“The vast majority of prostate cancer patients are
candidates for treatment with the Calypso System,”
says Dr. Tendulkar. “However, there are a few
contraindications such as, patients with implanted
devices including neurostimulators and cardiac
pacemakers, because these devices might interfere
with the transponder signals. Patients who have
had hip replacement surgery or who are obese are
not candidates for this treatment.”
In 2010, Dr. Tendulkar will be launching a pilot
research study that will compare the Calypso
System with other treatment modalities such as
cone beam CT scan-based image guidance and
ultrasound-based image guidance technology.
Modern external beam radiation therapy utilizes
CT scans and sophisticated software to create a
three-dimensional computer model of the area
being treated. This allows clinicians to more
precisely target treatments at the tumor and spare
surrounding healthy tissue or organs. The inten-
sity modulated radiotherapy is combined with
an image guidance system for localization of the
prostate. This combination provides the delivery of
a focused and individualized dose of radiation to a
small area within the pelvis.
“In our small pilot study, we want to make a
head-to-head comparison of each image-guided
technology to help us define the accuracy of each
method in delivering radiation therapy to treat
prostate cancer patients,” says Dr. Tendulkar.
“Initially, we expect to recruit three to five patients.
Depending on the preliminary data we collect
from that small group of patients, we may be able
to increase the patient pool to 15 or 20.” The pilot
study is being funded by a $50,000 grant from the
Scott Hamilton CARES Foundation.
Dr. Tendulkar notes there are research studies un-
der way at other academic and medical institutions
that are exploring whether the Calypso System can
be utilized to treat other cancers of the body, such
as those in the pancreas, lung, and head and neck.
2 | 3 | clevelandclinic.org/cancerconsult
For more information about the Calypso System, please visit www.clevelandclinic.org/calypso, or to refer a patient, call 216.445.8290.

CAnCeR COnSuLT ASTRO 2009 ediTiOn
Cleveland Clinic Radiation Oncology
resident Michael Burdick, MD, recently
earned first place in the Clinical Medicine
category at the American Medical Associa-
tion-Resident and Fellow Section Research
Symposium for his poster presentation:
“External Beam Radiotherapy Followed by
90Y Ibritumomab Tiuxetan in Relapsed
Bulky Follicular Lymphoma.” Dr. Burdick
presented the poster at the American
Society for Radiation Oncology annual
meeting. His paper on the project has been
accepted for publication in the Interna
tional Journal of Radiation Oncology, Biology
and Physics.
Dr. Burdick graduated from the University
of Virginia and earned his medical degree
from Virginia Commonwealth University.
Before coming to Cleveland Clinic, he
completed an internship at the University
of Washington. Dr. Burdick’s training also
involved a year at the National Institutes of
Health in brain tumor research, spurring
his interest in cancer.
“I wanted to pursue oncology, but I
vacillated between medical and radiation
oncology,” he says. “Radiation won
because of the cool technologies.”
Dr. Burdick says the chance to work with
a world-renowned staff drew him to
Cleveland Clinic. “I knew I would see every
Resident Wins 2009 American Medical Association Award
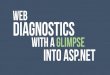
Top: Positron emission tomography/computed tomography (PET/CT) scan with 2-deoxy-2-[18F] fluoro-D-glucose (FDg) depicts a 9 cm x 5 cm para-aortic mass in a 79-year-old man with follicular lymphoma.
Bottom: Four months after treatment with external beam radiotherapy and 90y ibritumomab tiuxetan, FDg PET/CT revealed normalization of FDg uptake and near-complete resolution of the mass.
type of tumor, as well as every technique
used in radiation oncology at Cleveland
Clinic,” he says. “The residency program
has exceeded my expectations. I’ve gotten
excellent preparation for my boards,
but I’m also prepared to become a well-
rounded physician.”

CLeveLAnd CLiniC | TAuSSig CAnCeR inSTiTuTe | CAnCeR COnSuLT
While immunotherapy has improved treatment
since its approval in the late ‘90s, Cleveland Clinic
radiation oncologist Roger Macklis, MD, says that
sites harboring bulky disease are associated with
a particularly poor likelihood of responding and
shorter durability of response.
Dr. Macklis and his colleagues recently reported
encouraging results of a Phase II study in which
external beam radiotherapy (EBRT) was combined
with yttrium-90 ibritumomab tiuxetan (90Y-IT)
in 11 patients with relapsed or refractory bulky
follicular lymphoma.
Cleveland Clinic resident Michael Burdick, MD,
presented a poster on the study during the 2009
American Society for Radiation Oncology annual
meeting (see related story).
For the purpose of the study, bulky disease was
defined as >5 cm. Using computed tomography
(CT)-based planning, bulky disease sites were
contoured as the gross tumor volume with a
planning margin of 1 cm to 2 cm added, depending
on anatomical location. EBRT was delivered as
2400 cGy in 8 fractions.
Once the patient achieved complete blood count
recovery, 90Y-IT was administered at a dose of
0.3 or 0.4 mCi/kg, depending on platelet counts.
Response was measured by positron emission
tomography/CT and/or CT three to four months
after administration.
“In general, this combined approach appeared
to work as we hypothesized,” says Dr. Macklis.
“In contrast to prior patterns of failure analysis
data in this patient population, a brief course of
external beam radiotherapy prevented relapse in
sites of bulky disease.” Both in-field control and
Trial Paves Way for Multicenter Study of external Beam and Radioimmunotherapy in Low-grade Lymphoma Management
progression-free survival compared favorably
to historical data. The complete and overall
responses to combined therapy as measured
three to four months after 90Y-IT were 64 percent.
Median progression-free survival was 17.5 months.
“While the trial was not statistically significant
due to its nonrandomized design and small size,
we hope our results will create a paradigm for the
future,” says Dr. Macklis. Plans are currently being
considered for an industry-funded multicenter
trial expanding on this experience.
To learn more about this trial or to refer a patient to Dr. Macklis, call 216.444.5576 or email [email protected].
Between 20,000 and 25,000 patients in the United States present with indolent B-cell
non-Hodgkin lymphoma every year, representing a diverse epidemiologic cohort.
4 | 5 | clevelandclinic.org/cancerconsult

Taussig Cancer Institute Chairman Derek Ragha-
van, MD, PhD, chaired a roundtable discussion on
the “Grand Challenges in Contemporary Cancer
Treatment and Biology.” Tom Miller, CEO of work-
flow solutions at Siemens; Sir Bruce Ponder, MD,
director of the Cancer Research UK Cambridge
Research Institute; and William Hait, MD, senior
vice president and worldwide leader of hematolo-
gy and oncology at Johnson & Johnson, concluded
that while developing cancer treatments is time-
consuming and costly, information technologies
will be important in pairing the right patients with
the right treatments.
Partnering with others can help speed the develop-
ment process, Miller said. But accounting is the
greatest impediment to progress. “We don’t know
the return on the investment we do,” he said.
John Suh, MD, chairman of the Department
of Radiation Oncology in the Taussig Cancer
Institute, moderated a panel on the “Revolution in
Radiotherapy Technology,” with Jean Marc Andral,
president of Advanced Radiotherapy, IBA; Shawn
Guse, vice president of International Operations,
TomoTherapy and CEO of Compact Particle
Acceleration Corporation; Tomas Puusepp, CEO
at Elekta; Eric Lindquist, senior vice president of
Accuray; and Dow Wilson, president of Oncology
Systems, Varian. The group provided a firsthand
analysis of new directions and challenges for
innovators in radiotherapy.
“Radiation oncology is at the forefront in terms
of using evidence-based medicine to differenti-
ate various approaches to cancer,” Dr. Suh said.
“Technological advances and a better under-
standing of how tumors respond to treatment
have meant shorter and more precise radiation
treatment options. The question has become: At
what cost?”
summit showcases improving Prognosis in Cancer through innovation
In October 2009, Cleveland Clinic hosted a Medical Innovations Summit
that brought more than 900 prominent physicians, senior executives from
pharmaceutical and medical device companies, entrepreneurs, investors and
others together for an in-depth analysis of innovation in the field of cancer.
2009
Cleveland Clinic president and CEO Toby Cosgrove, MD, opened the summit with an address on
healthcare reform, saying that in the United States, we are debating health insurance reform instead of
health care reform. Rather than demand higher reimbursements for care, doctors and hospitals ought
to demand greater efficiency in delivering care, he said. In addressing innovation in healthcare, Dr.
Cosgrove said, “Some people see devices and drugs as a problem. We see them as part of the solution.”

Device manufacturers agreed that the economic
challenges of developing and testing technology
are huge. “One successful cancer drug would
produce more revenue than all of the companies
on this stage,” said Mr. Guse.
Panel members returned to a familiar summit
theme, stressing the importance of informatics to
improve access to patient data and increase out-
comes research. “Radiation plays a role in nearly
two-thirds of all cancer patients, but we are losing
market share in some areas to other care modali-
ties,” said Mr. Wilson. “We have great tools, but
we have to prove their worth. We have to make a
better case about the outcomes of radiation treat-
ments. Comparative effectiveness will become
more and more important.”
In his keynote address, Sam Palmisano, IBM
chairman, president and CEO, revealed that the
time has come for a smarter healthcare system.
“The single issue that is most critical to the future
of healthcare in this country—and the world—is
the need for a true healthcare system,” he said.
“And I believe we have a better chance now than
ever before to build it.”
Mr. Palmisano said that there is a broad
consensus—forged, in many respects, by the
example of such institutions as Cleveland
Clinic—that American healthcare must become
patient-centric. But it must also be value-focused,
evidence-based, accountable and sustainable.
Clearly, a smarter healthcare system, optimized
around the patient, would increase efficiency,
reduce errors, achieve better quality outcomes
and save lives. “It could embed best practices and
medical knowledge—as well as real-time patient
monitoring—into clinical and business workflows,
for error-free delivery of care,” said Mr. Palmi-
sano. “And that alone is ample justification for the
investment.”
The summit concluded with the unveiling of the
“Top 10” Medical Innovations for 2010, emerging
technologies that will shape healthcare this year.
The list of breakthrough devices and therapies was
selected by a panel of Cleveland Clinic physicians
and scientists. This year’s No. 1 innovation
was Bone Conduction of Sound for Single-
Sided Deafness: a new nonsurgical, removable
hearing and communication device designed to
imperceptibly transmit sound via the teeth to help
people with single-sided deafness.
For a complete list of the “Top Ten” and details
of next year’s summit, “Obesity, Diabetes & the
Metabolic Crisis,” visit clevelandclinic.org/
innovations.
6 | 7 | clevelandclinic.org/cancerconsult
“Radiation oncology is at the fore-
front in terms of using evidence-based
medicine to differentiate various
approaches to cancer.”
The two-day event highlighted the need for partnerships
among researchers and developers, since no one institu-
tion or company has the financial or intellectual assets
to go this route alone.

CAnCeR COnSuLT ASTRO 2009 ediTiOn
Clinical databases are becoming more prevalent at
institutions that treat large populations of prostate
cancer patients. The Cleveland Clinic database is
unique in its breadth and depth of information
and in its multidisciplinary orientation, notes
biostatistician Chandana Reddy, MS.
“We are the only institution that integrates radia-
tion and surgery patients in a single database,” she
says. “That structure was decided at the outset as
the most accurate way to track and compare out-
comes across different patient populations.”
Data on all patients treated by prostatectomy,
external beam radiation or brachytherapy are
entered from multiple sources. “To create a
complete profile for each patient, the database
includes patient demographics, family history to
second-degree relatives and all pre- and post-
treatment clinical data,” Reddy explains. Each
patient’s pre- and post-treatment PSA values,
biopsy Gleason score and tumor stage are
recorded, along with the treatment modality.
For patients who undergo external beam radiation
or brachytherapy, the database captures dosim-
etry, radiation dose and the number of fractions
or the number of brachytherapy seeds. Following
completion of treatment, all follow-up PSA results
are recorded to track patient outcomes in terms
of disease-free survival, biochemical recurrence,
cancer recurrence and all-cause mortality.
At the 2009 ASTRO meeting, the Cleveland Clinic
database was the foundation for three oral pre-
sentations and four poster presentations, includ-
ing an oral presentation by Andrew Vassil, MD,
(see related story). Other ASTRO presentations
that utilized the database featured an analysis of
Prostate Cancer database is valuable Research Tool
Cleveland Clinic Taussig Cancer Institute is home to one of the most sophisticated prostate cancer
databases in the world. Containing comprehensive baseline, treatment and follow-up data on more than
11,000 patients treated since 1986, the database is a powerful resource for prostate cancer research.
treatment effectiveness in prostate cancer patients
younger than 55 and an exploration of factors that
are predictive for early mortality in men treated for
localized prostate cancer.
“These studies demonstrate the power of our
database,” Reddy says. “Because it contains such
in-depth data on such a large number of patients,
researchers have the luxury of selecting exactly the
patient population they want to study.”
Another advantage for researchers is that individu-
al patient records in the database are indexed by a
unique patient number. This allows easy retrieval
and cross-referencing with stored prostate biopsy
tissue samples. “The tissue repository enhances the
utility of the prostate cancer database by providing
DNA for molecular studies,” Reddy explains.
Beyond pure research applications, the database
also is used for treatment planning and quality
monitoring, she adds. “Our core group of prostate
cancer specialists reviews the trends in patient treat-
ment and outcomes as a tool for improving quality
of care and pursuing new avenues of research. One
of the results from these review meetings was our
group’s research in the area of prostate cancer
specific mortality. We were the first institution to
begin studying this endpoint across all treatment
modalities, and we are now seeing other institu-
tions assess their patients for this endpoint.”
Historically, more than 100 papers have been
published based on research using the database. In
addition to the presentations at ASTRO in 2009, the
database was used for two oral presentations and
two posters presented at the American Brachyther-
apy Society annual meeting and three posters pre-
sented at the Genitourinary Cancers Symposium.

Andrew Vassil, MD, resident and investigator in
the Department of Radiation Oncology, presented
a study during the 2009 ASTRO annual meeting
assessing the duration of androgen deprivation
therapy used in the management of patients with
high-risk prostate cancer undergoing curative
external beam radiation therapy.
Dr. Vassil examined earlier studies and compared
them to more recent Cleveland Clinic outcomes.
Earlier research showed that for men with locally
advanced prostate cancer, the addition of long-
term (> 2 years) androgen deprivation (AD) in
addition to definitive external beam radiotherapy
resulted in improved local and distant control;
disease-specific survival; and, in some cases, over-
all survival. Other studies have shown that higher
doses of radiation therapy are safe, and may be
more effective for patients with localized prostate
cancer. AD therapy is associated with multiple side
effects, including an increased risk of heart attack.
Recently, with the advent of PSA screening, a stage
migration has occurred, resulting in diagnosis at
an earlier stage, younger age, lower PSA, and with
a less aggressive cancer. “Because of these prostate
cancer population changes, patients treated on pri-
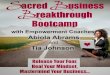
Above: high radiation dose is safely distributed to the prostate with relative sparing of normal structures such as the bladder and rectum.
Right: Multiple radiation fields may be shaped, modulated and combined to intersect at the tumor site and avoid high radiation doses to normal organs.
8 | 9 | clevelandclinic.org/cancerconsult
Changing Patient Population Prompts Study of Androgen deprivation Therapy in Prostate Cancer
or trials are not representative of current patients,”
says Dr. Vassil. “In addition, radiation techniques
and doses used in the past are now considered
suboptimal. Despite these significant changes, it
remains common practice to offer long-term AD to
patients with localized disease.”
Dr. Vassil and his colleagues reviewed Cleveland
Clinic institutional outcomes, stratified by dura-
tion of AD, to estimate its effect on prostate cancer
control and survival. The study included 553
patients with high-risk prostate cancer treated at
Cleveland Clinic.
All these patients received high-dose radiation
therapy using modern delivery techniques. Treat-
ment with more than six months of AD did not
appeared to improve PSA control or disease recur-
rence rates. These patients also had worse overall
survival and appeared to develop cancer resistant
to the effects of androgen suppression sooner (also
known as androgen-independent prostate cancer).
“Long-term AD may cause weight gain, hot flashes,
mood changes, bone mineral density loss and
heart disease for no therapeutic gain,” concludes
Dr. Vassil. “It is possible that modern radiation
techniques delivering high radiation doses
may overcome the need for long-term AD, thus
preserving patients’ quality of life after receiving
curative treatment.”

CAnCeR COnSuLT ASTRO 2009 ediTiOn
SBRT is a novel form of radiation delivery that is
becoming increasingly utilized to manage NSCLC
in patients for whom surgery is contraindicated,
because it delivers highly precise, very high-dose
radiotherapy (RT) in very few fractions. SBRT
requires very accurate tumor delineation and
methods by which tumor motion due to breathing
is accounted for during the delivery process.
SBRT has been shown to provide remarkably high
rates of local control, comparable to those seen
with surgery, but with little severe toxicity in what
is otherwise a fragile patient population. The
optimal treatment schedule in the setting of SBRT
is currently an active area of investigation. When
first being explored a decade ago, up to 10 treat-
ments might have made up a course of SBRT. The
primary objective of the RTOG 0915 randomized
Phase II study is to determine the one-year rate
of > grade 3 adverse events related to treatment
with single fraction versus 4 fractions of SBRT in
medically inoperable patients with stage I NSCLC.
Sponsors of the study are the Radiation Therapy
Oncology Group (RTOG) and the National Cancer
Institute.
“What is interesting in the RTOG 0915 study is that
we think the delivery of a single fraction or multiple
fractions will be essentially equivalent in eradicat-
ing the cancer,” says Dr. Videtic. “Now we’re inter-
ested in which treatment will be associated with the
lowest rate of side effects for these fragile patients,
even though the risk of developing complications
may be low to begin with. As we now are seeing
these patients many months and even years after
their cancer is eradicated, we are finding that for
tumors close to the rib cage, there may be a higher
risk for patients to develop delayed fractures.”
Lung cancer is the leading cause of cancer mortality
in the United States. Eighty percent of lung cancers
are NSCLC, and approximately 15 to 20 percent of
these patients present with early localized NSCLC.
Patients who undergo surgical treatments can
expect a five-year survival rate of 50 to 70 percent,
depending on the initial size of their tumors.
However, a significant number of NSCLC patients
do not qualify for the surgical treatment because of
co-morbidities including advanced heart disease,
emphysema, bronchitis or other complications
such as tumor location.
Medically inoperable early-stage NSCLC patients
have been historically treated with conventional ex-
ternal beam RT. Unfortunately, these RT treatment
results invariably proved inferior to surgical results,
likely due to the interaction between an inability to
control the cancer with modest RT doses and the
underlying medical conditions of the patients.
For example, one study involved 141 patients with
stage I NSCLC who were treated with RT using
modern techniques and staging. The median RT
dose delivered was 64 Gy (range: 48 Gy to 80 Gy).
The overall survival rate at one and five years was
39 percent and 13 percent, respectively, while the
progression-free survival was 48 percent and 28
percent at two and five years, respectively. Forty-
nine percent of patients had local failure as part
of their relapse pattern. In fact, other studies have
reported local recurrence to be the most common
cause of failure with standard RT.
SBRT was pioneered by Swedish and Japanese
medical researchers more than 10 years ago. In
the United States, Indiana University has been a
leader in SBRT research, conducting foundational
n E w R E S E A R C h :
Cleveland Clinic Leads RTOg Randomized Study for Patients With inoperable early-Stage Lung Cancer
Cleveland Clinic Radiation Oncologist Gregory Videtic, MD, is the principal investigator for a new
randomized Phase II study comparing stereotactic body radiation therapy (SBRT) schedules for
medically inoperable patients with stage I peripheral non-small cell lung cancer (NSCLC).
To refer a patient, please call Dr. Videtic at 216.444.9797.

research trials about six years ago. After promising
Phase I study results, a Phase II prospective study
was carried out, involving 70 patients who received
doses of 60 Gy to 66 Gy in three fractions during
one to two weeks. With a median follow-up of 17.5
months, actuarial local control at two years was 95
percent. However, the study also found that Grade
3 to 5 toxicity occurred in 14 patients, which on
analysis proved to be associated with tumor loca-
tion, i.e., lesions in close proximity to the tracheo-
bronchial tree and mediastinum. Currently, RTOG
is conducting a study on the maximally tolerated
SBRT dose for this class of tumors (RTOG 0813). All
ongoing studies in SBRT now make the distinction
between such tumors, termed central, and all oth-
ers, termed peripheral.
Since the efficacy and safety of SBRT for peripheral
tumors has become established, medical oncolo-
gists at Cleveland Clinic have collaborated with
radiation oncologists in offering SBRT treatments
to stage I NSCLC patients.
“It’s very gratifying that we can offer not only an
effective but safe treatment for NSCLC patients,
because before SBRT their options were extremely
limited,” says Dr. Videtic. “This represents a huge
shift in practice.”
Some of the secondary objectives of the RTOG 0915
study will include estimating the one-year local
control rate in patients and estimating the one-
year overall survival and disease-free survival rate.
Patients will be randomly assigned to two groups.
One group will receive a single fraction once, and
the second group will receive a single fraction once
a day for four days.
10 | 11 | clevelandclinic.org/cancerconsult
For more information about the RTOG 0915 study, visit http://www.clinicaltrials.gov/ct2/show/NCT00960999.
hOSPITAlS
Cleveland Clinictaussig Cancer institute9500 Euclid Ave./R35Cleveland, OH 44195216.444.7923
Fairview Hospital18101 Lorain Ave.Cleveland, OH 44111216.476.7000
Hillcrest Hospital6780 Mayfield Rd.Mayfield Heights, OH 44124440.312.4500
BeachwoodFamily Health and Surgery Center26900 Cedar Rd.Beachwood, OH 44122216.839.3000 or 800.801.2233
independenceCancer Center6100 Westcreek Rd.Ste. 15 & 16Independence, OH 44131216.524.7979, Medical Oncology216.447.9747, Radiation Oncology
lorainFamily Health and Surgery Center5700 Cooper Foster Park Rd.Lorain, OH 44053440.204.7400 or 800.272.2676
ParmaCancer Center6525 Powers Blvd.Parma, OH 44129440.743.4747
strongsvilleFamily Health and Surgery Center16761 SouthPark CenterStrongsville, OH 44136440.878.2500 or 800.239.1098
Willoughby HillsFamily Health Center2570 SOM Center Rd.Willoughby Hills, OH 44094440.943.2500 or 800.807.2888
WoosterFamily Health Center1740 Cleveland Rd.Wooster, OH 44691330.287.4500 or 800.451.9870
CAnCER CARE lOCATIOnS

CAnCeR COnSuLT ASTRO 2009 ediTiOn
“Patient data is one of the most important proper-
ties of Cleveland Clinic because it provides a solid
foundation for outcomes research,” she says. “If
we are to advance the care of patients, we have to
look retrospectively at how all of our new technolo-
gy is impacting patients in terms of the length and
quality of their lives.” Cleveland Clinic’s leadership
in implementing the electronic medical record
was a key factor in luring Dr. Xia from California to
Ohio as the first female head of Medical Physics.
Dr. Xia sees the role of her team of physicists
as helping radiation oncologists solve clinical
problems and speeding the implementation of
new findings into practice. With the evolution of
intensity modulated radiation therapy (IMRT) and
recent advances in image-guided radiation therapy
(IGRT), Dr. Xia says her team is focusing on motion
management, or adaptive therapy. “We know the
patient is a dynamic target,” she says. “We have to
determine the best way to use new technology to
individualize radiation oncology.”
Dr. Xia shared her insights in an education course
at ASTRO, “Transitioning from 3D IMRT to 4D
IMRT and the Roles of Image Guidance,” with co-
presenter Peter Balter, PhD, from M.D. Anderson
Cancer Center. Dr. Xia focused on how IGRT and
4D CT technologies can be used to improve dose
delivery precision and accuracy, particularly with
dynamically changing tumor volumes.
“In the old days, we treated large fields,” she says.
“We cast a net so big that anything within it would
be affected.” IMRT opened the possibility of con-
formal dose distributions to tumors of nearly any
shape. But conformal treatment presented its own
challenges.
“We could precisely target the tumor and spare
surrounding tissue, but if the tumor moved, we’d
miss it,” she says. The advantages of conformal
dose distribution can only be realized if radiation
oncologists can precisely associate the patient’s
anatomy with delivered dose in both spatial and
temporal fashion. Today, 4D planning includes
incorporating changes in patient anatomy into
treatment planning.
Drs. Xia and Balter examined lung, prostate, and
head and neck cancers to illustrate technical
challenges when tumors change by the second,
day or week. “Organ movements and anatomic
changes in patients require us to explicitly include
a time variable into both planning and delivery,”
says Dr. Xia.
Radiation Oncology Welcomes new Head of Medical Physics
When Ping Xia, PhD, came to Cleveland Clinic from the University of
California, San Francisco to head Medical Physics in the Department of
Radiation Oncology, she welcomed the chance to advance research.
Clinical Requirements of iMRt (time scale)
lung tumor
(second)
Prostate
(day)
Head and Neck
(week)
For more information, contact Dr. Xia at [email protected].

12 | 13 | clevelandclinic.org/cancerconsult
Cancer Consult provides information from Cleveland Clinic Taussig Cancer Institute specialists about innovative research and diagnostic and management techniques.
Please direct correspondence to John Suh, MD, Guest Medical Editor [email protected]
Taussig Cancer Institute/R35 Cleveland Clinic 9500 Euclid Avenue Cleveland, OH 44195
Cleveland Clinic Taussig Cancer Institute annually serves more than 26,000 cancer patients. More than 250 cancer specialists are committed to researching and applying the latest, most effective techniques for diagnosis and treatment to achieve long-term survival and improved quality of life for all cancer patients. Taussig Cancer Institute is part of Cleveland Clinic, an independent, not-for-profit, multispe-cialty academic medical center.
Cancer Consult guest Medical EditorJohn Suh, MD, Chairman,Radiation Oncology
Cancer Consult Editorial Board
Derek Raghavan, MD, PhD, Chairman, Taussig Cancer Institute
Brian Bolwell, MD, Chairman,Hematologic Oncology and Blood Disorders
Robert Dreicer, MD, Chairman, Solid Tumor Oncology
Brian Rini, MD Solid Tumor OncologyMedical Editor
Timothy Spiro, MD, Chairman, Regional Oncology
Gene Barnett, MD, Director, Brain Tumor and Neuro-Oncology Center
Eric Klein, MD, Chairman, Urologic Oncology,Glickman Urological & Kidney Institute
Managing Editor Marjie Heines
DesignerAmy Buskey-Wood
PhotographyRussell Lee, Tom Merce
MarketingLori Schmitt, RN, Andrew Kraynak,Melissa Mason
Cancer Consult is written for physicians and should be relied upon for medical education purposes only. It does not provide a complete overview of the topics covered and should not replace the independent judgment of a physician about the appropriateness or risks of a procedure for a given patient.
© 2010 The Cleveland Clinic Foundation
09-CNR-023
IGRT provides better defined margins and more
precise patient positioning, as well as better
localization of the target during treatment. But Dr.
Xia cautions that no single IGRT tool can address
all clinical issues. Each new tool must be carefully
evaluated to determine its usefulness in various
tumor types.
Dr. Xia is active in the Radiation Therapy Oncology
Group and says she plans to continue her study on
the development of 4D radiation therapy, includ-
ing deformable image registration to expedite
contouring in treatment planning, 4D planning
and 4D treatment delivery.
Why 4D Delivery?
• Track fast moving organs: adjust treatment
portals during treatment.
• Adapt to daily changes of the organ filling
(such as the bladder and rectum): adjust
treatment positions prior to treatment.
• Adapt to slow anatomy changes in head
and neck patients: adjust treatment plans
periodically during the treatment course.

Clinical TrialsDirectory Now Online
Radiation Therapy Oncology group (RTOg) Trials Open to Enrollment
RTOG 0227
Phase I/II study of pre-irradiation chemo-therapy with methotrexate, rituximab, and temozolomide and post-irradiation temozolomide for primary central nervous system lymphoma
RTOG 0413
A randomized Phase III study of conventional whole breast irradiation (WBI) versus partial breast irradiation (PBI) for women with stage 0, I, or II breast cancer
RTOG 0433
A Phase III international randomized trial of single versus multiple fractions for re-irradiation of painful bone metastases
RTOG 0436
A Phase III trial evaluating the addition of cetuximab to paclitaxel, cisplatin, and radiation for patients with esophageal cancer who are treated without surgery
RTOG 0534
A Phase III trial of short-term androgen deprivation with pelvic lymphnode or prostate bed only radiotherapy (SPPORT) in prostate cancer patients with a rising psa after radical prostatectomy
RTOG 0538
Phase III comparison of thoracic radiotherapy regimens in patients with limited small cell lung cancer also receiving cisplatin and etoposide
RTOG 0614
A randomized, Phase III, double-blind, placebo-controlled trial of memantine for prevention of cognitive dysfunction in patients receiving whole-brain radiotherapy
RTOG 0617
A randomized Phase III comparison of standard-dose (60 gy) versus high-dose (74 gy) conformal radiotherapy with concurrent and consolidation carboplatin/paclitaxel +/- cetuximab (IND #103444) in patients with stage IIIA/IIIB non-small cell lung cancer
RTOG 0619
A randomized Phase II trial of chemo-radiotherapy versus chemoradiotherapy and vandetanib for high-risk postoperative advanced squamous cell carcinoma of the head and neck
RTOG 0825
Phase III double-blind placebo-controlledtrial of conventional concurrent chemo-radiation and adjuvant temozolomide plus bevacizumab versus conventional concurrent chemoradiation and adjuvant temozolomide in patients with newly diagnosed glioblastoma
RTOG 0813
Seamless Phase I/II study of stereotactic lung radiotherapy (sbrt) for early-stage, centrally located, non-small cell lung cancer (NSCLC) in medically inoperable patients
Cleveland Clinic Taussig Cancer Institute offers an online tool for physicians, patients and caregivers to search for open clinical trials. The web-based clinical trials database lists all of the trials being managed by oncologists in the Taussig Cancer Institute that are accepting patients. At any given time, several hundred cancer clinical trials are under way on the man campus, and at Hillcrest and Fairview hospitals.
To search the database, visit clevelandclinic.org /cancerclinicaltrials

14 | 15 | clevelandclinic.org/cancerconsult
Critical to taussig Cancer institute’s success is the complete partnership established
with Cleveland Clinic’s nationally recognized teams of cancer care specialists. the
following leaders from other Cleveland Clinic institutes collaborate with taussig staff
to provide the most advanced oncologic care to our patients:
Cole Eye instituteArun Singh, MD
Dermatology & Plastic surgery instituteAllison Vidimos, MDPhilip Bailin, MD, MBAWilma Bergfeld, MDChristopher Gasbarre, DODavid Hamrock, MDDouglas Kress, MDEdward Maytin, MD, PhD Jonelle McDonnell, MDJon Meine, MDMelissa Piliang, MD Christine Poblete-Lopez, MDApra Sood, MDJames Taylor, MD Kenneth Tomecki, MD
Digestive Disease instituteFederico Aucejo, MDCarol Burke, MDSricharan Chalikonda, MDJames Church, MDGary Falk, MDVictor W. Fazio, MDJohn Fung, MD, PhDMichael Johnson, MDMatthew Kalady, MDIan Lavery, MD, BSK.V. Narayanan Menon, MDJames Merlino, MDCharles Miller, MDFeza H. Remzi, MDMatthew R. Walsh, MD
Endocrinology & Metabolism instituteAllan Siperstein, MD
glickman Urological & Kidney instituteRyan Berglund, MDSteven Campbell, MD, PhDKhaled Fareed, MDAmr Fergany, MDMichael Gong, MD, PhDJ. Stephen Jones, MD, FACSJihad Kaouk, MDEric Klein, MDDavid Levy, MDCharles S. Modlin, Jr., MDRobert Stein, MDAndrew J. Stephenson, MDJames C. Ulchaker, MD
Head & Neck instituteDaniel Alam, MDMichael Benninger, MDBrian Burkey, MDTodd Coy, DMDHusam Elias, MD, DMDMichael Fritz, MDMichael Huband, DDSP. Daniel Knott, MDJoseph Scharpf, MDPeter Weber, MDBenjamin Wood, MD
Miller Family Heart & Vascular instituteThomas Rice, MDDavid Mason, MDSudish Murthy, MD
Neurological instituteManmeet Ahluwalia, MDLilyana Angelov, MDGene Barnett, MDSamuel Chao, MDBruce Cohen, MDJoung Lee, MDJeremy Rich, MDBurak Sade, MDGlen H. Stevens, DO, PhDTanya Tekautz, MDMichael Vogelbaum, MD, PhDRobert Weil, MD
Ob/gyn & Women’s Health instituteJoseph Crowe, MDJill Dietz, MDRichard Drake, MDPedro Escobar, MDAlicia Fanning, MDKatherine Lee, MDLawrence Levy, MDChad Michener, MDHolly Pederson, MDPeter Rose, MDRobyn Stewart, MD
Orthopaedic & Rheumatologic institute Michael Joyce, MDSteven Lietman, MD
Pulmonary instituteRendell Aston, MDThomas Gildea, MDMichael Machuzak, MDPeter Mazzone, MDMadhu Sasidhar, MD
Pediatric institute & Children’s HospitalL. Kate Gowans, MDEric Kodish, MDMichael Levien, MDGregory Plautz, MDTanya Tekautz, MDMargaret Thompson, MD, PhD

Boutros J, Almasan A. Combining 2-deoxy-D-glucose with electron transport chain blockers: A double-edged sword. Cancer Biol Ther, Vol 8, Issue 13: 1241 – 1242, July 1, 2009.
Burdick MJ, Macklis, RM. Update on the Rational Use of Tositumomab and Iodine-131 Tositumomab Radioimmunotherapy for the Treatment of Non-Hodgkin’s Lymphoma. Oncotargets and Therapy. 2009: 2, 229-242.
Burdick MJ, Reddy CA, Ulchaker J, Angermeier K, Altman A, Chehade N, Mahadevan A, Kupelian PA, Klein EA, Ciezki JP. Comparison of Biochemical Relapse Free Survival between Primary Gleason 3 and Primary Gleason 4 for Biopsy Gleason 7 Prostate Cancer. Int J Radiat Oncol Biol Phys. 73(5):1439-45, 2009.
Cheng S, Iannettoni, Koshy M, Suntha M, Urba S. Squamous Cell Carcinoma of the Esophagus: Treat with How Many Modalities? 36:6, pp. 493-497. Seminars in Oncology, December 2009.
Chow E, James J, Barsevick A, Hartsell W, Ratcliffe S, Scarantino C, Ivker R, Roach M, Suh J, Peterson I, Konski A, Demas W, Bruner D. Functional interference clusters in cancer patients with bone metastases: A Secondary Analysis of RTOG 9714. Int J Radiat Oncol Biol Phys. E pub 24 July 2009.
Chow E, James J, Barsevick A, Hartsell W, Ratcliffe S, Scarantino C, Ivker R, Suh J, Peterson I, Konski A, Demas W, Bruner D. Confirmatory factor analysis of brief pain inventory (BPI) functional interference clustes in patients with bone metastases. J Pain Manage 2010; 3 (4).
Chung HT, Xia P, Chan L, Park-Somers E, Roach III, M. Does IGRT improve the toxicity profile in whole pelvic-treated high-risk prostate cancer? A comparison between IG-IMRT and IMRT. Int J Radiat Oncol Biol Phys 73(1):53-60 (2009).
Ciezki JP. Brachytherapy for Localized Prostate Cancer. Urology. 73(3):473-475, 2009.
Gerbi BJ, Antolak JA, Deibel FC. Followill DS, Herman MG, Higgins PD, Huq MS, Mihailidis DN, Yorke, ED. Recommendations for clinical electron beam dosimetry: supplement to the recommendations of Task Group 25. Med. Phys. 36, 3239-79 (2009).
Glinskii AB, Glinsky GV, Lin HY, Tang HY, Sun M, Davis FB, Luidens MK, Mousa SA, Hercbergs AH, Davis PJ. Modification of survival pathway gene expression in human breast cancer cells by tetraiodothyroacetic acid (tetrac). Cell Cycle. 2009 Nov 1;8(21) 3554-3562.
Hercbergs A, Davis PJ, Davis FB. Cieslieski M, and Leith JT. Radiosensitization of GL261 Glioma Cells by Tetrac (Tetraiodothyroacetic acid). Cell Cycle 2009 Aug 15; 8(16) 2586-2591
Hwang AB, Bacharach SL, Yom SS, Weinberg VK, Quivey JM, Franc BL, Xia P. Can PET or PET/CT Acquired in a Non-Treatment Position Be Accurately Registered to a Head and Neck Radiation Therapy Planning CT? Int J Radiat Oncol Biol Phys 73(2):578-84 (2009).
Koyfman SA, McCabe MS, Emanuel EJ, Grady, C. A Consent Form Template for Phase 1 Oncology Trials. IRB: Ethics & Human Research 31, No. 4 (2009): 1-8.
Khan MK, Hunter GK, Vogelbaum M, Suh JH, Chao ST. Evidence-Based Adjuvant Therapy for Gliomas: Current Concepts and Newer Developments. Indian J. Cancer. Apr-Jun:46(2);96-107, 2009.
Klein EA, Ciezki J, Kupelian PA, Mahadevan A. Outcomes for intermediate risk prostate cancer: are there advantages for surgery, external radiation, or brachytherapy? Urologic Oncology: Seminars and Original Investigations. 27(1): 671-71, 2009.
Lee N, Harris J, Garden AS, Straube W, Glisson BS, Xia P, Bosch W, Morrison WH, Quivey J, Thorstad W, Jones C, Ang KK. Intensity-Modulated Radiation Therapy with or without Chemotherapy for Nasopharyngeal Carcinoma: Radiation Therapy Oncology Group (RTOG) Phase II Trial 0225. J of Clinl Oncol, 27(22):3684-90 (2009).
Lin HY, Davis PJ, Tang HY, Mousa SA, Luidens MK, Hercbergs AH, Davis FB. The pro-apoptotic action of stilbene-induced COX-2 in cancer cells: Convergence with the anti-apoptotic effect of thyroid hormone. Cell Cycle 2009 June 15; 8 (12) 1877-1882.
Mackley HB, Adelstein JS, Reddy CA, Adelstein DJ, Rice TW, Saxton JP, Videtic GMM. Choice of Radiotherapy Planning Modality Influences Toxicity in the Treatment of Locally Advanced Esophageal Cancer. J Gastrointest Cancer. (published online May 1, 2009)
Mu G and Xia P. A Feasibility Study of Using Conventional Jaws to Deliver Complex IMRT Plans for Head and Neck Cancer. Phys Med Biol, 54 (18):5613-23 (2009).
RADIATIOn OnCOlOgy A Sampling of 2009 Journal Publications

Neznanov N, Gorbachev AA, Neznanova L, Komarov AP, Gurova KV, Gasparian AV, Banerjee AK, Almasan A, Fairchild RL, Andrei V. Gudkov AV (2009). Anti-malaria drug blocks proteotoxic stress response: anti-cancer implications. Cell Cycle. 2009 Dec;8(23):3960-70.
Platta CS, Khuntia D, Mehta, MP, Suh JH. Current Treatment Strategies for Brain Metastasis and Complications from Therapeutic Techniques: A Review of Current Literature. Am J Clin Oncol. (published online Aug 11, 2009)
Rosenberg LA, Prayson RA Lee J, Reddy C, Chao ST, Barnett GH, Vogelbaum MA, Suh JH. Long-term experience with World Health Organizations Grade III (Malignant) Meningiomas at a Single Institution. Int J Radiation Oncology Biol Phys., 74:427-432, 2009.
Serago CF, Adnani N, Bank MI, BenComo JA, Duan J, Fairobent L, Freedman DJ, Halvorsen PH, Hendee WR, Herman MG, Morse RK, Mower HW, Pfeiffer DE, Root WJ, Sherouse GW, Vossler MK, Wallace RE, Walters B. Code of Ethics for the American Association of Physicists in Medicine: Report of Task Group 109. Medical Physics 36:213-223, 2009.
Stephans KL, Reddy CA, Djemil T, Gajdos SM, Kolar M, Murthy S, Mason D, Mekhail T, Rice T, Videtic GMM. A Comparison of Two Stereotactic Body Radiation (SBRT) Fractionation Schedules for Medically Inoperable Stage I Non-Small Cell Lung Cancer (NSCLC): The Cleveland Clinic Experience. J Thorac Oncol 2009;4(8):976-982.
Stephans KL, Djemil T, Reddy C, Gajdos SM, Kolar M, Machuzak M, Mazzone P, Videtic GMM. Comprehensive Analysis of Pulmonary Function Test (PFT) Changes after Stereotactic Body Radiotherapy (SBRT) for Stage I Lung Cancer in Medically Inoperable Patients, J Thorac Oncol 2009; 4(7):838-844.
Stephenson AJ, Jones JS, Hernandez AV, Ciezki JP, Gong MC, Klein EA. Analysis of T1c Prostate Cancers Treated at Very Low Prostate-Specific Antigen Levels. European Urology. 5(3):610-616, 2009.
Stone NN, Potters L, Davis BJ, Ciezki JP, Zelefsky MJ, Roach M, Shinohara K, Fearn PA, Kattan MW, Stock RG. Multicenter Analysis of Effect of High Biologic Effective Dose on Biochemical Failure And Survival Outcomes In Patients With Gleason Score 7-10 Prostate Cancer Treated With Permanent Prostate Brachytherapy. Int. J. Radiat. Oncol. Biol. Phys. 73(2):341-346, 2009.
Suh JH, Chao ST, Vogelbaum MA. Management of brain metastases. Curr Neurol Neurosci Rep 9:223-230, 2009.
Tendulkar R, Obi B, Macklis R, Crowe R. Preoperative Breast Magnetic Resonance Imaging in Early Breast Cancer: Implications for Partial Breast Irradiation. Cancer 115(8):1621-30, 2009.
Videtic GMM, Reddy CA, Chao ST, Rice TW, Adelstein DJ, Barnett GH, Mekhail TM, Vogelbaum MA, Suh JH. Gender, race and survival: A study in non-small cell lung cancer brain metastases patients utilizing the RTOG RPA classification. Int J Radiat Oncol Biol. 15 November 2009 75(4): 1141-1147
Videtic GM, Gaspar L, Aref A, Germano I, Goldsmith B, Imperato J, Marcus K, McDermott M, McDonald M, Patchell R, Robins HI, Rogers CL, Suh JH, Wolfson A, Wippold FJ, Expert Panel on Radiation Oncology–Brain Metastases. American College of Radiology Appropriateness Criteria on Multiple Brain Metastases. Int J Radiat Oncol Biol Phys 15 November 2009:75 (4): 961-965.
Vitolo V, Millender LE, Quivey JM, Yom, SS, Schechter NR, Jereczek-Fossa BA, Milani F, Orecchia R, Xia P. Assessment of Carotid Artery Dose in the Treatment of Nasopharyngeal Cancer with IMRT Versus Conventional Radiotherapy. Radiother Oncol 90(2):213-20 (2009).
Vogelbaum MA, Berkey B, Peereboom D, Macdonald D, Giannini C, Suh JH, Jenkins R, Herman J, Brown P, Blumenthal DT, Biggs C, Schultz C, Mehta, M. Phase II Trial of Pre-Irradiation and Concurrent Temozolomide in Patients with Newly Diagnosed Anaplastic Oligodendrogliomas and Mixed Anaplastic Oligoastrocytomas: RTOG BR 0131. Neuro Oncol 2009: 11(2): 167-175, 2009.
Yalcin M, Bharali DJ, Lansing L, Dyskin E, Mousa SS, Hercbergs A, Davis FB, Davis PJ, Mousa SA. Tetraidthroacetic Acid (Tetrac) and Tetrac Nanoparticles Inhibit Growth of Human Renal Cell Carcinoma Xenografts. Anticancer Res 29: 3825-3832 (2009).
16 | 17 | clevelandclinic.org/cancerconsult

The Cleveland Clinic FoundationTaussig Cancer Institute9500 Euclid Avenue / AC311 Cleveland, OH 44195
S E R v I C E S F O R P h y S I C I A n S
Physician Directory View all Cleveland Clinic staff online at clevelandclinic.org/staff.
Physician liaison Referring physicians have a direct and personal link to Cleveland
Clinic with our Physician Liaison. For help with any interaction involving Cleveland
Clinic, contact Physician Liaison Kate Kenny at clevelandclinic.org/ContactKate.
Critical Care Transport worldwide Cleveland Clinic’s critical care transport team serves
critically ill and highly complex patients across the globe. The transport fleet comprises
mobile ICU vehicles, helicopters and fixed-wing aircraft. The transport teams are
staffed by physicians, critical care nurse practitioners, critical care nurses, paramedics
and ancillary staff, and are customized to meet the needs of the patient. Critical care
transport is available for children and adults.
To arrange a transfer for STEMI (ST elevated myocardial infarction), acute stroke, ICH
(intracerebral hemorrhage), SAH (subarachnoid hemorrhage) or aortic syndromes, call
877.279.CODE (2633).
For all other critical care transfers, call 216.444.8302 or 800.553.5056.
Track your Patient’s Care Online Whether you are referring from near or far,
DrConnect offers secure access to your patient’s treatment progress at Cleveland
Clinic. To establish a DrConnect account, visit clevelandclinic.org/drconnect or email
Remote Consults Request a remote medical second opinion from Cleveland Clinic.
MyConsult is particularly valuable for patients who wish to avoid the time and expense
of travel. Visit clevelandclinic.org/myconsult, email [email protected] or call
800.223.2273, ext 43223.
Outcomes Data Available The latest Outcomes book from Cleveland Clinic Taussig
Cancer Institute is available. Our Outcomes books contain clinical outcomes data and
information on volumes, innovations, research and publications. To view Outcomes
books for many Cleveland Clinic institutes, visit clevelandclinic.org/quality.
Taussig Cancer Institute Appointments/Referrals/Cancer Answer line
216.444.7923 or toll-free 866.223.8100
Bone Marrow Transplant Program Appointments/Referrals
216.445.5600 or 800.223.2273, ext. 55600
Bone Marrow Failure Clinic Appointments/Referrals
216.445.5962 or 800.223.2273, ext. 55962
Radiation Oncology Appointments/Referrals
216.444.5571 or 800.223.2273, ext. 45571
general Patient Referral 24/7 hospital
transfers or physician consults
800.553.5056
On the web at clevelandclinic.org/cancer
Stay Connected to Cleveland Clinic