Embed Size (px)
Citation preview

COIMMU-1189; NO. OF PAGES 9
Cancer immunotherapy strategies based on overcomingbarriers within the tumor microenvironmentThomas F Gajewski, Seng-Ryong Woo, Yuanyuan Zha,Robbert Spaapen, Yan Zheng, Leticia Corrales and Stefani Spranger
Available online at www.sciencedirect.com
For tumor antigen-specific T cells to effectively control the
growth of cancer cells in vivo, they must gain access to, and
function within, the tumor microenvironment. While tumor
antigen-based vaccines and T cell adoptive transfer strategies
can result in clinical benefit in a subset of patients, most of the
patients do not respond clinically. Even for tumor-infiltrating
lymphocyte (TIL)-based adoptive transfer for patients with
metastatic melanoma, which can provide tumor shrinkage in
around 50% of treated individuals, many patients are not
eligible, in part because there are not sufficient TIL present in
the resected tumor. Thus, the denominator is in fact larger, and
it has been suggested that absence of TIL may be a marker for
poor efficacy of immunotherapies in general. While qualitative
and/or quantitative features of the T cells are important
considerations for efficacy, a major component of primary
resistance likely can be attributed to the tumor
microenvironment. Data are accumulating suggesting that two
major categories of immune resistance within the tumor
microenvironment may exist: failure of T cell trafficking due to
low levels of inflammation and lack of chemokines for
migration, and dominant suppression through immune
inhibitory mechanisms. New therapeutic interventions are
being guided by these observations, and preliminary clinical
success is validating this working model.
Address
University of Chicago, United States
Corresponding author: Gajewski, Thomas F
Current Opinion in Immunology 2013, 25:xx–yy
This review comes from a themed issue on Cancer immunotherapy:
Clinical translation
Edited by Tom Gajewski and Ton Schumacher
0952-7915/$ – see front matter, Published by Elsevier Ltd.
http://dx.doi.org/10.1016/j.coi.2013.02.009
Introduction: probing the tumormicroenvironment as a predictive biomarkerfor clinical benefit from immunotherapyAnalysis of the tumor microenvironment in a systematic
fashion in patients began with the goal of identifying a
predictive biomarker associated with clinical benefit to
Please cite this article in press as: Gajewski TF, et al.: Cancer immunotherapy strategies based on
dx.doi.org/10.1016/j.coi.2013.02.009
www.sciencedirect.com
therapeutic cancer vaccines. The motivation for this pur-
suit was the observation that vaccine-induced immune
responses as measured in the peripheral blood did not
consistently correlate with anti-tumor activity. In fact, with
the most potent vaccine formulations, the majority of
patients indeed develop antigen-specific T cell responses,
yet only a minority of patients derive clinical benefit [1–4].
In addition, a subset of patients show pre-existing immune
responses against individual tumor antigens, yet they have
detectable growing metastatic disease. Collectively, these
observations pointed toward downstream resistance mech-
anisms at the level of the tumor microenvironment as a
potential explanation for tumor escape.
To begin to address this issue, we performed gene
expression profiling on pre-treatment biopsies from
patients participating in a peptide-based vaccine in
combination with IL-12. Patients were categorized as
having a favorable (CR + PR + SD) or unfavorable (PD)
clinical outcome, and supervised hierarchical clustering
was performed. This analysis revealed a small subset of
genes differentially expressed in the tumors between
these two patient populations. Interestingly, most of
these were genes encoding immunoregulatory factors,
including chemokines and evidence for the presence of
T cells at baseline [5,6]. A similar analysis was extended
to melanoma metastases from 44 additional patients,
which confirmed that this T cell-inflamed phenotype
was present in around 40% of patients [7�]. A similar
result has been observed in a MAGE-3-based vaccine
platform pursued by GSK-Bio, in which a similar T cell-
inflamed tumor microenvironment appeared to correlate
with clinical benefit from their vaccine [8,9]. Interestingly,
a small biomarker study also has been carried out with
melanoma patients being treated with the anti-CTLA-4
mAb ipilimumab. Part of that analysis included gene
expression profiling on pre-treatment biopsies which sim-
ilarly suggested the expression of T cell markers and
chemokine genes in patients who went on to derive clinical
benefit [10,11�]. Although these have all been small studies
and need to be validated prospectively, the results none-
theless suggest that patients in whom a ‘dialogue’ is already
established between the tumor and the host immune
response might be predisposed toward clinical benefit
from active immunization and also from CTLA-4
blockade. A corollary to this notion is that patients with
tumors that lack the ability to recruit activated T cells
may be resistant to these current immunotherapy
approaches [12].
overcoming barriers within the tumor microenvironment, Curr Opin Immunol (2013), http://
Current Opinion in Immunology 2013, 25:1–9
2 Cancer immunotherapy: Clinical translation
COIMMU-1189; NO. OF PAGES 9
Tumors lacking T cell-based inflammationmay require innate immune triggers topromote T cell traffickingA working model has emerged in which one might envi-
sion the need for a distinct set of immunotherapeutic
interventions dictated by the presence or absence of an
immune-permissive tumor microenvironment. Develop-
ing strategies for how to manipulate non-inflamed tumors
and render them permissive should benefit from a greater
understanding of how a spontaneous T cell response is
able to develop naturally in a subset of patients. Theor-
etically, in addition to the expression of (neo-)antigens
that can be recognized by T cells, the full activation of
such T cells would require innate immune signals that
serve as an endogenous ‘adjuvant’ and properly activate
antigen presenting cells (APCs). For melanoma, the pre-
sence of hundreds of point mutations in coding exons
[13], in addition to the expression of differentiation and
cancer-testis antigens that also have moderate immuno-
genicity, implies an abundance of potential antigens that
should not be rate-limiting. Therefore, it was hypothes-
ized that tumors that do indeed show a spontaneous T
cell-based inflammation may have been the ones that
Please cite this article in press as: Gajewski TF, et al.: Cancer immunotherapy strategies based on
dx.doi.org/10.1016/j.coi.2013.02.009
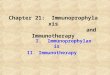
Figure 1
T cell-poor tumor
Reasons for imm
Therapeutic int
tumor cell stroma cell macrophage CD8 T ce
Innate immune activationStroma disruption
Manipulation of oncogene singaling pathway
Lack of innate immune activationLack of chemokines
Dense stromaImmunosuppressive oncogene expression
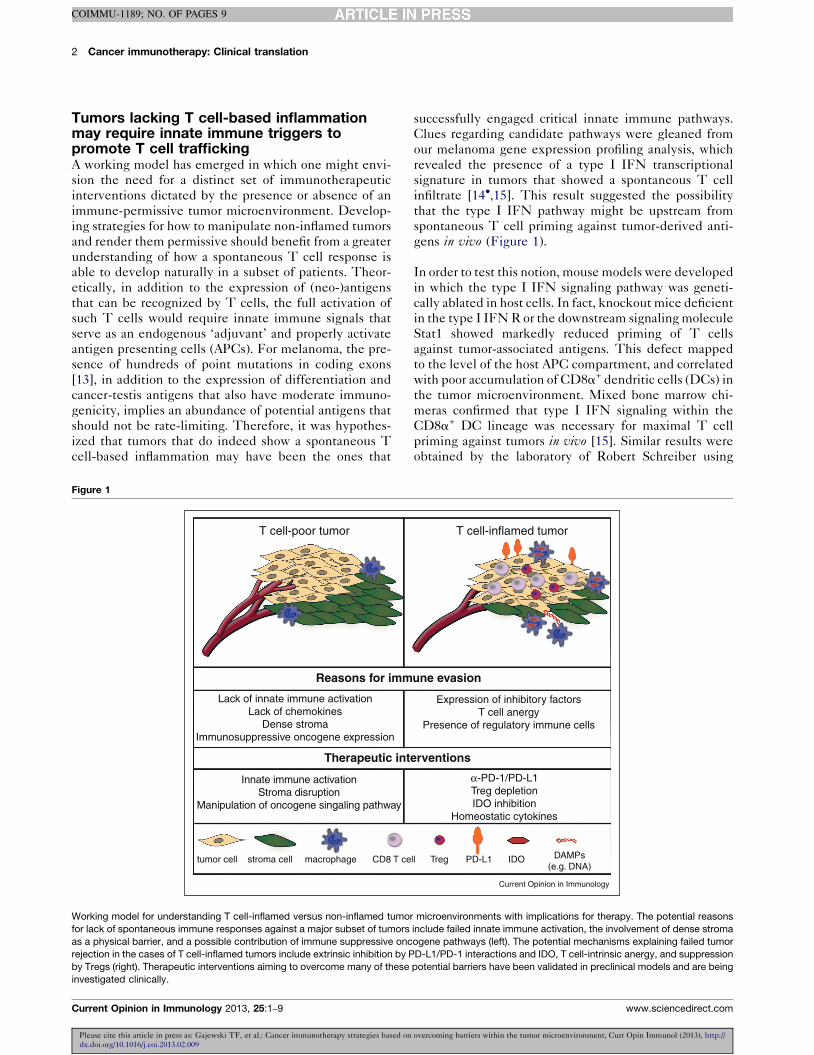
Working model for understanding T cell-inflamed versus non-inflamed tumo
for lack of spontaneous immune responses against a major subset of tumors
as a physical barrier, and a possible contribution of immune suppressive onc
rejection in the cases of T cell-inflamed tumors include extrinsic inhibition by P
by Tregs (right). Therapeutic interventions aiming to overcome many of these
investigated clinically.
Current Opinion in Immunology 2013, 25:1–9
successfully engaged critical innate immune pathways.
Clues regarding candidate pathways were gleaned from
our melanoma gene expression profiling analysis, which
revealed the presence of a type I IFN transcriptional
signature in tumors that showed a spontaneous T cell
infiltrate [14�,15]. This result suggested the possibility
that the type I IFN pathway might be upstream from
spontaneous T cell priming against tumor-derived anti-
gens in vivo (Figure 1).
In order to test this notion, mouse models were developed
in which the type I IFN signaling pathway was geneti-
cally ablated in host cells. In fact, knockout mice deficient
in the type I IFN R or the downstream signaling molecule
Stat1 showed markedly reduced priming of T cells
against tumor-associated antigens. This defect mapped
to the level of the host APC compartment, and correlated
with poor accumulation of CD8a+ dendritic cells (DCs) in
the tumor microenvironment. Mixed bone marrow chi-
meras confirmed that type I IFN signaling within the
CD8a+ DC lineage was necessary for maximal T cell
priming against tumors in vivo [15]. Similar results were
obtained by the laboratory of Robert Schreiber using
overcoming barriers within the tumor microenvironment, Curr Opin Immunol (2013), http://
T cell-inflamed tumor
une evasion
erventions
ll Treg PD-L1 IDO
α-PD-1/PD-L1Treg depletionIDO inhibition
Homeostatic cytokines
Expression of inhibitory factorsT cell anergy
Presence of regulatory immune cells
DAMPs(e.g. DNA)
Current Opinion in Immunology
r microenvironments with implications for therapy. The potential reasons
include failed innate immune activation, the involvement of dense stroma
ogene pathways (left). The potential mechanisms explaining failed tumor
D-L1/PD-1 interactions and IDO, T cell-intrinsic anergy, and suppression
potential barriers have been validated in preclinical models and are being
www.sciencedirect.com

Modulation of the tumor microenvironment Gajewski et al. 3
COIMMU-1189; NO. OF PAGES 9
completely different model systems [16�]. In those stu-
dies, conditional deletion of the type I IFN R in the
CD11chi compartment also led to poor spontaneous T cell
priming.
If host type I IFN production is critical as part of innate
immune recognition of tumors in vivo, then what is the
major receptor and signaling pathway that drives this
production, and what are the tumor-derived factors that
are sensed by host cells to induced type I IFNs? Several
key pathways have been defined and/or implicated, large-
ly based on pathogen models. These include toll-like
receptors that signal through MyD888 or Trif, cytosolic
RNA sensing via RIG-I and IPS-1, extracellular ATP
sensing through P2X7R, and cytosolic DNA sensing via
p204/IFI16 that forms a complex with STING and leads
to TBK1 activation, IRF3/7 phosphorylation and nuclear
translocation, and IFN-b gene transcription [15,17,18��].Using knockout mice deficient in MyD88, Trif, IPS-1, or
P2X7R we found no evidence for blunting of spontaneous
CD8+ T cell responses against tumor-associated antigens
in vivo. However, STING�/� mice showed a profound
deficiency in the induction of anti-tumor T cell responses
in vivo (Woo and Gajewski, unpublished observations).
These results suggest the possibility that tumor-derived
DNA, presumably liberated from dying tumor cells much
like protein antigens that become cross-presented, might
drive productive APC activation in vivo [19,20]. The
mechanisms of this effect are currently being elucidated.
This model is attractive as it has overlap with the mech-
anisms of induction of some types of autoimmunity such
as lupus, which also involve type I IFNs [21–23].
During the course of these experiments, components of
the inflammasome pathways [24] also have been inter-
rogated. Interestingly, preliminary evidence using in vitromodels has indicated that APCs deficient in specific
inflammasome proteins (e.g. the adapter ASC) show
markedly augmented IFN-b production (Corrales and
Gajewski, unpublished observation). As earlier data had
indicated that type I IFNs could inhibit the inflamma-
some [25�], these results suggest the possibility of a
mutual counter-regulatory loop between the STING
pathway and the inflammasome. The possibility that
negative regulation by components of the inflammasome
or other innate cell-expressed regulatory proteins might
restrict anti-tumor immunity in vivo is currently being
examined.
Together, these observations suggest the possibility that a
major subset of tumors might lack appropriate signals for
innate immune activation that would include type I IFN
production. Therefore, strategies to promote robust
innate signaling via APCs and/or other stromal cells in
the tumor microenvironment might facilitate improved
cross-priming of tumor antigen-specific CD8+ T cells and
also augment chemokine production for subsequent
Please cite this article in press as: Gajewski TF, et al.: Cancer immunotherapy strategies based on
dx.doi.org/10.1016/j.coi.2013.02.009
www.sciencedirect.com
effector T cell trafficking, and as a result lead to improved
tumor control. Several such strategies have been explored
in preclinical models and some are being investigated
clinically. The provision of TLR agonists in the tumor
microenvironment, or intratumoral introduction of type I
IFNs, appears to be capable of facilitating chemokine
production and desirable inflammation in the tumor site.
The TNF superfamily member LIGHT can engage the
LTbR on stromal cells and induce chemokine pro-
duction, T cell trafficking, and tumor rejection in vivo[26–28]. Interestingly, high-dose radiation to the tumor
site also appears to induce type I IFN production and to
promote T cell-mediated tumor control [29]. Ultimately,
strategies to increase the frequency of tumor antigen-
specific T cells (such as vaccines) in combination with
interventions to promote improved T cell trafficking into
the tumor microenvironment, will be attractive to pursue
in patients.
One additional consideration for the T cell-poor subset of
tumors is whether lack of T cell-based inflammation
might be explained by the presence of dense sessile
stroma. Evidence suggests that the T cell-poor subset
of tumors may express higher levels of pro-angiogenic
factors. Coukos and colleagues performed gene expres-
sion profiling of vascular endothelial cells in the ovarian
cancer tumor microenvironment and found distinct phe-
notypes associated with the presence or absence of a T
cell infiltrate [30,31]. One of these endothelial cell gene
products, the endothelin B receptor, could be manipu-
lated towards improved T cell trafficking. A high density
of fibroblasts, tumor-supporting macrophages, and extra-
cellular matrix may restrict T cell access. Hans Schrei-
ber’s laboratory has pursued a line of experimentation
demonstrating that tumor cells established in stroma are
much more difficult to reject immunologically as com-
pared to a poorly established tumor cell suspension in
mouse models [32,33]. Interestingly, it may be feasible to
manipulate the stromal composition in solid tumors. In a
pancreatic cancer context, Vonderheide and colleagues
have reported that an agonistic anti-CD40 antibody could
activate macrophages that enter the tumor microenviron-
ment and render the tumors more responsive to che-
motherapy [34]. Whether anti-CD40 may also improve
the effector phase of an anti-tumor T cell response is
actively being investigated.
The underlying molecular mechanisms that explain lack
of spontaneous immune priming and T cell infiltration in
a major subset of melanomas in unclear, but several
hypotheses are being interrogated. This ultimately
becomes a question of inter-patient heterogeneity. First,
it is now apparent that the permutations of oncogenic
signaling pathways that are activated in tumors are not
identical between individual patients, and it is concei-
vable that depending on the given constellation of
mutations, signals that suppress or enhance expression
overcoming barriers within the tumor microenvironment, Curr Opin Immunol (2013), http://
Current Opinion in Immunology 2013, 25:1–9

4 Cancer immunotherapy: Clinical translation
COIMMU-1189; NO. OF PAGES 9
of immune regulatory genes within the cancer cells may
vary. For example, activated Stat3 has been shown to
block chemokine expression in tumor cell lines [35,36]. If
such pathways are identified then perhaps they could be
targeted with specific inhibitors, so that a dialogue be-
tween the tumor and the host immune response can
become established. Second, it is possible that germline
polymorphisms (presumably in immune regulatory
genes) might regulate thresholds for activation of innate
or adaptive immune cells and thus lead to failure of
spontaneous T cell priming against tumor antigens.
The first example of a gene polymorphism linked to
response to an immunotherapy is the association of a
CCR5 polymorphism with clinical response to high-dose
IL-2 [37]. Interventions that augment activation of rate-
limiting immune activation events governed by these
polymorphisms could then be considered. Third, it is
conceivable that environmental differences may be oper-
ational between patients, in ways that influence systemic
immune capacity. Differences in the composition of
commensal flora have been shown to exert profound
effects on systemic immune responses and the incidence
of autoimmunity [38��]. In addition, exposure to CMV
and the accumulation of high frequencies of CMV-
specific effector/memory CD8+ T cells has been shown
to be associated with poor induction of immune responses
against tumor antigens following active immunization
[39]. If such observations become linked to the apparent
lack of spontaneous anti-tumor immunity in patients,
then manipulation of these immunologically relevant
environmental exposures may become critical.
Tumors that support T cell trafficking appearto show high expression of immunesuppressive pathways that can be targetedtherapeuticallyIf a subset of tumors does indeed support endogenous T
cell priming all the way through to migration of activated
CD8+ effector cells into a chemokine-rich tumor micro-
environment, then it may seem paradoxical that those
tumors exist at all and are not rejected spontaneously by
the host. However, several small functional studies of T
cells isolated from the melanoma tumor microenviron-
ment have suggested that those specific for tumor anti-
gens appear to be hyporesponsive [40–42]. Interestingly,
virus-specific T cells isolated from tumor sites (which are
probably passenger effector cells transiting along chemo-
kine gradients) can be functional, arguing for an antigen-
specific component to this dysfunction [40]. Interrogation
of melanoma metastases by gene expression profiling and
confirmatory assays for candidate immune inhibitory
mechanisms has provided correlative evidence for invol-
vement of at least four important suppressive pathways:
expression of PD-L1/B7-H1, expression of indoleamine-
2,3-dioxygenase (IDO), the presence of infiltrating
CD4+CD25+FoxP3+ regulatory T cells (Tregs), and T
cell-intrinsic anergy [43]. PD-L1/B7-H1 engages the
Please cite this article in press as: Gajewski TF, et al.: Cancer immunotherapy strategies based on
dx.doi.org/10.1016/j.coi.2013.02.009
Current Opinion in Immunology 2013, 25:1–9
inhibitory receptor PD-1 on activated T cells, which
diminishes T cell function [44��]. A large fraction of
TIL expresses PD-1 [45,46], arguing for functional
relevance of this pathway in the tumor microenviron-
ment. IDO is a tryptophan-catabolizing enzyme that was
originally identified as one of the factors involved in
immunologic tolerance at the maternal-fetal interface
[47]. It metabolizes tryptophan to kynurenine, thereby
reducing tryptophan availability and also promoting cel-
lular stress to which T cells are quite sensitive [48]. Tregs
have been shown to increase in number in many cancer
patients and also to be present in tumor sites [49,50].
Anergy is a T cell-intrinsic dysfunctional state that gener-
ally results when the T cell receptor for antigen (TCR) is
ligated in the absence of important costimulatory signals,
most importantly through CD28. The APCs in the tumor
microenvironment, as well as the tumor cells themselves,
usually show low expression of the CD28 ligands B7-1
(CD80) and B7-2 (CD86), arguing in favor of an anergy-
promoting context. We recently have identified the tran-
scription factor EGR2 as a critical regulator of the anergic
phenotype [51]. Conditional ablation of EGR2 in T cells
led to improved immune-mediated tumor control in vivo[51]. Preliminary data have indicated that many CD8+ T
cells infiltrating human melanomas are EGR2+, providing
more direct evidence for a functional contribution of T
cell anergy in tumor immune escape.
Preclinical models of anti-tumor immunity have been
utilized to investigate the therapeutic potential for strat-
egies to interfere with (or reverse) each of these immune
inhibitory pathways. Blocking mAbs against PD-L1, or
the use of PD-1-deficient T cells, can potentiate immune-
mediated tumor control, in some of the models resulting
in complete tumor rejection [52–54]. Small molecule
inhibitors of IDO enzymatic activity can slow tumor
growth in a T cell-dependent fashion [55,56]. Depletion
of Tregs has been achieved either by administering anti-
CD25 mAbs or the use of an IL-2-diptheria toxin fusion
protein, or by ex vivo depletion from T cells with anti-
CD25 beads before adoptive transfer [57–59]. Each of
these can partially control tumor growth in various models
in vivo. For T cell anergy, it had been shown that
transfection of tumor cells to express B7-1 could support
rejection of tumors that normally grow progressively [60–62]. However, this approach has been less effective with
established tumors [63]. Alternatively, reversal of anergy
in vitro can be achieved using cytokines that promote T
cell proliferation via utilization of the gc-containing cyto-
kine receptors [64]. In vivo, the homeostatic cytokines IL-
7 and IL-15 also can have therapeutic activity in tumor
models [65–67], as can adoptive transfer of T cells into
lymphopenic recipients which have liberation of
endogenous IL-7 and IL-15 [59,68–71].
Clinical trials manipulating each of the above immune
inhibitory mechanisms have been initiated in advanced
overcoming barriers within the tumor microenvironment, Curr Opin Immunol (2013), http://
www.sciencedirect.com

Modulation of the tumor microenvironment Gajewski et al. 5
COIMMU-1189; NO. OF PAGES 9
cancer patients. Arguably the farthest along in clinical
development is the investigation of mAbs that target the
PD-1/PD-L1 axis. Topalian and colleagues recently
reported the results of a phase I/II clinical trial of the
anti-PD-1 mAb developed by Medarex/BMS. A 28%
response rate was observed among the 95 melanoma
patients treated on this study, with many of these
responses being quite durable [72]. Similarly encouraging
results have been reported with an anti-PD-L1 mAb [73].
Preliminary biomarker investigation has suggested that
clinical benefit might be preferentially seen in the subset
of patients having PD-L1 expression and a T cell infil-
trate in the tumor site, arguing again that a T cell-
inflamed tumor microenvironment might serve as a
relevant predictive biomarker. IDO inhibition is being
pursued using small molecule inhibitors. A potent com-
pound developed by Incyte has progressed through phase
I clinical testing and biologically active doses that reverse
the tryptophan/kynurenine ratio have been established.
Phase II studies with this drug have been initiated.
Manipulation of Tregs has largely been attempted via
targeting of CD25. Denileukin diftitox, an IL-2-diptheria
toxin fusion protein, was originally developed as a treat-
ment for CD25+ cutaneous T cell lymphoma [74]. Partial
depletion of Tregs in cancer patients has been seen in
some of the studies, with clinical responses in melanoma
and improved immunogenicity of some vaccines reported
[75–77]. However, not all studies have noted a decrease in
Treg numbers with this approach [78] and the reasons for
differential outcomes are not yet clear. An anti-human
CD25 mAb has also been shown to reduce circulating
Treg numbers in cancer patients [79], and further work
with such Abs is ongoing. Administration of homeostatic
cytokines that may support T cell proliferation and
uncoupling of anergy (in addition to general T cell
expansion) is beginning to be explored. Phase I testing
of IL-7 has identified safe doses that successfully aug-
ment T cell numbers in patients [80,81]. Clinical grade
IL-15 has been produced by the NCI and a phase I study
of intravenous administration has been pursued [82].
While IL-2-like side effects have been observed, T cell
expansion has also been noted. A subcutaneous dose and
schedule also is being evaluated. Interestingly, a phase II
study of IL-21 in melanoma patients has been reported,
and a 22% clinical response rate was observed [83,84].
The mechanism of clinical activity remains to be deter-
mined, but could involve maintenance of anti-tumor T
cell function.
In preclinical models, adoptive transfer of tumor-reactive
T cells into lymphopenic recipients can support homeo-
static proliferation and improved tumor control in vivo[59,68]. This phenomenon occurs through the liberation
of endogenous IL-7 and IL-15, which in turn is capable of
reversing established T cell anergy [70]. It is attractive to
speculate that the successful utilization of lymphopenia-
inducing conditioning regimens for T cell adoptive
Please cite this article in press as: Gajewski TF, et al.: Cancer immunotherapy strategies based on
dx.doi.org/10.1016/j.coi.2013.02.009
www.sciencedirect.com
therapy in melanoma patients may, in part, be attributed
to prevention of anergy induction [85,86].
In addition to the inhibitory receptor PD-1 that can blunt
the function of tumor-infiltrating T cells, other negative
pathways have been identified that also appear to be
functionally relevant. Characterization of the EGR2 tran-
scriptome in T cell anergy has identified LAG-3 as one
important target gene (Zheng and Gajewski, unpublished
data). Analysis of tumor-infiltrating T cells has confirmed
the presence of LAG-3 on a major subset, and this re-
ceptor may mark the intrinsically dysfunctional anergic
subpopulation [87,88]. Tim-3 is another inhibitory re-
ceptor that has been shown to be expressed on a subset
of tumor-reactive T cells, both in murine and human
models, and also may mark a dysfunctional subset [89,90].
Blockade of either LAG-3 or Tim-3 has also been shown
to improve the function of anti-tumor T cells in different
model systems, providing a strong rationale for clinical
development of agents targeting these molecules as
immunotherapeutics.
An important consideration for blockade of immune
suppressive pathways is the fact that multiple inhibitory
mechanisms appear to be functioning in concert to shut
down specific T cells in the tumor microenvironment.
Thus, blockade of two or more pathways simultaneously
may be necessary for maximal clinical benefit. Preclinical
data have already shown marked synergy between Treg
depletion and homeostatic proliferation for anergy rever-
sal [59], as well as combined blockade of PD-1 and either
Tim-3 or LAG-3 [90,91]. Preliminary data have addition-
ally suggested synergy between anti-CTLA-4 mAb and
either anti-PD-L1 mAb or IDO inhibition (Spranger and
Gajewski, unpublished observations). Combinations of
anti-CTLA-4 or anti-PD-L1 and strategies to ligate
positive costimulatory receptors, including 4-1BB, also
have been observed to support improved tumor control
preclinically [92]. Therefore, clinical testing of combi-
nation immunotherapies should receive a high priority.
Conclusions and future directionsIncreasing our understanding of the tumor microenviron-
ment has provided a foundation for the rational devel-
opment of immunotherapeutic approaches for the
treatment of cancer. As a T cell-inflamed tumor micro-
environment may be a relevant predictive biomarker for
clinical benefit, novel approaches to induce this pheno-
type as a therapeutic strategy should be pursued. Proof-
of-concept approaches in preclinical models have largely
been evaluated using intratumoral injection, which will
not likely be practical for patients with metastatic cancer.
Therefore, a challenge will be devising technologies for
systemic administration of agents that selectively home to
tumor sites. One attractive approach is the use of tumor-
targeting mAbs that could be coupled with a payload of an
immunomodulatory factor, much in the way cytotoxic
overcoming barriers within the tumor microenvironment, Curr Opin Immunol (2013), http://
Current Opinion in Immunology 2013, 25:1–9

6 Cancer immunotherapy: Clinical translation
COIMMU-1189; NO. OF PAGES 9
chemotherapeutics have been conjugated to Abs against
HER2 or CD33 [93,94]. While the predictive biomarker
potential of a T cell-inflamed tumor microenvironment
has largely been evaluated in melanoma, it is important to
note that a similar phenotype has been reported in a
variety of solid tumors, including colorectal cancer, renal
cell carcinoma, non-small cell lung cancer, breast cancer,
and ovarian cancer [95,96]. As such, it is an attractive
hypothesis to consider that clinical benefit with immu-
notherapeutic agents might also be observed in the subset
of metastatic patients having this phenotype in other
cancer histologies besides melanoma. While the current
clinical successes with anti-CTLA-4 [97�] and anti-PD-1
[72] mAbs rely on the endogenous T cell response and
what is likely spontaneous T cell priming against tumor
antigens, deliberate increase of anti-tumor T cell fre-
quencies could theoretically act in synergy with blockade
of these or other inhibitory pathways. Thus, combination
studies with potent vaccines or adoptive T cell therapy
should be considered. Finally, while many patients who
show a clinical response to immunotherapies have a
durable clinical benefit, recurrence or progression is none-
theless frequently observed. Understanding the mechan-
isms of secondary resistance ultimately will be critical, in
order to develop the next set of therapeutic to overcome
new barriers that may arise as a result of potent immune
selective pressure.
AcknowledgmentsData discussed in this review were supported by R01CA161005,R01CA127475, R01CA118153, P01CA97296, and the Melanoma ResearchAlliance. Through the course of this work, the authors have appreciated thetechnical support of Michael Leung, Michelle Gao, and Glee Li, as well asinfrastructure support through multiple University of ChicagoComprehensive Cancer Center shared resources (Human ImmunologicMonitoring and cGMP facilities, Functional Genomics Facility, HumanTissue Resource, and Flow Cytometry Facility).
References and recommended readingPapers of particular interest, published within the period of review,have been highlighted as:
� of special interest�� of outstanding interest
1. Peterson AC, Harlin H, Gajewski TF: Immunization with Melan-Apeptide-pulsed peripheral blood mononuclear cells plusrecombinant human interleukin-12 induces clinical activityand T-cell responses in advanced melanoma. J Clin Oncol2003, 21:2342-2348.
2. Fourcade J, Kudela P, Andrade Filho PA, Janjic B, Land SR,Sander C, Krieg A, Donnenberg A, Shen H, Kirkwood JM et al.:Immunization with analog peptide in combination with CpGand montanide expands tumor antigen-specific CD8+ T cellsin melanoma patients. J Immunother 2008, 31:781-791.
3. Adams S, O’Neill DW, Nonaka D, Hardin E, Chiriboga L, Siu K,Cruz CM, Angiulli A, Angiulli F, Ritter E et al.: Immunization ofmalignant melanoma patients with full-length NY-ESO-1protein using TLR7 agonist imiquimod as vaccine adjuvant. JImmunol 2008, 181:776-784.
4. Rosenberg SA, Yang JC, Schwartzentruber DJ, Hwu P,Marincola FM, Topalian SL, Restifo NP, Dudley ME, Schwarz SL,Spiess PJ et al.: Immunologic and therapeutic evaluation of asynthetic peptide vaccine for the treatment of patients withmetastatic melanoma [see comments]. Nat Med 1998, 4:321-327.
Please cite this article in press as: Gajewski TF, et al.: Cancer immunotherapy strategies based on
dx.doi.org/10.1016/j.coi.2013.02.009
Current Opinion in Immunology 2013, 25:1–9
5. Gajewski TF, Meng Y, Harlin H: Chemokines expressed inmelanoma metastases associated with T cell infiltration. 2007ASCO Annual Meeting Proceedings Part I. J Clin Oncol 2007,25:8501.
6. Gajewski TF, Zha Y, Thurner B, Schuler G: Association of geneexpression profile in melanoma and survival to a dendritic cell-based vaccine. J Clin Oncol 2009, 27:9002.
7.�
Harlin H, Meng Y, Peterson AC, Zha Y, Tretiakova M, Slingluff C,McKee M, Gajewski TF: Chemokine expression in melanomametastases associated with CD8+ T-cell recruitment. CancerRes 2009, 69:3077-3085.
This study identified T cell-inflamed melanoma tumor microenvironmentcharacterized by expression of chemokines and other immunomodula-tory genes.
8. Louahed J, Gruselle O, Gaulis S, Coche T, Eggermont AM, Kruit W,Dreno B, Charion Sileni V, Lehmann F, Brichard VG: Expression ofdefined genes identified by pre-treatment tumor profiling:association with clinical responses to the GSK MAGE-A3immunotherapeutic in metastatic melanoma patients. J ClinOncol 2008, 26 (Abstract 9045).
9. Gajewski TF, Louahed J, Brichard VG: Gene signature inmelanoma associated with clinical activity: a potential clue tounlock cancer immunotherapy. Cancer J 2010, 16:399-403.
10. Hamid O, Schmidt H, Nissan A, Ridolfi L, Aamdal S, Hansson J,Guida M, Hyams DM, Gomez H, Bastholt L et al.: A prospectivephase II trial exploring the association between tumormicroenvironment biomarkers and clinical activity ofipilimumab in advanced melanoma. J Transl Med 2011, 9:204.
11.�
Ji RR, Chasalow SD, Wang L, Hamid O, Schmidt H, Cogswell J,Alaparthy S, Berman D, Jure-Kunkel M, Siemers NO et al.: Animmune-active tumor microenvironment favors clinicalresponse to ipilimumab. Cancer Immunol Immunother 2011,61:1019-1031.
This study provided evidence that melanomas with a pre-inflamed tumormicroenvironment may be associated with clinical benefit from anti-CTLA-4 mAb therapy.
12. Gajewski TF: Molecular profiling of melanoma and theevolution of patient-specific therapy. Semin Oncol 2011,38:236-242.
13. Pleasance ED, Cheetham RK, Stephens PJ, McBride DJ,Humphray SJ, Greenman CD, Varela I, Lin ML, Ordonez GR,Bignell GR et al.: A comprehensive catalogue of somaticmutations from a human cancer genome. Nature 2010,463:191-196.
14.�
Fuertes MB, Kacha AK, Kline J, Woo SR, Kranz DM, Murphy KM,Gajewski TF: Host type I IFN signals are required for antitumorCD8+ T cell responses through CD8alpha+ dendritic cells. JExp Med 2011.
See ref. [11�]
15. Fuertes MB, Woo SR, Burnett B, Fu YX, Gajewski TF: Type Iinterferon response and innate immune sensing of cancer.Trends Immunol 2012, 34:67-73.
16.�
Diamond MS, Kinder M, Matsushita H, Mashayekhi M, Dunn GP,Archambault JM, Lee H, Arthur CD, White JM, Kalinke U et al.:Type I interferon is selectively required by dendritic cells forimmune rejection of tumors. J Exp Med 2011, 208:1989-2003.
The above studies identified a key role for host type I IFN signaling viadendritic cells as a critical step in the generation of a natural T cellresponse against tumors in vivo.
17. Barber GN: Innate immune DNA sensing pathways: STING,AIMII and the regulation of interferon production andinflammatory responses. Curr Opin Immunol 2011, 23:10-20.
18.��
Ishikawa H, Ma Z, Barber GN: STING regulates intracellularDNA-mediated, type I interferon-dependent innate immunity.Nature 2009, 461:788-792.
This landmark paper identified the molecule STING as a critical partici-pant in the cytosolic DNA sensing pathway in innate immune recognition.
19. Unterholzner L, Keating SE, Baran M, Horan KA, Jensen SB,Sharma S, Sirois CM, Jin T, Latz E, Xiao TS et al.: IFI16 is an innateimmune sensor for intracellular DNA. Nat Immunol 2010,11:997-1004.
overcoming barriers within the tumor microenvironment, Curr Opin Immunol (2013), http://
www.sciencedirect.com

Modulation of the tumor microenvironment Gajewski et al. 7
COIMMU-1189; NO. OF PAGES 9
20. Holm CK, Jensen SB, Jakobsen MR, Cheshenko N, Horan KA,Moeller HB, Gonzalez-Dosal R, Rasmussen SB, Christensen MH,Yarovinsky TO et al.: Virus-cell fusion as a trigger of innateimmunity dependent on the adaptor STING. Nat Immunol 2012,13:737-743.
21. Niewold TB, Hua J, Lehman TJ, Harley JB, Crow MK: High serumIFN-alpha activity is a heritable risk factor for systemic lupuserythematosus. Genes Immun 2007, 8:492-502.
22. Gall A, Treuting P, Elkon KB, Loo YM, Gale M Jr, Barber GN,Stetson DB: Autoimmunity initiates in nonhematopoietic cellsand progresses via lymphocytes in an interferon-dependentautoimmune disease. Immunity 2012, 36:120-131.
23. Ahn J, Gutman D, Saijo S, Barber GN: STING manifests self DNA-dependent inflammatory disease. Proc Natl Acad Sci U S A2012, 109:19386-19391.
24. Rathinam VA, Vanaja SK, Fitzgerald KA: Regulation ofinflammasome signaling. Nat Immunol 2012, 13:332-333.
25.�
Guarda G, Braun M, Staehli F, Tardivel A, Mattmann C, Forster I,Farlik M, Decker T, Du Pasquier RA, Romero P et al.: Type Iinterferon inhibits interleukin-1 production and inflammasomeactivation. Immunity 2011, 34:213-223.
This report characterized a cross-inhibitory mechanism between twoinnate immune pathways: the inflammasome and type I IFNs.
26. Yu P, Lee Y, Liu W, Chin RK, Wang J, Wang Y, Schietinger A,Philip M, Schreiber H, Fu YX: Priming of naive T cells insidetumors leads to eradication of established tumors. NatImmunol 2004, 5:141-149.
27. Yu P, Lee Y, Wang Y, Liu X, Auh S, Gajewski TF, Schreiber H,You Z, Kaynor C, Wang X et al.: Targeting the primary tumor togenerate CTL for the effective eradication of spontaneousmetastases. J Immunol 2007, 179:1960-1968.
28. Oh SS, Moon C, Kim DH, Song H, Park S, Fu Y, Kim KD:Adenovirally delivered IFN-beta exerts antitumor effectsthrough transient T-lymphocyte depletion and Ag-specific T-cell proliferation. Int J Mol Med 2012, 29:1153-1157.
29. Burnette BC, Liang H, Lee Y, Chlewicki L, Khodarev NN,Weichselbaum RR, Fu YX, Auh SL: The efficacy of radiotherapyrelies upon induction of type i interferon-dependent innate andadaptive immunity. Cancer Res 2011, 71:2488-2496.
30. Buckanovich RJ, Facciabene A, Kim S, Benencia F, Sasaroli D,Balint K, Katsaros D, O’Brien-Jenkins A, Gimotty PA, Coukos G:Endothelin B receptor mediates the endothelial barrier to Tcell homing to tumors and disables immune therapy. Nat Med2008, 14:28-36.
31. Motz GT, Coukos G: The parallel lives of angiogenesis andimmunosuppression: cancer and other tales. Nat Rev Immunol2011, 11:702-711.
32. Singh S, Ross SR, Acena M, Rowley DA, Schreiber H: Stroma iscritical for preventing or permitting immunological destructionof antigenic cancer cells. J Exp Med 1992, 175:139-146.
33. Zhang B, Zhang Y, Bowerman NA, Schietinger A, Fu YX,Kranz DM, Rowley DA, Schreiber H: Equilibrium between hostand cancer caused by effector T cells killing tumor stroma.Cancer Res 2008, 68:1563-1571.
34. Beatty GL, Chiorean EG, Fishman MP, Saboury B, Teitelbaum UR,Sun W, Huhn RD, Song W, Li D, Sharp LL et al.: CD40 agonistsalter tumor stroma and show efficacy against pancreaticcarcinoma in mice and humans. Science 2011, 331:1612-1616.
35. Niu G, Heller R, Catlett-Falcone R, Coppola D, Jaroszeski M,Dalton W, Jove R, Yu H: Gene therapy with dominant-negativeStat3 suppresses growth of the murine melanoma B16 tumorin vivo. Cancer Res 1999, 59:5059-5063.
36. Burdelya L, Kujawski M, Niu G, Zhong B, Wang T, Zhang S,Kortylewski M, Shain K, Kay H, Djeu J et al.: Stat3 activity inmelanoma cells affects migration of immune effector cells andnitric oxide-mediated antitumor effects. J Immunol 2005,174:3925-3931.
37. Ugurel S, Schrama D, Keller G, Schadendorf D, Brocker EB,Houben R, Zapatka M, Fink W, Kaufman HL, Becker JC: Impact of
Please cite this article in press as: Gajewski TF, et al.: Cancer immunotherapy strategies based on
dx.doi.org/10.1016/j.coi.2013.02.009
www.sciencedirect.com
the CCR5 gene polymorphism on the survival of metastaticmelanoma patients receiving immunotherapy. Cancer ImmunolImmunother 2008, 57:685-691.
38.��
Wu HJ, Ivanov II, Darce J, Hattori K, Shima T, Umesaki Y,Littman DR, Benoist C, Mathis D: Gut-residing segmentedfilamentous bacteria drive autoimmune arthritis via T helper 17cells. Immunity 2010, 32:815-827.
This paradigm-shifting study demonstrated that commensal flora couldinfluence a systemic immune response, in this case an autoimmunemodel of arthritis.
39. Solana R, Tarazona R, Aiello AE, Akbar AN, Appay V, Beswick M,Bosch JA, Campos C, Cantisan S, Cicin-Sain L et al.: CMV andimmunosenescence: from basics to clinics. Immun Ageing2012, 9:23.
40. Harlin H, Kuna TV, Peterson AC, Meng Y, Gajewski TF: Tumorprogression despite massive influx of activated CD8(+) T cellsin a patient with malignant melanoma ascites. Cancer ImmunolImmunother 2006, 55:1185-1197.
41. Mortarini R, Piris A, Maurichi A, Molla A, Bersani I, Bono A,Bartoli C, Santinami M, Lombardo C, Ravagnani F et al.: Lack ofterminally differentiated tumor-specific CD8+ T cells at tumorsite in spite of antitumor immunity to self-antigens in humanmetastatic melanoma. Cancer Res 2003, 63:2535-2545.
42. Appay V, Jandus C, Voelter V, Reynard S, Coupland SE, Rimoldi D,Lienard D, Guillaume P, Krieg AM, Cerottini JC et al.: Newgeneration vaccine induces effective melanoma-specificCD8+ T cells in the circulation but not in the tumor site. JImmunol 2006, 177:1670-1678.
43. Gajewski TF: Failure at the effector phase: immune barriers atthe level of the melanoma tumor microenvironment. ClinCancer Res 2007, 13:5256-5261.
44.��
Dong H, Strome SE, Salomao DR, Tamura H, Hirano F, Flies DB,Roche PC, Lu J, Zhu G, Tamada K et al.: Tumor-associated B7-H1 promotes T-cell apoptosis: a potential mechanism ofimmune evasion. Nat Med 2002, 8:793-800.
This was the first study to suggest the PD-L1/B7-H1 expression ontumors could mediate immune escape, leading to the development ofblocking mAbs as a therapeutic.
45. Ahmadzadeh M, Johnson LA, Heemskerk B, Wunderlich JR,Dudley ME, White DE, Rosenberg SA: Tumor antigen-specificCD8 T cells infiltrating the tumor express high levels of PD-1and are functionally impaired. Blood 2009, 114:1537-1544.
46. Chapon M, Randriamampita C, Maubec E, Badoual C, Fouquet S,Wang SF, Marinho E, Farhi D, Garcette M, Jacobelli S et al.:Progressive upregulation of PD-1 in primary and metastaticmelanomas associated with blunted TCR signaling ininfiltrating T lymphocytes. J Invest Dermatol 2011,131:1300-1307.
47. Mellor AL, Sivakumar J, Chandler P, Smith K, Molina H, Mao D,Munn DH: Prevention of T cell-driven complement activationand inflammation by tryptophan catabolism duringpregnancy. Nat Immunol 2001, 2:64-68.
48. Munn DH, Mellor AL: IDO and tolerance to tumors. Trends MolMed 2004, 10:15-18.
49. Curiel TJ, Coukos G, Zou L, Alvarez X, Cheng P, Mottram P,Evdemon-Hogan M, Conejo-Garcia JR, Zhang L, Burow M et al.:Specific recruitment of regulatory T cells in ovarian carcinomafosters immune privilege and predicts reduced survival. NatMed 2004, 10:942-949.
50. Jandus C, Bioley G, Speiser DE, Romero P: Selectiveaccumulation of differentiated FOXP3(+) CD4(+) T cells inmetastatic tumor lesions from melanoma patients comparedto peripheral blood. Cancer Immunol Immunother 2008,57:1795-1805.
51. Zheng Y, Zha Y, Driessens G, Locke F, Gajewski TF:Transcriptional regulator early growth response gene 2 (Egr2)is required for T cell anergy in vitro and in vivo. J Exp Med 2012,209:2157-2163.
52. Dong H, Chen L: B7-H1 pathway and its role in the evasion oftumor immunity. J Mol Med 2003, 81:281-287.
overcoming barriers within the tumor microenvironment, Curr Opin Immunol (2013), http://
Current Opinion in Immunology 2013, 25:1–9

8 Cancer immunotherapy: Clinical translation
COIMMU-1189; NO. OF PAGES 9
53. Blank C, Brown I, Peterson AC, Spiotto M, Iwai Y, Honjo T,Gajewski TF: PD-L1/B7H-1 inhibits the effector phase of tumorrejection by T cell receptor (TCR) transgenic CD8+ T cells.Cancer Res 2004, 64:1140-1145.
54. Zhang L, Gajewski TF, Kline J: PD-1/PD-L1 interactions inhibitantitumor immune responses in a murine acute myeloidleukemia model. Blood 2009, 114:1545-1552.
55. Uyttenhove C, Pilotte L, Theate I, Stroobant V, Colau D,Parmentier N, Boon T, Van Den Eynde BJ: Evidence for a tumoralimmune resistance mechanism based on tryptophandegradation by indoleamine 2,3-dioxygenase. Nat Med 2003,9:1269-1274.
56. Liu X, Shin N, Koblish HK, Yang G, Wang Q, Wang K, Leffet L,Hansbury MJ, Thomas B, Rupar M et al.: Selective inhibition ofIDO1 effectively regulates mediators of antitumor immunity.Blood 2010, 115:3520-3530.
57. Litzinger MT, Fernando R, Curiel TJ, Grosenbach DW, Schlom J,Palena C: IL-2 immunotoxin denileukin diftitox reducesregulatory T cells and enhances vaccine-mediated T-cellimmunity. Blood 2007, 110:3192-3201.
58. Sutmuller RP, van Duivenvoorde LM, van Elsas A, Schumacher TN,Wildenberg ME, Allison JP, Toes RE, Offringa R, Melief CJ:Synergism of cytotoxic T lymphocyte-associated antigen 4blockade and depletion of CD25(+) regulatory T cells inantitumor therapy reveals alternative pathways forsuppression of autoreactive cytotoxic T lymphocyteresponses. J Exp Med 2001, 194:823-832.
59. Kline J, Brown IE, Zha YY, Blank C, Strickler J, Wouters H, Zhang L,Gajewski TF: Homeostatic proliferation plus regulatory T-celldepletion promotes potent rejection of B16 melanoma. ClinCancer Res 2008, 14:3156-3167.
60. Chen L, Ashe S, Brady WA, Hellstrom I, Hellstrom KE,Ledbetter JA, McGowan P, Linsley PS: Costimulation ofantitumor immunity by the B7 counterreceptor for the Tlymphocyte molecules CD28 and CTLA-4. Cell 1992, 71:1093-1102.
61. Townsend SE, Allison JP: Tumor rejection after directcostimulation of CD8+ T cells by B7-transfected melanomacells [see comments]. Science 1993, 259:368-370.
62. Gajewski TF, Fallarino F, Uyttenhove C, Boon T: Tumor rejectionrequires a CTLA4 ligand provided by the host or expressed onthe tumor: superiority of B7-1 over B7-2 for active tumorimmunization. J Immunol 1996, 156:2909-2917.
63. Fallarino F, Ashikari A, Boon T, Gajewski TF: Antigen-specificregression of established tumors induced by activeimmunization with irradiated IL-12- but not B7-1-transfectedtumor cells. Int Immunol 1997, 9:1259-1269.
64. Boussiotis VA, Barber DL, Nakarai T, Freeman GJ, Gribben JG,Bernstein GM, D’Andrea AD, Ritz J, Nadler LM: Prevention of Tcell anergy by signaling through the gamma c chain of the IL-2receptor. Science 1994, 266:1039-1042.
65. Pellegrini M, Calzascia T, Elford AR, Shahinian A, Lin AE,Dissanayake D, Dhanji S, Nguyen LT, Gronski MA, Morre M et al.:Adjuvant IL-7 antagonizes multiple cellular and molecularinhibitory networks to enhance immunotherapies. Nat Med2009, 15:528-536.
66. Klebanoff CA, Finkelstein SE, Surman DR, Lichtman MK,Gattinoni L, Theoret MR, Grewal N, Spiess PJ, Antony PA,Palmer DC et al.: IL-15 enhances the in vivo antitumor activity oftumor-reactive CD8+ T cells. Proc Natl Acad Sci U S A 2004,101:1969-1974.
67. Epardaud M, Elpek KG, Rubinstein MP, Yonekura AR, Bellemare-Pelletier A, Bronson R, Hamerman JA, Goldrath AW, Turley SJ:Interleukin-15/interleukin-15R alpha complexes promotedestruction of established tumors by reviving tumor-residentCD8+ T cells. Cancer Res 2008, 68:2972-2983.
68. Gattinoni L, Finkelstein SE, Klebanoff CA, Antony PA, Palmer DC,Spiess PJ, Hwang LN, Yu Z, Wrzesinski C, Heimann DM et al.:Removal of homeostatic cytokine sinks by lymphodepletionenhances the efficacy of adoptively transferred tumor-specific CD8+ T cells. J Exp Med 2005, 202:907-912.
Please cite this article in press as: Gajewski TF, et al.: Cancer immunotherapy strategies based on
dx.doi.org/10.1016/j.coi.2013.02.009
Current Opinion in Immunology 2013, 25:1–9
69. Wang LX, Li R, Yang G, Lim M, O’Hara A, Chu Y, Fox BA,Restifo NP, Urba WJ, Hu HM: Interleukin-7-dependentexpansion and persistence of melanoma-specific T cells inlymphodepleted mice lead to tumor regression and editing.Cancer Res 2005, 65:10569-10577.
70. Brown IE, Blank C, Kline J, Kacha AK, Gajewski TF: Homeostaticproliferation as an isolated variable reverses CD8+ T cellanergy and promotes tumor rejection. J Immunol 2006,177:4521-4529.
71. Kline J, Zhang L, Battaglia L, Cohen KS, Gajewski TF: Cellular andmolecular requirements for rejection of B16 melanoma in thesetting of regulatory T cell depletion and homeostaticproliferation. J Immunol 2012, 188:2630-2642.
72. Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC,McDermott DF, Powderly JD, Carvajal RD, Sosman JA, Atkins MBet al.: Safety, activity, and immune correlates of anti-PD-1antibody in cancer. N Engl J Med 2012, 366:2443-2454.
73. Brahmer JR, Tykodi SS, Chow LQ, Hwu WJ, Topalian SL, Hwu P,Drake CG, Camacho LH, Kauh J, Odunsi K et al.: Safety andactivity of anti-PD-L1 antibody in patients with advancedcancer. N Engl J Med 2012, 366:2443-2465.
74. Kuzel TM: DAB(389)IL-2 (denileukin diftitox, ONTAK): review ofclinical trials to date. Clin Lymphoma 2000, 1(Suppl. 1):S33-S36.
75. Rasku MA, Clem AL, Telang S, Taft B, Gettings K, Gragg H,Cramer D, Lear SC, McMasters KM, Miller DM et al.: Transient Tcell depletion causes regression of melanoma metastases. JTransl Med 2008, 6:12.
76. Morse MA, Hobeika AC, Osada T, Serra D, Niedzwiecki D,Lyerly HK, Clay TM: Depletion of human regulatory T cellsspecifically enhances antigen-specific immune responses tocancer vaccines. Blood 2008, 112:610-618.
77. Dannull J, Su Z, Rizzieri D, Yang BK, Coleman D, Yancey D,Zhang A, Dahm P, Chao N, Gilboa E et al.: Enhancement ofvaccine-mediated antitumor immunity in cancer patients afterdepletion of regulatory T cells. J Clin Invest 2005,115:3623-3633.
78. Attia P, Maker AV, Haworth LR, Rogers-Freezer L, Rosenberg SA:Inability of a fusion protein of IL-2 and diphtheria toxin(Denileukin Diftitox, DAB389IL-2, ONTAK) to eliminateregulatory T lymphocytes in patients with melanoma. JImmunother 2005, 28:582-592.
79. Rech AJ, Mick R, Martin S, Recio A, Aqui NA, Powell DJ Jr,Colligon TA, Trosko JA, Leinbach LI, Pletcher CH et al.: CD25blockade depletes and selectively reprograms regulatory Tcells in concert with immunotherapy in cancer patients. SciTransl Med 2012, 4:134ra162.
80. Sportes C, Babb RR, Krumlauf MC, Hakim FT, Steinberg SM,Chow CK, Brown MR, Fleisher TA, Noel P, Maric I et al.: Phase Istudy of recombinant human interleukin-7 administration insubjects with refractory malignancy. Clin Cancer Res 2010,16:727-735.
81. Mackall CL, Fry TJ, Gress RE: Harnessing the biology of IL-7 fortherapeutic application. Nat Rev Immunol 2011, 11:330-342.
82. Steel JC, Waldmann TA, Morris JC: Interleukin-15 biology and itstherapeutic implications in cancer. Trends Pharmacol Sci 2012,33:35-41.
83. Thompson JA, Curti BD, Redman BG, Bhatia S, Weber JS,Agarwala SS, Sievers EL, Hughes SD, DeVries TA, Hausman DF:Phase I study of recombinant interleukin-21 in patients withmetastatic melanoma and renal cell carcinoma. J Clin Oncol2008, 26:2034-2039.
84. Petrella TM, Tozer R, Belanger K, Savage KJ, Wong R, Smylie M,Kamel-Reid S, Tron V, Chen BE, Hunder NN et al.: Interleukin-21has activity in patients with metastatic melanoma: a phase IIstudy. J Clin Oncol 2012, 30:3396-3401.
85. Rosenberg SA, Dudley ME: Cancer regression in patients withmetastatic melanoma after the transfer of autologousantitumor lymphocytes. Proc Natl Acad Sci U S A 2004,101(Suppl. 2):14639-14645.
overcoming barriers within the tumor microenvironment, Curr Opin Immunol (2013), http://
www.sciencedirect.com

Modulation of the tumor microenvironment Gajewski et al. 9
COIMMU-1189; NO. OF PAGES 9
86. Dudley ME, Yang JC, Sherry R, Hughes MS, Royal R, Kammula U,Robbins PF, Huang J, Citrin DE, Leitman SF et al.: Adoptive celltherapy for patients with metastatic melanoma: evaluation ofintensive myeloablative chemoradiation preparativeregimens. J Clin Oncol 2008, 26:5233-5239.
87. Grosso JF, Kelleher CC, Harris TJ, Maris CH, Hipkiss EL, DeMarzo A, Anders R, Netto G, Getnet D, Bruno TC et al.: LAG-3regulates CD8+ T cell accumulation and effector function inmurine self- and tumor-tolerance systems. J Clin Invest 2007,117:3383-3392.
88. Matsuzaki J, Gnjatic S, Mhawech-Fauceglia P, Beck A, Miller A,Tsuji T, Eppolito C, Qian F, Lele S, Shrikant P et al.: Tumor-infiltrating NY-ESO-1-specific CD8+ T cells are negativelyregulated by LAG-3 and PD-1 in human ovarian cancer. ProcNatl Acad Sci U S A 2010, 107:7875-7880.
89. Fourcade J, Sun Z, Benallaoua M, Guillaume P, Luescher IF,Sander C, Kirkwood JM, Kuchroo V, Zarour HM: Upregulation ofTim-3 and PD-1 expression is associated with tumor antigen-specific CD8+ T cell dysfunction in melanoma patients. J ExpMed 2010, 207:2175-2186.
90. Sakuishi K, Apetoh L, Sullivan JM, Blazar BR, Kuchroo VK,Anderson AC: Targeting Tim-3 and PD-1 pathways to reverse Tcell exhaustion and restore anti-tumor immunity. J Exp Med2010, 207:2187-2194.
91. Woo SR, Turnis ME, Goldberg MV, Bankoti J, Selby M, Nirschl CJ,Bettini ML, Gravano DM, Vogel P, Liu CL et al.: Immune inhibitorymolecules LAG-3 and PD-1 synergistically regulate T-cellfunction to promote tumoral immune escape. Cancer Res 2012,72:917-927.
Please cite this article in press as: Gajewski TF, et al.: Cancer immunotherapy strategies based on
dx.doi.org/10.1016/j.coi.2013.02.009
www.sciencedirect.com
92. Wang S, Chen L: Immunobiology of cancer therapies targetingCD137 and B7-H1/PD-1 cosignal pathways. Curr Top MicrobiolImmunol 2011, 344:245-267.
93. Sievers EL, Larson RA, Stadtmauer EA, Estey E, Lowenberg B,Dombret H, Karanes C, Theobald M, Bennett JM, Sherman MLet al.: Efficacy and safety of gemtuzumab ozogamicin inpatients with CD33-positive acute myeloid leukemia in firstrelapse. J Clin Oncol 2001, 19:3244-3254.
94. Verma S, Miles D, Gianni L, Krop IE, Welslau M, Baselga J,Pegram M, Oh DY, Dieras V, Guardino E et al.: Trastuzumabemtansine for HER2-positive advanced breast cancer. N Engl JMed 2012, 367:1783-1791.
95. Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B,Lagorce-Pages C, Tosolini M, Camus M, Berger A, Wind P et al.:Type, density, and location of immune cells within humancolorectal tumors predict clinical outcome. Science 2006,313:1960-1964.
96. Galon J, Pages F, Marincola FM, Thurin M, Trinchieri G, Fox BA,Gajewski TF, Ascierto PA: The immune score as a new possibleapproach for the classification of cancer. J Transl Med 2012,10:1.
97.�
Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA,Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel JCet al.: Improved survival with ipilimumab in patients withmetastatic melanoma. N Engl J Med 2010.
This clinical trial of ipilimumab in patients with advanced melanomarepresents the first study ever to demonstrate improved overall survivalin this patient population.
overcoming barriers within the tumor microenvironment, Curr Opin Immunol (2013), http://
Current Opinion in Immunology 2013, 25:1–9