Embed Size (px)
Citation preview

CAPNOGRAPHYpresented by:
Fred Halazon, NREMT-P
Mike Burke, NREMT-P
Cunningham Fire

What is Capnography?Noninvasive, continuous measurement of exhaled carbon dioxide concentration over time
Digital display provides EtCO2 value
Provides a distinct waveform for each respiratory cycle


Overview
• Anatomy & Physiology• Capnographic waveform• Diagnosing different waveforms• Case studies

Relevance
Endotracheal tube VerificationCardiac ArrestVentilationBronchospastic DiseaseEarly detection of cellular hypoxia

History of Capnography in EMS
Colormetric- Useful device to confirm ET tube placement in patients not in cardiac arrestTube could be in esophagus or that circulation is not bringing CO2 to the lungs Prone to contamination, leads to false negatives

History of Capnography in EMS
Pulse oximetry preceded capnographyPulse oximetry measures oxygenationCapnography measures ventilationNew technologies now allow use in EMS

Capnometry
Provides only a numerical measurement of carbon dioxide (EtCO2)

Capnogram
A waveform display of carbon dioxide over time

Definition of Capnography
Numerical value of the EtCO2 ANDWaveform of the concentration present in the airway Respiratory rate detected from the actual airflow

Oxygen> lungs> alveoli> blood
Muscles + organs
Oxygen + Glucose
O2
CO2
CO2
CO2
O2
cellsenergy
blood
lungs
breath

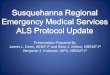
Capnographic Waveform
A B
C D
EExpirationInspiration Inspiration

Physiology of CO2
Concentration of CO2 in alveoli:
Varies INDIRECTLY with ventilation
Increase Ventilation: Decrease CO2 in Alveoli
Decrease Ventilation: Increase CO2 in Alveoli
Varies DIRECTLY with perfusion
Decrease Perfusion: Decrease CO2 in Alveoli
Increase Perfusion: Increase CO2 in Alveoli

Oxygenation and VentilationWhat is the difference?
Oxygenation: is the transport of O2 via the bloodstream to the cells
Oxygen is required for metabolism
Ventilation: is the movement of air into and out of the lungs
exhaling of CO2 via the respiratory tractCarbon dioxide is a byproduct of metabolism

Oxygenation
Measured by pulse oximetry (SpO2)Noninvasive measurementPercentage of oxygen in red blood cellsChanges in ventilation take several minutes to be detectedAffected by motion artifact, poor perfusion, temperature

Ventilation
Measured by the end-tidal CO2
Partial pressure (mm Hg) or volume (%) of CO2 in the airway at end of exhalationBreath-to-breath measurement provides information within secondsNot affected by motion artifact, distal circulation, temperatureWill see respiratory arrest immediately

Distinguishing between oxygenation and ventilation

If ventilation is held constant, then changes in EtCO2 are
due to changes in cardiac output

Cardiac Output(L)
EtCO2 (mm Hg)
2 20
3 28
4 32
5 36


Value of the Capnographic Waveform
Provides valid EtCO2 valueVisual assessment of patient airway integrityVerify proper ET tube placement (with pulmonary perfusion)Waveforms have characteristic shape like an ECG

Capnographic Waveform
Height shows amount of CO2
Length depicts time
45
0

End-tidal CO2 (EtCO2)
Allows monitoring for changes inVentilation—Asthma, COPD, airway edema, FBAO, stroke, overdoseDiffusion—Pulmonary edema, alveolar damage, Pneumonia Perfusion—shock, pulmonary embolus, cardiac arrest, severe dysrhythmiasRed Blood Cell Function: CO poisoning (COHb), hydrogen cyanide, severe anemia

Decreased EtCO2
Decreased MetabolismAnalgesia/ sedationHypothermia
Circulatory SystemCardiac arrestEmbolismSudden hypovolemia or hypotension
Respiratory SystemAlveolar hyperventilationBronchospasmMucus plugging
EquipmentLeak in systemPartial obstructionETT in hypopharynx

Increased EtCO2
Increased MetabolismPainHyperthermiaMalignant hyperthermiaShivering
Circulatory SystemIncreased cardiac output with constant ventilation
Respiratory SystemRespiratory insufficiencyRespiratory depressionObstructive lung disease
EquipmentDefective exhalation valveExhausted CO2 absorber

End tidal of 0
Respiratory failureCardiac arrestAirway displacementAirway obstructionDisconnection of ventilation system

Major Benefits in Pre-Hospital
Verifying ETT placement and continuous monitoring of position during transportCardiac Arrest
Effectiveness of cardiac compressionPredictor of survivalSign of return of cardiac function
VentilationBronchospastic Disease

ETT Displacement
Most likely occurs when patient is
moved

Dislodged

Dislodged

Right Main Bronchi/Pneumothorax

CPR
Force, depth, and rate of chest compressions
4 5
0
100% mortality if unable to achieve an EtCO2 of 10 mm Hg after 20 minutes

CPR

ROSC

End Tidal with Return of circulation
4 5
0

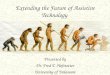
Hyperventilation
Hypocapnia < 35 mmHgNormal range is 35-45 mm Hg (5% vol)How would hyperventilation change the waveform? (26-30)
FrequencyDurationHeightShape

Hyperventilation
45
0

Hypoventilation
• Hypercapnia > 45 mmHg• How would hypoventilation change the
waveform? (4-12)– Frequency– Duration– Height– Shape

Hypoventilation
45
0

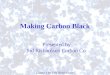
Bronchospasm
• Alveoli unevenly ventilated on inspiration• Prolonged expiratory time
– Air trapping– “Shark Fin” shaped waveform
• What about COPD?

Bronchospasm
45
0
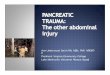
Bronchospasm

Bronchospasm

COPD

Asthma
Initial
After therapy

What is Wrong?

Documentation
• Continuous waveform allows for legal documentation
• Proof of correct tube placement, RR, EtCO2
• Effectiveness of treatment in patient care, early detection of deterioration

• The era is over when we can justify not knowing whether an ETT is in place or
not.
• We may not be able to intubate everybody, but we must always know
when the tube is in place or not.

Who get’s End tidal
• All pt’s with an ETT tube or King airway• All unconscious or altered pt’s • Any pt with BVM ventilation• Respiratory distress pt’s

Bottom line
Treat the patient in front of you

1. Barton, C. & Wang, E. (1994). Correlation of End-Tidal CO2 Measurements to Arterial PaCO2 in Nonintubated Patients. Annals of Emergency Medicine, 23 (3): 561-562.
2. Bergenholtz, K.F., RN, MSN, CRNP-CS. (2004). Using and understanding Capnography. Microstream capnography solutions. [email protected].
3. Bhavani-Shankar, K., MD, Philip, JH. Defining segments and phases of a time capnogram. Anesthesiology Analg (2000). 91(4): 973-977.
4. Bhavani-Shankar, K., MD. http://capnography.com/
5. Falk, J.L., Rackow, E.C., Weil, M.H. End-tidal carbon dioxide concentration during cardiopulmonary resuscitation. New England Journal of Medicine (1998) 318(10): 607-611.
6. Fowler, Ray, MD, FACEP. www.rayfowler.com
7. Fowler, W.S. Lung Function studies, II. The respiratory deadspace. American Journal of Physiology. (1998) 154: 405-416.
8. Kanowitz, A., MD, FACEP, EMS Director, Arvada, CO. (2004). [Capnography in EMS]. Unpublished raw data.
References

8. Katz SH, Falk JL. Misplaced endotracheal tubes by paramedics in an urban emergency medical services system. Annals of Emergency Medicine (2001) 37(1): 32-37.
9. Medtronic Physio-Control Corporation (2005). http://www.healthcareeducation.org
9. Raff, Hershel, PhD, (2003). Physiology Secrets (2nd ed.) Philadelphia, PA: Hanley & Belfus.
10.Scanlon, V.C. & Sanders, T., (1999). Essentials of Anatomy and Physiology (3rd ed.) Philadelphia, PA: F.A. Davis Co.
11.Thompson, J.E., RRT, FAARC, Jaffe, M.B., PhD. (2005 Jan). Capnography waveforms in the mechanically ventilated patient. Respiratory Care. 50(1): 100-109.
12.Wik L, et al: “Quality of cardiopulmonary resuscitation during out-of-hospital cardiac arrest.” JAMA. 293(3): 299-304, 2005.
13.Woodruff, D.W., RN, CNS, CCRN, MSN. (2006 Jan/Feb) Deciphering Diagnostics. Nursing made incredibly easy!, 4(1): 4-10.