Embed Size (px)
Citation preview
2014-2017
COMMUNITY ACCOUNTABILITY PLANNING SUBMISSIONS (CAPS) REFERENCE OVERVIEW 2014-2017
Version: October 1, 2013
Note: CAPS Guidelines are subject to change. The MultiSector Accountability Agreement (MSAA) takes precedence where there is conflict between these Guidelines and the MSAA.
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 2
Table of Contents 1. Introduction .................................................................................................................................................... 3
1.1 LHSIA, 2006 ............................................................................................................................................. 3
1.2 Overview of the CAPS/M-SAA Process .............................................................................................. 4
2. Key Planning Considerations for the CAPS and M-SAA ........................................................................ 5
2.1 Principles Guiding the Process ...................................................................................................... 5
2.2 Planning Assumptions ......................................................................................................................... 6
2.3 The 2011 – 14 Monitoring Process .................................................................................................... 6
2.4 Data Quality ............................................................................................................................................. 6
2.5 Board Approval & Failure to Comply ............................................................................................ 6
2.6 Timelines .................................................................................................................................................. 7
2.7 Financial Penalty ................................................................................................................................ 7
3. M-SAA Components ..................................................................................................................................... 8
3.1 CAPS Components ............................................................................................................................... 8
3.2 M-SAA Narrative Model Part A ........................................................................................................ 8
3.3 Reports ..................................................................................................................................................... 8
3.4 Directives, Guidelines and Policies .................................................................................................. 8
3.5 Performance ............................................................................................................................................ 8
3.6 Part Template for Project Funding ...................................................................................................... 9
3.7 Other Services .......................................................................................................................................... 9
4. Changes Needing LHIN Approval ............................................................................................................ 10
4.1 Proposing Operational Changes .................................................................................................. 10
4.2 Adding New Services, Service Enhancement ........................................................................... 10
4.3 Service Reduction, Transfer or Elimination Proposal (Service Integration) .................... 10
5. Guidelines for Balanced Operating Plans ............................................................................................... 12
5.1 Basic Requirement: A Balanced Operating Position ................................................................. 12
5.2 Budget Balancing Alternatives ........................................................................................................ 12
6. CAPS Links to M-SAA Performance ........................................................................................................ 13
6.1 The Indicator Development Process ........................................................................................... 13
7. Appendix A: Glossary ................................................................................................................................. 16
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 3
1. Introduction
It is a requirement of the Local Health System Integration Act, 2006 (“LHSIA”) that Local Health Integration Networks (“LHINs”) have a service accountability agreement (SAA) in place with each health service provider (HSP) that it funds. The current 2011-14 Multi-sector Service Accountability Agreements or M-SAAs for the Community Health Centre (CHC), Community Care Access Centre (CCAC), Mental Health & Addiction (MH&A) and Community Support Service (CSS) sectors expire on March 31, 2014 and thus must be replaced with new agreements that will take effect on April 1, 2014.
In order to facilitate the negotiation of the M-SAAs with HSPs in the CHC, CCAC, MH&A and CSS sectors, each HSP will be required to submit a planning document known as the Community Accountability Planning Submission (CAPS).
The CAPS and the new M-SAA will each cover a three year period. The purpose of the Guidelines is to provide additional information to assist HSPs in the community sector to complete their 2014-17 CAPS.
1.1 LHSIA, 2006
The LHSIA provides the underpinnings for the accountability relationship between LHINs and the community health service sector. The purpose of the LHSIA is to provide for an integrated health system that will improve the health of Ontarians through: (i) Better access to high quality health services (ii) Coordinated health care in local health systems and across the province (iii) Effective and efficient management of the health system at the local level.
LHIN Funding and the Accountability Agreement with the Ministry of Health and Long-Term Care (MOHLTC): The LHINs’ relationship to the province is set out in LHSIA and in a Memorandum of Understanding between each LHIN and the Minister of Health and Long-Term Care. Funding for the LHINs is provided by the MOHLTC on terms set out in an accountability agreement between the Minister and each LHIN (the “Accountability Agreement”). The Accountability Agreement sets out, among other items:
a) Performance goals and objectives for the LHIN and the local health system. b) Performance standards, targets and measures for the LHIN and the local health system. c) Requirements for the LHIN to report on its performance and that of the local health system. d) A requirement that the LHIN provide a plan for spending the funding that the LHIN receives
from the MOHLTC (the Annual Service Plan). e) A progressive performance management process.
Health Service Provider (HSP) Funding and SAAs: LHSIA also permits a LHIN to provide funding to an HSP for services that the HSP provides in, or for, the geographic area of the LHIN, however if a LHIN wishes to provide funding to an HSP it must first enter into a SAA with the HSP. LHSIA requires that the SAAs terms must be terms that
a. The LHIN considers appropriate. b. Are in accordance with:
i. The funding that the LHIN receives from the MOHLTC ii. The Accountability Agreement with the MOHLTC.
iii. Any other requirements that may be set out in regulations under the LHSIA.
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 4
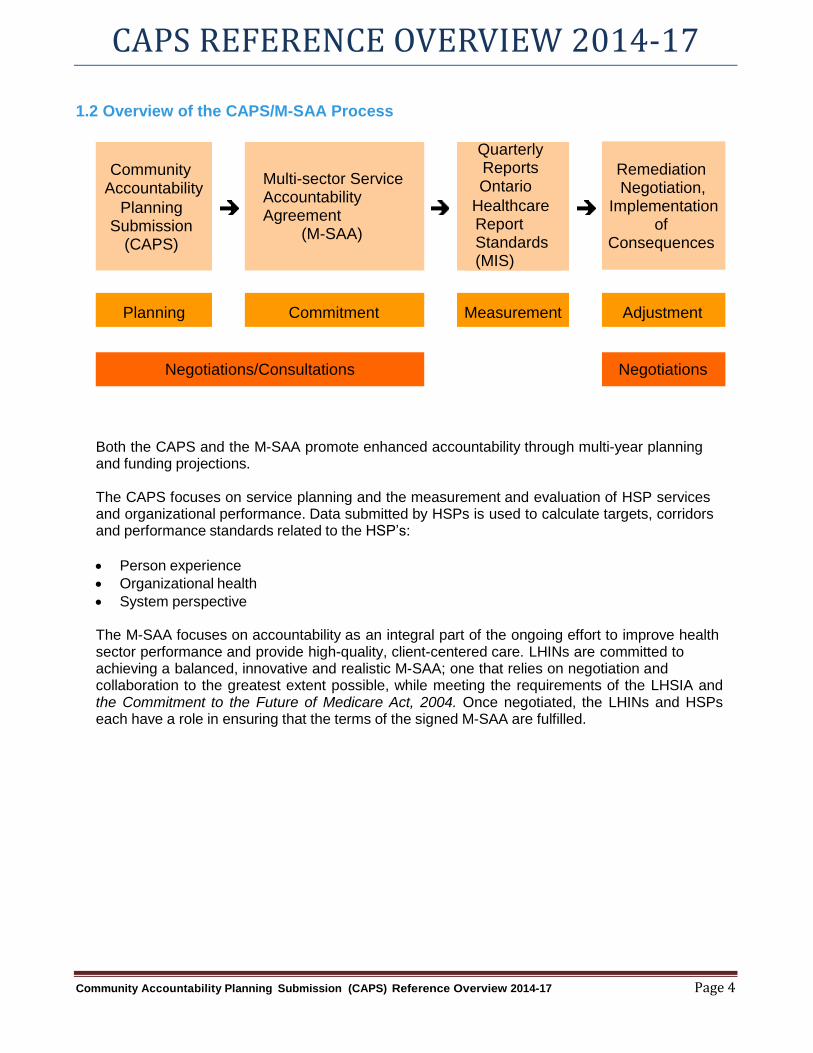
1.2 Overview of the CAPS/M-SAA Process
Community Accountability
Planning Submission
(CAPS)
Multi-sector Service Accountability Agreement
(M-SAA)
Quarterly Reports Ontario
Healthcare Report Standards (MIS)
Remediation
Negotiation,
Implementation of
Consequences
Planning Commitment Measurement Adjustment
Negotiations/Consultations Negotiations
Both the CAPS and the M-SAA promote enhanced accountability through multi-year planning and funding projections.
The CAPS focuses on service planning and the measurement and evaluation of HSP services and organizational performance. Data submitted by HSPs is used to calculate targets, corridors and performance standards related to the HSP’s:
Person experience
Organizational health
System perspective
The M-SAA focuses on accountability as an integral part of the ongoing effort to improve health sector performance and provide high-quality, client-centered care. LHINs are committed to achieving a balanced, innovative and realistic M-SAA; one that relies on negotiation and collaboration to the greatest extent possible, while meeting the requirements of the LHSIA and the Commitment to the Future of Medicare Act, 2004. Once negotiated, the LHINs and HSPs each have a role in ensuring that the terms of the signed M-SAA are fulfilled.
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 5
2. Key Planning Considerations for the CAPS and M-SAA
2.1 Principles Guiding the Process
HSPs should consider the following principles when preparing their submission and engaging their local and regional partners.
a) Accountability
The CAPS is owned and managed by the HSP.
The CAPS will inform the negotiation of the M-SAA between the LHIN and the HSP.
The HSP’s LHINs will provide guidance, approve and monitor the performance obligations of the M-SAA.
The HSP will be accountable to the LHIN for the achievement of the HSP’s performance obligations in the M-SAA.
b) Funding and Allocation
An HSP must plan to achieve a balanced operating position for the total entity for each year of the M-SAA that is consistent with relevant ministry policy and legislation/regulation.
An HSP’s funding can only be used in accordance with the terms of the M-SAA.
An HSP’s LHIN will also regularly monitor in-year forecasts of the financial position of LHIN-funded services. Confirmed forecasts of un-spent LHIN funding will be recovered within the fiscal year and reallocated to address financial pressures in the LHIN’s other HSPs.
c) Integration and Service Coordination
HSP planning must reflect the HSP’s ongoing responsibility to find efficiencies in administrative and direct service areas including review and/or consultation with other HSPs.
d) Local Health System Planning
HSP planning must be in alignment with the LHIN Integrated Health Service Plan (IHSP), the government’s health care priorities, and reflect best practices, evidence-informed decisions, and the pursuit of efficiency opportunities within the HSP and in collaboration with hospitals, community partners and other HSPs.
HSP planning must integrate the HSPs obligation under s. 16(6) and s. 24 of the LHSIA.
s. 16(6) Engagement by Health Service Providers each HSP shall engage the community of diverse persons and entities in the area where it provides health services when developing plans and setting priorities for the delivery of health services.
s. 24 Identifying integration opportunities Each LHIN and each HSP shall separately and in conjunction with each other identify opportunities to integrate the services of the local health system to provide appropriate, coordinated, effective and efficient services.
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 6
e) Local Community Engagement HSP planning must clearly include ongoing consultation and engagement by the HSP
with local health service providers and other stakeholders with a view towards closer cooperation and partnership between providers and between sectors.
2.2 Planning Assumptions
In the absence of definitive ministry funding targets in 2014, HSPs will completed the 2014-17 CAPS based on a planning assumption of a 0% base adjustment for the first three years of the Agreement. At the time of preparation of these guidelines, the LHIN has not determined the targeted allocations or incremental funding allocation adjustments for 2014/17. As such, HSPs are required to plan and submit a budget based on a 0% funding adjustment. An HSP must consider this planning assumption when developing its forecasts on service volume and indicator performance. If the HSP is considering a service target reduction to meet the 0% guideline, they must initiate a discussion with their LHIN representative.
2.3 The 2011 – 14 Monitoring Process
The LHINs will review the HSP performance results against the targets outlined in the 2014–17 M-SAA on a quarterly basis.
HSPs will be required to monitor their performance against variances. HSPs may be required to meet with their LHIN to review any variances, and at the discretion of the LHIN, will be required to propose an improvement plan.
2.4 Data Quality
The reporting of valid and reliable health care clinical and financial/statistical data is essential. The ability of HSPs to negotiate and meet their performance targets is highly dependent on how well the historical data reflects actual HSP performance. Improvements in the quality of health care data reported from HSPs will improve the ability of HSPs, LHINs and the province to set and meet performance targets.
2.5 Board Approval & Failure to Comply Each HSP Board must approve the 2014/17 CAPS prior to submission as this serves as the basis for the preparation of the M-SAA. HSPs should review the Timelines outlined below so that they can work within those timelines for a successful submission. Failure to meet the timelines outlined is a contravention of the M-SAA and the LHIN will take necessary performance improvement steps to rectify the non-compliance, as stipulated in the M-SAA.
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 7
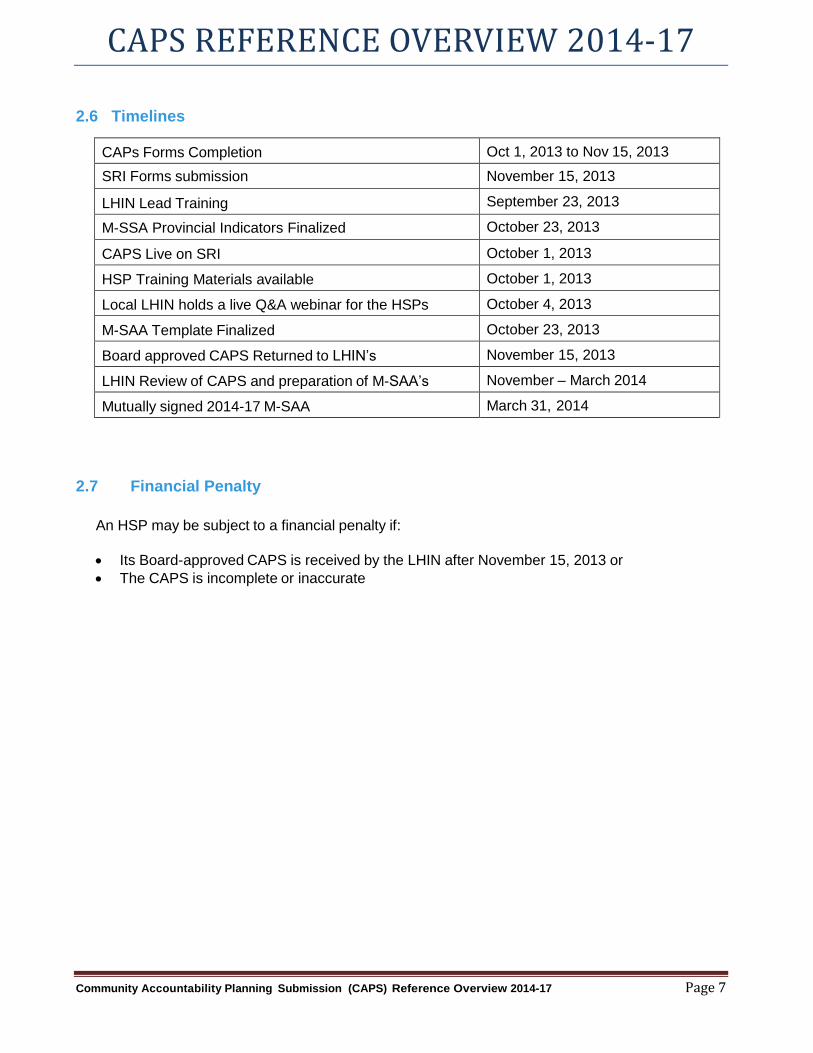
2.6 Timelines
CAPs Forms Completion Oct 1, 2013 to Nov 15, 2013
SRI Forms submission November 15, 2013
LHIN Lead Training September 23, 2013
M-SSA Provincial Indicators Finalized October 23, 2013
CAPS Live on SRI October 1, 2013
HSP Training Materials available October 1, 2013
Local LHIN holds a live Q&A webinar for the HSPs October 4, 2013
M-SAA Template Finalized October 23, 2013
Board approved CAPS Returned to LHIN’s November 15, 2013
LHIN Review of CAPS and preparation of M-SAA’s November – March 2014
Mutually signed 2014-17 M-SAA March 31, 2014
2.7 Financial Penalty
An HSP may be subject to a financial penalty if:
Its Board-approved CAPS is received by the LHIN after November 15, 2013 or
The CAPS is incomplete or inaccurate
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 8
Narrative Model Orientation 2014-17.ppt
3. M-SAA Components
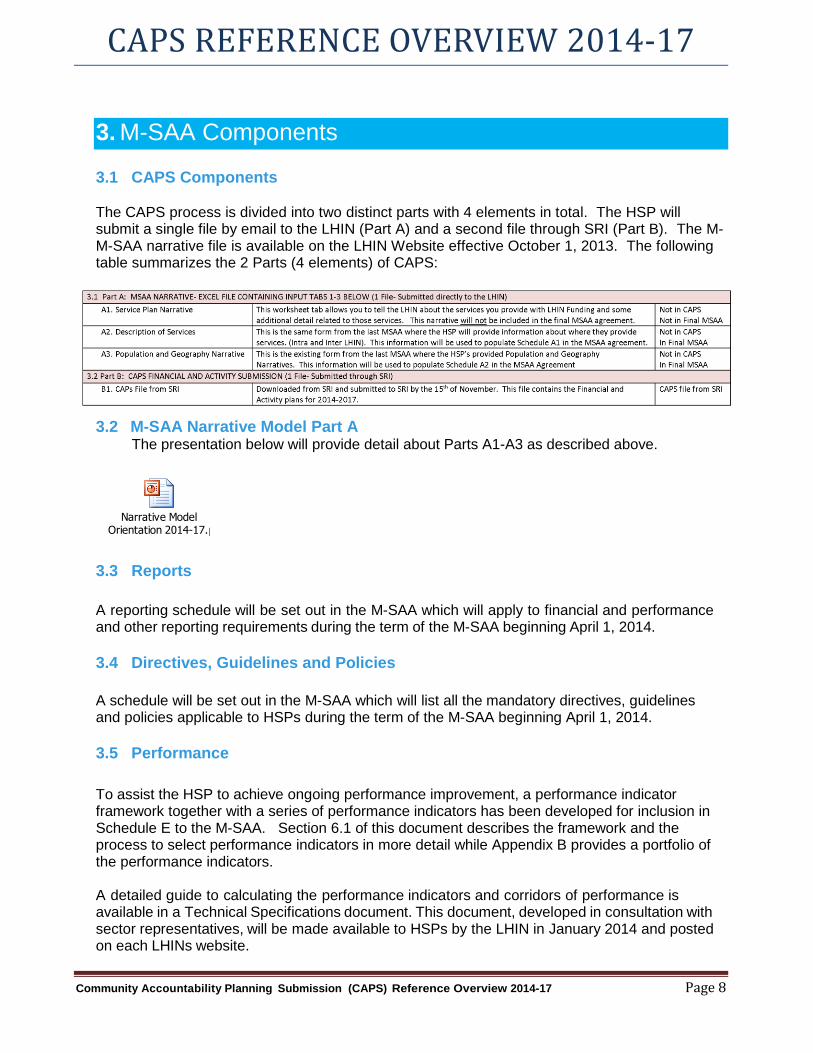
3.1 CAPS Components The CAPS process is divided into two distinct parts with 4 elements in total. The HSP will submit a single file by email to the LHIN (Part A) and a second file through SRI (Part B). The M-M-SAA narrative file is available on the LHIN Website effective October 1, 2013. The following table summarizes the 2 Parts (4 elements) of CAPS:
3.2 M-SAA Narrative Model Part A The presentation below will provide detail about Parts A1-A3 as described above.
3.3 Reports
A reporting schedule will be set out in the M-SAA which will apply to financial and performance and other reporting requirements during the term of the M-SAA beginning April 1, 2014.
3.4 Directives, Guidelines and Policies
A schedule will be set out in the M-SAA which will list all the mandatory directives, guidelines and policies applicable to HSPs during the term of the M-SAA beginning April 1, 2014.
3.5 Performance
To assist the HSP to achieve ongoing performance improvement, a performance indicator framework together with a series of performance indicators has been developed for inclusion in Schedule E to the M-SAA. Section 6.1 of this document describes the framework and the process to select performance indicators in more detail while Appendix B provides a portfolio of the performance indicators.
A detailed guide to calculating the performance indicators and corridors of performance is available in a Technical Specifications document. This document, developed in consultation with sector representatives, will be made available to HSPs by the LHIN in January 2014 and posted on each LHINs website.
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 9
3.6 Part Template for Project Funding
Schedule F, "Project Template" allows the LHIN to fund an HSP to undertake projects for the LHIN during the term of the SAA, without the need to negotiate a separate project funding agreement. The Project Template builds on the existing terms of the SAA between the LHIN and the HSP, and allows a quick start to projects.
3.7 Other Services
a) Preschool Speech and Language Services
These services are funded by the Ministry of Health and Long-Term Care and managed by the Ministry of Children and Youth Services. Any changes or reductions in these services must be negotiated and approved under the terms of the HSP’s agreement with the Ministry of Children and Youth Services.
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 10
4. Changes Needing LHIN Approval
4.1 Proposing Operational Changes
Certain types of operational changes will require pre-approval from the LHIN before the proposed change can be incorporated into the HSP’s CAPS. These would include any changes affecting funding or service levels, the reduction, elimination or transfer of a service and other integration activities.
4.2 Adding New Services, Service Enhancement
Guidelines and templates for the development of a pre-proposal, detailed proposal and business case to support a new or enhanced service will be provided by the individual LHIN. It is recommended that the LHIN be contacted prior to beginning work on a pre-proposal to determine any local variations or specific issues the LHIN wishes to see addressed.
The CAPS should be prepared to maintain service levels within the planning assumptions provided by the LHIN. Service enhancements that can be accommodated within the planning assumptions can be included in the CAPS. New service proposals (supported by business case submissions) that are approved by the LHIN will be incorporated into the M-SAA.
HSPs that wish to reduce or eliminate services or transfer them to another HSP must follow the steps set out in Section 4.3 of these guidelines.
4.3 Service Reduction, Transfer or Elimination Proposal (Service Integration)
Access to community health services is an important priority for the government, LHINs and HSPs. As a result, any proposed reduction, transfer or elimination of a service should be consistent with the overall goal of an integrated health system that provides access to high quality health services and coordinated health care in an effective and efficient manner. The LHIN must be provided with lead time (at least 60 days) to ensure that essential levels of service (both quality and quantity) are maintained.
A service reduction, transfer or elimination proposal should include:
Rationale for the service change and alternative measures considered during the decision
making process.
Anticipated funding adjustments, i.e. expected decrease or increase in funding associated
with the service change.
Impact on performance obligations.
Human resource impact, e.g. staff reduction or re-assignment.
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 11
Strategy for mitigating any anticipated client impacts of the service change.
Consultation process and outcomes with health care partners and the community.
Communications plan to communicate to both internal and external audiences.
Please note that section 27 of LHSIA requires an HSP to notify the LHIN of any integration with another person or entity that relates to services that are funded in whole or in part by the LHIN.
The templates and process for proposing a service reduction, elimination, or transfer are posted to each LHIN’s web site.
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 12
5. Guidelines for Balanced Operating Plans
5.1 Basic Requirement: A Balanced Operating Position
An HSP seeking funding from the LHIN is expected to submit a CAPS that demonstrates the HSP has achieved a balanced operating position for the total entity and will achieve and maintain a balanced operating position during each year of the M-SAA. A balanced operating position for the total entity is where the total expenses are less than or equal to all sources of revenue.
5.2 Budget Balancing Alternatives
HSP managers have always strived to maintain or enhance service levels within the confines of the available budget. The CAPS should be prepared to maintain service levels within the planning assumptions provided by the LHIN. The LHIN will expect HSPs to first consider all possible cost savings alternatives in lieu of reducing service levels such as:
a. Back office integration (combining with other HSPs to reduce the cost of administration, e.g.
shared accounting service).
b. Increase supplementary (non-LHIN/MOHLTC) revenue.
c. Program efficiencies, e.g. review of best practices in operations and service delivery.
d. Technology and automation, e.g. Use of laptops/Personal Digital Assistants (PDAs) to reduce time spent on paperwork.
e. Enhanced community support e.g. increased use of volunteers and contributions in kind.
f. Program consolidation (combining or linking programs internally or reducing the number of
sites).
g. Combining with another organization to achieve economies of scale and scope.
h. Effectiveness reviews – directing limited resources to the most effective programs and/or most vulnerable clients.
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 13
6. CAPS Links to M-SAA Performance
Note: This Section is currently under review by the M-SAA Indicators Work Group and will be updated by October 23, 2013. Some changes are anticipated that may affect Schedules in the M-SAA, but these will not affect the content or completion of CAPS at this time.
6.1 The Indicator Development Process
a) The LHIN Performance Indicator Framework
The LHIN Performance Indicator Framework was developed as a tool for LHINs to identify indicators to monitor the performance of HSPs. As a tactical and operational tool, the goal of the framework is to allow LHINs and HSPs to work together to identify and monitor indicators that support the achievement of provincial priorities. The framework focuses on the components of and enablers to the delivery of quality health care services (across the continuum of care) to the people of Ontario. Designed to support organizational and system performance measurement, the framework encourages HSPs to work together in support of improved outcomes and experiences.
The framework aligns with the (draft) provincial Health System Scorecard and aims to focus attention on the key priority areas identified by the LHINs in their Integrated Health Service Plans. It is a dynamic tool; one that may need to be adjusted in response to the conceptualization of quality and/or significant changes in the strategic direction of the Ministry of Health and Long-Term Care. For now, the framework serves as mechanism to help LHINs and HSPs to better coordinate and organize the delivery of quality health care.
b) Performance Dimensions
The components of and enablers to providing quality care are identified within the framework in three key areas of focus:
PERSON EXPERIENCE – focusing on the needs of the client, caregiver and family, ensuring Ontarians not only receive the high quality health care they need, when they need it, but that they are involved in their health care plans and can make informed decisions about the health services they receive. Preventative measures/initiatives are also put in place to support keeping people healthy throughout their life.
Indicator Components/Enablers: ACCESS, EFFECTIVE, SAFE, PERSON-CENTERED
ORGANIZATIONAL HEALTH – focusing on the health of the organization to support a healthy, sustainable health care system; ensuring the best use of health care resources and value of health care investment.
Indicator Components/Enablers: EFFICIENT, APPROPRIATELY RESOURCED, EMPLOYEE EXPERIENCE, GOVERNANCE
SYSTEM PERSPECTIVE – focusing on working with health care partners and communities to help integrate health services, to support a high quality health care delivery system that is better coordinated and more efficient.
Indicator Components/Enablers: INTEGRATION, COMMUNITY ENGAGEMENT, eHEALTH
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 14
c) Indicator Classifications
The following indicator classifications have been developed for use in all service accountability agreements, including the M-SAA:
Accountability Indicators*
Are included in service accountability agreements and may trigger consequences under the agreement
Will be associated with a target and corridor or at a minimum, have a benchmark (e.g. current level of service must be maintained/decreased, etc.)
May be tied to dedicated funding from the Ministry of Health and Long-Term Care
Are valid, feasible measures of system performance
Allow for comparability across like organizations and/or regions
Explanatory Indicators*
Are complementary indicators to the accountability indicators and will be documented in the technical specifications of the most appropriate accountability indicator(s)
Support planning, negotiation or problem-solving at the provincial, LHIN level or agency level
Support transparency and enable planning discussions
Support of improving and sustaining health system quality, effectiveness and efficiency
Are indicators where data may already be provided through existing reporting systems, and as such health service providers will not be required to report on these through SAA reporting requirements
Will not trigger consequences under the agreement (unless otherwise specified in Performance Improvement Plan or new funding obligations)
Developmental Indicators
Existing indicators that require further validation (review/testing) to ensure quality criteria (e.g. validity, reliability, etc.) are met prior to moving the indicators to accountability or explanatory status in the next agreement*
Will be dropped off the developmental list if the indicator is not ready to be made an accountability or explanatory indicator by the next SAA
Will not be included in the SAAs
*Technical specifications for all accountability and explanatory indicators have been developed in alignment with the ministry Resource for Indicator Standards (RIS). More information on RIS
is available at: http://www.health.gov.on.ca/en/pro/programs/ris/alpha_indicators.aspx
Within the M-SAA, indicators have also been designated as:
Core Indicators: a required indicator relevant to all LHINs and all community sectors;
Sector Specific Indicators: a required indicator relevant to a specific sector;
LHIN Specific Indicators: an indicator determined locally to be relevant.
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 15
d) Target Setting Process
Following the submission of the CAPS, LHINs and HSPs will negotiate the accountability indicator targets appropriate to the organization and local circumstance. Targets are expected to reflect on continuous improvement. Where provincial indicator targets or clinical benchmarks exist, the LHIN and HSPs will take these into consideration.
e) Corridors
All targets established through negotiations between the HSPs and the LHIN will have an associated performance corridor. A corridor is a range around an indicator target that is established for variance reporting purposes. The corridor takes into account expected variation such as statistical and seasonal fluctuations and other factors that affect an accountability indicator. Variances any time during the year that are outside the performance corridor will require a provider report to the LHIN. The report will include the amount of variance, the likely cause, identification of any related risks and the strategies being implemented to address those risks and the overall performance.
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 16
7. Appendix A: Glossary
Terms used throughout these guidelines are defined below. The terms that appear in a single section or part are defined there for ease of reference.
Accountability Agreement means the accountability agreement that must be signed between the LHINs and the Minister pursuant to the terms of the LHSIA. Further information can be found at s.18 of the LHSIA.
Annual Balanced Budget / Balanced Operating Position means that, in a given fiscal year, the total expenses of an entity are less than or equal the total revenue, from all sources, for the entity.
CAPS means Community Accountability Planning Submission which is a document used to negotiate a three year service accountability agreement between the LHIN and HSP.
CMFA means the Commitment to the Future of Medicare Act, 2004. The CMFA contains provisions applicable to SAAs. Further information can be found in Part III of the CFMA. Link to Act: http://www.e-laws.gov.on.ca/html/statutes/english/elaws_statutes_04c05_e.htm
FLS means French Language Services.
FLSA means French Language Services Act. Link to Act: http://www.e-laws.gov.on.ca/html/statutes/english/elaws_statutes_90f32_e.htm
HSP means health service provider as that term is defined in the LHSIA.
IHSP means the Integrated Health Service Plan developed and published by each LHIN pursuant to s.15 of the LHSIA. A copy of a LHIN’s IHSP is available through the LHIN’s office or on its web site.
Integration has the same meaning as is set out in part 1 of the LHSIA, specifically: “integrate” includes (a) to co-ordinate services and interactions between different persons and entities; (b) to partner with another person or entity in providing services or in operating; (c) to transfer, merge or amalgamate services, operations, persons or entities; (d) to start or cease providing services; (e) to cease to operate or to dissolve or wind up the operations of a person or entity; and “integration” has a similar meaning. Further information on integration can be found in Part V of the LHSIA.
LHIN means Local Health Integration Network. The LHINs are 14 networks established by the LHSIA across the province. Specific information about geographic parameters and contact information can be found at www.lhins.on.ca.
LHSIA means the Local Health System Integration Act, 2006. LHSIA is the legislation that established the LHINS, and sets out the terms by which the LHINs may exercise the powers devolved from the Minister in respect of planning, funding and integration of their local health system. Link to the Act: http://www.e-laws.gov.on.ca/html/statutes/english/elaws_statutes_06l04_e.htm
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 17
M-SAA means Multi-sector Service Accountability Agreement. The M-SAA is the service accountability agreement that the LHINs are required to enter into with the HSPs pursuant to the terms of LHSIA. More information on the service accountability agreement can be found in s. 20 of LSHIA and Part III of the CFMA.
Minister means the Minister of Health and Long-Term Care.
MIS means Management Information System. MIS is the term used to identify and report data organized in a format consistent with Ontario Health Care Reporting Standards.
MOHLTC means the Ministry of Health and Long-Term Care.
Multi-year Funding Targets means an allocation for the first fiscal year of the agreement and funding targets for up to two additional years, consistent with the term of the agreement. Funding targets are to be used for planning purposes only and may be revised upward or downward at the discretion of the LHIN.
OHRS means Ontario Healthcare Reporting Standards. The OHRS is a set of reporting standards and chart of accounts consistent with national health care reporting standards.
SAA means a Service Accountability Agreement as that term is defined in the CFMA. SAAs are executed between LHINs and HSPs and include Hospitals (H-SAA), Long-Term Care Homes (L-SAA) and Multi-Sector (M-SAA).
TPBE means Transfer Payment Business Entity. TPBE is a program within the overall funding envelope, e.g. Palliative Care, Substance Abuse, ect.
TPBE TPBE Description
ABI Acquired Brain Injury AO Attendant Outreach ASTHMA ASTHMA CCAC Community Care Access Centre CH Charitable Homes CHC Community Health Centres CHCX CHCX CMH Children’s Mental Health CMHP Community Mental Health Program CMHSH Community Mental Health Supportive Housing CSS Community Support Services DP DP EPC Elderly Persons Centres HNSA Homemaking & Nurses Services Act HOSP Operation of Hospitals IB Interim Beds
CAPS REFERENCE OVERVIEW 2014-17
Community Accountability Planning Submission (CAPS) Reference Overview 2014-17 Page 18
TPBE TPBE Description
MH Municipal Homes NH Nursing Homes OSTEO OSTEO PALC Palliative Care PG Problem Gambling PHOSP Private Hospitals POMS Psychiatric Outpatient Medical Salaries PSW Personal Support Worker- Training Grants SAP Substance Abuse SH Supportive Housing SPH Specialty Psychiatric Hospital
SRI means Self Reporting Initiative. It can be found at https://www.sri.moh.gov.on.ca/UserRegistration/faces/login/index.jsp.