Embed Size (px)
Citation preview

Journal of Clinical Pathology, 1979, 32, 1128-1134
Carcinoma in situ of the male breastF. M. COLE AND A. H. QIZILBASH
From the Departments ofPathology, McMaster University Medical Centre and Henderson GeneralHospital, Hamilton, Ontario, Canada
SUMMARY Two cases of carcinoma in situ of the male breast are described: in one patient it aroseas a complication of gynecomastia; in the other, it occurred 'de novo' and proceeded to infiltrationwith widespread metastases. We reviewed 233 cases diagnosed clinically and histopathologically asgynecomastia to see if we could discover other instances of malignant transformation but none wasfound. Thirty-two cases of infiltrating male breast cancer were also examined. In 11 there wasassociated intraduct change. In only one of the 32 cases was there evidence of associated microscopicgynecomastia.
Carcinoma in situ occurring in the ductal epitheliumof the female breast is a well recognised entity(Carter and Smith, 1977). The analogous lesion inthe male breast, however, is rarely recorded. Wedescribe two patients with this condition. One patientpresented with a breast mass which proved to becarcinoma in situ. This was excised, but an in-filtrating carcinoma later developed at or near thesite of the original excision. The second patientpresented with classical gynecomastia. Histologicallythis showed gynecomastia with focal areas of in situmalignancy superimposed.As a result of these findings we evaluated 32 cases
of infiltrating cancer of the male breast in an attemptto determine how frequently, if ever, the in situductal change coexisted with an infiltrating lesion,and we also examined 233 cases of gynecomastia tofind out if other patients showed a similar transitionfrom benign epithelial hyperplasia to carcinoma insitu.
Case reports
CASE IA 64-year-old man presented in June 1968 witha slightly bloodstained discharge from the rightnipple which had been present for about one week.He also complained of a small, firm, painless mass,about 1 cm in diameter, which was situated 1 cmmedial to the nipple. This had been present forabout six months. His past health had been goodapart from long-standing chronic bronchitis andemphysema. A general physical examination revealed
Received for publication 30 April 1979
no abnormality apart from the breast lesion whichwas excised through a subareolar incision.
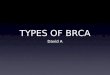
Pathological findingsThe specimen consisted of a portion of fibrofattytissue measuring 3 x 2 x 1 cm, in which there wasan ill-defined mass, 1 x 1 x 1 cm. On sectiondilated ducts could be identified, and gentle pressureresulted in soft, grey-white material exuding fromthe ducts. Microscopically the dilated ducts werefilled with epithelium and comedones (Fig. 1). Theepithelium was many layers thick and thrown intopapillary projections which in places completelyfilled the duct lumen. Calcification was presentwithin the amorphous comedones, within theepithelium, and in the adjacent stroma. The epithelialcells showed marked atypia with variations in nuclearsize, shape, and staining properties (Fig. 2). Mitoticfigures were frequent-3 or 4 per high-power field.Many were atypical in form. The stroma was denseand acellular with no periductular loose fibroustissue. Serial histological sections were prepared(5 microns thick) through the entire mass, and one inevery 20 was stained and examined. At no point wasthere any evidence of infiltration. The findings wereinterpreted as showing intraduct carcinoma in situwith no evidence of previous gynecomastia orinfiltration.
Subsequent courseThe patient was seen again in 1972 with anothermass situated beneath the previous surgical incision.There was no clinical evidence of axillary lymph nodeor distant metastases. The mass measured 2 x 1 x1 cm and was hard and ill-defined. Microscopically
1128
copyright. on A
ugust 27, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.11.1128 on 1 N
ovember 1979. D
ownloaded from

Carcinoma in situ of the male breast
Fig. 1 Dilatedducts filled withcomedones andpapillary epithelium.Haematoxylin and
s eosin x 40
Fig. 2 High-powerdetail of the epitheliumwhich is many layersthick with markedcytological atypia andcalcifications. H andE x 500
1129
copyright. on A
ugust 27, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.11.1128 on 1 N
ovember 1979. D
ownloaded from

F. M. Cole and A. H. Qizilbash
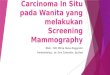
there was an extensive infiltrating duct carcinomawhich was provoking a brisk fibrous tissue stromalresponse (Fig. 3). There was no evidence of residualintraduct change. Five lymph nodes showed non-specific, reactive hyperplasia only with no sign ofmetastases. A further local recurrence occurred in1972 and 1974, and again it was removed togetherwith nine lymph nodes, all of which contained meta-stases. In 1975 the patient had a pathological fractureof the left hip. This was treated by pinning andplating. Tissue removed from the fracture site con-tained metastatic tumour of similar appearance tothe breast tumour. A radiological survey demon-strated metastatic lesions in the sternum and tworibs. A bilateral orchidectomy was carried out. Hewas seen in the follow-up clinic until 1976 duringwhich time his response to therapy was good, but hewas then lost to follow-up.
CASE 2A 32-year-old man was admitted with a mass in theright breast which had been present for about sixmonths. There was no discharge or pain. His generalhealth was excellent and he was receiving nomedication. His previous medical history was non-contributory. The mass was situated immediatelybeneath the nipple and measured 3 x 2 cm. It wasfirm and movable with no attachment to muscle.There was some tenderness to palpation but no pain.
The other breast was normal. A general physicalexamination revealed no abnormality. The mass wasr_moved and the left nipple was left intact.
Pathological findingsThe specimen consisted of a firm, rubbery disc oitumour, 3 cm in diameter and 2 cm thick. It was cutinto 3 mm slices and blocked. Microscopically thechanges were predominantly gynecomastia (Fig. 4).The stroma in the periductal areas was hyperplasticand loosely arranged, and the ducts showed elon-gation and branching. There was very markedepithelial proliferation, together with areas in whichthe ducts were almost completely obliterated. Therewas loss of nuclear polarity and marked pleo-morphism and hyperchromatism (Fig. 5). Mitoticfigures, both normal and abnormal, were plentiful(5 to 6 per high-power field), and occasional foci ofcalcification were seen. These appearances wereinterpreted as representing in situ carcinomatouschange. Serial histological sections were cut andone in 20 was stained and examined. No infiltrationwas evident. The pathological diagnosis wasgynecomastia of the florid type with superimposedareas of intraduct carcinoma. All residual breasttissue was then excised together with five axillarylymph nodes. Examination of the remainder of thebreast tissue showed changes similar to that seen inthe original material. There were no metastases in
Fig. 3 Details ofinfiltrating duct carcinoma.
i_;: ~~~H and E x 125
1130
copyright. on A
ugust 27, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.11.1128 on 1 N
ovember 1979. D
ownloaded from

Carcinoma in situ of the male breast
Fig. 4 Low-powerview showing changesofgynecomastia. Hand E x 30
Fig. 5 High-power viewshowing almost completeobliteration of the duct,loss of nuclear polarity,and marked nuclearatypicality. H andE x 300
1131
copyright. on A
ugust 27, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.11.1128 on 1 N
ovember 1979. D
ownloaded from

F. M. Cole and A. H. Qizilbash
the lymph nodes. He was seen one year after surgeryand at that time had no signs or symptoms ofrecurrence.
Review of 233 cases of gynecomastia and 32 casesof infiltrating cancer
Two hundred and thirty-three cases of gynecomastiaon file were reviewed. The histological criteria ofWilliams (1963) were used, and all cases fell intoone of two types described by her.
TYPE 1The florid type is characterised by increased numbersof ducts, in some cases showing pseudolobularformation. The ducts have irregular lumens, and theepithelium consists of three or more layers withsmall papillae. Around the ducts there are cuffs ofloose connective tissue, and these are well de-marcated from the stroma, which is increased involume and consists of dense collagen tissue withvarying fibroblastic proliferation.
TYPE 2The quiescent type is characterised by slightlyincreased numbers of ducts with irregular lumens andoften slight ectasia. Little or no proliferation of theepithelium is present. There is no loose connectivetissue around the ducts, and the stroma extends as
far as the basement membrane of the ducts. Thestroma is increased in volume without pronouncedfibroblastic activity and often with hyalinisation.The cases of the florid type often show brisk
epithelial proliferative changes, but in no case didthese changes even approach the degree ofcytologicalabnormality and mitotic activity, both normal andabnormal, that were seen in the present case 2. Inno case was there evidence of the calcific foci.
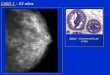
Thirty-two cases of infiltrating breast cancer werereviewed. Detailed accounts of both clinical andpathological features of large series have beendescribed by other authors (Crichlow, 1972; Hollebet al., 1968; Liechty et al., 1967; Norris and Taylor,1969; Scheike, 1975; Visfeldt and Scheike, 1963)and will be discussed here only in relation to severalrelevant findings. Of the 32 tumours, 23 were poorlydifferentiated infiltrating duct cancers. Four showedclear glandular differentiation, two were classified asencephaloid cancers, two were predominantly pap-illary, and one was mucinous. Eleven of theinfiltrating lesions showed a clearly defined intra-duct component (Fig. 6). In eight of these 11 casesthe intraduct lesions were of the comedo type, andall showing this type of change also showed focalcalcification occurring either within the epitheliumor in the comedones. In one of the 32 tumours theadjacent breast tissue showed gynecomastia also.
Fig. 6 Intraductcarcinoma withadjacent infiltratingcancer. H andEx 80
1132
copyright. on A
ugust 27, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.11.1128 on 1 N
ovember 1979. D
ownloaded from

Carcinoma in situ of the male breast 1133
Discussion
Carcinoma in situ is a rare lesion whether arising'de novo' in the male breast ducts, as in case 1, or inassociation with gynecomastia, as in case 2. Littlemention is made in the literature regarding the'de novo' in situ lesion. In many large comprehensivestudies dealing with male mammary cancer (Crich-low, 1972; Holleb et al., 1968; Liechty et al., 1967;Norris and Taylor, 1969; Scheike, 1975; Visfeldtand Scheike, 1963) intraduct cancer without aninfiltrating lesion is either not mentioned or it isspecifically stated that it was not seen. One study(McDivitt et al., 1968) makes passing mention of thein situ lesion, stating that it is entirely similarhistologically to that seen in the female breast butno further details are given. In our study of 32 casesof infiltrating duct cancer, there were 11 cases inwhich there was accompanying intraduct cancer inthe ducts of the adjacent breast tissue. This might beregarded as evidence supporting the origin ofinfiltrating lesions from a preceding intraductcarcinoma. If infiltration is preceded by intraductchange then the infrequency with which it is seenmight reflect a very short phase which occurs beforeinfiltration takes place. It is of some interest to notethat, of the 11 cases in which intraduct change wasseen in association with infiltration, in eight cases itwas of the comedo type and in all eight cases therewas microscopic calcification. This feature was alsoseen in cases 1 and 2 but not in the cases comprisingthe series of gynecomastia.
There is some epidemiological and histopatho-logical evidence of a relationship between gyne-comastia and cancer but there is almost unanimousagreement that this association is probably rare.Patients with conditions in which clinical gyne-comastia is a feature appear to suffer a higherincidence of breast cancer. Bilharzia damages theliver and causes hyperoestrogenism with gynecom-astia in men. The disease is common in Egypt, and itis claimed that male breast cancer constitutes about5 % of all breast malignancies, a far higher incidencethan is encountered in other countries (El Gazayerliand Abdel-Aziz, 1963).Among 21 cases of male breast cancer, Jackson
et al. (1965) found three patients with Klinefelter'ssyndrome and considered there may be a relationshipbetween this syndrome in which gynecomastia isa feature and mammary cancer. They claimed thatthis represents a vastly increased incidence whencompared with non Klinefelter males. Gynecomastiaand breast cancer have also followed administrationof oestrogens for prostatic cancer (Abramson andWarshawsky, 1948; Howard and Grosjean, 1948;O'Grady and McDivitt, 1969) but, considering the
extensive use of oestrogens for this condition, thiscomplication rate must be regarded as almostnegligible.
Microscopic gynecomastia occasionally showsflorid and sometimes worrisome epithelial hyper-plasia but only occasionally has definite malignantchange been documented. Authors who have studiedlarge numbers of cases (Karsner, 1946; Lyall, 1947;Wheeler et al., 1954; Sirtori and Veronesi, 1957;Williams, 1963; Haagensen, 1971) have encounteredthis change only once or at the most on two occasions.Nevertheless, McDivitt et al. (1968) mention a smallgroup in which the epithelial atypicality is somarked that a firm differentiation between hyper-plasia and in situ cancer cannot be made. In thepresent study, case 2 showed these abnormalities toa degree far in excess of the other 233 cases reviewed.The infrequency of this coexistence is also supportedby our own observations that, of the 32 cases ofinfiltrating cancer, in only one instance was thereassociated histological gynecomastia.
We thank the many pathologists who allowed us toexamine the pathological material. We also thankMrs Jackie Rowan who typed the manuscript.
References
Abramson, W., and Warshawsky, H. (1948). Cancer ofthebreast in the male, secondary to estrogenic admin-istration. Journal of Urology, 59, 76-82.
Carter, D., and Smith, R. R. L. (1977). Carcinoma in situof the breast. Cancer, 40, 1189-1193.
Crichlow, R. W. (1972). Carcinoma of the male breast.Surgery, Gynecology and Obstetrics, 134, 1011-1019.
El Gazayerli, M. M., and Abdel-Aziz, A. S. (1963). Onbilharziasis and male breast cancer in Egypt. BritishJournal of Cancer, 17, 566-571.
Haagensen, C. D. (1971). In Diseases of the Breast, 2ndedition, pp. 76-85. Saunders, Philadelphia and London.
Holleb, A. I., Freeman, H. P., and Farrow, J. H. (1968).Cancer of the male breast. Part 2. New York StateJournal of Medicine, 68, 656-663.
Howard, R. R., and Grosjean, W. A. (1948). Bilateralmammary cancer in a male coincident with prolongedstilbestrol therapy. Surgery, 25, 300-303.
Jackson, A. W., Muldal, S., Ockey, C. H., and O'Connor,P. J. (1965). Carcinoma of male breast in associationwith Klinefelter syndrome. British Medical Journal, 1,223-225.
Karsner, H. T. (1946). Gynecomastia. American JournalofPathology, 22, 235-315.
Liechty, R. D., Davis, J., and Gleysteen, J. (1967).Cancer of the male breast: forty cases. Cancer, 20,1617-1624.
Lyall, A. (1947). Chorioncarcinoma of the testis withgynaecomastia: report of a case with early breastcancer. British Journal of Surgery, 34, 278-280.
copyright. on A
ugust 27, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.11.1128 on 1 N
ovember 1979. D
ownloaded from

1134 F. M. Cole and A. H. Qizilbash
McDivitt, R. W., Stewart, F. W., and Berg, J. W. (1968).Tumors of the Breast (Atlas of Tumor Pathology,Second Series, fasc. 2), pp. 106-109. Armed ForcesInstitute of Pathology, Washington, DC.
Norris, H. J., and Taylor, H. B. (1969). Carcinoma of themale breast. Cancer, 23, 1428-1435.
O'Grady, W. P., and McDivitt, R. W. (1969). Beast cancerin a man treated with diethylstilbestrol. Archives ofPathology, 88, 162-165.
Scheike, 0. (1975). Male breast cancer. Acta Pathologicaet Microbiologica Scandinavica, Supplement, 251, 3-35.
Sirtori, C., and Veronesi, U. (1957). Gynecomastia.Cancer, 10, 645-654.
Visfeldt, J., and Scheike, 0. (1963). Male breast cancer.Cancer, 32, 985-990.
Wheeler, C. E., Cawley, E. P., Gray, H. T., and Curtis,A. C. (1954). Gynecomastia. Annals ofInternal Medicine,40, 985-1004.
Williams, M. J. (1963). Gynecomastia. American Journalof Medicine, 34, 103-112.
Requests for reprints to: Dr F. M. Cole, Section ofLaboratory Medicine, McMaster University MedicalCentre, 1200 Main Street West, Hamilton, Ontario,L8S 4J9, Canada.
copyright. on A
ugust 27, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.11.1128 on 1 N
ovember 1979. D
ownloaded from