Embed Size (px)
DESCRIPTION
Management of Carcinoma Nasopharynx
Citation preview

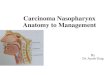
Carcinoma Nasopharynx
Moderator: Dr Sushmita Ghoshal

Department of Radiotherapy, PGIMER, Chandigarh
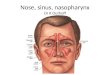
Anatomy

Department of Radiotherapy, PGIMER, Chandigarh
Anatomy
Foramen lacerum
Foramen spinosum
Foramen ovale
Foramen rotundum

Department of Radiotherapy, PGIMER, Chandigarh
Parapharyngeal Space
• The parapharyngeal space is located deep within the neck lateral to the pharynx and medial to the ramus of the mandible.
• Shape of an inverted pyramid with the floor at the skull base and it’s tip at the greater cornu of the hyoid bone
• Two compartments :– Prestyloid– Retrostyloid
Retrostyloid Space
Prestyloid Space

Department of Radiotherapy, PGIMER, Chandigarh
Lymphatic Drainage• Richest lymphatic plexus in the head
and neck region.• Submucosal lymphatics congregate at
the pretubal region – “pretubal plexus”.• These then pass on to the
retropharyngeal nodes as 8 -12 trunks which decussate in the midline.
• Lymphatic trunks pierce the level of the base of the skull and run between the pharyngobasilar fascia and the longus capitis.
• The lymphatic trunks drain in three directions:– To the retropharyngeal nodes.– To do the posterior cervical nodal and
the confluence of the 11th, cranial nerve and the jugular lymph node chains, situated at the tip of the mastoid.
– To the Jugulo-digastric nodes (Lederman )

Department of Radiotherapy, PGIMER, Chandigarh
Anatomy: RPLN• The retropharyngeal nodes are
present in two groups.– Median group.– Lateral group.
• The median group consists of 1 - 2 nodes interconnected in the midline.
• The lateral group consists of 1- 3 nodes located between the lateral aspect of the posterior pharyngeal wall and the carotid artery.
• These nodes are present from the vertebral levels C1- C3.
• The superior-most lymph node of the latter group is also known as the node of Rouviere.
• This node lies in front of the arch of the Atlas being separated from it by the longus colli muscle.

Department of Radiotherapy, PGIMER, Chandigarh
CT anatomy

Department of Radiotherapy, PGIMER, Chandigarh
Incidence

Department of Radiotherapy, PGIMER, Chandigarh
Incidence: Sex

Department of Radiotherapy, PGIMER, Chandigarh
Clinical Features• Most common: Asymptomatic cervical
lymphadenopathy (87%)• MC node involved is the posterior deep cervical (direct
drainage from the lateral pharyngeal)• Other presenting symptoms:
– Nasal twang to speech– Unilateral serous otitis media ( in adults)– Cranial nerve palsy:
• U/L Cr nv. II to VI (petrosphenoidal syndrome of Jacod)
• U/L Cr nv. XI to XII ( Retroparotid syndrome of Villaret.)
• Cr nv V and VI most commonly involved. • Cr nv I, VII and VIII rarely involved.
– Sore throat : Oropharyngeal extension– Pain: Compression of Vth cranial nerve ( facial pain)– Trismus: Mandibular nerve involvement or pterygoid
muscle invasion.

Department of Radiotherapy, PGIMER, Chandigarh
Cranial Nerve involvement
0
5
10
15
20
25
30
35
40
45
50
I II III IV V VI VII VIII IX X XI XII
Lederman et al Leung et al

Department of Radiotherapy, PGIMER, Chandigarh
Local Spread
Nasal cavity & PNS
Orbital invasionBase of Skull, Clivus
Sphenoid sinus
Cavernous Sinus
Lateral Parapharyngeal space
Middle ear cavity
Oropharynx (tonsillar pillars)
C1 vertebrae

Department of Radiotherapy, PGIMER, Chandigarh
Nodal Spread

Department of Radiotherapy, PGIMER, Chandigarh
Etiology
Normal Epithelium
Low Grade Dysplasia
High Grade Dysplasia
Invasive Carcinoma
Metastatic Carcinoma
P53 Mutation
Gain Chromosome 12
Deletion 11 and 13
Deletion of Chromosomes 3p and 9p
Inactivation of Chromosome p14, 15 and 16
EBV infection

Department of Radiotherapy, PGIMER, Chandigarh
Investigations
• Staging:– CT– MRI– Endoscopy– PET scan– Chest Xray– USG Abdomen– Bone Scans
• Other Investigations– EBV Serology

Department of Radiotherapy, PGIMER, Chandigarh
Staging
• Several staging systems are in use:– Complex anatomy and spread patterns– Lack of international consensus:
• Separate Chinese, Hong Kong and American staging systems
• Systems available:– Fletcher (1967)– Ho’s staging (1978)– IUAC (1988)– Huaqing staging (1994)– AJCC (2002)

Department of Radiotherapy, PGIMER, Chandigarh
Comparison System Staging
T1 T2 T3 T4
Fletcher (1967)
< 1 cm diameter
> 1 cm but confined to
nasopharynx
Beyond nasopharynx
Involving skull base or cranial
nerves
Ho (1978)
Confined to
nasopharynx
Extending to nasal fossa or oropharynx
Bone/ Cranial nerve/ orbital / hypopharyngea
l / infratemporal
fossa involvement
NA
IUAC (1988)
Limited to one site in nasophary
nx
Extending to two sites in
nasopharynx
No bony destruction
Bony destruction including
eustachian tube
Huaqing (1994)
Limited to nasophary
nx
Involving the nasal cavity, oropharynx,
anterior cervical vertebrae, PPS before SO line
Pterygoid process / posterior
cranial nerve / posterior cervical
vertebrae / BOS / PPS beyond SO
line
Infratemporal fossa /
cavernous sinus / PNS /
direct invasion of C2 or C1 /
anterior cranial nerves

Department of Radiotherapy, PGIMER, Chandigarh
Ho’s vs AJCC

Department of Radiotherapy, PGIMER, Chandigarh
AJCC system: T staging
• T1: – Tumor confined to the nasopharynx
• T2: – Tumor extends to soft tissues
• T2a : Extends to the oropharynx or the nasal fossa
• T2b : With parapharyngeal extension
• T3: – Tumor invades bony structures and/or paranasal
sinuses
• T4: – Tumor with intracranial extension and/or
involvement of cranial nerves, infratemporal fossa, hypopharynx, orbit, or masticator space

Department of Radiotherapy, PGIMER, Chandigarh
AJCC system: N staging• N0:
– No regional lymph node metastasis
• N1: – Unilateral metastasis in lymph
node(s), < 6 cm in greatest dimension, above the supraclavicular fossa
• N2:– Bilateral metastasis in lymph
node(s), < 6 cm in greatest dimension, above the supraclavicular fossa
• N3:– N3a: Metastasis in a lymph
node(s) >6 cm – N3b: Extension to the
supraclavicular fossa
Ho’s Triangle

Department of Radiotherapy, PGIMER, Chandigarh
Staging: AJCC 2002
Stage I Stage IIA Stage IIB
Stage III Stage IVA Stage IVB

Department of Radiotherapy, PGIMER, Chandigarh
Pathology
• Some authors consider carcinomas to be of two types:– Keratinizing – Non keratinizing
• Others consider carcinomas to be of 4 types:– Keratinizing Squamous– Non Keratinizing Squamous– Lymphoepithelioma– Undifferentiated carcinomas
• WHO 3 types:– Type I : SCC– Type II : Non Keratinizing carcinoma– Type III : Undifferentiated carcinoma

Department of Radiotherapy, PGIMER, Chandigarh
Endemic NPC• Known to occur in China, Hong Kong, South Eastern
Asia, Greenland• Associated with EBV virus infection• In India similar pathology seen in Kashmiris.• Present a decade younger.• Not associated with smoking or alcohol consumption• Associated with undifferentiated carcinoma ( WHO II and
III)• Associated with more advanced disease at presentation• Nodal stage also more advanced and more frequently
involved.• Both chemo and radio sensitive
– Histologically more vascularized (Better Rx response)– Greater % of cell in the growth fraction.
• Better loco regional control and survival than sporadic variants.
• Several markers for predicting biological behavior

Department of Radiotherapy, PGIMER, Chandigarh
Prognostic factors• Most important stage.• Parapharyngeal extension is associated with a
poorer prognosis.• A Chinese series found that 4th cranial nerve
involvement – poor prognosis.• Nodal disease status:
– Bilateral cervical lymphadenopathy – Supraclavicular lymphadenopathy – Lymph node fixity
• Lymphoepithelioma histology: better prognosis• Undifferentiated histology: better prognosis• Molecular markers:
– Ki -67 over expression– P 53– E – cadherin expression

Department of Radiotherapy, PGIMER, Chandigarh
Treatment strategyStage
Early stage
Late stageExternal Radiation EBRT + ICBT
KPS > 70 KPS < 70
Concurrent Chemoradiation
Palliative Radiotherapy

Department of Radiotherapy, PGIMER, Chandigarh
Dose response
• Significant dose response relationship exists.
• Several series demonstrate that an increased-dose leads to better survival– Doses of 90 Gy delivered by boost increase
the local control and the distant metastasis free rate significantly over doses > 70 Gy
– Price however paid in increased morbidity
• Local recurrence rate reduced with the use of larger fields (Field size more than 250 cm2 associated with a doubling of local control as compared to field size of 100 cm2)

Department of Radiotherapy, PGIMER, Chandigarh
Dose-response
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
50 - 60 Gy 60 - 67.5 Gy > 67.5 Gy
T1
T2
T3
T4

Department of Radiotherapy, PGIMER, Chandigarh
Doses used• Radical radiotherapy:
– 60 – 66 Gy in 2 Gy per fraction over 6 – 6 ½ weeks
– Higher dose can be given with more conformal techniques:
• ICBT• IMRT• 3 DCRT
– In our patients with poor nutrition, advanced disease and absence of individualized care split course radiotherapy is an alternative
• 35 Gy in 15 # • 25 – 30 Gy in 10 – 15 # after 2-3 weeks
• Palliative radiotherapy:– 30 Gy / 10#– 20 Gy / 5#– 800 -1000 cGy single fraction

Department of Radiotherapy, PGIMER, Chandigarh
Treatment volume• The nasopharynx.• Posterior 2 cm of nasal cavity.• Posterior ethmoid sinuses.• Entire sphenoid sinus and the basiocciput• Cavernous sinus.• Base of skull, including the foramen ovale,
carotid canal and foramen spinosum.• Pterygoid fossae• Posterior 1/3rd of maxillary sinus.• Lateral and posterior oropharyngeal wall to
the level of mid-tonsillar fossa? Posterior 1/4th of orbit ( Fletcher – YES,
Perez - NO )

Department of Radiotherapy, PGIMER, Chandigarh
Nodal volumes
• The entire neck is at high risk for microscopic spread of disease.
• The neck nodes that should be treated are:– Upper deep jugular– Submandibular– Jugulodigastric– Midjugular– Posterior cervical– Retropharyngeal

Department of Radiotherapy, PGIMER, Chandigarh
Treatment planning
• Positioning:– Supine position.– Head should be extended
• Immobilization– To ensure accuracy in setup patient should be
immobilized with a custom-made thermoplastic cast.
• Localization:– All nodes are delineated with the use of radio –
opaque lead wires.– The outer canthus the eye opposite to which
simulation film is taken is marked with a lead wire.– Tumor localization performed with the help of CT
and clinical details.

Department of Radiotherapy, PGIMER, Chandigarh
Techniques• Techniques
– Conventional technique– Three-dimensional conformal radiation therapy.– Intensity-modulated radiotherapy.– Image-guided radiotherapy.
• Energy selection:– Co60 : 1.25 MeV– LINAC : 4 – 6 MV– Higher-energies used in certain Western
centers during the boost phase to:• Reduce dose to the mandible,
temporomandibular joints, ears and subcutaneous tissue (lateral edge effect)
– Kutcher and associates however warn that use of these high energy beams may be associated with underdosage near the surface and near the paranasal sinus cavities.

Department of Radiotherapy, PGIMER, Chandigarh
Portal selection
• For Initial Phase:– Two parallel opposing fields– Three field approach
• For the boost phase:– Fletcher’s Technique ( 4 fields – antral
boost)– Anterolateral wedge pair technique– Ho’s technique ( with separate
parapharyngeal boost)

Department of Radiotherapy, PGIMER, Chandigarh
Two field technique
• Clinical field markings:– Superior border:
• 2.5 cm above the zygomatic arch• 5 cm above the zygomatic arch in case of
intracranial extension– Anterior border:
• 2 cm beyond the anterior most extent of the disease (usually placed just along the lateral canthus of the eye)
– Posterior border:• Along the tip of the mastoid or behind the
posterior most extent of cervical lymphadenopathy
– Inferior border:• Along the superior border of the clavicle

Department of Radiotherapy, PGIMER, Chandigarh
Two Field technique• Radiological boundaries:
– Superior border:• Splitting the pituitary fossa and extending
along the superior surface of the sphenoid sinus• In case of IC extension to include at least 1 cm
above the pituitary fossa.– Anterior border:
• At least 2 cm of the nasal cavity and maxillary antrum.
• At least 2 cm margin to the gross tumor extent– Posterior border:
• Kept open if gross cervical LAD• Else match with tips of spinous processes of the
cervical vertebrae.

Department of Radiotherapy, PGIMER, Chandigarh
Technique

Department of Radiotherapy, PGIMER, Chandigarh
Three field technique
• The superior, anterior and posterior boundaries are kept as same.
• Inferior boundary restricted to the level of the thyroid notch unless cervical LAD is present
• In latter case matching done more inferiorly.
• Dose prescription done usually at 3 cm depth.
• Several measures need to be taken to circumvent the problem of field matching

Department of Radiotherapy, PGIMER, Chandigarh
Field Matching• Without asymmetrical jaws:
– Using laryngeal block:• A laryngeal block is placed at the level of the larynx.• The block has a thickness such that it is located 1cm
medial to the lateral border of thyroid cartilage• The block extends from the superior border of the
lower field to 2 cm below the level of the cricoid cartilages.
– Using collimator tilt:• A collimator rotation may be given for the lateral
fields to counteract the divergence of the lower anterior field – 5° for Co 60.
• May increase the dose to the supero-anterior portion of the field where the eyes are located
• With asymmetrical jaws: – Using an isocentric technique with half beam block for 3
fields overdosage at the field junction can be avoided.– Alternative is to use half beam block in the lower
anterior field only and use a small shield of 1 – 2 cm in midline to shield the spinal cord.

Department of Radiotherapy, PGIMER, Chandigarh
Additional modifications
• In both 3 field and 2 field techniques a higher dose can be given to the eye due to the beam divergence.
• Lateral fields need to angled – a “posterior” tilt needs to be given
• Magnitude by which the field edge shifts at the midline ( for Co60)– 5° – 0.5 cm– 10° – 1.2 cm
5° 10°
1.20.5
1.1
2.5

Department of Radiotherapy, PGIMER, Chandigarh
Actual Implementation
270°
5°
275°
Lateral Canthus

Department of Radiotherapy, PGIMER, Chandigarh
Doses Prescribed
• 40 – 44 Gy in 2 Gy per fraction over 20 – 22 fractions ( 4 – 4½ weeks) for the entire field.
• Rest of the dose ( 20 – 26 Gy) to delivered with spine shielding:– Lateral fields:
• Posterior border drawn along the junction of the posterior 1/3rd and the anterior 2/3rd of the vertebral bodies ( Co60).
• In LINACs the posterior edge of the vertebrae may be choosen.
• Clinically marked straight along the lobule of ear.
– Anterior fields:• 2 cm wide midline shield is adequate.

Department of Radiotherapy, PGIMER, Chandigarh
Boosting neck nodes
• Photons only:– Antero-posterior glancing fields ( ± wedges)
– Medial border is 2 cm from midline.– Additional boost radiation may be delivered
by posterior fields to increase the dose to the posterior cervical nodes after the course of RT is completed.
• Electrons:– Direct abutting lateral fields used.– Energy selected 9 MeV– Prescribed at 85% isodose ( Usually 3 cm
depth)– 6 x 6 cm usually adequate– Treated at extended SSD of 110 cm

Department of Radiotherapy, PGIMER, Chandigarh
Nasopharynx Boost• A 4 field approach can be used to boost
the nasopharynx to additional 10 – 15 Gy.• Volume treated is roughly cuboidal and
has the dimensions of 7 cm x 6 cm.• The anterior fields are tilted “medially”
by 20° – 30° in order to – Increase the dose to the Posterior
nasopharynx– Spare the anterior nasal cavity and the
deeper brain-stem
• Opposing lateral fields also used with lower border at the level of angle of mandible.

Department of Radiotherapy, PGIMER, Chandigarh
Field marking
• The boundaries for the anterior facial fields are:– Superiorly – below the eyeball– Medially – 1 cm in either side of midline– Inferiorly – upto the commissure of lips– Laterally – Usually a distance of 6 cm – allow beam
fall-off.
• In order to ensure that the superior border of the anterior field matches the lateral fields the head position is adjusted (hyperextended) based upon the collimator lights.
• Beam weights are adjusted to ensure that the brain doesn't receive excess dose.– Anterior : Lateral = 33% : 66%

Department of Radiotherapy, PGIMER, Chandigarh
4 field technique

Department of Radiotherapy, PGIMER, Chandigarh
Dose distribution

Department of Radiotherapy, PGIMER, Chandigarh
Nasopharynx Boost
• In case of gross anterior extension:– Three field, lateral wedge pair arrangement is
preferred – Anterior border of the lateral fields are extended
to cover the anterior disease adequately– Alternative technique is to use differential beam
weights– Electrons may be used to supplement the doses to
the anterior diseases with lateral photon fields.
• In lateralized anterior extension:– Anterior field may be “wedged” with thin end
towards side where disease is present.
• In inferior extension:– Boost fields are by necessity parallel opposing.

Department of Radiotherapy, PGIMER, Chandigarh
Ho’s Technique• Proponent: Prof John H C Ho • Developed: late 1960s• Extensive experience : 3 decades• Special features:
– Different CTV specification – Field arrangements and patient position are
different.– Arrangement of different shields specified based
upon bony anatomy – customized shields not necessary.
– Reproducible treatment plan.– Lack of CT planning facilities circumvented.– Ease of use in a busy radiotherapy department Cost
saving additional factor.• Over 10,000 patients have been treated in
Hong Kong – excellent long term results in early disease T1, T2 and T3.

Department of Radiotherapy, PGIMER, Chandigarh
Ho’s technique: Planning
• Patient is immobilized in FLEXED head position in the initial phase.
• Similar to the planning technique for pituitary.
• Allows easier shielding of the brainstem and the oral cavity and reduces the field size requirements.
• Dose: 40 Gy in 20 #

Department of Radiotherapy, PGIMER, Chandigarh
Ho’s technique: Planning
• Three field arrangement:– Opposed lateral fields
irradiate the upper cervical lymphatics ( upto level III) en bloc.
– An anterior field irradiates the lower field.
– Shielding of the lateral fields is done to adjust for the beam overlap with the anterior field.
– In the lower anterior field a midline shield is placed throughout the treatment.
Below vocal cords C6
0.5 cm above the anterior clinoid process
Bisecting the maxillary antrum

Department of Radiotherapy, PGIMER, Chandigarh
Ho’s technique: Planning• Specialized arrangement of
shielding is done for all patients.– Brain Stem: Shielded with 5
HVL block placed in a manner such that it is 0.5 cm behind the upper edge of the clivus and 1 cm below the lower edge.
– Eye: 5 HVL shield placed 1.5 cm behind the lateral canthus.
– Posterior tongue also shielded with standard block.
– Pituitary and temporal lobes: upper half of the pituitary fossa shielded.

Department of Radiotherapy, PGIMER, Chandigarh
Ho’s technique: Planning• In the boost phase a 3 field
arrangement was used.• Patient was replanned in the
EXTENDED head position with oral stent.
• Anterior cervico-facial field was used in all patients
• Lower border of the later fields reduced down to level of angle of mandible.
• Allowed dose reduction to: TM joints, ear, parotids & pinnae.
• Dose prescribed: 22.5 Gy in 9 #
• Total tumor dose was 62.5 Gy in 29#
• Biologically equivalent to 66 Gy in 33#

Department of Radiotherapy, PGIMER, Chandigarh
Ho’s technique: Planning• In patients with
parapharyngeal disease a posterior oblique boost was given after the 2nd phase.
• Dose prescribed was 20 Gy /10#
• This field was usually 5.5 cm x 8 cm in size.
• Ascending ramus of the mandible was shielded in this phase.

Department of Radiotherapy, PGIMER, Chandigarh
Ho’s vs 3D CRT and IMRT
T1 NO MO
T4 N2 MO
Kam et al: IJROBP 2003

Department of Radiotherapy, PGIMER, Chandigarh
Results by Ho’s Technique

Department of Radiotherapy, PGIMER, Chandigarh
Conventional Radiation

Department of Radiotherapy, PGIMER, Chandigarh
Conventional Radiation

Department of Radiotherapy, PGIMER, Chandigarh
Altered fractionation
• Concomitant boost technique has been evaluated in a large series by Teo et al (IJROBP 2000).
• Study prematurely terminated as:– 40% incidence of temporal lobe neuropathy– 17% incidence of cranial nerve palsies– 50% patients had one or other form of
neurological complication– 2.6% treatment related mortality– Neural complications were more severe
and occurred earlier than conventional techniques.
– No difference in outcome

Department of Radiotherapy, PGIMER, Chandigarh
Conformal Radiation• Includes 3 D CRT , IMRT and IGRT• Potential:
– Dose escalation – Conformal avoidance
• Results are immature for IMRT• Largest series of IMRT by Kam et al:
– 63 patients – Median F/U 30 months– Only 4 had local failure ( None marginal miss)– OS was 90%– Distant metastasis primary cause of failure– Grade III mucositis: 41% patients– Late toxicity till 2 yrs : Xerostomia (21%)

Department of Radiotherapy, PGIMER, Chandigarh
Brachytherapy
• The following requirements should be fulfilled prior to taking up a patient for brachytherapy:– Tumor thickness less than 10 mm.– Absence of intracranial, paranasal sinus and
oropharyngeal involvement.– Absence of involvement of underlying bone or
infratemporal fossa.– Absence of metastatic disease.– Expertise in nasopharyngeal intracavitary
brachytherapy.
“In effect, nasopharyngeal brachytherapy is ineffective in tumors extending beyond the
nasopharynx” -Xiao-Kang Zheng

Department of Radiotherapy, PGIMER, Chandigarh
Techniques• Techniques:
– Temporary intracavitary application– Temporary interstitial implantation– Permanent interstitial implantation
• Dose-rates used:– Low dose rate (LDR).– High dose rate (HDR).
• Situations used:– Routine use as a boost after XRT ( Hong Kong,
China and Netherlands)– Use with documented residual disease ( USA)– Recurrence ( Hong Kong, USA - Syed and Chinese
Series)

Department of Radiotherapy, PGIMER, Chandigarh
History of brachytherapy• In 1920s, Pierquin and Richard
were the first persons is to employ brachytherapy in the treatment of nasopharyngeal carcinomas.
• In the Christie hospital at Manchester, Peterson used a 15 mg radium tube inserted in a cork with a diameter of 15 to 20 mm.
• The dose prescribed was 80 rads in seven days to a depth of 0.5 cm.
Peterson described this technique as a useful alternative to small
field X-ray technique but not superior to the use of X-rays
Cork Ra226 tube
String at either end of the cork

Department of Radiotherapy, PGIMER, Chandigarh
Applicator Design• Several applicator
designs available:– Mould technique– Levendag’s– Forzhou (Chinese
district)– Simple catheter based

Department of Radiotherapy, PGIMER, Chandigarh
Mould Technique
• Customized mould prepared for each patient
• Uses a special quick setting silicone jel to take the nasopharyngeal impression.
• The source placement for an average nasopharynx are:– 2 sources for 1 wall– 3 sources for two adjoining
wall– 4 sources for 3 walls
• Intersource separation kept at 1 – 1.5 cm.

Department of Radiotherapy, PGIMER, Chandigarh
Technique of Insertion

Department of Radiotherapy, PGIMER, Chandigarh
Rotterdam Applicator• Designed by Levendag.• Designed so that the applicator could be worn
by the patient comfortably continuously throughout the fractionated course of treatment given.
• Made up of silicone which is flexible and closely conforms to the curvature of the nasopharynx.
• Applicator design based upon a 3 D model of the nasopharynx ( based on CT of two patients)
• Allows closer fit to the base of the skull and situated at a fixed distance from the soft palate.
• A silicone bridge and flange used to fix the applicator against the posterior nasal septum and the anterior one respectively.

Department of Radiotherapy, PGIMER, Chandigarh
Rotterdam Applicator• Tube diameter
– Outer diameter 15 F (5.5 mm)– Inner diameter 9 F ( 3.5 mm)
• Can accommodate the 6 F HDR source easily.
• Two tubes ensure catheter stability.
• The tubes are diverging at the base

Department of Radiotherapy, PGIMER, Chandigarh
Prescription and points• Several anatomical points defined by
Levendag to calculated dose to the tumor as well as critical normal tissues.
• Tumor points:– Na (Nasopharynx) – 2 – BOS (Base of Skull) - 2– R (Node of Rouviere) - 1
• Normal Tissue points:– OC ( Optic Chiasm) - 1– P (Pituitary gland) - 1 – C (Cord) – 1– Pa (Soft Palate) – 2– Re (Retina) - 2– No ( Nose) - 2

Department of Radiotherapy, PGIMER, Chandigarh
Prescription points
BOS
PaR
NaRe
POC
C
Pa Pa
CR
OC
Re Re
BOS BOS
Na Na
P
NoNo
No
Line 1
Line 2

Department of Radiotherapy, PGIMER, Chandigarh
Dose prescribed
• In case EBRT given in dose of 60 Gy:– 3 Gy x 2 fractions per day for 6 fractions
by HDR– Total dose ~ 78 Gy– Minimum interfraction gap of 6 hrs.
• In case of EBRT given in dose of 70 Gy:– 3 Gy x 2 fractions for 4 fractions by
HDR– Total dose ~ 82 Gy– Minimum interfraction gap of 6 hrs.

Department of Radiotherapy, PGIMER, Chandigarh
Advantages• Comfortable applicator – can be kept between
fractions• Optimization possible – Na, BOS and the R
points.• Can be reused after steam sterilization.• Reduced normal tissue dose – to the retina,
palate and the nasal cavity• In earlier work Levendag used to use two other
points:– FL point:
• corresponding to the BOS point• Approximates the position of the foramen lacerum
– FO point:• Situated at the foramen ovale• Taken 2 cm lateral to the midline in then same
plane as the BOS point.

Department of Radiotherapy, PGIMER, Chandigarh
Disadvantages
• Nasal synechia have been observed in few patients.– Corresponds to the hyperdose sleeve of
200% isodose around the applicator.– Approximately occurs in a radius of 6 mm
around the source axis after standard prescription
– Reduced by use of nasal pack for 7 days after ICBT
• Optimization can result in increased dose to some points (especially the spinal point).

Department of Radiotherapy, PGIMER, Chandigarh
Chemoradiation
• Sequence:– Induction– Concurrent– Adjuvant
• Concurrent regimen is best.• Principle:
– Local cooperation– Spatial cooperation
• We use Concurrent Cisplatin in doses of 50 mg/m2 D1 and D22.

Department of Radiotherapy, PGIMER, Chandigarh
Results: NACT

Department of Radiotherapy, PGIMER, Chandigarh
Results: Adjuvant CT
• Adjuvant Chemotherapy:– Of no benefit even if CDDP based.– Chi et al reported results of a phase III
randomized trial (2002) N = 157– Adjuvant chemotherapy with 24 hr
infusional Cisplatin 20 mg/m2, 5-fluorouracil 2,200 mg/m2, and leucovorin 120 mg/m2 x 9 cycles after 70 Gy XRT• 5-year overall survival 60.5% vs. 54.5%
(p = 0.5) • 5 yr relapse-free survival rates 49.5% vs.
54.4% (p = 0.38)

Department of Radiotherapy, PGIMER, Chandigarh
Results: Concurrent CT• Huncharek et al performed a meta-analysis in 2002.• 6 RCTs included• Statistically significant increase in the disease free
survival by approximately 20% to 40% • OS improved by ~ 20% (Statistically NS)• Better results with Cisplatin + 5 FU based regimen
( Al Sarraf)

Department of Radiotherapy, PGIMER, Chandigarh
Results : Metastatic disease

Department of Radiotherapy, PGIMER, Chandigarh
NPC in Children• Problem of long term toxicity:
– Skull deformities– Neurological deficits– Pituitary dysfunction– Hearing impairment– TM joint ankylosis– Visual defects
• RT is the treatment modality of choice:– Dose 50 -60 Gy– Boost only after skull growth is complete (15yrs)– Lower neck usually not treated if clinically –ve.
• Outcome: – DFS is 70 – 80% in T1 and T2 tumors– DFS is 40 – 50% in T3 – T 4 tumors

Department of Radiotherapy, PGIMER, Chandigarh
Recurrence
• 2 types described (Wang et al)– Persistent disease– Relapse: Appearing 1 yr after treatment.
• Detecting recurrence:– Tc99m SPECT– MRI – High signal intensity on T1
weighted spin echo images
• Options:– Palliative treatment– Radiation therapy– Surgery

Department of Radiotherapy, PGIMER, Chandigarh
Surgery
• Usually indicated in situations like isolated nodal recurrence
• Local recurrences have been salvaged by extensive craniofacial surgery

Department of Radiotherapy, PGIMER, Chandigarh
Radiotherapy• EBRT• Brachytherapy
– Both temporary and permanent implants used.– Best results from Gold grain implantation.
• IMRT and 3 DCRT– Investigational
• Sterotactic Radiosurgery• Chemotherapy
– Cisplatin or taxane based– Mainstay in:
• Distant spread• Early recurrence• Extensive disease

Department of Radiotherapy, PGIMER, Chandigarh
Radiotherapy
• External radiotherapy:– High energy beams are better choosen– Small 6 x 6 field used to treat site of local
recurrence– Doses in range of 20 – 30 Gy.– Indications:
• Limited tumour size, • a relatively long period since previous
irradiation (minimal time period ~ 1 year)• Good performance status and • Lack of evidence of skin or soft tissue
damage (skin fibrosis, atrophy or telangiectasis) from the previous irradiation course

Department of Radiotherapy, PGIMER, Chandigarh
Results of RT

Department of Radiotherapy, PGIMER, Chandigarh
Results

Department of Radiotherapy, PGIMER, Chandigarh
Neurological Sequelae• Hypothalamo-Pituitary dysfunction
– Median incidence of clinical dysfunction is 3%. – Cumulative incidence of endocrine dysfunction
higher at 67% at 2 yrs. – Most common disturbance seen in GH secretion. – Thyroid hormone production affected the least.
• Hearing defects:– Almost 7% patients become deaf with standard
therapy.– Otitis media seen in 14% patients– Prolonged tinnitus may be seen in 30% patients
• Temporal lobe injury:– Incidence as high as 3% after 2 yrs.– Toxicity more in altered fractionation regimens
• Cranial nerve injury:– The incidence is as high as 6%.

Department of Radiotherapy, PGIMER, Chandigarh
Other Sequelae
• Significant xerostomia can be seen in as high as 80 %
• Some degree of xerostomia is seen all patients.
• Fibrosis of the subcutaneous tissue is seen when doses exceeding 50 Gy are used in almost 16% patients.
• Significant trismus, can occur in 5 to 10% patients.
• This particular complication can be reduced by using a three-field approach for boosting the nasopharynx.

Department of Radiotherapy, PGIMER, Chandigarh
Conclusions
• Nasopharyngeal malignancies make up a different population of head and neck malignancies.
• These are eminently radio sensitive and curable.
• Treatment planning is by necessity complicated and time consuming.
• Brachytherapy can be used for boosting the local activities.
• Chemoradiation is standard treatment in locally advanced tumors

Thank You