Embed Size (px)
Citation preview
Carcinoma of the Pancreas Presenting as Acute DuodenalObstruction Without Jaundice: *
A Report of Four Cases
RicHARD JOSEPH WHITE, M.D.Fort Worth, Texas
THE SYNDROME of a slowly-oncomingjaundice, usually without too much pain,with a dilated, easily palpable gallbladder,is all too familiar to surgeons. An interest-ing variant has been encountered in fourrecent cases. All these patients complainedof severe and unremitting vomiting andnone had clinical jaundice. In two therewas a mass, palpable under anesthesia,which did not feel like a gallbladder; onehad severe pain. Radiographic studiesshowed high-grade duodenal obstructionin both.At laparotomy large tumors in the head
of the pancreas, predominantly in theupper portion, had so flattened the C-loopof the duodenum by extrinsic pressure asto almost completely obstruct it, and inone instance the mass eroded through themedial duodenal wall and grew extensivelyin the lumen. All were massive and therewas no thought of resection of the tumors.Jaundice developed later in three patients,and cholecystojejunostomy was done inone. Gasteroenterostomy was done in everycase. This clinical picture of acute duo-denal obstruction due to carcinoma of thepancreas without jaundice is rare, yet thechance happening that I encountered it forthe first time less than three years ago andhave seen three examples since, is strange.Very little has been written about this
lesion. In 1950, Marshak, Dreiling andFriedman3 reported four such cases andsaid they had never seen it before. This is
* Presented before the Southern Surgical As-sociation, Boca Raton, Florida, December 6-8,1960.
the only specific reference to this con-dition I have been able to find. Sohmer andCoyer,7 in 1955, in a study of 34 cases ofcarcinoma of the pancreas encountered ina ten-year period, reported one case ofhigh grade obstruction of the duodenum,just proximal to the ligament of Treitzwith infiltration of the root of the mes-entery, and liver metastases from car-cinoma of the tail of the pancreas.Probably most surgeons have encountered
duodenal obstruction appearing some timeafter cholecystojejunostomy for the reliefof jaundice, due to carcinoma of the headof the pancreas gradually compromisingthe duodenum by further growth. Pipesand Pareira 5 record five such cases. Nonewere near terminal from their carcinomaand all were symptomatically relieved fora time by gastroenterostomy. They couldfind no consideration of this problem inthe literature. Gullich2 says that gastro-intestinal x-ray studies were done in ap-proximately 100 cases of carcinoma of thepancreas that he collected. Pertinent find-ings were present in 52.8 per cent oftumors of the head and 44.4 per cent ofthe body and tail. Carcinoma of the headtypically produced x-ray changes in thedistal stomach, pylorus and duodenum.The stomach may be displaced forward,upwards or to the left. There may be dis-tortion with apparent lengthening of thepylorus or out-pouching of the lessercurvature simulating gastric ulcer. In ad-vanced cases there may be pyloric ob-struction. Deformities of the duodenalcap were the most frequent finding and
769
Annals of SurgeryMay 1961
. .. }2bgh.
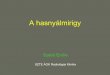
FIG. 1. ( Case 2 ) High grade duodenal obstruction.
consisted of dilatation and kinking, for-ward displacement, eccentric displacement,such as being molded on lesser curvature,filling defects or obstruction. The duo-denal loop may show irregularity, a wideswing to the right, displacement anteriorlyor to the left or constriction. Nightingale,Boyd and Mersheimer 4 also collected 100cases of pancreatic carcinoma. Nausea andvomiting was quite common, as in otherseries, occurring in 38 per cent, but no
mention was made of duodenal obstruction.An autopsy report in a clinical path-
ological conference at Cook County Hos-pital 1 of a patient who had pyloric ob-struction followed in less than a week byjaundice from carcinoma of the head ofthe pancreas invading the duodenum andcommon bile duct. This closely resemblesCase 3 of my series. Shenstone and Ford 6
reviewed 159 cases of carcinoma of thepancreas and state that invasion of theduodenum, pylorus and stomach withmalignant ulceration of the mucosa was
not an infrequent necropsy observationwith partial and complete malignant ob-struction of the duodenum and pylorusoccasionally noted, but there was no men-
tion of this as a primary symptom produc-ing vomiting without jaundice.
This presentation illustrates a rare clin-
ical picture in which advanced malignantdisease is first manifested by unremittingvomiting and radiological signs of high gradeduodenal obstruction without jaundice.Jaundice appeared in due course in threeof the patients.The unusual situation must be due to
rapid growth of the tumor adjacent to theduodenum, either stretching it tightly or
invading massively, before the usual in-vasion of the common bile duct. The dis-ease is the same and the prognosis thesame, but the startling picture of acuteand practically complete duodenal ob-struction without jaundice presented in thefour cases are examples of a rare aspect ofa very malignant disease.
Case ReportsCase 1. St. Joseph's Hospital, 4,537. W. H. W.,
aged 75, M., admitted 3/25/58. Chief Com-
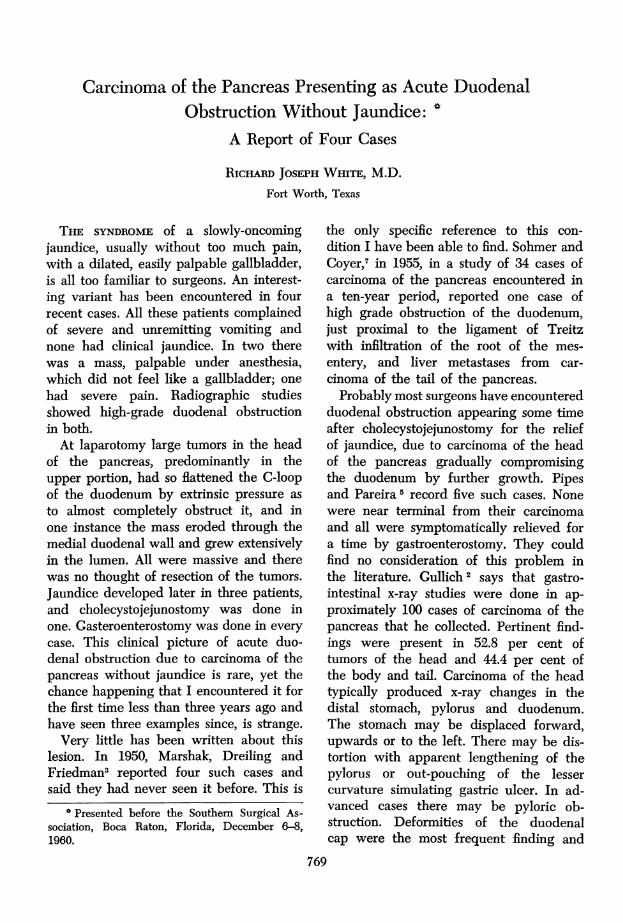
FIG. 2. (Case 2) Microscopic section of tumor.
770 WHITE
Volume 153 CARCINOMA OF THE PANCREAS 771Number 5
plaint: Vomiting for ten days. X-ray filmsshowed obstruction of the second portion of theduodenum and a hugely dilated stomach. He hadno history of gastric distress previously and asfar as he knew had had no bleeding. The pos-sibility of a carcinoma of the pancreas was con-sidered by the radiologist though there was nojaundice. After two days of fluid and electrolytereplacement he was operated upon. A nodularmass, the size of a large fist was felt in theretroperitoneal area in the region of the head of _nthe pancreas encroaching on the duodenal loopwith a dilated first portion of the duodenum. Itwas obviously carcinoma. The gallbladder wasdilated slightly. A posterior gastroenterostomywas done. He lived 7 months and becamejaundiced shortly before death.
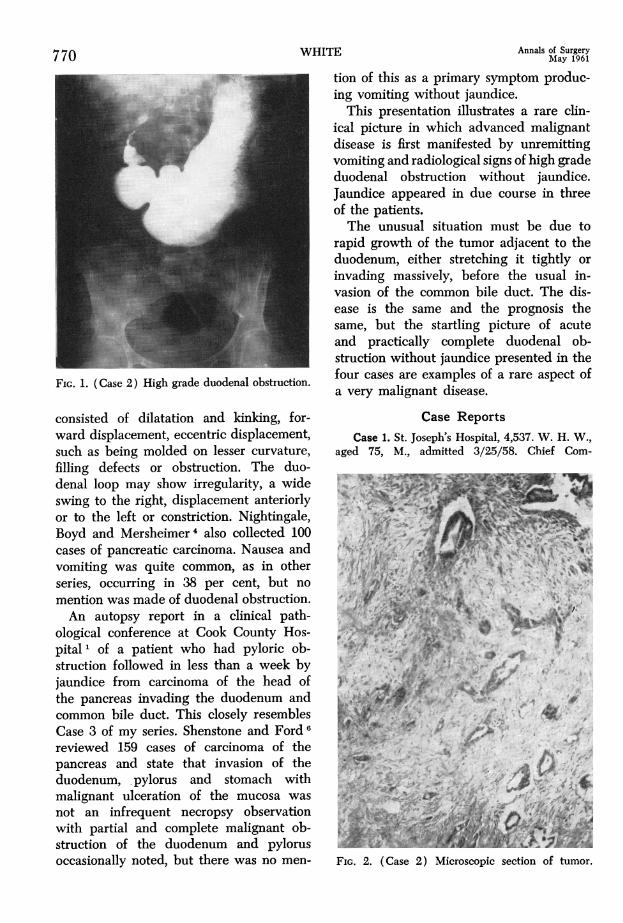
FIG. 4. (Case 3) Three-hour film of stomachand duodenum.
The duodenal bulb was normal in contour. Thepyloric canal was wide.
At operation on 1/27/58, a mass the size of agolf ball was felt, apparently posterior to theduodenum and originating in the pancreas. It
4L. ~ ~ ~ ~ ~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~,
FIG. 3. (Case 3) Immediate film of stomach.
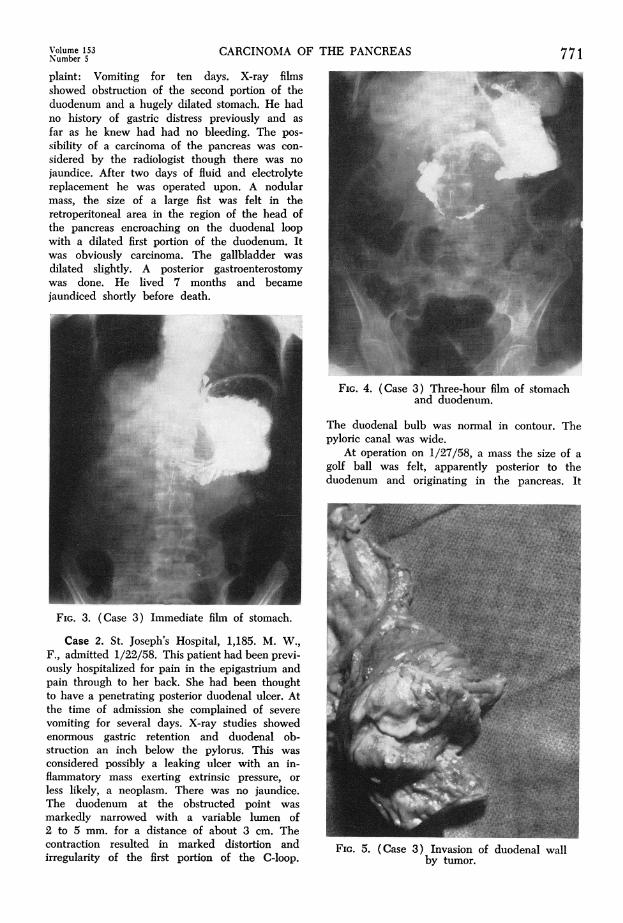
Case 2. St. Joseph's Hospital, 1,185. M. W.,F., admitted 1/22/58. This patient had been previ-ously hospitalized for pain in the epigastrium andpain through to her back. She had been thoughtto have a penetrating posterior duodenal ulcer. Atthe time of admission she complained of severevomiting for several days. X-ray studies showed _iAenormous gastric retention and duodenal ob-struction an inch below the pylorus. This wasconsidered possibly a leaking ulcer with an in-flammatory mass exerting extrinsic pressure, orless likely, a neoplasm. There was no jaundice.The duodenum at the obstructed point wasmarkedly narrowed with a variable lumen of2 to 5 mm. for a distance of about 3 cm. Thecontraction resulted in marked distortion and FIG. 5. (Case 3) Invasion of duodenal wallirregularity of the first portion of the C-loop. by tumor.- I - ---- - - -
772 ~~~~~~~~~~~~WHITE Annals of Surgery772 WHITE AMay 1961- - -~~~~~~~ -~~ had never been sick before and had not noticed
..v..any yellow color to her skin.A definite abdominal mass could not be felt
even though there was x-ray evidence of its pres-ence in the region of the head of the pancreas,and there was almost complete obstruction of thedistal portion of the stomach. It seemed to be
4 compressed in its distal half and especially inthe region of the antrum. The mucosal pattemappeared intact. In three hours a small amountof barium had left the stomach and at this timea large, 8 x 10 cm. well-defined mass in theregion of the head of the pancreas was demon-strated. The mass was thought to be carcinomaof the head of the pancreas, or cyst of thepancreas or enlarged retroperitoneal lymph nodes.
After fluid and electrolyte correction, an
I A' ! ....abdominal exploration was performed on JanuaryAW 9, 1960. Under anesthesia before opening the
abdoe,the mass was easily palpable. Whenexposed through an upper right rectus incision, itwas 3 or 4 inches in diameter, and apparentlyoriginated in the head of the pancreas. Itstretched the duodenum tightly, producing me-chanical obstruction. No evidence of peritonealcarcinomatosis or liver infiltration was seen. The
~~~~~~~~~~~~~~~~~. ...
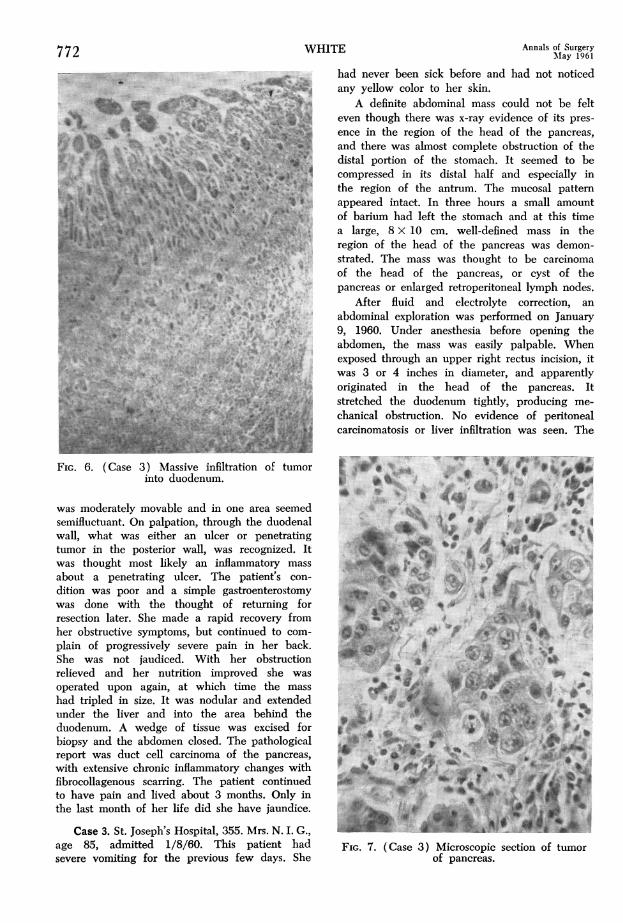
FIG.. 6. (Case 3) Massive infiltration of tumor ~into duodenum.
*~~~....... ... *0 .....was moderately movable and in one area seemed '-
semifluctuant. On palpation, through the duodenal . Uwall, what was either an ulcer or penetrating 'Xtumor in the posterior wall, was recognized. Itwas thought most likely an inflammatory massabout a penetrating ulcer. The patient's con-dition was poor and a simple gastroenterostomy _was done with the thought of retuming forresection later. She made a rapid recovery from dher obstructive symptoms, but continued to com- Awplain of progressively severe pain in her back. /4She was not jaudiced. With her obstructionrelieved and her nutrition improved she wasoperated upon again, at which time the masshad tripled in size. It was nodular and extendedunder the liver and into the area behind the -. *duodenum. A wedge of tissue was excised forbiopsy and the abdomen closed. The pathologicalreport was duct cell carcinoma of the pancreas, Kwith extensive chronic inflammatory changes with _fibrocollagenous scarring. The patient continuedto have pain and lived about 3 months. Only inthe last month of her life did she have jaundice.
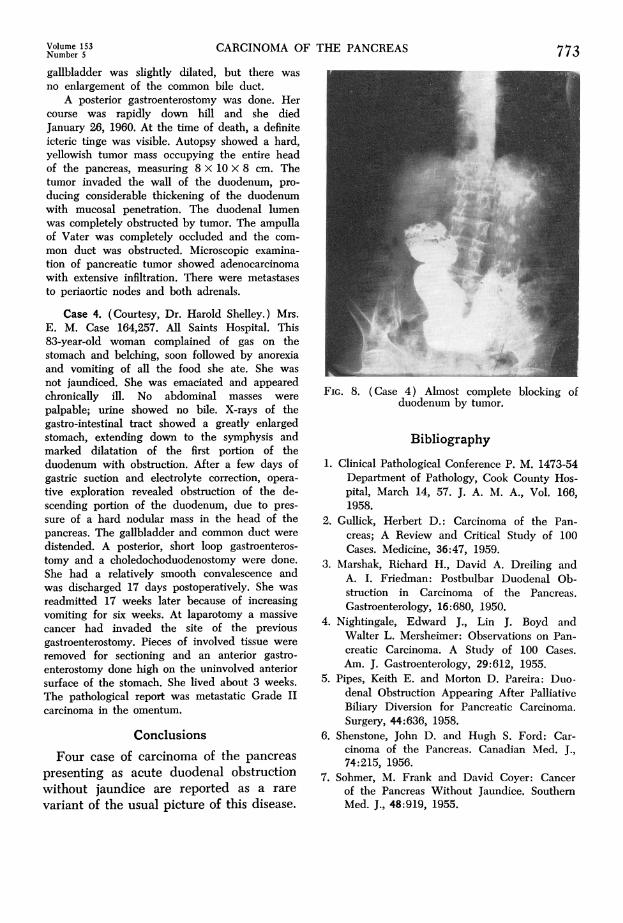
Case 3. St. Joseph's Hospital, 355. Mrs. N. I. G.,age 85, admitted 1/8/60. This patient had FIG. 7. (Case 3) Microscopic section of tumorsevere vomiting for the previous few days. She of pancreas.
Volume 153 CARCINOMA OF THE PANCREAS 773Number 573gallbladder was slightly dilated, but there wasno enlargement of the common bile duct.
A posterior gastroenterostomy was done. Hercourse was rapidly down hill and she diedJanuary 26, 1960. At the time of death, a definiteicteric tinge was visible. Autopsy showed a hard,yellowish tumor mass occupying the entire headof the pancreas, measuring 8 x 10 X 8 cm. Thetumor invaded the wall of the duodenum, pro-ducing considerable thickening of the duodenumwith mucosal penetration. The duodenal lumenwas completely obstructed by tumor. The ampullaof Vater was completely occluded and the com-mon duct was obstructed. Microscopic examina-tion of pancreatic tumor showed adenocarcinomawith extensive infiltration. There were metastasesto periaortic nodes and both adrenals.
Case 4. (Courtesy, Dr. Harold Shelley.) Mrs.E. M. Case 164,257. All Saints Hospital. This83-year-old woman complained of gas on thestomach and belching, soon followed by anorexiaand vomiting of all the food she ate. She wasnot jaundiced. She was emaciated and appearedchronically ill. No abdominal masses werepalpable; urine showed no bile. X-rays of thegastro-intestinal tract showed a greatly enlargedstomach, extending down to the symphysis andmarked dilatation of the first portion of theduodenum with obstruction. After a few days ofgastric suction and electrolyte correction, opera-tive exploration revealed obstruction of the de-scending portion of the duodenum, due to pres-sure of a hard nodular mass in the head of thepancreas. The gallbladder and common duct weredistended. A posterior, short loop gastroenteros-tomy and a choledochoduodenostomy were done.She had a relatively smooth convalescence andwas discharged 17 days postoperatively. She wasreadmitted 17 weeks later because of increasingvomiting for six weeks. At laparotomy a massivecancer had invaded the site of the previousgastroenterostomy. Pieces of involved tissue wereremoved for sectioning and an anterior gastro-enterostomy done high on the uninvolved anteriorsurface of the stomach. She lived about 3 weeks.The pathological report was metastatic Grade IIcarcinoma in the omentum.
ConclusionsFour case of carcinoma of the pancreas
presenting as acute duodenal obstructionwithout jaundice are reported as a rarevariant of the usual picture of this disease.
FIG. 8. (Case 4) Almost complete blocking ofduodenum by tumor.
Bibliography
1. Clinical Pathological Conference P. M. 1473-54Department of Pathology, Cook County Hos-pital, March 14, 57. J. A. M. A., Vol. 166,1958.
2. Gullick, Herbert D.: Carcinoma of the Pan-creas; A Review and Critical Study of 100Cases. Medicine, 36:47, 1959.
3. Marshak, Richard H., David A. Dreiling andA. I. Friedman: Postbulbar Duodenal Ob-struction in Carcinoma of the Pancreas.Gastroenterology, 16:680, 1950.
4. Nightingale, Edward J., Lin J. Boyd andWalter L. Mersheimer: Observations on Pan-creatic Carcinoma. A Study of 100 Cases.Am. J. Gastroenterology, 29:612, 1955.
5. Pipes, Keith E. and Morton D. Pareira: Duo-denal Obstruction Appearing After PalliativeBiliary Diversion for Pancreatic Carcinoma.Surgery, 44:636, 1958.
6. Shenstone, John D. and Hugh S. Ford: Car-cinoma of the Pancreas. Canadian Med. J.,74:215, 1956.
7. Sohmer, M. Frank and David Coyer: Cancerof the Pancreas Without Jaundice. SouthernMed. J., 48:919, 1955.