Embed Size (px)
DESCRIPTION
Handout on Cardiac Failure
Citation preview

7/21/2019 Cardiac Failure
http://slidepdf.com/reader/full/cardiac-failure-56d98b5bb63b3 1/12
1
Cardiac failure - terms
• O2 DELIVERY = O2 content x cardiac
output
• O2 CONTENT = O2 sat x Hb x 1.39 x10ml/
L (1gm Hb carries 1.39 ml O2 at 100%
saturation)
• CARDIAC OUTPUT = HR X Stroke
volume
CF Terms
• STROKE VOLUME depends on preload,
afterload and contractility (inotropic state)
• PRELOAD (the load before contraction)
equates to the filling volume of the heart
• AFTERLOAD (the load after the
contraction of the heart) the resistance the
ventricles face on ejection of blood e.g.BP
CF terms
• CONTRACTILITY (inotropic state) -the efficiency (greater velocity) and force
of contraction of heart muscle• MYOCARDIAL O2 DEMAND -
increases with HR, wall stress (afterloadand preload), and contractility
• WALL STRESS = pressure x radius /2 x wall thickness

7/21/2019 Cardiac Failure
http://slidepdf.com/reader/full/cardiac-failure-56d98b5bb63b3 2/12
2
CF – terms
• Myocardial hypertrophy in response to
PRESSURE overload acutely -> increase wall
stress -> replication of myofibrils in parallel,
thickening of individual myocytes, &
CONCENTRIC HYPERTROPHY
• Response to ventricular VOLUME overload ->
replication of sarcomeres in series, elongation of
myocytes & DILATATION -> moderate increase
sys stress ->moderate ECCENTRIC hypertrophy
Cardiac failure
• A state in which there is inadequate cardiac
output to meet the body’s metabolic needs
at normal physiologic venous pressures.
Due to
• Primary abnormality of the myocardium
• Excessive workload e.g. VSD or AV
regurgitation.
Acute Cardiac Failure
is acute functioning uncoupling between
compensatory mechanisms and decreased
myocardial function -> homeostaticimbalance and overt symptoms

7/21/2019 Cardiac Failure
http://slidepdf.com/reader/full/cardiac-failure-56d98b5bb63b3 3/12
3
Chronic CF
Cardiac pump dysfunction with activation of
compensatory responses that ultimately ->
silent and progressive deterioration of
myocardial function
SHOCK
Acute circulatory dysfunction with completely
overwhelmed physiological compensatory
mechanisms. This results in death if not
treated promptly.
Cardiac failure
Compensatory mechanisms
• Increased heart rate.
• Frank Starling Mechanism.
• Sympathetic nervous system activation.
• Increased 2-3 DPG.
• Increased natruretic peptide.
• Myocardial hypertrophy.

7/21/2019 Cardiac Failure
http://slidepdf.com/reader/full/cardiac-failure-56d98b5bb63b3 4/12
4
CF - Haemodynamic changes
Increase in - heart rate
- ventricular E.D. volume
- ventricular E.D. pressure
- atrial pressure
- systemic vascular resistance
Decrease in - systemic blood flow
CF Compensatory mechanisms
• Starling’s Law of the Heart
The force of contraction (ventricular) and
the volume of ejected blood increase
directly with an increase in the initial
volume of ventricle at the time of systole
(EDV).
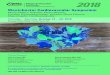
Frank-Starling’s Law of the Heart
End-Diastolic Volume
Stroke
Volume
Normal Range:
SV increases with EDV
Maximum Capacity
To Produce SV
Mechanism: Length-Force Relations of Muscle Contraction

7/21/2019 Cardiac Failure
http://slidepdf.com/reader/full/cardiac-failure-56d98b5bb63b3 5/12
5
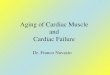
Family of Ventricular Function Curves
Atrial Pressure (Preload)
Cardiac
Output
Increase in
Cardiac
Contractility
or
Increase in
Heart Rate
Sympathetic stimulation
increases heart rate andcontractility
Parasympathetic stimulation
decreases heart rate
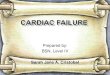
Family of Frank-Starling Curves
Stroke
Volume
Preload (End-Diastolic Volume)
Increase in
Cardiac
Contractility
At a given EDV, SV increases
With cardiac contractility
Low
High

7/21/2019 Cardiac Failure
http://slidepdf.com/reader/full/cardiac-failure-56d98b5bb63b3 6/12
6
CF Compensatory mechanisms
Effects of catecholamines
• Increased contractility -> increased CO, BP
• Increased heart rate
• Decreased renal perfusion, renin
production,angiotensin II & aldosterone,
systemic vasoconstriction, Na and H2O
retention -> increase in CO
CF Compensatory mechanisms
•
2,3-Diphosphoglycerate is increased in CF
resulting in a shift to the right of the oxygen
dissociation curve which facilitates oxygen
unloading to the tissues.
• Atrial Natruretic peptide (ANP) is released from
the atrial wall in response to atrial stretch ->
urinary loss of Na and water. ANP is a vasodilator
and reduces tachycardia.

7/21/2019 Cardiac Failure
http://slidepdf.com/reader/full/cardiac-failure-56d98b5bb63b3 7/12
7
CF - compensatory mechanisms
Sympathetic NS stimulation
• In the NORMAL STATE state inhibitory
impulses from arterial & cardiopulmonary
baroceptor afferent nerves control
sympathetic outflow. Parasympathetic
outflow is under baroceptor (+) control.
• In CF- inhibitory (-) input decreases,
excitatory (+) increases -> Sympathetic NS
stimulated. Parasympathetic blunted.
CF- Compensatory mechanisms
Sympathetic NS stimulation
• Norepinephrine (NE) released and with
endothelin-1 and vasopressin -> BP rise,
vasoconstriction-> AFTERLOAD up.
Cyclic AMP increased -> Influx Ca into
myocytes -> CONTRACTILITY & CO
up.
• Heart rate increased
• Decreased renal perfusion -> renin -> Na &
H2O retention ->PRELOAD up.
CF Compensatory mechanisms
• Myocardial hypertrophy . The myocytes
respond to changes in loading conditions in
CF by hypertrophy.
•
Angiotensin II -> myocyte hypertrophy.
• Aldosterone -> collagen synthesis

7/21/2019 Cardiac Failure
http://slidepdf.com/reader/full/cardiac-failure-56d98b5bb63b3 8/12
8
CF- Sympathetic NS stimulation
- harmful effects
• Myocyte injury and necrosis
• Accelerated apoptosis (normal process of
programmed cell death).
• Increase HR and contractility & increase
wall stress -> increase O2 consumption
• Hypertrophy -> O2 demand up, myocyte
damage and fibrosis-> decrease CO.
• ACUTE improvement, CHRONIC decline.
CF Causes - categories
• Increased blood VOLUME - AI, MI, TI, L to R
shunts, overtransfusion & hypervolaemia.
• Increased PRESSURE load, AS, HOCM, CoA,
hypertension.
• Myocardial DYSFUNCTION - Cardiomyopathy,
myocarditis, dysrhythmias, toxic.
• FILLING disorders.
• Increased METABOLIC demands
CF – Causes – age groups
• FOETAL or CONGENITAL - SVT,
erythroblastosis foetalis, AV malformation
• CF IN THE FIRST WEEK - Duct
dependent ( Hypoplastic LHS, Severe ASand CoA)and non duct dependent(TAVR,
AV malform, myocardial dysfunction
syndrome, SVT, sepsis).

7/21/2019 Cardiac Failure
http://slidepdf.com/reader/full/cardiac-failure-56d98b5bb63b3 9/12
9
CF Causes – age groups
• INFANCY
Obstructive lesions – severe CoA & AS
L to R shunts
Mixing lesions – TAPVR, TGA, truncus
Myo/pericardial – SVT, myocarditis,
cardiomyopathy, purulent pericarditis.
CF Causes - age groups
CHILD & ADOLESCENT
Acquired – myocarditis, cardiomyopathy,
AIDS, cardiotoxic drugs and
substance abuse.
Factors complicating congenital lesions -
anaemia, infective endocarditis, surgery,
myocardial deterioration.
CF NY Classification
• Class I - no limitation of ordinary activity
• Class II - slight limitation, no symptoms at
rest, symptoms on ordinary activity
•
Class III – marked limitation of physical
activity, no symptoms at rest, symptoms on
< ordinary activity.
• Class IV – symptomatic at rest.

7/21/2019 Cardiac Failure
http://slidepdf.com/reader/full/cardiac-failure-56d98b5bb63b3 10/12
10
CF Clinical manifestations
• TACHYCARDIA (except primary bradycardia or
complete heart block)
•
SYSTEMIC VENOUS CONGESTION –
hepatomegaly, raised JVP, oedema (facial in
infants), pleural effusions,ascites
• PULMONARY VENOUS CONGESTION-
increased RR, retractions, nasal flaring, grunting,
creps, wheeze, pulm. oedema, irritability(low O2)
CF Clinical manifestations
• LOW CO – fatigue, pallor, sweating, cool
extremities, low pulse volume, decreased
capillary refill.
• VOLUME OVERLOAD – cardiac
enlargement, gallop , regurgitant murmur
• Low urine output.
• Growth failure and weight loss.
CF -Evaluation
• History
• Physical examination.
• Investigations –Cxray, ECG, 2DE, pulse
oximetry, blood gases, O2 challenge, U &E,
CBC, urinalysis, blood culture, serum Ca,
blood glucose, others indicated by history
and P.E.

7/21/2019 Cardiac Failure
http://slidepdf.com/reader/full/cardiac-failure-56d98b5bb63b3 11/12
11
CF – History
• Poor feeding in small infants
• SOB worse on feeding (exertionaldyspnoea), respiratory symptoms in infants
• Sweating – increased on feeding
• Poor weight gain and linear growth
• In older child – fatigue, exertionaldyspnoea, orthopnoea, oedema of face andlegs
CF – Treatment
• Identify and treat underlying cause
• Correct aggravating factors e.g. anaemia
and sepsis, arrhythmias, hypertension
• NON-PHARMACOLOGICAL
• PHARMACOLOGICAL
CF Treatment
Non-pharmacological
• SEVERE – bed rest, prop-up, O2, fluid
restriction, salt restriction, adequate
calories.
•
AMBULANT – No added salt
mild exercise

7/21/2019 Cardiac Failure
http://slidepdf.com/reader/full/cardiac-failure-56d98b5bb63b3 12/12
12
CF Treatment
Pharmacological
• Diuretics
• Vasodilators
• ACE inhibitors
• Beta adrenergic blockade
• Digoxin
• Beta agonists – used in ICU setting
dobutamine, dopamine, isoprenaline