Embed Size (px)
Citation preview

Cardiac Function in Duchenne’s Muscular Dystrophy
Results of IO-Year Follow-up Study and Noninvasive Tests
ROBERT H. HUNSAKER, B.S. PHILLIP K. FULKERSON, M.D. FRED J. BARRY, M.D.* RICHARD P. LEWIS, M.D. CARL V. LEIER, M.D. DONALD V. UNVERFERTH, M.D.
Columbus, Ohio
From the Division of Cardiology, Department of Medicine, Ohio State University College of Medi- cine, Columbus, Ohio. This study is supported in part by the S. J. Roessler Foundation, the Central Ohio Chapter of the American Heart Association, and Eagles Cardiovascular Research Fund. Re- quests for reprints should be addressed to Dr. Donald V. Unverferth, 466 West 10th Avenue, 657 Means Hall, Columbus, Ohio 43210. Manuscript accepted on January 20, 1982. l Present address: 122 Barrington Drive, Oak Ridge, Tennessee.
The purposes of this study were to: (1) evaluate the progression of cardiac involvement in Duchenne’s muscular dystrophy using sys- tolic time intervals (PEP/LVET); (2) determine if the degree of cardiac involvement bears a relation to the severity of skeletal muscle disease; and (3) describe the M-mode and two-dimensional echocardiographic findings. In 1970, systolic time intervals were studied in 16 patients. During the lo-year interim, two patients were lost to follow-up study, and five patlls dled. Nine remahhg patlents were re-studied in 1980 with M-mode and two-dlmenslonal echo- cardiography as well as systolic time intervals. The PEP/LVET value of these nine patients increased from 0.37 f 0.05 (x f SD) in 1970 to 0.47 f 0.07 (p <O.OOS) in 1980. Three patients remained am- bulatory, and their PEPILVET value (0.41 f 0.04) was slgnlfkantly better than that of the nonambulatory patients (0.50 f 0.07, p <O-05). The M-mode echocardiography percentage diameter change was also worse in the nonambulatory group (21 f 4 percent versus 34 f 7 percent, p CO.02). The five patients who were non- ambulatory in 1970 died in the intervening 10 years. This study demonstrated that the heart disease of Duchenne’s muscular dys- trophy is progressive and that the severity of skeletal muscle disease is probably associated wlth the degree of cardiac dysfunction.
Progressive muscular dystrophy was first described clinically in 1852 [ 11, and cardiac muscle involvement was suspected as early as 1860 [2]. Since that time, numerous studies have elucidated the cardiac pathology [2-l 21, electrocardiographic findings [ 1 l- 181, hemody- namics [9,19], and results of noninvasive tests of left ventricular function [20-241 in patients with Duchenne’s muscular dystrophy. While autopsy studies suggest that myocardial involvement occurs in more than 85 percent of patients [6], the incidence of clinically important cardiac disease is not known because of the incapacitating nature of skeletal myopathy.
Tachycardia [ 251 or increased anterior forces noted on the elec- trocardiogram [ 11,12.18] have often been the first clue to cardiac disease in Duchenne’s muscular dystrophy. Echocardiography and systolic time intervals have now proved sensitive indicators of cardiac dysfunction [20,21]. These noninvasive tests have demonstrated systolic and diastolic abnormalities with Duchenne’s muscular dys- trophy [20-241. Studies have not clearly defined whether the severity of cardiac dysfunction correlates with the degree of skeletal myopathy or objectively determined whether the cardiac disease is progres- sive.
Auguei 1982 The Am&can Journal of Medicine Volume 73 235
DUCHENNE’S MUSCULAR DYSTROPHY---HUNSAKER ET AL.
+ P~O.005
_..“_I
1970 1980 L-
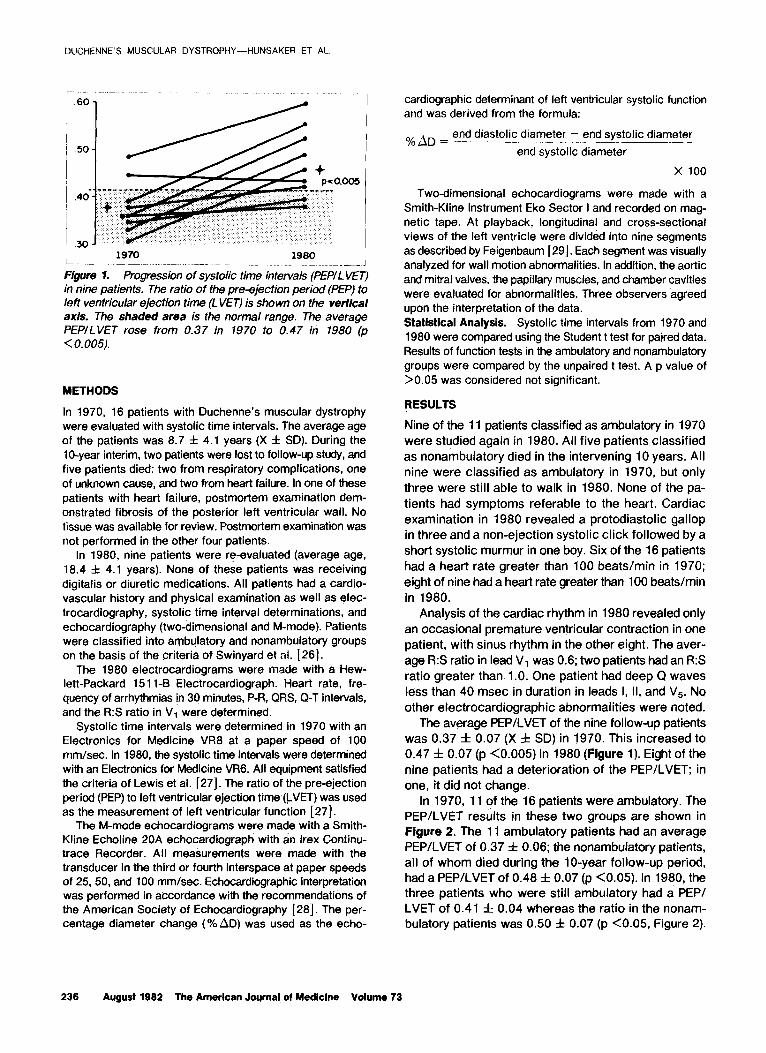
figure 1. Progression of systolic time intervals (PEPILVET) in nine patients. The ratio of the pre-ejection period (PEP) to left ventricular ejection time (L VET) is shown on the verfical axis. The shaded area is the normal range. The average PEPILVET rose from 0.37 in 1970 to 0.47 in 1980 (p < 0.005).
METHODS
In 1970, 16 patients with Duchenne’s muscular dystrophy were evaluated with systolic time intervals. The average age of the patients was 8.7 f 4.1 years (X f SD). During the lo-year interim, two patients were lost to follow-up study, and five patients died: two from respiratory complications, one of unknown cause, and two from heart failure. In one of these patients with heart failure, postmortem examination dem- onstrated fibrosis of the posterior left ventricular wall. No tissue was available for review. Postmortem examination was not performed in the other four patients.
In 1980, nine patients were re-evaluated (average age, 18.4 f 4.1 years). None of these patients was receiving digitalis or diuretic medications. All patients had a cardio- vascular history and physical examination as well as elec- trocardiography, systolic time interval determinations, and echocardiography (two-dimensional and M-mode). Patients were classified into ambulatory and nonambulatory groups on the basis of the criteria of Swinyard et al. [ 261.
The 1980 electrocardiograms were made with a Hew- lett-Packard 15 11-B Electrocardiograph. Heart rate, fre- quency of arrhythmias in 3q minutes, P-R, QRS, Q-T intervals, and the R:S ratio in VI were determined.
Systolic time intervals were determined in 1970 with an Electronics for Medicine VR8 at a paper speed of 100 mm/set. In 1980, the systolic time intervals were determined with an Electronics for Medicine VR6. All equipment satisfied the criteria of Lewis et al. [27]. The ratio of the pre-ejection period (PEP) to left ventricular ejection time &VET) was used as the measurement of left ventricular function [27].
The M-mode echocardiograms were made with a Smith- Kline Echoline 20A echocardiograph with an lrex Continu- trace Recorder. All measurements were made with the transducer in the third or fourth interspace at paper speeds of 25, 50, and 100 mm/set. Echocardiographic interpretation was performed in accordance with the recommendations of the American Society of Echocardiography [28]. The per- centage diameter change (% AD) was used as the echo-
cardiographic determinant of left ventricular systolic function and was derived from the formula:
end diastolic diameter - end s stolic diameter O/,AD = ..-__~.._.._____.-._~Y_~.__ end systolic diameter
x 100
Two-dimensional echocardiograms were made with a Smith-Kline Instrument Eko Sector I and recorded on mag- netic tape. At playback, longitudinal and cross-sectional views of the left ventricle were divided into nine segments as described by Feigenbaum [ 291. Each segment was visually analyzed for wall motion abnormalities. In addition, the aortic and mitral valves. the papillary muscles, and chamber cavities were evaluated for abnormalities. Three observers agreed upon the interpretation of the data. Statistical Analysis. Systolic time intervals from 1970 and 1980 were compared using the Student t test for paired data. Results of function tests in the ambulatory and nonambulatory groups were compared by the unpaired t test. A p value of >0.05 was considered not significant.
RESULTS
Nine of the 11 patients classified as ambulatory in 1970
were studied again in 1980. All five patients classified
as nonambulatory died in the intervening 10 years. All
nine were classified as ambulatory in 1970, but only three were still able to walk in 1980. None of the pa- tients had symptoms referable to the heart. Cardiac examination in 1980 revealed a protodiastolic gallop in three and a non-ejection systolic click followed by a short systolic murmur in one boy. Six of the 16 patients had a heart rate greater than 100 beatslmin in 1970; eight of nine had a heart rate greater than 100 beats/min in 1980.
Analysis of the cardiac rhythm in 1980 revealed only an occasional premature ventricular contraction in one patient, with sinus rhythm in the other eight. The aver- age R:S ratio in lead VI was 0.6; two patients had an R:S ratio greater than 1 .O. One patient had deep Q waves less than 40 msec in duration in leads I, II, and Vs. No other electrocardiographic abnormalities were noted.
The average PEP/LVET of the nine follow-up patients was 0.37 f 0.07 (X f SD) in 1970. This increased to 0.47 f 0.07 (p <0.005) in 1980 (figure 1). Eight of the nine patients had a deterioration of the PEP/LVET; in one, it did not change.
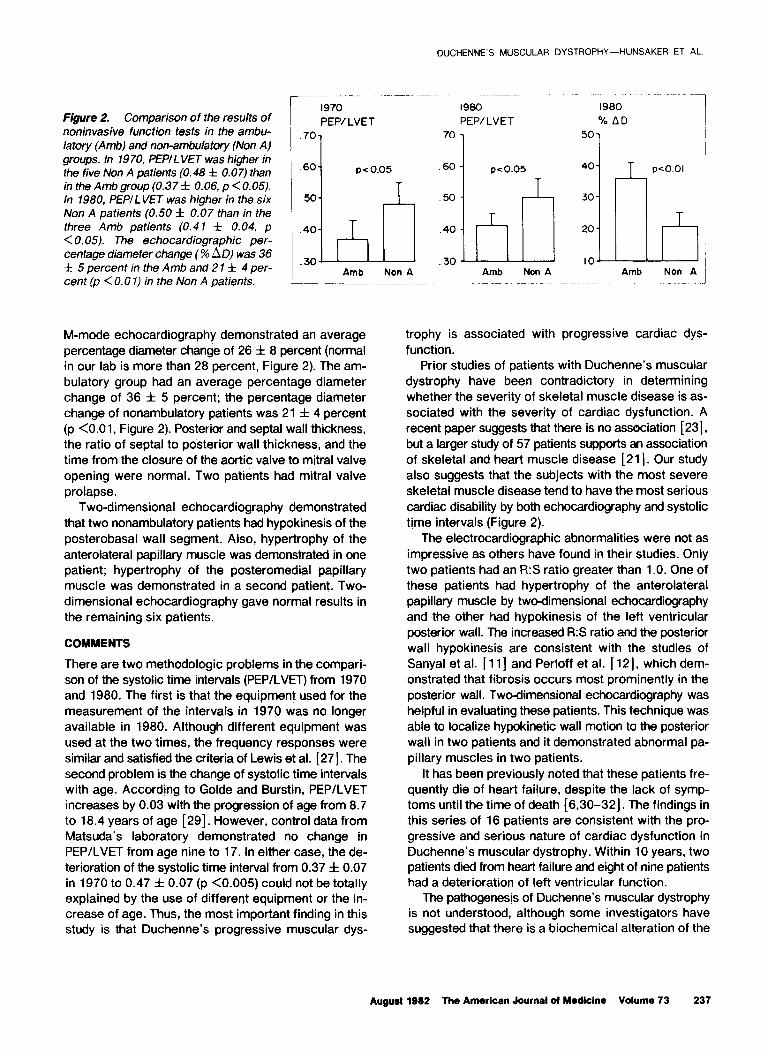
In 1970, 11 of the 16 patients were ambulatory. The PEPILVET results in these two groups are shown in Flgure 2. The 11 ambulatory patients had an average PEPILVET of 0.37 f 0.06; the nonambulatory patients, all of whom died during the lo-year follow-up period, had a PEP/LVET of 0.48 f 0.07 (p <0.05). In 1980, the three patients who were still ambulatory had a PEP/ LVET of 0.41 f 0.04 whereas the ratio in the nonam- bulatory patients was 0.50 f 0.07 (p <0.05, Figure 2).
236 August 1962 The American Journal of Medicine Volume 73
DUCHENNE’S MUSCULAR DYSTROPHY-HUNSAKER ET AL.
Figure 2. Comparison of the results of noninvasive function tests in the ambu- latory (Amb) and non-ambulatory (Non A) groups. In 1970, PEPI LVET was higher in
the five Non A patients (0.48 f 0.07) than in the Amb group (0.37 f 0.06, p <0.05). In 1980, PEPILVET was higher in the six Non A patients (0.50 f 0.07 than in the three Amb patients (0.41 f 0.04, p < 0.05). The echocardiographic per- centage diameter change (% AD) was 36 f 5 percent in the Amb and 2 1 f 4 per- cent (p < 0.0 I) in the Non A patients.
_
L
1970 1960 1980
PEP/ LVET PEPILVET % AD
.60 p < 0.05
M-mode echocardiography demonstrated an average percentage diameter change of 26 f 8 percent (normal in our lab is more than 28 percent, Figure 2). The am- bulatory group had an average percentage diameter change of 36 f 5 percent: the percentage diameter change of nonambulatory patients was 21 f 4 percent (p <O.Ol, Figure 2). Posterior and septal wall thickness, the ratio of septal to posterior wall thickness, and the time from the closure of the aortic valve to mitral valve opening were normal. Two patients had mitral valve prolapse.
Two-dimensional echocardiography demonstrated that two nonambulatory patients had hypokinesis of the posterobasal wall segment. Also, hypertrophy of the anterolateral papillary muscle was demonstrated in one patient; hypertrophy of the posteromedial papillary muscle was demonstrated in a second patient. Two- dimensional echocardiography gave normal results in the remaining six patients.
COMMENTS
There are two methodologic problems in the compari- son of the systolic time intervals (PEP/LVET) from 1970 and 1980. The first is that the equipment used for the measurement of the intervals in 1970 was no longer available in 1980. Although different equipment was used at the two times, the frequency responses were similar and satisfied the criteria of Lewis et al. [27]. The second problem is the change of systolic time intervals with age. According to Golde and Burstin, PEP/LVET increases by 0.03 with the progression of age from 8.7 to 18.4 years of age [ 291. However, control data from Matsuda’s laboratory demonstrated no change in PEPILVET from age nine to 17. In either case, the de- terioration of the systolic time interval from 0.37 f 0.07 in 1970 to 0.47 f 0.07 (p <0.005) could not be totally explained by the use of different equipment or the in- crease of age. Thus, the most important finding in this study is that Duchenne’s progressive muscular dys-
Non A
.60
50
pco.05 40
00 1
30
20
IO Amb Non A
T peo.01
I3 Non A
trophy is associated with progressive cardiac dys- function.
Prior studies of patients with Duchenne’s muscular dystrophy have been contradictory in determining whether the severity of skeletal muscle disease is as- sociated with the severity of cardiac dysfunction. A recent paper suggests that there is no association [ 231, but a larger study of 57 patients supports an association of skeletal and heart muscle disease [21]. Our study also suggests that the subjects with the most severe skeletal muscle disease tend to have the most serious cardiac disability by both echocardiography and systolic tjme intervals (Figure 2).
The electrocardiographic abnormalities were not as impressive as others have found in their studies. Only two patients had an R:S ratio greater than 1 .O. One of these patients had hypertrophy of the anterolateral papillary muscle by two-dimensional echocardiography and the other had hypokinesis of the left ventricular posterior wall. The increased R:S ratio and the posterior wall hypokinesis are consistent with the studies of Sanyal et al. [ 1 l] and Perloff et al. [ 121, which dem- onstrated that fibrosis occurs most prominently in the posterior wall. Two-dimensional echocardiiraphy was helpful in evaluating these patients. This technique was able to localize hypokinetic wall motion to the posterior wall in two patients and it demonstrated abnormal pa- pillary muscles in two patients.
It has been previously noted that these patients fre- quently die of heart failure, despite the lack of symp- toms until the time of death [6,30-32). The findings in this series of 16 patients are consistent with the pro- gressive and serious nature of cardiac dysfunction in Duchenne’s muscular dystrophy. Within 10 years, two patients died from heat-l failure and eight of nine patients had a deterioration of left ventricular function.
The pathogenesis of Duchenne’s muscular dystrophy is not understood, although some investigators have suggested that there is a biochemical alteration of the
August 1882 The American Journal ol Medicine Volume 73 237
DUCHENNE’S MUSCULAR DYSTROPHY-HUNSAKER ET AL
lipid portion of the membranes of skeletal muscle cells ACKNOWLEDGMENT [33-351. This study suggests that the heart muscle We would like to thank Michelle Newlin, R.N., for her shares a progressive muscular dystrophic abnormality assistance in the follow-up of these patients and Tami with skeletal muscle. Further studies on factors com- West for the preparation of the manuscript. We espe- mon to the skeletal and cardiac muscle cells may help cially appreciate the help of Jerry Mendell, M.D., for in defining the abnormality. permitting us to study his patients.
REFERENCES
4.
5.
6.
7.
a.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
Rubin IL, Buchberg AS: The heart in progressive muscular dystrophy. Am Heart J 1952; 43: 161-169.
Globus JH: The pathologic findings in the heart muscle in progressive muscular dystrophy. Arch Neurol Psychiatry 1923; 9: 59-72.
Zatuchni J, Aegerter EE, Molthan L, Shuman CR: The heart in progressive muscular dystrophy. Circulation 1951; 3: 846-853.
Nothacker WG, Netsky MG: Myocardial lesions in progressive muscular dystrophy. Arch Pathol 1950; 50: 576590.
Storstein 0, Austarheim K: Progressive muscular dystrophy of the heart. Acta Med Stand 1955; 150: 431-436.
Weisenfeld S, Messinger WJ: Cardiac involvement in pro- gressive muscular dystrophy. Am Heart J 1952; 43: 170-187.
Lowenstein AS, Arbeit SR, Rubin IL: Cardiac involvement in progressive muscular dystrophy. An electrocardiographic and ballistocardiographic study. Am J Cardiol 1962;9: 528-533.
Moore WF: Cardiac involvement in progressive muscular dystrophy. J Pediatr 1954; 44: 683-687.
Demany MA, Zimmerman HA: Progressive muscular dystro- phy. Hemodynamic, angiographic and pathologic study of a patient with myocardial involvement. Circulation 1969; 40: 377-383.
Harvey WP. Harvey JC, Fenoglio JJ, McAllister HA: Clinical pathologic conference. Am Heart J 1977; 93: 239-247.
Sanyal SK, Johnson WW. Thapar MK, Pitner SE: An ultra- structural basis for electrocardiographic alterations asso- ciated with Duchenne’s progressive muscular dystrophy. Circulation 1978; 57: 1122-l 129.
Perloff JK. Roberts WC, DeLeon AC Jr, O’Doherty D: The distinctive electrocardiogram of Duchenne’s progressive muscular dystrophy. Am J Med 1967; 42: 179-188.
Schott J, Jacobi M, Wald MA: Electrocardiographic patterns in the differential diagnosis of progressive muscular dys- trophy. Am J Med Sci 1955; 229: 517-524.
Skyring A, McKustck VA: Clinical genetic and electrocar- diographic studies in childhood muscular dystrophy. Am J Med Sci 1961; 242: 534-547.
lshikawa K, Yanagisawa A, lshihara T, Tamura T, lnoue M: Sequential changes of orthogonal electrocardiograms in progressive muscular dystrophy of the Duchenne type. Am Heart J 1979; 98: 73-82.
Zatuchni J, Baute A: Duchenne electrocardiogram in myotonia dystrophica. J Electrocardiol 1978; 11: 395-398.
Fitch CW, Ainger LE: The frank vectorcardiogram and the electrocardiogram in Duchenne progressive muscular dystrophy. Circulation 1967; 35: 1124- 1140.
Slucka C: The electrocardiogram in Duchenne progressive muscular dystrophy. Circulation 1968; 38: 933-940.
Gailani S, Danowski TS, Fisher DS: Muscular dystrophy. Catheterization studies indicating latent congestive heart
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
failure. Circulation 1958; 17: 583-568. Kovick RB, Fogelman AM, Abbasi AS, Peter JB, Pearce ML:
Echocardiographic evaluation of posterior left ventricular wall motion in muscular dystrophy. Circulation 1975; 52: 447-454.
Matsuda M, Akatsuka N, Yamaguchi T, et al.: Systolic time intervals in patients with progressive muscular dystrophy of the Duchenne type. Jpn Heart J 1977; 18: 636 651.
Ahmad M, Sanderson JE, Dubowitz V, Hallidie-Smith KA: Echocardiographic assessment of left ventricular function in Duchenne’s muscular dystrophy. Br Heart J 1978; 40: 734-740.
Farah MG, Evans EB, Vignos PJ Jr: Echocardiographic eval- uation of left ventricular function in Duchenne’s muscular dystrophy. Am J Med 1980; 69: 248-254.
Heymsfield SB, McNish T, Perkins JV, Felner JM: Sequence of cardiac changes in Duchenne muscular dystrophy. Am Heart J 1978; 95: 283-294.
Boas EP, Lowenburg H: The heart in progressive muscular dystrophy. Studies with the cardiotachometer. Arch Intern Med 1931; 47: 376-383.
Swinyard CA, Deaver GG. Greenspon L: Gradients of functional ability of importance in rehabilitation of patients with pro- gressive muscular and neuromuscular disease. Arch Phys Med Rehabil 1957; 38: 574.
Lewis RP. Leighton RF, Forester WF, Weissler AM: Systolic time intervals. In: Weissler AM, ed. Non-invasive cardiology. New York: Grune & Stratton, 1974: 301.
Sahn DJ, DeMaria A, Kisslo J, Weyman H: The Committee on M-Mode Standardization of the American Society of Echocardiography: recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation 1978; 58: 1072.
Golde D, Burstin L: Systolic phases of the cardiac cycle in children. Circulation 1970; 42: 1029-1036.
Perloff JK, DeLeon AC Jr, O’Doherty D: The cardiomyopathy of progressive muscular dystrophy. Circulation 1966; 33: 625-648.
Gilroy J, Cahalan JL, Berman R, Newman M: Cardiac and pulmonary complications in Duchenne’s progressive muscular dystrophy. Circulation 1963; 27: 484-493.
Berenbaum AA, Horowitz W: Heart involvement in progressive muscular dystrophy. Am Heart J 1956; 51: 622-627.
Rowland LP: Pathogenesis of muscular dystrophies. Arch Neurol 1976; 33: 315-321.
Roses AD, Herbstreith MH, Appel SH: Membrane protein ki- nase alteration in Duchenne muscular dystrophy. Nature 1975; 254: 350-35 1.
l-lowland JL, lyer SL: Erythrocyte lipids inheterozygous carriers of Duchenne muscular dystrophy. Science 1977; 198: 309-310.
238 August 1982 The American Journal of Medlclne Volume 73


















