Embed Size (px)
Citation preview

Cardiac Rehabilitation – Cardiac Rehabilitation – The Evidence Base & The Evidence Base &
Implications for PracticeImplications for Practice
Rod Taylor MSc, PhDRod Taylor MSc, PhDDept of Public Health & EpidemiologyDept of Public Health & Epidemiology
University of BirminghamUniversity of Birmingham
Bisperbjerg Hospital, Copenhagen11th & 12th December 2003

Presentation
• Update on the Cochrane systematic reviews of [exercise-based] CR?
• What are implications for current CR practice & future?

Acknowledgements
• Judy Jolliffee - St Loye’s School of Health Studies, Exeter, UK
• Karen Rees - Department of Social Medicine, University of Bristol, UK
• Canadian Coordinating Centre for Health Technology Assessment (CCOHTA)

Exercise Based CR - Meta Analyses
Oldridge
1988
O’Connor
1989
Cochrane I
2000
Cochrane II 2003*
Diagnosis MI MI CHD CHD
RCTs (n) 10 22 34 48
CCR/Ex only - - 20/14 30/19
Patients (n) 4,347 4,554 7,996 8,940
Outcomes Mortality Mortality Mortality
Risk factors
HRQL
Mortality
Risk factors
HRQL
Sub-group analysis
*Taylor et al, Am J Med 2004 [in press]

Making policy decisions…

Whose getting rehab?
0 20 40 60 80 100
% loss to follow up
Outcome blinding
Adequate concealment
Mean age
Include Women
Include CABG/ PTCA
Exclusively MI
Percentage
Trials before 1990 Trials since 1990

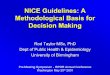
What’s the overall impact of CR on events?
Relative Risk
0.50 0.75 1.0 1.25
Need for PTCAN=12 trials
Need for CABGN=23 trials
Non fatal MIN=33 trials
Cardiac MortalityN=31 trials
Total mortalityN=41 trials
FAVOURS REHABILITATION

Impact of CR – Risk Factors
Mean Reduction
(95% CI)
Blood Pressure Systolic blood pressure (mmHg) [9 trials]
Diastolic blood pressure (mmHg) [6 trials]
-0.5 (-6.5 to 5.5)
-0.6 (4.5 to 2.8)
Blood Lipids Total cholesterol (mmol/l) [19 trials]
HDL cholesterol (mmol/l) [14 trials]
LDL cholesterol (mmol/l) [14 trials]
Triglycerides (mmol/l) [13 trials]
-0.34 (-0.56 to -0.11)
0.03 (-0.06 to 0.11)
-0.32 (-0.55 to -0.10)
-0.28 (-0.49 to -0.06)
Relative Risk (95% CI)
Smoking [13 trials] 0.77 (0.62 to 0.94)

Do we improve patient’s quality of life?
• Nine trials (20%) assessed HRQoL using either validated measures or measures that covered 3 domains [physical, psychological and social well being]
• Range of both generic (SF-36, NHP, Karolinska, QWB, TTO) and disease specific HRQoL measures were used (QLMI).
• Although all RCTs studies improvement in HRQoL with CR, few studies reported improvements in excess of usual care

Other Cardiac Rx’s – how do we compare?
Relative reduction in all cause mortality
Reduction in all cause mortality
per 1000 per year
ß-blockers Freemantle, 1999
31 trials
[24,974]
23% (15% to 31%)
12 (6 to 17)
ACE inhibitorsNofE Gudelines, 2001
22 trials
[102,476]
17% (2% to 11%) 4 (1 to 6)
StatinsLa Rosa, 1999
3 trials
[17,617]
23% (15% to 30%)
4 (2 to 6)
AntiplateletsAntiplatelet trialists, 1994
11 trials
[18,773]
24% (16% to 32%)
7 (1 to 3)
Cardiac rehabCochrane, 2003
44 trials
[~9,000]
16% (4% to 27%) 9 (15 to 116)

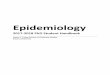
Subgroups?
Odds Ratio
0.5 1.0 1.5
Jadad score >3 [4]Jadad score =<3 [28]
Publication after 1995 [6]Publication up to 1995 [27]
Follow up >24 months [16]Follow up 24 months [17]
Dose >1,000 [8]Dose 1,000 [5]
CCR [21]EX CR [12]
All CHD diagnoses [9]Post MI only [23]

Are we effective in the long-term?
• Three CR RCTs assessed CR outcomes for 10-years– Bethall et al (1999) – 11 yr fu– Hamalanien et al (1989 & 1995) – 10 & 15 yr fu on
Kallio trial– Dorn et al (1999) 19 yr fu on NEDHP trial
• None report a significant reduction in mortality
• Implication– Importance of maintenance of lifestyle changes

NEDHP survival curve

Heart Failure - Mortality

Heart Failure – VO2max

2
““The drug itself has no side effects - The drug itself has no side effects - but the number of health economists needed to but the number of health economists needed to prove its value may cause dizziness and nausea”prove its value may cause dizziness and nausea”

How much does CR cost?
Gray et al (1997) • Random selection of 16 UK CR centres• Detailed collection of health service salary (1994)
costs– Centre cost per programme/year - £33K (95% CI: £28K
to £38K)– Patient cost per/year - £223 (95%CI: £262 to £332)
• Predictors of cost - No. of patients/centre, no. of patient hrs– X - No. of assessments, equipment available, drop out
rate & range of indications

Is CR Cost Effective?
Author Setting Currency year
Cost Effectiveness
Lowensteyn (2000)
Canada 1996 <$15,000 per LYG
Ades (1997) US 1995 $4,950 per year of life
Oldridge (1993)
Canada 1991 $9,200 per QALY
$21,800 per LYG

Comparative Cost Effectiveness
Intervention Comparator Cost-effectiveness Ratio
Smoking cessation program97 No therapy US$220 per LYG* (1991)
Education to promote cholesterol reduction118
No intervention US$3,475 per LYG** (1999)
Coronary artery angioplasty (one vessel, severe angina)97
Medical care US$8,700 per QALY*** (1993)
Lipid lowering (Simvastatin) for secondary prevention97
No therapy US$9,630 per LYG (1996)
Cardiac rehabilitation98 (Included study - Oldridge et al. 1993)
Usual care US$21,800 per LYG (1991) US$9,200 per QALY (1991)
CABG118 PTCA US$26,570 per LYG** (1999)
Tissue plasminogen activator118 Treatment with streptokinase US$35,257 per LYG** (1999)
Thrombolytic reperfusion (t-PA, anterior MI, age 41-60)97
Streptokinase US$49,900 per LYG (1993)
Captopril (in 50 year old patients surviving MI)117
No captopril US$76,000 per QALY (1998)
Coronary artery angioplasty (one vessel, mild angina)97
Medical care US$126,400 per QALY (1993)

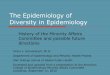
Can we (effectively) deliver in
alternative settings?
difference in exercise capacity METS-.790825 1.20199
Combined
Carlson (33))
Sparks (29)
Miller (8,9,11)
Bell (17)

Conclusions
• Updated review of Cochrane systematic review of RCTs confirms medium term mortality and risk factor benefits of exercise-based CR
• Increasing evidence of these benefits not only in post MI patients but also other patient groups [revascularisation, angina and heart failure patients]

Conclusions cont
• Remains relatively little RCT evidence of CR in women and older individuals
• Positive impact of CR on quality of life remains unclear
• Limited evidence for the equivalence of home/community-based CR compared to traditional hospital-based programmes