Embed Size (px)
Citation preview

Cardiac resynchronisation therapy for heart failure
M. Dayer & R. PopatDepartment of Cardiology, Royal Brompton Hospital, London.
Abstract
Heart failure is an increasingly common problem in Europe, affecting between 0.4 and 2% of the population. Cardiac resynchronisation therapy has now established itself as a new treatment for patients with more severe heart failure. However, at present it only appears to help around two-thirds of the patients in whom it is implanted. This chapter will focus on the evidence behind this new therapy and discuss how we might improve the success rate in the future.
Keywords: heart failure, cardiac resynchronisation therapy, echocardiography
1 Introduction
Chronic heart failure (CHF) is a constellation of symptoms underpinned by failure of the heart, in particular the left ventricle, to supply the body with the quantity of blood it requires to func-tion normally. Typical symptoms include shortness of breath on relatively minor exertion and fatigue. Some patients become cachectic; they gradually lose their muscle mass, probably as a consequence of both inactivity and the disease process itself. For many, fl uid retention in their lungs (pulmonary oedema), lower limbs (peripheral oedema) and abdomen (ascites) is a major problem. It is not uncommon for patients to gradually accrue 10 l or more of excess fl uid, which may lead to a prolonged hospital stay.
Heart failure is a common disease in Europe and is increasing in prevalence. It affects some-where between 0.4 and 2% [1] of the population, the variation being due to inconsistent defi ni-tions and methods of data capture. It is predominantly a disease of the elderly, with a mean age of onset of 74 years. The most frequent cause in the UK is ischaemic heart disease.
The prognosis of heart failure is thought to be poor, with an estimated mortality of around 60% after 5 years [2]. This rather dismal prognosis, comparable to many cancers, may improve [3], and the widespread adoption of drugs, particularly beta-blockers and angiotensin converting enzyme inhibitors, will hopefully impact benefi cially in the future.
Cardiac resynchronisation therapy (CRT) has now established itself as an important thera-peutic option for patients with severe CHF. Many patients with heart failure have ventricles which contract in an uncoordinated or dyssynchronous manner. CRT, which involves activat-ing the various chambers of the heart, using a pacemaker, in a carefully timed sequence, can improve heart function in such individuals. We will review some of the evidence supporting its use in carefully selected patients with heart failure, and discuss why it appears to work only in about two-thirds of patients and how we may improve this fi gure in the future. The technical details of device programming and implantation are beyond the scope of this chapter.
WITPress_RRPS_ch005.indd 87WITPress_RRPS_ch005.indd 87 4/29/2008 4:43:13 PM4/29/2008 4:43:13 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
doi:10.2495/978-1-84564-096-5/05
88 REPAIR AND REDESIGN OF PHYSIOLOGICAL SYSTEMS
2 Basic concepts and techniques
2.1 Methods for assessing the severity of heart failure
There are various methods for standardising the assessment of patients with heart failure which clinicians fi nd useful. It is usual to combine several measures to attempt to describe how severely affected patients are with heart failure.
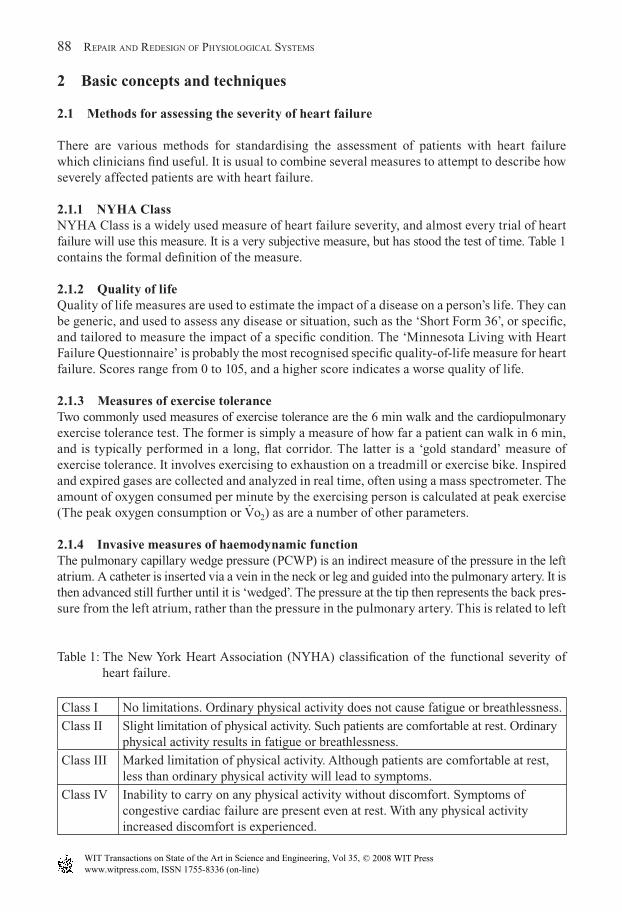
2.1.1 NYHA ClassNYHA Class is a widely used measure of heart failure severity, and almost every trial of heart failure will use this measure. It is a very subjective measure, but has stood the test of time. Table 1 contains the formal defi nition of the measure.
2.1.2 Quality of lifeQuality of life measures are used to estimate the impact of a disease on a person’s life. They can be generic, and used to assess any disease or situation, such as the ‘Short Form 36’, or specifi c, and tailored to measure the impact of a specifi c condition. The ‘Minnesota Living with Heart Failure Questionnaire’ is probably the most recognised specifi c quality-of-life measure for heart failure. Scores range from 0 to 105, and a higher score indicates a worse quality of life.
2.1.3 Measures of exercise toleranceTwo commonly used measures of exercise tolerance are the 6 min walk and the cardiopulmonary exercise tolerance test. The former is simply a measure of how far a patient can walk in 6 min, and is typically performed in a long, fl at corridor. The latter is a ‘gold standard’ measure of exercise tolerance. It involves exercising to exhaustion on a treadmill or exercise bike. Inspired and expired gases are collected and analyzed in real time, often using a mass spectrometer. The amount of oxygen consumed per minute by the exercising person is calculated at peak exercise (The peak oxygen consumption or V
.o2) as are a number of other parameters.
2.1.4 Invasive measures of haemodynamic functionThe pulmonary capillary wedge pressure (PCWP) is an indirect measure of the pressure in the left atrium. A catheter is inserted via a vein in the neck or leg and guided into the pulmonary artery. It is then advanced still further until it is ‘wedged’. The pressure at the tip then represents the back pres-sure from the left atrium, rather than the pressure in the pulmonary artery. This is related to left
Table 1: The New York Heart Association (NYHA) classifi cation of the functional severity of heart failure.
Class I No limitations. Ordinary physical activity does not cause fatigue or breathlessness.
Class II Slight limitation of physical activity. Such patients are comfortable at rest. Ordinary physical activity results in fatigue or breathlessness.
Class III Marked limitation of physical activity. Although patients are comfortable at rest, less than ordinary physical activity will lead to symptoms.
Class IV Inability to carry on any physical activity without discomfort. Symptoms of congestive cardiac failure are present even at rest. With any physical activity increased discomfort is experienced.
WITPress_RRPS_ch005.indd 88WITPress_RRPS_ch005.indd 88 4/29/2008 4:43:13 PM4/29/2008 4:43:13 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
CARDIAC RESYNCHRONISATION THERAPY FOR HEART FAILURE 89
ventricular function. When ventricular function worsens, the left atrial pressure, and hence the PCWP, rise. Typically pressures above 30 mm Hg are associated with severe symptoms. Patients with heart failure typically have reduced cardiac outputs (the amount of blood pumped by the heart over a given time period, usually measured in litres/minute; a typical resting value is approximately 5 l/min). There are an ever-increasing number of methods for estimating cardiac output, which are beyond the scope of this chapter.
2.2 Normal cardiac anatomy and function
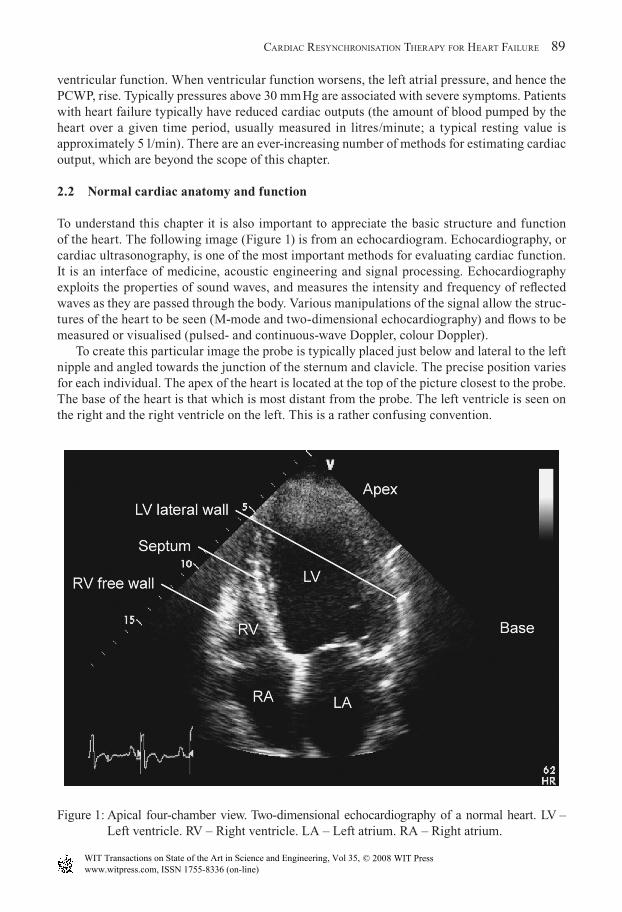
To understand this chapter it is also important to appreciate the basic structure and function of the heart. The following image (Figure 1) is from an echocardiogram. Echocardiography, or cardiac ultrasonography, is one of the most important methods for evaluating cardiac function. It is an interface of medicine, acoustic engineering and signal processing. Echocardiography exploits the properties of sound waves, and measures the intensity and frequency of refl ected waves as they are passed through the body. Various manipulations of the signal allow the struc-tures of the heart to be seen (M-mode and two-dimensional echocardiography) and fl ows to be measured or visualised (pulsed- and continuous-wave Doppler, colour Doppler).
To create this particular image the probe is typically placed just below and lateral to the left nipple and angled towards the junction of the sternum and clavicle. The precise position varies for each individual. The apex of the heart is located at the top of the picture closest to the probe. The base of the heart is that which is most distant from the probe. The left ventricle is seen on the right and the right ventricle on the left. This is a rather confusing convention.
Figure 1: Apical four-chamber view. Two-dimensional echocardiography of a normal heart. LV – Left ventricle. RV – Right ventricle. LA – Left atrium. RA – Right atrium.
WITPress_RRPS_ch005.indd 89WITPress_RRPS_ch005.indd 89 4/29/2008 4:43:13 PM4/29/2008 4:43:13 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
90 REPAIR AND REDESIGN OF PHYSIOLOGICAL SYSTEMS
The ejection fraction is an estimate of the percentage change in volume of the left ventricle as it contracts. It is typically measured by echocardiography. There are a number of techniques described to estimate this value. In healthy individuals, 60–80% of the blood is ejected by the ventricle during contraction. During heart failure this falls to below 55%. In patients more severely affected by typical systolic left ventricular failure an ejection fraction of less than 35% is not uncommon.
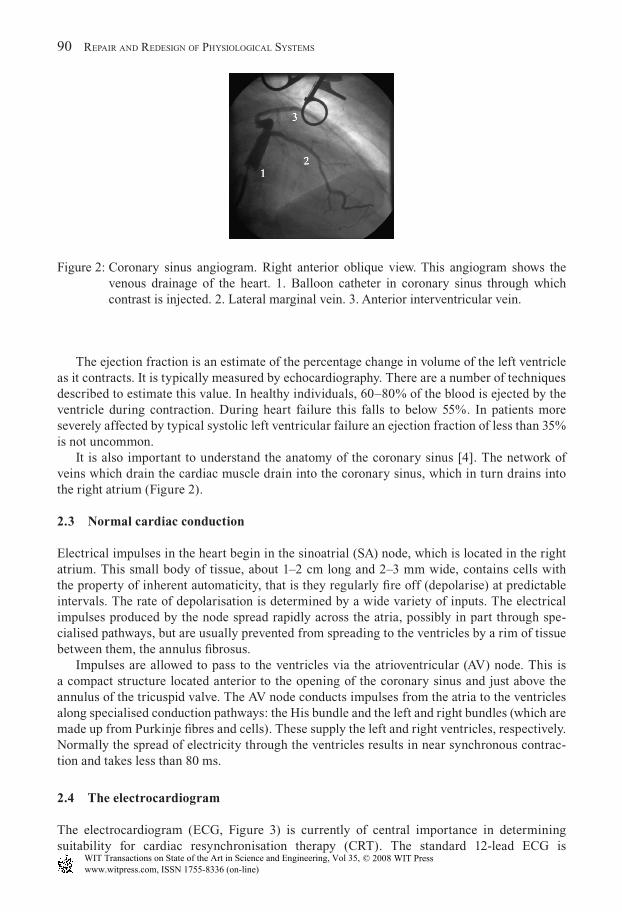
It is also important to understand the anatomy of the coronary sinus [4]. The network of veins which drain the cardiac muscle drain into the coronary sinus, which in turn drains into the right atrium (Figure 2).
2.3 Normal cardiac conduction
Electrical impulses in the heart begin in the sinoatrial (SA) node, which is located in the right atrium. This small body of tissue, about 1–2 cm long and 2–3 mm wide, contains cells with the property of inherent automaticity, that is they regularly fi re off (depolarise) at predictable intervals. The rate of depolarisation is determined by a wide variety of inputs. The electrical impulses produced by the node spread rapidly across the atria, possibly in part through spe-cialised pathways, but are usually prevented from spreading to the ventricles by a rim of tissue between them, the annulus fi brosus.
Impulses are allowed to pass to the ventricles via the atrioventricular (AV) node. This is a compact structure located anterior to the opening of the coronary sinus and just above the annulus of the tricuspid valve. The AV node conducts impulses from the atria to the ventricles along specialised conduction pathways: the His bundle and the left and right bundles (which are made up from Purkinje fi bres and cells). These supply the left and right ventricles, respectively. Normally the spread of electricity through the ventricles results in near synchronous contrac-tion and takes less than 80 ms.
2.4 The electrocardiogram
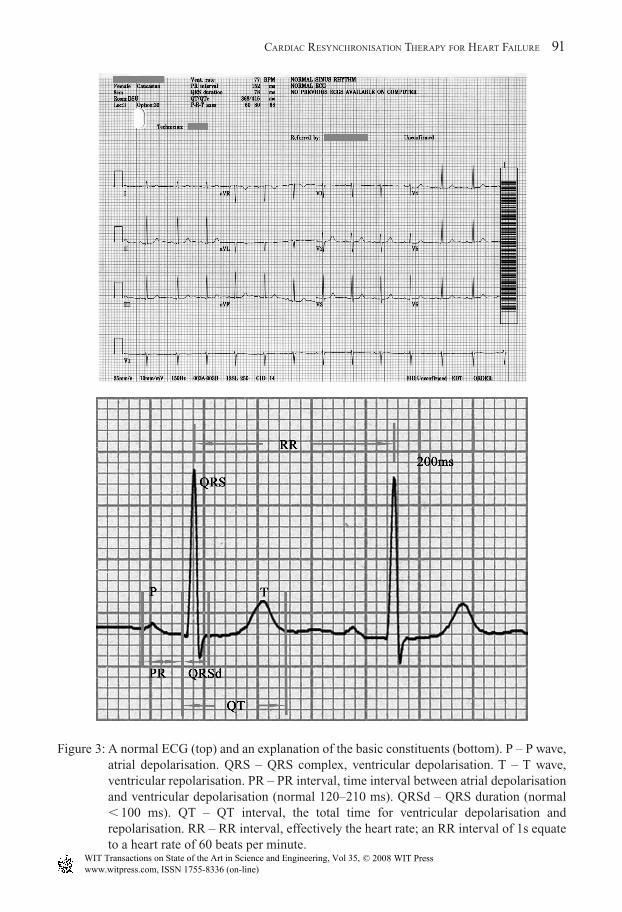
The electrocardiogram (ECG, Figure 3) is currently of central importance in determining suitability for cardiac resynchronisation therapy (CRT). The standard 12-lead ECG is
Figure 2: Coronary sinus angiogram. Right anterior oblique view. This angiogram shows the venous drainage of the heart. 1. Balloon catheter in coronary sinus through which contrast is injected. 2. Lateral marginal vein. 3. Anterior interventricular vein.
WITPress_RRPS_ch005.indd 90WITPress_RRPS_ch005.indd 90 4/29/2008 4:43:15 PM4/29/2008 4:43:15 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
CARDIAC RESYNCHRONISATION THERAPY FOR HEART FAILURE 91
Figure 3: A normal ECG (top) and an explanation of the basic constituents (bottom). P – P wave, atrial depolarisation. QRS – QRS complex, ventricular depolarisation. T – T wave, ventricular repolarisation. PR – PR interval, time interval between atrial depolarisation and ventricular depolarisation (normal 120–210 ms). QRSd – QRS duration (normal � 100 ms). QT – QT interval, the total time for ventricular depolarisation and repolarisation. RR – RR interval, effectively the heart rate; an RR interval of 1s equate to a heart rate of 60 beats per minute.
WITPress_RRPS_ch005.indd 91WITPress_RRPS_ch005.indd 91 4/29/2008 4:43:16 PM4/29/2008 4:43:16 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
92 REPAIR AND REDESIGN OF PHYSIOLOGICAL SYSTEMS
representative of the heart’s electrical activity, recorded by 10 electrodes placed on the body surface.
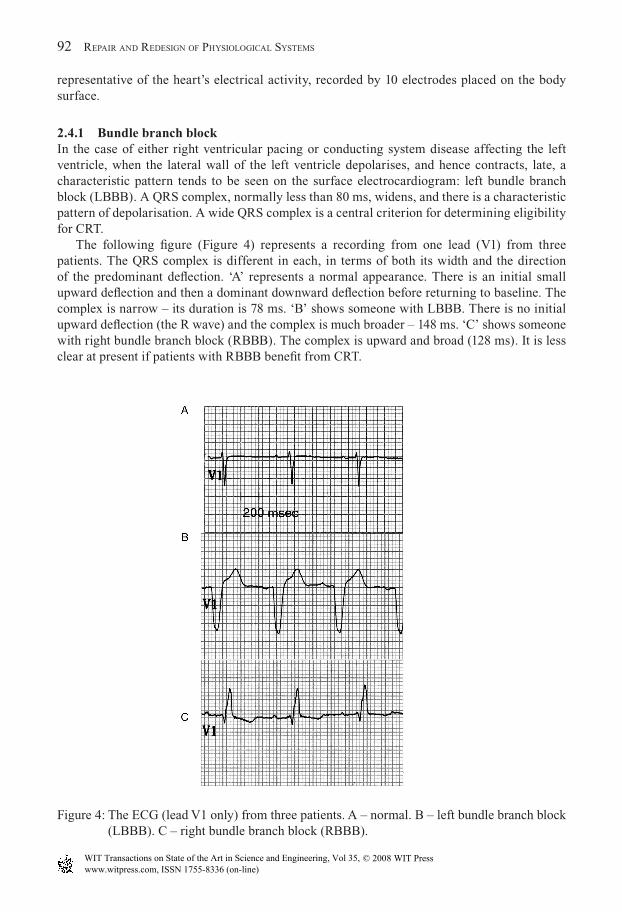
2.4.1 Bundle branch blockIn the case of either right ventricular pacing or conducting system disease affecting the left ventricle, when the lateral wall of the left ventricle depolarises, and hence contracts, late, a characteristic pattern tends to be seen on the surface electrocardiogram: left bundle branch block (LBBB). A QRS complex, normally less than 80 ms, widens, and there is a characteristic pattern of depolarisation. A wide QRS complex is a central criterion for determining eligibility for CRT.
The following fi gure (Figure 4) represents a recording from one lead (V1) from three patients. The QRS complex is different in each, in terms of both its width and the direction of the predominant defl ection. ‘A’ represents a normal appearance. There is an initial small upward defl ection and then a dominant downward defl ection before returning to baseline. The complex is narrow – its duration is 78 ms. ‘B’ shows someone with LBBB. There is no initial upward defl ection (the R wave) and the complex is much broader – 148 ms. ‘C’ shows someone with right bundle branch block (RBBB). The complex is upward and broad (128 ms). It is less clear at present if patients with RBBB benefi t from CRT.
Figure 4: The ECG (lead V1 only) from three patients. A – normal. B – left bundle branch block (LBBB). C – right bundle branch block (RBBB).
WITPress_RRPS_ch005.indd 92WITPress_RRPS_ch005.indd 92 4/29/2008 4:43:19 PM4/29/2008 4:43:19 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
CARDIAC RESYNCHRONISATION THERAPY FOR HEART FAILURE 93
3 Conventional pacing and cardiac resynchronisation therapy
3.1 Conventional permanent pacing
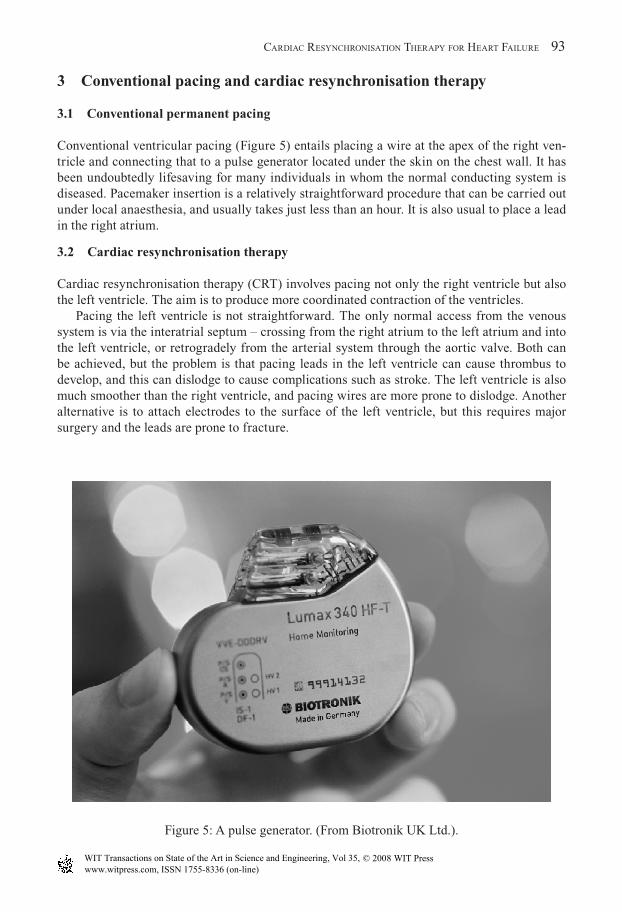
Conventional ventricular pacing (Figure 5) entails placing a wire at the apex of the right ven-tricle and connecting that to a pulse generator located under the skin on the chest wall. It has been undoubtedly lifesaving for many individuals in whom the normal conducting system is diseased. Pacemaker insertion is a relatively straightforward procedure that can be carried out under local anaesthesia, and usually takes just less than an hour. It is also usual to place a lead in the right atrium.
3.2 Cardiac resynchronisation therapy
Cardiac resynchronisation therapy (CRT) involves pacing not only the right ventricle but also the left ventricle. The aim is to produce more coordinated contraction of the ventricles.
Pacing the left ventricle is not straightforward. The only normal access from the venous system is via the interatrial septum – crossing from the right atrium to the left atrium and into the left ventricle, or retrogradely from the arterial system through the aortic valve. Both can be achieved, but the problem is that pacing leads in the left ventricle can cause thrombus to develop, and this can dislodge to cause complications such as stroke. The left ventricle is also much smoother than the right ventricle, and pacing wires are more prone to dislodge. Another alternative is to attach electrodes to the surface of the left ventricle, but this requires major surgery and the leads are prone to fracture.
Figure 5: A pulse generator. (From Biotronik UK Ltd.).
WITPress_RRPS_ch005.indd 93WITPress_RRPS_ch005.indd 93 4/29/2008 4:43:20 PM4/29/2008 4:43:20 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
94 REPAIR AND REDESIGN OF PHYSIOLOGICAL SYSTEMS
These limitations can be resolved by inserting pacing wires down the coronary sinus. Although this is a standard approach, it is technically challenging; it requires a great deal of skill to achieve implants successfully, and procedures typically take between 1 and 2 hours. Lead technology still needs a lot of improvement, as these leads are much more prone to dislodge than those placed in the right atrium or ventricle.
4 Dyssynchrony
Dyssynchrony and its assessment is a concept of abnormal ventricular function which is important to understand in the context of cardiac resynchronisation therapy, as the correction of dyssyn-chrony is the proposed mechanism by which CRT works. In this context, dyssynchrony is the term used to describe the situation in which one part of the heart is working out of step with another part. The presence of dyssynchrony does not imply the presence of heart failure, but when present in heart failure it is often associated with more severe symptoms. There are three types of dyssynchrony: atrio-ventricular (AV) dyssynchrony, interventricular dyssynchrony and intraventricular dyssynchrony.
It is hard to determine the precise prevalence of the different types of dyssynchrony in patients with heart failure, as the methods for determining interventricular and intraventricular dyssynchrony are many and varied, and there remains some debate in the literature over defi ni-tions. This situation is likely to be dealt with as further studies become available.
4.1 Atrioventricular dyssynchrony
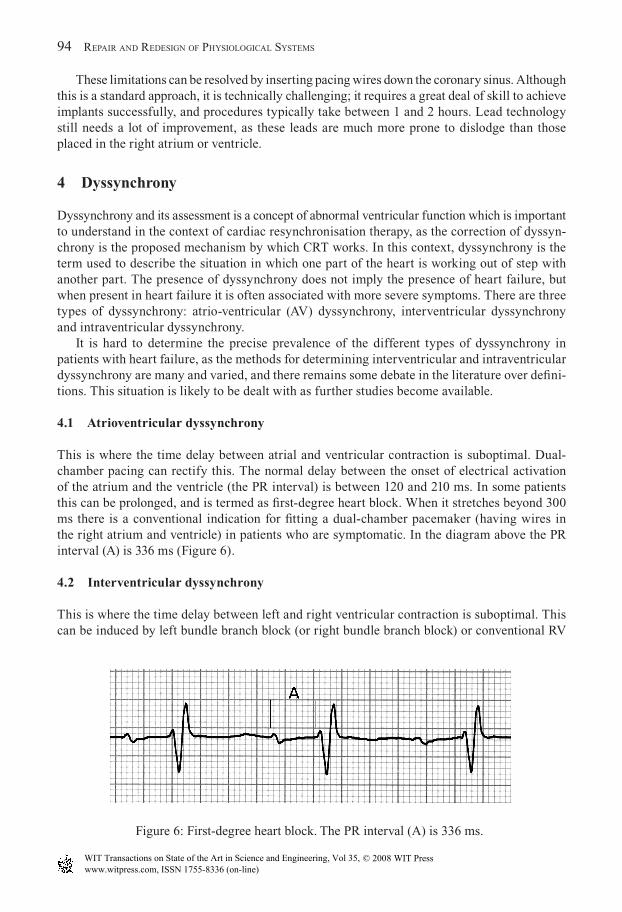
This is where the time delay between atrial and ventricular contraction is suboptimal. Dual-chamber pacing can rectify this. The normal delay between the onset of electrical activation of the atrium and the ventricle (the PR interval) is between 120 and 210 ms. In some patients this can be prolonged, and is termed as fi rst-degree heart block. When it stretches beyond 300 ms there is a conventional indication for fi tting a dual-chamber pacemaker (having wires in the right atrium and ventricle) in patients who are symptomatic. In the diagram above the PR interval (A) is 336 ms (Figure 6).
4.2 Interventricular dyssynchrony
This is where the time delay between left and right ventricular contraction is suboptimal. This can be induced by left bundle branch block (or right bundle branch block) or conventional RV
Figure 6: First-degree heart block. The PR interval (A) is 336 ms.
WITPress_RRPS_ch005.indd 94WITPress_RRPS_ch005.indd 94 4/29/2008 4:43:20 PM4/29/2008 4:43:20 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press

CARDIAC RESYNCHRONISATION THERAPY FOR HEART FAILURE 95
apical pacing, and can be rectifi ed by CRT. It can be evaluated using echocardiography. Two echocardiographic techniques are commonly used to evaluate interventricular dyssynchrony. One simple technique is to measure the time from the onset of the QRS complex to start of ejection of blood through the pulmonary valve (right side) and aortic valve (left side) using pulsed-wave Doppler (Figure 7). A difference between these two intervals of greater than 40 ms has been proposed to indicate interventricular dyssynchrony [5].
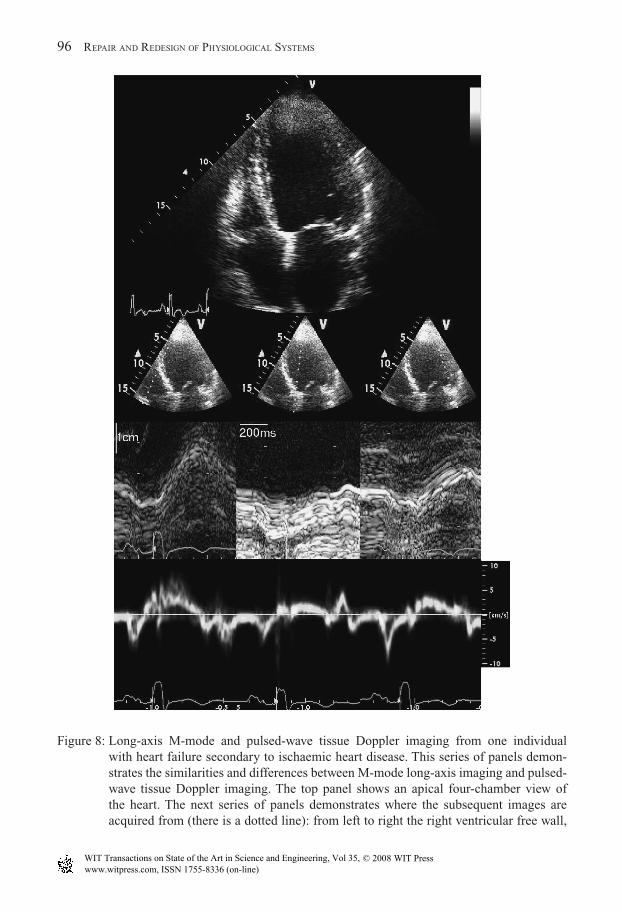
Tissue Doppler imaging (TDI) has also been used. This technique follows a particular part of the ventricular wall as it moves through systole and diastole and records the instantaneous velocities at intervals through this period. In this situation the peak systolic velocities of the right ventricular free wall, septum and left ventricular lateral wall, and their timing in relation to the QRS complex are recorded (Figure 8).
4.3 Intraventricular dyssynchrony
This is where the time delay between the contraction of different segments of the left ventricle is suboptimal. It is seen particularly in patients with heart failure and broad QRS durations. This can be rectifi ed by CRT.
There appear to be an increasing number of methods for determining intraventricular left ventricular dyssynchrony, as it is believed that these methods can be used to refi ne patient
Figure 7: Pulsed-wave Doppler to assess timing difference between pulmonary (P) and aortic (A) blood fl ow in a patient with heart failure secondary to ischaemic heart disease. In this example the difference is negligible and there is no interventricular dyssynchrony.
WITPress_RRPS_ch005.indd 95WITPress_RRPS_ch005.indd 95 4/29/2008 4:43:21 PM4/29/2008 4:43:21 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
96 REPAIR AND REDESIGN OF PHYSIOLOGICAL SYSTEMS
Figure 8: Long-axis M-mode and pulsed-wave tissue Doppler imaging from one individual with heart failure secondary to ischaemic heart disease. This series of panels demon-strates the similarities and differences between M-mode long-axis imaging and pulsed-wave tissue Doppler imaging. The top panel shows an apical four-chamber view of the heart. The next series of panels demonstrates where the subsequent images are acquired from (there is a dotted line): from left to right the right ventricular free wall,
WITPress_RRPS_ch005.indd 96WITPress_RRPS_ch005.indd 96 4/29/2008 4:43:21 PM4/29/2008 4:43:21 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
CARDIAC RESYNCHRONISATION THERAPY FOR HEART FAILURE 97
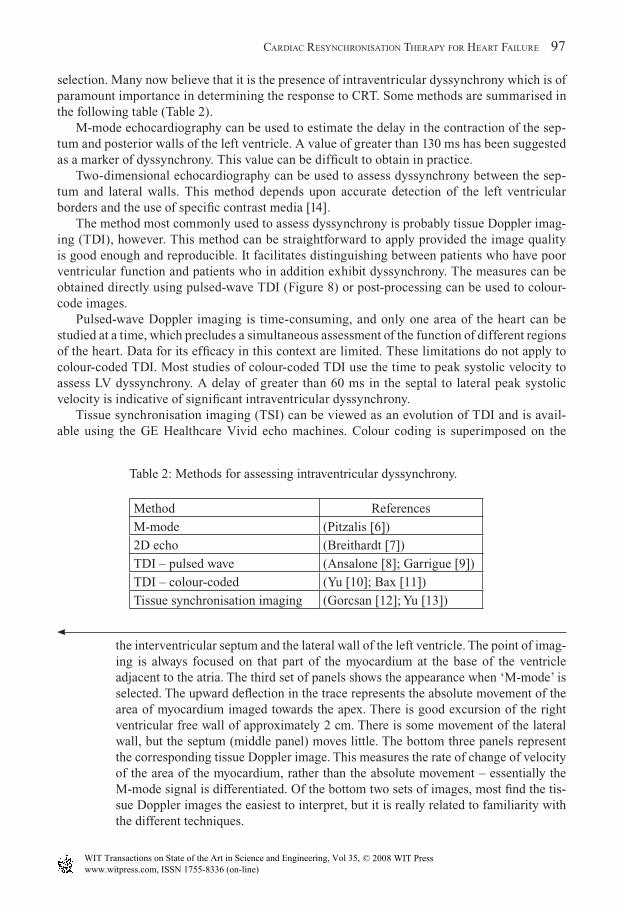
selection. Many now believe that it is the presence of intraventricular dyssynchrony which is of paramount importance in determining the response to CRT. Some methods are summarised in the following table (Table 2).
M-mode echocardiography can be used to estimate the delay in the contraction of the sep-tum and posterior walls of the left ventricle. A value of greater than 130 ms has been suggested as a marker of dyssynchrony. This value can be diffi cult to obtain in practice.
Two-dimensional echocardiography can be used to assess dyssynchrony between the sep-tum and lateral walls. This method depends upon accurate detection of the left ventricular borders and the use of specifi c contrast media [14].
The method most commonly used to assess dyssynchrony is probably tissue Doppler imag-ing (TDI), however. This method can be straightforward to apply provided the image quality is good enough and reproducible. It facilitates distinguishing between patients who have poor ventricular function and patients who in addition exhibit dyssynchrony. The measures can be obtained directly using pulsed-wave TDI (Figure 8) or post-processing can be used to colour-code images.
Pulsed-wave Doppler imaging is time-consuming, and only one area of the heart can be studied at a time, which precludes a simultaneous assessment of the function of different regions of the heart. Data for its effi cacy in this context are limited. These limitations do not apply to colour-coded TDI. Most studies of colour-coded TDI use the time to peak systolic velocity to assess LV dyssynchrony. A delay of greater than 60 ms in the septal to lateral peak systolic velocity is indicative of signifi cant intraventricular dyssynchrony.
Tissue synchronisation imaging (TSI) can be viewed as an evolution of TDI and is avail-able using the GE Healthcare Vivid echo machines. Colour coding is superimposed on the
the interventricular septum and the lateral wall of the left ventricle. The point of imag-ing is always focused on that part of the myocardium at the base of the ventricle adjacent to the atria. The third set of panels shows the appearance when ‘M-mode’ is selected. The upward defl ection in the trace represents the absolute movement of the area of myocardium imaged towards the apex. There is good excursion of the right ventricular free wall of approximately 2 cm. There is some movement of the lateral wall, but the septum (middle panel) moves little. The bottom three panels represent the corresponding tissue Doppler image. This measures the rate of change of velocity of the area of the myocardium, rather than the absolute movement – essentially the M-mode signal is differentiated. Of the bottom two sets of images, most fi nd the tis-sue Doppler images the easiest to interpret, but it is really related to familiarity with the different techniques.
Table 2: Methods for assessing intraventricular dyssynchrony.
Method References
M-mode (Pitzalis [6])
2D echo (Breithardt [7])
TDI – pulsed wave (Ansalone [8]; Garrigue [9])
TDI – colour-coded (Yu [10]; Bax [11])
Tissue synchronisation imaging (Gorcsan [12]; Yu [13])
WITPress_RRPS_ch005.indd 97WITPress_RRPS_ch005.indd 97 4/29/2008 4:43:22 PM4/29/2008 4:43:22 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
98 REPAIR AND REDESIGN OF PHYSIOLOGICAL SYSTEMS
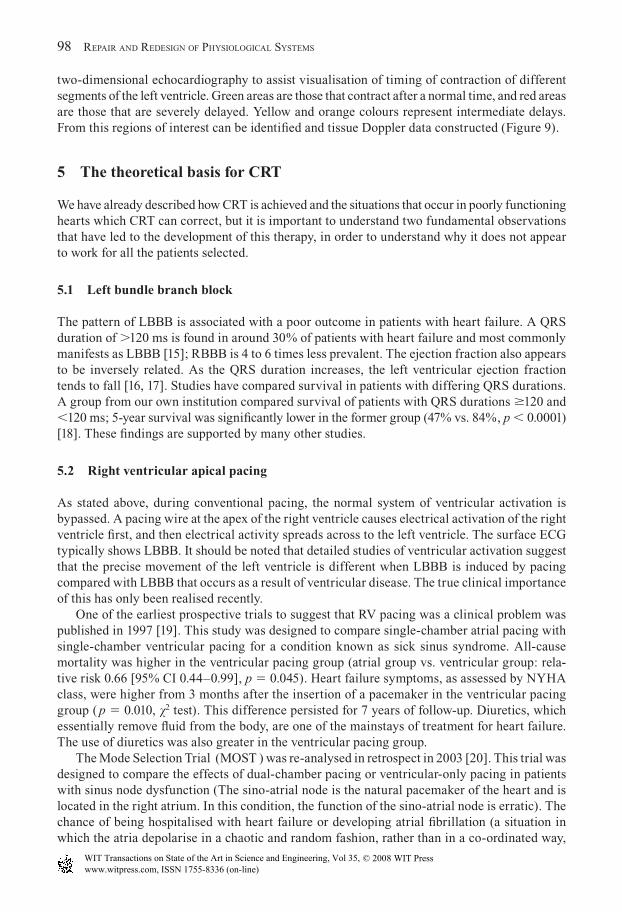
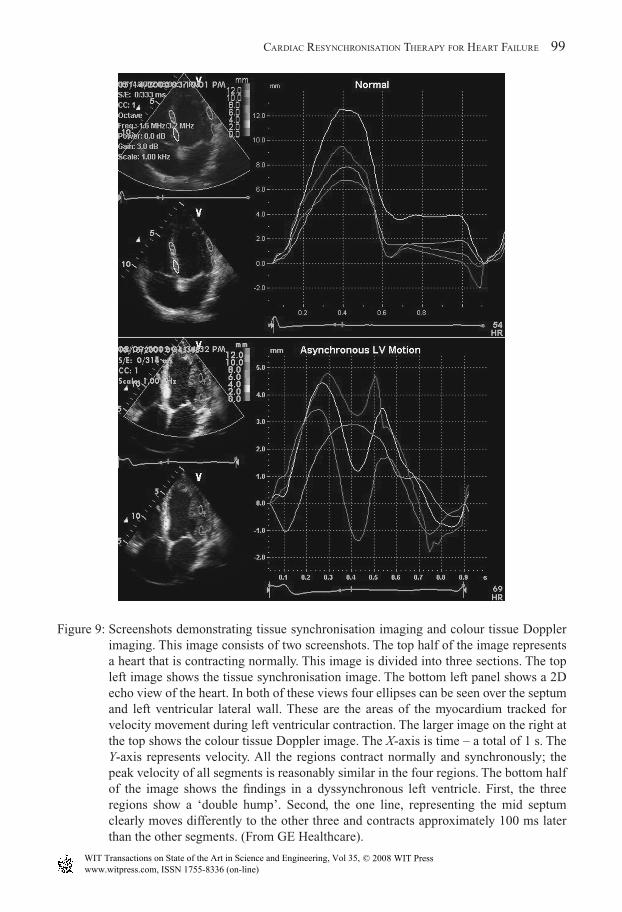
two-dimensional echocardiography to assist visualisation of timing of contraction of different segments of the left ventricle. Green areas are those that contract after a normal time, and red areas are those that are severely delayed. Yellow and orange colours represent intermediate delays. From this regions of interest can be identifi ed and tissue Doppler data constructed (Figure 9).
5 The theoretical basis for CRT
We have already described how CRT is achieved and the situations that occur in poorly functioning hearts which CRT can correct, but it is important to understand two fundamental observations that have led to the development of this therapy, in order to understand why it does not appear to work for all the patients selected.
5.1 Left bundle branch block
The pattern of LBBB is associated with a poor outcome in patients with heart failure. A QRS duration of �120 ms is found in around 30% of patients with heart failure and most commonly manifests as LBBB [15]; RBBB is 4 to 6 times less prevalent. The ejection fraction also appears to be inversely related. As the QRS duration increases, the left ventricular ejection fraction tends to fall [16, 17]. Studies have compared survival in patients with differing QRS durations. A group from our own institution compared survival of patients with QRS durations �120 and �120 ms; 5-year survival was signifi cantly lower in the former group (47% vs. 84%, p � 0.0001) [18]. These fi ndings are supported by many other studies.
5.2 Right ventricular apical pacing
As stated above, during conventional pacing, the normal system of ventricular activation is bypassed. A pacing wire at the apex of the right ventricle causes electrical activation of the right ventricle fi rst, and then electrical activity spreads across to the left ventricle. The surface ECG typically shows LBBB. It should be noted that detailed studies of ventricular activation suggest that the precise movement of the left ventricle is different when LBBB is induced by pacing compared with LBBB that occurs as a result of ventricular disease. The true clinical importance of this has only been realised recently.
One of the earliest prospective trials to suggest that RV pacing was a clinical problem was published in 1997 [19]. This study was designed to compare single-chamber atrial pacing with single-chamber ventricular pacing for a condition known as sick sinus syndrome. All-cause mortality was higher in the ventricular pacing group (atrial group vs. ventricular group: rela-tive risk 0.66 [95% CI 0.44–0.99], p � 0.045). Heart failure symptoms, as assessed by NYHA class, were higher from 3 months after the insertion of a pacemaker in the ventricular pacing group ( p � 0.010, �2 test). This difference persisted for 7 years of follow-up. Diuretics, which essentially remove fl uid from the body, are one of the mainstays of treatment for heart failure. The use of diuretics was also greater in the ventricular pacing group.
The Mode Selection Trial (MOST ) was re-analysed in retrospect in 2003 [20]. This trial was designed to compare the effects of dual-chamber pacing or ventricular-only pacing in patients with sinus node dysfunction (The sino-atrial node is the natural pacemaker of the heart and is located in the right atrium. In this condition, the function of the sino-atrial node is erratic). The chance of being hospitalised with heart failure or developing atrial fi brillation (a situation in which the atria depolarise in a chaotic and random fashion, rather than in a co-ordinated way,
WITPress_RRPS_ch005.indd 98WITPress_RRPS_ch005.indd 98 4/29/2008 4:43:23 PM4/29/2008 4:43:23 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
CARDIAC RESYNCHRONISATION THERAPY FOR HEART FAILURE 99
Figure 9: Screenshots demonstrating tissue synchronisation imaging and colour tissue Doppler imaging. This image consists of two screenshots. The top half of the image represents a heart that is contracting normally. This image is divided into three sections. The top left image shows the tissue synchronisation image. The bottom left panel shows a 2D echo view of the heart. In both of these views four ellipses can be seen over the septum and left ventricular lateral wall. These are the areas of the myocardium tracked for velocity movement during left ventricular contraction. The larger image on the right at the top shows the colour tissue Doppler image. The X-axis is time – a total of 1 s. The Y-axis represents velocity. All the regions contract normally and synchronously; the peak velocity of all segments is reasonably similar in the four regions. The bottom half of the image shows the fi ndings in a dyssynchronous left ventricle. First, the three regions show a ‘double hump’. Second, the one line, representing the mid septum clearly moves differently to the other three and contracts approximately 100 ms later than the other segments. (From GE Healthcare).
WITPress_RRPS_ch005.indd 99WITPress_RRPS_ch005.indd 99 4/29/2008 4:43:23 PM4/29/2008 4:43:23 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
100 REPAIR AND REDESIGN OF PHYSIOLOGICAL SYSTEMS
often leading to a rapid and irregular heart rate) was directly related to the proportion of time the right ventricle was paced. For patients who were paced more than 80% of the time, com-pared with the remainder, the relative risk of hospitalisation with heart failure was 3.6 (95% CI 1.93–6.70, p � 0.0001).
The Dual-Chamber and VVI Implantable Defi brillator (DAVID) trial was set up to prove that in the context of an implantable defi brillator (ICD), regular pacing of the atria and ventricle at a rate of 70 beats/min would be more benefi cial than simple back-up pacing if the heart rate dropped to below 40 beats/min. An ICD is a pacing device that can deliver a shock to the heart in the event of an abnormal ventricular rhythm such as ventricular tachycardia or fi brillation. The study was terminated early due to an excess of deaths and hospitalisations for heart failure in the regular pacing group [21].
In the Multicenter Automatic Defi brillator Implantation Trial II (MADIT II) single- and dual-chamber ICDs were implanted. The patients with defi brillators lived longer, but had higher rates of heart failure admissions. One hypothesis is that unnecessary RV pacing led to worsen-ing ventricular function [22].
In summary, when the activation of the ventricle is not as it should be, either because of intrinsic disease in the conducting system or because of right ventricular apical pacing, then the chances of heart failure developing or worsening are higher. It was this concept that led to the development of cardiac resynchronisation, the principle of which is to change the pattern of ventricular activation by pacing the left ventricle and the right ventricle almost simultaneously, and in particular to cause early activation of the basal segments of the lateral left ventricular wall. These are the areas of the myocardium that need to be activated in patients with LBBB. Logically, the presence of a broad QRS complex was used as a selection criterion. The fi rst stud-ies suggesting that this was a viable approach were published in 1994 [23, 24].
6 The evidence for dual-chamber pacemakers and CRT in heart failure
6.1 Dual-chamber pacing
In more advanced cases of CHF many patients have signifi cant mitral regurgitation, due to left ventricular dilatation stretching the supporting tissues. The mitral valve separates the left atrium from the left ventricle. Regurgitation of this valve permits blood to fl ow back towards the lungs rather than onwards through the aorta and around the body. Blood often fl ows back into the atrium before it escapes through the aortic valve during systole; this is termed presystolic mitral regurgitation. The movement of blood from the left atrium to the left ventricle in the period of diastole may also be abnormal. As the left ventricle fails and becomes stiffer, the pres-sures in it at the end of diastole rise.
Both presystolic mitral regurgitation and fi lling abnormalities can be corrected by dual chamber (and hence CRT), at least at rest, by shortening the AV delay. In the early 1990s signifi -cant improvements in NYHA class and increases in blood pressure were noted [25]. However, subsequent trials failed to confi rm these fi ndings [26, 27].
The reason why dual-chamber pacing is unlikely to benefi t most patients is twofold. First, as has already been argued above, apical right ventricular pacing can worsen cardiac function. Second, the optimal AV delay varies with different heart rates and between individuals [28]. We do not yet have the technology to optimise the AV delay for all individuals in all circumstances. Thus dual-chamber pacing is not recommended for patients with heart failure in the absence of a conventional indication for pacing. Furthermore in the context of biventricular pacing,
WITPress_RRPS_ch005.indd 100WITPress_RRPS_ch005.indd 100 4/29/2008 4:43:23 PM4/29/2008 4:43:23 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
CARDIAC RESYNCHRONISATION THERAPY FOR HEART FAILURE 101
optimising the AV delay remains diffi cult, and may be of limited relevance, unless it is mark-edly prolonged [29]. Evidence that optimising the AV delay in the context of CRT is benefi cial is lacking at present.
6.2 CRT
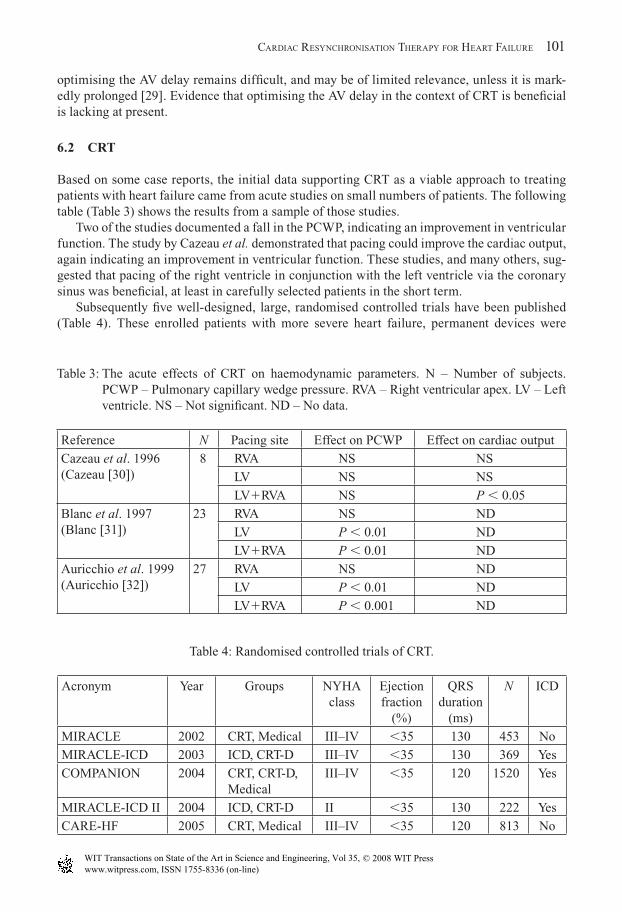
Based on some case reports, the initial data supporting CRT as a viable approach to treating patients with heart failure came from acute studies on small numbers of patients. The following table (Table 3) shows the results from a sample of those studies.
Two of the studies documented a fall in the PCWP, indicating an improvement in ventricular function. The study by Cazeau et al. demonstrated that pacing could improve the cardiac output, again indicating an improvement in ventricular function. These studies, and many others, sug-gested that pacing of the right ventricle in conjunction with the left ventricle via the coronary sinus was benefi cial, at least in carefully selected patients in the short term.
Subsequently fi ve well-designed, large, randomised controlled trials have been published (Table 4). These enrolled patients with more severe heart failure, permanent devices were
Table 3: The acute effects of CRT on haemodynamic parameters. N – Number of subjects. PCWP – Pulmonary capillary wedge pressure. RVA – Right ventricular apex. LV – Left ventricle. NS – Not signifi cant. ND – No data.
Reference N Pacing site Effect on PCWP Effect on cardiac output
Cazeau et al. 1996(Cazeau [30])
8 RVA NS NS
LV NS NS
LV�RVA NS P � 0.05
Blanc et al. 1997(Blanc [31])
23 RVA NS ND
LV P � 0.01 ND
LV�RVA P � 0.01 ND
Auricchio et al. 1999(Auricchio [32])
27 RVA NS ND
LV P � 0.01 ND
LV�RVA P � 0.001 ND
Table 4: Randomised controlled trials of CRT.
Acronym Year Groups NYHA class
Ejection fraction
(%)
QRS duration
(ms)
N ICD
MIRACLE 2002 CRT, Medical III–IV �35 130 453 No
MIRACLE-ICD 2003 ICD, CRT-D III–IV �35 130 369 Yes
COMPANION 2004 CRT, CRT-D, Medical
III–IV �35 120 1520 Yes
MIRACLE-ICD II 2004 ICD, CRT-D II �35 130 222 Yes
CARE-HF 2005 CRT, Medical III–IV �35 120 813 No
WITPress_RRPS_ch005.indd 101WITPress_RRPS_ch005.indd 101 4/29/2008 4:43:23 PM4/29/2008 4:43:23 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
102 REPAIR AND REDESIGN OF PHYSIOLOGICAL SYSTEMS
implanted, and follow-up over at least 6 months was performed. Importantly, the criteria for selecting patients have been symptoms, ejection fraction and a broad QRS complex. In total over 3000 patients with heart failure have been studied in these trials. Of note, all patients in these trials were in normal sinus rhythm and on optimal medical therapy.
6.2.1 MIRACLEThe Multicenter Insync RAndomized CLinical Evaluation (MIRACLE) was the fi rst randomised controlled trial to be published, in 2002 [33]. In addition to the entry criteria above, patients were required to have evidence of a dilated left ventricle (end-diastolic dimension �55 mm) and objective evidence of impaired exercise tolerance with a 6 min walk distance of �450 m. Four hundred and fi fty-three patients were successfully entered into the study and followed up for 6 months. Two hundred and twenty-fi ve patients were randomly assigned to the control group, and the remainder received a CRT device. There were signifi cant improvements in 6-min walk distance, quality of life and NYHA class, as well as in other measures. Seventy-nine per cent of patients who received a device reported an improvement in their state over the study period. There was no signifi cant reduction in death rate.
6.2.2 MIRACLE-ICDIt is now common to implant devices that have the ability to both resynchronise and defi brillate (CRT-D). This trial was the fi rst large-scale trial to evaluate these devices [34]. All 369 patients had a CRT-D device inserted, but only 187 had the CRT function activated. The remainder served as controls, with only the defi brillator active. Compared with the control group there was a signifi cant improvement in quality of life, NYHA class and peak oxygen consumption. There was no difference in survival between the groups; however, the study was not adequately powered to detect such a difference.
6.2.3 MIRACLE-ICD IIThis study enrolled a slightly different group of patients [35]. Whereas in the other trials dis-cussed here the patients had severe symptoms of heart failure, the patients enrolled into this trial were less unwell and in NYHA class II. One hundred and ninety-one had successful implan-tation of devices. There were signifi cant improvements in cardiac function and structure as assessed by echocardiography, as well as in NYHA class. There was no major change in peak V.o2 or 6-min walk test. Larger studies are being performed in patients with less severe heart
failure to determine whether, over a longer time period, these patients benefi t from CRT.
6.2.4 COMPANIONThe COMPANION trial, published in 2004, was also an important study [36], and one of the largest to date, enrolling 1520 patients with heart failure. Three hundred and eight received optimal medical therapy alone, 617 received CRT and 595 received CRT with an additional defi brillator function (CRT-D). Enrolment criteria were NYHA class III–IV heart failure, an ejection fraction of �35% and a QRS duration of �120 ms. Death was a secondary endpoint in this study. CRT alone reduced the risk of death (hazard ratio 0.76; 95% CI 0.58–1.01, p � 0.059), CRT-D reduced the risk of death signifi cantly (hazard ratio 0.64; 95% CI 0.48–0.86, p � 0.003). In addition, in both pacemaker groups quality of life improved, as did NYHA class compared with optimal medical therapy alone.
6.2.5 CARE-HFThe CARE-HF study was presented in 2005 [37]. Eight hundred and thirteen patients with NYHA class III–IV heart failure were enrolled and followed up for an average of 29.4 months.
WITPress_RRPS_ch005.indd 102WITPress_RRPS_ch005.indd 102 4/29/2008 4:43:24 PM4/29/2008 4:43:24 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
CARDIAC RESYNCHRONISATION THERAPY FOR HEART FAILURE 103
Patients were in normal sinus rhythm, the ejection fraction had to be less than 35% and the QRS duration had to be more than 120 ms. If it was between 120 and 149 ms then, in addition, there had to be echocardiographic evidence that the contraction of the LV was dyssynchronous. All patients were on optimal medical therapy. This was the fi rst trial to conclusively demon-strate that CRT could reduce the risk of death in these patients, and its importance cannot be understated. The hazard ratio for death for patients treated with CRT compared to those treated with medication alone was 0.64 (95% CI 0.48–0.85, p � 0.002). In addition, quality of life improved – the NYHA class was 2.1 � 1.0 in the CRT group vs. 2.7 � 0.9 in the medication group (p � 0.001), and the Minnesota Living with Heart Failure score was 31� 22 vs. 40 � 22 (p � 0.001).
The evidence base behind CRT is now robust. They are recommended in patients with NYHA class III–IV heart failure and a broad QRS complex by both the American and the European 2005 heart failure guidelines.
‘Resynchronisation therapy using bi-ventricular pacing can be considered in patients with reduced ejection fraction and ventricular dyssynchrony (QRS width �120 ms), who remain symptomatic (NYHA III-IV) despite optimal medical therapy to improve symptoms…hospi-talizations….and mortality.’
Guidelines for the diagnosis and treatment of chronic heart failure, European Society of Cardiology, 2005.
‘There is strong evidence to support the use of CRT to improve symptoms, exercise capacity, quality of life, LVEF and survival and to decrease hospitalizations in patients with persist-ently symptomatic HF undergoing optimal medical therapy who have cardiac dyssynchrony (As evidenced by a prolonged QRS duration).’
Guideline update for the diagnosis and management of chronic heart failure in the adult, American Heart Association/American College of Cardiology, 2005.
An increasing number of devices are being implanted in the UK. Indeed, some cardiolo-gists in training are now being trained solely to manage heart failure patients and implant these devices. But things are not so simple. These devices are expensive, an issue of great importance in today’s world – a CRT device with defi brillator costs over £15000 in the UK, excluding the costs of care. It must be remembered that inserting these devices has its own risks. The procedure itself requires admission to hospital, at least overnight, and is uncomfortable. The patient is not able to use the arm on the side of the implant normally for approximately 6 weeks until healing takes place. There are also a number of other potential complications related to the procedure, including pneumothorax, lead displacement, infection, perforation of the heart/coronary sinus and death. A recent meta-analysis suggested a death rate of 0.4% [38].
Importantly, a signifi cant number of patients (around 30%) do not derive any clinical benefi t from resynchronisation using symptoms, ejection fraction and a broad QRS complex as selec-tion criteria [6, 33]. This exposes a large number of patients to harm and wastes resources. Hence, we cannot be satisfi ed with these criteria as the only markers for patients who may benefi t from CRT.
One proposed way forward is to look directly for evidence of dyssynchrony, using the echocardiographic techniques described above, in an attempt to identify who will benefi t from so-called resynchronisation therapy. It has become clear from studies that LBBB is not an invariant marker of dyssynchrony [39], and many patients with a normal QRS duration have uncoordinated left ventricular contraction and may benefi t from CRT [40].
WITPress_RRPS_ch005.indd 103WITPress_RRPS_ch005.indd 103 4/29/2008 4:43:24 PM4/29/2008 4:43:24 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
104 REPAIR AND REDESIGN OF PHYSIOLOGICAL SYSTEMS
7 Echocardiographic measures of dyssynchrony and response to CRT
7.1 Interventricular dyssynchrony
It was initially thought that one method by which CRT worked was the correction of interven-tricular dyssynchrony. Indeed, there is a good relationship between interventricular dyssyn-chrony and the QRS duration [41]. A number of studies have now suggested that measures of interventricular dyssynchrony do not predict benefi t from CRT, especially for patients with CHF [11, 42, 43].
7.2 Intraventricular dyssynchrony
M-mode echo has not been found to be sensitive or specifi c in determining which patients respond to CRT [44]. For 2D echo measures, the situation is arguably worse; there are no data currently available on the effectiveness of these approaches in determining long-term outcome. There has, however, been a lot of interest in tissue Doppler measures.
Using TDI a delay of greater than 60 ms in the septal to lateral peak systolic velocity has been shown to predict an acute response to CRT [11; other studies, using more complicated models, have shown promising results, with a high sensitivity and specifi city [45]. Two studies using TSI have suggested sensitivities of 87% and specifi cities of 81 and 100% [12, 13] in predict-ing response to CRT. These techniques offer great promise in improving patient selection.
Other methodologies which require further investigation include strain and strain rate imaging [46], speckle tracking of radial strain [47], displacement mapping [48] and three-dimensional echo [49]. There is no doubt that there will be continuous refi nement of echocardiographic technology and signal processing to assist patient selection for CRT.
8 Other reasons for non-response
It is suggested that selecting a patient on ECG criteria alone is probably inadequate and newer echocardiographic techniques, which assess intraventricular dyssynchrony in particular, may improve our ability to identify patients who will benefi t from CRT.
Studies using ‘non-contact mapping’ allow detailed understanding of the precise patterns of electrical activation of the heart. This technique has already shown us that the ECG is not always a reliable indicator of left ventricular activation, underscoring that it is probably not the best method of selecting patients for CRT. It is reasonable to assume that the position of the left ventricular lead in relation to the pattern of ventricular activation is important in determining the overall success of CRT, and that a poorly placed lead may worsen the situation. Certainly some [50, 51], but not all, studies have suggested this. Lambiase et al. [52], using non-contact mapping, found that when the coronary sinus lead was placed in an area where there was slow conduction, patients did not respond to CRT [52].
The precise coronary venous anatomy varies from patient to patient around a basic template [4]. Therefore, it may not be feasible to implant a lead in a desirable location. In addition, lead instability, no electrical capture of the myocardium or concurrent stimulation of other struc-tures, in particular the diaphragm, which is often intolerable, may prevent suitable positioning of the left ventricular lead. There is requirement of better lead technology or a need to accept that the epicardial route is the best method for some patients. It may be possible to visualise suitable cardiac veins pre-operatively using CT scanning [53], permitting improved selection of patients who are likely to have a successful transvenous implant.
WITPress_RRPS_ch005.indd 104WITPress_RRPS_ch005.indd 104 4/29/2008 4:43:24 PM4/29/2008 4:43:24 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
CARDIAC RESYNCHRONISATION THERAPY FOR HEART FAILURE 105
At present a pragmatic approach has to be adopted – an attempt is made transvenously, and if any suitable position can be obtained, preferably laterally, then that position is accepted. If no suitable vein can be found then the possibility of epicardial lead placement remains.
9 Conclusions
That cardiac resynchronisation therapy can benefi t many patients with heart failure is now uncontested by most. However, there is still much debate as to which patients actually benefi t. In addition to those who meet the classic criteria, whether this therapy can help a large number of patients with less severe heart failure, a narrow QRS complex, right bundle branch block or atrial fi brillation remains to be determined. It is a technology like so many others in medicine – applied before we understand how it works, who benefi ts and who it harms. This is perhaps an interesting, and not necessarily fl attering refl ection of doctors.
A time can be foreseen when a more precise anatomical and functional pre-operative assessment of patients, using a combination of approaches such as echocardiography and CT scanning, will allow us to be more confi dent as to which patients should be selected for CRT. In particular tissue Doppler assessment of intraventricular dyssynchrony appears promising.
Guidelines have been published at present by highly infl uential organisations, based on the best evidence that we have today. The irony of these is that we know many will not benefi t, and many who may benefi t will be denied therapy. There are an increasing number of clini-cians who are prepared to offer any patient with severe symptoms secondary to heart failure a CRT device, and when faced with a desperate patient it is hard to deny them a chance. However, it must never be forgotten that there are fi nite resources, and that all procedures carry the risk of harm.
References
[1] Mosterd, A., Hoes, A.W. & de Bruyne, M.C., Prevalence of heart failure and left ven-tricular dysfunction in the general population. European Heart Journal, 20, pp. 447–455, 1999.
[2] McMurray, J.J. & Stewart, S., Epidemiology, aetiology, and prognosis of heart failure. Heart, 83, pp. 596–602, 2000.
[3] MacIntyre, K., Capewell, S. & Stewart, S., Evidence of improving prognosis in heart failure: trends in case fatality in 66547 patients hospitalized between 1986 and 1995. Circulation, 102, pp. 1126–1131, 2000.
[4] Singh, J.P., Houser, S., Heist, E.K. & Ruskin, J.N., The coronary venous anatomy: a segmental approach to aid cardiac resynchronization therapy. Journal of the American College of Cardiology, 46, pp. 68–74, 2005.
[5] Bax, J.J., Ansalone, G., Breithardt, O.A., Derumeaux, G., Leclercq, C., Schalij, M.J., Sogaard, P., St John Sutton, M. & Nihoyannopoulos, P., Echocardiographic evaluation of cardiac resynchronization therapy: ready for routine clinical use? A critical appraisal. Journal of the American College of Cardiology, 44, pp. 1–9, 2004.
[6] Pitzalis, M.V., Iacoviello, M., Romito, R., Massari, F., Rizzon, B., Luzzi, G., Guida, P., Andriani, A., Mastropasqua, F. & Rizzon, P., Cardiac resynchronization therapy tailored by echocardiographic evaluation of ventricular asynchrony. Journal of the American College of Cardiology, 40, pp. 1615–1622, 2002.
WITPress_RRPS_ch005.indd 105WITPress_RRPS_ch005.indd 105 4/29/2008 4:43:24 PM4/29/2008 4:43:24 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
106 REPAIR AND REDESIGN OF PHYSIOLOGICAL SYSTEMS
[7] Breithardt, O.A., Stellbrink, C., Kramer, A.P., Sinha, A.M., Franke, A., Salo, R., Schiffgens, B., Huvelle, E. & Auricchio, A., Pacing Therapies for Congestive Heart Failure (PATH-CHF) Study group, Echocardiographic quantifi cation of left ventricular asynchrony predicts an acute hemodynamic benefi t of cardiac resynchronization therapy. Journal of the American College of Cardio logy, 40, pp. 536–545, 2002.
[8] Ansalone, G., Giannantoni, P., Ricci, R., Trambaiolo, P., Laurenti, A., Fedele, F. & Santini, M., Doppler myocardial imaging in patients with heart failure receiving biventricular pacing treatment. American Heart Journal, 142, pp. 881–896, 2001.
[9] Garrigue, S., Reuter, S., Labeque, J.N., Jais, P., Hocini, M., Shah, D.C., Haissaguerre, M. & Clementy, J., Usefulness of biventricular pacing in patients with congestive heart fail-ure and right bundle branch block. American Journal of Cardiology, 88, pp. 1436–1441, 2001.
[10] Yu, C.M., Chau, E., Sanderson, J.E., Fan, K., Tang, M.O., Fung, W.H., Lin, H., Kong, S.L.,Lam, Y.M., Hill, M.R. & Lau, C.P., Tissue Doppler echocardiographic evidence of reverse remodeling and improved synchronicity by simultaneously delaying regional con-traction after biventricular pacing therapy in heart failure. Circulation, 105, pp. 438–445, 2002.
[11] Bax, J.J., Marwick, T.H., Molhoek, S.G., Bleeker, G.B., van Erven, L., Boersma, E., Steendijk, P., van der Wall, E.E. & Schalij, M.J., Left ventricular dyssynchrony predicts benefi t of cardiac resynchronization therapy in patients with end-stage heart failure before pacemaker implantation. American Journal of Cardiology, 92, pp. 1238–1240, 2004.
[12] Gorcsan, J., 3rd, Kanzaki, H., Bazaz, R., Dohi, K. & Schwartzman, D., Usefulness of echocardiographic tissue synchronization imaging to predict acute response to car-diac resynchronization therapy. American Journal of Cardiology, 93, pp. 1178–1181, 2004.
[13] Yu, C.M., Zhang, Q., Fung, J.W., Chan, H.C., Chan, Y.S., Yip, G.W., Kong, S.L., Lin, H., Zhang, Y. & Sanderson, J.E., A novel tool to assess systolic asynchrony and identify responders of cardiac resynchronization therapy by tissue synchronization imaging. Journal of the American College of Cardiology, 45, pp. 677–684, 2005.
[14] Kawaguchi, M., Murabayashi, T., Fetics, B.J., Nelson, G.S., Samejima, H., Nevo, E. & Kass, D.A., Quantitation of basal dyssynchrony and acute resynchronization from left or biventricular pacing by novel echo-contrast variability imaging. Journal of the American College of Cardiology, 39, pp. 2052–2058, 2002.
[15] Kashani, A. & Barold, S.S., Signifi cance of QRS complex duration in patients with heart failure. Journal of the American College of Cardiology, 46, pp. 2183–2192, 2005.
[16] Shenkman, H.J., Pampati, V. & Khandelwal, A.K., Congestive heart failure and QRS duration: establishing prognosis study. Chest, 122, pp. 528–534, 2002.
[17] Sandhu, R. & Bahler, R.C., Prevalence of QRS prolongation in a community hospital cohort of patients with heart failure and its relation to left ventricular systolic dysfunc-tion. American Journal of Cardiology, 93, pp. 244–246, 2004.
[18] Kalra, P.R., Sharma, R. & Shamim, W., Clinical characteristics and survival of patients with chronic heart failure and prolonged QRS duration. International Journal of Cardiology, 86, pp. 225–231, 2002.
[19] Anderson, H.R., Nielson, J.C., Thomsen, P.E.B., Mortensen, P.T., Vesterlund, T. & Pederson, A.K., Long-term follow-up of patients from a randomised trial of atrial versus ventricular pacing for sick-sinus syndrome. Lancet, 350, pp. 1210–1216, 1997.
[20] Sweeney, M., Hellkamp, A. & Ellenbogen, K., Adverse effect of ventricular pacing on heart failure and atrial fi brillation among patients with a normal baseline QRS duration
WITPress_RRPS_ch005.indd 106WITPress_RRPS_ch005.indd 106 4/29/2008 4:43:24 PM4/29/2008 4:43:24 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
CARDIAC RESYNCHRONISATION THERAPY FOR HEART FAILURE 107
in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation, 107, pp. 2932–2937, 2003.
[21] Sharma, A.D., Rizo-Patron, C. & Hallstrom, A.P., Percent right ventricular pacing predicts outcome in the DAVID Trial. Heart Rhythm, 2, pp. 830–834, 2005.
[22] Steinberg, J.S., Fischer, A. & Wang, P., The clinical implications of cumulative right ventricular pacing in the Multicenter Automatic Defi brillator Trial II. Journal of Cardio-vascular Electrophysiology, 16, pp. 359–365, 2005.
[23] Bakker, P.F., Meijburg, H., de Jonge, N., van Mechelen, R., Wittkamp, F., Mower, M. & Thomas, A., Benefi cial effects of biventricular pacing in congestive heart failure [abstract]. Pacing & Clinical Electrophysiology, 17, pp. 820, 1994.
[24] Cazeau, S., Ritter, P., Backdach, S., Lazarus, A., Limousin, M., Henao, L., Mundler, O., Daubert, J.C. & Mugica, J., Four chamber pacing in dilated cardiomyopathy. Pacing & Clinical Electrophysiology, 17 (Part 2), pp. 1974–1979, 1994.
[25] Hochleitner, M., Hortnagl, H., Ng, C.K., Zechmann, W. & Gschnitzer, F., Usefulness of physiological dual chamber pacing in drug resistant idiopathic dilated cardiomyopathy. American Journal of Cardiology, 25, pp. 281–288, 1990.
[26] Gold, M., Feliciano, Z., Gottlieb, S. & Fisher, M., Dual chamber pacing with a short atrioventricular delay in congestive heart failure: a randomised study. Journal of the American College of Cardiology, 26, pp. 967–973, 1995.
[27] Linde, C., Gadler, F., Edner, M., Nordlander, R. & Rosenqvist, R., Results of atrioven-tricular synchronous pacing with optimized delay in patients with severe congestive heart failure. American Journal of Cardiology, 75, pp. 919–923, 1995.
[28] Whinnett, Z.I., Davies, J.E., Wilson, K., Chow, A.W., Foale, R.A., Davies, D.W., Hughes, A.D., Francis, D.P. & Mayet, J., Determination of optimal atrioventricular delay for cardiac resynchronization therapy using acute non-invasive blood pressure. Europace, 8, pp. 358–366, 2006.
[29] Salukhe, T.V., Francis, D.P., Morgan, M., Clague, J.R., Sutton, R., Poole-Wilson, P. & Henein, M.Y., Mechanism of cardiac output gain from cardiac resynchronization therapy in patients with coronary artery disease or idiopathic dilated cardiomyopathy. American Journal of Cardiology, 97, pp. 1358–1364, 2006.
[30] Cazeau, S., Ritter, P., Lazarus, A., Gras, D., Backdach, H., Mundler, O. & Mugica, J., Multisite pacing for end-stage heart failure: early experience. Pacing & Clinical Electro-physiology, 19, pp. 1748–1757, 1996.
[31] Blanc, J.J., Etienne, Y., Gilard, M., Mansourati, J., Munier, S., Boschat, J., Benditt, D. G. & Lurie, K.G., Evaluation of different ventricular pacing sites in patients with severe heart failure: results of an acute haemodynamic study. Circulation, 96, pp. 3272–3277, 1997.
[32] Auricchio, A., Stellbrink, C., Block, M., Sack, S., Vogt, J., Bakker, P., Klein, H., Kramer, A., Ding, J., Salo, R., Tockman, B., Pochet, T. & Spinelli, J., Effect of pacing chamber and atrioventricular delay on acute systolic function of paced patients with congestive heart failure. The Pacing Therapies for Congestive Heart Failure Study Group. The Guidant Congestive Heart Failure Research Group. Circulation, 99, pp. 2993–3001, 1999.
[33] Abraham, W.T., Fisher, W.G., Smith, A.L., Delurgio, D.B., Leon, A.R., Loh, E., Kocovic, D.Z., Packer, M., Clavell, A.L., Hayes, D.L., Ellestad, M., Trupp, R.J., Underwood, J., Pickering, F., Truex, C., McAtee, P. & Messenger, J., Cardiac resynchronization in chronic heart failure. New England Journal of Medicine, 346, pp. 1845–1853, 2002.
[34] Young, J.B., Abraham, W.T., Smith, A.L., Leon, A.R., Lieberman, R., Wilkoff, B., Canby, R.C., Schroeder, J.S., Liem, L.B., Hall, S. & Wheelan, K., Combined cardiac
WITPress_RRPS_ch005.indd 107WITPress_RRPS_ch005.indd 107 4/29/2008 4:43:24 PM4/29/2008 4:43:24 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
108 REPAIR AND REDESIGN OF PHYSIOLOGICAL SYSTEMS
resynchronization and implantable cardioversion defi brillation in advanced chronic heart failure: the MIRACLE ICD Trial [see comment]. Journal of American Medical Associa-tion, 289, pp. 2685–2694, 2003.
[35] Abraham, W.T., Young, J.B., Leon, A.R., Adler, S., Bank, A.J., Hall, S.A., Lieberman, R., Liem, L.B., O’Connell, J.B., Schroeder, J.S. & Wheelan, K.R., Effects of cardiac resyn-chronization on disease progression in patients with left ventricular systolic dysfunc-tion, an indication for an implantable cardioverter-defi brillator, and mildly symptomatic chronic heart failure. Circulation, 110, pp. 2864–2868, 2004.
[36] Bristow, M.R., Saxon, L.A., Boehmer, J., Krueger, S., Kass, D.A., De Marco, T., Carson, P., DiCarlo, L., DeMets, D., White, B.G., DeVries, D.W. & Feldman, A.M., Cardiac-resynchronization therapy with or without an implantable defi brillator in advanced chronic heart failure [see comment]. New England Journal of Medicine, 350, pp. 2140–2150, 2004.
[37] Cleland, J.G., Daubert, J.C., Erdmann, E., Freemantle, N., Gras, D., Kappenberger, L. & Tavazzi, L., The effect of cardiac resynchronization on morbidity and mortality in heart failure. New England Journal of Medicine, 352, pp. 1539–1549, 2005.
[38] McAlister, F., Ezekowitz, J., Wiebe, N., Rowe, B., Spooner, C., Crumley, E., Hartling, L., Kaul, P., Nichol, G. & Klassen, T., Cardiac resynchronization therapy for congestive heart failure. Evidence Report: Technology Assessment, 106, pp. 1–8, 2004.
[39] Fung, J.W., Yu, C.M., Yip, G., Zhang, Y., Chan, H., Kum, C.C. & Sanderson, J.E., Variable left ventricular activation pattern in patients with heart failure and left bundle branch block. Heart, 90, pp. 17–19, 2004.
[40] Yu, C.M., Lin, H., Zhang, Q. & Sanderson, J.E., High prevalence of left ventricular systolic and diastolic asynchrony in patients with congestive heart failure and normal QRS dura-tion. Heart, 89, pp. 54–60, 2003.
[41] Rouleau, F., Merheb, M., Geffroy, S., Berthelot, J., Chaleil, D., Dupuis, J.M., Victor, J. & Geslin, P., Echocardiographic assessment of the interventricular delay of activation and correlation to the QRS width in dilated cardiomyopathy. Pacing & Clinical Electrophysio-logy, 24, pp. 1500–1506, 2001.
[42] Bordachar, P., Lafi tte, S., Reuter, S., Sanders, P., Jais, P., Haissaguerre, M., Roudaut, R., Garrigue, S. & Clementy, J., Echocardiographic parameters of ventricular dyssynchrony validation in patients with heart failure using sequential biventricular pacing. Journal of the American College of Cardiology, 44, pp. 2157–2165, 2004.
[43] Boriani, G., Muller, C.P., Seidl, K.H., Grove, R., Vogt, J., Danschel, W., Schuchert, A., Djiane, P., Biffi , M., Becker, T., Bailleul, C. & Trappe, H.J., Randomized comparison of simultaneous biventricular stimulation versus optimized interventricular delay in cardiac resynchronization therapy. The Resynchronization of the HaemodYnamic Treatment for Heart failure Management II Implantable Cardioverter Defi brillator (RHYTHM II ICD) study. American Heart Journal, 15, pp. 1057–1065, 2006.
[44] Marcus, G.M., Rose, E., Viloria, E.M., Schafer, J., De Marco, T., Saxon, L.A., Foster, E. & VENTAK CHF/CONTAK-CD Biventricular Pacing Study Investigators, Septal to pos-terior wall motion delay fails to predict reverse remodeling or clinical improvement in patients undergoing cardiac resynchronization therapy. Journal of the American College of Cardiology, 46, pp. 2208–2214, 2005.
[45] Bax, J.J., Abraham, T., Barold, S.S., Breithardt, O.A., Fung, J.W., Garrigue, S., Gorcsan, J., 3rd, Hayes, D.L., Kass, D.A., Knuuti, J., Leclercq, C., Linde, C., Mark, D.B., Monaghan, M.J., Nihoyannopoulos, P., Schalij, M.J., Stellbrink, C. & Yu, C.M., Cardiac
WITPress_RRPS_ch005.indd 108WITPress_RRPS_ch005.indd 108 4/29/2008 4:43:24 PM4/29/2008 4:43:24 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press
CARDIAC RESYNCHRONISATION THERAPY FOR HEART FAILURE 109
resynchronization therapy: Part 1--issues before device implantation. Journal of the American College of Cardiology, 46, pp. 2153–2167, 2005.
[46] Breithardt, O.A., Stellbrink, C., Herbots, L., Claus, P., Sinha, A.M., Bijnens, B., Hanrath, P. & Sutherland, G.R., Cardiac resynchronization therapy can reverse abnormal myocardial strain distribution in patients with heart failure and left bundle branch block. Journal of the American College of Cardiology, 42, pp. 486–494, 2003.
[47] Suffoletto, M.S., Dohi, K., Cannesson, M., Saba, S. & Gorcsan, J., 3rd, Novel speckle-tracking radial strain from routine black-and-white echocardiographic images to quantify dyssynchrony and predict response to cardiac resynchronization therapy [see comment]. Circulation, 113, pp. 960–968, 2006.
[48] Sun, J.P., Chinchoy, E., Donal, E., Popovic, Z.B., Perlic, G., Asher, C.R., Greenberg, N.L., Grimm, R.A., Wilkoff, B.L. & Thomas, J.D., Evaluation of ventricular synchrony using novel Doppler echocardiographic indices in patients with heart failure receiving cardiac resynchronization therapy. Journal of the American Society of Echocardiography, 17, pp. 845–850, 2004.
[49] Zhang, Q., Yu, C.M., Fung, J.W., Zhang, Y., Chan, Y.S., Chan, H.C., Yip, G.W. & Sanderson, J.E., Assessment of the effect of cardiac resynchronization therapy on intra-ventricular mechanical synchronicity by regional volumetric changes. American Journal of Cardiology, 95, pp. 126–129, 2005.
[50] Butter, C., Auricchio, A., Stellbrink, C., Fleck, E., Ding, J., Yu, Y., Huvelle, E. & Spinelli, J., Effect of resynchronization therapy stimulation site on the systolic function of heart failure patients. Circulation, 104, pp. 3026–3029, 2001.
[51] Auricchio, A., Stellbrink, C., Sack, S., Block, M., Vogt, J., Bakker, P., Huth, C., Schondube, F., Wolfhard, U., Bocker, D., Krahnefeld, O. & Kirkels, H., Long-term clini-cal effect of hemodynamically optimized cardiac resynchronization therapy in patients with heart failure and ventricular conduction delay. Journal of the American College of Cardiology, 39, pp. 2026–2033, 2002.
[52] Lambiase, P.D., Rinaldi, A., Hauck, J., Mobb, M., Elliott, D., Mohammad, S., Gill, J.S. & Bucknall, C.A., Non-contact left ventricular endocardial mapping in cardiac resyn-chronisation therapy. Heart, 90, pp. 44–51, 2004.
[53] Jongbloed, M.R., Lamb, H.J., Bax, J.J., Schuijf, J.D., de Roos, A., van der Wall, E.E. & Schalij, M.J., Noninvasive visualization of the cardiac venous system using multislice computed tomography. Journal of the American College of Cardiology, 45, pp. 749–753, 2005.
WITPress_RRPS_ch005.indd 109WITPress_RRPS_ch005.indd 109 4/29/2008 4:43:25 PM4/29/2008 4:43:25 PM
www.witpress.com, ISSN 1755-8336 (on-line) WIT Transactions on State of the Art in Science and Engineering, Vol 35, © 2008 WIT Press