Embed Size (px)
Citation preview

CRASC
Ii(ouHdMHtaRmdacoertCopvH
NFRMDN
BpNafNMmoCRiibepN
fn
Tp
BWA
Twttstt
IRSN
BppigMdac(rwRatpspiawvmCifht
1697Abstracts
ARDIAC RESYNCHRONIZATION THERAPY IN PATIENTS WITHECURRENT HEART FAILURE AND INTERMITTENT LBBButhor Block Rehan Mahmud, Alawi A. Alsheikh-Ali,alem Alkaabi, Arshad Rasheed. Sheikh Khalifa Medicality, Abu Dhabi, United Arab Emirates
ntroduction: Indications for cardiac resynchronization therapy (CRT)nclude prolonged QRS duration (typically LBBB), advanced heart failureHF, NYHA III/IV), and severe left ventricular (LV) dysfunction. The rolef CRT in patients with intermittent LBBB associated with acute HF isnknown.ypothesis: CRT will prevent recurrent HF associated with intermittentevelopment of LBBB.ethods: Consecutive patients with multiple admissions for severe acuteF associated with development of LBBB are described. Optimal drug
herapy failed to prevent recurrent HF hospitalizations and LBBB did notppear to be rate related.esults: Nine patients (age range 48-56 yrs, 8 males) had recurrent ad-issions for acute HF and new LBBB. All patients had only moderate LV
ysfunction (ejection fraction 30 to 35%). In between HF hospitalizations,ll patients had narrow QRS durations (� 120 ms) and NYHA functionallass II. One patient died of flash pulmonary edema associated with newnset LBBB while being monitored. This was associated with severelectromechanical dyssynchrony by echocardiogram. The other 8 patientseceived CRT. During follow up for an average of 13 months, no hospi-alization for HF occurred.onclusion: In patients with intermittent LBBB and acute HF, but withtherwise narrow QRS durations in-between HF exacerbations, CRT mayrevent recurrent HF hospitalizations. The benefit may be related to pre-ention of electromechanical dyssynchrony, which may trigger or mediateF exacerbations. Cause of intermittent LBBB in these patients is unclear.
PPA GAIN-OF-FUNCTION MUTATION ASSOCIATED WITHAMILIAL ATRIAL FIBRILLATIONobert L. Abraham, MD, Tao Yang, MD, PhD,arcia Blair, MSc, Dan M. Roden, MD,awood Darbar, MD. Vanderbilt University Medical Center,ashville, TN
ackground: Studies have increasingly identified genetics as an importantredisposing factor for developing atrial fibrillation (AF). Mutations inPPA, encoding the circulating hormone atrial natriuretic peptide (ANP)
s well as other functional proteins, have recently been implicated inamilial AF. The mechanisms underlying AF susceptibility with mutantPPA however remain uncertain.ethods: Participants in the Vanderbilt AF database and a set of anony-ized controls were screened for NPPA mutations. We studied the effects
f bath-applied wild-type (WT) and a mutant NPPA protein product onHO cells transfected with KCNQ1 and KCNE1.esults and Conclusions: We identified a novel NPPA mutation, A117V,
n a Caucasian family with lone AF. No NPPA mutations were identifiedn the anonymized controls. The affected kindred included 6 family mem-ers who were heterozygous for the mutation and 2 family members witharly onset paroxysmal lone AF. The mutation propagates to a preproANProtein fragment identified as the kaliuretic hormone. Compared to WT
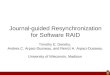
PPA fragment, the mutant A117V fragment generated a strong gain-of- punctional effect on cardiac IKs, with an IC50 of 0.6�0.1 nM vs. 3.7�0.6M for WT fragment (P�0.01) (Table).
he effects of Wt NPPA and mutant A117V fragments on cardiac IKs
roperties (10 nM, �SE, �20 mV, n�7 each)
ActivatingIKs (pA/pF)
IKs tail(pA/pF) V1/2 (mV)
T-activation
(ms) IC50 (nM)
aseline 31.6�6.9 17.5�3.4 28.5�3.2 1784�113 n/at fragment 63.1�10.4* 34.8�3.9* 13.6�2.7* 1106�85* 3.7�0.6*117V 99.7�10.7# 57.5�3.8# 1.4�0.6# 844�49# 0.6�0.1#
*p�0.01 vs. baseline, #p�0.01 vs. Wt fragment.
hus, we have identified a novel NPPA mutation in a Caucasian kindredith familial AF. Functional studies suggest that the protein product of
he mutation, kaliuretic hormone, may predispose to familial AFhrough enhanced and accelerated IKs activation, which is predicted tohorten the action potential duration. This supports evidence that mu-ations or rare variants in the NPPA gene pathway may each contributeo familial AF.
MPLANTABLE CARDIAC DEVICES IN THE ELDERLY-HOWISKY IS IT?enthil Thambidorai1; Manu Kaushik1; Aimin Chen1;azih Kadri1. 1Creighton University, Omaha, NE
ackground: Despite the efficacy of implantable cardiac devices in elderlyatients, a bias against their use seems to persist. A major concern aboutlacing these devices in elderly patients is the complication rate. Thencidence of complications in the elderly are not well recorded from theeneral population and most randomized trials excluded elderly patients.ethods: We retrospectively reviewed all consecutively implanted car-iac devices (pacemakers-PPM and internal cardioverter defibrillator-ICD)t Creighton University from January 2003 to December 2006. Clinicalharacteristics and echocardiography were recorded at baseline. All acute�1 month) and chronic complications (1 year) were obtained from charteview. Lead threshold and impedance data were recorded. Age � 75 yearsas used to discriminate the elderly group. Mean follow-up was 2.2 years.esults: There were a total of 673 patients with 395 PPM implantationsnd 278 ICD implantations. Overall there were no significant differences inhe overall complication rates based on age group (9.92% vs 11.25%;�ns). Further stratified analysis based on age by each decade revealed noignificant between all groups, even in patients �80 years of age (n�190atients, rate�10%). There were significantly higher risk of complicationsn ICD patients as opposed to PPM patients (12.95% vs 8.86%; p�0.04)nd were persistent in both the �75 and �75 years old age groups. Thereere no differences in the lead related malfunction in the 2 groups (4.25%s 5.0%; p�ns). Multivariate analysis revealed clinical risk factors to beost predictive of complications.onclusions: Age should not be taken into consideration for devicemplantations in the general population independent of other clinical riskactors. Irrespective of age, defibrillator implantations carry a significantlyigher risk of complications than pacemaker implantations. Our data seemso suggest no increased risk of lead related malfunction in the elderly
opulation.