Embed Size (px)
Citation preview

Cardiac Risk Factor Awareness and Managementin Patients With Systemic Lupus ErythematosusKAREN H. COSTENBADER,1 ELIZABETH WRIGHT,2 MATTHEW H. LIANG,1 AND
ELIZABETH W. KARLSON1
Objective. To assess awareness and management of traditional cardiac risk factors (CRFs) in patients with systemiclupus erythematosus (SLE) and physicians.Methods. SLE patients (n � 110) completed a questionnaire concerning CRFs. Medical records were reviewed blinded toquestionnaire results for the presence and management of 6 CRFs: hypertension, hypercholesterolemia, smoking, obesity,diabetes mellitus, and physical inactivity.Results. Subjects were predominantly female (97%), mean (�SD) age was 43.4 years (�11.8), mean SLE duration was15.3 years (�7.2), and 51% had >2 CRFs by self report. Twenty-three percent had never had their cholesterol levelschecked. Hypercholesterolemia was more frequently documented in the medical records than reported by the patient(33% versus 24%). Physical inactivity was more frequently self reported than documented (59% versus 23%). Rheuma-tologists and patients had low interrater reliability for the presence of hypercholesterolemia (� � 0.26) and physicalinactivity (� � –0.02). More than half (58%) of CRFs were treated, and 21% of subjects with elevated cholesterol receiveda medication.Conclusion. Recognition, recording, and management of CRFs falls short given the significance of the problem.
KEY WORDS. Systemic lupus erythematosus; Cardiac risk factor; Coronary artery disease; Compliance.
INTRODUCTION
The high morbidity and mortality due to premature coro-nary artery disease in patients with systemic lupus ery-thematosus (SLE) is now widely recognized (1–9). Womenwith SLE ages 35–44 years are �50 times more likely tohave a myocardial infarction than age-matched controlwomen in the Framingham Offspring Study (9). Noninva-sive techniques have also uncovered high rates of asymp-
tomatic coronary artery disease in the SLE population.Abnormal cardiac thallium perfusion scans are found innearly 39%; abnormal electrocardiograms in 16% of SLEpatients; and atherosclerosis is noted in the autopsy re-sults of 42–54% of SLE patients (10–14).
Known risk factors for cardiovascular disease—hyper-tension, hyperlipidemia, smoking, diabetes mellitus, obe-sity, and physical inactivity—are very prevalent in SLEpatients (15–20). Many researchers have called for aggres-sive monitoring and treatment of known cardiac risk fac-tors (CRFs) in patients with SLE (21–24). Studies fromBaltimore (15,16) and Toronto (25,26) suggest that in aca-demic centers SLE patients and their physicians tend notto be aware of the problem and that there is room forimprovement of traditional CRF management.
We administered a questionnaire concerning CRFs tooutpatients with SLE and performed a blinded review ofeach subject’s medical record. Our goals were to deter-mine the prevalence of CRFs in a group of patients withSLE treated at an academic medical center serving amainly white, mixed urban and suburban population; toassess the awareness and management of CRFs reportedby these SLE patients and their physicians; and finallyto examine the agreement between patient perceptionsand medical record documentation of CRFs in thesepatients.
Dr. Costenbader’s work supported by a Physician Scien-tist Development Award from the Arthritis Foundation andAmerican College of Rheumatology, and a grant from theArthritis National Research Foundation. Dr. Liang’s worksupported by NIH grant P60-AR-47782 and a KirklandScholar Award. Dr. Karlson’s work is supported by NIHgrants P01-AR-36308 and K08-AR-02074-0 and an ArthritisFoundation Arthritis Investigator Award.
1Karen H. Costenbader, MD, MPH, Matthew H. Liang, MD,MPH, Elizabeth W. Karlson, MD: Brigham and Women’sHospital, and Harvard Medical School, Boston, Massachu-setts; 2Elizabeth Wright, PhD: Brigham and Women’s Hos-pital, Boston, Massachusetts.
Address correspondence to Karen H. Costenbader, MD,MPH, Division of Rheumatology, Immunology and Allergy,Brigham and Women’s Hospital, 75 Francis Street, Boston,MA 02115. E-mail: [email protected].
Submitted for publication November 17, 2003; accepted inrevised form March 27, 2004.
Arthritis & Rheumatism (Arthritis Care & Research)Vol. 51, No. 6, December 15, 2004, pp 983–988DOI 10.1002/art.20824© 2004, American College of Rheumatology
ORIGINAL ARTICLE
983

PATIENTS AND METHODS
Patient recruitment. One hundred forty-three patientswith SLE treated at the Brigham and Women’s Hospitaloutpatient rheumatology clinic were identified for thisstudy based on their prior involvement in one or both of 2studies involving SLE patients performed by our researchgroup. Initial patient identification, enrollment, and base-line data collection have been described previously(27,28). In brief, all subjects met American College ofRheumatology criteria for the classification of SLE (diag-nosis confirmed by chart review) (29) and had active dis-ease (at least 2 outpatient visits to the rheumatology clinicin the year prior to enrollment).
Data collection. Baseline information was collected ondemographics, self efficacy, socioeconomic factors, in-cluding household income, type of health insurance, andeducation. Self efficacy was measured with the ArthritisSelf-Efficacy Scale, a valid and highly reliable instrumentthat measures a person’s sense of confidence in his or herability to control daily symptoms of SLE (30). As followupto the original studies performed in 1994–1998, 143 pa-tients were contacted and mailed a 19-item cardiovascularhealth questionnaire (CHQ) pertaining to their own cardio-vascular health and traditional cardiac risk factors: hyper-tension, smoking, obesity, high cholesterol, diabetes, andexercise patterns (See Appendix A available at the Arthri-tis Care & Research Web site at http://www.interscience.wiley.com/jpages/0004-3591:1/suppmat/index.html). TheCHQ is adapted from the National Health and NutritionExamination Survey I Epidemiologic Followup Study (31)and asks about knowledge of CRFs, whether a physicianhas advised a lifestyle or medication change, and whetherthey have followed this advice. Compliance on self reportwas based on subjects’ responses as to whether they hadfollowed their physicians’ advice.
One rheumatologist (KHC), blinded to the responses onthe CHQ, reviewed all available inpatient and outpatientmedical records for each patient for all of their providersfrom the time of SLE diagnosis to the time that the CHQwas returned. A standardized data form was used to col-
lect information that included whether modifiable CRFs—including smoking, obesity, blood pressure, fasting lipidprofile, fasting blood sugar, and physical inactivity—wereever noted by a physician in the time that the patient wastreated at the Robert B. Brigham Arthritis Center, andwhether, if abnormal, the patient was advised regardinglifestyle change (e.g., advised to quit smoking or to cutdown on salt in diet if hypertensive) or prescribed medi-cations. Compliance on medical record review was basedon long-term responses to health status and health behav-ior modifications.
Definitions of abnormal CRF status were taken from theliterature (see Table 1) (32–35). In addition, the long-termoutcomes of all attempts at risk factor modification werenoted. Cardiac events including angina, myocardial infarc-tion, congestive heart failure, sudden death, arrhythmia,transient ischemic attack, and stroke were recorded alongwith their management.
This study was approved by the Brigham and Women’sHospital Institutional Review Board.
Statistical analysis. We employed descriptive statisticsfor patient demographic factors, CRF knowledge, preva-lence, management, and compliance with management.Fisher’s exact tests were used for comparison of self reportto medical record review for CRF prevalence, manage-ment, and compliance. To compare the CHQ responders tononresponders, t-tests were used. Kappa statistics for in-terobserver reliability were used to compare CRF preva-lence in self reports with the medical records. Percentagreement was used to compare self report and medicalrecord data for CRF management and compliance with thatmanagement because the cell sizes for that data were small(35). Agreement between self report and medical recordwas defined as both CHQ and medical record review doc-umenting the presence or absence of a CRF, its manage-ment, or compliance with that management. Univariatemodels (Fisher’s exact tests and t-tests) and linear regres-sion analyses were used to test multiple potential predic-tors of agreement between self report and medical recorddata for CRF prevalence and for CRF management. All data
Table 1. Definitions of modifiable cardiac risk factors*
Cardiac risk factor definition Source (ref.)
Hypertension: BP � 140/90 mm Hg on � 2 occasions National High Blood PressureEducation Program (32)
Hypercholesterolemia (fasting, in mg/dl): Totalcholesterol � 240; LDL � 160; HDL � 35;triglycerides � 250
National Cholesterol EducationProgram (33)
Cigarette smoking: never, past, currentDiabetes mellitus: Previously diagnosed DM taking
medications or fasting plasma glucose � 126 mg/dl.†American Diabetes
Association, (34)Obesity: noted as overweight or obeseLifestyle: active or sedentary (medical record); exercise
quantification into 5 levelsCanada Fitness Survey (45)
* BP � blood pressure; LDL � low-density lipoprotein; HDL � high-density lipoprotein; DM � diabetesmellitus.† Oral glucose tolerance tests were not performed on any of the patients in this study.
984 Costenbader et al
were analyzed using SAS software (SAS Institute, Cary,NC).
RESULTS
Patient characteristics. Completed CHQs were returnedby 112 (78%) SLE patients. Two of these were excludedfrom the final analyses because complete medical recordscould not be obtained. The 110 subjects included in theanalysis were 97% female, with a mean (�SD) age of 43.4years (�11.8 years) and a mean disease duration of 15.3years (� 7.2 years). In general, it was a fairly affluent andwell-educated group of patients with only 10% below thenational poverty level and 67% having obtained more thana high school education. Sixty-eight percent subscribed toprivate medical insurance (of these, 14% were enrolled inan HMO), 20% received either Medicare or Medicaid, and12% had no insurance or received free care from the hos-pital. Eighty-five percent of the subjects were white, ademographic distribution typical of our clinic. Eighteendifferent American Board of Internal Medicine-certifiedrheumatologists, all American College of Rheumatologymembers, managed the subjects. Eleven (61%) of thesephysicians were men and 9 (50%) were senior physicianswith �10 years of subspecialty practice. A rheumatologyfellow was not the primary rheumatologist for any of thesubjects. Only 1 rheumatologist routinely provided pri-mary care for his patients.
The nonresponding subjects (n � 33) were slightlyyounger but not statistically so, with a mean age of 37.5years (�11.1; P � 0.07). There were no differences in termsof sex, race, SLE duration, or educational level betweenthe CHQ responders and nonresponders.
CRF knowledge. The CHQ results demonstrated thatsubjects were able to correctly identify most cardiac riskfactors, including obesity (89% correctly identified),smoking (81% correctly identified), hypercholesterolemia(80% correctly identified), and hypertension (78% cor-rectly identified). Fewer subjects were able to identifydiabetes mellitus as a risk factor for cardiac disease (51%),which may reflect the low prevalence of diabetes in oursubjects (�5% of the subjects had documented diabetesmellitus).
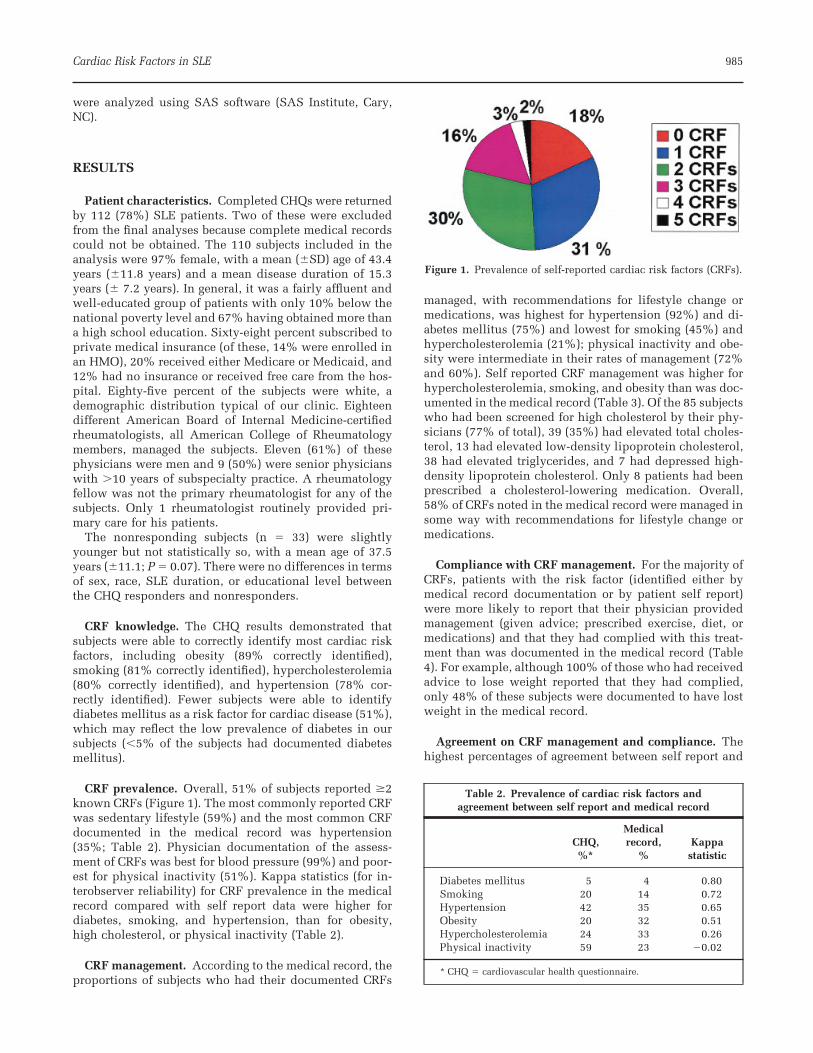
CRF prevalence. Overall, 51% of subjects reported �2known CRFs (Figure 1). The most commonly reported CRFwas sedentary lifestyle (59%) and the most common CRFdocumented in the medical record was hypertension(35%; Table 2). Physician documentation of the assess-ment of CRFs was best for blood pressure (99%) and poor-est for physical inactivity (51%). Kappa statistics (for in-terobserver reliability) for CRF prevalence in the medicalrecord compared with self report data were higher fordiabetes, smoking, and hypertension, than for obesity,high cholesterol, or physical inactivity (Table 2).
CRF management. According to the medical record, theproportions of subjects who had their documented CRFs
managed, with recommendations for lifestyle change ormedications, was highest for hypertension (92%) and di-abetes mellitus (75%) and lowest for smoking (45%) andhypercholesterolemia (21%); physical inactivity and obe-sity were intermediate in their rates of management (72%and 60%). Self reported CRF management was higher forhypercholesterolemia, smoking, and obesity than was doc-umented in the medical record (Table 3). Of the 85 subjectswho had been screened for high cholesterol by their phy-sicians (77% of total), 39 (35%) had elevated total choles-terol, 13 had elevated low-density lipoprotein cholesterol,38 had elevated triglycerides, and 7 had depressed high-density lipoprotein cholesterol. Only 8 patients had beenprescribed a cholesterol-lowering medication. Overall,58% of CRFs noted in the medical record were managed insome way with recommendations for lifestyle change ormedications.
Compliance with CRF management. For the majority ofCRFs, patients with the risk factor (identified either bymedical record documentation or by patient self report)were more likely to report that their physician providedmanagement (given advice; prescribed exercise, diet, ormedications) and that they had complied with this treat-ment than was documented in the medical record (Table4). For example, although 100% of those who had receivedadvice to lose weight reported that they had complied,only 48% of these subjects were documented to have lostweight in the medical record.
Agreement on CRF management and compliance. Thehighest percentages of agreement between self report and
Figure 1. Prevalence of self-reported cardiac risk factors (CRFs).
Table 2. Prevalence of cardiac risk factors andagreement between self report and medical record
CHQ,%*
Medicalrecord,
%Kappastatistic
Diabetes mellitus 5 4 0.80Smoking 20 14 0.72Hypertension 42 35 0.65Obesity 20 32 0.51Hypercholesterolemia 24 33 0.26Physical inactivity 59 23 �0.02
* CHQ � cardiovascular health questionnaire.
Cardiac Risk Factors in SLE 985

medical record review for whether CRFs were managed insome way were seen for hypertension (80%) and diabetes(66%), and lowest for physical inactivity (37%; Table 3).Percentages of agreement between the CHQ and the med-ical record for compliance with CRF management werelow overall, except for diabetes, in which 100% agreementwas found. Only 47% agreement was found for compli-ance with the management of obesity, 40% for the man-agement of hypercholesterolemia, and only 30% was seenfor the management of physical inactivity (Table 4).
In univariate models and linear regression analyses,among multiple potential predictors of agreement betweenself report and medical record documentation of CRF pres-ence, only patient education beyond high school wasfound to be a significant predictor of agreement. Otherpredictors examined in the model included race, age, du-ration of SLE, household income below the poverty level,and self efficacy. None of these predictors was signifi-cantly associated with agreement between self report andmedical record documentation of CRF management either.
Only 12 vascular events occurred in 1,632 person-yearsof observation (7.4%/10 person-years) and precluded anystudy of the demographic or clinical characteristics ofthese subjects.
DISCUSSION
The increased cardiovascular mortality associated withSLE has been documented for �25 years (1). A report byPetri et al in 1992 was the first indication that known CRFswere not being attended and suggested a failed opportu-
nity (16). Bruce and colleagues (26) have recently foundthat women in the Toronto SLE cohort continue to havemore traditional CRFs, including more sedentary lifestylesand at-risk body habitus, than do control subjects. A de-cade later, it seems there is still room for improvement.More than 50% of the subjects in our study, followed at alarge academic teaching hospital serving the surroundingurban and suburban communities, reported having �2CRFs. Our predominantly white, female population had amean age in the 40s, had a mean duration of SLE of 15years, was generally well educated, and very few patientshad household incomes below the national poverty level.This contrasts to earlier studies in the Baltimore lupuscohort, an urban, predominantly African American andpoorer SLE population (15,16,36) that have reported highprevalences and poor awareness of CRFs. Despite demo-graphic dissimilarities with our patient panel, the leadingCRF in this population was also sedentary lifestyle (15).Unlike these studies, our retrospective assessment of pa-tient awareness and management of CRFs included thepractices of 18 different rheumatologists and was not in-fluenced by the practices of any one physician in particu-lar.
Our patient population had a fairly high knowledge ofCRFs and was able to identify most traditional CRFs. Over-all, 58% of the modifiable CRFs identified were treated insome way, ranging from 92% for hypertension to 21% forhypercholesterolemia. Physician documentation and man-agement were much better for hypertension and diabetesthan for hypercholesterolemia, obesity, and physical inac-tivity.
We found discrepancies between subject self report andphysician documentation of CRFs and their management.In particular, rheumatologists and their SLE patients hadlow interrater reliability for the presence of high choles-terol, obesity, and physical inactivity. Our results suggestthat SLE patients are unaware of their elevated cholesteroland that, despite many recommendations to the contrary,aggressive physician management of hypercholesterol-emia is lacking. Although hypercholesterolemia waspresent in 39 (35%), only 8 were prescribed cholesterol-lowering medications—drugs proven to reduce cardiovas-cular mortality. According to the National Cholesterol Ed-ucation Program guidelines current at the time, at least 13should have received cholesterol-lowering medications(33). Twenty-three percent had never had their cholesterollevels checked. Agreement between SLE patients and theirrheumatologists as to whether CRFs had been addressedand whether patients had complied with these manage-ment strategies was best for hypertension and diabetes,and poorest for hypercholesterolemia, obesity, and physi-cal inactivity. The only patient characteristic found to bepredictive of patient–physician agreement was havinggreater than a high school education.
Bruce and colleagues have also retrospectively exam-ined CRF management in a group of Canadian SLE patientswho had had acute coronary events. They found that rheu-matologists had performed well in decreasing steroiddoses and treating hypertension, whereas other CRFs(such as smoking cessation, hypercholesterolemia, andobesity) had been managed less well (25). Al-Herz and
Table 3. Cardiovascular risk factor management andagreement between self report and medical record
CHQ,%*
Medicalrecord, %
Agreement,%
Diabetes mellitus 83 75 66Smoking 67 45 52Hypertension 96 92 80Obesity 62 60 50Hypercholesterolemia 66 21 50Physical inactivity 82 72 37
* CHQ � cardiovascular health questionnaire.
Table 4. Compliance with cardiovascular risk factormanagement and agreement between self report and
medical record
CHQ,%*
Medicalrecord,
%Agreement,
%
Diabetes 100 100 100Smoking 27 67 57Hypertension 98 48 50Obesity 100 48 47Hypercholesterolemia 100 50 40Physical inactivity 84 10 30
* CHQ � cardiovascular health questionnaire.
986 Costenbader et al

colleagues recently reviewed the assessment of CRFs in 1academic lupus center and 5 private practices in Vancou-ver (37). They found better documentation of CRFs in thelupus clinic than in the private practices, but only 62% ofthe patients seen in the academic center and 15% of thepatients seen in private practice had been screened forhyperlipidemia.
Our SLE patients acknowledged more physical inactiv-ity than was noted in the medical records. Although it maybe that physicians discuss these risk factors but do notdocument these conversations, it is also possible that thesediscussions are delayed or never broached due to the com-plexity of managing SLE itself. Patients with chronic dis-eases, such as diabetes and rheumatoid arthritis (38–40),are less likely to receive the highest quality preventivehealth care, perhaps because of the demand of dealingwith more urgent problems, or perhaps because of pa-tients’ and physicians’ exhaustion in dealing with chronichealth problems.
However, the message about CRFs in SLE may be gettingthrough to patients despite lack of documentation in themedical record. Patients consistently reported higher ratesof CRF management and compliance with managementstrategies than we found in the medical record. In addi-tion, patients’ perceptions of their efforts at lifestyle mod-ification probably differ from those of the physicians whodid not see or document weight loss, blood pressure, orcholesterol reduction.
Our study is retrospective and self-reported informationis vulnerable to response bias and recall bias, which wehave attempted to gauge by looking for confirmatory infor-mation from medical records. The medical record, how-ever, is subject to inaccuracies because the thoroughnessof documentation varies, and this variation may not berandom. The record is also a poor source for understand-ing whether a treatment was considered but not chosen,and for what reasons. It is suggested that some risk factors,such as obesity, smoking, and physical inactivity, are moreaccurately gauged through self reports on questionnaires(41).
Although 23% failed to respond to the CHQ, responsebias may be minimal. The nonresponders were slightlyyounger than the responders. This difference was not sta-tistically significant. All patients were followed at a singleacademic hospital and this may limit the generalizabilityof our results. However, it is all the more remarkable that,within this select group, CRF management and patient–physician communication concerning CRFs were still sub-optimal.
To decrease cardiovascular morbidity and mortality inSLE, experts have called for the rigorous implementationof therapies proven to reduce heart disease in the generalpopulation in SLE patients (21–25). Our study adds to theliterature that the state of the art is not the state of practice;and it would be profitable to ask “Why?” Potential barriersat every level of the shaping of health practices and behav-iors are suggested. First, there is no evidence that modify-ing traditional CRFs in SLE would improve cardiovascularoutcomes tremendously. Indeed, recent studies suggestthat even after adjustment for traditional CRFs, SLE and/orits therapy are independently associated with risk of ath-
erosclerosis (42–44). Second, long-term compliance withsmoking cessation, increasing physical activity, andweight reduction are notoriously difficult in the generalpopulation and perhaps even more difficult in individualswith SLE. The determinants of adherence and adherence-enhancing strategies in SLE have had little study. Last, themedications used in the management of hyperlipidemiahave not been evaluated for their efficacy, effectiveness,and tolerability in SLE.
ACKNOWLEDGMENTSThe authors acknowledge the comments of Drs. ElenaLosina and Ola Nived.
REFERENCES
1. Urowitz MB, Bookman AA, Koehler BE, Gordon DA, SmytheHA, Ogryzlo MA. The bimodal mortality pattern of systemiclupus erythematosus. Am J Med 1976;60:221–5.
2. Wallace DJ, Podell T, Weiner J, Klinenberg JR, Forouzesh S,Dubois EL. Systemic lupus erythematosus—survival patterns:experience with 609 patients. JAMA 1981;245:934–8.
3. Ginzler EM, Diamond HS, Weiner M, Schlesinger M, Fries JF,Wasner C, et al. A multicenter study of outcome in systemiclupus erythematosus. I. Entry variables as predictors of prog-nosis. Arthritis Rheum 1982;25:601–11.
4. Ginzler E, Berg A. Mortality in systemic lupus erythematosus.J Rheumatol 1987;14 Suppl 13:218–22.
5. Gladman DD, Urowitz MB. Morbidity in systemic lupus ery-thematosus. J Rheumatol 1987;14 Suppl 13:223–26.
6. Rosner S, Ginzler EM, Diamond HS, Weiner M, SchlesingerM, Fries JF, et al. A multicenter study of outcome in systemiclupus erythematosus. II. Causes of death. Arthritis Rheum1982;25:612–17.
7. Rubin LA, Urowitz MB, Gladman DD. Mortality in systemiclupus erythematosus: the bimodal pattern revisited. QJM1985;55:87–98.
8. Ward MM, Pyun E, Studenski S. Causes of death in systemiclupus erythematosus: long-term followup of an inception co-hort. Arthritis Rheum 1995;38:1492–99.
9. Manzi S, Meilahn EN, Rairie JE, Conte CG, Medsger TA Jr,Jansen-McWilliams L, et al. Age-specific incidence rates ofmyocardial infarction and angina in women with systemiclupus erythematosus: comparison with the FraminghamStudy. Am J Epidemiol 1997;145:408–15.
10. Hosenpud JD, Montanaro A, Hart MV, Haines JE, Specht HD,Bennett RM, et al. Myocardial perfusion abnormalities inasymptomatic patients with systemic lupus erythematosus.Am J Med 1984;77:286–92.
11. Shome GP, Sakauchi M, Yamane K, Takemura H, KashiwagiH. Ischemic heart disease in systemic lupus erythematosus: aretrospective study of 65 patients treated with prednisolone.Jpn J Med 1989;28:599–603.
12. Bulkley BH, Roberts W. The heart in systemic lupus erythem-atosus and the changes induced in it by corticosteroidtherapy: a study of 36 necropsy patients. Am J Med 1975;58:243–64.
13. Haider YS, Roberts WC. Coronary arterial disease in systemiclupus erythematosus: quantification of degrees of narrowingin 22 necropsy patients (21 women) aged 16 to 37 years. Am JMed 1981;70:775–81.
14. Kong TQ, Kellum RE, Haserik JR. Clinical diagnosis of cardiacinvolvement in systemic lupus erythematosus: a correlationof clinical and autopsy findings in thirty patients. Circulation1962;26:7–11.
15. Petri M, Spence D, Bone LR, Hochberg MC. Coronary arterydisease risk factors in the Johns Hopkins Lupus Cohort: prev-alence, recognition by patients and preventive practices.Medicine (Baltimore) 1992;71:291–302.
Cardiac Risk Factors in SLE 987
16. Petri M, Perez-Guttman S, Spence D, Hochberg MC. Riskfactors for coronary artery disease in patients with systemiclupus erythematosus. Am J Med 1992;93:513–19.
17. DeInocencio J, Lovell DJ. Cardiac function in systemic lupuserythematosus. J Rheumatol 1994;21:2147-56.
18. Leong KH, Koh ET, Feng PH, Boey ML. Lipid profiles insystemic lupus erythematosus. J Rheumatol 1994;21:1264–7.
19. Bruce IN, Urowitz MB, Gladman DD, Hallett DC. The naturalhistory of hypercholesterolemia in systemic lupus erythema-tosus. J Rheumatol 1999;26:2137–43.
20. Formiga F, Meco JF, Pinto X, Jacob J, Moga I, Pujol R. Lipidand lipoprotein levels in premenopausal systemic lupus ery-thematosus patients. Lupus 2001;10:359–63.
21. Hallegua DS, Wallace DJ. How accelerated atherosclerosis inSLE has changed our management of the disorder. Lupus2000;9:228–31.
22. Lockshin MD, Salmon JE, Roman MJ. Atherosclerosis andlupus: a work in progress [editorial]. Arthritis Rheum 2001;44:2215–7.
23. Aranow C, Ginzler EM. Coronary artery disease in SLE: highsuspicion leads to early recognition. J Musculoskel Med 2000;17:473–82.
24. Salmon JE, Roman MJ. Accelerated atherosclerosis in sys-temic lupus erythematosus: implications for patient manage-ment. Curr Opin Rheumatol 2001;13:341–4.
25. Bruce IN, Gladman DD, Urowitz MB. Detection and modifi-cation of risk factors for coronary artery disease in patientswith systemic lupus erythematosus: a quality improvementstudy. Clin Exp Rheumatol 1998;16:435–40.
26. Bruce IN, Urowitz MB, Gladman DD, Ibanez D, Steiner G. Riskfactors for coronary heart disease in women with systemiclupus erythematosus: the Toronto risk factor study. ArthritisRheum 2003;48:3159–67.
27. Daltroy LH, Eaton HM, Phillips CB, Karlson EW, Kaul H,Kinney GL, et al. Patient-partner communication, social sup-port, and self-efficacy for lupus management: preliminaryresults [abstract]. Arthritis Care Res 1999;12:S23.
28. Karlson EW, Daltroy LH, Lew RA, Wright EA, Partridge AJ,Fossel AH, et al. The relationship of socioeconomic status,race, and modifiable risk factors to outcomes in patients withsystemic lupus erythematosus. Arthritis Rheum 1997;40:47–56.
29. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, RothfieldNF, et al. The 1982 revised criteria for the classification ofsystemic lupus erythematosus. Arthritis Rheum 1982;25:1271–7.
30. Lorig K, Chastain RL, Ung E, Shoor S, Holman HR. Develop-ment and evaluation of a scale to measure perceived self-efficacy in people with arthritis. Arthritis Rheum 1989;32:37–44.
31. Finucane FF, Freid VM. J. H. M. plan and operation of theNational Health and Nutrition Examination Survey I Epide-
miologic Followup Study, 1986. Hyattsville (MD): NationalCenter for Health Statistics Vital Health Stat DHHS; 1990.Publication PHS. p. 90–1307.
32. Sixth report of the Joint National Committee on Prevention,Detection, Evaluation, and Treatment of High Blood Pressure.Bethesda (MD): National Heart, Lung and Blood Institute.National High Blood Pressure Education Program; 1997.
33. Summary of the second report of the National CholesterolEducation Program (NCEP) Expert Panel on Detection, Eval-uation, and Treatment of High Blood Cholesterol in Adults(Adult Treatment Panel II). JAMA 1993;269:3015–23.
34. American Diabetes Association: report of the Expert Commit-tee on the Diagnosis and Classification of Diabetes Mellitus.Diabetes Care 1999;22:S5–19.
35. Landis JR, Koch GG. The measurement of observer agreementfor categorical data. Biometrics 1977;33:159–74.
36. Petri M. Detection of coronary artery disease and the role oftraditional risk factors in the Hopkins Lupus Cohort. Lupus2000;9:170–5.
37. Al-Herz A, Ensworth S, Shojania K, Esdaile JM. Cardiovascu-lar risk factor screening in systemic lupus erythematosus.J Rheumatol 2003;30:493–6.
38. MacLean CH, Louie R, Leake B, McCaffrey DF, Paulus HE,Brook RH, et al. Quality of care for patients with rheumatoidarthritis. JAMA 2000;284:984–92.
39. Redelmeier DA, Tan SH, Booth GL. The treatment of unre-lated disorders in patients with chronic medical diseases.N Engl J Med 1998;338:1516–20.
40. Grant RW, Cagliero E, Murphy-Sheehy P, Singer DE, NathanDM, Meigs JB. Comparison of hyperglycemia, hypertension,and hypercholesterolemia management in patients with type2 diabetes. Am J Med 2002;112:603–9.
41. Katz JN, Chang LC, Sangha O, Fossel AH, Bates DW. Cancomorbidity be measured by questionnaire rather than med-ical record review? Med Care 1996;34:73–84.
42. Esdaile JM, Abrahamowicz M, Grodzicky T, Li Y, Panaritis C,du Berger R, et al. Traditional Framingham risk factors fail tofully account for accelerated atherosclerosis in systemic lu-pus erythematosus. Arthritis Rheum 2001;44:2331–7.
43. Asanuma Y, Oeser A, Shintani AK, Turner E, Olsen N, FazioS, et al. Premature coronary-artery atherosclerosis in systemiclupus erythematosus. N Engl J Med 2003;349:2407–15.
44. Roman MJ, Shanker BA, Davis A, Lockshin MD, SammaritanoL, Simantov R, et al. Prevalence and correlates of acceleratedatherosclerosis in systemic lupus erythematosus. N EnglJ Med 2003;349:2399–406.
45. Pereira MA, FitzerGerald SJ, Gregg EW, Joswiak ML, Ryan WJ,Suminski RR, et al. A collection of Physical Activity Ques-tionnaires for health-related research. Med Sci Sports Exerc1997;29:S1–205.
988 Costenbader et al













