Embed Size (px)
Citation preview


Cardiology TODAY
VOLUME XXII No. 4JULY-AUGUST 2018
PAGES 105-144
Rs. 1700/- ISSN 0971-9172 RNI No. 66903/97
www.cimsasia .com
MANAGING DIRECTOR & PUBLISHERDr. Monica Bhatia
EDITOR IN CHIEFOP Yadava
SECTION EDITORSSR Mittal (ECG, CPC), David Colquhou n (Reader’s Choice)
NATIONAL EDITORIAL ADVISORY BOARDArun K Purohit, Arun Malhotra, Ashok Seth, Ashwin B Mehta, CN Manjunath, DS Gambhir, GS Sainani, Harshad R Gandhi, I Sathyamurthy, Jagdish Hiremath, JPS Sawhney, KK Talwar, K Srinath Reddy, KP Misra, ML Bhatia, Mohan Bhargava, MR Girinath, Mukul Misra, Nakul Sinha, PC Manoria, Peeyush Jain, Praveen Jain, Ramesh Arora, Ravi R Kasliwal, S Jalal, S Padmavati, Satyavan Sharma, SS Ramesh, Sunil Kumar Modi, Yatin Mehta, Yogesh Varma, R Aggarwala.
INTERNATIONAL EDITORIAL ADVISORY BOARDAndrew M Tonkin, Bhagwan Koirala, Carlos A Mestres, Chuen N Lee, David M Colquhoun, Davendra Mehta, Enas A Enas, Gerald M Pohost, Glen Van Arsdell, Indranill Basu Ray, James B Peter, James F Benenati, Kanu Chatterjee, Noe A Babilonia, Pascal R Vouhe,Paul A Levine, Paul Simon, P K Shah, Prakash Deedwania, Salim Yusuf, Samin K Sharma, Sanjeev Saxena, Sanjiv Kaul, Yutaka Imoto.
DESK EDITORGandhali
DESIGNER A run Kharkwal
OFFICES CIMS Medica India Pvt Ltd(Previously known as UBM Medica India Pvt Ltd.)Registered OfficeMargosa Building, No. 2, 3rd Floor, 13th Cross, Margosa Road, Malleshwaram, Bengaluru -560 003 Karnataka, IndiaTel: +91-80-4346 4500Fax: +91-80-4346 4530
Corporate OfficeBoomerang (Kanakia Spaces), Wing-B1, 403,4th Floor, Chandiwali Farm Road, ChadiwaliPowai, Mumbai - 400 072Tel.: +91-22-6612 2600 Fax : +91-22-6612 2626
Regional Off ice709, 7th Floor, Devika Tower, Nehru Place, New Delhi-110 019, India. Tel: +91-11-4285 4300Fax: +91-11-4285 4310
EDITORIAL'Wired' Medicine or 'Mired' Medicine 107OP YADAVA
REVIEW ARTICLEAging Slowly, Living Longer and Future Projections for Exponential Survival and Longevity 109VINOD NIKHRA
REVIEW ARTICLECurrent Management of Acute Heart failure 120MOHAN BHARGAVA, MOHIT M BHAGWATI, PRACHAL BHARGAVA
REVIEW ARTICLENon Cardiac Surgery - How to 'Clear' a Patient ? 129PC MANORIA, PANKAJ MANORIA, NIDHI MISHRA
Cardiology Today VOL.XXII NO. 4 JULY-AUGUST 2018 105

FOR MARKETING QUERIESAparna Mayekar: +91-9930937020+91-22-6612 [email protected]
FOR EDITORIAL QUERIESDr Gandhali : +91-22-6612 [email protected]
©2018 CIMS Medica India Pvt Ltd (Previously known as UBM Medica India Pvt Ltd) Copyright in the material contained in this journal (save for advtg. and save as otherwise indicated) is held by CIMS Medica India Pvt Ltd Margosa Building, No. 2, 3rd Floor, 13th Cross, Margosa Road, Malleshwaram, Bengal uru-560 003, Karnataka, India. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, photocopying or otherwise, without prior permission of the publisher and copyright owner.
The products and services advertised are those of individual advertisers and are not necessarilty endorsed by or connected with the publisher or with Cardiology Today or CIMS Medica India Pvt Ltd. Cardiology Today does not guarantee, directly or indirectly, the quality or efficacy of any product or services described in the advertisements in this issue, which are purely commercial in nature.
The editorial opinions expressed in this publication are those of individual authors and not necessarily those of the publisher. Whilst every effort has been made to ensure the accuracy of the information in this publication, the publisher accepts no responsibility for errors or omissions.
For reprints (minimum order: 500) contact the production Department. Further copies of Cardiology Today are available from CIMS Medica India Pvt Ltd, 709, Devika Tower, Nehru Place, New Delhi-110 019, India.
Cardiology Today is Published and Printed by CIMS Medica India Pvt Ltd, Margosa Building, No. 2, 3rd Floor, 13th Cross, Margosa Road, Malleshwaram, Bengaluru - 560 003, IndiaTel: +91-80-4346 4500 (Board); Fax: +91-80-4346 4530
Printed at Modest Print Pack (P) Ltd., C-52, DDA Sheds Okhla Industrial Area, Phase-I, New Delhi-110 020.
ECG OF THE MONTHT Wave Inversion 135SR MITTAL
PICTORIAL CMEGiant Ramus Artery 143MONIKA MAHESHWARI
106 Cardiology Today VOL.XXII NO. 4 JULY-AUGUST 2018
EDITORIAL

Cardiology Today VOL.XXII NO. 4 JULY-AUGUST 2018 107
‘Wired’ Medicine or ‘Mired’ Medicine
EDITORIAL
In this contemporary world of ours, which is totally wired and full of electro-magnetic vibrations, a scary thought crosses the mind, that with all the cardiac implants around, some of which life-sustaining, can there be a science fiction Frankenstein scenario of a fraudulently intended attempt at dysfunctioning someone’s device. With cardiac pacemakers, can someone from a distance remotely disable the cardiac pacemaker functions or alter its parameters or with an automatic implantable cardio-defibrillator reset the parameters with a view to harming the patient? Can a metallic cardiac valve leaflet motion be disabled and paralyzed by an ill intended magnetic field? Can in a patient with a left ventricular assist device or a total artificial heart, the programmers and drivers of the heart be disabled? All of these are scary thoughts but mundane ones and it behooves us to look at our checks and counter checks to prevent any such eventuality coming to fruition.
Is cardiac device hacking therefore a clinical problem? Certainly, it is not a moot question and is infact worthy of deliberation with due diligence. This issue was brought to the fore-front by a media scare which was created by a report in 2016 regarding hacking of the permanent pacemakers used by Abbott. Latter responded by producing a ‘Firm-ware’ patch for addressing the issue. The fix however was a bigger problem, than the original problem itself.
However, if a recent publication in the Journal of American College of Cardiology by Baranchuk et al1 is to be believed, then ‘it is a hypothetical scenario … with a just a soap-opera take on it’. Lending credence is the fact that till date not a single such case of hacking has been reported in human beings. However, according to Baranchuk et al1 a bigger possibility is of a hacker interfering with network of a hospital system, which communicates with the individual’s cardiac device and a clinical event may be missed by the over-seeing tracking authority in a hospital. Just as when the ACC statement allays a lot of concerns on this front, it also issues a caveat to the physicians, device manufacturers and the regulators to look into these potential areas of concern going forwards.
DR. OP YADAVACEO and Chief Cardiac Surgeon
National Heart Institute,New Delhi

108 Cardiology Today VOL.XXII NO. 4 JULY-AUGUST 2018
Notwithstanding the preceding reassuring words of the ACC’s Electrophysiology section leadership group, the very fact that the human mind has conceived this idea and the pen written about it is proof enough that sooner or later such an event shall occur. Only debate … When? And the first such case may not be with a malevolent intent, but sheerly out of curiosity, and to satisfy man’s universal craving … me first.
God save the King !
REFERENCE1. Baranchuk A, Refaat MM, Patton KK et al. Cyber security for cardiac implantable electronic devices, what should you know.
J Am Coll Cardiol. Feb 2018. DOI:10.1016/j.jacc.2018.01.023

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 109
Aging Slowly, Living Longer and Future Projections for Exponential Survival and Longevity
REVIEW ARTICLE
VINOD NIKHRAKeywords
z aging z metabolic dysfunction z ROS z longevity z life extension z cryonics z human brain project z CR z SIRT
Dr Vinod Nikhra is Senior Consultant (Physician) and the Teaching Faculty at Hindu Rao Hospital, Delhi
AbstractLIVING AND AGING: The phenomenon of aging is universal in the kingdom of living. With time, all living beings age. There have been immense developments in the scientific understanding of biology of aging and the changes that take place with aging at cellular and molecular levels. At the same time, the progress in healthcare and technology has made it possible to delay the aging process and bring about healthy aging. A longer life and aging slowly are mutually related. Healthy food, adequate physical activity and wholesome lifestyle keep the daily attrition-related damage at a minimum and can retard aging. With the progress of science and technology, there are futuristic visions of achieving significant longevity.LIFE-FORMS, LIFESPAN AND LONGEVITY: Under the socio-cultural layers, we human beings are biological life-forms and share the same fate like other members of the bio-spora. The lifespan of an organism is limited, though not fixed and goes through the phases of life - birth, maturity, aging and death. An organism’s lifespan is limited, and so is that of the human-being. The microscopic roundworm, Caenorhabditis elegans, has a lifespan of about 3 weeks, a mouse of about 3 years, bats of about 20 years, and humans can live for about 100 years. The plants live longer, many surviving to hundreds of years, still not showing changes related to aging. There is nothing inherent in anatomy or physiology that limits the lifespan. At the biological level, the root factors evolving the protective mechanism called the survival instinct, endorse that the evolution has prepared us for longevity, not the brevity.METABOLIC DYSFUNCTION, ROS AND DECAY: Aging may mean decay, as the repairing process falters and there is a failure to restore and rejuvenate body tissues. Aging is, thus, a collection of cumulative changes at the cellular and molecular levels occurring gradually. The reactive oxygen species (ROS) or free radical theory is fundamental to the understanding of aging. The uncontrolled metabolic dysfunction

110 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
THE ESSENCE OF LIFEThe phenomenon of aging is universal in the kingdom of living. With time, all living beings age. There have been immense developments in scientific research and there has evolved a scientific understanding of the biology of aging. A vast body of knowledge can now explain the changes that take place with aging at cellular and molecular levels. At the same time, the progress in healthcare and technology makes it possible to delay aging process and bring about healthy aging. There are possibilities of being able to reverse the aging process as well in near future.1
LIFE IN MODERN TIMESWe live in the unprecedented times. There is a boom of advances in every field, from the art to the science and technology including medical sciences. The incredible advances in the field of medical science make it possible to cure acute disorders and avoid untimely demise. Chronic diseases like obesity, diabetes, hypertension, cardiovascular
disease (CVD) and cerebrovascular disease including stroke can be efficiently managed leading to virtual freedom from their complications. This has led to an appreciable increase in life expectancy and lifespan. The modern day high-tech interventions and revolutionized medicine and enable us to enjoy a good quality of life (QOL) and maintain an optimal level of function well into the later years. The Health is the prime instrument that lets us enjoy life and the preservation of health associated with aging slowly, is the best formula for longevity.
The lifespan of organisms, including human beings, is not fixed but limited.2 As an organism, we go through the phases of birth, maturation, youth, aging and death. Our physiological potential is marred as we live through the life as a biological-being and go on accumulating damage caused to body tissues due to disease processes and unhealthy lifestyles resulting in an accelerated aging and premature death. But, there are some important emerging trends in the current times. A good number of people are
surviving in their sixties and entering into the postretirement phase of life. With better health care and public health efforts, there is an increased average life expectancy in general and improved survival rates in particular. There is a significant reduction in chronic illness and disability during the advanced years due to improved lifestyles and better healthcare, making it possible to slow aging and living a longer and healthy life.
LONGEVITY: THE ETERNAL DREAMLonger life and aging slowly are mutually related.3 The healthy food, adequate physical activity and wholesome lifestyle keep the daily attrition-related damage at minimum and can retard aging. An optimal healthcare adds further. An individual’s life-course may appear unpredictable, but it is not. The genetic and environmental factors, both being of equal importance, and behavioural patterns can successfully predict the life expectancy. With the progress of science and technology, there are futuristic visions of achieving significant longevity, if not immortality.
REVIEW ARTICLE
is linked to accelerated aging. Thus, obesity is a disturbed metabolic state, having potential to cause metabolic syndrome, in which insulin resistance leads to diabetes, heart disease and other changes akin to aging related disorders. The life span has also been linked to metabolic rate and metabolic stability.GENETIC KEY AND CR: There are longevity clusters in population groups. The centenarians, in addition to being free of the negative genetic variations common in other human beings, have some positive mutations that increase the possibility of longer life span. The state of nutrition has a bearing on aging and the life span. The CR protects against disease, slows aging and prolongs life. With CR regimen, there is less free radical production, less mitochondrial mutation and less programmed cell deaths. The CR and CRAN reduce incidence of various diseases of aging such as cancer, heart disease, diabetes, osteoporosis, neurological decline and diseases such as Alzheimer's and Parkinson's, and improve the immune response. FUTURISTIC VISIONS OF SURVIVAL: The Life Extension Program (LEP) aims to increase the maximum lifespan beyond the current maximum for humans. It can be visualised to go through three steps - taking advantage of the existing knowledge for slowing aging like CR and CRAN; utilizing the advances in genetics and biotechnology; and using the future nanotechnology and artificial intelligence revolution to repair the mutation and other defect due to aging at molecular and cellular levels. The futuristic goal is, thus, to achieve rejuvenation and state of non-aging. A debatable aspect of LEP is cryonics, the practice of freezing a body at the time of clinical death with the aim of enabling eventual resuscitation back to life in the remote future. Another form of futuristic survival, quantum immortality, is to upload the mind like a computer software on to a new human-body-form generated by cloning, or onto a computer system and survive in a virtual environment. The initiative of the European Union, the Human Brain Project relates to this futuristic option and aims to scan and upload the human brain.CONCLUSION - QUEST FOR IMMORTALITY: A longer life is not separate from aging slowly, rather they are mutually related. With the scientific progress the futuristic visions of achieving significant longevity, if not immortality, seems quite possible. The eternal dream is on the verge of becoming a reality.

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 111
The eternal dream of living a long life is on the verge of becoming a reality.
People live life for different reasons. But in essence, we live because the life gives us joy. Primarily, we are because we live. Life gone, there is no world for us. All things apart, living is itself the objective. This is well demonstrated by all powerful survival instinct pervading through the bio-spora. Aging is just a temporal notion and the life is never enough. The more you live, more you cherish, weaving a world for you. A world, in which you want to live for forever. This is the prime thing, the eternal dream.
PLAN FOR HEALTHY AGING Further, aging process should not impact the life force and need not disable a person. We should plan for a healthy middle age and later years. Herein, comes the concept of a healthy or successful aging which can improve the QOL and make longevity possible.4 There are certain issues, when we consider the aging process. The first concerns the aging in terms of length of time. The second issue relates to the functional aspects of the aging. The Older adults may develop disability or incapacity for independent living as the result of damage load due to pre-existing diseases or due to the aging process itself. The third factor occurs at a more sublime level and involves behavioural attitudes and prejudices in the individuals themselves or prevalent in the society. A child, a youth or an older adult all have equal right to survive and to look forward to a better living. There need not exist any prejudice against those older in age. The life force need not be diluted at any age. THE AGING PROCESSAT CELLULAR AND MOLECULAR LEVELSIn essence, the aging is a disorder of accumulated recurrent and chronic injury at cellular and molecular levels.5
The developmental damage load during early phases of life complicates further, having a bearing on the residual functional capacity and the aging process.
The aging process is, thus, influenced by 3 factors: the developmental damage load, damaging effects of early life situations, and adverse effects of chronic disease processes. The advances in gerontology hold promise to deal with the damage. In the near future, the damages can be corrected using gene technology, rejuvenative medication and futuristic nanobiotechnology. The optimal healthcare and a careful and healthy lifestyle, meanwhile, can help in slowing the aging process.
THE PLASICITY OF LIFESPAN Life-Forms, Lifespan And Evolution Under the socio-cultural layers, we human beings are biological animals and share the same fate like other members of the bio-spora. The lifespan of an organism is limited, though not fixed and goes through the phases of life - birth, maturity, aging and death. Reproduction, whether sexual or asexual, allows new organisms to replace the old ones. The new organisms replacing in time the older ones, adapt to the changes in the echosphere, allowing evolution to take place. The advantageous changes are passed on to the next generation, the deleterious ones are eliminated along with the organism in due course of time. Thus, goes on the evolution and life. Studies show that in the roundworm, C. elegans, a mutation of the genes involved in the insulin-signaling pathway, namely daf2 and daf16 genes can induce an up to 2-fold increase in life span.5 Several external, behavioural and internal factors including the environment, genes, sex and reproduction, nutrition and food style, the accumulation of cellular attrition and damage, and the inherent ability to repair, influence aging process, life span and QOL during lifespan. The process of aging, though, begins much earlier before becoming apparent.
Organisms have different but limited life spans. The microscopic roundworm, C. elegans, has a lifespan of about 3 weeks, a mouse of about 3 years, bats of about 20 years, and humans can live for about 100 years. The plants live longer, many surviving to hundreds
of years, still not showing changes related to aging. The simple organisms, such as hydra, have an indefinite life span, apparently free of an intrinsic senescence. But, there is nothing inherent in anatomy or physiology that limits the lifespan. The evolutionary process is not against longevity and the organisms are programmed not to die but survive the adversities. Even the programmed cell death, an intrinsic phenomenon occurring at cellular level called apoptosis, is a mechanism meant to favour survival of the organism. At the biological level, the root factors, which evolve the protective mechanism called the survival instinct, endorse the fact that the evolution has prepared for longevity, not the brevity. To stay alive is a basic instinctive drive, being a natural precondition for all other activities. Today, a period of about 30,000 days is the average human lifespan. For a centenarian, it is about 40,000 days. Long ago, the average life expectancy was less than 20 years or about 7,000 days. Two centuries back, the life expectancy in 1796, was around 10,000 days which doubled a century later. Thus, the human lifespan though finite, is not fixed.
The Aging Process: Biology of Decay Whereas aging may mean decaying, as the repairing process weakens, living means restoring and rejuvenating the body tissues.7 According to the Reliability theory, at some phase in life, the aging system falters, leading to failure unless the cause is corrected or the faltering parts are replaced.8 The aging process, thus, contributes to the age-related decline in performance, productivity and health.
There are three main causes of decay: disease, trauma and aging. Looking at the brighter side, a number of advances in healthcare have virtually nullified the deterioration due to diseases, including both, infectious and non-infectious. Aging is a collection of cumulative changes at the cellular and molecular levels. It is not an event. Thus, we do not age all of a sudden, rather it comes gradually. Hence, the aging is a process made of various components. As we, go on understanding the components of aging and developing

112 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
the means to correct them, we can look ahead to win over the biological decay.
Attrition and Stress of Living With life, there occurs exposure to continuous attrition and damage, and accumulation of wastes and toxins.9 There occur some alterations in the genome due to inner causes like mitochondrial generation of free radicals and external factors like cosmic radiations. Every time a cell divides, there is a potential for error. Oxidative stress is also a potential source of damage at molecular level. Free radicals are generated within mitochondria and have the potential to alter the cellular material and internal structures. These factors have been linked with aging process at the cellular level.
The cells possess a number of systems for functional and structural maintenance and repair. In fact, the DNA-repair capability correlates well with the lifespan of a species. Also, there is a correlation between the ability to respond to stress and life span.10 An increased stress resistance has been noted in long-lived genetic strains. Stem cells have a higher resilience than the well-differentiated cells. Genes influence the life span of organisms, the body appearance, structure and functioning of inner organs. Studies also show that genes account for about 25 percent of what determines the life span.
Reproductive IssuesLife birth, growth, reproduction, aging, death and evolution through generations. Studies show that unmated fruit flies live longer than those which mate. In females, perhaps, the egg laying process imposes a stress on survival. Also, species with smaller litter sizes as compared to their own body size tend to survive long. In the same species, the body size may influence the aging and survival. The Aristocrat study – which compared the number of children and the age at which the mothers had their first child, and related these values with the age at death, inferred that women who reached an older age and a higher life span delivered less children and at a later age.11
REVIEW ARTICLE
Metabolic Dysfunction, ROS and Antioxidants The free radical theory is fundamental to the understanding of aging. Uncontrolled metabolic dysfunction is linked to accelerated aging. Thus, obesity is a disturbed metabolic state, having potential to cause metabolic syndrome, in which insulin resistance leads to diabetes, CVD and other related disorders. The life span has been linked to metabolic rate. Metabolism generates ROS that can damage DNA and proteins. Animals that live fast, die young; because a high metabolic rate produces large number of free radicals. According to this theory, long-lived animals should have high concentrations of antioxidant enzymes in their tissues and low concentrations of free radicals. Another related theory states that metabolic stability is a better predictor of longevity than metabolic rate. It proposes that an organism’s ability to maintain stable levels of free radicals is more important than how fast it produces them. Further, metabolic stability is more important than metabolic rate in determining life span, and long-lived organisms are more resistant to pathogens and other environmental stresses.
The ROS or free radicals are highly energetic molecules. They are chemically hyper-active and react with molecules including DNA and cellular proteins, oxidizing and damaging them and giving rise to mutations and other abnormalities leading them to become dysfunctional.12 The antioxidants, on the other hand, mop-up free radicals and help in reducing their damaging effects. In the mice experimental studies, the antioxidant effect was obvious in increasing the longevity as well as in preventing morbidity. Thus, by suitably using antioxidants, it is possible to delay or retard the underlying process of aging. On the other hand, the pharmacological agents that reduce ROS concentrations may even be harmful, because they could disturb the delicate balance necessary for normal cell function. The accumulation of free-radical damage, thus, may be the key regulator of life span. Genetic alterations in certain tissues may give rise
to the ability to resist free radical damage. The concept that mild stress might
lead to health benefits is called hormesis.13 Plants given low doses of herbicide, for example, can actually become stronger and grow better. It is thought that Sirtuin-activating compounds (STACs) increase lifespan because they are produced by plants when stressed or starving. Plants make these molecules to turn on their own protective sirtuin genes in order to defend themselves. Resveratrol is a plant extract of complex composition.14 Its use seems to mimic CR. Studies have proved resveratrol’s role in yeast longevity. Feeding lab mice resveratrol suppresses the growth of implanted tumours. But, the molecule is unstable and sensitive to light and air, having a short shelf-life. A high level of resveratrol is present in red wines. The molecule, which is concentrated in the skins of grapes, is highly insoluble in water. Traditionally, wine is stored in dark, light-proof bottles, corked to keep oxygen out. Resveratrol is thus preserved in red wines.
THE GENETIC KEY FOR LONGEVITY Molecular biology experiments with organisms such as yeast, nematodes, fruit flies and mice have succeeded in increasing the life span by altering single genes. The altered organisms age more slowly and live longer. Further, genetic manipulations causing these changes work through a common pathway across many species endorsing that there is an evolutionary genetic program that controls aging.
THE WORM-SIDE STORY: The tiny nematodes, Caenorhabditis elegans, when exposed to environmental stress during their development, enter into a state akin to hibernation by modifying themselves into a spore like forms, called dauers. They remain in this suspended condition for long periods, till the surroundings again become hospitable to growth. This phenomenon is an indication that an organism can, as part of physiology, regulate their life span. Further, altering the single gene - called daf-2 in C. elegans DNA, doubles the lifespan. Daf-2 appears to be a master control gene and modifies

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 113
the functions of many other genes. These other genes act in various ways - some make anti-oxidant proteins that protect the cells from oxidative damage and other may protect the cells from getting infections by bacteria. The daf-2 also encodes an insulin receptor, which links aging to another program, CR, that can extend life span in various organisms.
THE MITOCHONDRIAL GENETIC MUTATIONS: The genetic mutations in mitochondria, appear to trigger changes leading the cells to die and accelerate the aging process. By altering a gene called polymerase-in mice, which functions as a spellchecker during the copying of mitochondrial DNA led them to age fast. Because the mitochondria also control the natural process of cell death, called apoptosis, mistakes by the spell-checker gene enhance apoptosis. As mitochondrial mutations accumulate, there are increased cell deaths and appearance of the aging characteristics.
THE NEW ENGLAND CENTENARIAN PROJECT: The Project underlines that there is a tendency toward longevity clusters in population groups.15 In many centenarians’ families, longevity appears to be a dominant trait. Also, that one in 10,000 people alive today has longevity genes. Nevertheless, the clustering of genetic variations among centenarians suggests that there may be one or two genes common among long-lived individuals that have a much stronger influence than others. Human beings have the similar genes but vary from each other based on SNPs or single nucleotide polymorphisms. Some of these SNPs might increase the risk of hyperlipidaemia, CVD or Alzheimer’s disease. In addition to being free of the negative genetic variations common in other human beings, the centenarians also have some positive mutations that increase the possibility of longer life span.
CR AND CR WITH ADEQUATE NUTRITION CALORIE RESTRICTION (CR)The state of nutrition has a bearing on aging process and the life span. CR influences life expectancy. In general,
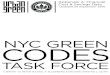
the CR regimen protects against disease and slows aging (Figure 1). The animals on CR, have lower levels of circulating blood glucose, insulin and triglycerides. In this context, limiting fat, protein or carbohydrate, without accompanying CR, does not increase the maximum lifespan. It seems probable that CR is an effective way to prolong life by reducing the amount of free radicals produced. There are less mitochondrial mutations and less programmed cell deaths. The effects of CR on lifespan, disease, and aging processes are applicable to virtually all species.
An optimal CR reduces the incidence of virtually all diseases of aging such as cancer, CVD, diabetes, osteoporosis, auto-immune disorders, cognitive decline and diseases such as Alzheimer's and Parkinson's diseases. CR extends maximum and average life spans and improves disease resistance. Ingestion of fewer calories also alters fat deposition, obesity, and hormones.16 But, CR is not without certain adverse effects. There occur hunger pangs, a decreased ability to handle stresses, such as cold temperatures or infection, osteoporosis and loss of muscle mass, and loss of fertility.
THE ROLE OF CR AND EXERCISE Exercise helps, both physically and
mentally. There takes place a number of molecular changes in the brain due to exercise. It increases the production of brain-derived neurotrophic factor (BDNF), which protects nerve cells and increases the number of nerve cells that are involved in various aspects of memory and cognition. But, losing weight via increased caloric expenditure, i.e. exercise, does not give the same health benefits obtained by CR. The reason lies in the free radical concept. Reducing food intake with CR will reduce oxidative damage. Exercise, in fact, contributes to increased free radical generation by burning food faster. But, these negative effects are more than offset by the health benefits of exercise, so that average lifespan is certainly increased by exercise. But, exercise does not add anything to the maximum lifespan and fairly little to the average lifespan when there is already a calorie restriction.
The human brain begins to shrink in volume at about age 30, as a normal process of aging continues to lose volume until the end of life. Aerobic exercise slows down the loss of brain tissue in older adults. These effects are predominantly seen in three key areas of the brain: the frontal, temporal and parietal regions. The frontal region regulates memory, planning, scheduling, decision-making,
Figure 1. Caloric Restriction and Longevity Circuits
OXIDATIVE DAMAGE
THEORY
HORMESIS
HYPOTHESIS
Tissue
Sress CALORIC
RESTRICTION
GROWTH HORMONE: IGF-1
AXIS
GLUCOSE-INSULIN
PATHWAYS
Insulin
Signalling
DNA Damage
Genome Stability
Growth Hormone
IGF-1 Signalling

114 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
etc. The temporal region is related to memory and memory consolidation. The parietal region is related to recall and navigation.
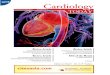
THE LINKS BETWEEN SIRTUINS AND CR There is a relationship between sirtuins, insulin-signaling pathway and CR.17 The sirtuins are controlled by insulin and another closely related hormone, insulin-like growth factor-1 (IGF-1). In mammals, there is SIRT1 gene (equivalent to Sir2 in yeast) which rises when levels of insulin and IGF-1 fall, as they do in a calorie-restricted organism. When sirtuins are triggered by STACs they don’t cause infertility, as occurs with CR. Thus, with STACs we can get all the benefits of CR without the trade-offs like infertility.18 The yeast is a single-celled fungus whose life span is defined by the number of times (on average 20-40) it can divide. Thus, the reorganization of DNA over the course of the lifetime is limited. But when the cell’s DNA is stabilized, both the average and maximum lifespans increase. One of the proteins that stabilizes the chromosomes of a yeast cell, encoded by a gene of the same name, is called sir2. The Sir2 gene is activated when the yeast cells are stressed. The Sir2 gene acts to stabilize the chromosome, so the cells live longer (Figure 2). When an extra copy of Sir2 gene was introduced into a yeast cell, enabling to generate about twice as much sir2 protein and stabilizing the DNA, the yeast lived about 30 percent longer. The sirtuins, thus, appear to be pro-survival molecules.
Sir2 is believed to be the founding member, in evolutionary terms, of a family of genes known as sirtuins that are present in all complex life forms. Another gene has been identified that controls Sir2, a master regulator called, PNC1. Stress turns on the PNC1 gene, the activity of which turns on Sir2. The STACs activate the sir2 protein. On feeding these molecules to yeast cells, roundworms and flies, the organisms live longer. These molecules act through Sir2, and are ineffective when the gene is deleted. The STACs have been found universally efficacious, even in humans.
RESEARCH INTO THE AGING PROCESSRELATING LAB RESEARCH TO HUMAN LONGEVITY Intervention studies in lab animals have led to understanding about types of receptors and complex metabolic pathways in mammals and humans. The links between insulin signaling, CR, and obesity could be centred on fat tissue. Fat is known to make hormones called adipokines, which may act on other tissues to alter longevity. Fat is also a source of molecules involved in oxidative stress, such as free radicals. Insulin signaling has connections to diabetes and metabolic syndrome. Calorie-restricted animals also exhibit an altered metabolism. They are slightly less efficient at converting food into energy but produce fewer free radicals and less oxidative damage. In human muscle, there is a decrease in oxidative metabolism with age. Given these emerging connections among diabetes, oxidative metabolism, and
aging in muscle and fat, there appears to be a common oxidative pathway that becomes less efficient with age.
AGING PROCESS AND THEORIES OF AGING Numerous studies and diverse observations have led to understanding of the phenomenon of aging. There are two main group of theories to explain the aging process: the systems theory (reliability theory) and those based on the biological evolution. A synthesis of the two group of theories may seem an attractive proposition.
THE RELIABILITY THEORY - Considers aging as a set of processes, which contribute to the age-related decline in performance, productivity and health, and ultimately death with the passage of time. Thus, the failure is an outcome, when the system deviates from optimistically anticipated and desired behavior. The reliability theory predicts that a system may deteriorate with age even if it is built from non-aging elements with constant failure rate. The system's redundancy for irreplaceable elements is responsible for the aging phenomenon. This theory allows to predict the age-related failure kinetics for a given system and why mortality rates increase exponentially with age. Further, a living organism may be formed with a high load of initial damage at birth or early-life conditions and their lifespan and aging patterns may be sensitive to this initial damage load during early development.
EVOLUTIONARY THEORIES OF AGING - The major evolutionary theories of aging include the mutation accumulation theory, the antagonistic pleiotropy theory, the disposable soma theory and theory of programmed death.19 The most viable evolutionary theories seem to be the mutation accumulation theory and the antagonistic pleiotropy theory, though they are not mutually exclusive.
PREDICTATORS OF LIFESPAN AND LONGEVITY There is an unusual pattern of human lifespan inheritance. It has been
Figure 2. CR and Longevity Promotion: SIRT and Other Players
Adiposity, Cytokine, IIS
Signaling, Thyroid Hormone
Adiponectin
Longevity
Promotion
Activation of SIRT1, PI3K/Akt signaling and Erk1/2) Signaling
Activation of Stress Defense and Survival Pathways / Attenuation of Proinflammatory Mediators
CR
REVIEW ARTICLE

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 115
discovered that there is no lifespan heritability, if parental lifespan is below a threshold age of 75-85 years and there is a strong heritability of human lifespan if parents live longer lives. It has also been found that the early circumstances of human life, such as the month of birth, may have a profound effect 30 years later on the chances of survival. These findings indicate that there may have been critical periods early in human development that are particularly sensitive to seasonal variations in living conditions, such as seasonal vitamin deficiencies or seasonal exposure to pathogens, etc. Studies also show that paternal age at person's conception may be an important predictor of lifespan. This may be related to the mutation load or other genetic damage in paternal sperm cells playing a significant role in determining the human lifespan.20 Numerous studies demonstrate that manifestations of aging can be postponed or even reversed, and that lifespan can be significantly extended in experimental animals. Studies have found remarkable plasticity of aging and longevity and a significant potential for further extension of human lifespan. On this basis we begin to think of aging as a disease that can be cured, or at least be slowed down.
WHERE DO WE STAND? FUTURISTIC VISIONS OF LONGEVITYIn the current times, there has come a growing interest for fitness and general health. People are looking forward for meaningful therapies, which can protect health and preserve life. There is an increased awareness for fitness, longer life and lasting health, and enthusiasm for living a long life.21 The latter is the driving force behind working for the life extension. The survival instinct is winning over the prejudices, fixations and obstacles, and exciting changes are taking place in the scientific world of gerontology, biotechnology and nanobiology which hold immense promise for slowing the aging and prolonging lifespan.
It is quite reasonable to take stock of the things, where do we stand and what lies in store for us in the near and
far future? This exercise will guide us in warding off unreasonable expectations from aging research; it will also help in consolidating our visions. A whole new generation of futurist visionaries believe that it will be possible to maintain human health at a youthful level for many extra decades by healthy living, employing new methods of anti-aging medicine and rejuvenation science. For the first time in human history, we have come close to understand, to slow down and probably reverse the aging.
THE MEANING OF LIFE EXTENSION Life extension stands for an increase in the maximum lifespan beyond the current maximum lifespan for humans. Exponential life extension can be defined as increase in life expectancy and life span by 50 per cent or more.22 For those who regard aging as a disease, therapeutic methods to extend maximum lifespan are anti-aging medicine. It was in 1970, the American Aging Association was formed under the initiative of Denham Harman, the originator of the free radical theory of aging. The bestselling book ‘Life Extension’ by Pearson and Shaw popularized the phrase and emphasised antioxidant supplements. In 1980, Saul Kent, the author of the book ‘The Life Extension Revolution’, created the Life Extension Foundation, a non-profit organization. The Life Extension Foundation later established, the Alcor Life Extension Foundation, the largest cryonics organization. In 1993 the American Academy of Anti-Aging Medicine (A4M) was formed to create an anti-aging medical specialty distinct from geriatrics. The most recent development in life extension has been the work of biogerontologist Aubrey de Grey, who proposes that the damage to macromolecules, cells, tissues and organs can be repaired by advanced nanobiotechnology.23
THE VISIONS FOR FUTURE: PURSUING END OF AGING As we are understanding the biological principles of life and the aging process,
and are able to utilize experimental research, the life extension program (LEP) can be visualised to go through three steps - Step One: Taking advantage of the existing knowledge for slowing aging like CR; Step Two: Utilizing the advances in genetics and biotechnology; and Step Three: Using the future nanotechnology and artificial intelligence revolution, which may have the potential to allow us to repair the mutations and other defects due to aging at molecular and cellular levels. Further, the way to cure aging is to rejuvenate tissues, not just to slow aging. Thus, the futuristic goal is to achieve rejuvenation and state of non-aging.24
THE SEVEN TYPES OF DAMAGE WITH AGE: The first is cell loss. Certain tissues, like heart and brain, lose cells with aging and these cells are not naturally replaced. The stem cell therapy can be used to restore the cells in these tissues. Second, mutations in chromosomes affect organ function and the life span and can cause cancer. Targeted gene therapy can be used to delete the telomere elongation genes in particular tissues at risk of developing cancer. The third is the mitochondrial mutations. Insertional gene therapy can introduce modified versions of the 13 protein-coding mitochondrial genes into nuclear DNA, which will prevent accumulation of mutations in the mitochondrial DNA. The fourth is the senescent cells. Immune therapy can be used to destroy senescent cells. Fifth, the extracellular cross-linking. It can be possible to design drugs that can break the cross links between long-lived molecules in the extra-cellular matrix, such as collagen and elastin. The sixth is the extra cellular junk. This is important in Alzheimer’s and Parkinson’s diseases and other neurodegenerative disorders. A2E seems to be responsible for macular degeneration and malformed proteins in the brain are thought to be responsible for Alzheimer’s disease. There is needed a therapy which can slow down the accumulation and get rid of it as well. The insertional gene therapy by introducing bacterial or fungal genes can break down the damaging accumulated chemicals and

116 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
proteins, including oxidized cholesterol causing atherosclerosis. The seventh, is to keep alive or preserved till the technology is practically available. Until molecular repair technologies are available, good health practices, nutritional supplements, CR and organ transplantation, and cryopreservation after death are the best hopes.
THE CONCEPT OF IMMORTALITY Immortality or eternal life is the concept existing for a potentially infinite length of time. The ideas of immortality exist since time immemorial in mythological tales. The modern sci-fi writers have also woven immortal worlds in their fiction. In more recent times, people have had their dead bodies cryopreserved in the hope that advances in medical science will allow them to be unfrozen, cured, and restored to health at some point in the future.25
There are three main causes of death: aging, disease and trauma. The hardest cause of death to overcome is trauma. In the postulated future world where aging will be correctable and diseases will be triumphed over, a trauma would still kill, unless technology advances to such extent that a body can automatically heal itself after a severe trauma (technological immortality), as it heals for the smaller ones.
An interesting possibility involves uploading the mind like a computer software on to a new human-body-form generated by cloning, or simply uploading human consciousness onto a computer system, and survive in a virtual environment.26 Quantum immortality is the name for this kind of speculation.27 The important aspects of current practical scientific thinking about immortality are human cloning, cryonics and nanotechnology. These projections lead us to notions of immortality or an unending existence.
DARKER-SIDE OF LIFE EXTENSIONIt appears that with the advancements in medical science, genetics, biotechnology and nanoscience, a true extension of human lifespan will come in the near
future.28 However, it may come at a price and there are fears associated with the extended life.
z The Tithonus Option: Today, the majority of people living in
the developed countries can expect to live well into their seventies. Even so, the final years are usually marked by impaired health and often senile dementia. There is a fear that anti-aging technology may present us with the extended lifespan but limited improvement in QOL. The nightmare, that we will live longer, but in bad health and mental deterioration, has been called Tithonus option - immortal life with sub-functional brain or eternal dementia.
The three possible futuristic outcomes may seem probable: The first, we will live and die as we do today. There may accrue no benefit of aging research. The second possibility, called the Tithonus option, is that the technology will give extended lifespan but will not be able to reduce prevalence of dementia and debility. The third possibility is that technology will be able to repair the damage done to our tissues with age, including neurons, thus granting us longevity with good quality of life.
z Life on Support Systems: In intensive care units, it is commonly
seen that for the critically ill patients, more and more invasive procedures are performed to save the life and more and more of vital functions are taken over by bio-machines. The person is considered living till the brain functions. It is an artificially prolonged life on support systems, amounting to a nightmare of proportion of the Tithonus option: a long life with zero quality of life.
While genetic engineering and nanotechnology may help in extending the life significantly, it does not follow that future technology will be able to repair all wear-and-tear on the brain and other body organs. If the future technology cannot repair all microscopic injuries, the Tithonus option will result. Considering a poor-quality-of-life better than no life, we may fall in the trap, finally accepting Tithonus option. People may regard it better than cryopreservation in hope of a novel treatment in the remote future.29
POSITIVE PROJECTIONS FOR EXTENDED LIFE Life extension is the natural progression of curing diseases by treatment and preventing the effects of aging altogether.30 The human life is sacred and should be cherished and preserved. The extended life spans will bring positive effects on society of a host of people with the wisdom of 150 years of life and the youthful vitality, which has been called the Gursky option, so named after Ian McDonald's novel, ‘The Days of Solomon Gursky’, where the inventions allow humans to stave off disease and improve their bodies. The issue of overpopulation should not be feared as with spread of benefits of technology, education, and women’s rights, fertility rates will decline. Life extension will not place a burden on health care but will itself be associated with good health and disability limitation. Older adults with extended life will be economically productive members of society.31 Delayed aging will lead to various social changes. The age stratification in the society will disappear, and along with it, many of our current social mores. The new ideas and new possibilities will evolve.32
CRYONICS AND BEYOND: CRYOFREEZING FOR THE FUTURE Cryonics is the practice of freezing a body at the time of clinical death with the aim of enabling eventual resuscitation back to life in the remote future. Cryonics offers a bridge to the future33 and a speculative life support technology that seeks to preserve human life in a state that will be viable and treatable by future medicine.34 Further, modern cryonics is based on a more sophisticated understanding of death called ‘information-theoretic death’. In the past, death was defined as cardiac arrest and the current medical definition of death is based on the cessation of electrical activity in the cerebral cortex. A person is dead according to the information theoretic criterion if their memories, personality, hopes, dreams, etc. have been destroyed in the information theoretic sense, and the
REVIEW ARTICLE

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 117
structures in the brain that encode memory and personality have been so disrupted that it is no longer possible to recover them. The information-theoretic death is ‘absolutely irreversible death’ in when the structures in the brain that encode memory and personality have been so disrupted that it is no longer possible to recover them, and the destruction of the brain has occurred to such an extent that any information it may have ever held is irrevocably lost for all eternity.35
The cryo-preserved bodies, not irreversibly dead as per the understanding of information-theoretic death, are kept indefinitely preserved in a thermos-type container filled with liquid nitrogen until the cryo-preservation damage would be possibly reversed at some time in future when the advanced state of science will allow the cause of the fatal disease to be cured and negate of the damage to the body because of the aging process. The support for cryopreservation is based on debatable projections of future technologies and of their ability to enable molecular-level repair of tissues and organs.
CRYOPRESERVATION: THE FROZEN LIFEThe cryopreservation process must begin immediately after legal death is declared as the individual organs remain biologically alive for some time, and vitrification, particularly of the brain, is possible. The legal death is a declaration by medical personnel that there is nothing more can be done to save the patient. But, the declaration of legal death does not mean that life has suddenly ended - death is a gradual process, not a sudden event. Acting immediately, the body is suitable for cryopreservation or the preservation of the brain is possible. Cryonicists try to minimize ischemic and reperfusion injury by beginning cardiopulmonary support and cooling as soon as possible after pronouncement of death (Figure 3).
The body is cooled to just above 0°C and the blood is replaced with a preservant and a solution is injected to stop ice crystals formation in organs and tissues,
then the body is further cooled gradually to -130°C. Anti-freeze compounds are then injected to stop cells being damaged. Finally the body is placed in a container which is lowered into a tank of liquid nitrogen at -196°C. The body or body parts, for instance brain, are cryopreserved in liquid nitrogen contained in the Dewar flask, which is custom-designed to contain four whole-body patients and six cryopreserved heads with brains inside, immersed in liquid nitrogen at -196°C. It is an insulated container which consumes no electric power. Liquid nitrogen is added periodically to replace the small amount that evaporates.
Newer forms of cryonics use a process called vitrification.36 Vitrification employs low temperatures and cryoprotectants to turn tissue into a glass-like state where decay is extremely slow. It is also possible to develop hybrid procedures involving elements of both cryonics and chemical brain preservation.37
HEAD (NEURO-) Vs. WHOLE-BODY CROPRESERVATION During the 1980s, the cryonics corporations shifted emphasis from
whole body to ‘neuro-preservation’ (i.e. head-only cryopreservation), on the assumption that the rest of the body could be regrown and reconstructed with nanotechnology. The main goal now is to preserve the information contained in the structure of the brain, on which memory and personal identity depends, and the available scientific and medical evidence suggests that the mechanical structure of the brain is wholly responsible for personal identity and memories. The chemical brain preservation can be viewed as a life-saving medical procedure. It allows the brain to be preserved for a long period and in the future, the information in a chemically preserved brain may be able to be decoded and emulated in a computer. Recent advances indicate this may soon be a real possibility. Damage caused by freezing and fracturing is thought to be potentially repairable in the distant future, using nanotechnology. The main limitation of current cryonics is that it is uncertain whether the information in the brain is truly preserved. Nonetheless, there is indirect evidence that cryonics as currently practiced may preserve the
Figure 3. Cryopreservation in action
Legal death declared, process to begin in 2-15 min.
The body packed with ice, and
Injected with chemicals to stop clotting
Body taken to cryonics facility.
Cooled to just over freezing point.
Blood replaced with Solutions to preserve organs
Another solution injected to stop ice crystal
formation in organs and tissues.
The body cooled to - 130 degree C
The body placed in a container.
The container put in a tank of liquid nitrogen
at temperature - 196 degree C.

118 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
information in the brain which could be recovered.
The hypothesis of chemical brain preservation as life extension was proposed by Drexler in 198738 and Olson in 1988. The systematic brain lesion studies have shown that the brain is completely responsible for the mind and the identity is defined by anatomy: that is, brain connectivity. Our memories and personalities are captured in the synaptic and dendritic connections in the brain, referred to as the connectome.39,40 The information theory of death and understanding of the connectome imply that death does not occur until the information in the connectome is irreversibly lost.41,42 Chemical brain preservation is not currently an option, but it is extremely likely that within a few years, whole brain preservation protocols with strong scientific support in favour of connectome preservation will be available. When this happens, chemical brain preservation can be viewed as a life-saving medical procedure.
In the distant future, technology may advance to the state where the information of an individual’s brain design can be extracted from his or her preserved brain and the complete connectome to be obtained from preserved brains. The next key piece of technology in making chemical brain preservation a life-saving procedure is whole brain emulation (WBE). WBE involves replicating the informational structure of the brain in software that could then be run in a computer. Knowledge of the connectome should allow for a complete emulation of brain function, and the technologies for mapping the connectome and for WBE have been advancing rapidly.43 The development of WBE and the computer technology to implement it is now an initiative of the European Union known as the Human Brain Project,44 which aims to develop a complete emulation of a mouse brain and later that for the human brain. The Human Brain Project aims to scan and upload a significant portion of the human brain.45
CRYONICS: THE FACTSAround 350 people worldwide have
had their bodies preserved in cryogenic chambers after death in the hope to be revived in the future. The experts at the Cryonics Institute (CI), Michigan have claimed that cryonically bringing someone back to life should definitely be doable in 100 years or sooner. The CI has about 160 patients frozen in specialised tanks of liquid nitrogen at its headquarters and has almost 2,000 people signed up to be frozen after they die.46 Two main US cryonics organisations are Alcor at Arizona, and the CI at Michigan. A Russian body KrioRus and Alcor's European laboratory in Portugal are the two facilities outside the US to offer the service. Aside from Trans Time, the other three cryonics organizations in the world which are storing human patients in liquid nitrogen are the Alcor Life Extension Foundation (founded in 1972 by Fred and Linda Chamberlain), the Cryonics Institute (founded in 1976 by Robert Ettinger), and KrioRus (located near Moscow in Russia, founded in 2006).
Cryopreservation arrangements can be expensive, currently ranging from $35,000 at the Cryonics Institute to $200,000 at Alcor. KrioRus' charges $37,600 for the procedure. But, even assuming perfect cryopreservation techniques, many scientists still regard the eventual revival as a long shot. It is being claimed that cryonics may replace traditional burials and cremations in the next few decades, leading to Cryo-Parlours in place of Funeral Parlours.
CONCLUSION: FROM AGING SLOWLY TO EXPONENTIAL LIFE EXTENSION AND IMMORTALITYCLARKE’S THIRD LAWThe aging is universal in the kingdom of living. We find people aging; we ourselves age and grow older. There has evolved a whole novel understanding of the biology of aging. Aging is a complex process and affects virtually all organs of the body. A vast body of knowledge can now explain the changes that take place with aging at molecular and cellular level. But, irrational hopes from technology move us away from terra-ferma and are
detrimental to rational scientific behavior. Thinking rationally, it is unlikely that something like a pill or potion, can reverse the changes and dysfunction associated with aging. At the same time, the progress in healthcare and technology has made possible to slow aging. Further, there are possibilities of being able to reverse the aging process. The possibility of a lengthy-healthy life is alluring. As the life expectancy at birth rises and there is taking place an improvement in average and maximum lifespan, the possibility of living life more than never before seems logical. Science gives visions; technology makes the visions possible. The future technology appears to offer us visions that rival the dreams of myth and legend. As per the Arthur C. Clarke's Third Law47 - ‘any sufficiently advanced technology is indistinguishable from magic’. One of these magical dreams is that of exponential life extension.
THE LIFE BEAUTIFUL An ideal body weight is desirable. Doing something new helps the brain. Research shows that most people lose over 20 percent of their muscle mass by age 70, leading to infirmity. People can reverse this aspect of aging by regular exercising. Reducing stress and adopting coping mechanisms is important. Taking a walk, praying, meditating or having lunch with a friend, are some of the stress-busting measures. People, who build the stress-busting habits into their daily routine, benefit much. Finally, finding life interesting is a primal desire, which encourages you to live and go on discovering the multiple facets of life on the Earth and beyond.
REGENERATIVE MEDICINE Apart from CR, regenerative medicine is the next concrete step for achieving longevity. The most promising in regenerative medicine is therapeutic cloning. A new organ can be grown for transplantation using one’s own cells. The process would involve transferring the nucleus from a cell to an enucleated
REVIEW ARTICLE

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 119
human egg, which would then grow to the blastocyst stage. Stem cells would be harvested from the blastocyst and transformed into the desired tissues for transplant. Regenerative medicine aims higher; it does not retard or slow aging but corrects organ failure and diseases that accompany aging. It is an advanced form of future medicine.
QUEST FOR IMMORTALITYLife is not a myth but an eternal truth. We are because we live. Living a healthy and long life is a common dream. All of us nourish the dream; all of us wish to realize it. Various diseases and infirmity annihilate the dream. Falling prey to aging we lose our health and fitness and pass through an abridged life. Scientifically speaking, longer life is not separate from aging slowly, rather they are mutually related. With the scientific progress the futuristic visions of achieving significant longevity, if not immortality seems quite possible. The eternal dream is on the verge of becoming a reality.
FOOTNOTES1. Affiliation – Senior Chief Medical Officer and Consultant, Department of Medicine, Hindu Rao Hospital and NDMC Medical College, New Delhi, India. Email: [email protected]. Disclosures – None.3. The Figures 1-3 in this Review Article are subject to Copyright by Dr Vinod Nikhra.
REFERENCES1. Johnson SC, Rabinovitch PS, Kaeberlein M. 2013. mTOR
is a key modulator of ageing and age-related disease. Nature. 2013 Jan 17;493(7432):338-45. doi: 10.1038/nature11861.
2. Petralia RS, Mattson MP, and Yao PJ. 2014. Aging and longevity in the simplest animals and the quest for immortality. Ageing Res Rev. 0: 66–82.
3. Tosato M, Zamboni V, Ferrini A, Cesari M. 2017. The aging process and potential interventions to extend life expectancy. Clin Interv Aging. 2(3): 401–12.
4. Strawbridge WJ, Wallhagen MI, Cohen RD. 2002. Successful Aging and Well-Being: Self-Rated Compared
with Rowe and Kahn. The Gerontologist, 42:6, 727–33.5. Poulose N, Raghavan R. 2014. Aging and Injury:
Alterations in Cellular Energetics and Organ Function. Aging Dis, 5:2, 101–08.
6. Uno M, Nishida E. 2016. Lifespan-regulating genes in C. elegans. NPJ Aging Mech Dis. 2016; 2: 16010. doi: 10.1038/npjamd.2016.10.
7. McHugh D. 2017. Senescence and aging: Causes, consequences, and therapeutic avenues, J of Cell Biology. DOI: 10.1083/jcb.201708092.
8. Gavrilov LA, Gavrilova NS. 2001. The reliability theory of aging and longevity. J Theor Biol. 213:4; 527-45.
9. Gray DA, Woulfe J. 2005. Lipofuscin and Aging: A Matter of Toxic Waste. Sci. Aging Knowl. Environ., 2005:5, p. re1.
10. Epel ES, Lithgow GJ.2014. Stress Biology and Aging Mechanisms: Toward Understanding the Deep Connection Between Adaptation to Stress and Longevity. J Gerontol A Biol Sci Med Sci.; 69(Suppl 1): S10–S16.
11. Doblhammer G. 2000. Reproductive history and mortality later in life: A comparative study of England and Wales and Austria, Population Studies, 54:2, 169-176, DOI: 10.1080/713779087.
12. Cui H, Kong Y, Zhang H. 2012. Oxidative Stress, Mitochondrial Dysfunction, and Aging, J Signal Transduct. doi 10.1155/2012/646354.
13. Mattson MP. 2008. Hormesis Defined. Ageing Res Rev. 7:1; 1–7, doi: 10.1016/j.arr.2007.08.007.
14. Berman AY, Motechin RA, Wiesenfeld MY, Holz MK. 2017. The therapeutic potential of resveratrol: a review of clinical trials. Npj Precision Oncology, vol 1, Article number: 35.
15. Sebastiani P, Perls TT. 2012. The Genetics of Extreme Longevity: Lessons from the New England Centenarian Study, Front Genet. 3: 277, doi: 10.3389/fgene.2012.00277.
16. Masoro EJ. 2000. There takes place an improvement in the immune response, as well. restriction and aging: an update. Experimental Gerontology 35; 299–305.
17. Guarente, L. 2000. Sir2 links chromatin silencing, metabolism, and aging. Genes Dev. 14, 1021–26.
18. Guarente L. 2013. Calorie restriction and sirtuins revisited. Genes Dev. 27:19; 2072–85. doi: 10.1101/gad.227439.113.
19. ScientificWorldJournal. 2002 Feb 7;2:339-56. Evolutionary theories of aging and longevity. Gavrilov LA, Gavrilova NS.
20. Palmore EB. 1982. Predictors of the Longevity Difference: A 25-Year Follow-Up. The Gerontologist, Vol 22:6, 513–18, https://doi.org/10.1093/geront/22.6.513.
21. Marshall J. 2006. Life extension research: an analysis of contemporary biological theories and ethical issues. Med Health Care Philos. 9:1;87-96.
22. Cerullo MA. 2016. The Ethics of Exponential Life Extension through Brain Preservation. Journal of Evolution and Technology, 26:1, 94-105.
23. de Grey A. 2003. ‘The foreseeability of real anti-aging medicine: focusing the debate’. Exp. Gerontology 38:9; 927-34.
24. Norman A, Reedy C. 2017. An End to Aging: Can Science Allow Humans to Become Immortal? Future Society. Futurism, accessed https://futurism.com/1-evergreen-an-end-to-aging-heres-how-were-fighting-death on 10 July 2018.
25. Ben B. 2000. Immortality: How Science Is Extending Your Life Span-and Changing the World. Avon: New York ISBN 0-380-79318-0.
26. Alexander B. 2010. Rapture: Human Immortality and Electronic Civilization. Publish America. ISBN 978-1-4489-3367-9.
27. Sandberg A. 2013. Feasibility of whole brain emulation. In Theory and philosophy of artificial intelligence, ed. V.C. Müller, 251–64. Berlin, Springer.
28. Stephen C. 2012. Immortality: The Quest to Live Forever and How it Drives Civilization. Crown. ISBN 0-307-88491-0.
29. Nikhra V. 2006. Ageing slowly, Living longer. Spandan Innovative in association with Sahni Publications. ISBN-81-7564-371-4.
30. de Grey A, Rae M. 2008. Ending Aging: The Rejuvenation Breakthroughs That Could Reverse Human Aging in Our Lifetime. ISBN 978-0230342200. St. Martin's Griffin.
31. Zhavoronkov A. 2013. The ageless generation: How advances in biomedicine will transform the global economy. New York: Palgrave Macmillan ISBN 978-0230342200.
32. de Grey A. 2005. Life extension, human rights, and the rational refinement of repugnance. Journal of Medical Ethics 31: 659–63.
33. Moen OM. 2015. The case for cryonics. Journal of Medical Ethics. Published online first February 25. doi:10.1136/medethics-2015-102715.
34. Merkle R. Lecture at the Farquhar College of Arts and Sciences Division of Math, Science, and Technology, Nova South-Eastern University. Merkle discussed "Life, Death, and Cryonics" on Thursday, October 2, 2008.
35. Whetstine L, Streat S, Darwin M, Crippen D. 2005. Pro/con ethics debate: When is dead really dead? Critical Care 9: 538–42.
36. Pichugin Y, Fahy G, Morin R. 2006. Cryopreservation of rat hippocampal slices by vitrification. Cryobiology 52: 228–40.
37. McIntyre RL, Fahy GM. 2015. Aldehyde-stabilized cryopreservation. Cryobiology.71:3; 448-58
38. Drexler KE. 1987. Engines of creation: The coming era of nanotechnology. London: Anchor. ISBN: 978-0385199735.
39. Sporns O, Tononi G, Kötter R. 2005. The human connectome: A structural description of the human brain. PLoS Computational Biology 1:4; e42.
40. Dubnau HK, Oyibo H, Zhan G, et al. 2012. Sequencing the connectome. PLoS Biology 10:10; e1001411. Article?id=10.1371.
41. Seung HS. 2011. Towards functional connectomics. Nature 471:170–72.
42. Seung HS. 2013. Connectome: How the brain’s wiring makes us who we are. New York: Houghton Mifflin Harcourt.
43. Eth D, Foust J, Whale B. 2013. The prospects of whole brain emulation within the next half-century. Journal of Artificial General Intelligence, 4:3; 130-52.
44. Human Brain Project. n.d. Human Brain Project website. https://www.humanbrainproject.eu.
45. Human Brain Project SP2. n.d. Human Brain Project Strategic Human Brain Data. https://www.humanbrainproject.eu/strategic-human-brain-data.
46. Harry Pettit, Mail Online 15 January 2018. http://www.dailymail.co.uk/sciencetech/article-5270257/Cryogenics-corpses-brought-10-years.html.
47. Arthur C. Clarke. 2000. Profiles of the Future: An Inquiry into the Limits of the Possible. ISBN-13: 978-1898801214. Publisher: Phoenix, The Orion Publishing Group Ltd.

120 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
Current Management of Acute Heart failure
REVIEW ARTICLE
MOHAN BHARGAVA, MOHIT M BHAGWATI, PRACHAL BHARGAVAKeywords z acute heart failure z decompensated geart failure z acute hypertensive failure z cardiogenic shock z vasodilators z vasopressins z inotropes z beta blockers
Dr. Mohan Bhargava is Principal Consultant and Interventional Cardiologist, Dr Mohit Bhagwati is 3rd yr SR, at Max Superspeciality Hospital, Saket, New Delhi & Dr Prachal Bhargava is Masters in Emergency Medicine 3rd yr SR, Aster CMI Hospital Bangalore
AbstractAcute Heart failure (AHF) can be defined as the new onset (sudden or gradual) or recurrence of symptoms and signs of HF which requires urgent therapy and results in hospitalization. It is one of the most common causes of emergency visits and ICU admissions. The annual incidence of HF in India is 491,600–1.8 million. Acute heart failure should be suspected in patients who present to the hospital with complaints of sudden or gradual onset dyspnea, edema or chest discomfort. Initial diagnosis of AHF should be based on a history , prior cardiac history and potential precipitating factors, as well as on the assessment of signs/symptoms of congestion and/or hypoperfusion by physical examination and further confirmed by appropriate additional investigations such as ECG, Chest X-ray, laboratory assessment (with specific biomarkers) and Echocardiography. Risk stratification can serve as important clinical tool in identifying high risk patients. Due to the high risk of mortality and re-hospitalization in the first 3 months after discharge, a risk stratification for post discharge events is necessary. There are well-defined criteria for ICU/CCU admission. Treatment of AHF is a complex multi-step process involving various goals at different levels of care including emergency care, hospital management, pre-discharge planning and post-discharge management and prevention of re-hospitalization. AHF continues to be a challenge for physicians across the globe and a systematic plan based management shall help us overcome this challenge with less difficulty.
INTRODUCTION Acute heart failure (AHF) can be defined as the new onset (sudden or gradual) or recurrence of symptoms and signs of HF
which requires urgent therapy and results in hospitalization. It is one of the most common causes of emergency visits and intensive care unit (ICU) admissions. In

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 121
US, 4 million patients are hospitalized every year with a diagnosis of heart failure (HF), and AHF contributes to more than 7 million hospital days every year.1 In India, the prevalence of heart failure is estimated to range from 1.3 to 4.6 million, with an annual incidence of 491,600–1.8 million.2 In Trivandrum heart failure registry, one out of three patients was admitted with AHF at least once in one year after recruitment to the registry.3 AHF can be the first presentation or it can be due acute decompensation of chronic heart failure. Ischemic heart disease and acute valve insufficieny are one of the most common primary caused while infection, uncontrolled hypertension, rhythm disturbances or non-adherence with drugs/diet are the most common triggers for sudden decompensation.
DIAGNOSIS OF ACUTE HEART FAILUREAcute heart failure should be suspected in patients who present to the hospital with complaints of sudden or gradual onset dyspnea, edema or chest discomfort. Initial diagnosis of AHF should be based on a history , prior cardiac history and potential precipitating factors, as well as on the assessment of signs/symptoms of congestion and/or hypoperfusion by physical examination and further confirmed by appropriate additional investigations such as ECG, Chest X-ray, laboratory assessment (with specific biomarkers) and Echocardiography. Usually signs and symptoms of AHF reflect fluid overload (pulmonary congestion and/or peripheral odema) or, less often, reduced cardiac output with peripheral hypoperfusion (Table 1). Clinical classification of AHF is based on bedside physical examination on basis of the presence of clinical symptoms/signs of congestion (‘wet’ vs. ‘dry’ if present vs. absent) and/or peripheral hypoperfusion (‘cold’ vs. ‘warm’ if present vs. absent). The combination of these options thus divides AHF into four groups: warm and wet (well perfused and congested) —most commonly present; cold and wet (hypoperfused and congested); cold and dry (hypoperfused without congestion); and warm and dry (compensated, well
perfused without congestion). This classification may be helpful to guide
Table 1: Signs and symptoms of acute heart failure Symptoms Signs
Due to Volume Dyspnea (Exertional dyspnea, Fine crackles, pleural effusion
overload orthopnea, paroxysmal
nocturnal dyspnea)
Foot and leg discomfort Pedal edema
Abdominal bloating, early Ascitis, increased weight, positive
satiety, anorexia hepatojugular reflux
Due to Fatigue Cold extremities
Hypoperfusion
Altered mental status, daytime Pallor, hypotension
drowsiness, confusion
Dizziness, presyncope, Narrow pulse pressure
or syncope
Other Depression Orthostatic hypotension
(hypovolemia)
Sleep disturbances S4
Palpitation Systolic/diastolic murmurs
therapy in the initial phase and carries prognostic information.4-6 However, the
Fig 1: Initial management of acute heart failure

122 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
sensitivity and specificity of clinical signs and symptoms are often not satisfactory, so careful clinical evaluation needs to be followed by certain investigations like Chest Xray, ECG, 2D Echocardioraphy, and blood investigations including natriuretic peptides and renal function test. The initial evaluation of the patient with acute HF should focus on establishing a definitive diagnosis of AHF as rapidly and efficiently as possible, initiating emergency treatment for potentially life-threatening conditions (e.g., shock, respiratory failure, identifying and addressing any relevant clinical triggers or other conditions requiring specific treatment (e.g., ACS, acute pulmonary embolism), risk stratifying the patient in order to triage patient to appropriate level of care (e.g., ICU, telemetry unit, observation unit) and defining the clinical profile of the patient (based on blood pressure, volume status, and renal function) in order to rapidly implement the most appropriate therapy. European Society of Cardiology, in its 2016 guidelines of Acute and Chronic heart failure recommends the following approach to initial management of acute heart failure (Figure 1).7
AHF can be classified on the basis of the presence or absence of a prior history of
HF. New-onset or de novo HF amounts to about 20% of hospitalizations for AHF.8 Majority of AHF are sudden decompensation of chronic heart failure.(Table 2). These patients usually have a less dramatic clinical presentation, since the chronic nature of the disorder has allowed for recruitment of compensatory mechanisms and usually these patients are already being treated with neurohormonal antagonists and loop diuretics, such that neurohormonal activation may be less profound but diuretic resistance is more common. Acute hypertension of reactive type is also associated with AHF, these patients are more likely to have sudden onset of symptoms. Frank pulmonary edema with evident rales and florid congestion on chest x-ray film is much more common in this group of patients, likely related to difference in LV compliance, acuity of pressure changes, and pulmonary lymphatic capacity, however this group tends to respond well to therapy and have lower in-hospital mortality.8 Other less common causes of heart failure are isolated right HF or high output HF.
Apart from classical signs and symptoms, certain investigations are routinely indicated to aid in diagnosis of Acute heart failure. Cardiac biomarkers of heart failure like BNP and NT-proBNP
are the important counter regulatory hormones in HF with vasodilatory effects. They play an important role in the differential diagnosis of patients presenting in the emergency department (ED) with dyspnea and are strongly recommended by clinical practice guidelines.10,11 The negative predictive value of natriuretic peptides is greater than the positive predictive value, so it can be used as a good rule out test in the emergency department (thresholds: BNP <100 pg/mL, NT-proBNP <300 pg/mL). Cardiac troponin is frequently elevated in patients presenting with AHF, and elevated levels are associated with worse in-hospital and post-discharge outcomes. Apart from natriuretic peptides and troponins, the following laboratory assessments should be performed at admission in all patients with AHF: blood urea nitrogen (BUN) (or urea), creatinine, electrolytes (sodium, potassium), liver function tests, thyroid-stimulating hormone (TSH), glucose and complete blood count; D-dimer is indicated in patients with a suspicion of acute pulmonary embolism.7 Creatinine, BUN and electrolytes should be measured every 1–2 days while in the hospital and before discharge from the hospital. Pre-discharge assessment of NPs may be considered for prognostic evaluation.
REVIEW ARTICLE
Table 2: Classification of acute heart failure9
Clinical Symptom Triggers Signs and Clinical Course
Classification Onset Symptoms Assessment
Decompensated Usually Noncomplicance, ischemia, Perpherial edems, SEP: variable Variable, high rehospitalization
heart failure gradual Infections orthopnea, dyspnea CXR: often clear despite rate
exertion elevated filling pressure
Acute Usually Hypertension, atrial Dyspnea (often severe) SBP: high High acuity, but patient often
hypertensive sudden arrhythmias, tachypnea, tachycardia (>180/100mmHg) responds quickly to therapy
failure ACS rales common CXR with pulmonary with vasodilators, noninvasive
edema ventilation.
Hypoxemia common
Cardiogenic Variable Progression of advanced HF End-organ hypo- SBP: low or low normal High inpatient mortality
Shock or major myocardial insuit perfusion; Oliguria, LV function usually Poor prognosis unless readily
(e.g., large AMI, acute confusion, cool severely depressed reversible cause or mechanical
myocarditis) extremities RV dysfunction support, transplanation
common
Laboratory evidence of
end-organ dysfunction
(renal, hepatic)

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 123
2. Hospital Management3. Pre-discharge planning4. Post-discharge management and
prevention of rehospitalisation
Phase I- Emergency careThe initial goals of emergency care after making a precise clinical diagnosis of heart failure are to treat life threatening abnormalities, provide urgent symptom relief, establish etiology and precipitating factors of AHF and transfer the patient in ward or intensive care unit for further management. Patients should be classified on the basis of congestion and perfusion and initial treatment should be started (Figure 2).
Dyspnea is the most common symptom in patients with AHF and immediate treatment should be provided to all patients to relieve dyspnea. Pulse oxymetry shouId be done in all patients
Invasive haemodynamic evaluation with a pulmonary artery catheter is not indicated routinely for the diagnosis of AHF. Chest Xray, ECG and 2d Echocardiography is indicated in all patients presenting with acute heart failure. 2D Echo should be done urgently in patients who are hemodynamically unstable.
RISK STRATIFICATIONRisk stratification can serve as important clinical tool in identifying high risk patients. Data from ADHERE Registry has been used to develop a classification and regression tree (CART) analysis to identify the best predictors of in-hospital mortality.12 They identified elevated BUN, lower SBP, and higher serum creatinine at admission to be the best predictors of in-hospital mortality. As there is a substantial risk of mortality or re hospitalization in the first 60 to 90 days after discharge in AHF patients, a risk stratification for post discharge events should also be done. Systolic BP has been found to be an important predictor of outcomes. There was a relatively monotonic relationship between blood pressure and mortality across the spectrum of blood pressure in the OPTIMISE HF registry.13 Apart from SBP, BUN and Natriuretic peptides are independent predictors of outcome in patients of AHF.14,15 All patients who present with AHF to the emergency department should be preferably admitted in the hospital. The criteria for ICU/CCU admission include any of the following:16
z need for intubation (or already intubated)
z signs/symptoms of hypoperfusion z oxygen saturation (SpO2) <90%
(despite supplemental oxygen) z use of accessory muscles for
breathing, respiratory rate >25/min z heart rate <40 or >130 bpm, SBP
<90 mmHg.
TREATMENT OF ACUTE HEART FAILURETreatment of AHF is a complex multi-step process involving various goals at different level of care and can be divided into four phases :1. Emergency Care
of HF and inhaled oxygen should be provided to all patients who have hypoxemia (SpO2<90). However, routine oxygen administration is not indicated in patients without hypoxemia and has shown to have adverse effects like vasoconstriction.17 Special care is needed in COPD patients where oxygen can be detrimental. Non-invasive ventilation in form of NIPPV (non-invasive positive pressure ventilation) and CPAP (continuous positive airway pressure) has been found effective in controlling dyspnea, heart rate and acidosis in patients who have cardiogenic pulmonary edema.18 Endotracheal intubation and mechanical ventilation is indicated if here is a contradiction to non-invasive ventilation (NIV) or if the patient is unable to tolerate NIV. Morphine may be useful in patients with anxiety, however it should not be routinely used
Figure 2: Clinical classification of AHF patients and their management

124 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
Vasodilators can be used as first-line therapy in combination with diuretics in the management of AHF patients to improve congestive symptoms, in the absence of hypotension.22 They decrease preload by venodilatation and decrease afterload by arterial dilatation, in addition increase stroke volume. Despite theoretical benefit, no robust evidence is there which prove their mortality benefit.23 These should be used with caution in patients who are preload or afterload dependent (e.g., severe diastolic dysfunction, aortic stenosis, mitral stenosis, coronary artery disease (CAD), since these drugs may cause severe hypotension. (Table 3)
The inotropic drugs are inodilators (inotropic drugs with vasodilatory properties), increase cardiac output through cAMP-mediated inotropy and reduce pulmonary capillary wedge pressure (PCWP) through vasodilation. (Table 4). However, use of inotropes is associated with slight risk in in-hospital and long term mortality.24,25 Inotropes should be reserved for patients with a severe reduction in cardiac output resulting in compromised vital organ
as it increases the likelihood of invasive ventilation, ICU admission and mortality.
Intravenous Loop Diuretics are the most frequently used initial treatment strategy in AHF and are cornerstone of the management of patients presenting with AHF and congestion. In addition to increased renal salt and water excretion, diuretics have some vasodilatory effect. However, In patients with AHF and signs of hypoperfusion, diuretics should be avoided before adequate perfusion is attained. Time to first administration of diuretic after entering the emergency, i.e., door to furosemide time (D2F time) should be less than 60 minutes and early treatment with intravenous loop diuretics is associated with lower in-hospital mortality in patients presenting at the ED for AHF (Figure 3).19 IV loop diuretics should be given in doses between 1 and 2.5 times the patient's oral loop diuretic dose for those receiving chronic diuretic therapy. However for newly diagnosed patients 20-40 mg of Furosemide or 10-20 mg of Torsemide should be administered. DOSE, a randomized double-blind study, prospectively compared diuretic strategies in AHF and found that there was no significant difference in either of the co-primary endpoints of global assessment of symptoms and change in
creatinine at 72 hours with administration by bolus compared to infusion or with the low- versus high-dose strategy.20 Thiazide diuretics, metolazone and natriuretic doses of mineralocorticoid receptors can be added to loop diuretics to augment the effect or to overcome diuretic resistance.21
REVIEW ARTICLE
Table 3: Commonly used Vasodilators in Acute Heart FailureDrugs Dose Adverse Effects Others
Nitroglycerine Start with10–20 µg/min, Hypotension, headache Tolerance on
increase up to 200 µg/min continuous use
Isosorbide dinitrate Start with 1 mg/h, Hypotension, Tolerance on
increase up to 10 mg/h headache continuous use
Sodium Nitroprusside Start with 0.3 µg/kg/min Hypotension, Light sensitive
and increase up to isocyanate toxicity
5 µg/kg/min
Nesiritide Bolus 2 µg/kg + Hypotension
infusion 0.01 µg/kg/min
Table 4: Inotropes and Vasopressors used in AHFDrug Dose
Noradrenaline 0.2-1 mcg/kg/min
Adrenaline 1mg IV bolus every 2-3 minutes for resuscitation
or 0.05-0.5 mcg/kg/min
Dopamine 3-5 mcg/kg/min for inotropic action,
>5mcg/kg/min for vasopressor action
Dobutamine 2-20 mcg/kg/min
Levosimendan 12mcg/kg iv bolus over 10 minutes,
0.1 mcg/kg/min(0.05-2 mcg/kg/min)
Milrinone 25-75 mcg/kg iv bolus over 10-20 minutes,
0.375-0.75mcg/kg/min
Figure 3: Effect of Door to Furosemide time on In hospital mortality in AHF

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 125
perfusion, which occurs most often in hypotensive AHF. They should not be used in the setting of hypovolemia or other potentially correctable factors of shock. If beta-blockade is thought to be contributing to hypoperfusion, levosimendan is preferable over dobutamine to reverse the effect of beta-blockade.26 Levosimendan is not suitable for treatment of patients with hypotension (SBP <85 mmHg) or cardiogenic shock unless in combination with other inotropes or vasopressors.27 Vasopressors like adrenaline, noradrenaline and dopamine are used raise blood pressure and redistribute blood to the vital organs. However, they also increase LV afterload. Among them, norepinephrine has fewer side effects and lower mortality associated with it and remains inotrope of choice.28
OTHER PHARMACOLOGICAL MEASURESDigoxin rapidly improves hemodynamics without increasing heart rate or decreasing BP by its positive inotropic action. However it is mostly indicated in patients with AF and rapid ventricular rate (>110 bpm) and given in boluses of 0.25–0.5 mg intravenously. Due to various drug-drug interactions and toxicity, it is not recommended routinely.29 Digoxin is now only used as reserve drug in patients not responding to other therapy. Vasopressin antagonists such as tolvaptan block the action of arginine vasopressin (AVP) at the V2 receptor in renal tubules. It promotes aquauresis. It can be used to treat patients with volume overload and resistant hyponatraemia.30 However, studies of short-term therapy when compared to placebo in AHF did not show any benefit.31 Thromboembolism prophylaxis with heparin or another anticoagulant is recommended only if there is an indication like acute coronary syndrome, acute pulmonary embolism, atrial fibrillation or if the patient is on existing treatment with oral anticoagulants. Ultrafiltration using renal replacement therapy has a theoretical advantage over diuretics of removing isotonic fluid without causing neurohormonal activation.32 However, various studies comparing loop diuretics and ultrafiltration failed to show any
significant benefit of ultrafiltration over diretics.33-34 The use of ultrafiltration is limited to patients with refractory volume overload, oliguria unresponsive to fluid resuscitation measures, severe hyperkalemia (K+ >6.5 ), severe acidosis (pH <7.2), serum urea level >150 mg/dL and serum creatinine >3.4 mg/dL. Intra-aortic balloon pump is not indicated routinely, however ventricular assist devices and other mechanical supports may be used as a bridge to decision in refractory cardiogenic shock.7
PHASE II- HOSPITAL MANAGEMENTThe goals of in hospital management after providing acute treatment and stabilizing hemodynamics, volume status, initiate or optimize chronic HF therapy. Etiology of AHF should be identified and all other co-morbidities must be addressed. Standard hemodynamic monitoring of heart rate, blood pressure, respiratory rate and oxygen saturation should be done in all patients. Patients should be weighed daily and accurate fluid balance chart including intake output measurement should be done in all patients. Laboratory monitoring should include daily analysis of electrolytes and
renal function, especially when RAAS inhibitors are introduced. Evaluation for myocardial ischemia may be needed if there is suspicion of ischemia as a trigger of decompensation. Dietary sodium restriction (2 g daily) and fluid restriction (2 L daily) may be useful to help treat congestion, however its role is not yet certain.35 Thromboembolism prophylaxis should be given as per guidelines in case of prolonged immobility. Invasive hemodynamic monitoring is not indicated routinely, however intra-arterial blood pressure monitoring can be done in hypotensive patients.
If the patient of AHF has been admitted due to acute decompensation of chronic heart failure, every attempt should be made to continue disease modifying guideline based oral therapy. In the absence of hemodynamic instability or contraindications, beta-blocker therapy should be continued in patients already on beta blockers during the admission for AHF, unless significant hypotension or cardiogenic shock are present. Patients who had beta blocker withdrawn had higher in-hospital mortality, short-term mortality, and combined short-term rehospitalization.36 RAAS inhibitors can
Table 5 : Criteria for Hospital discharge in Acute Heart failure38
Recommended in all AHF patients Exacerbating factors addressed.
Near optimal volume status observed.
Transition from intravenous to oral diuretic
successfully completed.
Patient and family education completed,
including clear discharge instructions
LVEF documented
Smoking cessation counseling initiated
Near optimal pharmacologic therapy achieved,
including ACE inhibitor and beta blocker (for
patients with reduced LVEF), or intolerance
documented
Follow-up clinic visit scheduled, usually for 7-10 days
Should be considered for patients Oral medication regimen stable for 24 hours
with advanced HF or recurrent No intravenous vasodilator or inotropic
admissions for HF agent for 24 hours
Ambulation before discharge to assess functional
capacity after therapy
Plans for post discharge management
(scale present in home, visiting nurse or telephone
follow up generally no longer than 3 days after
discharge)
Referral for disease management, if available

126 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
be temporarily stopped if worsening renal failure necessitates their discontinuation. In case of HF with reduced ejection fraction (HFrEF) diagnosed de novo, all attempts should be made to initiate oral guideline directed medical therapy inside the hospital.
PHASE III- PRE DISCHARGE PLANNINGThe goals of pre-discharge planning in a patient admitted with AHF comprises of preparing and evaluating the readiness for discharge, initiation of guideline directed medical therapy, address the side effects of medication and worsening of renal function with optimal management and optimizing therapy in order to prevent early re-hospitalization (Table 5). All attempts should be made to achieve dry weight of the patient before discharge as persistent clinical congestion at discharge
is associated with a high risk for re-hospitalization.37 Evaluation of functional capacity with simple maneuvers such as climbing one flight of stairs or walking down the corridor should be done before discharge. Observation for a period of 24 hours after discontinuation of vasoactive or inotropic support is ideal, but shorter periods may suffice for patients whose symptoms have significantly improved and who tolerate weaning of intravenous support well.
PHASE IV- POST DISCHARGE MANAGEMENT AND PREVENTION OF RE HOSPITALIZATIONA robust post-discharge care plan should be implemented in all AHF patients as the natural history of AHF is characterized by relatively low in-hospital mortality but a high rate of recurrent post discharge events. Recurrent hospitalizations for
AHF results in a substantial clinical worsening of patients.39 Therefore patients discharged from the hospital require post discharge support with a care plan, early physician follow-up and patient-centered discharge instructions about diet, exercise and adherence to medication. This care plan includes up-titration of guideline directed medical therapy with regular monitoring, need and timing of device therapy if required and education for lifestyle management. All details regarding medication, dietary sodium restriction, and recommended activity level should be provided in detail. Early follow up prevents re hospitalization and should be scheduled within 7 to 10 days after discharge, or even earlier in high risk patients.40 Alcohol moderation and smoking cessation should be advised and a regular monitoring of body weight, electrolytes and renal function should be done. All disease modifying drugs should be escalated to maximum possible doses to achieve maximal benefit. (Table 6) Early initiatation and upgradation of GDMT has shown to decrease post discharge outcomes more than any other factor.41 All other co-morbidities should also be given importance while evaluating a multi-disciplinary approach to treat heart failure.
MECHANICAL CIRCULATORY DEVICES IN AHFSome patients of AHF may not respond to medical therapy alone and may require intra-aortic balloon pump support or Impella device support prior to revascularization, while some patients would require ECMO (extra corporeal membrane oxygenation) or LVAD (left ventricular assist device) which is lifesaving, or in some patients they may be used as bridge to heart transplant.43-46 (Figure 4).
FUTURE DIRECTIONSAHF continues to be the biggest problem for cardiologists across the globe, several therapies tried so far target symptoms, the syndrome. However, various studies are being carried out targeting the pathophysiology of the syndrome. The concept of “One therapy fits all” doesn’t
Table 6: Starting dose and target doses of drugs in Guideline directed medical therapy.42
Drugs Starting dose Target dose
Beta Blockers
Bisoprolol 1.25 mg once daily 10 mg once daily
Carvedilol 3.125 mg twice daily 25 mg twice daily for weight <85 kg
and 50 mg twice daily for weight > 85 kg
Metoprolol succinate 12.5–25 mg/d 200 mg daily
ARNI
Sacubitril/valsartan 24/26 mg–49/51 mg 97/103 mg twice daily
twice daily
ACE inhibitor
Captopril 6.25 mg thrice daily 50 mg thrice daily
Enalapril 2.5 mg twice daily 10–20 mg twice daily
Lisinopril 2.5–5 mg daily 20–40 mg daily
Ramipril 1.25 mg daily 10 mg daily
ARB
Candesartan 4–8 mg daily 32 mg daily
Losartan 25–50 mg daily 150 mg daily
Valsartan 40 mg twice daily 160 mg twice daily
Aldosterone antagonists
Eplerenone 25 mg daily 50 mg daily
Spironolactone 12.5–25 mg daily 25–50 mg daily
Vasodilators
Fixed-dose 20 mg/37.5 mg 2 tabs thrice daily
combination (one tab)
isosorbide dinitrate thrice daily
/hydralazine
Ivabradine 2.5–5 mg twice daily Maximum dose
Titrate to heart 7.5 mg twice daily
Rate 50–60 bpm
REVIEW ARTICLE

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 127
hold true for AHF due to heterogeneity of the disease. Current research on natriuretic peptides like urodilation and soluble guanylate cyclase activators like cinaciguat are promising and further large trials are required to prove their benefit.47-48 More and more intensive device-based management of refractory cardiogenic shock is being studied to save the most sick fraction of AHF patients by providing them circulatory support. Guideline-based management of HF continues to be the cornerstone of HF management till we get some robust evidence.
CONCLUSIONAHF remains one of the most common causes of emergency department visits, especially in the elderly population. It is not only a difficult disease to manage, but carries a high in-hospital and 30 day mortality. AHF patients require prompt diagnosis and quick risk stratification and should be managed in an aggressive manner with diuretics, vasodilators, inotropes, oxygen and positive pressure ventilation. Patients should be stabilized and disease-modifying guideline-directed medical therapy of HF should be initiated before discharge in all patients to prevent re-hospitalization. AHF continues to be a
challenge for physicians across the globe and a systematic plan based management shall make us overcome this challenge with less difficulty.
REFERENCES1. Mozaffarian D, Benjamin EJ, Go AS, et al: Heart disease
and stroke statistics—2016 update: a report from the American Heart Association. Circulation 2016; 133: pp. e38-e60
2. Huffman MD, Prabhakaran D. Heart failure: Epidemiology and prevention in India. Natl Med J India 2010;23:283-8
3. Harikrishnan S, Sanjay G, Agarwal A, Kumar NP,et al. One-year mortality outcomes and hospital readmissions of patients admitted with acute heart failure: Data from the Trivandrum Heart Failure Registry in Kerala, India. Am Heart J. 2017 ;189:193-199
4. Ponikowski P, Jankowska EA. Pathogenesis and clinical presentation of acute heart failure. Rev Esp Cardiol (Engl Ed) 2015;68:331–337.
5. Nohria A, Tsang SW, Fang JC,et al. Clinical assessment identifies hemodynamic profiles that predict outcomes in patients admitted with heart failure. J Am Coll Cardiol 2003;41:1797–1804
6. Stevenson LW. Design of therapy for advanced heart failure. Eur J Heart Fail 2005; 7:323–331
7. Ponikowski P, Voors AA, Anker SD, et al: 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016; 37: 2129-2200
8. Nieminen MS, Brutsaert D, Dickstein K, et al: EuroHeart Failure Survey II (EHFS II): a survey on hospitalized acute heart failure patients: description of population. Eur Heart J 2006; 27: 2725-2736
9. Felker GM, Teerlink JR: Diagnosis and Management of Acute Heart Failure. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 24, 462-489
10. Knebel F, Schimke I, Pliet K,et al . NT-ProBNP in acute heart failure: correlation with invasively measured hemodynamic parameters during recompensation. J Card Fail. 2005 ;11(5):S38-41
11. Maisel AS, Krishnaswamy P, Nowak RM, et al: Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med 2002; 347:161-16
12. Fonarow GC, Adams KF, Abraham WT, et al: for the Adhere Scientific Advisory Committee. Risk stratification for in-hospital mortality in acutely decompensated heart failure: classification and regression tree analysis. JAMA 2005; 293: 572-580
13. Gheorghiade M, Abraham WT, Albert NM, et al: Systolic blood pressure at admission, clinical characteristics, and outcomes in patients hospitalized with acute heart failure. JAMA 2006; 296: pp. 2217-2226
14. Filippatos G, Rossi J, Lloyd-Jones DM, et al: Prognostic value of blood urea nitrogen in patients hospitalized with worsening heart failure: insights from the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Chronic Heart Failure (ACTIV in CHF) study. J Card Fail 2007; 13: 360-364
15. Kociol RD, Horton JR, Fonarow GC, et al: Admission, discharge, or change in B-type natriuretic peptide and long-term outcomes: data from Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) linked to Medicare claims. Circ Heart Fail 2011; 4: 628-636
16. Mebazaa A , Yilmaz MB, Levy P, Ponikowski P, Peacock WF, Laribi S, Ristic AD, Lambrinou E, Masip J, Riley JP, McDonagh T, Mueller C, DeFilippi C, Harjola V-P, Thiele H, Piepoli MF, Metra M, Maggioni A, McMurray J, Dickstein K, Damman K, Seferovic PM, Ruschitzka F, Leite-Moreira AF, Bellou A, Anker SD, Filippatos G. Recommendations on pre-hospital and early hospital management of acute heart failure: a consensus paper from the HFA of the ESC, the European Society of Emergency Medicine and the Society of Academic Emergency Medicine. Eur J Heart Fail 2015;17:544–558
17. Sepehrvand N, and Ezekowitz JA: Oxygen therapy in patients with acute heart failure: friend or foe? JACC Heart Fail 2016; 4: 783-790
18. Gray A, Goodacre S, Newby DE, et al: Noninvasive ventilation in acute cardiogenic pulmonary edema. N Engl J Med 2008; 359:142-151
19. Matsue Y, Damman K, Voors AA, Kagiyama N, Yamaguchi T, Kuroda S, Okumura T,Kida K, Mizuno A, Oishi S, Inuzuka Y, Akiyama E, Matsukawa R, Kato K, Suzuki S,Naruke T, Yoshioka K, Miyoshi T, Baba Y, Yamamoto M, Murai K, Mizutani K, Yoshida K, Kitai T. Time-to-Furosemide Treatment and Mortality in Patients Hospitalized With Acute Heart Failure. J Am Coll Cardiol. 2017 27;69(25):3042-3051. doi:10.1016/j.jacc.2017.04.042. PubMed PMID: 28641794.
20. Felker GM, Lee KL, Bull DA, Redfield MM, Stevenson LW, Goldsmith SR, LeWinter MM, Deswal A, Rouleau JL, Ofili EO, Anstrom KJ, Hernandez AF, McNulty SE, Velazquez EJ, Kfoury AG, Chen HH, Givertz MM, Semigran MJ, Bart BA, Mascette AM, Braunwald E, O'Connor CM; NHLBI Heart Failure Clinical Research Network. Diuretic strategies in patients with acute decompensated heart failure. N Engl J Med. 2011 Mar 3;364(9):797-805. doi: 10.1056/NEJMoa1005419. PubMed PMID: 21366472; PubMed Central PMCID: PMC3412356
21. Mentz RJ , Kjeldsen K, Rossi GP, Voors AA, Cleland JGF, Anker SD, Gheorghiade M, Fiuzat M, Rossignol P, Zannad F, Pitt B, O'Connor C, Felker GM. Decongestion in acute heart failure. Eur J Heart Fail 2014;16:471–482
22. Singh A, Laribi S, Teerlink JR, Mebazaa A. Agents with vasodilator properties in acute heart failure. Eur Heart J. 2017 Feb 1;38(5):317-325. doi:10.1093/eurheartj/ehv755. PubMed PMID: 28201723.
Age Comorbidities
Neurological function
Medical therapy Inotropic support
Vasopressor support Fluids
Ventilatory supportRevascularization
Patient stablePatient unstable
Weaning
Weaning
Standard therapy
Weaning
Destination therapy Heart transplantation
LVAD support
Impairedneurological
function
Age, comorbidities
Age, comorbidities
Normal neurological
function
Cardiac functionrecovers
No cardiac function recovery
Assess neurology/ end organ function
Consider surgicalLVAD/BiVAD
Cardiac functionrecovers
Figure 4: Algorithm for use of Ventricular assist device16

128 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
REVIEW ARTICLE
23. Ho EC, Parker JD, Austin PC, et al: Impact of nitrate use on survival in acute heart failure: a propensity-matched analysis. J Am Heart Assoc 2016; 5:
24. Mebazaa A, Parissis J, Porcher R, et al: Short-term survival by treatment among patients hospitalized with acute heart failure: the global ALARM-HF registry using propensity scoring methods. Intensive Care Med 2011; 37: pp. 290-301
25. Felker GM, Benza RL, Chandler AB, et al: Heart failure etiology and response to milrinone in decompensated heart failure: results from the OPTIME-CHF study. J Am Coll Cardiol 2003; 41: pp. 997-1003
26. Mebazaa A , Nieminen MS, Filippatos GS, Cleland JG, Salon JE, Thakkar R, Padley RJ, Huang B, Cohen-Solal A. Levosimendan vs. dobutamine: outcomes for acute heart failure patients on β-blockers in SURVIVE. Eur J Heart Fail 2009;11:304–311
27. Gong B , Li Z, Yat Wong PC. Levosimendan treatment for heart failure: a systematic review and meta-analysis. J Cardiothorac Vasc Anesth 2015;29:1415–25
28. De Backer D , Biston P, Devriendt J, Madl C, Chochrad D, Aldecoa C, Brasseur A, Defrance P, Gottignies P, Vincent J-L. Comparison of dopamine and norepinephrine in the treatment of shock. N Engl J Med 2010;362:779–789
29. Gheorghiade M, and Braunwald E: Reconsidering the role for digoxin in the management of acute heart failure syndromes. JAMA 2009; 302: 2146-2147
30. Gheorghiade M , Konstam MA, Burnett JC, Grinfeld L, Maggioni AP, Swedberg K, Udelson JE, Zannad F, Cook T, Ouyang J, Zimmer C, Orlandi C, Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators. Short-term clinical effects of tolvaptan, an oral vasopressin antagonist, in patients hospitalized for heart failure: the EVEREST Clinical Status Trials. JAMA 2007;297:1332–1343
31. Felker GM, Mentz RJ, Cole R, et al: Efficacy and safety of tolvaptan in patients hospitalized with acute heart failure. J Am Coll Cardiol 2017; 69:1399-1416
32. Felker GM, and Mentz RJ: Diuretics and ultrafiltration in acute decompensated heart failure. J Am Coll Cardiol 2012; 59: 2145-2153
33. Patarroyo M, Wehbe E, Hanna M, et al: Cardiorenal outcomes after slow continuous ultrafiltration therapy in refractory patients with advanced decompensated heart failure. J Am Coll Cardiol 2012; 60:1906-1912
34. Costanzo MR, Negoianu D, Jaski BE, et al: Aquapheresis versus intravenous diuretics and hospitalizations for heart failure. JACC Heart Fail 2016; 4:95-105
35. Aliti G, Rabelo ER, Clausell N, et al: Aggressive fluid and sodium restriction in acute decompensated heart failure: a randomized clinical trial. JAMA Intern Med 2013; 173:1058-1064
36. Prins KW, Neill JM, Tyler JO, et al: Effects of beta-blocker withdrawal in acute decompensated heart failure: a systematic review and meta-analysis. JACC Heart Fail 2015; 3:647-653
37. Ambrosy AP, Pang PS, Khan S, et al: Clinical course and predictive value of congestion during hospitalization in patients admitted for worsening signs and symptoms of heart failure with reduced ejection fraction: findings from the EVEREST trial. Eur Heart J 2013; 34: 835-843
38. Heart Failure Society of America, Lindenfeld J, Albert NM, Boehmer JP, Collins SP, Ezekowitz JA, Givertz MM, Katz SD, Klapholz M, Moser DK, Rogers JG, Starling RC, Stevenson WG, Tang WH, Teerlink JR, Walsh MN. HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Card Fail. 2010 ; 16 (6):e1-194. doi:10.1016/j.cardfail.2010.04.004. PubMed PMID: 20610207
39. O'Connor CM, Miller AB, Blair JE, et al: Causes of death and rehospitalization in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction: results from Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan (EVEREST) program. Am Heart J 2010; 159: 841-849 e1
40. Hernandez AF, Greiner MA, Fonarow GC, et al: Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA 2010; 303: 1716-1722
41. Fonarow GC, Abraham WT, Albert NM, et al: Association between performance measures and clinical outcomes
for patients hospitalized with heart failure. JAMA 2007; 297: -70
42. Yancy CW, Jessup M, Bozkurt B, et al. 2016 ACC/ AHA/HFSA focused update on new pharmacological therapy for heart failure: an update of the 2013 ACCF/ AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2016;68:1476–88
43. Mizuno M, Sato N, Kajimoto K, Sakata Y, Minami Y, Munakata R, Hagiwara N,Takano T; Acute Decompensated Heart Failure Syndromes [ATTEND] investigators.Intra-aortic balloon counterpulsation for acute decompensated heart failure. Int J Cardiol. 2014 Oct 20;176(3):1444-6. doi: 10.1016/j.ijcard.2014.08.154. Epub 2014 Sep 2. PubMed PMID: 25223815
44. Hall SA, Uriel N, Carey SA, Edens M, Gong G, Esposito M, O'Kelly R, Annamalai S, Aghili N, Adatya S, Kapur NK. Use of a percutaneous temporary circulatory support device as a bridge to decision during acute decompensation of advanced heart failure. J Heart Lung Transplant. 2018 Jan;37(1):100-106. doi:10.1016/j.healun.2017.09.020. Epub 2017 Sep 30. PubMed PMID: 29056460
45. Dangers L, Bréchot N, Schmidt M, Lebreton G, Hékimian G, Nieszkowska A, Besset S, Trouillet JL, Chastre J, Leprince P, Combes A, Luyt CE. Extracorporeal Membrane Oxygenation for Acute Decompensated Heart Failure. Crit Care Med. 2017 Aug;45(8):1359-1366. doi: 10.1097/CCM.0000000000002485. PubMed PMID: 28471885
46. Tallaj J.A., Pamboukian S.V., Bourge R.C. (2008) Role of Left Ventricular Assist Devices in Acute Heart Failure Syndrome and the Future of the Replacement Heart. In: Mebazaa A., Gheorghiade M., Zannad F.M., Parrillo J.E. (eds) Acute Heart Failure. Springer, London
47. Packer M, O’Connor C, McMurray JJ, et al. Effect of ularitide on cardiovascular mortality in acute heart failure. N Engl J Med. 2017;376:1956–1964
48. Erdmann E, Semigran MJ, Nieminen MS, et al. Cinaciguat, a soluble guanylate cyclase activator, unloads the heart but also causes hypotension in acute decompensated heart failure. Eur Heart J. 2013;34:57–67.
REVIEW ARTICLE

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 129
Non Cardiac Surgery – How to ‘Clear’ a Patient ?
REVIEW ARTICLE
PC MANORIA*, PANKAJ MANORIA**, NIDHI MISHRA***
Keywords z functional capacity z preoperative cardiac testing z electrocardiogram z left ventricular function z anticoagulants z statins
Dr. P.C. Manoria is Director, Dr. Pankaj Manoria is Chief Intervention Cardiologist at Manoria Heart & Critical Care Hospital, Bhopal and Dr. Nidhi Mishra is Asst. Professor, Deptt. of Biochemistry, Mahaveer Institute of Medical Sciences, Bhopal
AbstractWorldwide around 20 million people undergo non-cardiac surgery annually, of which a large proportion are geriatric patients. Mortality from surgery increases with age, and cardiovascular complications are the most common cause of death. Cardiac complications after non-cardiac surgery depend on procedure-related risk, patient-related risk and functional capacity (FC). Perioperative cardiac morbidity evaluation can be assessed using the revised cardiac risk index. It is reasonable to perform a 12-lead electrocardiogram (ECG) preoperatively in patients with known Coronary Artery Disease (CAD), peripheral arterial disease, significant arrhythmia, cerebrovascular disease, or other structural heart disease, except in case of low-risk procedure. In patients with unknown cause of dyspnea or in patients with HF with worsening dyspnea or any change in clinical status, it is reasonable to assess left ventricular (LV) function preoperatively by echocardiography. Assessment of functional capacity by exercise stress testing is useful only if it will change management. In patients in whom functional capacity is not known, cardiopulmonary testing may be considered prior to elevated-risk noncardiac surgery. Preoperative revascularization for noncardiac surgery is recommended only when it is indicated as per guidelines for acute coronary syndrome (ACS). In patients undergoing surgery, the benefit of continuation of anticoagulants should be weighed against risk of bleeding procedure. Management of anticoagulant use is also crucial. A careful evaluation of the patient taking into consideration the procedure related risk, the patient related risk and functional capacity coupled with use of appropriate drugs and necessary precautions paves the way for minimizing cardiovascular morbidity and mortality in the peri-operative period and also shorten the hospital stay.
Worldwide, it is estimated that around 20 million people undergo noncardiac surgery annually.1 One-third of surgeries are performed in geriatric population. The overall mortality is 1-5%; in individuals <65 years the average mortality is 1% whereas in individuals above 65 years
the morality is higher (about 5%). Cardiovascular complications are the most common cause of death.2,3 All deaths in the first 48 hours are due to cardiac causes like heart failure (HF), acute coronary syndrome. The deaths from 48 hours to 6 weeks are usually due to a non

130 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
REVIEW ARTICLE
cardiac causes like Pneumonia, Sepsis, Pulmonary Embolism, Renal Failure etc. Pre-operative evaluation is of paramount importance as appropriate preventive and therapeutic strategies may decrease cardiovascular (CV) morbidity and mortality and shorten the hospital stay.
The main purpose of peri-operative evaluation is to get familiar with the following basic questions.
z What are the underlying risk factors which the patient is having prior to non-cardiac surgery?
z What is the anticipated patient related risk?
z What is the proper preoperative treatment to reduce the anticipated risk during surgery and steps to be taken in the post operative period to reduce morbidity and mortality
The cardiac complications after non-cardiac surgery depends on 3 factors: 1. Procedure related risk.2. Patient related risk. 3. Functional capacity (FC).
PROCEDURE RELATED RISKThe surgical risk for cardiac events depends on the type of procedure being carried out. High risk procedures have a mortality of 5%, intermediate risk procedures 1-5% and low risk procedures <1% (Table 1)
PATIENT RELATED RISKThe patient related risk depends on the underlying disease as shown in Table 2.
FUNCTIONAL CAPACITYIt is an important test in preoperative cardiac risk assessment and is measured in metabolic equivalents (METs). Exercise testing provides an objective assessment of FC but without this it can be estimated from the ability to perform activities in daily life (Table 3).
Poor functional capacity is associated with an increased incidence of post operative cardiac events. When functional capacity is good, the prognosis is excellent even in presence of stable IHD or risk factors.
Peri-operative cardiac morbidity risk evaluation: This is commonly assessed by Revised Cardiac Risk Index.
Revised cardiac risk index: The revised cardiac risk index (4,5) is a simple tool that has been validated to assess the peri-operative risk of major cardiac events. The variables of this score are shown in Table 4 and single point is assigned to every risk factor present. The risk of cardiac arrest, or death 30 days after surgery are shown in Table 5. Patients having zero or only one risk factor have a low risk of major adverse cardiac events (MACE), whereas those with 2 or more risk factors have elevated risk.
ANCILLARY PREOPERATIVE CARDIAC TESTING- RECOMMENDATIONS12- Lead electrocardiogram
It is reasonable to perform a 12-lead electrocardiogram (ECG) preoperatively in patients with known Coronary Artery Disease (CAD), peripheral arterial disease, significant arrhythmia, cerebrovascular disease, or other structural heart disease, except for those patients who are going for low-risk procedure. Routine use of preoperative 12-lead ECG is not useful and is not recommended. A 12- lead ECG gives important prognostic information in patients with known CAD related to short-term and long term morbidity and mortality. It also provides a baseline that can be compared postoperatively if any change in the clinical status of the patient occurs. An interval of 1 to 3 months is considered to be an acceptable interval between the scheduled noncardiac surgery and obtaining a 12-lead ECG; however, optimal timing is unknown.
ASSESSMENT OF LEFT VENTRICULAR FUNCTION In patients with unknown cause of dyspnea or in patients with HF with worsening dyspnea or any change in clinical status, it is reasonable to assess left ventricular (LV) function preoperatively by echocardiography. Reassessment of LV function can be considered in clinically stable patients, if it was done more than a year ago. However, routine evaluation of LV function is not recommended preoperatively.6 There is an association documented in literature between reduced LV systolic function and peri-operative
Table 1: Procedure related riskHigh (5%) Intermediate (1-5%) Low (<1%)
Emergent major operations (elderly) *Carotid endarterectomy Endoscopic procedures
Aortic & other major vascular surgery Head and neck surgery Superficial procedure
Peripheral vascular surgery *Intraperitoneal, Intrathoracic surgery Cataract surgery
Anticipated prolonged surgical procedures Orthopedic surgery Breast surgery
Prostate surgery Dental
Pulmonary, renal/liver transplant. Gynecology, urologic-minor
Table 2: Patient related riskMajor Intermediate Minor
ACS Prior Myocardial infarction Advanced age
Decompensated HF Mild angina Abnormal ECG
Significant Arrhythmias Compensated HF Rhythm other than sinus
Severe VHD* Stenotic lesions like AS, MS Diabetes Mellitus Past stroke
Poor FC Renal insufficiency Uncontrolled hypertension
*VHD : Valvular Heart Disease, AS: Aortic Stenosis, MS:Mitral Stenosis

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 131
complications, more so in patients with postoperative HF. Greatest risk is seen in patients with left ventricular ejection fraction (LVEF) of <35% at rest. There are very little data on assessment of diastolic dysfunction preoperatively. However, it is recommended to perform LV function in patients who are candidates for potential solid organ transplantation as per transplantation specific guidelines.
EXERCISE STRESS TESTINGIn patients undergoing elevated risk procedure with unknown or poor functional capacity (<4 METs), it is reasonable to assess the functional capacity by exercise stress testing, only if it will change management. In patients with excellent exercise tolerance (>10 METs) or those with moderate to good exercise tolerance (>4 METs) scheduled for elevated risk noncardiac
surgery, it reasonable to proceed for surgery without any further stress testing. Routine screening with noninvasive stress testing is not recommended.7
CARDIOPULMONARY TESTINGIn patients in whom functional capacity is not known, cardiopulmonary testing may be considered prior to elevated-risk noncardiac surgery.
Many studies have shown that a low anaerobic threshold predicts peri-operative cardiac complications and postoperative death. The proposed discriminative anaerobic threshold ranges between 9 and 11 mL O2/kg/min.
PHARMACOLOGICAL TESTINGIn patients who have poor functional capacity scheduled for elevated-risk noncardiac surgery, it is reasonable to evaluate with either dobutamine stress
echocardiogram or pharmacologic stress myocardial perfusion imaging (Table 6), only if it changes further management. However routine screening is not recommended in patients going for low risk noncardiac surgery.8
There is a lack of randomized controlled trials (RCTs) on the use of preoperative stress testing. Evidence is based on large number of studies which have shown that the presence of moderate to large areas of myocardial ischemia, predicts increased peri-operative MI and/or death. Also if a patient has a normal study, it has a high negative predictive value for peri-operative MI and/or cardiac death. Also, fixed defects seen on myocardial perfusion imaging (MPI) have a low peri-operative predictive value for cardiac events compared with normal MPI, but have an increased risk of long term events, likely related to the presence of underlying CAD.4 Stress echocardiography appears to be slightly superior in predicting postoperative cardiac events compared to nongated MPI with thallium. However, there is a lack of RCTs for such comparison. It should be noted that these do not address evaluation of patients scheduled for liver or kidney transplantation that has its own specific set of guidelines.
In ambulatory patients, exercise electrocardiography can provide useful information related to any underlying ischemia and functional status. This is at times combined with either echocardiography or MPI. However, in patients who have ECGs that limit interpretation (like LV hypertrophy, left bundle branch block, etc.), imaging with either echocardiography or MPI should be pursued. In patients having left bundle branch block who undergo exercise MPI, septal perfusion defects are seen, which are not related to CAD and decrease the specificity of the study.
Table 3: Assessment of functional capacitySeverity Assessment
Poor Unable to climb a flight of stairs (< 4 METs)
Moderate Climbing flight of stairs (4-7 METs)
Good Participation in moderate recreational activities (>7 METs)
Very Good Participation in strenuous sports, swimming (> 10 METs)
Table 4: Revised cardiac risk index variables2
Variables Pts
Hx of IHD 1
Hx of CHF 1
Hx of CVD 1
Insulin for diabetes 1
Serum creatinine >2.0 mg/dL 1
High-risk surgery 1
Table 5: Assessment of cardiac events in preoperative period based on RCRI pointsTotal RCRI points Risk of MI, cardiac arrest, or
death 30 days after surgery
0 0.4% (95% CI: 0.1-0.8)
1 1.0% (95% CI: 0.5-1.4)
2 2.4% (95% CI: 1.3-3.5)
≥3 5.4% (95% CI :2.8-7.9)
Table 6: Recommendations for non cardiac surgery in patients who have undergone coronary interventions Recommendations COR LOE
Elective noncardiac surgery should not be performed within 14 days of balloon angioplasty in patients in III Harm C
whom aspirin will need to be discontinued perioperatively.
Elective noncardiac surgery should not be performed within 30 days after BMS implantation or within III Harm B
6-12 months after DES implantation in patients in whom DAPT will need to be discontinued perioperatively.
Elective non cardiac surgery after DES implantation may be considered after 180 days if the risk of further IIb B
delay is greater than the expected risks of ischemia and stent thrombosis.

132 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
Hence, in such cases, pharmacological stress testing is preferred with adenosine, dipyridamole, or regadenoson. In patients with valvular heart disease or pulmonary hypertension, an echocardiographic stress test is preferred as it provides clinically important information.4
CORONARY ANGIOGRAPHY There is insufficient data to recommend routine use of coronary angiography preoperatively for noncardiac surgical procedures (excluding patients undergoing kidney or liver transplantation). There is also very little information regarding the significance of coronary computed tomographic (CT) angiography and calcium scoring due to limited data.9
Peri-operative Medical Therapy and Interventions-RecommendationsCoronary revascularizationPreoperative revascularization for noncardiac surgery is recommended only when it is indicated as per guidelines for acute coronary syndrome (ACS). Routine
coronary revascularization to reduce peri-operative cardiac events in noncardiac surgery is not recommended.10 There are no prospective RCTs supporting either coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI) to decrease intra-operative or postoperative cardiac events as part of peri-operative management for noncardiac surgery. However, patients with ACS prior to noncardiac surgery should be managed according to guideline-directed therapy for ACS. In those who are scheduled for time-sensitive noncardiac surgery, balloon angioplasty or bare-metal stent (BMS) placement is preferred for management.
Elective noncardiac surgery in patients with prior PCI—Timing and recommendationsNon cardiac surgery in the early period following BMS/DES implantation is problematic because withdrawal of antiplatelet drugs is associated with the risk of stent thrombosis, the highest risk of which occurs in the first 4 to
6 weeks after stent implantation.11,12 In case dual anitplatelet therapy (DAPT) has to be discontinued for urgent or emergent surgery, such a decision should be individualized, weighing the risk and benefit.
The recommendations for non cardiac surgery in patients who have undergone balloon angioplasty or stenting with BMS/DES are outlined in Table No 7.
If surgery is to be performed in BMS implantation before 30 days or DES implantation before 6-12 months, then the strategy for using antiplatelet drugs depends on the bleeding risk of the patient as outlined in Table 8.
In such subset of patients, the surgeon should be encouraged to operate on aspirin at least in patients with low or intermediate bleeding risk.
ANTICOAGULANT THERAPYIn patients undergoing surgery, the benefit of continuation of anticoagulants should be weighed against risk of bleeding procedure. Low bleeding risk surgeries, like, cataract surgery or minor dermatological surgeries, do not predispose to prolonged bleeding, and in such cases, anticoagulant therapy can be continued.13
There are no studies on the prevention of peri-operative myocardial ischemia or MI by anticoagulants in peri-operative period for noncardiac surgeries. Depending on the location of the prosthetic valve along with associated risk factors for thromboembolism (which include the presence of atrial fibrillation (AF), previous thromboembolism, LV dysfunction, hypercoagulable condition,
Table 8: Peri-operative beta blocker therapyRecommendations COR LOEbB should be continued in patients undergoing surgery who have been on it chronically. I BSRIt is reasonable for the management of bB after surgery to be guided by clinical circumstances, independent IIa BSRof when the agent was started. In patients with intermediate –or high-risk myocardial ischemia noted in preoperative risk stratification tests, IIb CSRit may be reasonable to begin peri-operative bB. In patients with 3 or more RCRI risk factors (.e.g diabetes mellitus, HF, CAD, renal insufficiency, IIb BSR cerebrovascular accident), it may be reasonable to begin bB before surgery. In patients with a compelling long-term indication for beta blocker therapy but no other RCRI risk factors, IIb BSRinitiating beta blockers in the periopreative setting as an approach to reduce periopreative risk is of uncertain benefit. In patients in whom beta-blocker therapy is initiated, it may be reasonable to begin peri-operative beta blockers IIb BSRlong enough in advance to assess safety and tolerability, preferably more than 1 day before surgery. bB therapy should not be started on the day of surgery. III BSR
Table 7 : Use of antiplatelet drugs in patients requiring early surgery after coronary intervention.
BLEEDING RISK
Low Intermediate HighCataract, Oral GI Surgeries, Intracranial, Prostate, aortic ENT,dental surgery Cholecystectomy, Posterior segment surgery Appendicetomy etc.
Continue aspirin Stop clopidogrel Stop aspirin and and clopidogrel and clopidogrel continue aspirin and bridge with cangrelor: 0.75 mg/kg/min or tirofiban: 0.1 mg/kg min. If renal dys- function, decrease dose to 0.05 mg/ kg and start 24-48 hrs. after last dose and
continue till 4-8 hrs. before surgery
REVIEW ARTICLE

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 133
or older generation prosthetic aortic valve), patients on vitamin K antagonist (VKA) may or may not require bridging with either unfractionated heparin or low molecular-weight heparin.
In patient having a mechanical mitral valve, bridging anticoagulation is appropriate with interruption of anticoagulation in peri-operative period regardless of the presence or absence of risk factors of thromboembolism. Same is true for patients with mechanical aortic valve with one or more risk factors of thromboembolism.13
Bridging anticoagulation is recommended in the time period when then international normalized ratio (INR) is subtherapeutic preoperatively.
Patients with atrial fibrillation (AF) who are managed with VKA therapy and are at low risk of thromboembolism (CHA2DS2-VASc score of 0 to 1) or those who are back to normal sinus rhythm, undergoing surgery with increased risk of bleeding, holding VKA therapy for 1 week to allow normalization of INR without bridging anticoagulation is acceptable. VKA therapy is then resumed once homeostasis is achieved.14,15
In patients who have high risk of thromboembolism (prior strokes, mechanical valves, CHA2DS2-VASc score >2), bridging anticoagulation is preferred once VKA therapy is withheld and INR is subtherapeutic.
DIRECT ORAL ANTICOAGULANTS In patients on direct thrombin inhibitors (e.g., dabigatran) undergoing noncardiac surgery with normal renal function, anticoagulation can be discontinued 48 to 72 hours before the procedure. In those with mildly impaired renal function (with creatinine clearance of 50-80 mL/min), this can be withheld 4 to 5 days prior to procedure. Longer duration may be required in case of severe renal insufficiency (creatinine clearance of <50 mL/min).16
For patients on oral direct factor Xa inhibitors having normal renal function undergoing elective procedures, anticoagulation can be stopped 48 hours prior to the scheduled noncardiac elective surgery. Prolonged discontinuation can be exercised in patients with high risk of
bleeding or with mild renal insufficiency (creatinine clearance 50-80 mL/min).
Due to the rapid offset and onset, bridging anticoagulation is not required in patients on newer oral anticoagulants. This is reserved only for patients with a very high risk of postoperative thromboembolism and requires extended interruption of such as in cases where oral diet is restricted for some time (e.g., intestinal surgeries). It should be resumed when homeostasis is achieved. Caution should be exercised in patients with high risk of bleeding as onset of action is rapid (within 2-3 hours). Resuming dabigatran can be delayed in patients with high risk of bleeding or it can be administered in a lower dose for the first 2 to 3 days.
Activated partial thromboplastin time for dabigatran can be monitored; levels close to control levels suggest a low serum concentration of these agents.
REVERSAL OF VKASIn case emergent reversal of anticoagulation is required for VKA, vitamin K is not recommended because the effect is not predictable and not immediate. This can even delay the return to therapeutic level of anticoagulation when VKAs are restarted.
Fresh frozen plasma or prothombin complex concentrates are recommended in patients with mechanical prosthetic valves receiving VKA therapy where homeostasis has to maintained in case of uncontrollable bleeding or in a patient requiring emergent noncardiac surgery.13
b-blocker therapyThe use of beta blocker (bB) in peri-operative period17 is outlined in Table 9.
Statin therapy Peri-operative statins therapy for noncardiac surgery should be continued in patients taking them. It is also reasonable to initiate statin therapy in those going for vascular surgery. Statins may also be considered in patients scheduled for elevated risk procedure who have clinical indications for initiation of statin therapy.18
Alpha-2 agonist Alpha-2 agonists are not useful in
prevention of cardiac events in peri-operative period.
Calcium channel blockersThere is limited data on the efficacy of calcium channel blockers in peri-operative therapy for patients undergoing noncardiac surgery. Most of the benefits shown are attributed to diltiazem. There was no decrease in the incidence of myocardial ischemia with the use of dihydropyridines and verapamil. It should be kept in mind that verapamil and diltiazem can worsen and even precipitate HF in patients with decreased ejection fraction (EF) and/or clinical HF. More studies are needed to make specific recommendations regarding peri-operative use of calcium channel blockers.
Angiotensin-Converting Enzyme InhibitorsIt is reasonable to continue angiotensin-converting enzyme (ACE) inhibitors or angiotensin blockers (ARBs) perioperatively. If they are held before, it is reasonable to restart as soon as possible postoperatively.19
Intravenous nitroglycerinUse of intravenous nitroglycerin prophylactically to prevent myocardial ischemia has shown to be ineffective in patients undergoing noncardiac surgery.
PREOPERATIVE EVALUATION IN SPECIFIC PATIENT POPULATION-GENERAL CONSIDERATIONSAge Age plays an important role in determining MACE as there is an increased prevalence of cerebrovascular disease, diabetes mellitus, and other medical condition as age increase.
Coronary artery diseaseCardiac morbidity during and/ or after noncardiac surgery depends on how it is defined. These can just be elevation in cardiac biomarkers alone or may involve typical symptoms and signs of ischemia. There is an association of prior cardiovascular (CAD) events with MACE after noncardiac surgery.20

134 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
A study by Livhits, et al., showed that the rate of postoperative MI decreased significantly with increase in time from prior MI and date of procedure. It also showed an improved 30-day mortality. This suggests that a noncardiac surgery should be performed after at least 2 months of MI in the absence of coronary intervention. Risk of MACE depends on the type of coronary intervention at the time of MI prior to surgery. A recent MI (occurring within 6 months of noncardiac surgery) is also an independent risk factor of peri-operative stroke, associated with an increase in peri-operative mortality of 8-fold.
Heart failureActive HF or patients with history of HF are at a higher risk of peri-operative complications, based on data from many studies. One such study involved population-based data analysis of 38047 patients. This study showed that compared with 30-day postoperative mortality rate in patients with CAD (2.9%) risk was higher in patients with non ischemic HF (9.3%) and ischemic HF (9.2%) An LVEF <35% in the absence of symptoms, itself is an independent risk factor for peri-operative morbidity and mortality in patients undergoing elevated-risk noncardiac surgery.21 Studies in patients having symptomatic diastolic dysfunction, with and without systolic dysfunction, has also been shown to be associated with higher incidence rate of MACE, high rates of postoperative HF, and prolonged length of hospital stay.
Peri-operative arrhythmiasIt is important to seek underlying cause of any arrhythmia that occurs in the peri-operative period as it can be precipitated by underlying cardiopulmonary disease, ischemia, drug toxicity, metabolic derangements, etc. These can alter outcomes in patients undergoing noncardiac surgery. Specific recommendations related to peri-operative arrhythmias cannot be provided due to the limited number of studies to determine surgical risk in such cases. Few studies have shown supraventricular and ventricular arrhythmias to have low risk of peri-operative cardiac events. There is no
increase in cardiac complications or any increased risk of nonfatal MI or cardiac death in patients seen to have frequent ventricular premature beats, couplets or nonsustained ventricular tachycardia, and couplets in peri-operative period for noncardiac surgery.22,23 Patients who develop such arrhythmias may require referral to a cardiologist for further evaluation. Atrial fibrillation (AF) is very common, especially in older patients. Patients with preoperative AF who are asymptomatic and stable do not require any changes in their medical management, apart from adjustment of anticoagulation, in the peri-operative period. There is potential, however, of peri-operative formation of left atrial thrombus in patients with persistent AF, undergoing thoracic surgeries or other noncardiac surgeries involving physical manipulation of the heart.
CONCLUSIONClearing a cardiac patient for non-cardiac surgery is a common issue in our day to practice. Cardiovascular complications like heart failure and acute coronary syndrome are the commonest cause of death in first 48 hours while mortality from 48 hours to 6 weeks is usually due to a non-cardiac complication like pneumonia, sepsis, pulmonary embolism, renal failure etc. A careful evaluation of the patient taking into consideration the procedure related risk, the patient related risk and functional capacity coupled with use of appropriate drugs and necessary precautions paves the way for minimizing cardiovascular morbidity and mortality in the peri-operative period and also shorten the hospital stay.
REFERENCES1. Lee TH, Marcantonio ER, Mangione CM, et al. Derivation
and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999;100:1043–9.
2. Weiser TG, Regenbogen SE, Thompson KD, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet 2008;372:139–44.
3. Bakker EJ, Ravensbergen NJ, Poldermans D. peri-operative cardiac evaluation, monitoring, and risk reduction strategies in noncardiac surgery patients. Curr Opin Crit Care 2011;17:409–15.
4. Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHA guideline on peri-operative cardiovascular evaluation and management of patients under-going noncardiac surgery: a report of the American College of Cardiology/ American Heart Association Task Force on practice guidelines. J Am Coll Cardiol 2014;64:e77–137.
5. Ford MK, Beattie WS, Wijeysundera DN. Systematic review: prediction of peri- operative cardiac complications and mortality by the revised cardiac risk index. Ann Intern Med 2010;152:26–35.
6. Rohde LE, Polanczyk CA, Goldman L, Cook EF, Lee RT, Lee TH. Usefulness of transthoracic echocardiography as a tool for risk stratification of patients undergoing major noncardiac surgery. Am J Cardiol 2001;87:505–9.
7. Eagle K A, Coley CM, Newell JB, et al. Combining clinical and thallium data optimizes preoperative assessment of cardiac risk before major vascular surgery. Ann Intern Med 1989;110:859–66.
8. Das MK, Pellikka PA, Mahoney DW, et al. Assessment of cardiac risk before nonvascular surgery: dobutamine stress echocardiography in 530 patients. J Am Coll Cardiol 2000;35:1647–53.
9. Ahn JH, Park JR, Min JH, et al. Risk stratification using computed tomography coronar y angiography in patients undergoing intermediate-risk noncardiac surgery. J Am Coll Cardiol 2013;61:661–8.
10. McFalls EO, Ward HB, Moritz TE, et al. Coronary-artery revascularization before elective major vascular surgery. N Engl J Med 2004;351:2795–804.
11. Kaluza GL, Joseph J, Lee JR, Raizner ME, Raizner AE. Catastrophic outcomes of noncardiac surgery soon after coronary stenting. J Am Coll Cardiol 2000;35:1288–94.
12. Tokushige A, Shiomi H, Morimoto T, et al. Incidence and outcome of surgical procedures after coronary bare-metal and drug-eluting stent implantation: a report from the CREDO-Kyoto PCI/CABG registry cohort-2. Circ Cardiovasc Interv 2012;5:237–46.
13. Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:e57–185.
14. January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation 2014;130:e199–267.
15. Douketis JD, Spyropoulos AC, Kaatz S, et al. peri-operative Bridging Anticoagulation in Patients with Atrial Fibrillation. N Engl J Med 2015;373:823–33.
16. Schulman S, Carrier M, Lee AY, et al. peri-operative Management of Dabigatran: A Prospective Cohort Study. Circulation 2015;132:167–73.
17. Wijeysundera DN, Duncan D, Nkonde-Price C, et al. peri-operative beta blockade in noncardiac surgery: a systematic review for the 2014 ACC/AHA guideline on peri-operative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol 2014;64:2406–25.
18. Lindenauer PK, Pekow P, Wang K, Gutierrez B, Benjamin EM. Lipid-lowering therapy and in-hospital mortality following major noncardiac surgery. JAMA 2004;291:2092–9.
19. Rosenman DJ, McDonald FS, Ebbert JO, Erwin PJ, LaBella M, Montori V M. Clinical consequences of withholding versus administering renin-angiotensin- aldosterone system antagonists in the preoperative period. J Hosp Med 2008; 3:319–25.
20. Livhits M, Ko CY, Leonardi MJ, Zingmond DS, Gibbons MM, de Virgilio C. Risk of surgery following recent myocardial infarction. Ann Surg 2011;253: 857–64.
21. Healy KO, Waksmonski CA, Altman RK, Stetson PD, Reyentovich A, Maurer MS. peri-operative outcome and long-term mortality for heart failure patients undergoing intermediate- and high-risk noncardiac surgery: impact of left ventricular ejection fraction. Congest Heart Fail 2010;16:45–9.
22. Mahla E, Rotman B, Rehak P, et al. peri-operative ventricular dysrhythmias in patients with structural heart disease undergoing noncardiac surgery. Anesth Analg 1998;86:16–21.
23. O’Kelly B, Browner WS, Massie B, Tubau J, Ngo L, Mangano DT. Ventricular arrhythmias in patients undergoing noncardiac surgery. The Study of peri-operative Ischemia Research Group. JAMA 1992;268:217–21.
REVIEW ARTICLE

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 135
T Wave Inversion
ECG OF THE MONTH
SR MITTAL
AbstractT wave inversion can be primary or secondary. T wave inversion without any associated QRS changes are called primary. T wave inversion secondary to depolarization abnormalities (QRS changes) are called secondary. Primary T wave inversion can be as benign as persistent juvenile pattern or early repolarization variant. Anxiety, hyperventilation, meals and upright posture can produce transient benign T wave inversions. Acute abdominal disorders, hypothyroidism, hypokalemia and cerebrovascular accidents can produce T wave inversion even in persons without history or clinical signs of heart disease. Transmural or nontransmural myocardial infarction are common cause of deep symmetrical T wave inversion. Biphasic or inverted T waves in leads V1 to V4 in a case of angina suggests tight occlusion of proximal left anterior descending coronary artery. Common cardiac causes of T wave inversion include mitral valve prolapse, recent Stokes-Adams attack, post-tachycardia T wave inversion, pericardial constriction and cardiomyopathies.
Keywords z acute abdomen z cardiomyopathy z cerebrovascular accidents z coronary artery disease z electrocardiography z pericardial diseases z T wave
INVERTED T WAVES[A] NORMAL VARIANTS(a) Persistent Juvenile PatternT wave inversion in right precordial leads is common in children but in some persons it may persist in adulthood. It is more common in women. T wave is inverted in leads V1 to V4 (Figure 1). T wave depth usually decreases from V1 to V4.
(b) AnxietyChanges may normalize on exercise.
Dr. SR Mittal is Head, Department of Cardiology at Mittal Hospital and Research Centre, Ajmer, Rajasthan
(c) Hyperventilation Changes may normalise on exercise. (d) Orthostatic Variation T wave is inverted on assumption of upright posture. It usually affects inferior leads. it is common in asthenic individuals.
(e) Post Prandial
(f) Pregnancy

136 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
(g) Idiopathic Global T Wave Inversion
Global T wave inversion means inversion of T wave in all the standard leads
except lead aVR. This may occur in several conditions including myocardial ischemia, CNS disorders, myocarditis, apical hypertrophic cardiomyopathy, cardiac tumors and pheochromyocytoma. It is called idiopathic when no cause is
detected even on detailed evaluation. It is common in females.1,2 Such T wave changes without any underlying disease per se do not imply a poor prognosis.
(h) Early repolarization variant Prominent, biphasic T wave inversion with ST segment elevation (Figure 2) is seen in leads V1 to V4.
3 It is usually seen in athletes. Exercise normalizes T wave inversion.
[B] NON CARDIAC CAUSES (a) Acute Abdominal Disorders Pancreatitis (Figure 3), Cholecystitis (Figure 4), Peritonitis.
(b) Endocrine Disorders(i) HypothyroidismThere is generalized diminution of amplitude or shallow inversion of T wave. Sinus bradycardia and low voltage QRS are other findings.
(ii) Hypoadrenalism (iii) Hypopituitarism (iv) Pheochromocytoma
(c) Electrolyte Abnormalities HypokalemiaFlattening or inversion of T wave is associated with ST segment depression, increased prominence of ‘u’ wave and prolongation of QTc interval
Figure 1. Electrocardiogram from a case of persistent juvenile pattern showing T wave inversion (arrows) in leads V1 to V4.
Figre 2. Electrocardiogram from a case of early repolarization variant showing mild ST segment elevation with shallow T wave inversion (arrows) in leads V3 to V5.
Figure 3. Electrocardiogram from a case of acute pancreatitis showing T wave inversion (arrows) in leads I, aVL, V3 to V6.
Figure 4. Electrocardiogram from a case of acute cholecystitis showing shallow T wave inversion in leads V3 to V5 (arrows).
Figure 5. Electrocardiogram from a case of hypokalemia showing T wave inversions (arrows), prominent U wave (*) and prolonged QTc.
ECG OF THE MONTH

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 137
(Figure 5). Concomitant hypomagne-semia also affects the ECG. Therefore, ECG findings, therefore, may not exactly correlate with serum potassium levels.
(d) Acute Pulmonary EmbolismT wave is inverted in leads III, aVF and V1 to V4. Right bundle branch block may be present.
(e) Cerebrovascular InjuryStroke4,5, intracranial bleed6 and subarachnoid hemorrhage 7 are associated with electrocardiographic changes even in those patients who have no history or
clinical signs of primary heart disease. Widening and inversion of T waves in precordial leads is accompanied by QTc prolongation and brandycardia. Exact mechanism is not clear.
Autonomic neural stimulation from the hypothalamus or elevated levels of catecholamines could be responsible for the ECG changes.
(f) Following Truncal Vagotomy, Radical Neck Dissection and Bilateral Carotid Endarterectomy8
[C] CARDIAC CAUSES (a) Myocardial Infarction (i) Evolved phase of transmural infarc-
tion. Terminal portion of the T wave is the
first to become inverted followed by the middle and initial portion (Figure 6).9 T waves may be very deep (Figure 7) but may decrease or even normalize with time.1 Opposite leads may show prominent T wave 1. Negative T wave in leads II, III and aVF may produce prominent T wave in leads I and aVL and vice versa. Failure of reperfusion
Figure 6. Electrocardiogram from a case of anterior myocardial infarction showing initial inversion of terminal part of T wave.
Figure 7. Electrocardiogram from a case of evolved anterior myocardial infarction.
Figure 9. Electrocardiogram from a case of non ST elevation inferior myocardial infarction showing symmetrical T wave inversion in leads III.
Figure 8. Electrocardiogram from a case of non ST elevation anterior myocardial infarction showing shallow symmetrical T wave inversion in leads aVL, V3 to V6 (ar-rows).
Figure 10. Electrocardiogram showing inverted T waves in leads V1 to V4 without Q wave or ST elevation (Wellens’ sign)

138 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
ECG OF THE MONTH
Figure 11. Electrocardiogram showing T wave inversion in lead aVL with reciprocal prominent T waves in leads II, III, aVF.
Figure 12. Electrocardiogram from a case of mitral valve prolapse showing T wave inversion in leads II, III, aVF and V3 to V6.
Figure 13. Electrocardiogram from a case of complete A-V block with history of Stokes-Adams attack showing deep T wave inversion in lead V4.
In patients with chronic stable an-gina, it may predict clinically signifi-cant mid LAD lesion.12,13
(b) Mitral valve prolapse.T wave may show shallow inversion in leads II, III, aVF, V5 and V6 (Figure 12).
(c) Following a Recent Stokes- Adams AttackT wave is broad. QTc is prolonged (Figure 13). There is high degree atrio-ventricular block.
(d) Post- tachycardia T wave Inversion ST segment depression may be associated with T wave inversion following reversal of supraventricular or ventricular tachycardia (Figure 14). Changes may persist for hours to days.
(e) Rate Dependent T wave inversion Tachycardia dependent T wave inversion (Figure 15) may be seen in presence of myocardial ischemia. Bradycardia dependent T wave inversion (Figure 16). may be seen in setting of prolonged QT syndrome.
(f) Pericardial Effusion/ constrictionDiffuse low voltage or shallow inversion of T wave is associated with low voltage QRS complex (Figure 17). There are no reciprocal changes. Depth of inversion of T wave correlates with the degree of peri-cardial adherence to the myocardium and underlying myocardial damage.
(g) Hypertrophic CardiomyopathyTall QRS are accompanied by diffuse deep T wave inversion14 (Figure 18, 19). Normal QRS with diffuse unexplained T wave inversion should also raise suspicion of hypertrophic cardiomyopathy. (h) Other Cardiomyopathies and MyocarditisST depression and T wave inversion are common in leads V4 to V6 (Figure 20). Abnormal Q waves, slow progression or non progression of r wave and deep S wave in leads V2 and V3 can be other find-ings.
may result in failure of inversion of T wave.
(ii) Subendocardial infarction (Non ST elevation acute coronary syndrome).
T wave inversion is usually symmetric but is usually not deep.
(iii) Wellens sign In a case of acute coronary syndrome,
biphasic or inverted T waves in leads V1 to V4 without Q wave or significant ST segment elevation (Figure 10) suggest tight occlusion of proximal left anterior descending coronary artery.10,11 Precordial R wave progression may be normal.
(iv) T wave inversion in aVL (Figure 11).

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 139
Figure 14. Electrocardiogram during supraventricular tachycardia (A) and after conversion to sinus rhythm (B) showing post tachycardia T wave inversion.
Figure 15. Electrocardiogram from a case of Wenkebach A-V block showing T wave inversion following short R-R cycle in lead V3 (arrow).
Figure 16. Electrocardiogram from a case of atrial fibrillation with right bundle branch block showing T wave inversion in cycles following longer pause (arrow).
Figure 17. Electrocardiogram from a case of pericardial constriction showing low QRS voltage and diffuse shallow T wave inversion.
Figure 18. Electrocardiogram from a case of hypertrophic cardiomyopathy showing tall QRS with diffuse deep T wave inversion.
Figure 19. Electrocardiogram from another case of hypertrophic cardiomyopathy showing tall QRS with diffuse deep T wave inversion.
(i) Arrhythmogenic Right Ventricular CardiomyopathyT wave inversion is common in leads V1 and V2.
(j) Myocardial Tumors
(k) Secondary T wave Abnormalities
Intraventricular conduction defects like fascicular blocks, bundle branch block (Figure 21), pre-excitation, ventricular ectopics, paced beats and ventricular hypertrophy (Figure 22) are associated with down sloping ST segment
depression with T wave inversion. These changes are secondary to depolarization abnormalities. In the context of left ventricular hypertrophy, these changes suggest increased cardiovascular risk.15,16 T wave is directed away from later portion of the QRS complex. In these conditions, if the direction of T wave is similar to

140 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
Figure 20. Electrocardiogram from a case of congestive cardiomyopathy showing diffuse T wave inversion, non-progression of r in leads V1 to V4 and deep S waves in leads V2 and V3.
Figure 21. Electrocardiogram from a case of left bundle branch block showing secondary T wave inversion in leads I, aVL, V5 and V6.
Figure 22. Electrocardiogram from a case of left ventricular hypertrophy showing secondary T wave inversion in leads III, aVF, V4 to V6.
the terminal part of QRS, it is abnormal and suggests myocardial disease. If the intraventricular conduction, defect is intermittent, T wave changes may persist for hours or days after normalization of ventricular depolarization. Such changes have been termed as “Memory T wave” changes.8,17,18
REFERENCES1. De Luna B, Goldwasser D, Fid M, Bayes Genis A. Surface
electrocardiography. In Fuster V, Walsh RA, Harrington RA (eds) Hurst’s The Heart. Mc Graw Hill, New York; 2011:307-70.
2. Walder LA, Spodick DH et al. Global T wave inversion. Long term follow up. J Am Coll Cardiol 1993;21:1652.
3. Uberoi A, Jain N, Froelicher V et al. Early repolarization in an ambulatory clinical population. Circulation 2011; 124:2208-14.
4. Togha M, Sharifpour A, Ashraf H et al. Electrocardio-graphic abnormalities in acute cerebrovascular events in patient with / without cardiovascular disease. Ann Indian Acad Neurol 2013;16:66–71.
5. Murthy SB. Shah S, Venkatasubba Rao CP, et al. Clinical characteristics of myocardial stunning in acute stroke. J Clin Neurosci 2014;21:1279-52.
6. Qaga AY, Suleiman A, Alsumrain M et al. Electrocardio-graphic abnormalities in patients presenting with intrac-ranial parenchymal hemorrhage. Acta Cardiol 2012;67: 635-9.
7. Chatterjee S. ECG changes in subarachnoid hemorrhage: A Synoposis. Neth Heart J 2011;19:31-4.
8. Mirvis DM, Goldberger AL. Electrocardiography. In Mann DL, Zipes DP, Libby P, Bonow RO (eds). Braunwald’s Heart Disease. Elsevier, Philadelphia; 2015:114-52.
9. Wagner GS, Lim TH. Myocardial infarction. In Wagner GS(ed). Marriott’s Practical Electrocardiography, Wolters Kluwer, Philadelphia; 2001:178-207.
10. De Zwaan C, Bar FW, Wellens HJ. Characteristic electro-cardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients ad-mitted because of impending myocardial infarction. Am Heart J 1982;103:730-6.
11. Htut Oo SZMW, Khalighi K, Kodali A, May C, Aung TT, Snyder R. Ominous T wave inversions: Wellens’ syndrome revisited. J Community Hosp Intern Med Perspect 2016; 6 : 10.3402/Jchimp. V6.32011.
12. Farhan HL, Hassan KS, Al Belushi A, et al. Diagnostic val-ue of electrocardiographic T wave inversion in lead aVL in diagnosing coronary artery disease in patients with chronic stable angina. Oman Med J 2010;25:124-7.
13. Hassen GW1, Costea A2, Smith T et al. The neglected lead on electrocardiogram: T wave inversion in lead aVL,
nonspecific finding or a sign for left anterior descending artery lesion ? J Emerg Med 2014;46:165-70.
14. Levis J. ECG Diagnosis : Apical hypertrophic cardiomyo-pathy. Perm J 2013;17:84.
15. Larsen CT, Dahlin J, Blackburn H, et al. Prevalence and prognosis of electrocardiographic left ventricular hyper-trophy, ST segment depression and negative T wave. The Copenhagen city heart study. Eur Heart J 2002;23:315-24.
16. Okin PM, Devereux RB, Nieminen MS. Electrocardio-graphic strain pattern and prediction of cardiovascular morbidity and mortality in hypertensive patients. Hyper-tension 2004;44:48-54.
17. Kernohan RJ. Post – paroxysmal tachycardia syndrome. Br Heart J 1969;31:803-6.
18. Kolb JC. Cardiac memory – persistent T wave changes after ventricular pacing. J Emerg Med 2002;23:191-7.
ECG OF THE MONTH

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 141
Q1. In children T waves may be normally inverted in leads
(A) I, aVL(B) V5, V6 (C) V1 to V4(D) V7 to V9
Q2. Transient non-ischemic T wave inversion can occur during
(A) Anxiety (B) Hyperventilation (C) Assumption of upright posture(D) All
Q3. Non-ischemic T wave inversion can be seen in
(A) Post-prandial period(B) Pregnancy (C) Exercise (D) Fasting
Q4. Global T wave inversion can be seen in
(A) Cerebrovascular accidents (B) Cardiac tumors(C) Pheochromocytoma (D) None
Q5. Global T wave inversion is not seen in
(A) Myocardial ischemia (B) Myocarditis (C) Dilated cardiomyopathy (D) Left bundle branch block
Q6. Early repolarization variant produces changes in leads
(A) II, III, aVF (B) V5 & V6 (C) V2 to V4(D) V7 to V9
Q7. Early repolarization variant produces
(A) ST segment elevation (B) Biphasic T waves(C) Deep symmetrical T wave
inversion (D) Q waves
MCQsQ15. Acute pulmonary embolism
produces T wave inversion in leads
(A) III, aVF(B) V1 to V4(C) I & aVL(D) V5 & V6 Q16. T wave inversion can be seen in (A) Stroke (B) Intracranial bleed(C) Subarachnoid hemorrhage (D) Subdural hematoma
Q17. Hypothalamic bleed can produce (A) Widening of T wave (B) QTc prolongation (C) Tachycardia (D) All
Q18. Which of the following can produce T wave inversion
(A) Truncal vagotomy (B) Radical neck dissection (C) Bilateral carotid endarterectomy (D) None
Q19. In ST elevation myocardial infarction, which portion of T wave is the first to become inverted
(A) Initial (B) Middle (C) Terminal
Q20. In a case of acute coronary syndrome inverted T waves in leads V1 to V4 suggests tight occlusion of proximal
(A) LAD(B) LCX(C) RCA(D) Left main coronary artery
Q21. In a case of ST elevation myocardial infarction, T wave inversion suggest
(A) Successful reperfusion (B) Failure of reperfusion (C) Ongoing ischemia (D) Infarction in opposite leads
Q8. Exercise can normalize T wave inversion produced by
(A) Anxiety (B) Hyperventilation (C) Early repolarization variant(D) Myocardial ischemia
Q9. Which of the following conditions can produce T wave inversion
(A) Acute pancreatitis (B) Cholelithiasis (C) Renal colic (D) Nephrotic syndrome
Q10. Which of the following conditions can produce T wave inversion
(A) Acute cholecystitis (B) Acute peritonitis (C) Hyperthyroidism (D) Acute gastritis
Q11. Low voltage QRS, sinus bradycardia and generalized diminution of T waves suggests
(A) Cardiac tamponade (B) Cor-pulmonale (C) Myxoedema (D) All
Q12. T wave inversion with prolongation of QTc interval is seen in
(A) Hypokalemia (B) Cerebrovascular injury (C) Recent Stokes-Adams attack(D) All
Q13. T wave inversion is seen in (A) Hyperkalemia (B) Hypomagnesemia (C) Hypocalcemia (D) Hyponatremia
Q14. Hypokalemia produces (A) Flattening of T wave (B) ST segment depression (C) Prominence of U wave (D) Shortening of QTc interval
T Wave Inversion

142 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018
PICTORIAL CME
Answers:(1) C, (2) D, (3) A, B (4) A, B, C (5) D, (6) C, (7) A, B, (8) A, B, C, (9) A, (10) A, B, (11) C, (12) D, (13) B, (14) A, B, C, (15)A, B, (16) A, B, C, (17) A, B, (18) A, B, C, (19) C, (20) A, (21) A, (22) B, (23) B, D, (24) C, (25) A, (26) A, B, (27) A, (28) A, (29) A, B, C, (30) A, (31) B, (32) C. Q22. In patients with chronic stable
angina, T inversion in lead aVL suggest occlusion of
(A) Proximal LAD(B) Mid LAD (C) Proximal D1(D) Proximal major obtuse marginal
Q23. Mitral valve prolapse can produce T wave inversion in leads
(A) I and aVL(B) II, III and aVF(C) V1 to V3(D) V5, V6
Q24. Broad inverted T waves, QTc prolongation and high degree A-V block suggest
(A) Severe hypokalemia (B) Hypothalamic bleed(C) Recent Stokes- Adam’s attack (D) Severe hypothyroidism
Q25. Post tachycardia T wave inversion suggests
(A) Non specific change(B) Myocardial ischemia(C) Myocardial infarction (D) Electrolyte imbalance
Q26. Combination of sinus tachycardia, low voltage QRS and diffuse shallow T wave inversion should suggest
(A) Gross pericardial effusion (B) Pericardial constriction (C) Myxoedema (D) Cor pulmonale
Q27. Combination of tall QRS, horizontal ST segment, diffuse deep T wave inversion, absence of Q wave and any sequential change on repeated ECG should suggest
(A) Hypertrophic cardiomyopathy (B) Myocardial infarction (C) Myocarditis (D) Cardiomyopathy
Q28. Arrhythmogenic right ventricular dysplasia produces T wave inversion in leads
(A) V1, V2 (B) V5, V6(C) I, aVL (D) II, III, aVF
Q29. Secondary T wave abnormalities are seen in
(A) Fascicular blocks(B) Pre-excitation (C) Paced beats (D) None
Q30. In secondary T wave abnormalities, T wave are directed
(A) Away from later portion of QRS(B) Towards the later portion of QRS(C) Away from the initial portion of
QRS (D) Towards the initial portion of QRS
Q31. Secondary T wave directed towards later portion of QRS suggests
(A) Non specific change (B) Myocardial damage (C) Early repolarization (D) Electrolyte imbalance
Q32. Persistent T wave inversion after recovery from transient paced rhythm suggests
(A) Myocardial ischemia (B) Myocardial infarction (C) Memory T wave(D) Hypokalemia
ECG OF THE MONTH

Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018 143
PICTORIAL CME
MONIKA MAHESHWARI
Dr. Monika Maheshwari is Professor at Jawahar Lal Nehru Medical College, Ajmer, Rajasthan
Giant Ramus Artery
Congenital coronary anomalies are rare. Recently one such case of giant ramus artery was encountered by us (Figure 1, 2) and is picturised herein mimicking double left anterior descend-ing coronary artery.
Figure 1: Left Coronary Angiogram (RAO: 29.7° Caudal: 27.6° view) showing giant ramus artery simulating double left anterior descending coronary artery.
Figure 2. Left Coronary Angiogram (RAO: 2.1° Caudal: 28.8° view) showing giant ramus artery

144 Cardiology Today VOL. XXII NO. 4 JULY-AUGUST 2018