Embed Size (px)
Citation preview

2/27/2017
1
Cardiorenal Syndrome:
Critical Link Between Heart and Kidney
Chris M. Bell, ACNP
Cardiology Associates of North Mississippi
Objectives
• Review the 5 Subtypes of the Cardiorenal Syndrome (CRS)
• Discuss the epidemiology and discriminating features of the CRS
• Assist in helping to understand the complexity of physiological, biochemical and neurohormonal derangements that complicate patient care
• Discuss treatment considerations in clinical management

2/27/2017
2
Heart Failure Hits Home
ACC/AHA Guidelines: Management of Fluid Status
• Patients should not be discharged from the hospital until a stable and effective diuretic regimen is established, and ideally, not until euvolemiais achieved
• Patients who are sent home before these goals are reached are at high risk of recurrence of fluid retention and early readmission because unresolved edema may itself attenuate the response to diuretics
• 2009 Focused Update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: J Am Coll Cardiol. 2009;53(15):1343-1382. doi:10.1016/j.jacc.2008.11.009
The dilemma – we know what needs to be achieved but we have not been able to accomplish the desired outcome with any consistency or sustainability in many acutely decompensated heart failure patients
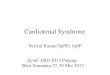
Inadequate Diuresis During ADHF Treatment
(Adhere Registry)
Note: For the chart, n represents the number of patients who have both baseline and discharge weight, and the percentage is calculated based on the total patients in the corresponding population. Patients without baseline or discharge weight are omitted from the histogram calculations.
ADHERE® Database
TheNation
=26,757, 68%
Change in Weight From Admission to Discharge
7% 6%
13%
24%
30%
15%
3% 2%
0
10
20
30
40
50
En
rolled
Dis
ch
arg
es (
%)
(<-20) (-20 to -15) (-15 to -10) (-10 to -5) (-5 to 0) (0 to 5) (5 to 10) (>10)
Change in Weight (lb)

2/27/2017
3
Renal Disease Affects Readmissions and Mortality
• Majority (71%) of CHF patients with SCr >2.5 mg/dL (10% of CHF patients) will be readmitted within 6 months1
• Concurrent renal disease, seen in 6.5% of acute CHF patients in a Canadian study, is a significant independent predictor of 30-day and 1-year mortality2
1. Krumholz et al. Am Heart J. 2000;139:72.2. Jong et al. Arch Intern Med. 2002;162:1689.
Impact of Renal Function on Survival in HF Ibopamine Trial n=1906
Hillege et al. Circ. 2000; 102:203-210
Definitions • Cardiorenal Syndrome (CRS)
– A condition in which there is dysfunction of both the cardiac and renal function
• Seen in heart failure patients who have renal dysfunction
• Seen in renal patients that develop cardiac dysfunction
– Risk Factors that increase chances for both• HTN, Diabetes, Atherosclerosis

2/27/2017
4
Schematic Overload
Schematic Overload with more Arrows
CRS Classifications
• Type 1 CRS reflects an abrupt worsening of cardiac function (e.g. acute cardiogenic shock or decompensated congestive heart failure) leading to acute kidney injury.
• Type 2 CRS describes chronic abnormalities in cardiac function (e.g. chronic congestive heart failure) causing progressive and permanent chronic kidney disease.
• Type 3 CRS consists in an abrupt worsening of renal function (e.g. acute kidney ischemia or glomerulonephritis) causing acute cardiac disorder (e.g. heart failure, arrhythmia, ischemia).
• Type 4 CRS describes a state of chronic kidney disease (e.g. chronic glomerulardisease) contributing to decreased cardiac function, cardiac hypertrophy and/ or increased risk of adverse cardiovascular events.
• Type 5 CRS reflects a systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal dysfunction.
Ronco C. Cardiorenal syndromes: definition and classification. Contrib
Nephrol. 2010;164:33–38. Epub 2010
Apr 20

2/27/2017
5
• Type 1 CRS reflects an abrupt worsening of cardiac function (e.g. acute cardiogenic shock or decompensated congestive heart failure) leading to acute kidney injury.
• Type 2 CRS describes chronic abnormalities in cardiac function (e.g. chronic congestive heart failure) causing progressive and permanent chronic kidney disease.
• Type 3 CRS consists in an abrupt worsening of renal function (e.g. acute kidney ischemia or glomerulonephritis) causing acute cardiac disorder (e.g. heart failure, arrhythmia, ischemia).
• Type 4 CRS describes a state of chronic kidney disease (e.g. chronic glomerular disease) contributing to decreased cardiac function, cardiac hypertrophy and/ or increased risk of adverse cardiovascular events.
• Type 5 CRS reflects a systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal dysfunction.
CRS Type I – Key concepts• Acute
• Generally, four broad subsets of heart failure1
– Acutely decompensated failure
– Hypertensive failure with preserved EF and pulmonary edema
– Cardiogenic shock
– Right ventricular failure
• Consider pre-existing risk factors, such as2,3
– Underlying renal insufficiency
– Worsening heart failure class
– Tachyarrhythmias
– Hypo/Hypertension
– High dose diuretic therapy
• Primary clinical observation is inadequate renal perfusion leading to low cardiac output with marked elevation of venous pressures resulting in renal congestion1. Nohria A, et al. J Am Coll Cardiol. 2008;51(13):1268-1274.2. Forman DE, et al. J Am Coll Cardiol. 2004;43(1):61-67.3. Cowie MR, Eur Heart J. 2006;27(10):1216-1222.
CRS Type I – Treatment Considerations
• Decongestion is paramount
• If this is a relatively new condition the traditional approaches are often successful1
– Diuretics
– Vasodilators
– And, in the case of cardiogenic shock -- pressors
• If acute on chronic, then it is often more difficult due to refractory treatment responsiveness2
1. Dickstein K, et al. 2010 Europace. 2010;12(11):1526-1536.2. Pasquale Congest Heart Fail. 2007;13(2):93-98.

2/27/2017
6
CRS Type 1 – Treatment Considerations cont.
• Diuretics
– Loop diuretic preferred and intravenously
• Bolus vs Continuous – Dose Trial1
• Augmented with low dose Dopamine – DAD-HF2
• Ultrafiltration – To Be or Not to Be3,4,5
– UNLOAD, CARRESS, AVOID-HF – Up in the Air
• Consider plasma refill rate/hemoconcentration6
1. Felker GM. New England Journal of Medicine. 2011;364(9):797-805.2. Giamouzis G, J Card Fail. 2010;16(12):922-930.3. Costanzo MR, J Am Coll Cardiol. 2007;49(6):675-683.4. Bart BA, New England Journal of Medicine. 2012;367(24):2296-2304.5. New England Journal of Medicine. 2013;368(12):1157-1160.6. Testani JM, Circulation. 2010;122(3):265-272.
CRS Type 1 – Treatment Considerations cont.
• Vasodilators
– Nitroglycerin and nitropreside
• Limited data and cautious recommendations1,2
– Nesiritide
• Initially looked good but fell out of favor3
1. Mullens W, 2008;52(3):200-207.2. Yancy CW, et al. 2013 ACCF/AHA guideline J Am Coll Cardiol. 2013;62(16):e147-
239.3. Chen HH, Circ Heart Fail. 2013;6(5):1087-1094.
CRS Type 1 – Treatment Considerations cont.
• Inotropes/pressors– More symptomatic relief, palliative measures, or
bridge to decision – overall associated with high morbidity and mortality, especially arrhythmogenic death1
• More novel agents 2,3
– Vasopressin
– Levosimendan
– Relaxin 1. Yancy CW, et al. 2013 ACCF/AHA guideline J Am Coll Cardiol.
2013;62(16):e147-239.2. Konstam MA, Jama. 2007;297(12):1319-1331.3. Triposkiadis F, Expert Opin Investig Drugs. 2009;18(6):695-707.

2/27/2017
7
• Type 1 CRS reflects an abrupt worsening of cardiac function (e.g. acute cardiogenic shock or decompensated congestive heart failure) leading to acute kidney injury.
• Type 2 CRS describes chronic abnormalities in cardiac function (e.g. chronic congestive heart failure) causing progressive and permanent chronic kidney disease.
• Type 3 CRS consists in an abrupt worsening of renal function (e.g. acute kidney ischemia or glomerulonephritis) causing acute cardiac disorder (e.g. heart failure, arrhythmia, ischemia).
• Type 4 CRS describes a state of chronic kidney disease (e.g. chronic glomerular disease) contributing to decreased cardiac function, cardiac hypertrophy and/ or increased risk of adverse cardiovascular events.
• Type 5 CRS reflects a systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal dysfunction.
CRS Type 2 – Key Concepts
• Chronic abnormalities – Cardiac is Primary (Type 2 and Type 4 are often very difficult to distinguish)
• Make an effort to discern which is primary – cardiac vsrenal
• Very few chronic heart failure patients present without some degree of renal dysfunction (ADHERE); furthermore, this co-existent relationship is associate with poor out comes.1
1. Heywood JT, J Card Fail. 2007;13(6):422-430.
CRS Type 2 – Treatment Considerations
• Primary goal is evidence based care of the patient– Aggressively prudent up-titration of ACE/ARB
• Hypotension, NSAIDS
– Carvedilol may have a more favorable effect on renal function1
– Spironolactone should be considered with attention to hyperkalemia
– How does PARADIGM fit into the CRS paradigm• Possibly more favorable renal effects2
– Diuretics and diuretic resistance1. Bakris GL, Kidney Int. 2006;70(11):1905-1913.2. Solomon SD, Lancet. 2012;380(9851):1387-1395.

2/27/2017
8
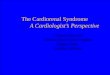
Krämer et al. Am J Med. 1999;106:90.
Elevated Neurohormone Levels Cause Diuretic
Resistance
Proximal Tubule
Angiotensin II increases sodium reabsorption
Glomerulus
Norepinephrine(and endothelin) decreases
renal blood flow and GFR
Collecting Duct
Aldosterone increases sodium reabsorption

2/27/2017
9
CRS Type 2 – Treatment Considerations cont
• Diuretic Resistence1
– Short-term (braking phenomena)
• Poorly understood
– Long-term distal nephron hypertrophy
• May be benefited by combination therapy
1. Brater DC. Diuretic therapy. N Engl J Med. 1998;339(6):387-395.
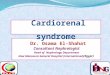
Short-Term (Braking Phenomena)
1. Wilcox et al. Kidney Int. 1987;31:135.
F = Furosemide
Na+ Reaccumulation Between Furosemide Doses
Na+ Intake
Na+ Excretion
Net Diuresis After 4 Days of Rx = 0 mL
300
250
200
150
100
50
0Before F F1 F2 F3 F4
Time, Days
UN
aV
, m
Eq
/6h
Long Term tolerance
Tubular hypertrophy to compensate for salt loss
Brater. N Engl J Med. 1998;339:387.

2/27/2017
10
Ellison. Cardiology. 2001;96:132-143.
Result of diuretic tolerance
20
18
16
14
12
10
8
6
4
2
0
[Furosemide], µg/mL
0.01 0.1 1 10 100
Normal
CRF
CHFSecretory
Defect
DecreasedMaximalResponse
FE
Na
,%
Fractional Na Excretion
• Type 1 CRS reflects an abrupt worsening of cardiac function (e.g. acute cardiogenic shock or decompensated congestive heart failure) leading to acute kidney injury.
• Type 2 CRS describes chronic abnormalities in cardiac function (e.g. chronic congestive heart failure) causing progressive and permanent chronic kidney disease.
• Type 3 CRS consists in an abrupt worsening of renal function (e.g. acute kidney ischemia or glomerulonephritis) causing acute cardiac disorder (e.g. heart failure, arrhythmia, ischemia).
• Type 4 CRS describes a state of chronic kidney disease (e.g. chronic glomerular disease) contributing to decreased cardiac function, cardiac hypertrophy and/ or increased risk of adverse cardiovascular events.
• Type 5 CRS reflects a systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal dysfunction.

2/27/2017
11
CRS Type 3—Key Concepts
• Acute Kidney Injury
– Contrast induced kidney injury
– Drug-induced nephropathies
– Kidney injury post major surgery
– Rhabdomyloysis
– Post-infectious glomerulonephritis
CRS Type 3 – Treatment Considerations
• Avoid the insult
– Assess for vulnerable patient populations
– Hydrate
• Novel therapies
– Avert System Technology (AVERT clinical trial (NCT
01976299)
• Type 1 CRS reflects an abrupt worsening of cardiac function (e.g. acute cardiogenic shock or decompensated congestive heart failure) leading to acute kidney injury.
• Type 2 CRS describes chronic abnormalities in cardiac function (e.g. chronic congestive heart failure) causing progressive and permanent chronic kidney disease.
• Type 3 CRS consists in an abrupt worsening of renal function (e.g. acute kidney ischemia or glomerulonephritis) causing acute cardiac disorder (e.g. heart failure, arrhythmia, ischemia).
• Type 4 CRS describes a state of chronic kidney disease (e.g. chronic glomerular disease) contributing to decreased cardiac function, cardiac hypertrophy and/ or increased risk of adverse cardiovascular events.
•
• Type 5 CRS reflects a systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal dysfunction.

2/27/2017
12
CRS Type 4—Key Concepts
• Chronic abnormalities – Renal vs Primary
(Type 2 and Type 4 are often very difficult to
distinguish)
• Principle concept is clinical management
aimed at slowing the progression of renal
dysfunction
CRS Type 4 – Treatment Considerations
• Appreciate the degree of renal insufficiency when considering medications and dosage, i.e. digoxin
• Be mindful of over diuresis
• Consider the possibility of chronic anemia
– No benefit in RED-HF(epo)1
– Interesting benefits of FAIR-HF (iron)2
1. Swedberg K, N Engl J Med. 2013;368(13):1210-1219.2. Anker SD, N Engl J Med. 2009;361(25):2436-2448.
• Type 1 CRS reflects an abrupt worsening of cardiac function (e.g. acute cardiogenic shock or decompensated congestive heart failure) leading to acute kidney injury.
• Type 2 CRS describes chronic abnormalities in cardiac function (e.g. chronic congestive heart failure) causing progressive and permanent chronic kidney disease.
• Type 3 CRS consists in an abrupt worsening of renal function (e.g. acute kidney ischemia or glomerulonephritis) causing acute cardiac disorder (e.g. heart failure, arrhythmia, ischemia).
• Type 4 CRS describes a state of chronic kidney disease (e.g. chronic glomerular disease) contributing to decreased cardiac function, cardiac hypertrophy and/ or increased risk of adverse cardiovascular events.
• Type 5 CRS reflects a systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal dysfunction.

2/27/2017
13
CRS Type 5—Key Concepts
• Essentially, a simultaneous acute/chronic
dysfunction of both the cardio and renal
systems
• Limited studies and least understood;
however, as more organs fail outcomes are
obviously worse
CRS Type 5—Treatment Considerations
• Prompt identification and treatment of the offending source
• Hydration
– Conservative vs Liberal1
• Pressor consideration
– Norepinephrine and vasopressor dopamine are both associated with high mortality but norepinephrine may have less adverse events2
1. Wiedemann HP, N Engl J Med. 2006;354(24):2564-2575.
2. De Backer D, N Engl J Med. 2010;362(9):779-789.
CRS – Complicated
• Cardio-Renal Syndrome is very real and very complicated
• It is a marker for Advanced Management
• It is a tremendous burden leading to readmissions and death
• Effective treatment must be unique to the patient

2/27/2017
14