Embed Size (px)
Citation preview
The Society of Thoracic Surgeons
Frequently Asked Questions: Adult Cardiac Surgery Database
Version 2.52.1
AUGUST, 2007
How to use the “interactive” FAQ Document:
1. To review all clinical questions in an individual section, click on the section title below.
Section A: seq# 40-80 Section F: seq# 750-870 Section K: seq# 1630-1880 Section P: seq# 2710-3010 Section B: seq# 100-210 Section G: seq# 890-1040 Section L: seq# 1920-2350 Section Q: seq# 3020-3080 Section C: seq# 220-340 Section H: seq# 1050-1200 Section M: seq# 2360-2560 Section R: seq# 3090-3210 Section D: seq# 350-550 Section I: seq# 1210-1500 Section N: seq# 2570-2600 Section S: seq# 3220-3240 Section E: seq# 560-670 Section J: seq# 1520-1620 Section O: seq# 2610-2700
2. To review an individual Seq# clinical question, click on the Seq# title below. 310 ICUInHrs 2470 OCarAFib 340 TotHrICU 2560 OCarOthr 440 RenFail 2710 Complics 490 InfEndo 2750 COpReOth 850 ArrhyTyp 2780 CISternDeep 1050 NumDisV 2830 CNStrokP 1260 EmergRsn 2950 COtCoag 1280 OpCAB 3090-3180 Section R. 1310 OpOCard 3220 Readm30 1380 PerfusTm 3240 ReadmPro 1410 XClampTm 1640 OpMitral 1650 OpTricus 3. CC/TM: Corrections/Clarifications to Training Manual NEW Date SeqNo FieldName Definition From
version 2.41
9/03 GENERAL QUESTIONS #1 -Patient has CABG; while still in hospital has thoracic aortic dissection, then re-op for bleeding then expires while still in hospital. -Another patient has CABG then re-op for bleeding on same day during which time the patient gets another SVG, patient discharged alive. My surgeon thinks that in both these cases, we should complete 2 STS forms for each patient.
The STS is set up to capture only one, primary procedure per admission with any subsequent interventions captured as complications. We realize that some important information will be missed, primarily OR information.
2/04 GENERAL STATEMENT #1 “Pre-op", "intra-op" and "post-op" defined according to the STS Adult Cardiac Database. Pre-op: time period prior to the OR until the patient enters the OR Intra-op: from the time the patient enter the OR until the patient exits the OR Post-op: from the time the patient exits the OR until the patient leaves the hospital
3/04 ONE PATIENT ADMISSION = ONE DATA COLLECTION FORM
8/04 A patient has an AVR done. Within days a serious perivalvular leak develops. The patient returns to the OR during the same hospitalization for a redo AVR- first valve removed, new valve placed. Does this reoperation require a new Data Collection Form or is the redo AVR coded as a complication/return to OR under the original Data Collection Form?
ONE ADMISSION = ONE DATA COLLECTION FORM. As long as the patient does not leave the hospital, all complications or postoperative events need to be captured in the complications section of the original Data Collection Form. If the patient would have been discharged and readmitted to repair the perivalvular leak, a new Data Collection Form would need to be started.
9/04 Case #1: female patient had an AVR. Returned to surgery during the same admission for a repair of the ascending aorta. Is the aorta repair considered a complication from the first surgery? Case #2: female patient had a 5 vessel bypass. Within a few hours patient had a sudden cardiac arrest, returned to surgery and had an additional vein graft placed.
For both cases the surgeon feels the second surgeries should be treated as separate surgeries and collected on a separate Data Collection Form. For the purposes of the STS, both of the second surgeries are considered complications (or postoperative events) of the first surgery and should be captured in the "Complications Section" of the Data Collection Form. The general rule is ONE ADMISSION = ONE DATA COLLECTION FORM. If these patients were discharged and then readmitted to return to surgery, then a new Data Collection Form would need to been completed on the second surgeries.
01/06
GENERAL STATEMENT #2
The patient has an original AVR and single CABG. The patient returns to the operating room 5 days later for ischemia and has a double CABG. How do I code this?
Code the return as a Re-op Other Cardiac
9/04 Our cardiothoracic surgeon performed a Thymectomy in the OR as the primary surgical procedure. Do I fill out an STS Data Collection Form to track the procedure?
I would. Obviously, this record will not be included in the risk models and you will not be able to populate all of the fields. Including all procedures that your cardiothoracic surgeon perform into the Adult Cardiac Database is a great way to keep track of your cardiothoracic surgeons' procedures.
03/06
GENERAL STATEMENT #3
Should the valve repairs done via a thoracotomy be captured in the database? It is our understanding that a mediastinal incision should be made to be applicable to the database.
Yes, any surgery performed on a structure of the heart or great vessels should be included in the Adult Cardiac Database. Surgical approach and incisions have changed over time, but the end result is still the same - repair of a cardiac structure.
11/04 GENERAL STATEMENT #4 The following guideline was developed to assist your decision of whether or not to include a case in the Adult Cardiac Surgery Database. 1. Patient enters OR -- no incision -- no procedure = do not capture this procedure a. Patient in ED with torn aorta, coding as enters the OR, dies before incision made= do not capture this procedure 2. Patient enters OR -- with skin incision and surgical intervention on heart and/or great vessels -- procedure aborted = capture as "Other Cardiac Procedure - Other" a. Patient in OR with incision, cannulated, patient arrests and expires = "Other Cardiac Procedure - Other" b. Patient in OR for redo CABG, while performing mediansternotomy, aorta is nicked, patient expires = "Other Cardiac Procedure - Other" 3. Patient enters OR -- with skin incision and no further surgical intervention -- procedure aborted = capture as "Other Non Cardiac Procedure - Other" a. Patient enters the OR for AVR, chest opened, Aorta too fragile, procedure aborted, no AVR = "Other Non Cardiac Procedure - Other"
1/06 What are we accomplishing by collecting the data described in General Statement #4 from 11/04? We were informed from STS that the "other cardiac" and "other non-cardiac" sections were to be used in conjunction with a CAB or a valve only. This data is not used in harvest, correct?
The data is used in harvest, but not for any Risk-adjusted outcomes. These fields are NOT to be used only in conjunction with CAB or Valve surgeries. The Adult Cardiac database is intended to include any surgery done on the structures of the heart and/or great vessels. Advantages of including these procedures are the ability to monitor outcomes for all cardiac surgeries, tracking of 100% of CT surgery volume, and, as technology changes, tracking and trending outcomes of new procedures (i.e. Arrhythmia Correction surgery, MAZE).
08/06 OpOCard Message: Pt goes into OR for valve procedure. During induction of anesthesia, and prior to surgical inc, pt codes. Sternotomy performed for purpose of cardiac massage. Pt expires. Does this procedure count?
General Statement #4 of the FAQ will help you with decisions to include or not include patients of this type. This would be close to Scenario #3. Include as an Other-NonCardiac Other.
4/05 GENERAL STATEMENT #5 How do we code an Aortic Edwards Lifesciences Model 2625 Porcine Valve and a Mitral Edwards Lifesciences 6625LP Porcine valve?
The Mitral Edwards Lifescience 6625LP is listed in the 2.52.1 mitral implant list. It is the C-E Duraflex Porcine Bioprosthesis #76 listed on page 72 of the Version 2.52.1 Data Specifications, and on the DCF is B28. The Aortic Edwards Lifescience model 2625 is the C-E standard porcine bioprosthesis # 23 on page 65 of the V2.52.1 Data Specifications and on the DCF as B7. Both are stented valves. Please refer to the Edwards Lifescience web site under products to view additional information concerning the various types of valves and their features. If you ever have a question about a specific Model number of a valve, please refer to the manufacturer's website as most will let you search by model number. The Valve Key includes all valves that were FDA approved at the time when the 2.52.1 data specifications went out to the software vendors to be upgraded back in 2003. If the exact valve name is not on the valve key list or in the 2.52.1 data specifications and the manufacturer's website says the valve is not exactly the same as one on the valve key, please code as 777-Other. The valve key will be updated will all FDA approved valve implants at the time of the next specification upgrade. You might consider adding a custom field for any time you code 777 to allow you to track devices that are implanted that do not yet appear on the valve key.
12/06 GENERAL STATEMENT #6 The question has been raised with regard to contacting patients for 30 follow up to determine their readmit status. Some facilities obtain consents prior to contacting patients while some have other ways of collecting that data. What is the STS position with regard to obtaining consent from the patient prior to contacting them to determine 30 day status?
There is no specific position taken by the STS with regard to consent to contact patients. Many hospitals contact patients as a matter of course. It is important to have accurate 30 follow up information.
12/06 GENERAL STATEMENT #7 When a patient remains in the hospital during the harvest period and is not discharged for weeks after the harvest is completed how do we handle the completion of the outcomes?
This patients’ record can be submitted during the initial harvest and resubmitted when the patient has been discharge in the subsequent harvest. This will allow for all the outcomes to be captured.
10 Software Vendor Name Name (assigned by STS) given to identify software vendor (up to 8 characters). Vendors should use standard name identification across sites. Changes to Vendor Name Identification must be approved by the STS.
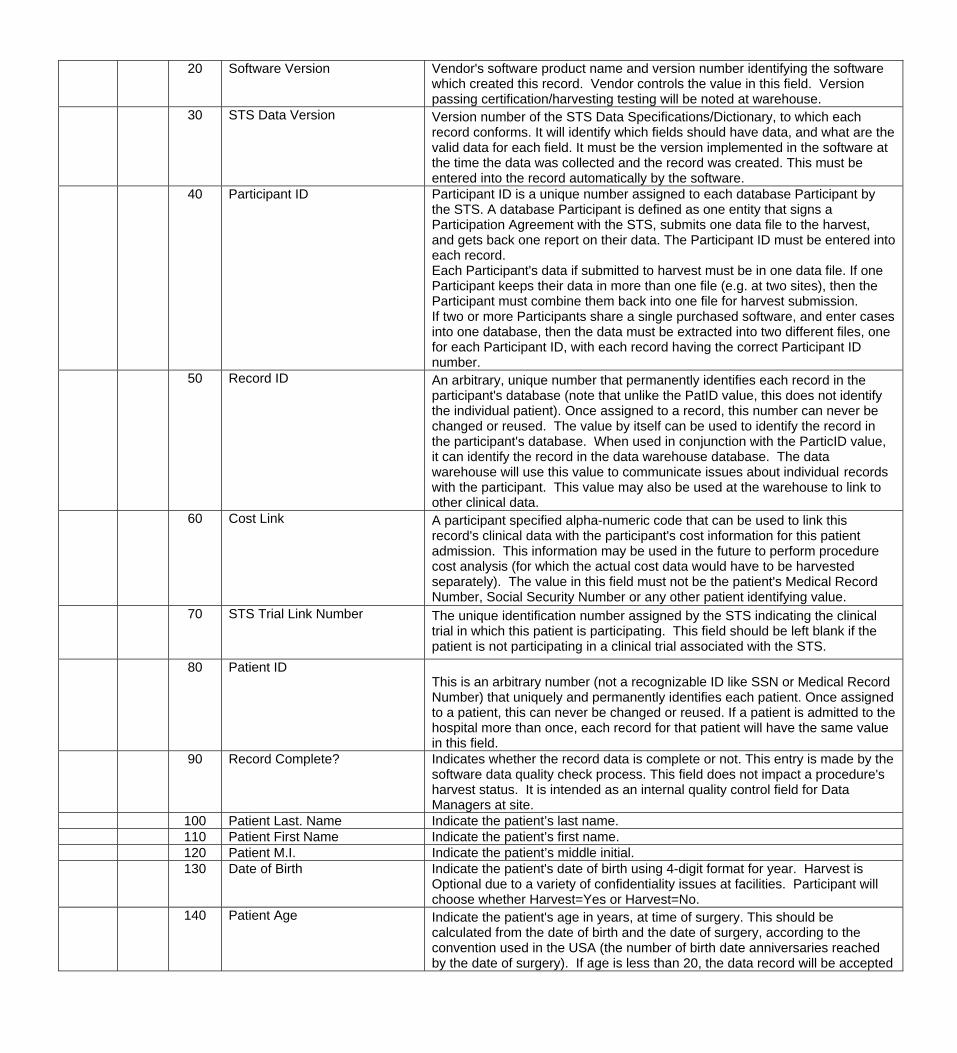
20 Software Version Vendor's software product name and version number identifying the software which created this record. Vendor controls the value in this field. Version passing certification/harvesting testing will be noted at warehouse.
30 STS Data Version Version number of the STS Data Specifications/Dictionary, to which each record conforms. It will identify which fields should have data, and what are the valid data for each field. It must be the version implemented in the software at the time the data was collected and the record was created. This must be entered into the record automatically by the software.
40 Participant ID Participant ID is a unique number assigned to each database Participant by the STS. A database Participant is defined as one entity that signs a Participation Agreement with the STS, submits one data file to the harvest, and gets back one report on their data. The Participant ID must be entered into each record. Each Participant's data if submitted to harvest must be in one data file. If one Participant keeps their data in more than one file (e.g. at two sites), then the Participant must combine them back into one file for harvest submission. If two or more Participants share a single purchased software, and enter cases into one database, then the data must be extracted into two different files, one for each Participant ID, with each record having the correct Participant ID number.
50 Record ID An arbitrary, unique number that permanently identifies each record in the participant's database (note that unlike the PatID value, this does not identify the individual patient). Once assigned to a record, this number can never be changed or reused. The value by itself can be used to identify the record in the participant's database. When used in conjunction with the ParticID value, it can identify the record in the data warehouse database. The data warehouse will use this value to communicate issues about individual records with the participant. This value may also be used at the warehouse to link to other clinical data.
60 Cost Link A participant specified alpha-numeric code that can be used to link this record's clinical data with the participant's cost information for this patient admission. This information may be used in the future to perform procedure cost analysis (for which the actual cost data would have to be harvested separately). The value in this field must not be the patient's Medical Record Number, Social Security Number or any other patient identifying value.
70 STS Trial Link Number The unique identification number assigned by the STS indicating the clinical trial in which this patient is participating. This field should be left blank if the patient is not participating in a clinical trial associated with the STS.
80 Patient ID This is an arbitrary number (not a recognizable ID like SSN or Medical Record Number) that uniquely and permanently identifies each patient. Once assigned to a patient, this can never be changed or reused. If a patient is admitted to the hospital more than once, each record for that patient will have the same value in this field.
90 Record Complete? Indicates whether the record data is complete or not. This entry is made by the software data quality check process. This field does not impact a procedure's harvest status. It is intended as an internal quality control field for Data Managers at site.
100 Patient Last. Name Indicate the patient’s last name. 110 Patient First Name Indicate the patient’s first name. 120 Patient M.I. Indicate the patient’s middle initial. 130 Date of Birth Indicate the patient's date of birth using 4-digit format for year. Harvest is
Optional due to a variety of confidentiality issues at facilities. Participant will choose whether Harvest=Yes or Harvest=No.
140 Patient Age Indicate the patient's age in years, at time of surgery. This should be calculated from the date of birth and the date of surgery, according to the convention used in the USA (the number of birth date anniversaries reached by the date of surgery). If age is less than 20, the data record will be accepted
into the database, but will not be included in the national analysis and report.
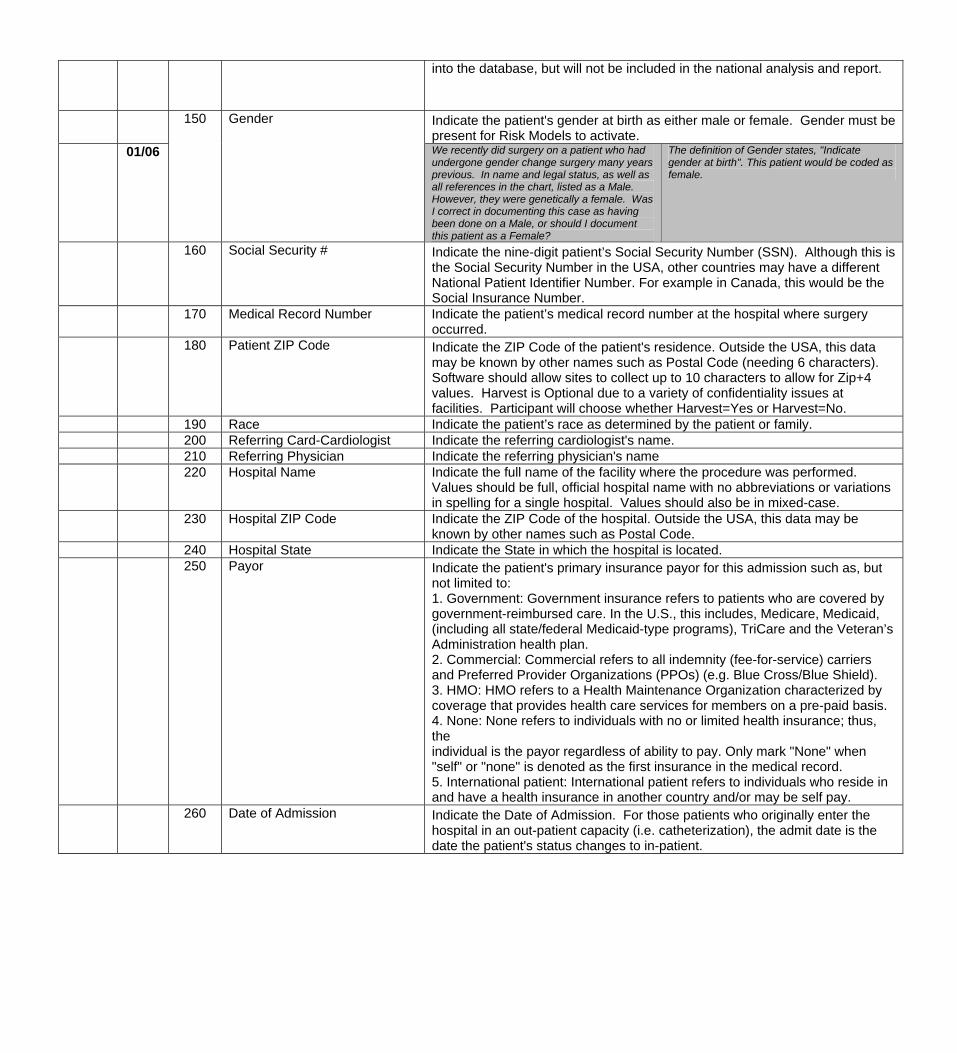
Indicate the patient's gender at birth as either male or female. Gender must be present for Risk Models to activate.
01/06
150 Gender
We recently did surgery on a patient who had undergone gender change surgery many years previous. In name and legal status, as well as all references in the chart, listed as a Male. However, they were genetically a female. Was I correct in documenting this case as having been done on a Male, or should I document this patient as a Female?
The definition of Gender states, "Indicate gender at birth". This patient would be coded as female.
160 Social Security # Indicate the nine-digit patient’s Social Security Number (SSN). Although this is the Social Security Number in the USA, other countries may have a different National Patient Identifier Number. For example in Canada, this would be the Social Insurance Number.
170 Medical Record Number Indicate the patient’s medical record number at the hospital where surgery occurred.
180 Patient ZIP Code Indicate the ZIP Code of the patient's residence. Outside the USA, this data may be known by other names such as Postal Code (needing 6 characters). Software should allow sites to collect up to 10 characters to allow for Zip+4 values. Harvest is Optional due to a variety of confidentiality issues at facilities. Participant will choose whether Harvest=Yes or Harvest=No.
190 Race Indicate the patient’s race as determined by the patient or family. 200 Referring Card-Cardiologist Indicate the referring cardiologist's name. 210 Referring Physician Indicate the referring physician's name 220 Hospital Name Indicate the full name of the facility where the procedure was performed.
Values should be full, official hospital name with no abbreviations or variations in spelling for a single hospital. Values should also be in mixed-case.
230 Hospital ZIP Code Indicate the ZIP Code of the hospital. Outside the USA, this data may be known by other names such as Postal Code.
240 Hospital State Indicate the State in which the hospital is located. 250 Payor Indicate the patient's primary insurance payor for this admission such as, but
not limited to: 1. Government: Government insurance refers to patients who are covered by government-reimbursed care. In the U.S., this includes, Medicare, Medicaid, (including all state/federal Medicaid-type programs), TriCare and the Veteran’s Administration health plan. 2. Commercial: Commercial refers to all indemnity (fee-for-service) carriers and Preferred Provider Organizations (PPOs) (e.g. Blue Cross/Blue Shield). 3. HMO: HMO refers to a Health Maintenance Organization characterized by coverage that provides health care services for members on a pre-paid basis. 4. None: None refers to individuals with no or limited health insurance; thus, the individual is the payor regardless of ability to pay. Only mark "None" when "self" or "none" is denoted as the first insurance in the medical record. 5. International patient: International patient refers to individuals who reside in and have a health insurance in another country and/or may be self pay.
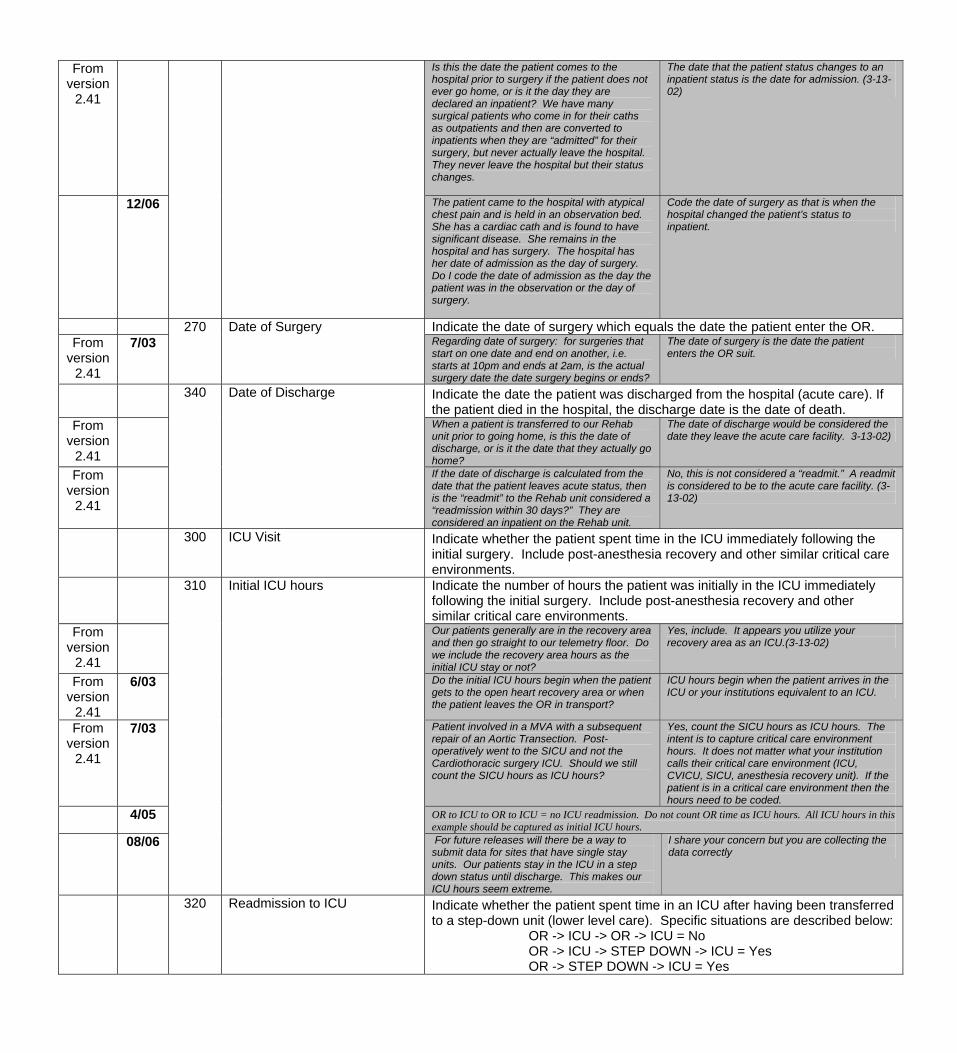
260 Date of Admission Indicate the Date of Admission. For those patients who originally enter the hospital in an out-patient capacity (i.e. catheterization), the admit date is the date the patient's status changes to in-patient.
From version
2.41
Is this the date the patient comes to the hospital prior to surgery if the patient does not ever go home, or is it the day they are declared an inpatient? We have many surgical patients who come in for their caths as outpatients and then are converted to inpatients when they are “admitted” for their surgery, but never actually leave the hospital. They never leave the hospital but their status changes.
The date that the patient status changes to an inpatient status is the date for admission. (3-13-02)
12/06 The patient came to the hospital with atypical chest pain and is held in an observation bed. She has a cardiac cath and is found to have significant disease. She remains in the hospital and has surgery. The hospital has her date of admission as the day of surgery. Do I code the date of admission as the day the patient was in the observation or the day of surgery.
Code the date of surgery as that is when the hospital changed the patient’s status to inpatient.
Indicate the date of surgery which equals the date the patient enter the OR. From
version 2.41
7/03 270 Date of Surgery
Regarding date of surgery: for surgeries that start on one date and end on another, i.e. starts at 10pm and ends at 2am, is the actual surgery date the date surgery begins or ends?
The date of surgery is the date the patient enters the OR suit.
Indicate the date the patient was discharged from the hospital (acute care). If the patient died in the hospital, the discharge date is the date of death.
From version
2.41
When a patient is transferred to our Rehab unit prior to going home, is this the date of discharge, or is it the date that they actually go home?
The date of discharge would be considered the date they leave the acute care facility. 3-13-02)
From version
2.41
340 Date of Discharge
If the date of discharge is calculated from the date that the patient leaves acute status, then is the “readmit” to the Rehab unit considered a “readmission within 30 days?” They are considered an inpatient on the Rehab unit.
No, this is not considered a “readmit.” A readmit is considered to be to the acute care facility. (3-13-02)
300 ICU Visit Indicate whether the patient spent time in the ICU immediately following the initial surgery. Include post-anesthesia recovery and other similar critical care environments.
Indicate the number of hours the patient was initially in the ICU immediately following the initial surgery. Include post-anesthesia recovery and other similar critical care environments.
From version
2.41
Our patients generally are in the recovery area and then go straight to our telemetry floor. Do we include the recovery area hours as the initial ICU stay or not?
Yes, include. It appears you utilize your recovery area as an ICU.(3-13-02)
From version
2.41
6/03 Do the initial ICU hours begin when the patient gets to the open heart recovery area or when the patient leaves the OR in transport?
ICU hours begin when the patient arrives in the ICU or your institutions equivalent to an ICU.
From version
2.41
7/03 Patient involved in a MVA with a subsequent repair of an Aortic Transection. Post-operatively went to the SICU and not the Cardiothoracic surgery ICU. Should we still count the SICU hours as ICU hours?
Yes, count the SICU hours as ICU hours. The intent is to capture critical care environment hours. It does not matter what your institution calls their critical care environment (ICU, CVICU, SICU, anesthesia recovery unit). If the patient is in a critical care environment then the hours need to be coded.
4/05 OR to ICU to OR to ICU = no ICU readmission. Do not count OR time as ICU hours. All ICU hours in this example should be captured as initial ICU hours.
08/06
310 Initial ICU hours
For future releases will there be a way to submit data for sites that have single stay units. Our patients stay in the ICU in a step down status until discharge. This makes our ICU hours seem extreme.
I share your concern but you are collecting the data correctly
320 Readmission to ICU Indicate whether the patient spent time in an ICU after having been transferred to a step-down unit (lower level care). Specific situations are described below: OR -> ICU -> OR -> ICU = No OR -> ICU -> STEP DOWN -> ICU = Yes OR -> STEP DOWN -> ICU = Yes
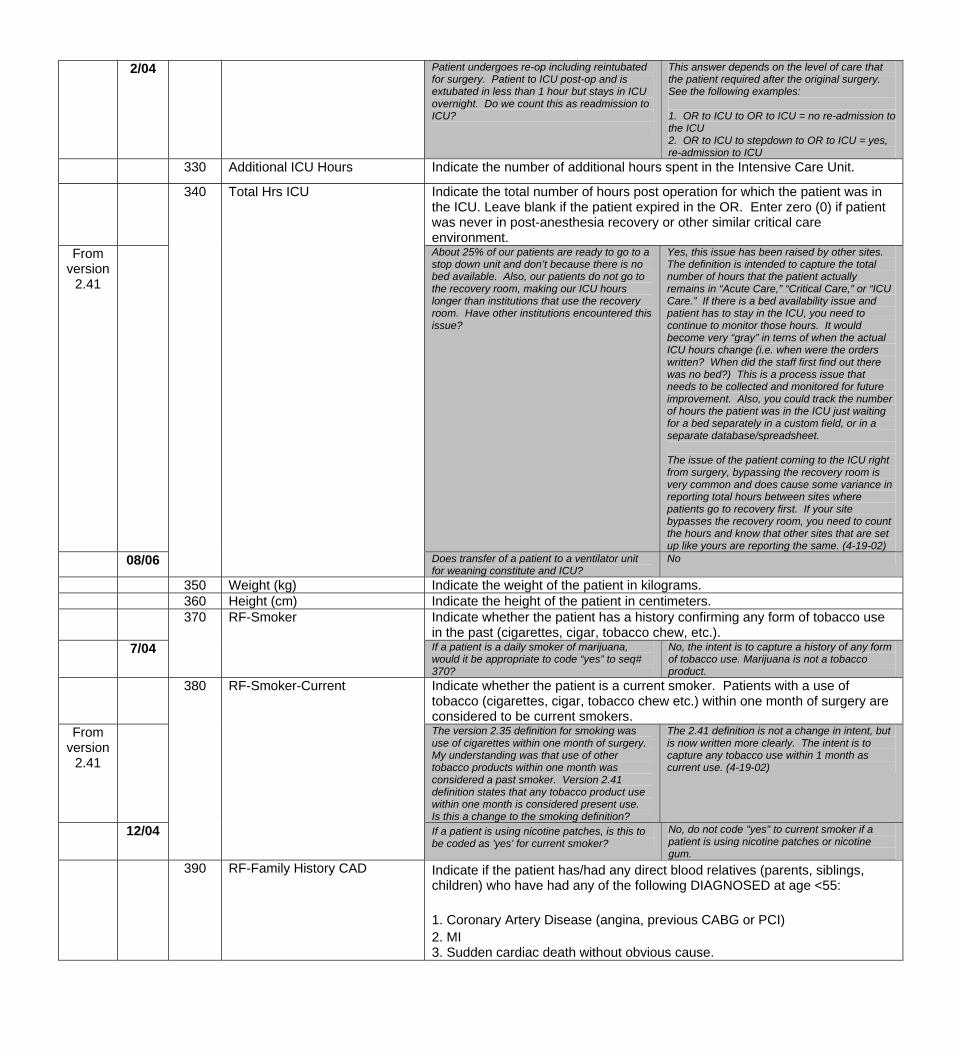
2/04 Patient undergoes re-op including reintubated for surgery. Patient to ICU post-op and is extubated in less than 1 hour but stays in ICU overnight. Do we count this as readmission to ICU?
This answer depends on the level of care that the patient required after the original surgery. See the following examples: 1. OR to ICU to OR to ICU = no re-admission to the ICU 2. OR to ICU to stepdown to OR to ICU = yes, re-admission to ICU
330 Additional ICU Hours Indicate the number of additional hours spent in the Intensive Care Unit.
Indicate the total number of hours post operation for which the patient was in the ICU. Leave blank if the patient expired in the OR. Enter zero (0) if patient was never in post-anesthesia recovery or other similar critical care environment.
From version
2.41
About 25% of our patients are ready to go to a stop down unit and don’t because there is no bed available. Also, our patients do not go to the recovery room, making our ICU hours longer than institutions that use the recovery room. Have other institutions encountered this issue?
Yes, this issue has been raised by other sites. The definition is intended to capture the total number of hours that the patient actually remains in “Acute Care,” “Critical Care,” or “ICU Care.” If there is a bed availability issue and patient has to stay in the ICU, you need to continue to monitor those hours. It would become very “gray” in terns of when the actual ICU hours change (i.e. when were the orders written? When did the staff first find out there was no bed?) This is a process issue that needs to be collected and monitored for future improvement. Also, you could track the number of hours the patient was in the ICU just waiting for a bed separately in a custom field, or in a separate database/spreadsheet. The issue of the patient coming to the ICU right from surgery, bypassing the recovery room is very common and does cause some variance in reporting total hours between sites where patients go to recovery first. If your site bypasses the recovery room, you need to count the hours and know that other sites that are set up like yours are reporting the same. (4-19-02)
08/06
340 Total Hrs ICU
Does transfer of a patient to a ventilator unit for weaning constitute and ICU?
No
350 Weight (kg) Indicate the weight of the patient in kilograms. 360 Height (cm) Indicate the height of the patient in centimeters. Indicate whether the patient has a history confirming any form of tobacco use
in the past (cigarettes, cigar, tobacco chew, etc.). 7/04
370 RF-Smoker
If a patient is a daily smoker of marijuana, would it be appropriate to code “yes” to seq# 370?
No, the intent is to capture a history of any form of tobacco use. Marijuana is not a tobacco product.
Indicate whether the patient is a current smoker. Patients with a use of tobacco (cigarettes, cigar, tobacco chew etc.) within one month of surgery are considered to be current smokers.
From version
2.41
The version 2.35 definition for smoking was use of cigarettes within one month of surgery. My understanding was that use of other tobacco products within one month was considered a past smoker. Version 2.41 definition states that any tobacco product use within one month is considered present use. Is this a change to the smoking definition?
The 2.41 definition is not a change in intent, but is now written more clearly. The intent is to capture any tobacco use within 1 month as current use. (4-19-02)
12/04
380 RF-Smoker-Current
If a patient is using nicotine patches, is this to be coded as 'yes' for current smoker?
No, do not code "yes" to current smoker if a patient is using nicotine patches or nicotine gum.
390 RF-Family History CAD Indicate if the patient has/had any direct blood relatives (parents, siblings, children) who have had any of the following DIAGNOSED at age <55: 1. Coronary Artery Disease (angina, previous CABG or PCI) 2. MI 3. Sudden cardiac death without obvious cause.
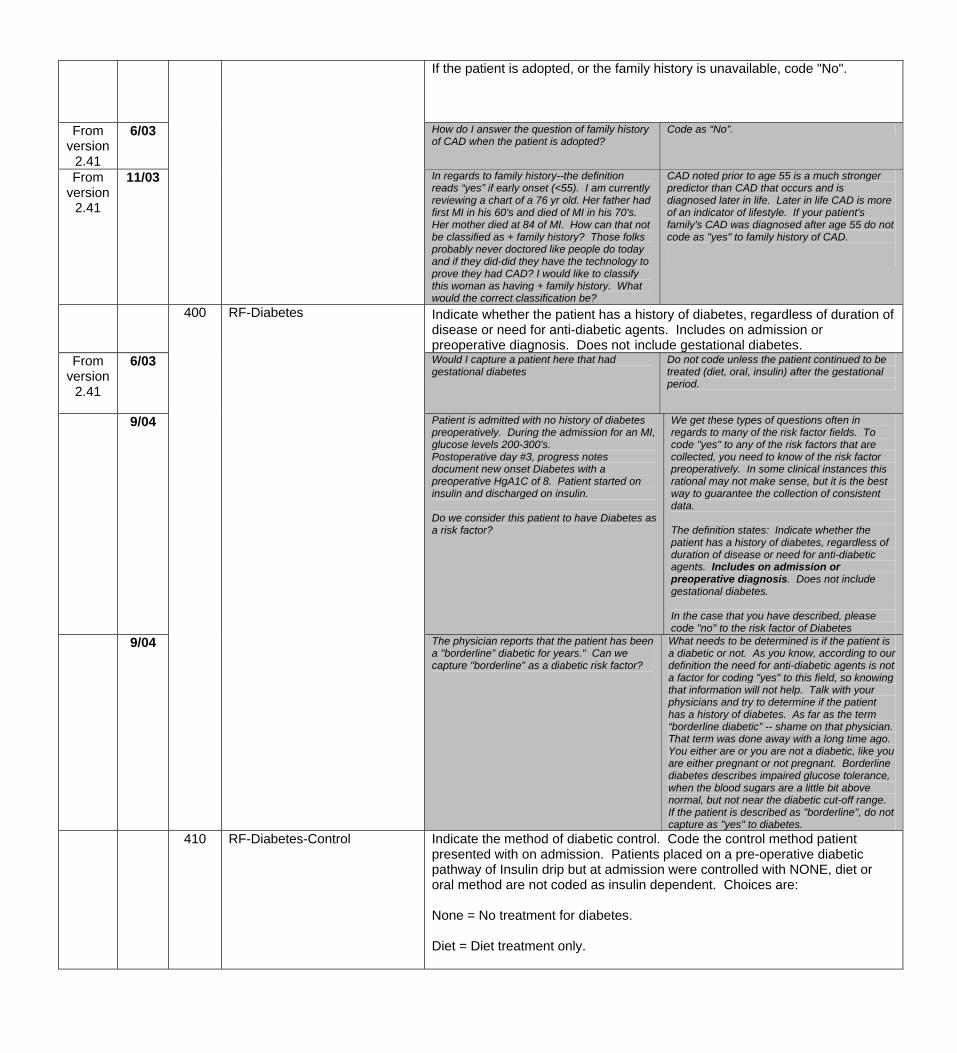
If the patient is adopted, or the family history is unavailable, code "No".
From version
2.41
6/03 How do I answer the question of family history of CAD when the patient is adopted?
Code as “No”.
From version
2.41
11/03 In regards to family history--the definition reads “yes” if early onset (<55). I am currently reviewing a chart of a 76 yr old. Her father had first MI in his 60's and died of MI in his 70's. Her mother died at 84 of MI. How can that not be classified as + family history? Those folks probably never doctored like people do today and if they did-did they have the technology to prove they had CAD? I would like to classify this woman as having + family history. What would the correct classification be?
CAD noted prior to age 55 is a much stronger predictor than CAD that occurs and is diagnosed later in life. Later in life CAD is more of an indicator of lifestyle. If your patient's family's CAD was diagnosed after age 55 do not code as "yes" to family history of CAD.
Indicate whether the patient has a history of diabetes, regardless of duration of disease or need for anti-diabetic agents. Includes on admission or preoperative diagnosis. Does not include gestational diabetes.
From version
2.41
6/03 Would I capture a patient here that had gestational diabetes
Do not code unless the patient continued to be treated (diet, oral, insulin) after the gestational period.
9/04 Patient is admitted with no history of diabetes preoperatively. During the admission for an MI, glucose levels 200-300's. Postoperative day #3, progress notes document new onset Diabetes with a preoperative HgA1C of 8. Patient started on insulin and discharged on insulin. Do we consider this patient to have Diabetes as a risk factor?
We get these types of questions often in regards to many of the risk factor fields. To code "yes" to any of the risk factors that are collected, you need to know of the risk factor preoperatively. In some clinical instances this rational may not make sense, but it is the best way to guarantee the collection of consistent data. The definition states: Indicate whether the patient has a history of diabetes, regardless of duration of disease or need for anti-diabetic agents. Includes on admission or preoperative diagnosis. Does not include gestational diabetes. In the case that you have described, please code "no" to the risk factor of Diabetes
9/04
400 RF-Diabetes
The physician reports that the patient has been a "borderline” diabetic for years." Can we capture "borderline" as a diabetic risk factor?
What needs to be determined is if the patient is a diabetic or not. As you know, according to our definition the need for anti-diabetic agents is not a factor for coding "yes" to this field, so knowing that information will not help. Talk with your physicians and try to determine if the patient has a history of diabetes. As far as the term “borderline diabetic” -- shame on that physician. That term was done away with a long time ago. You either are or you are not a diabetic, like you are either pregnant or not pregnant. Borderline diabetes describes impaired glucose tolerance, when the blood sugars are a little bit above normal, but not near the diabetic cut-off range. If the patient is described as "borderline", do not capture as "yes" to diabetes.
410 RF-Diabetes-Control Indicate the method of diabetic control. Code the control method patient presented with on admission. Patients placed on a pre-operative diabetic pathway of Insulin drip but at admission were controlled with NONE, diet or oral method are not coded as insulin dependent. Choices are: None = No treatment for diabetes. Diet = Diet treatment only.
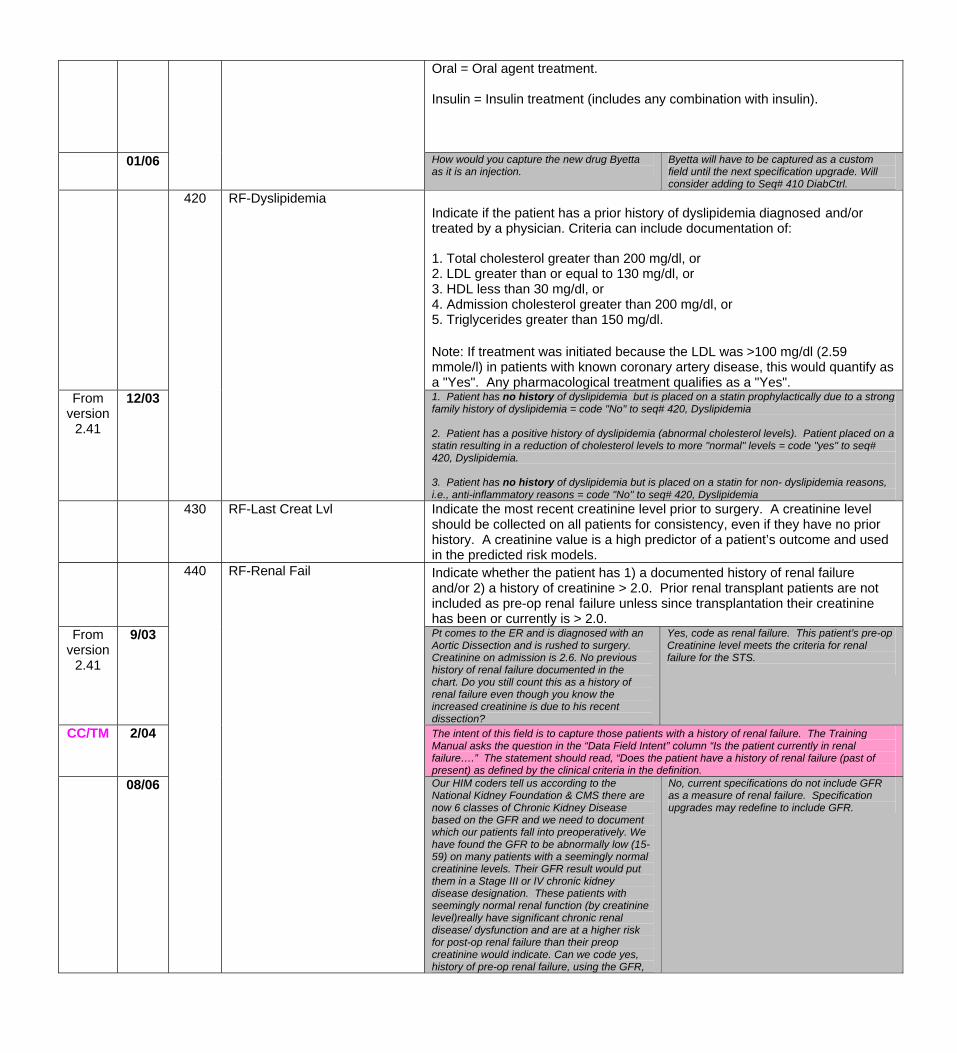
Oral = Oral agent treatment. Insulin = Insulin treatment (includes any combination with insulin).
01/06 How would you capture the new drug Byetta as it is an injection.
Byetta will have to be captured as a custom field until the next specification upgrade. Will consider adding to Seq# 410 DiabCtrl.
Indicate if the patient has a prior history of dyslipidemia diagnosed and/or treated by a physician. Criteria can include documentation of:
1. Total cholesterol greater than 200 mg/dl, or 2. LDL greater than or equal to 130 mg/dl, or 3. HDL less than 30 mg/dl, or 4. Admission cholesterol greater than 200 mg/dl, or 5. Triglycerides greater than 150 mg/dl. Note: If treatment was initiated because the LDL was >100 mg/dl (2.59 mmole/l) in patients with known coronary artery disease, this would quantify as a "Yes". Any pharmacological treatment qualifies as a "Yes".
From version
2.41
12/03
420 RF-Dyslipidemia
1. Patient has no history of dyslipidemia but is placed on a statin prophylactically due to a strong family history of dyslipidemia = code "No" to seq# 420, Dyslipidemia 2. Patient has a positive history of dyslipidemia (abnormal cholesterol levels). Patient placed on a statin resulting in a reduction of cholesterol levels to more "normal" levels = code "yes" to seq# 420, Dyslipidemia. 3. Patient has no history of dyslipidemia but is placed on a statin for non- dyslipidemia reasons, i.e., anti-inflammatory reasons = code "No" to seq# 420, Dyslipidemia
430 RF-Last Creat Lvl Indicate the most recent creatinine level prior to surgery. A creatinine level should be collected on all patients for consistency, even if they have no prior history. A creatinine value is a high predictor of a patient’s outcome and used in the predicted risk models.
Indicate whether the patient has 1) a documented history of renal failure and/or 2) a history of creatinine > 2.0. Prior renal transplant patients are not included as pre-op renal failure unless since transplantation their creatinine has been or currently is > 2.0.
From version
2.41
9/03 Pt comes to the ER and is diagnosed with an Aortic Dissection and is rushed to surgery. Creatinine on admission is 2.6. No previous history of renal failure documented in the chart. Do you still count this as a history of renal failure even though you know the increased creatinine is due to his recent dissection?
Yes, code as renal failure. This patient’s pre-op Creatinine level meets the criteria for renal failure for the STS.
CC/TM 2/04 The intent of this field is to capture those patients with a history of renal failure. The Training Manual asks the question in the “Data Field Intent” column “Is the patient currently in renal failure….” The statement should read, “Does the patient have a history of renal failure (past of present) as defined by the clinical criteria in the definition.
08/06
440 RF-Renal Fail
Our HIM coders tell us according to the National Kidney Foundation & CMS there are now 6 classes of Chronic Kidney Disease based on the GFR and we need to document which our patients fall into preoperatively. We have found the GFR to be abnormally low (15-59) on many patients with a seemingly normal creatinine levels. Their GFR result would put them in a Stage III or IV chronic kidney disease designation. These patients with seemingly normal renal function (by creatinine level)really have significant chronic renal disease/ dysfunction and are at a higher risk for post-op renal failure than their preop creatinine would indicate. Can we code yes, history of pre-op renal failure, using the GFR,
No, current specifications do not include GFR as a measure of renal failure. Specification upgrades may redefine to include GFR.
as directed by the National Kidney Foundation and CMS?
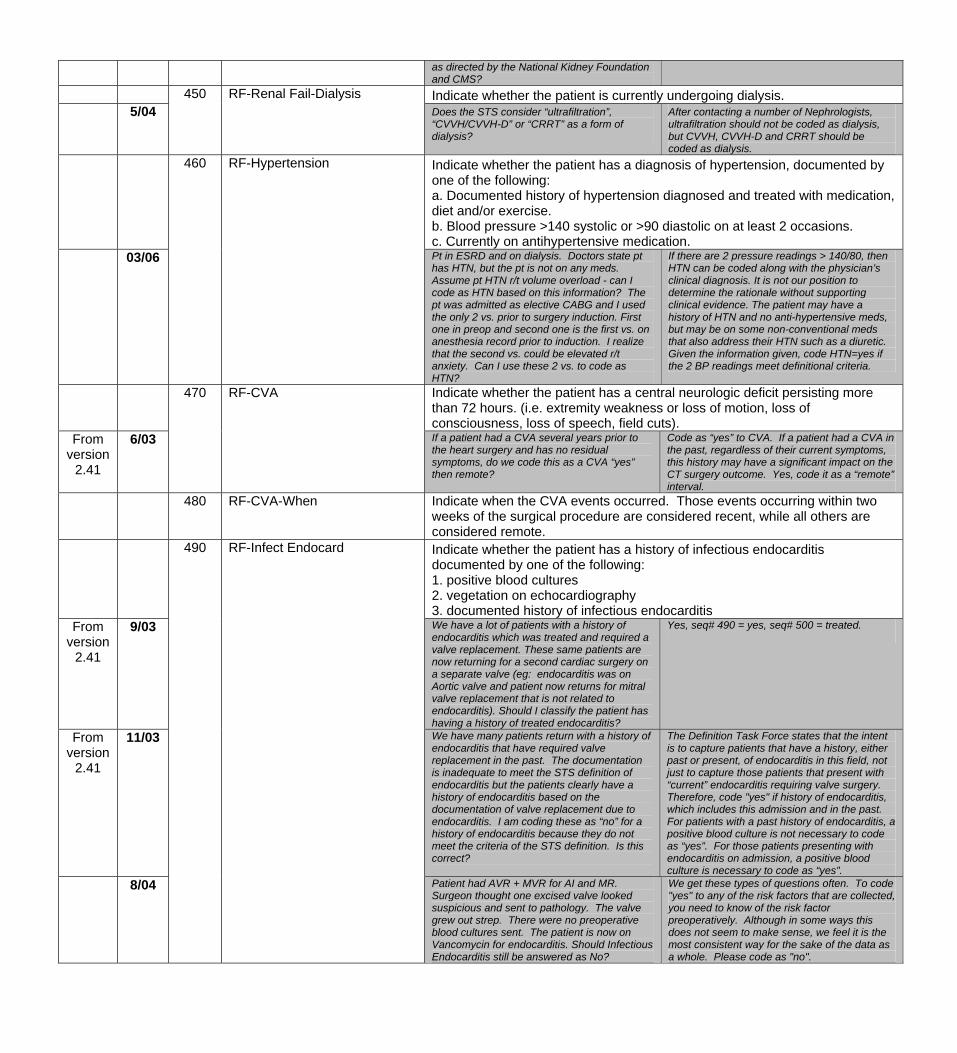
450 RF-Renal Fail-Dialysis Indicate whether the patient is currently undergoing dialysis. 5/04 Does the STS consider “ultrafiltration”,
“CVVH/CVVH-D” or “CRRT” as a form of dialysis?
After contacting a number of Nephrologists, ultrafiltration should not be coded as dialysis, but CVVH, CVVH-D and CRRT should be coded as dialysis.
460 RF-Hypertension Indicate whether the patient has a diagnosis of hypertension, documented by one of the following: a. Documented history of hypertension diagnosed and treated with medication, diet and/or exercise. b. Blood pressure >140 systolic or >90 diastolic on at least 2 occasions. c. Currently on antihypertensive medication.
03/06 Pt in ESRD and on dialysis. Doctors state pt has HTN, but the pt is not on any meds. Assume pt HTN r/t volume overload - can I code as HTN based on this information? The pt was admitted as elective CABG and I used the only 2 vs. prior to surgery induction. First one in preop and second one is the first vs. on anesthesia record prior to induction. I realize that the second vs. could be elevated r/t anxiety. Can I use these 2 vs. to code as HTN?
If there are 2 pressure readings > 140/80, then HTN can be coded along with the physician’s clinical diagnosis. It is not our position to determine the rationale without supporting clinical evidence. The patient may have a history of HTN and no anti-hypertensive meds, but may be on some non-conventional meds that also address their HTN such as a diuretic. Given the information given, code HTN=yes if the 2 BP readings meet definitional criteria.
Indicate whether the patient has a central neurologic deficit persisting more than 72 hours. (i.e. extremity weakness or loss of motion, loss of consciousness, loss of speech, field cuts).
From version
2.41
6/03
470 RF-CVA
If a patient had a CVA several years prior to the heart surgery and has no residual symptoms, do we code this as a CVA “yes” then remote?
Code as “yes” to CVA. If a patient had a CVA in the past, regardless of their current symptoms, this history may have a significant impact on the CT surgery outcome. Yes, code it as a “remote” interval.
480 RF-CVA-When Indicate when the CVA events occurred. Those events occurring within two weeks of the surgical procedure are considered recent, while all others are considered remote.
Indicate whether the patient has a history of infectious endocarditis documented by one of the following: 1. positive blood cultures 2. vegetation on echocardiography 3. documented history of infectious endocarditis
From version
2.41
9/03 We have a lot of patients with a history of endocarditis which was treated and required a valve replacement. These same patients are now returning for a second cardiac surgery on a separate valve (eg: endocarditis was on Aortic valve and patient now returns for mitral valve replacement that is not related to endocarditis). Should I classify the patient has having a history of treated endocarditis?
Yes, seq# 490 = yes, seq# 500 = treated.
From version
2.41
11/03 We have many patients return with a history of endocarditis that have required valve replacement in the past. The documentation is inadequate to meet the STS definition of endocarditis but the patients clearly have a history of endocarditis based on the documentation of valve replacement due to endocarditis. I am coding these as “no” for a history of endocarditis because they do not meet the criteria of the STS definition. Is this correct?
The Definition Task Force states that the intent is to capture patients that have a history, either past or present, of endocarditis in this field, not just to capture those patients that present with “current” endocarditis requiring valve surgery. Therefore, code "yes" if history of endocarditis, which includes this admission and in the past. For patients with a past history of endocarditis, a positive blood culture is not necessary to code as “yes”. For those patients presenting with endocarditis on admission, a positive blood culture is necessary to code as “yes”.
8/04
490 RF-Infect Endocard
Patient had AVR + MVR for AI and MR. Surgeon thought one excised valve looked suspicious and sent to pathology. The valve grew out strep. There were no preoperative blood cultures sent. The patient is now on Vancomycin for endocarditis. Should Infectious Endocarditis still be answered as No?
We get these types of questions often. To code "yes" to any of the risk factors that are collected, you need to know of the risk factor preoperatively. Although in some ways this does not seem to make sense, we feel it is the most consistent way for the sake of the data as a whole. Please code as "no".
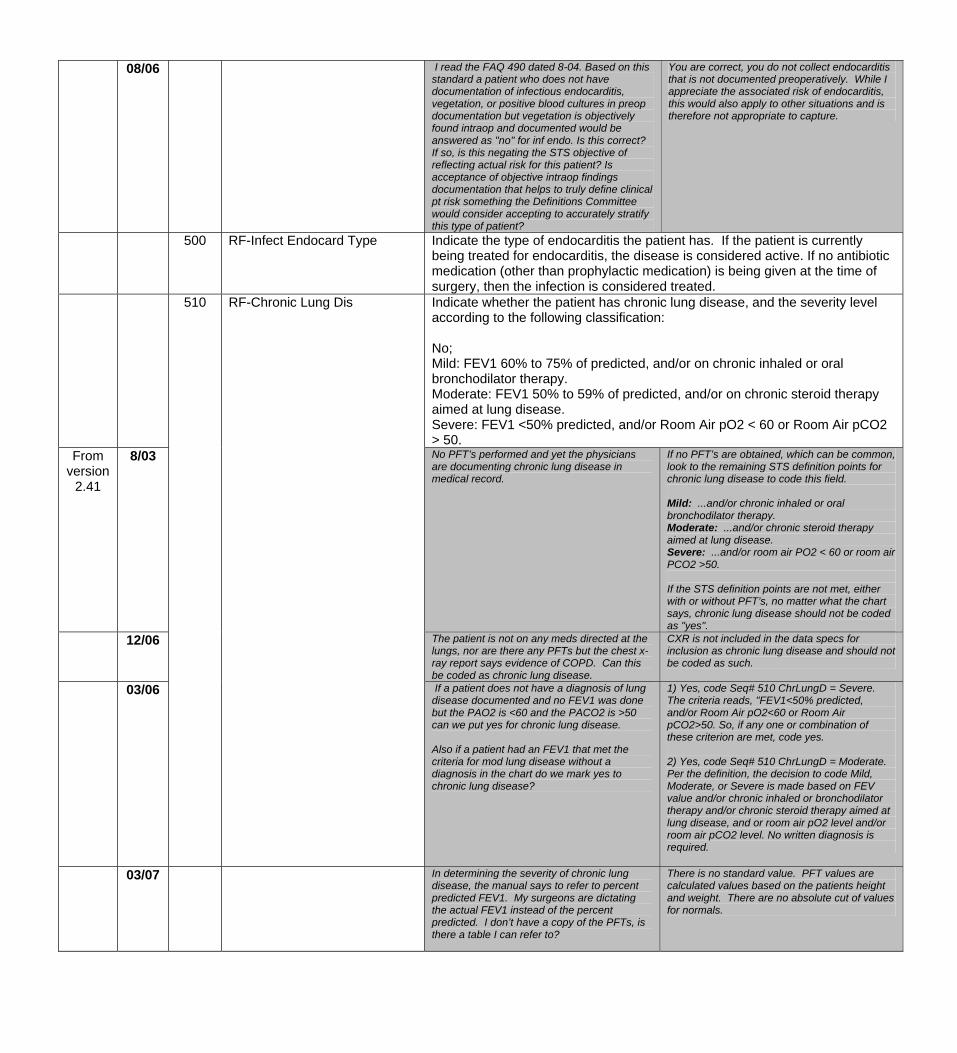
08/06 I read the FAQ 490 dated 8-04. Based on this standard a patient who does not have documentation of infectious endocarditis, vegetation, or positive blood cultures in preop documentation but vegetation is objectively found intraop and documented would be answered as "no" for inf endo. Is this correct? If so, is this negating the STS objective of reflecting actual risk for this patient? Is acceptance of objective intraop findings documentation that helps to truly define clinical pt risk something the Definitions Committee would consider accepting to accurately stratify this type of patient?
You are correct, you do not collect endocarditis that is not documented preoperatively. While I appreciate the associated risk of endocarditis, this would also apply to other situations and is therefore not appropriate to capture.
500 RF-Infect Endocard Type Indicate the type of endocarditis the patient has. If the patient is currently being treated for endocarditis, the disease is considered active. If no antibiotic medication (other than prophylactic medication) is being given at the time of surgery, then the infection is considered treated.
Indicate whether the patient has chronic lung disease, and the severity level according to the following classification: No; Mild: FEV1 60% to 75% of predicted, and/or on chronic inhaled or oral bronchodilator therapy. Moderate: FEV1 50% to 59% of predicted, and/or on chronic steroid therapy aimed at lung disease. Severe: FEV1 <50% predicted, and/or Room Air pO2 < 60 or Room Air pCO2 > 50.
From version
2.41
8/03 No PFT’s performed and yet the physicians are documenting chronic lung disease in medical record.
If no PFT’s are obtained, which can be common, look to the remaining STS definition points for chronic lung disease to code this field. Mild: ...and/or chronic inhaled or oral bronchodilator therapy. Moderate: ...and/or chronic steroid therapy aimed at lung disease. Severe: ...and/or room air PO2 < 60 or room air PCO2 >50. If the STS definition points are not met, either with or without PFT’s, no matter what the chart says, chronic lung disease should not be coded as "yes".
12/06
510 RF-Chronic Lung Dis
The patient is not on any meds directed at the lungs, nor are there any PFTs but the chest x-ray report says evidence of COPD. Can this be coded as chronic lung disease.
CXR is not included in the data specs for inclusion as chronic lung disease and should not be coded as such.
03/06
If a patient does not have a diagnosis of lung disease documented and no FEV1 was done but the PAO2 is <60 and the PACO2 is >50 can we put yes for chronic lung disease. Also if a patient had an FEV1 that met the criteria for mod lung disease without a diagnosis in the chart do we mark yes to chronic lung disease?
1) Yes, code Seq# 510 ChrLungD = Severe. The criteria reads, "FEV1<50% predicted, and/or Room Air pO2<60 or Room Air pCO2>50. So, if any one or combination of these criterion are met, code yes. 2) Yes, code Seq# 510 ChrLungD = Moderate. Per the definition, the decision to code Mild, Moderate, or Severe is made based on FEV value and/or chronic inhaled or bronchodilator therapy and/or chronic steroid therapy aimed at lung disease, and or room air pO2 level and/or room air pCO2 level. No written diagnosis is required.
03/07
In determining the severity of chronic lung disease, the manual says to refer to percent predicted FEV1. My surgeons are dictating the actual FEV1 instead of the percent predicted. I don’t have a copy of the PFTs, is there a table I can refer to?
There is no standard value. PFT values are calculated values based on the patients height and weight. There are no absolute cut of values for normals.
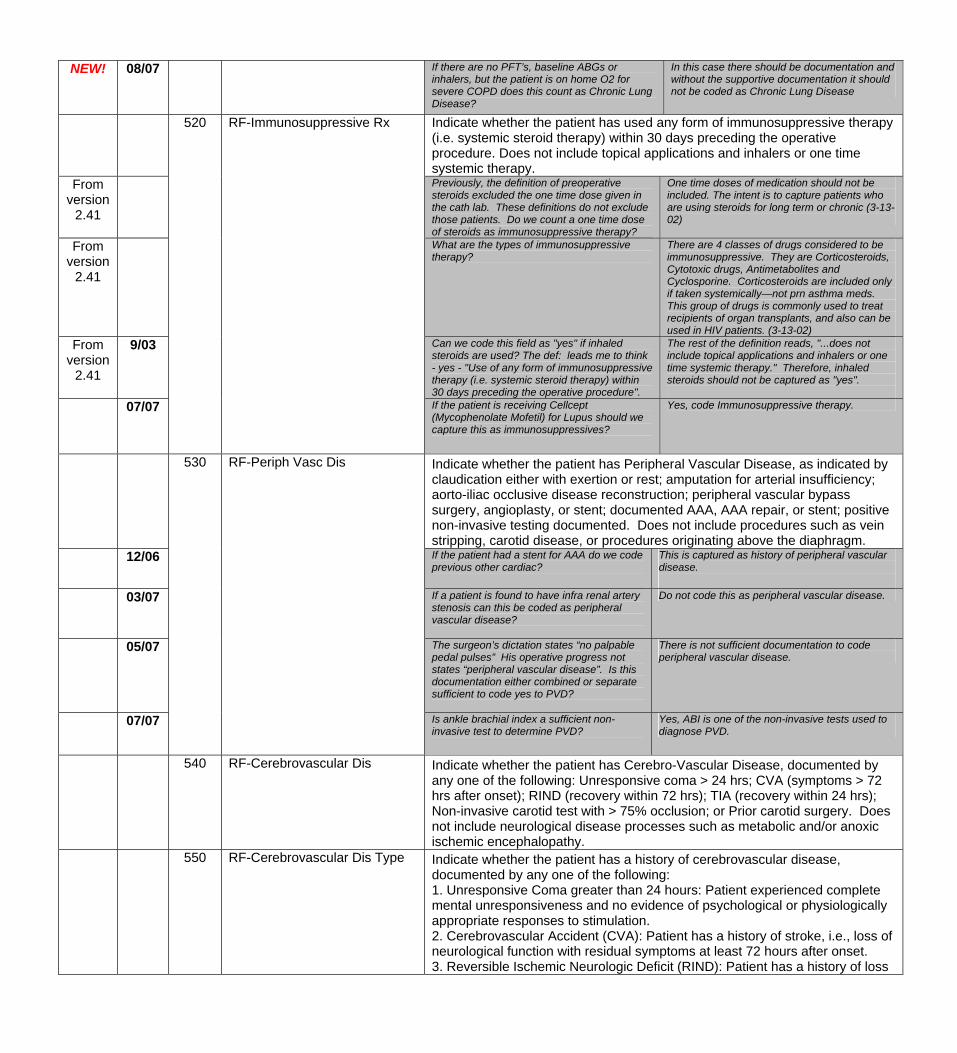
NEW! 08/07 If there are no PFT’s, baseline ABGs or inhalers, but the patient is on home O2 for severe COPD does this count as Chronic Lung Disease?
In this case there should be documentation and without the supportive documentation it should not be coded as Chronic Lung Disease
Indicate whether the patient has used any form of immunosuppressive therapy (i.e. systemic steroid therapy) within 30 days preceding the operative procedure. Does not include topical applications and inhalers or one time systemic therapy.
From version
2.41
Previously, the definition of preoperative steroids excluded the one time dose given in the cath lab. These definitions do not exclude those patients. Do we count a one time dose of steroids as immunosuppressive therapy?
One time doses of medication should not be included. The intent is to capture patients who are using steroids for long term or chronic (3-13-02)
From version
2.41
What are the types of immunosuppressive therapy?
There are 4 classes of drugs considered to be immunosuppressive. They are Corticosteroids, Cytotoxic drugs, Antimetabolites and Cyclosporine. Corticosteroids are included only if taken systemically—not prn asthma meds. This group of drugs is commonly used to treat recipients of organ transplants, and also can be used in HIV patients. (3-13-02)
From version
2.41
9/03
520 RF-Immunosuppressive Rx
Can we code this field as "yes" if inhaled steroids are used? The def: leads me to think - yes - "Use of any form of immunosuppressive therapy (i.e. systemic steroid therapy) within 30 days preceding the operative procedure".
The rest of the definition reads, "...does not include topical applications and inhalers or one time systemic therapy." Therefore, inhaled steroids should not be captured as "yes".
07/07 If the patient is receiving Cellcept (Mycophenolate Mofetil) for Lupus should we capture this as immunosuppressives?
Yes, code Immunosuppressive therapy.
530 RF-Periph Vasc Dis Indicate whether the patient has Peripheral Vascular Disease, as indicated by claudication either with exertion or rest; amputation for arterial insufficiency; aorto-iliac occlusive disease reconstruction; peripheral vascular bypass surgery, angioplasty, or stent; documented AAA, AAA repair, or stent; positive non-invasive testing documented. Does not include procedures such as vein stripping, carotid disease, or procedures originating above the diaphragm.
12/06
If the patient had a stent for AAA do we code previous other cardiac?
This is captured as history of peripheral vascular disease.
03/07
If a patient is found to have infra renal artery stenosis can this be coded as peripheral vascular disease?
Do not code this as peripheral vascular disease.
05/07 The surgeon’s dictation states “no palpable pedal pulses” His operative progress not states “peripheral vascular disease”. Is this documentation either combined or separate sufficient to code yes to PVD?
There is not sufficient documentation to code peripheral vascular disease.
07/07 Is ankle brachial index a sufficient non-invasive test to determine PVD?
Yes, ABI is one of the non-invasive tests used to diagnose PVD.
540 RF-Cerebrovascular Dis Indicate whether the patient has Cerebro-Vascular Disease, documented by any one of the following: Unresponsive coma > 24 hrs; CVA (symptoms > 72 hrs after onset); RIND (recovery within 72 hrs); TIA (recovery within 24 hrs); Non-invasive carotid test with > 75% occlusion; or Prior carotid surgery. Does not include neurological disease processes such as metabolic and/or anoxic ischemic encephalopathy.
550 RF-Cerebrovascular Dis Type Indicate whether the patient has a history of cerebrovascular disease, documented by any one of the following: 1. Unresponsive Coma greater than 24 hours: Patient experienced complete mental unresponsiveness and no evidence of psychological or physiologically appropriate responses to stimulation. 2. Cerebrovascular Accident (CVA): Patient has a history of stroke, i.e., loss of neurological function with residual symptoms at least 72 hours after onset. 3. Reversible Ischemic Neurologic Deficit (RIND): Patient has a history of loss
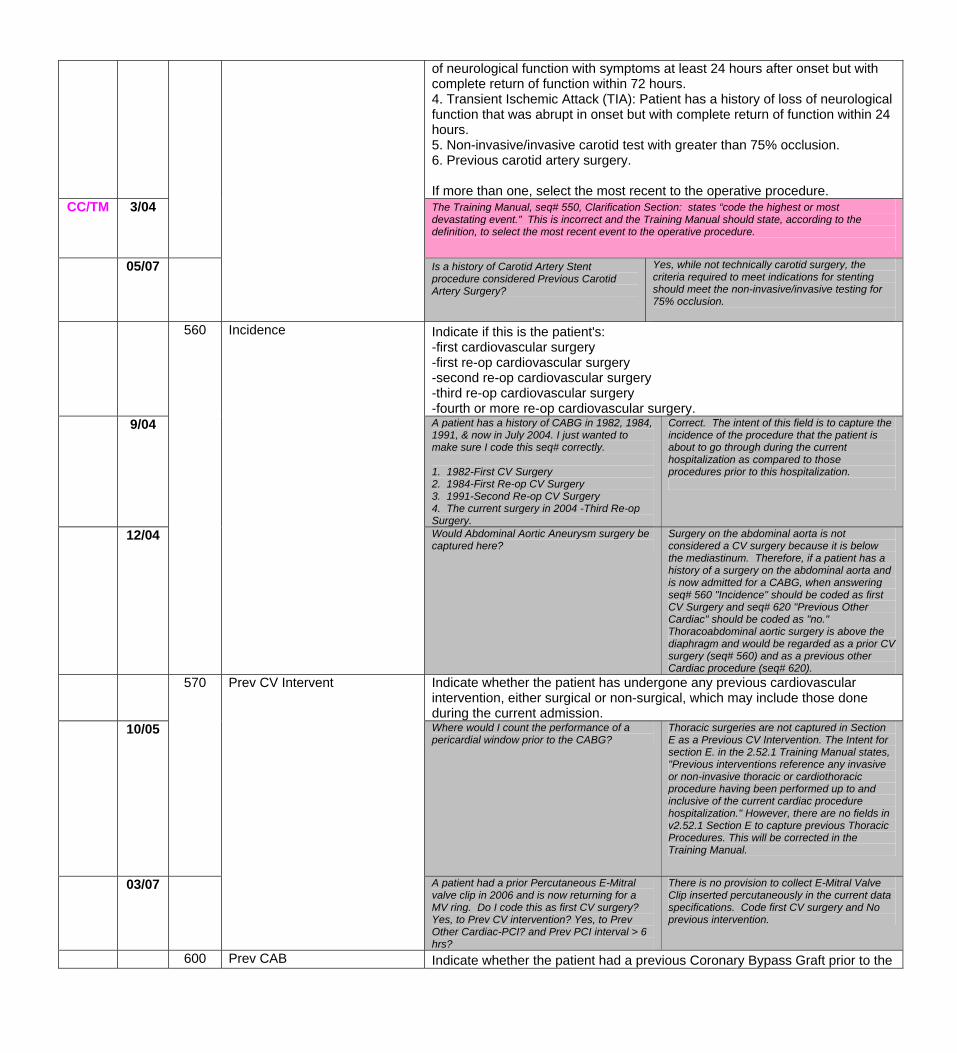
of neurological function with symptoms at least 24 hours after onset but with complete return of function within 72 hours. 4. Transient Ischemic Attack (TIA): Patient has a history of loss of neurological function that was abrupt in onset but with complete return of function within 24 hours. 5. Non-invasive/invasive carotid test with greater than 75% occlusion. 6. Previous carotid artery surgery. If more than one, select the most recent to the operative procedure.
CC/TM
3/04 The Training Manual, seq# 550, Clarification Section: states “code the highest or most devastating event.” This is incorrect and the Training Manual should state, according to the definition, to select the most recent event to the operative procedure.
05/07 Is a history of Carotid Artery Stent procedure considered Previous Carotid Artery Surgery?
Yes, while not technically carotid surgery, the criteria required to meet indications for stenting should meet the non-invasive/invasive testing for 75% occlusion.
Indicate if this is the patient's: -first cardiovascular surgery -first re-op cardiovascular surgery -second re-op cardiovascular surgery -third re-op cardiovascular surgery -fourth or more re-op cardiovascular surgery.
9/04 A patient has a history of CABG in 1982, 1984, 1991, & now in July 2004. I just wanted to make sure I code this seq# correctly. 1. 1982-First CV Surgery 2. 1984-First Re-op CV Surgery 3. 1991-Second Re-op CV Surgery 4. The current surgery in 2004 -Third Re-op Surgery.
Correct. The intent of this field is to capture the incidence of the procedure that the patient is about to go through during the current hospitalization as compared to those procedures prior to this hospitalization.
12/04
560 Incidence
Would Abdominal Aortic Aneurysm surgery be captured here?
Surgery on the abdominal aorta is not considered a CV surgery because it is below the mediastinum. Therefore, if a patient has a history of a surgery on the abdominal aorta and is now admitted for a CABG, when answering seq# 560 "Incidence" should be coded as first CV Surgery and seq# 620 "Previous Other Cardiac" should be coded as "no." Thoracoabdominal aortic surgery is above the diaphragm and would be regarded as a prior CV surgery (seq# 560) and as a previous other Cardiac procedure (seq# 620).
Indicate whether the patient has undergone any previous cardiovascular intervention, either surgical or non-surgical, which may include those done during the current admission.
10/05
570 Prev CV Intervent
Where would I count the performance of a pericardial window prior to the CABG?
Thoracic surgeries are not captured in Section E as a Previous CV Intervention. The Intent for section E. in the 2.52.1 Training Manual states, "Previous interventions reference any invasive or non-invasive thoracic or cardiothoracic procedure having been performed up to and inclusive of the current cardiac procedure hospitalization." However, there are no fields in v2.52.1 Section E to capture previous Thoracic Procedures. This will be corrected in the Training Manual.
03/07
A patient had a prior Percutaneous E-Mitral valve clip in 2006 and is now returning for a MV ring. Do I code this as first CV surgery? Yes, to Prev CV intervention? Yes, to Prev Other Cardiac-PCI? and Prev PCI interval > 6 hrs?
There is no provision to collect E-Mitral Valve Clip inserted percutaneously in the current data specifications. Code first CV surgery and No previous intervention.
600 Prev CAB Indicate whether the patient had a previous Coronary Bypass Graft prior to the
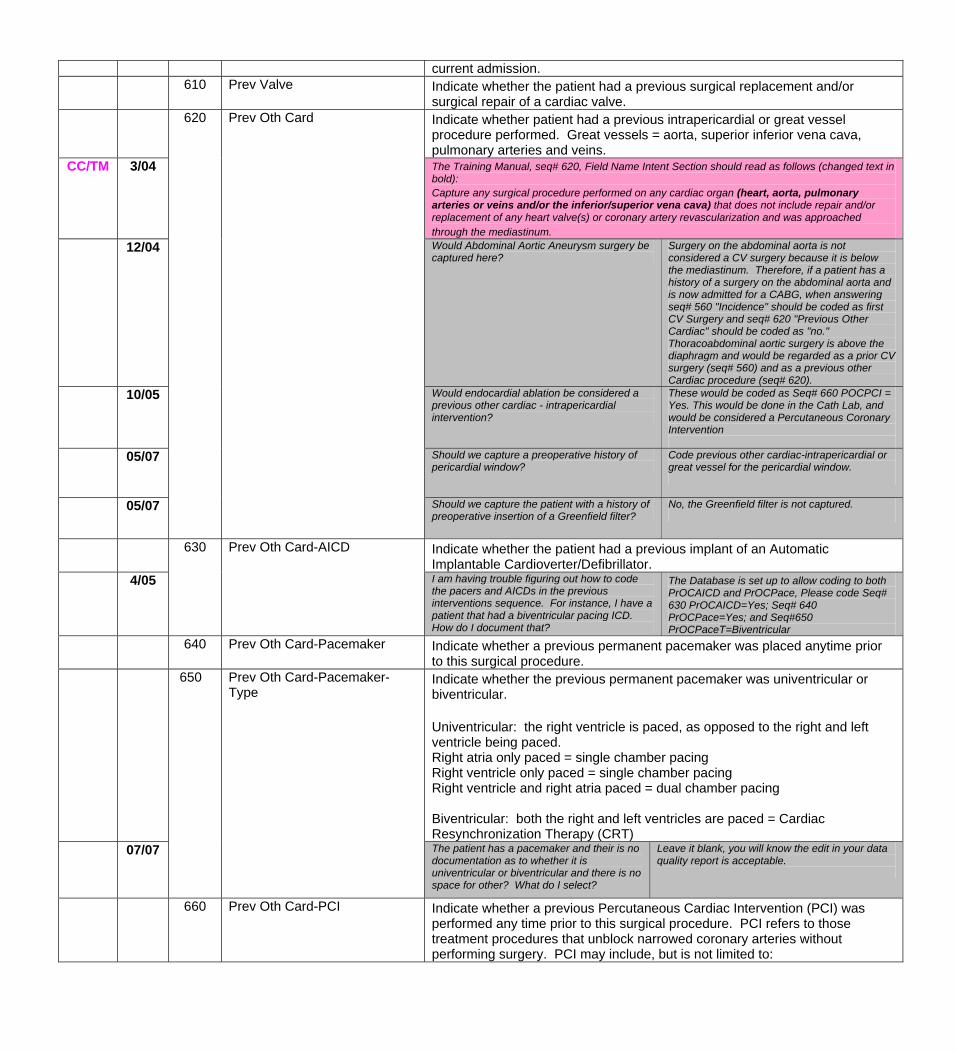
current admission. 610 Prev Valve Indicate whether the patient had a previous surgical replacement and/or
surgical repair of a cardiac valve. Indicate whether patient had a previous intrapericardial or great vessel
procedure performed. Great vessels = aorta, superior inferior vena cava, pulmonary arteries and veins.
CC/TM 3/04 The Training Manual, seq# 620, Field Name Intent Section should read as follows (changed text in bold): Capture any surgical procedure performed on any cardiac organ (heart, aorta, pulmonary arteries or veins and/or the inferior/superior vena cava) that does not include repair and/or replacement of any heart valve(s) or coronary artery revascularization and was approached through the mediastinum.
12/04 Would Abdominal Aortic Aneurysm surgery be captured here?
Surgery on the abdominal aorta is not considered a CV surgery because it is below the mediastinum. Therefore, if a patient has a history of a surgery on the abdominal aorta and is now admitted for a CABG, when answering seq# 560 "Incidence" should be coded as first CV Surgery and seq# 620 "Previous Other Cardiac" should be coded as "no." Thoracoabdominal aortic surgery is above the diaphragm and would be regarded as a prior CV surgery (seq# 560) and as a previous other Cardiac procedure (seq# 620).
10/05
620 Prev Oth Card
Would endocardial ablation be considered a previous other cardiac - intrapericardial intervention?
These would be coded as Seq# 660 POCPCI = Yes. This would be done in the Cath Lab, and would be considered a Percutaneous Coronary Intervention
05/07 Should we capture a preoperative history of pericardial window?
Code previous other cardiac-intrapericardial or great vessel for the pericardial window.
05/07 Should we capture the patient with a history of preoperative insertion of a Greenfield filter?
No, the Greenfield filter is not captured.
Indicate whether the patient had a previous implant of an Automatic Implantable Cardioverter/Defibrillator.
4/05
630 Prev Oth Card-AICD
I am having trouble figuring out how to code the pacers and AICDs in the previous interventions sequence. For instance, I have a patient that had a biventricular pacing ICD. How do I document that?
The Database is set up to allow coding to both PrOCAICD and PrOCPace, Please code Seq# 630 PrOCAICD=Yes; Seq# 640 PrOCPace=Yes; and Seq#650 PrOCPaceT=Biventricular
640 Prev Oth Card-Pacemaker Indicate whether a previous permanent pacemaker was placed anytime prior to this surgical procedure.
650 Prev Oth Card-Pacemaker-Type
Indicate whether the previous permanent pacemaker was univentricular or biventricular. Univentricular: the right ventricle is paced, as opposed to the right and left ventricle being paced. Right atria only paced = single chamber pacing Right ventricle only paced = single chamber pacing Right ventricle and right atria paced = dual chamber pacing Biventricular: both the right and left ventricles are paced = Cardiac Resynchronization Therapy (CRT)
07/07
The patient has a pacemaker and their is no documentation as to whether it is univentricular or biventricular and there is no space for other? What do I select?
Leave it blank, you will know the edit in your data quality report is acceptable.
660 Prev Oth Card-PCI Indicate whether a previous Percutaneous Cardiac Intervention (PCI) was performed any time prior to this surgical procedure. PCI refers to those treatment procedures that unblock narrowed coronary arteries without performing surgery. PCI may include, but is not limited to:
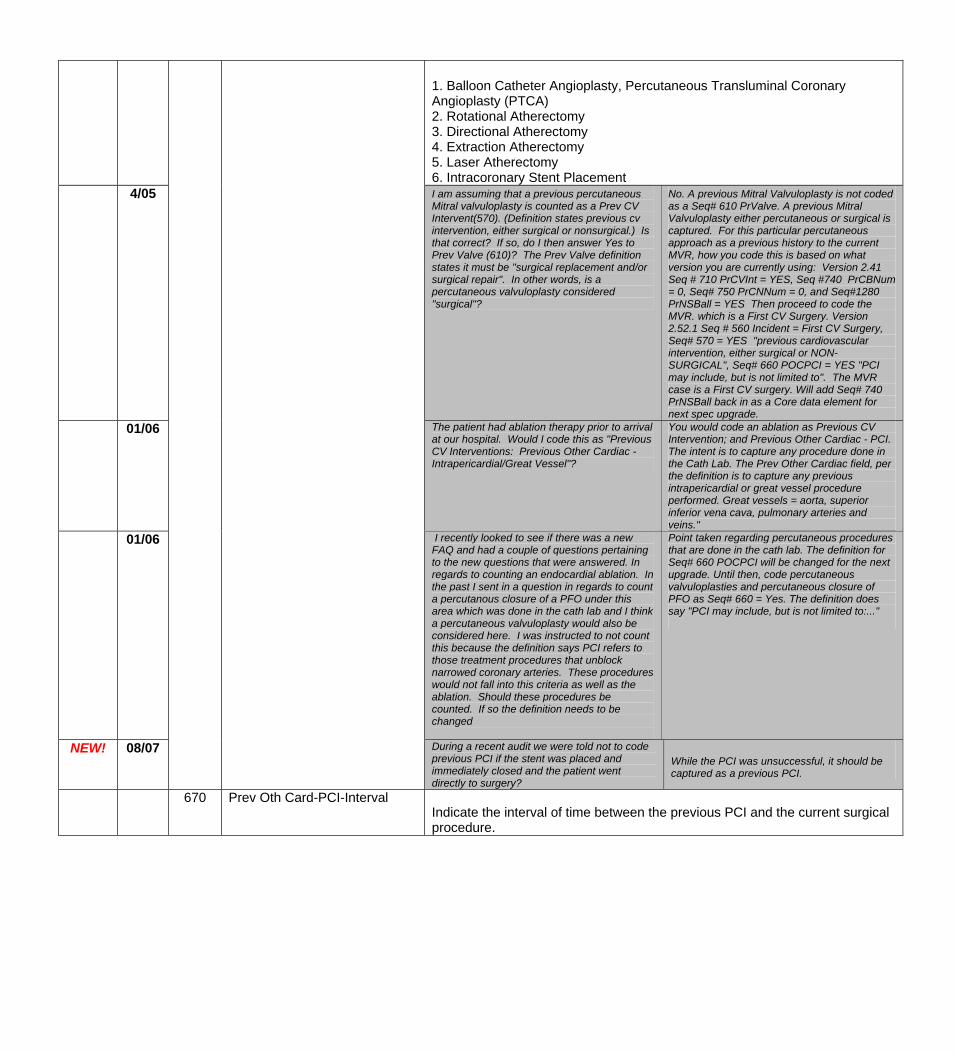
1. Balloon Catheter Angioplasty, Percutaneous Transluminal Coronary Angioplasty (PTCA) 2. Rotational Atherectomy 3. Directional Atherectomy 4. Extraction Atherectomy 5. Laser Atherectomy 6. Intracoronary Stent Placement
4/05 I am assuming that a previous percutaneous Mitral valvuloplasty is counted as a Prev CV Intervent(570). (Definition states previous cv intervention, either surgical or nonsurgical.) Is that correct? If so, do I then answer Yes to Prev Valve (610)? The Prev Valve definition states it must be "surgical replacement and/or surgical repair". In other words, is a percutaneous valvuloplasty considered "surgical"?
No. A previous Mitral Valvuloplasty is not coded as a Seq# 610 PrValve. A previous Mitral Valvuloplasty either percutaneous or surgical is captured. For this particular percutaneous approach as a previous history to the current MVR, how you code this is based on what version you are currently using: Version 2.41 Seq # 710 PrCVInt = YES, Seq #740 PrCBNum = 0, Seq# 750 PrCNNum = 0, and Seq#1280 PrNSBall = YES Then proceed to code the MVR. which is a First CV Surgery. Version 2.52.1 Seq # 560 Incident = First CV Surgery, Seq# 570 = YES "previous cardiovascular intervention, either surgical or NON-SURGICAL", Seq# 660 POCPCI = YES "PCI may include, but is not limited to". The MVR case is a First CV surgery. Will add Seq# 740 PrNSBall back in as a Core data element for next spec upgrade.
01/06 The patient had ablation therapy prior to arrival at our hospital. Would I code this as "Previous CV Interventions: Previous Other Cardiac - Intrapericardial/Great Vessel"?
You would code an ablation as Previous CV Intervention; and Previous Other Cardiac - PCI. The intent is to capture any procedure done in the Cath Lab. The Prev Other Cardiac field, per the definition is to capture any previous intrapericardial or great vessel procedure performed. Great vessels = aorta, superior inferior vena cava, pulmonary arteries and veins."
01/06
I recently looked to see if there was a new FAQ and had a couple of questions pertaining to the new questions that were answered. In regards to counting an endocardial ablation. In the past I sent in a question in regards to count a percutanous closure of a PFO under this area which was done in the cath lab and I think a percutaneous valvuloplasty would also be considered here. I was instructed to not count this because the definition says PCI refers to those treatment procedures that unblock narrowed coronary arteries. These procedures would not fall into this criteria as well as the ablation. Should these procedures be counted. If so the definition needs to be changed
Point taken regarding percutaneous procedures that are done in the cath lab. The definition for Seq# 660 POCPCI will be changed for the next upgrade. Until then, code percutaneous valvuloplasties and percutaneous closure of PFO as Seq# 660 = Yes. The definition does say "PCI may include, but is not limited to:..."
NEW! 08/07 During a recent audit we were told not to code previous PCI if the stent was placed and immediately closed and the patient went directly to surgery?
While the PCI was unsuccessful, it should be captured as a previous PCI.
670 Prev Oth Card-PCI-Interval Indicate the interval of time between the previous PCI and the current surgical procedure.
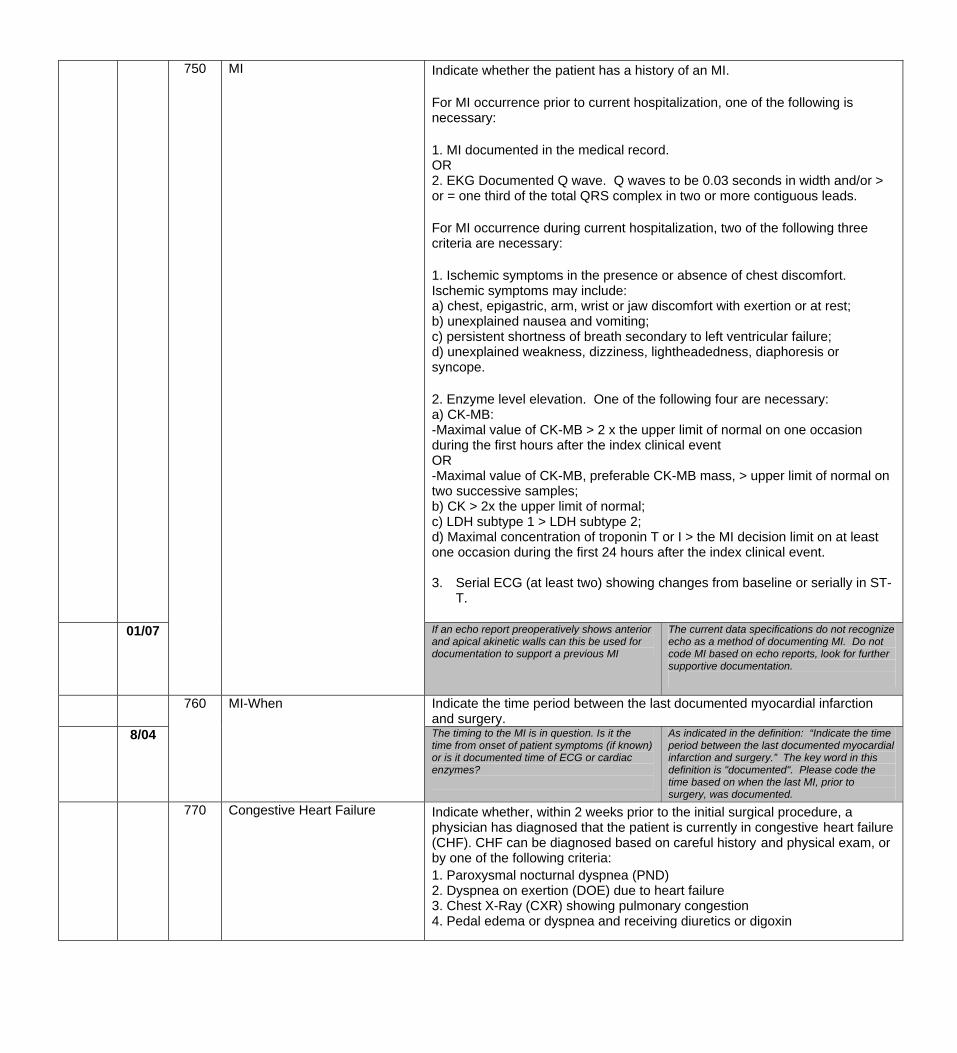
750 MI Indicate whether the patient has a history of an MI. For MI occurrence prior to current hospitalization, one of the following is necessary: 1. MI documented in the medical record. OR 2. EKG Documented Q wave. Q waves to be 0.03 seconds in width and/or > or = one third of the total QRS complex in two or more contiguous leads. For MI occurrence during current hospitalization, two of the following three criteria are necessary: 1. Ischemic symptoms in the presence or absence of chest discomfort. Ischemic symptoms may include: a) chest, epigastric, arm, wrist or jaw discomfort with exertion or at rest; b) unexplained nausea and vomiting; c) persistent shortness of breath secondary to left ventricular failure; d) unexplained weakness, dizziness, lightheadedness, diaphoresis or syncope. 2. Enzyme level elevation. One of the following four are necessary: a) CK-MB: -Maximal value of CK-MB > 2 x the upper limit of normal on one occasion during the first hours after the index clinical event OR -Maximal value of CK-MB, preferable CK-MB mass, > upper limit of normal on two successive samples; b) CK > 2x the upper limit of normal; c) LDH subtype 1 > LDH subtype 2; d) Maximal concentration of troponin T or I > the MI decision limit on at least one occasion during the first 24 hours after the index clinical event. 3. Serial ECG (at least two) showing changes from baseline or serially in ST-
T.
01/07 If an echo report preoperatively shows anterior and apical akinetic walls can this be used for documentation to support a previous MI
The current data specifications do not recognize echo as a method of documenting MI. Do not code MI based on echo reports, look for further supportive documentation.
Indicate the time period between the last documented myocardial infarction and surgery.
8/04
760 MI-When
The timing to the MI is in question. Is it the time from onset of patient symptoms (if known) or is it documented time of ECG or cardiac enzymes?
As indicated in the definition: “Indicate the time period between the last documented myocardial infarction and surgery.” The key word in this definition is "documented". Please code the time based on when the last MI, prior to surgery, was documented.
770 Congestive Heart Failure Indicate whether, within 2 weeks prior to the initial surgical procedure, a physician has diagnosed that the patient is currently in congestive heart failure (CHF). CHF can be diagnosed based on careful history and physical exam, or by one of the following criteria: 1. Paroxysmal nocturnal dyspnea (PND) 2. Dyspnea on exertion (DOE) due to heart failure 3. Chest X-Ray (CXR) showing pulmonary congestion 4. Pedal edema or dyspnea and receiving diuretics or digoxin
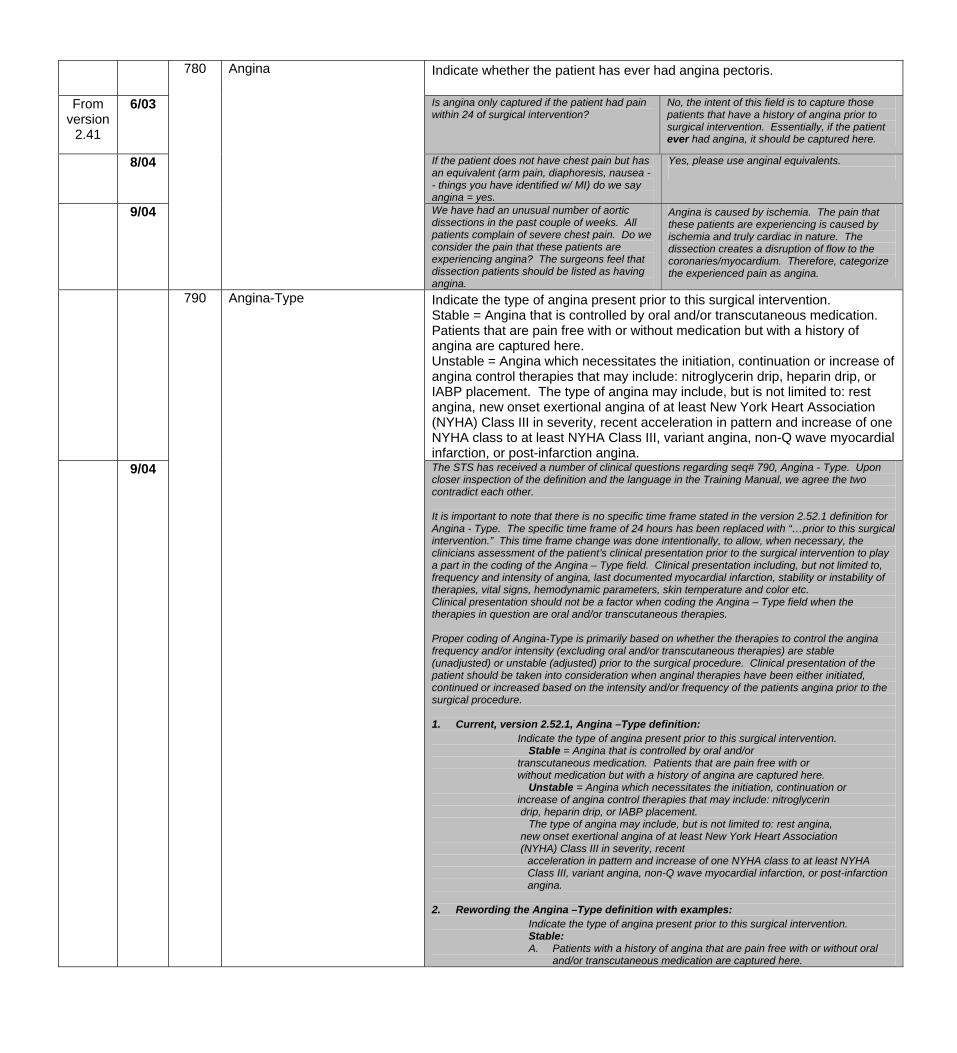
Indicate whether the patient has ever had angina pectoris.
From version
2.41
6/03 Is angina only captured if the patient had pain within 24 of surgical intervention?
No, the intent of this field is to capture those patients that have a history of angina prior to surgical intervention. Essentially, if the patient ever had angina, it should be captured here.
8/04 If the patient does not have chest pain but has an equivalent (arm pain, diaphoresis, nausea -- things you have identified w/ MI) do we say angina = yes.
Yes, please use anginal equivalents.
9/04
780 Angina
We have had an unusual number of aortic dissections in the past couple of weeks. All patients complain of severe chest pain. Do we consider the pain that these patients are experiencing angina? The surgeons feel that dissection patients should be listed as having angina.
Angina is caused by ischemia. The pain that these patients are experiencing is caused by ischemia and truly cardiac in nature. The dissection creates a disruption of flow to the coronaries/myocardium. Therefore, categorize the experienced pain as angina.
Indicate the type of angina present prior to this surgical intervention. Stable = Angina that is controlled by oral and/or transcutaneous medication. Patients that are pain free with or without medication but with a history of angina are captured here. Unstable = Angina which necessitates the initiation, continuation or increase of angina control therapies that may include: nitroglycerin drip, heparin drip, or IABP placement. The type of angina may include, but is not limited to: rest angina, new onset exertional angina of at least New York Heart Association (NYHA) Class III in severity, recent acceleration in pattern and increase of one NYHA class to at least NYHA Class III, variant angina, non-Q wave myocardial infarction, or post-infarction angina.
9/04
790 Angina-Type
The STS has received a number of clinical questions regarding seq# 790, Angina - Type. Upon closer inspection of the definition and the language in the Training Manual, we agree the two contradict each other. It is important to note that there is no specific time frame stated in the version 2.52.1 definition for Angina - Type. The specific time frame of 24 hours has been replaced with “…prior to this surgical intervention.” This time frame change was done intentionally, to allow, when necessary, the clinicians assessment of the patient’s clinical presentation prior to the surgical intervention to play a part in the coding of the Angina – Type field. Clinical presentation including, but not limited to, frequency and intensity of angina, last documented myocardial infarction, stability or instability of therapies, vital signs, hemodynamic parameters, skin temperature and color etc. Clinical presentation should not be a factor when coding the Angina – Type field when the therapies in question are oral and/or transcutaneous therapies. Proper coding of Angina-Type is primarily based on whether the therapies to control the angina frequency and/or intensity (excluding oral and/or transcutaneous therapies) are stable (unadjusted) or unstable (adjusted) prior to the surgical procedure. Clinical presentation of the patient should be taken into consideration when anginal therapies have been either initiated, continued or increased based on the intensity and/or frequency of the patients angina prior to the surgical procedure. 1. Current, version 2.52.1, Angina –Type definition: Indicate the type of angina present prior to this surgical intervention. Stable = Angina that is controlled by oral and/or transcutaneous medication. Patients that are pain free with or without medication but with a history of angina are captured here. Unstable = Angina which necessitates the initiation, continuation or increase of angina control therapies that may include: nitroglycerin drip, heparin drip, or IABP placement. The type of angina may include, but is not limited to: rest angina, new onset exertional angina of at least New York Heart Association (NYHA) Class III in severity, recent
acceleration in pattern and increase of one NYHA class to at least NYHA Class III, variant angina, non-Q wave myocardial infarction, or post-infarction angina.
2. Rewording the Angina –Type definition with examples: Indicate the type of angina present prior to this surgical intervention. Stable:
A. Patients with a history of angina that are pain free with or without oral and/or transcutaneous medication are captured here.
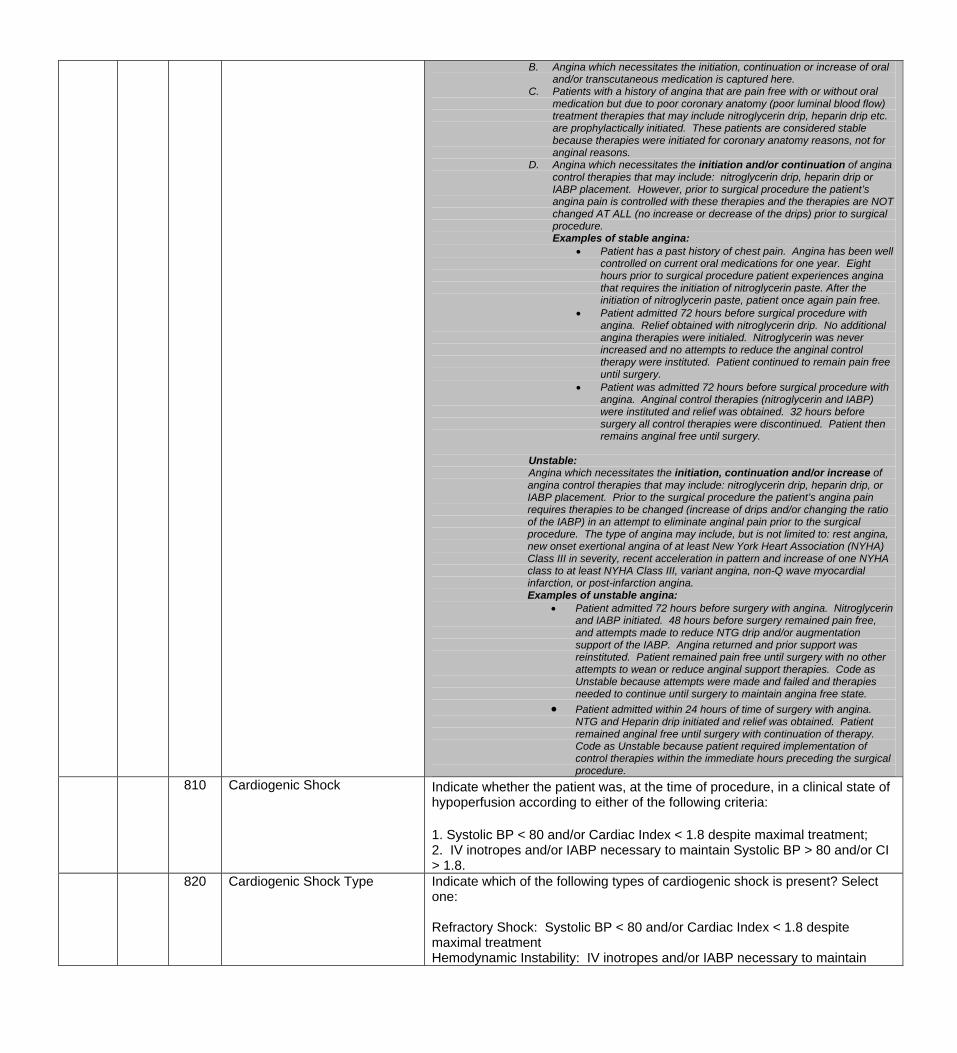
B. Angina which necessitates the initiation, continuation or increase of oral and/or transcutaneous medication is captured here.
C. Patients with a history of angina that are pain free with or without oral medication but due to poor coronary anatomy (poor luminal blood flow) treatment therapies that may include nitroglycerin drip, heparin drip etc. are prophylactically initiated. These patients are considered stable because therapies were initiated for coronary anatomy reasons, not for anginal reasons.
D. Angina which necessitates the initiation and/or continuation of angina control therapies that may include: nitroglycerin drip, heparin drip or IABP placement. However, prior to surgical procedure the patient’s angina pain is controlled with these therapies and the therapies are NOT changed AT ALL (no increase or decrease of the drips) prior to surgical procedure. Examples of stable angina:
• Patient has a past history of chest pain. Angina has been well controlled on current oral medications for one year. Eight hours prior to surgical procedure patient experiences angina that requires the initiation of nitroglycerin paste. After the initiation of nitroglycerin paste, patient once again pain free.
• Patient admitted 72 hours before surgical procedure with angina. Relief obtained with nitroglycerin drip. No additional angina therapies were initialed. Nitroglycerin was never increased and no attempts to reduce the anginal control therapy were instituted. Patient continued to remain pain free until surgery.
• Patient was admitted 72 hours before surgical procedure with angina. Anginal control therapies (nitroglycerin and IABP) were instituted and relief was obtained. 32 hours before surgery all control therapies were discontinued. Patient then remains anginal free until surgery.
Unstable:
Angina which necessitates the initiation, continuation and/or increase of angina control therapies that may include: nitroglycerin drip, heparin drip, or IABP placement. Prior to the surgical procedure the patient’s angina pain requires therapies to be changed (increase of drips and/or changing the ratio of the IABP) in an attempt to eliminate anginal pain prior to the surgical procedure. The type of angina may include, but is not limited to: rest angina, new onset exertional angina of at least New York Heart Association (NYHA) Class III in severity, recent acceleration in pattern and increase of one NYHA class to at least NYHA Class III, variant angina, non-Q wave myocardial infarction, or post-infarction angina. Examples of unstable angina:
• Patient admitted 72 hours before surgery with angina. Nitroglycerin and IABP initiated. 48 hours before surgery remained pain free, and attempts made to reduce NTG drip and/or augmentation support of the IABP. Angina returned and prior support was reinstituted. Patient remained pain free until surgery with no other attempts to wean or reduce anginal support therapies. Code as Unstable because attempts were made and failed and therapies needed to continue until surgery to maintain angina free state.
• Patient admitted within 24 hours of time of surgery with angina. NTG and Heparin drip initiated and relief was obtained. Patient remained anginal free until surgery with continuation of therapy. Code as Unstable because patient required implementation of control therapies within the immediate hours preceding the surgical procedure.
810 Cardiogenic Shock Indicate whether the patient was, at the time of procedure, in a clinical state of hypoperfusion according to either of the following criteria: 1. Systolic BP < 80 and/or Cardiac Index < 1.8 despite maximal treatment; 2. IV inotropes and/or IABP necessary to maintain Systolic BP > 80 and/or CI > 1.8.
820 Cardiogenic Shock Type Indicate which of the following types of cardiogenic shock is present? Select one: Refractory Shock: Systolic BP < 80 and/or Cardiac Index < 1.8 despite maximal treatment Hemodynamic Instability: IV inotropes and/or IABP necessary to maintain
Systolic BP > 80 and CI > 1.8.
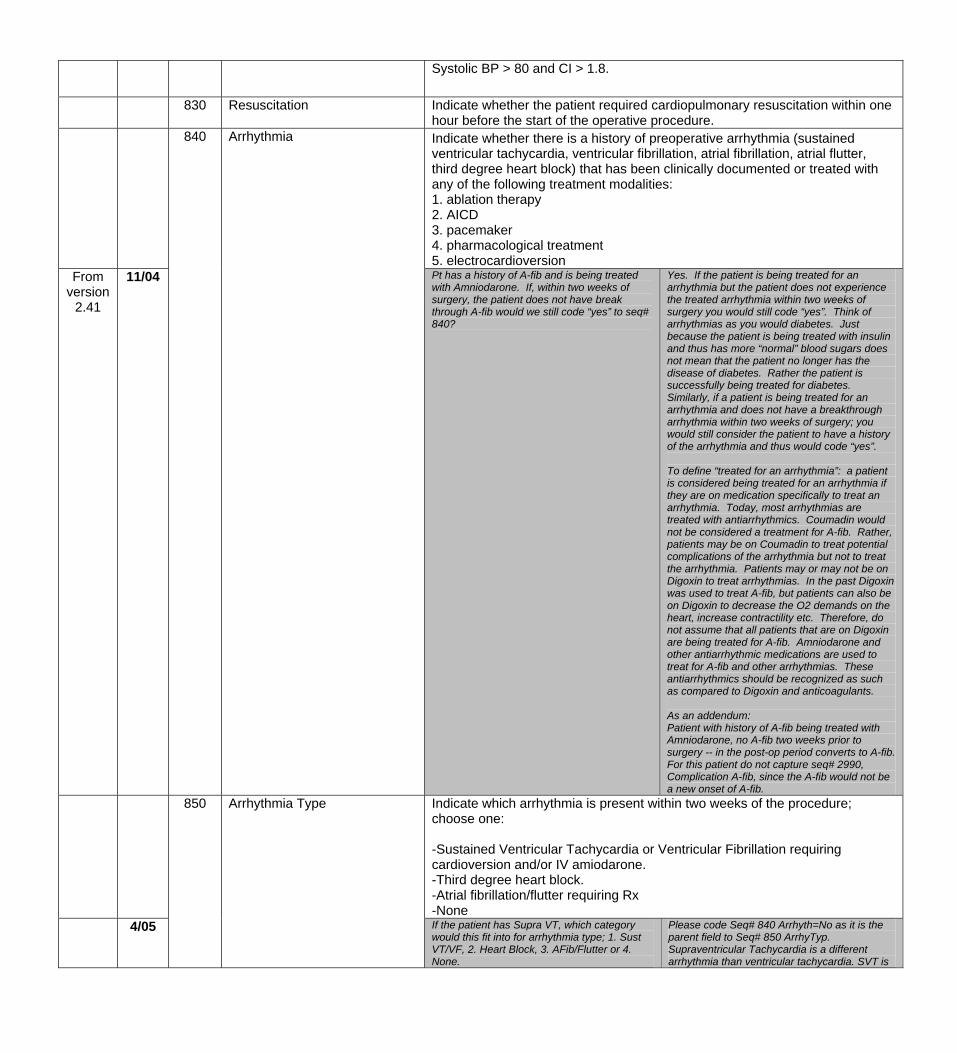
830 Resuscitation Indicate whether the patient required cardiopulmonary resuscitation within one hour before the start of the operative procedure.
Indicate whether there is a history of preoperative arrhythmia (sustained ventricular tachycardia, ventricular fibrillation, atrial fibrillation, atrial flutter, third degree heart block) that has been clinically documented or treated with any of the following treatment modalities: 1. ablation therapy 2. AICD 3. pacemaker 4. pharmacological treatment 5. electrocardioversion
From version
2.41
11/04
840 Arrhythmia
Pt has a history of A-fib and is being treated with Amniodarone. If, within two weeks of surgery, the patient does not have break through A-fib would we still code “yes” to seq# 840?
Yes. If the patient is being treated for an arrhythmia but the patient does not experience the treated arrhythmia within two weeks of surgery you would still code “yes”. Think of arrhythmias as you would diabetes. Just because the patient is being treated with insulin and thus has more “normal” blood sugars does not mean that the patient no longer has the disease of diabetes. Rather the patient is successfully being treated for diabetes. Similarly, if a patient is being treated for an arrhythmia and does not have a breakthrough arrhythmia within two weeks of surgery; you would still consider the patient to have a history of the arrhythmia and thus would code “yes”. To define “treated for an arrhythmia”: a patient is considered being treated for an arrhythmia if they are on medication specifically to treat an arrhythmia. Today, most arrhythmias are treated with antiarrhythmics. Coumadin would not be considered a treatment for A-fib. Rather, patients may be on Coumadin to treat potential complications of the arrhythmia but not to treat the arrhythmia. Patients may or may not be on Digoxin to treat arrhythmias. In the past Digoxin was used to treat A-fib, but patients can also be on Digoxin to decrease the O2 demands on the heart, increase contractility etc. Therefore, do not assume that all patients that are on Digoxin are being treated for A-fib. Amniodarone and other antiarrhythmic medications are used to treat for A-fib and other arrhythmias. These antiarrhythmics should be recognized as such as compared to Digoxin and anticoagulants. As an addendum: Patient with history of A-fib being treated with Amniodarone, no A-fib two weeks prior to surgery -- in the post-op period converts to A-fib. For this patient do not capture seq# 2990, Complication A-fib, since the A-fib would not be a new onset of A-fib.
Indicate which arrhythmia is present within two weeks of the procedure; choose one: -Sustained Ventricular Tachycardia or Ventricular Fibrillation requiring cardioversion and/or IV amiodarone. -Third degree heart block. -Atrial fibrillation/flutter requiring Rx -None
4/05
850 Arrhythmia Type
If the patient has Supra VT, which category would this fit into for arrhythmia type; 1. Sust VT/VF, 2. Heart Block, 3. AFib/Flutter or 4. None.
Please code Seq# 840 Arrhyth=No as it is the parent field to Seq# 850 ArrhyTyp. Supraventricular Tachycardia is a different arrhythmia than ventricular tachycardia. SVT is
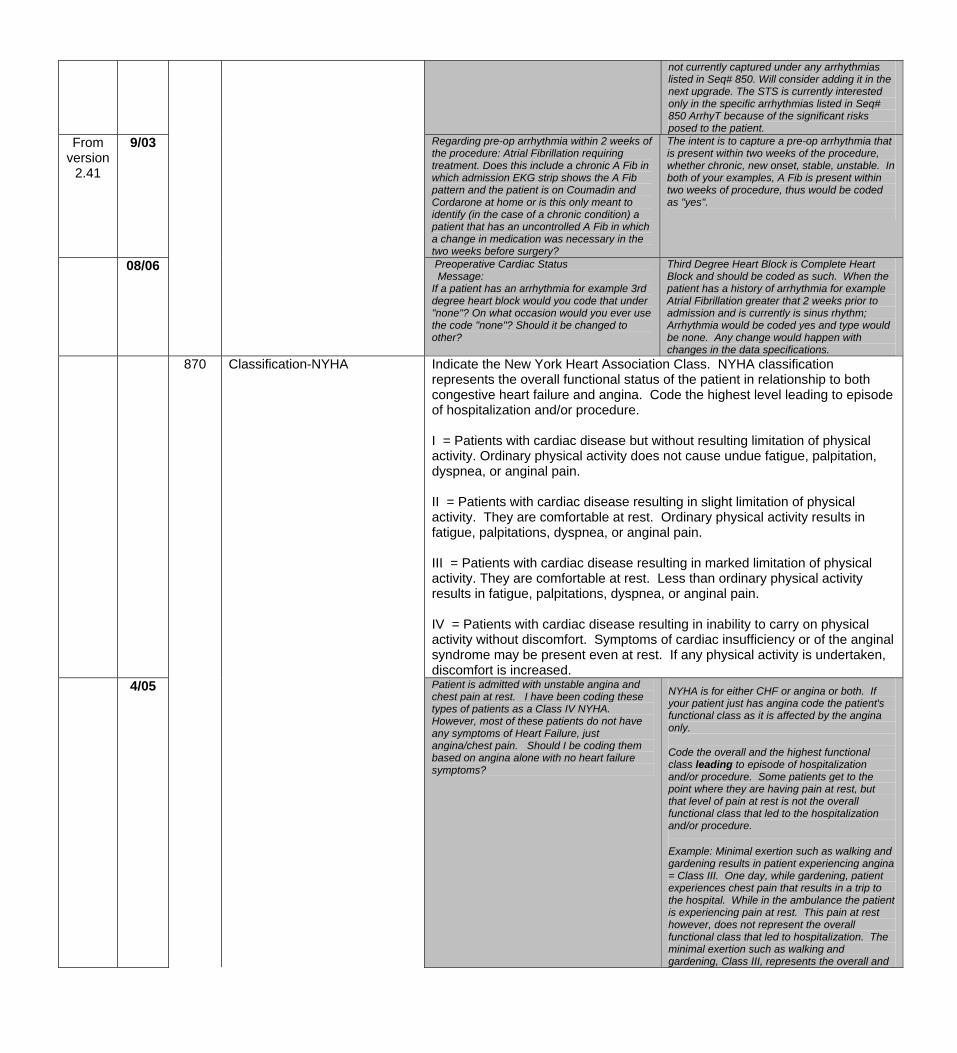
not currently captured under any arrhythmias listed in Seq# 850. Will consider adding it in the next upgrade. The STS is currently interested only in the specific arrhythmias listed in Seq# 850 ArrhyT because of the significant risks posed to the patient.
From version
2.41
9/03 Regarding pre-op arrhythmia within 2 weeks of the procedure: Atrial Fibrillation requiring treatment. Does this include a chronic A Fib in which admission EKG strip shows the A Fib pattern and the patient is on Coumadin and Cordarone at home or is this only meant to identify (in the case of a chronic condition) a patient that has an uncontrolled A Fib in which a change in medication was necessary in the two weeks before surgery?
The intent is to capture a pre-op arrhythmia that is present within two weeks of the procedure, whether chronic, new onset, stable, unstable. In both of your examples, A Fib is present within two weeks of procedure, thus would be coded as "yes".
08/06 Preoperative Cardiac Status Message: If a patient has an arrhythmia for example 3rd degree heart block would you code that under "none"? On what occasion would you ever use the code "none"? Should it be changed to other?
Third Degree Heart Block is Complete Heart Block and should be coded as such. When the patient has a history of arrhythmia for example Atrial Fibrillation greater that 2 weeks prior to admission and is currently is sinus rhythm; Arrhythmia would be coded yes and type would be none. Any change would happen with changes in the data specifications.
Indicate the New York Heart Association Class. NYHA classification represents the overall functional status of the patient in relationship to both congestive heart failure and angina. Code the highest level leading to episode of hospitalization and/or procedure. I = Patients with cardiac disease but without resulting limitation of physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, dyspnea, or anginal pain. II = Patients with cardiac disease resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity results in fatigue, palpitations, dyspnea, or anginal pain. III = Patients with cardiac disease resulting in marked limitation of physical activity. They are comfortable at rest. Less than ordinary physical activity results in fatigue, palpitations, dyspnea, or anginal pain. IV = Patients with cardiac disease resulting in inability to carry on physical activity without discomfort. Symptoms of cardiac insufficiency or of the anginal syndrome may be present even at rest. If any physical activity is undertaken, discomfort is increased.
4/05
870 Classification-NYHA
Patient is admitted with unstable angina and chest pain at rest. I have been coding these types of patients as a Class IV NYHA. However, most of these patients do not have any symptoms of Heart Failure, just angina/chest pain. Should I be coding them based on angina alone with no heart failure symptoms?
NYHA is for either CHF or angina or both. If your patient just has angina code the patient's functional class as it is affected by the angina only. Code the overall and the highest functional class leading to episode of hospitalization and/or procedure. Some patients get to the point where they are having pain at rest, but that level of pain at rest is not the overall functional class that led to the hospitalization and/or procedure.
Example: Minimal exertion such as walking and gardening results in patient experiencing angina = Class III. One day, while gardening, patient experiences chest pain that results in a trip to the hospital. While in the ambulance the patient is experiencing pain at rest. This pain at rest however, does not represent the overall functional class that led to hospitalization. The minimal exertion such as walking and gardening, Class III, represents the overall and
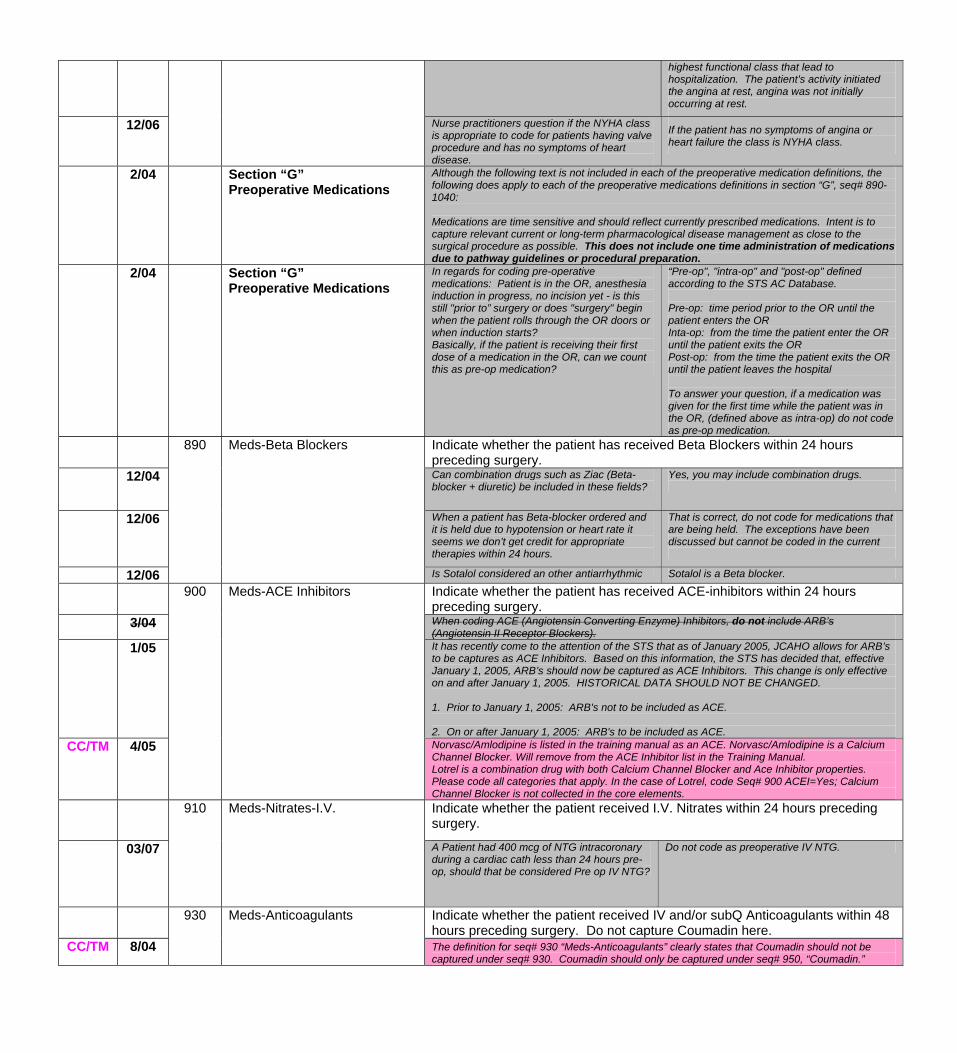
highest functional class that lead to hospitalization. The patient's activity initiated the angina at rest, angina was not initially occurring at rest.
12/06 Nurse practitioners question if the NYHA class is appropriate to code for patients having valve procedure and has no symptoms of heart disease.
If the patient has no symptoms of angina or heart failure the class is NYHA class.
2/04 Section “G” Preoperative Medications
Although the following text is not included in each of the preoperative medication definitions, the following does apply to each of the preoperative medications definitions in section “G”, seq# 890-1040: Medications are time sensitive and should reflect currently prescribed medications. Intent is to capture relevant current or long-term pharmacological disease management as close to the surgical procedure as possible. This does not include one time administration of medications due to pathway guidelines or procedural preparation.
2/04 Section “G” Preoperative Medications
In regards for coding pre-operative medications: Patient is in the OR, anesthesia induction in progress, no incision yet - is this still "prior to” surgery or does "surgery" begin when the patient rolls through the OR doors or when induction starts? Basically, if the patient is receiving their first dose of a medication in the OR, can we count this as pre-op medication?
“Pre-op", "intra-op" and "post-op" defined according to the STS AC Database. Pre-op: time period prior to the OR until the patient enters the OR Inta-op: from the time the patient enter the OR until the patient exits the OR Post-op: from the time the patient exits the OR until the patient leaves the hospital To answer your question, if a medication was given for the first time while the patient was in the OR, (defined above as intra-op) do not code as pre-op medication.
Indicate whether the patient has received Beta Blockers within 24 hours preceding surgery.
12/04
890 Meds-Beta Blockers
Can combination drugs such as Ziac (Beta-blocker + diuretic) be included in these fields?
Yes, you may include combination drugs.
12/06 When a patient has Beta-blocker ordered and it is held due to hypotension or heart rate it seems we don’t get credit for appropriate therapies within 24 hours.
That is correct, do not code for medications that are being held. The exceptions have been discussed but cannot be coded in the current
12/06 Is Sotalol considered an other antiarrhythmic Sotalol is a Beta blocker. Indicate whether the patient has received ACE-inhibitors within 24 hours
preceding surgery. 3/04 When coding ACE (Angiotensin Converting Enzyme) Inhibitors, do not include ARB’s
(Angiotensin II Receptor Blockers). 1/05
900 Meds-ACE Inhibitors
It has recently come to the attention of the STS that as of January 2005, JCAHO allows for ARB’s to be captures as ACE Inhibitors. Based on this information, the STS has decided that, effective January 1, 2005, ARB’s should now be captured as ACE Inhibitors. This change is only effective on and after January 1, 2005. HISTORICAL DATA SHOULD NOT BE CHANGED. 1. Prior to January 1, 2005: ARB's not to be included as ACE. 2. On or after January 1, 2005: ARB's to be included as ACE.
CC/TM 4/05 Norvasc/Amlodipine is listed in the training manual as an ACE. Norvasc/Amlodipine is a Calcium Channel Blocker. Will remove from the ACE Inhibitor list in the Training Manual. Lotrel is a combination drug with both Calcium Channel Blocker and Ace Inhibitor properties. Please code all categories that apply. In the case of Lotrel, code Seq# 900 ACEI=Yes; Calcium Channel Blocker is not collected in the core elements.
910
Meds-Nitrates-I.V. Indicate whether the patient received I.V. Nitrates within 24 hours preceding surgery.
03/07 A Patient had 400 mcg of NTG intracoronary during a cardiac cath less than 24 hours pre- op, should that be considered Pre op IV NTG?
Do not code as preoperative IV NTG.
Indicate whether the patient received IV and/or subQ Anticoagulants within 48 hours preceding surgery. Do not capture Coumadin here.
CC/TM 8/04
930 Meds-Anticoagulants
The definition for seq# 930 “Meds-Anticoagulants” clearly states that Coumadin should not be captured under seq# 930. Coumadin should only be captured under seq# 950, “Coumadin.”
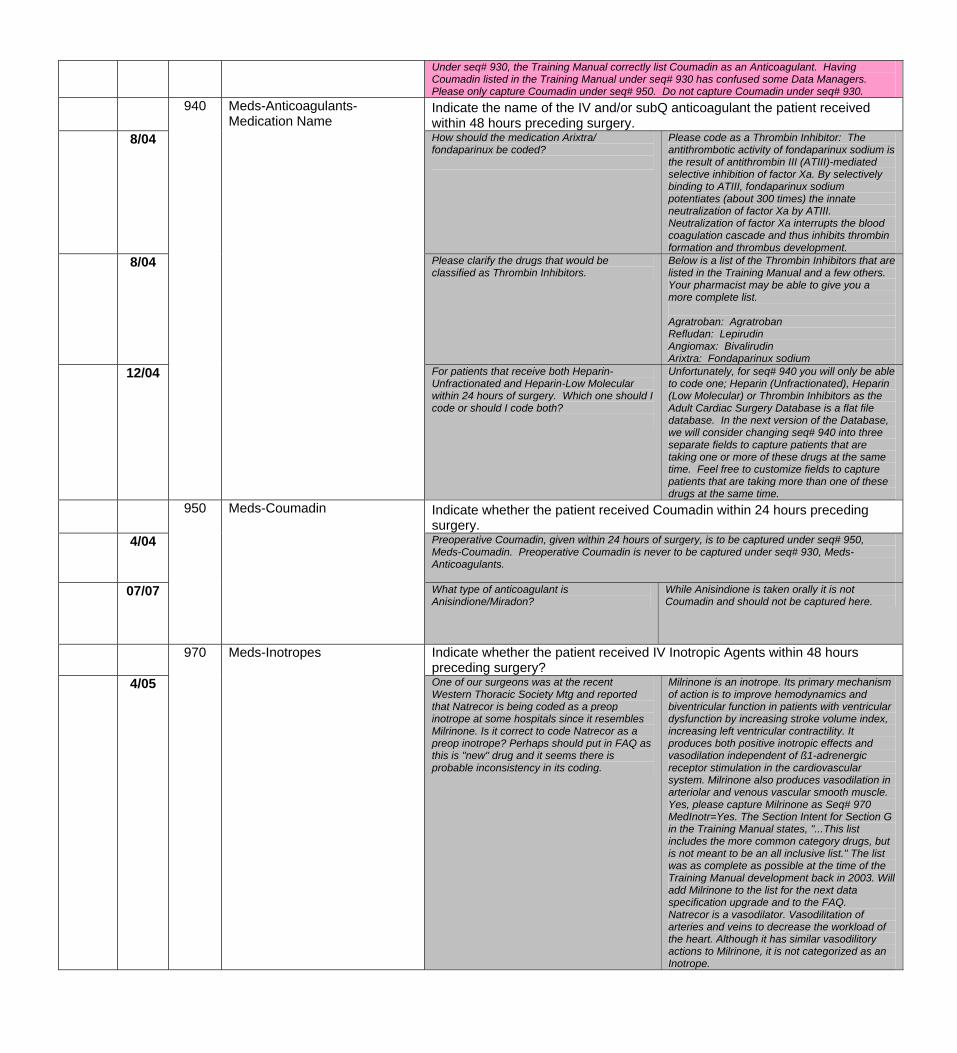
Under seq# 930, the Training Manual correctly list Coumadin as an Anticoagulant. Having Coumadin listed in the Training Manual under seq# 930 has confused some Data Managers. Please only capture Coumadin under seq# 950. Do not capture Coumadin under seq# 930.
Indicate the name of the IV and/or subQ anticoagulant the patient received within 48 hours preceding surgery.
8/04 How should the medication Arixtra/ fondaparinux be coded?
Please code as a Thrombin Inhibitor: The antithrombotic activity of fondaparinux sodium is the result of antithrombin III (ATIII)-mediated selective inhibition of factor Xa. By selectively binding to ATIII, fondaparinux sodium potentiates (about 300 times) the innate neutralization of factor Xa by ATIII. Neutralization of factor Xa interrupts the blood coagulation cascade and thus inhibits thrombin formation and thrombus development.
8/04 Please clarify the drugs that would be classified as Thrombin Inhibitors.
Below is a list of the Thrombin Inhibitors that are listed in the Training Manual and a few others. Your pharmacist may be able to give you a more complete list. Agratroban: Agratroban Refludan: Lepirudin Angiomax: Bivalirudin Arixtra: Fondaparinux sodium
12/04
940 Meds-Anticoagulants-Medication Name
For patients that receive both Heparin-Unfractionated and Heparin-Low Molecular within 24 hours of surgery. Which one should I code or should I code both?
Unfortunately, for seq# 940 you will only be able to code one; Heparin (Unfractionated), Heparin (Low Molecular) or Thrombin Inhibitors as the Adult Cardiac Surgery Database is a flat file database. In the next version of the Database, we will consider changing seq# 940 into three separate fields to capture patients that are taking one or more of these drugs at the same time. Feel free to customize fields to capture patients that are taking more than one of these drugs at the same time.
Indicate whether the patient received Coumadin within 24 hours preceding surgery.
4/04
950 Meds-Coumadin
Preoperative Coumadin, given within 24 hours of surgery, is to be captured under seq# 950, Meds-Coumadin. Preoperative Coumadin is never to be captured under seq# 930, Meds-Anticoagulants.
07/07 What type of anticoagulant is Anisindione/Miradon?
While Anisindione is taken orally it is not Coumadin and should not be captured here.
Indicate whether the patient received IV Inotropic Agents within 48 hours preceding surgery?
4/05
970 Meds-Inotropes
One of our surgeons was at the recent Western Thoracic Society Mtg and reported that Natrecor is being coded as a preop inotrope at some hospitals since it resembles Milrinone. Is it correct to code Natrecor as a preop inotrope? Perhaps should put in FAQ as this is "new" drug and it seems there is probable inconsistency in its coding.
Milrinone is an inotrope. Its primary mechanism of action is to improve hemodynamics and biventricular function in patients with ventricular dysfunction by increasing stroke volume index, increasing left ventricular contractility. It produces both positive inotropic effects and vasodilation independent of ß1-adrenergic receptor stimulation in the cardiovascular system. Milrinone also produces vasodilation in arteriolar and venous vascular smooth muscle. Yes, please capture Milrinone as Seq# 970 MedInotr=Yes. The Section Intent for Section G in the Training Manual states, "...This list includes the more common category drugs, but is not meant to be an all inclusive list." The list was as complete as possible at the time of the Training Manual development back in 2003. Will add Milrinone to the list for the next data specification upgrade and to the FAQ. Natrecor is a vasodilator. Vasodilitation of arteries and veins to decrease the workload of the heart. Although it has similar vasodilitory actions to Milrinone, it is not categorized as an Inotrope.
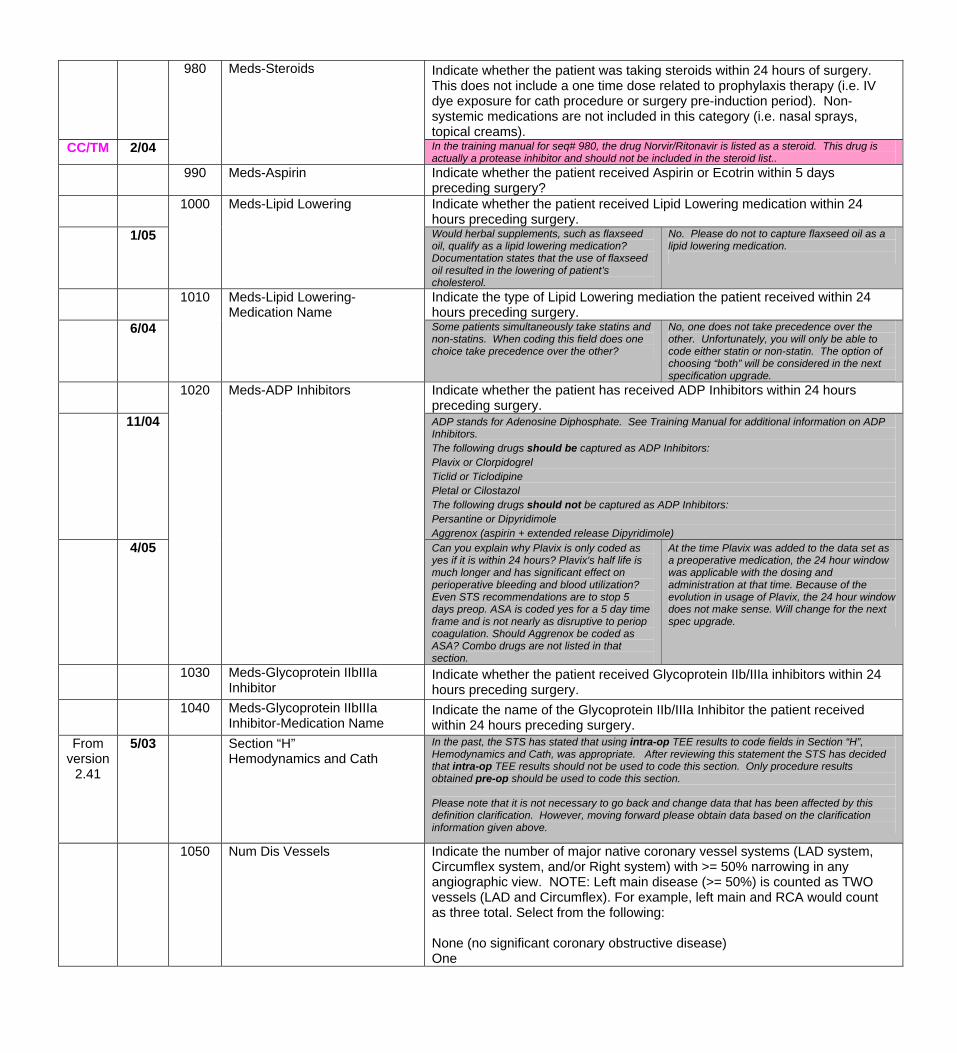
Indicate whether the patient was taking steroids within 24 hours of surgery. This does not include a one time dose related to prophylaxis therapy (i.e. IV dye exposure for cath procedure or surgery pre-induction period). Non-systemic medications are not included in this category (i.e. nasal sprays, topical creams).
CC/TM 2/04
980 Meds-Steroids
In the training manual for seq# 980, the drug Norvir/Ritonavir is listed as a steroid. This drug is actually a protease inhibitor and should not be included in the steroid list..
990 Meds-Aspirin Indicate whether the patient received Aspirin or Ecotrin within 5 days preceding surgery?
Indicate whether the patient received Lipid Lowering medication within 24 hours preceding surgery.
1/05
1000 Meds-Lipid Lowering
Would herbal supplements, such as flaxseed oil, qualify as a lipid lowering medication? Documentation states that the use of flaxseed oil resulted in the lowering of patient’s cholesterol.
No. Please do not to capture flaxseed oil as a lipid lowering medication.
Indicate the type of Lipid Lowering mediation the patient received within 24 hours preceding surgery.
6/04
1010 Meds-Lipid Lowering-Medication Name
Some patients simultaneously take statins and non-statins. When coding this field does one choice take precedence over the other?
No, one does not take precedence over the other. Unfortunately, you will only be able to code either statin or non-statin. The option of choosing “both” will be considered in the next specification upgrade.
Indicate whether the patient has received ADP Inhibitors within 24 hours preceding surgery.
11/04 ADP stands for Adenosine Diphosphate. See Training Manual for additional information on ADP Inhibitors. The following drugs should be captured as ADP Inhibitors: Plavix or Clorpidogrel Ticlid or Ticlodipine Pletal or Cilostazol The following drugs should not be captured as ADP Inhibitors: Persantine or Dipyridimole Aggrenox (aspirin + extended release Dipyridimole)
4/05
1020 Meds-ADP Inhibitors
Can you explain why Plavix is only coded as yes if it is within 24 hours? Plavix's half life is much longer and has significant effect on perioperative bleeding and blood utilization? Even STS recommendations are to stop 5 days preop. ASA is coded yes for a 5 day time frame and is not nearly as disruptive to periop coagulation. Should Aggrenox be coded as ASA? Combo drugs are not listed in that section.
At the time Plavix was added to the data set as a preoperative medication, the 24 hour window was applicable with the dosing and administration at that time. Because of the evolution in usage of Plavix, the 24 hour window does not make sense. Will change for the next spec upgrade.
1030 Meds-Glycoprotein IIbIIIa Inhibitor
Indicate whether the patient received Glycoprotein IIb/IIIa inhibitors within 24 hours preceding surgery.
1040 Meds-Glycoprotein IIbIIIa Inhibitor-Medication Name
Indicate the name of the Glycoprotein IIb/IIIa Inhibitor the patient received within 24 hours preceding surgery.
From version
2.41
5/03 Section “H” Hemodynamics and Cath
In the past, the STS has stated that using intra-op TEE results to code fields in Section “H”, Hemodynamics and Cath, was appropriate. After reviewing this statement the STS has decided that intra-op TEE results should not be used to code this section. Only procedure results obtained pre-op should be used to code this section. Please note that it is not necessary to go back and change data that has been affected by this definition clarification. However, moving forward please obtain data based on the clarification information given above.
1050 Num Dis Vessels Indicate the number of major native coronary vessel systems (LAD system, Circumflex system, and/or Right system) with >= 50% narrowing in any angiographic view. NOTE: Left main disease (>= 50%) is counted as TWO vessels (LAD and Circumflex). For example, left main and RCA would count as three total. Select from the following: None (no significant coronary obstructive disease) One
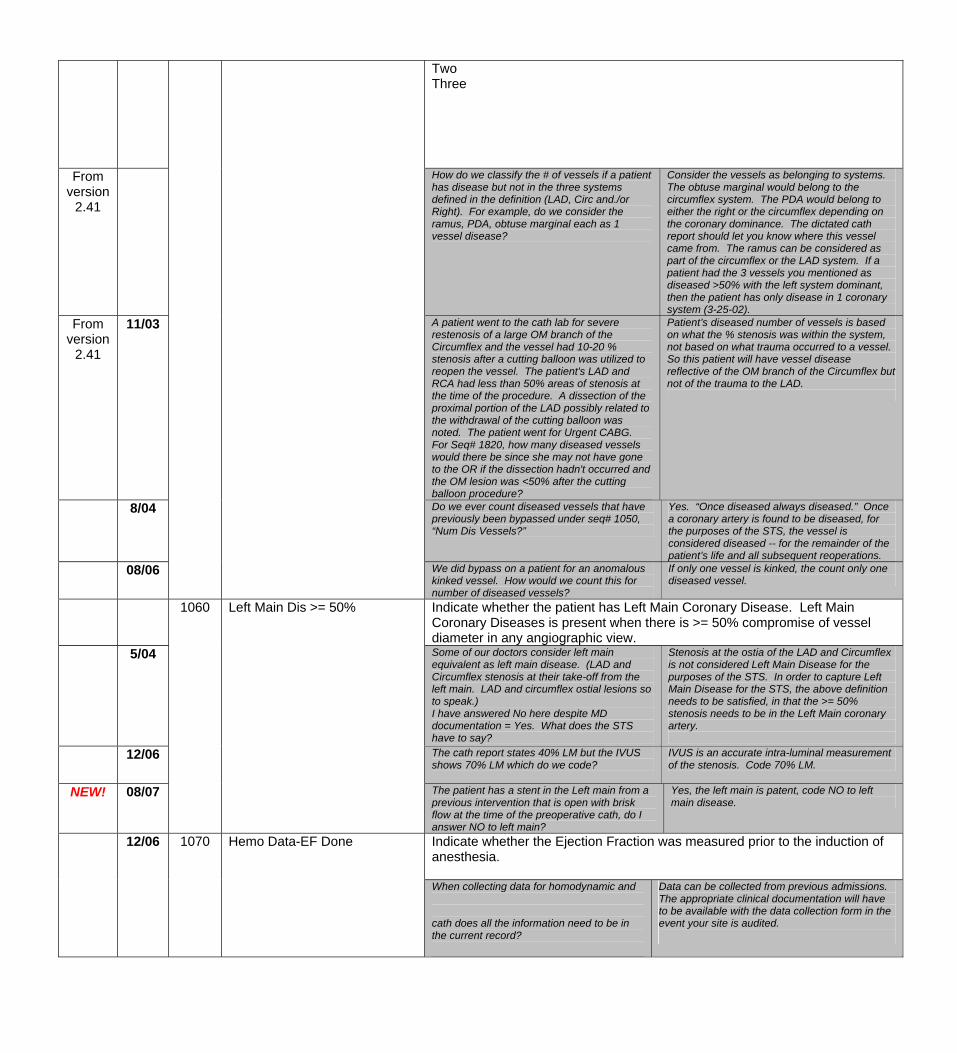
Two Three
From version
2.41
How do we classify the # of vessels if a patient has disease but not in the three systems defined in the definition (LAD, Circ and./or Right). For example, do we consider the ramus, PDA, obtuse marginal each as 1 vessel disease?
Consider the vessels as belonging to systems. The obtuse marginal would belong to the circumflex system. The PDA would belong to either the right or the circumflex depending on the coronary dominance. The dictated cath report should let you know where this vessel came from. The ramus can be considered as part of the circumflex or the LAD system. If a patient had the 3 vessels you mentioned as diseased >50% with the left system dominant, then the patient has only disease in 1 coronary system (3-25-02).
From version
2.41
11/03 A patient went to the cath lab for severe restenosis of a large OM branch of the Circumflex and the vessel had 10-20 % stenosis after a cutting balloon was utilized to reopen the vessel. The patient's LAD and RCA had less than 50% areas of stenosis at the time of the procedure. A dissection of the proximal portion of the LAD possibly related to the withdrawal of the cutting balloon was noted. The patient went for Urgent CABG. For Seq# 1820, how many diseased vessels would there be since she may not have gone to the OR if the dissection hadn't occurred and the OM lesion was <50% after the cutting balloon procedure?
Patient’s diseased number of vessels is based on what the % stenosis was within the system, not based on what trauma occurred to a vessel. So this patient will have vessel disease reflective of the OM branch of the Circumflex but not of the trauma to the LAD.
8/04 Do we ever count diseased vessels that have previously been bypassed under seq# 1050, “Num Dis Vessels?”
Yes. “Once diseased always diseased.” Once a coronary artery is found to be diseased, for the purposes of the STS, the vessel is considered diseased -- for the remainder of the patient’s life and all subsequent reoperations.
08/06 We did bypass on a patient for an anomalous kinked vessel. How would we count this for number of diseased vessels?
If only one vessel is kinked, the count only one diseased vessel.
Indicate whether the patient has Left Main Coronary Disease. Left Main Coronary Diseases is present when there is >= 50% compromise of vessel diameter in any angiographic view.
5/04
1060 Left Main Dis >= 50%
Some of our doctors consider left main equivalent as left main disease. (LAD and Circumflex stenosis at their take-off from the left main. LAD and circumflex ostial lesions so to speak.) I have answered No here despite MD documentation = Yes. What does the STS have to say?
Stenosis at the ostia of the LAD and Circumflex is not considered Left Main Disease for the purposes of the STS. In order to capture Left Main Disease for the STS, the above definition needs to be satisfied, in that the >= 50% stenosis needs to be in the Left Main coronary artery.
12/06 The cath report states 40% LM but the IVUS shows 70% LM which do we code?
IVUS is an accurate intra-luminal measurement of the stenosis. Code 70% LM.
NEW! 08/07 The patient has a stent in the Left main from a previous intervention that is open with brisk flow at the time of the preoperative cath, do I answer NO to left main?
Yes, the left main is patent, code NO to left main disease.
Indicate whether the Ejection Fraction was measured prior to the induction of anesthesia.
12/06 1070 Hemo Data-EF Done
When collecting data for homodynamic and cath does all the information need to be in the current record?
Data can be collected from previous admissions. The appropriate clinical documentation will have to be available with the data collection form in the event your site is audited.
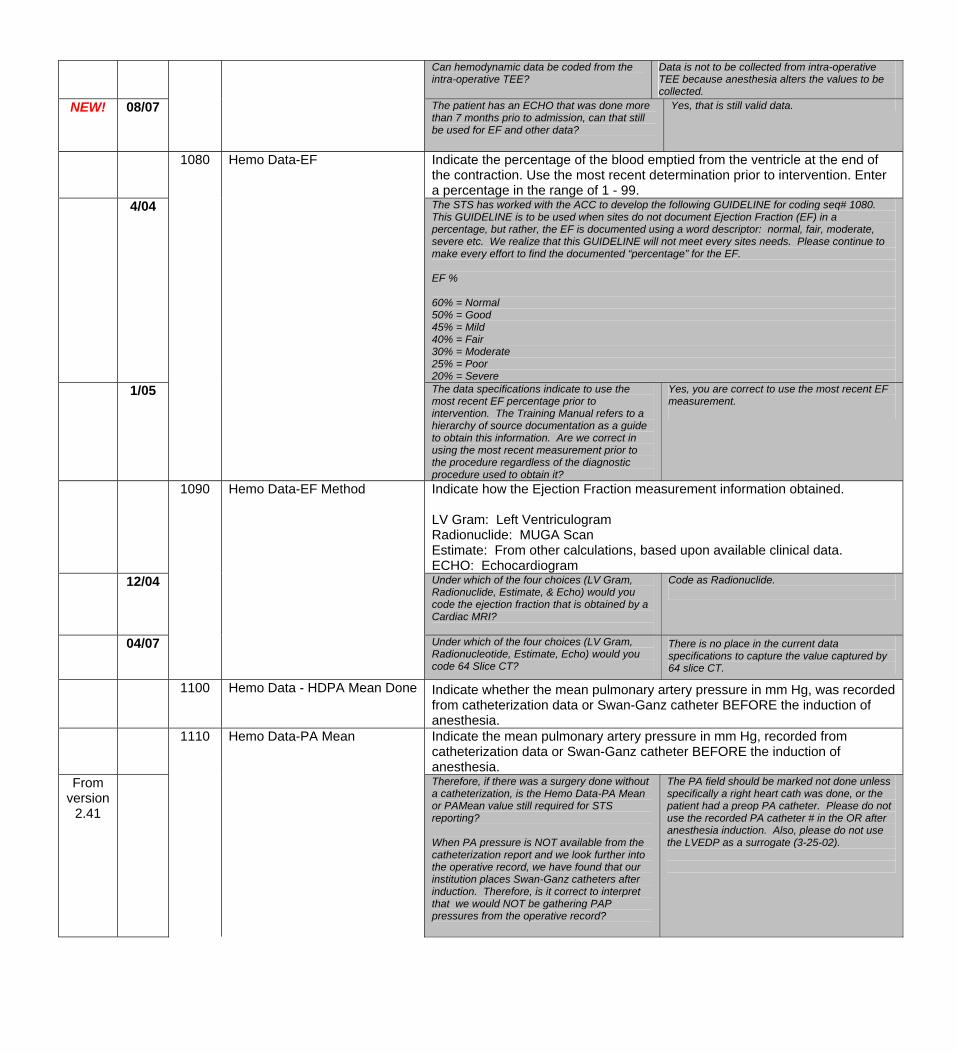
Can hemodynamic data be coded from the intra-operative TEE?
Data is not to be collected from intra-operative TEE because anesthesia alters the values to be collected.
NEW! 08/07 The patient has an ECHO that was done more than 7 months prio to admission, can that still be used for EF and other data?
Yes, that is still valid data.
Indicate the percentage of the blood emptied from the ventricle at the end of the contraction. Use the most recent determination prior to intervention. Enter a percentage in the range of 1 - 99.
4/04 The STS has worked with the ACC to develop the following GUIDELINE for coding seq# 1080. This GUIDELINE is to be used when sites do not document Ejection Fraction (EF) in a percentage, but rather, the EF is documented using a word descriptor: normal, fair, moderate, severe etc. We realize that this GUIDELINE will not meet every sites needs. Please continue to make every effort to find the documented “percentage” for the EF. EF % 60% = Normal 50% = Good 45% = Mild 40% = Fair 30% = Moderate 25% = Poor 20% = Severe
1/05
1080 Hemo Data-EF
The data specifications indicate to use the most recent EF percentage prior to intervention. The Training Manual refers to a hierarchy of source documentation as a guide to obtain this information. Are we correct in using the most recent measurement prior to the procedure regardless of the diagnostic procedure used to obtain it?
Yes, you are correct to use the most recent EF measurement.
Indicate how the Ejection Fraction measurement information obtained. LV Gram: Left Ventriculogram Radionuclide: MUGA Scan Estimate: From other calculations, based upon available clinical data. ECHO: Echocardiogram
12/04
1090 Hemo Data-EF Method
Under which of the four choices (LV Gram, Radionuclide, Estimate, & Echo) would you code the ejection fraction that is obtained by a Cardiac MRI?
Code as Radionuclide.
04/07 Under which of the four choices (LV Gram, Radionucleotide, Estimate, Echo) would you code 64 Slice CT?
There is no place in the current data specifications to capture the value captured by 64 slice CT.
1100 Hemo Data - HDPA Mean Done Indicate whether the mean pulmonary artery pressure in mm Hg, was recorded from catheterization data or Swan-Ganz catheter BEFORE the induction of anesthesia.
Indicate the mean pulmonary artery pressure in mm Hg, recorded from catheterization data or Swan-Ganz catheter BEFORE the induction of anesthesia.
From version
2.41
1110 Hemo Data-PA Mean
Therefore, if there was a surgery done without a catheterization, is the Hemo Data-PA Mean or PAMean value still required for STS reporting? When PA pressure is NOT available from the catheterization report and we look further into the operative record, we have found that our institution places Swan-Ganz catheters after induction. Therefore, is it correct to interpret that we would NOT be gathering PAP pressures from the operative record?
The PA field should be marked not done unless specifically a right heart cath was done, or the patient had a preop PA catheter. Please do not use the recorded PA catheter # in the OR after anesthesia induction. Also, please do not use the LVEDP as a surrogate (3-25-02).
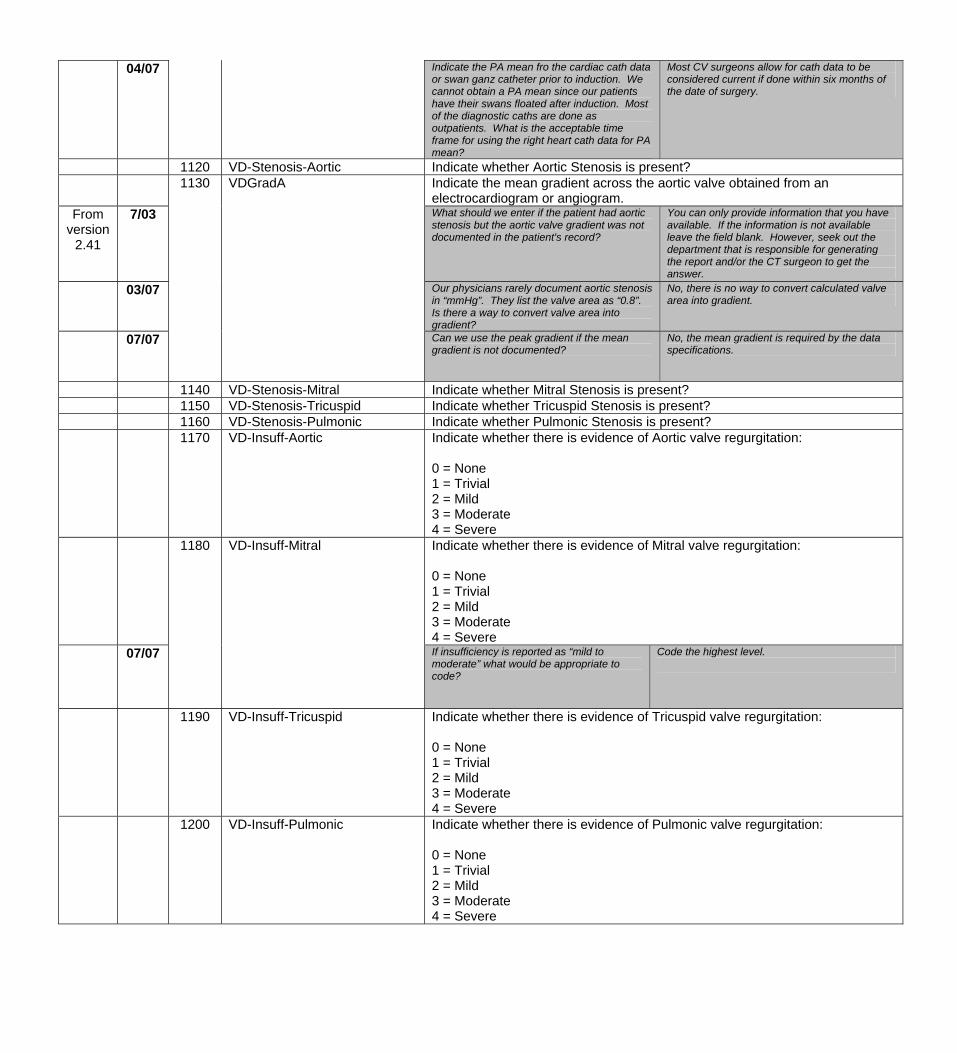
04/07 Indicate the PA mean fro the cardiac cath data or swan ganz catheter prior to induction. We cannot obtain a PA mean since our patients have their swans floated after induction. Most of the diagnostic caths are done as outpatients. What is the acceptable time frame for using the right heart cath data for PA mean?
Most CV surgeons allow for cath data to be considered current if done within six months of the date of surgery.
1120 VD-Stenosis-Aortic Indicate whether Aortic Stenosis is present? Indicate the mean gradient across the aortic valve obtained from an
electrocardiogram or angiogram. From
version 2.41
7/03
1130 VDGradA
What should we enter if the patient had aortic stenosis but the aortic valve gradient was not documented in the patient's record?
You can only provide information that you have available. If the information is not available leave the field blank. However, seek out the department that is responsible for generating the report and/or the CT surgeon to get the answer.
03/07
Our physicians rarely document aortic stenosis in “mmHg”. They list the valve area as “0.8”. Is there a way to convert valve area into gradient?
No, there is no way to convert calculated valve area into gradient.
07/07 Can we use the peak gradient if the mean gradient is not documented?
No, the mean gradient is required by the data specifications.
1140 VD-Stenosis-Mitral Indicate whether Mitral Stenosis is present? 1150 VD-Stenosis-Tricuspid Indicate whether Tricuspid Stenosis is present? 1160 VD-Stenosis-Pulmonic Indicate whether Pulmonic Stenosis is present? 1170 VD-Insuff-Aortic Indicate whether there is evidence of Aortic valve regurgitation:
0 = None 1 = Trivial 2 = Mild 3 = Moderate 4 = Severe
1180 VD-Insuff-Mitral Indicate whether there is evidence of Mitral valve regurgitation: 0 = None 1 = Trivial 2 = Mild 3 = Moderate 4 = Severe
07/07 If insufficiency is reported as “mild to moderate” what would be appropriate to code?
Code the highest level.
1190 VD-Insuff-Tricuspid Indicate whether there is evidence of Tricuspid valve regurgitation: 0 = None 1 = Trivial 2 = Mild 3 = Moderate 4 = Severe
1200 VD-Insuff-Pulmonic Indicate whether there is evidence of Pulmonic valve regurgitation: 0 = None 1 = Trivial 2 = Mild 3 = Moderate 4 = Severe
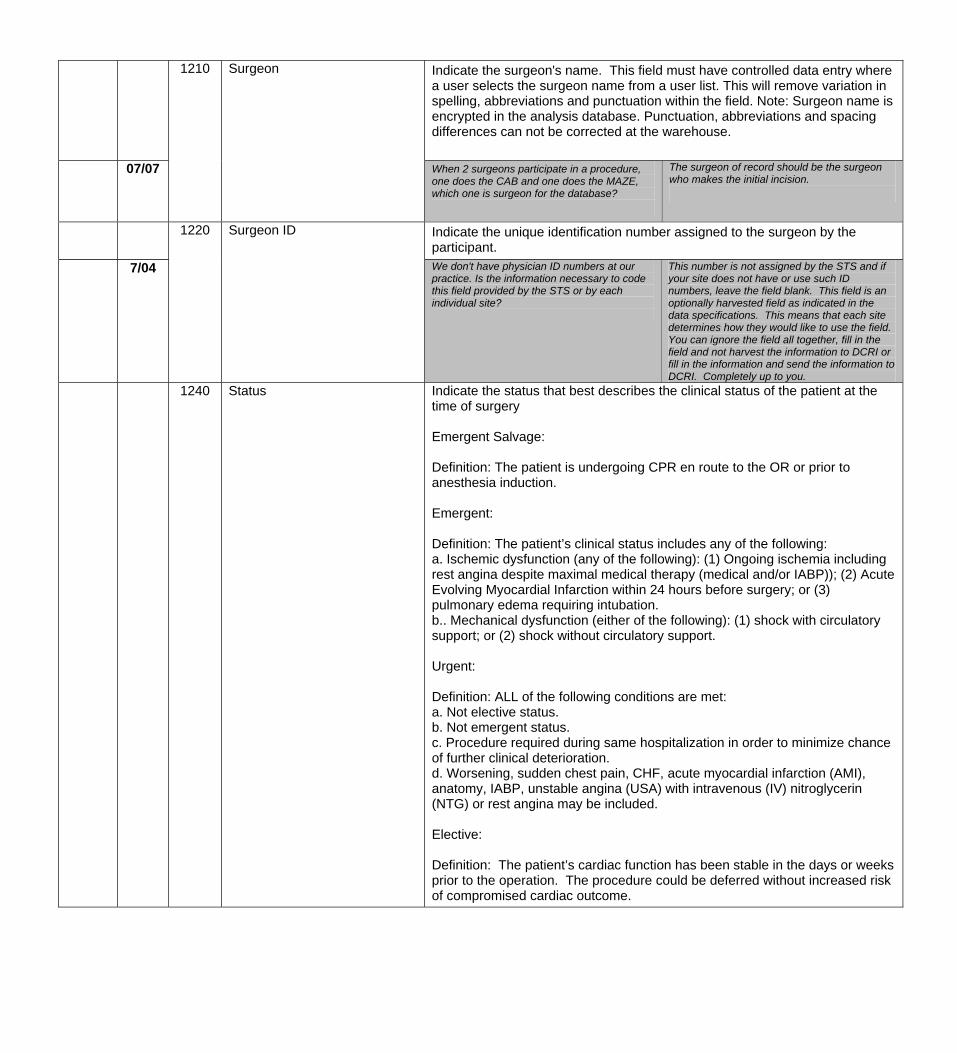
1210 Surgeon Indicate the surgeon's name. This field must have controlled data entry where a user selects the surgeon name from a user list. This will remove variation in spelling, abbreviations and punctuation within the field. Note: Surgeon name is encrypted in the analysis database. Punctuation, abbreviations and spacing differences can not be corrected at the warehouse.
07/07 When 2 surgeons participate in a procedure, one does the CAB and one does the MAZE, which one is surgeon for the database?
The surgeon of record should be the surgeon who makes the initial incision.
Indicate the unique identification number assigned to the surgeon by the participant.
7/04
1220 Surgeon ID
We don't have physician ID numbers at our practice. Is the information necessary to code this field provided by the STS or by each individual site?
This number is not assigned by the STS and if your site does not have or use such ID numbers, leave the field blank. This field is an optionally harvested field as indicated in the data specifications. This means that each site determines how they would like to use the field. You can ignore the field all together, fill in the field and not harvest the information to DCRI or fill in the information and send the information to DCRI. Completely up to you.
1240 Status Indicate the status that best describes the clinical status of the patient at the time of surgery Emergent Salvage: Definition: The patient is undergoing CPR en route to the OR or prior to anesthesia induction. Emergent: Definition: The patient’s clinical status includes any of the following: a. Ischemic dysfunction (any of the following): (1) Ongoing ischemia including rest angina despite maximal medical therapy (medical and/or IABP)); (2) Acute Evolving Myocardial Infarction within 24 hours before surgery; or (3) pulmonary edema requiring intubation. b.. Mechanical dysfunction (either of the following): (1) shock with circulatory support; or (2) shock without circulatory support. Urgent: Definition: ALL of the following conditions are met: a. Not elective status. b. Not emergent status. c. Procedure required during same hospitalization in order to minimize chance of further clinical deterioration. d. Worsening, sudden chest pain, CHF, acute myocardial infarction (AMI), anatomy, IABP, unstable angina (USA) with intravenous (IV) nitroglycerin (NTG) or rest angina may be included. Elective: Definition: The patient’s cardiac function has been stable in the days or weeks prior to the operation. The procedure could be deferred without increased risk of compromised cardiac outcome.
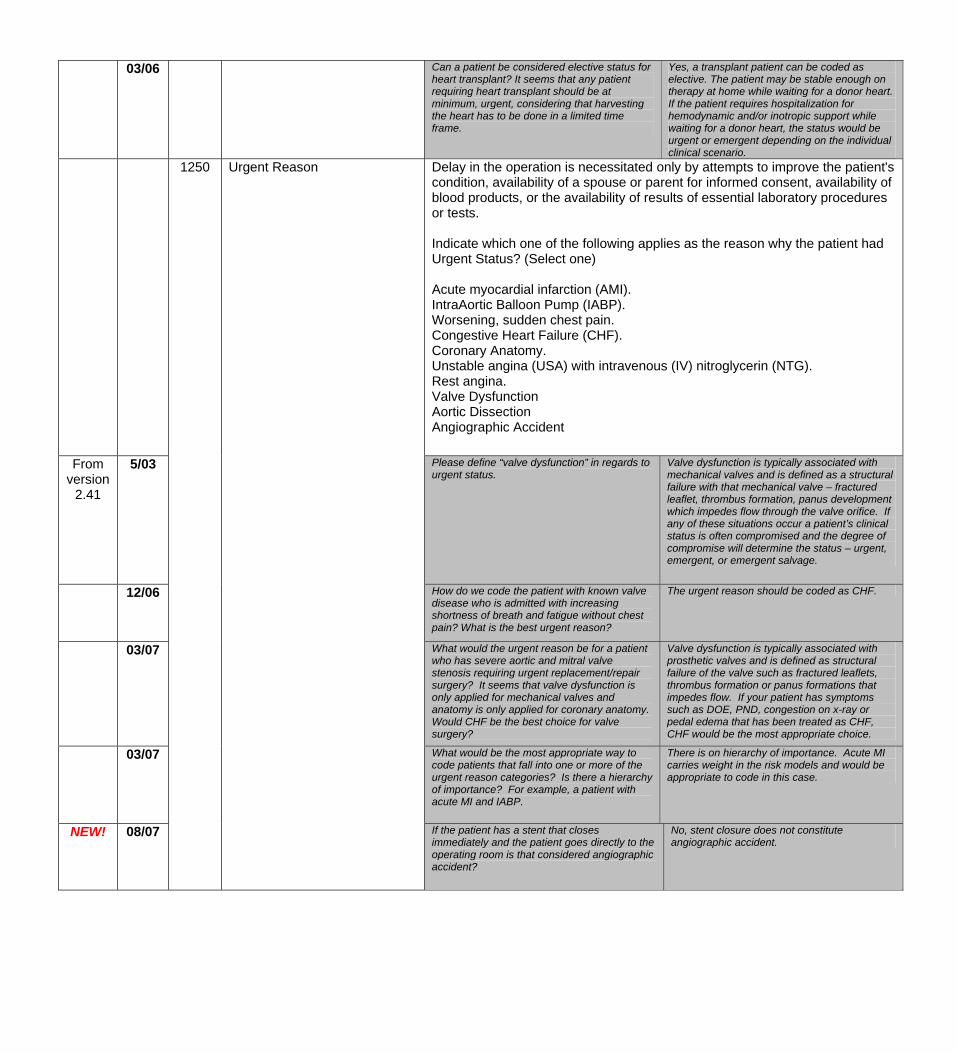
03/06 Can a patient be considered elective status for heart transplant? It seems that any patient requiring heart transplant should be at minimum, urgent, considering that harvesting the heart has to be done in a limited time frame.
Yes, a transplant patient can be coded as elective. The patient may be stable enough on therapy at home while waiting for a donor heart. If the patient requires hospitalization for hemodynamic and/or inotropic support while waiting for a donor heart, the status would be urgent or emergent depending on the individual clinical scenario.
Delay in the operation is necessitated only by attempts to improve the patient's condition, availability of a spouse or parent for informed consent, availability of blood products, or the availability of results of essential laboratory procedures or tests. Indicate which one of the following applies as the reason why the patient had Urgent Status? (Select one) Acute myocardial infarction (AMI). IntraAortic Balloon Pump (IABP). Worsening, sudden chest pain. Congestive Heart Failure (CHF). Coronary Anatomy. Unstable angina (USA) with intravenous (IV) nitroglycerin (NTG). Rest angina. Valve Dysfunction Aortic Dissection Angiographic Accident
From version
2.41
5/03
1250 Urgent Reason
Please define “valve dysfunction” in regards to urgent status.
Valve dysfunction is typically associated with mechanical valves and is defined as a structural failure with that mechanical valve – fractured leaflet, thrombus formation, panus development which impedes flow through the valve orifice. If any of these situations occur a patient’s clinical status is often compromised and the degree of compromise will determine the status – urgent, emergent, or emergent salvage.
12/06
How do we code the patient with known valve disease who is admitted with increasing shortness of breath and fatigue without chest pain? What is the best urgent reason?
The urgent reason should be coded as CHF.
03/07
What would the urgent reason be for a patient who has severe aortic and mitral valve stenosis requiring urgent replacement/repair surgery? It seems that valve dysfunction is only applied for mechanical valves and anatomy is only applied for coronary anatomy. Would CHF be the best choice for valve surgery?
Valve dysfunction is typically associated with prosthetic valves and is defined as structural failure of the valve such as fractured leaflets, thrombus formation or panus formations that impedes flow. If your patient has symptoms such as DOE, PND, congestion on x-ray or pedal edema that has been treated as CHF, CHF would be the most appropriate choice.
03/07
What would be the most appropriate way to code patients that fall into one or more of the urgent reason categories? Is there a hierarchy of importance? For example, a patient with acute MI and IABP.
There is on hierarchy of importance. Acute MI carries weight in the risk models and would be appropriate to code in this case.
NEW! 08/07 If the patient has a stent that closes immediately and the patient goes directly to the operating room is that considered angiographic accident?
No, stent closure does not constitute angiographic accident.
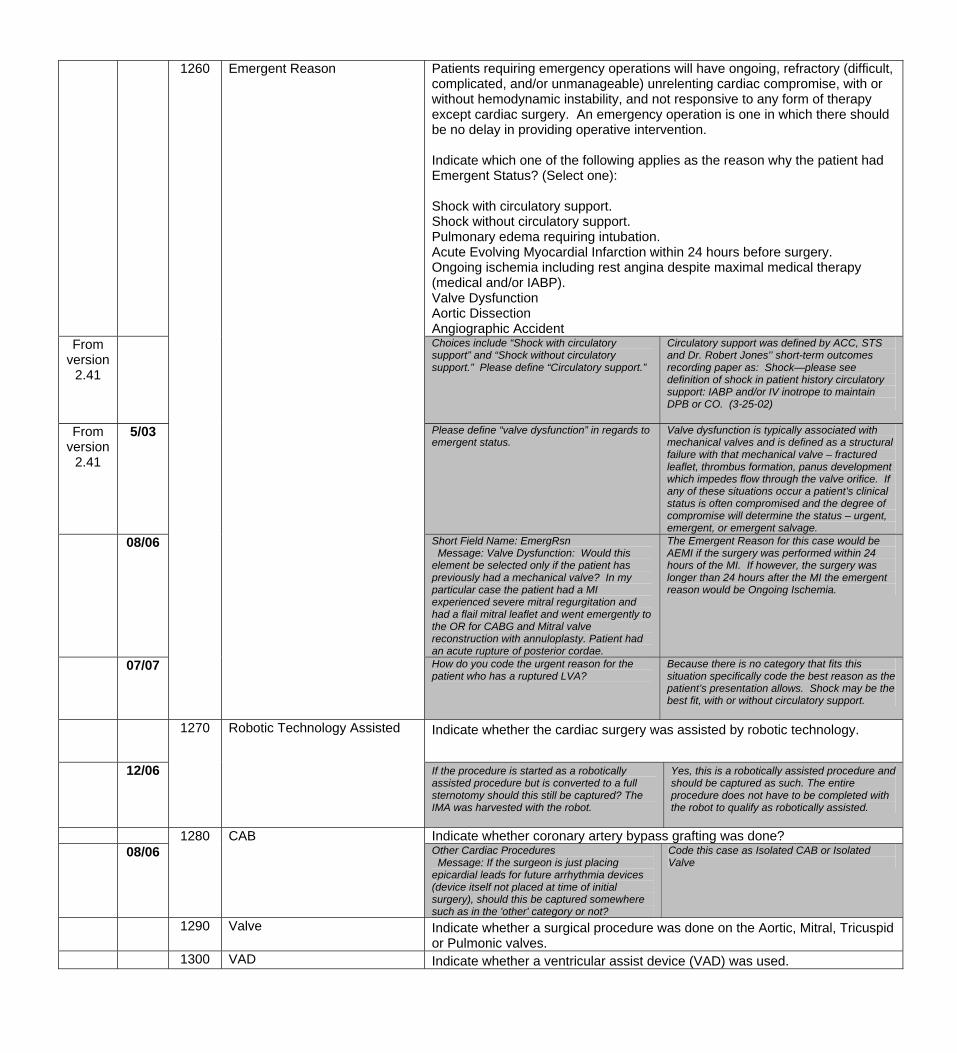
Patients requiring emergency operations will have ongoing, refractory (difficult, complicated, and/or unmanageable) unrelenting cardiac compromise, with or without hemodynamic instability, and not responsive to any form of therapy except cardiac surgery. An emergency operation is one in which there should be no delay in providing operative intervention. Indicate which one of the following applies as the reason why the patient had Emergent Status? (Select one): Shock with circulatory support. Shock without circulatory support. Pulmonary edema requiring intubation. Acute Evolving Myocardial Infarction within 24 hours before surgery. Ongoing ischemia including rest angina despite maximal medical therapy (medical and/or IABP). Valve Dysfunction Aortic Dissection Angiographic Accident
From version
2.41
Choices include “Shock with circulatory support” and “Shock without circulatory support.” Please define “Circulatory support.”
Circulatory support was defined by ACC, STS and Dr. Robert Jones'’ short-term outcomes recording paper as: Shock—please see definition of shock in patient history circulatory support: IABP and/or IV inotrope to maintain DPB or CO. (3-25-02)
From version
2.41
5/03 Please define “valve dysfunction” in regards to emergent status.
Valve dysfunction is typically associated with mechanical valves and is defined as a structural failure with that mechanical valve – fractured leaflet, thrombus formation, panus development which impedes flow through the valve orifice. If any of these situations occur a patient’s clinical status is often compromised and the degree of compromise will determine the status – urgent, emergent, or emergent salvage.
08/06
1260 Emergent Reason
Short Field Name: EmergRsn Message: Valve Dysfunction: Would this element be selected only if the patient has previously had a mechanical valve? In my particular case the patient had a MI experienced severe mitral regurgitation and had a flail mitral leaflet and went emergently to the OR for CABG and Mitral valve reconstruction with annuloplasty. Patient had an acute rupture of posterior cordae.
The Emergent Reason for this case would be AEMI if the surgery was performed within 24 hours of the MI. If however, the surgery was longer than 24 hours after the MI the emergent reason would be Ongoing Ischemia.
07/07 How do you code the urgent reason for the patient who has a ruptured LVA?
Because there is no category that fits this situation specifically code the best reason as the patient’s presentation allows. Shock may be the best fit, with or without circulatory support.
1270 Robotic Technology Assisted Indicate whether the cardiac surgery was assisted by robotic technology.
12/06 If the procedure is started as a robotically assisted procedure but is converted to a full sternotomy should this still be captured? The IMA was harvested with the robot.
Yes, this is a robotically assisted procedure and should be captured as such. The entire procedure does not have to be completed with the robot to qualify as robotically assisted.
Indicate whether coronary artery bypass grafting was done? 08/06
1280 CAB Other Cardiac Procedures Message: If the surgeon is just placing epicardial leads for future arrhythmia devices (device itself not placed at time of initial surgery), should this be captured somewhere such as in the 'other' category or not?
Code this case as Isolated CAB or Isolated Valve
1290 Valve Indicate whether a surgical procedure was done on the Aortic, Mitral, Tricuspid or Pulmonic valves.
1300 VAD Indicate whether a ventricular assist device (VAD) was used.
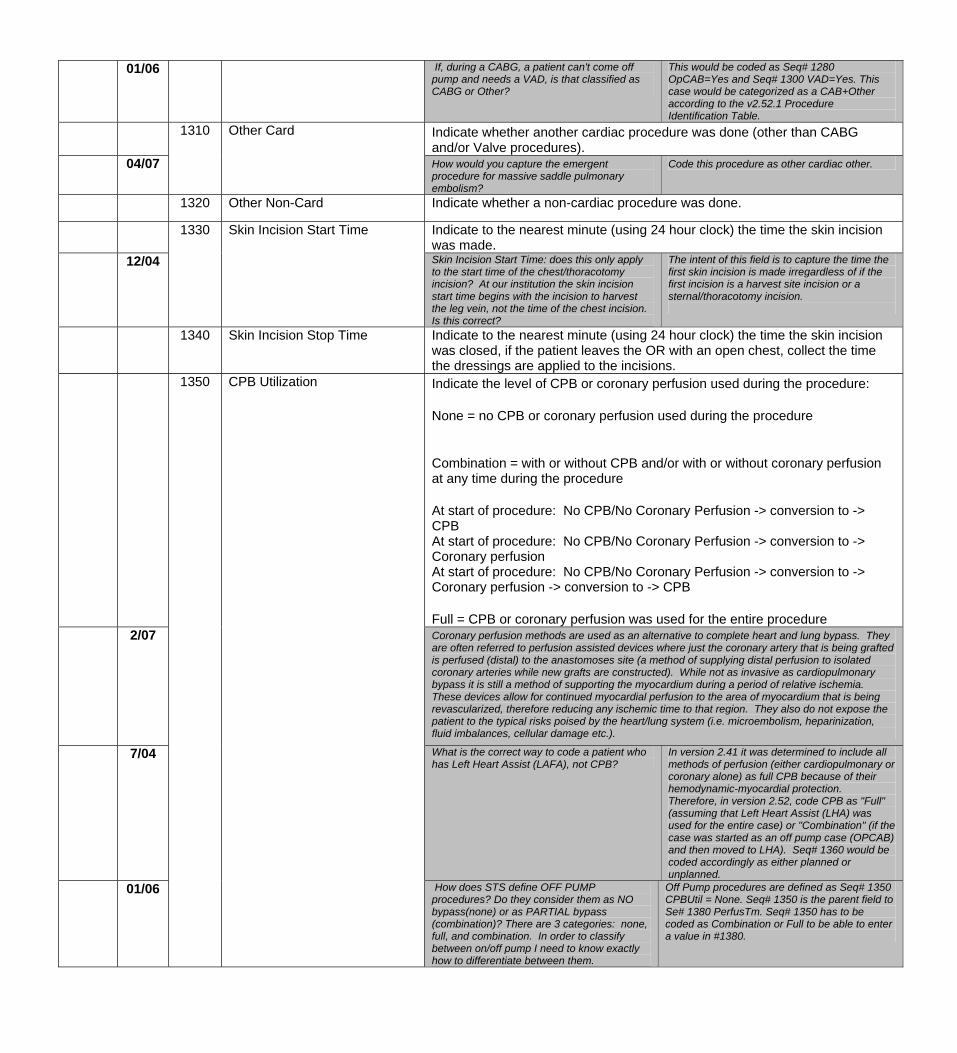
01/06 If, during a CABG, a patient can't come off pump and needs a VAD, is that classified as CABG or Other?
This would be coded as Seq# 1280 OpCAB=Yes and Seq# 1300 VAD=Yes. This case would be categorized as a CAB+Other according to the v2.52.1 Procedure Identification Table.
Indicate whether another cardiac procedure was done (other than CABG and/or Valve procedures).
04/07
1310 Other Card
How would you capture the emergent procedure for massive saddle pulmonary embolism?
Code this procedure as other cardiac other.
1320 Other Non-Card Indicate whether a non-cardiac procedure was done.
1330
Skin Incision Start Time Indicate to the nearest minute (using 24 hour clock) the time the skin incision was made.
12/04 Skin Incision Start Time: does this only apply to the start time of the chest/thoracotomy incision? At our institution the skin incision start time begins with the incision to harvest the leg vein, not the time of the chest incision. Is this correct?
The intent of this field is to capture the time the first skin incision is made irregardless of if the first incision is a harvest site incision or a sternal/thoracotomy incision.
1340
Skin Incision Stop Time
Indicate to the nearest minute (using 24 hour clock) the time the skin incision was closed, if the patient leaves the OR with an open chest, collect the time the dressings are applied to the incisions.
1350 CPB Utilization Indicate the level of CPB or coronary perfusion used during the procedure: None = no CPB or coronary perfusion used during the procedure Combination = with or without CPB and/or with or without coronary perfusion at any time during the procedure At start of procedure: No CPB/No Coronary Perfusion -> conversion to -> CPB At start of procedure: No CPB/No Coronary Perfusion -> conversion to -> Coronary perfusion At start of procedure: No CPB/No Coronary Perfusion -> conversion to -> Coronary perfusion -> conversion to -> CPB Full = CPB or coronary perfusion was used for the entire procedure
2/07 Coronary perfusion methods are used as an alternative to complete heart and lung bypass. They are often referred to perfusion assisted devices where just the coronary artery that is being grafted is perfused (distal) to the anastomoses site (a method of supplying distal perfusion to isolated coronary arteries while new grafts are constructed). While not as invasive as cardiopulmonary bypass it is still a method of supporting the myocardium during a period of relative ischemia. These devices allow for continued myocardial perfusion to the area of myocardium that is being revascularized, therefore reducing any ischemic time to that region. They also do not expose the patient to the typical risks poised by the heart/lung system (i.e. microembolism, heparinization, fluid imbalances, cellular damage etc.).
7/04 What is the correct way to code a patient who has Left Heart Assist (LAFA), not CPB?
In version 2.41 it was determined to include all methods of perfusion (either cardiopulmonary or coronary alone) as full CPB because of their hemodynamic-myocardial protection. Therefore, in version 2.52, code CPB as "Full" (assuming that Left Heart Assist (LHA) was used for the entire case) or "Combination" (if the case was started as an off pump case (OPCAB) and then moved to LHA). Seq# 1360 would be coded accordingly as either planned or unplanned.
01/06 How does STS define OFF PUMP procedures? Do they consider them as NO bypass(none) or as PARTIAL bypass (combination)? There are 3 categories: none, full, and combination. In order to classify between on/off pump I need to know exactly how to differentiate between them.
Off Pump procedures are defined as Seq# 1350 CPBUtil = None. Seq# 1350 is the parent field to Se# 1380 PerfusTm. Seq# 1350 has to be coded as Combination or Full to be able to enter a value in #1380.
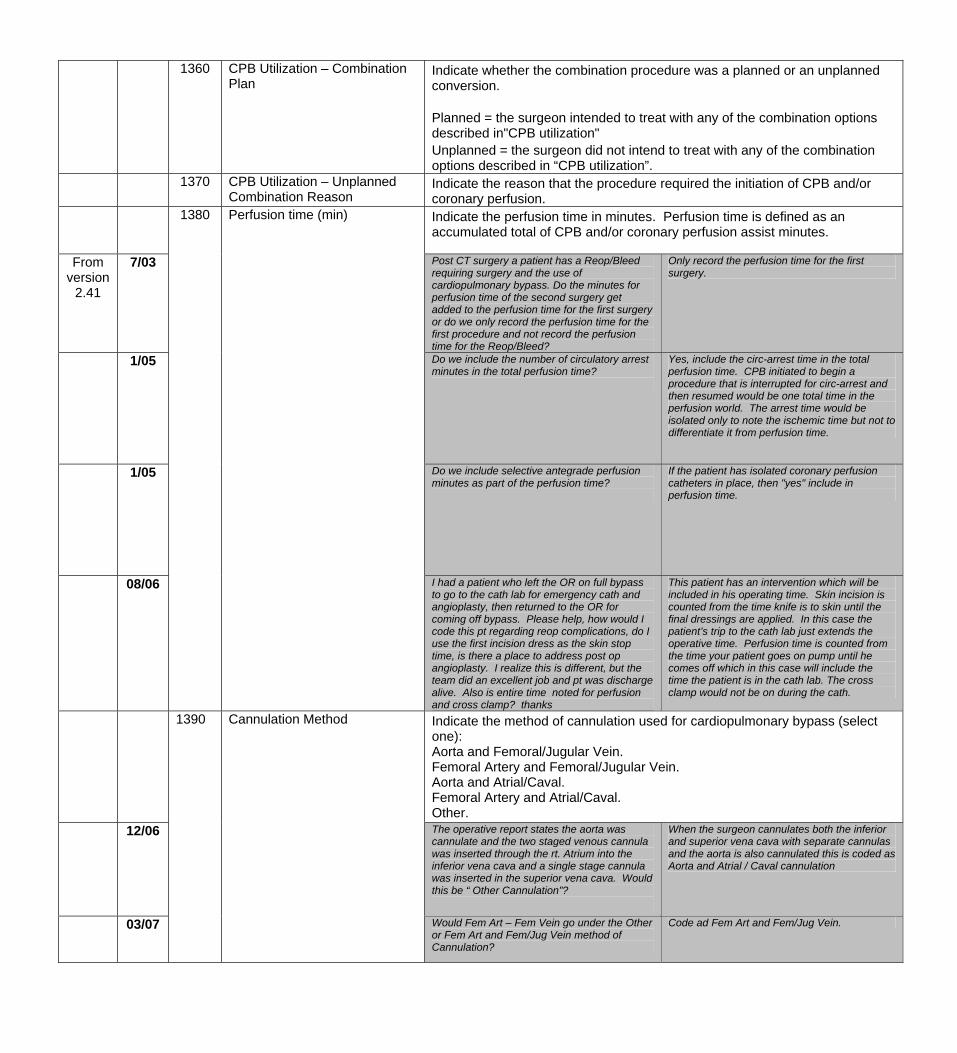
1360 CPB Utilization – Combination Plan
Indicate whether the combination procedure was a planned or an unplanned conversion. Planned = the surgeon intended to treat with any of the combination options described in"CPB utilization" Unplanned = the surgeon did not intend to treat with any of the combination options described in “CPB utilization”.
1370 CPB Utilization – Unplanned Combination Reason
Indicate the reason that the procedure required the initiation of CPB and/or coronary perfusion.
1380 Perfusion time (min) Indicate the perfusion time in minutes. Perfusion time is defined as an accumulated total of CPB and/or coronary perfusion assist minutes.
From version
2.41
7/03 Post CT surgery a patient has a Reop/Bleed requiring surgery and the use of cardiopulmonary bypass. Do the minutes for perfusion time of the second surgery get added to the perfusion time for the first surgery or do we only record the perfusion time for the first procedure and not record the perfusion time for the Reop/Bleed?
Only record the perfusion time for the first surgery.
1/05 Do we include the number of circulatory arrest minutes in the total perfusion time?
Yes, include the circ-arrest time in the total perfusion time. CPB initiated to begin a procedure that is interrupted for circ-arrest and then resumed would be one total time in the perfusion world. The arrest time would be isolated only to note the ischemic time but not to differentiate it from perfusion time.
1/05 Do we include selective antegrade perfusion minutes as part of the perfusion time?
If the patient has isolated coronary perfusion catheters in place, then "yes" include in perfusion time.
08/06
I had a patient who left the OR on full bypass to go to the cath lab for emergency cath and angioplasty, then returned to the OR for coming off bypass. Please help, how would I code this pt regarding reop complications, do I use the first incision dress as the skin stop time, is there a place to address post op angioplasty. I realize this is different, but the team did an excellent job and pt was discharge alive. Also is entire time noted for perfusion and cross clamp? thanks
This patient has an intervention which will be included in his operating time. Skin incision is counted from the time knife is to skin until the final dressings are applied. In this case the patient’s trip to the cath lab just extends the operative time. Perfusion time is counted from the time your patient goes on pump until he comes off which in this case will include the time the patient is in the cath lab. The cross clamp would not be on during the cath.
1390 Cannulation Method Indicate the method of cannulation used for cardiopulmonary bypass (select one): Aorta and Femoral/Jugular Vein. Femoral Artery and Femoral/Jugular Vein. Aorta and Atrial/Caval. Femoral Artery and Atrial/Caval. Other.
12/06
The operative report states the aorta was cannulate and the two staged venous cannula was inserted through the rt. Atrium into the inferior vena cava and a single stage cannula was inserted in the superior vena cava. Would this be “ Other Cannulation”?
When the surgeon cannulates both the inferior and superior vena cava with separate cannulas and the aorta is also cannulated this is coded as Aorta and Atrial / Caval cannulation
03/07
Would Fem Art – Fem Vein go under the Other or Fem Art and Fem/Jug Vein method of Cannulation?
Code ad Fem Art and Fem/Jug Vein.
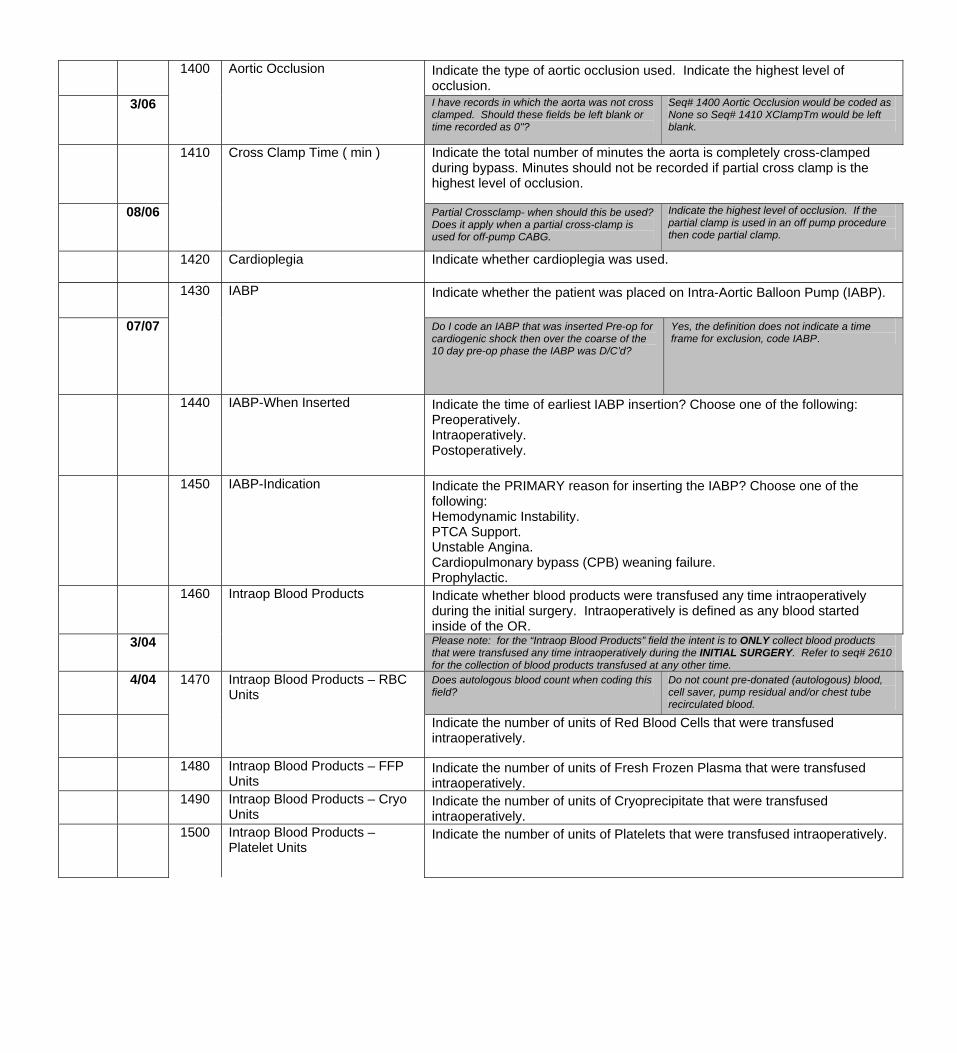
1400
Aortic Occlusion Indicate the type of aortic occlusion used. Indicate the highest level of occlusion.
3/06
I have records in which the aorta was not cross clamped. Should these fields be left blank or time recorded as 0"?
Seq# 1400 Aortic Occlusion would be coded as None so Seq# 1410 XClampTm would be left blank.
Indicate the total number of minutes the aorta is completely cross-clamped during bypass. Minutes should not be recorded if partial cross clamp is the highest level of occlusion.
08/06
1410 Cross Clamp Time ( min )
Partial Crossclamp- when should this be used? Does it apply when a partial cross-clamp is used for off-pump CABG.
Indicate the highest level of occlusion. If the partial clamp is used in an off pump procedure then code partial clamp.
1420 Cardioplegia Indicate whether cardioplegia was used.
1430 IABP Indicate whether the patient was placed on Intra-Aortic Balloon Pump (IABP).
07/07 Do I code an IABP that was inserted Pre-op for cardiogenic shock then over the coarse of the 10 day pre-op phase the IABP was D/C’d?
Yes, the definition does not indicate a time frame for exclusion, code IABP.
1440
IABP-When Inserted
Indicate the time of earliest IABP insertion? Choose one of the following: Preoperatively. Intraoperatively. Postoperatively.
1450 IABP-Indication Indicate the PRIMARY reason for inserting the IABP? Choose one of the following: Hemodynamic Instability. PTCA Support. Unstable Angina. Cardiopulmonary bypass (CPB) weaning failure. Prophylactic.
Indicate whether blood products were transfused any time intraoperatively during the initial surgery. Intraoperatively is defined as any blood started inside of the OR.
3/04
1460 Intraop Blood Products
Please note: for the “Intraop Blood Products” field the intent is to ONLY collect blood products that were transfused any time intraoperatively during the INITIAL SURGERY. Refer to seq# 2610 for the collection of blood products transfused at any other time.
4/04 Does autologous blood count when coding this field?
Do not count pre-donated (autologous) blood, cell saver, pump residual and/or chest tube recirculated blood.
1470 Intraop Blood Products – RBC Units
Indicate the number of units of Red Blood Cells that were transfused intraoperatively.
1480 Intraop Blood Products – FFP Units
Indicate the number of units of Fresh Frozen Plasma that were transfused intraoperatively.
1490 Intraop Blood Products – Cryo Units
Indicate the number of units of Cryoprecipitate that were transfused intraoperatively.
1500
Intraop Blood Products – Platelet Units
Indicate the number of units of Platelets that were transfused intraoperatively.
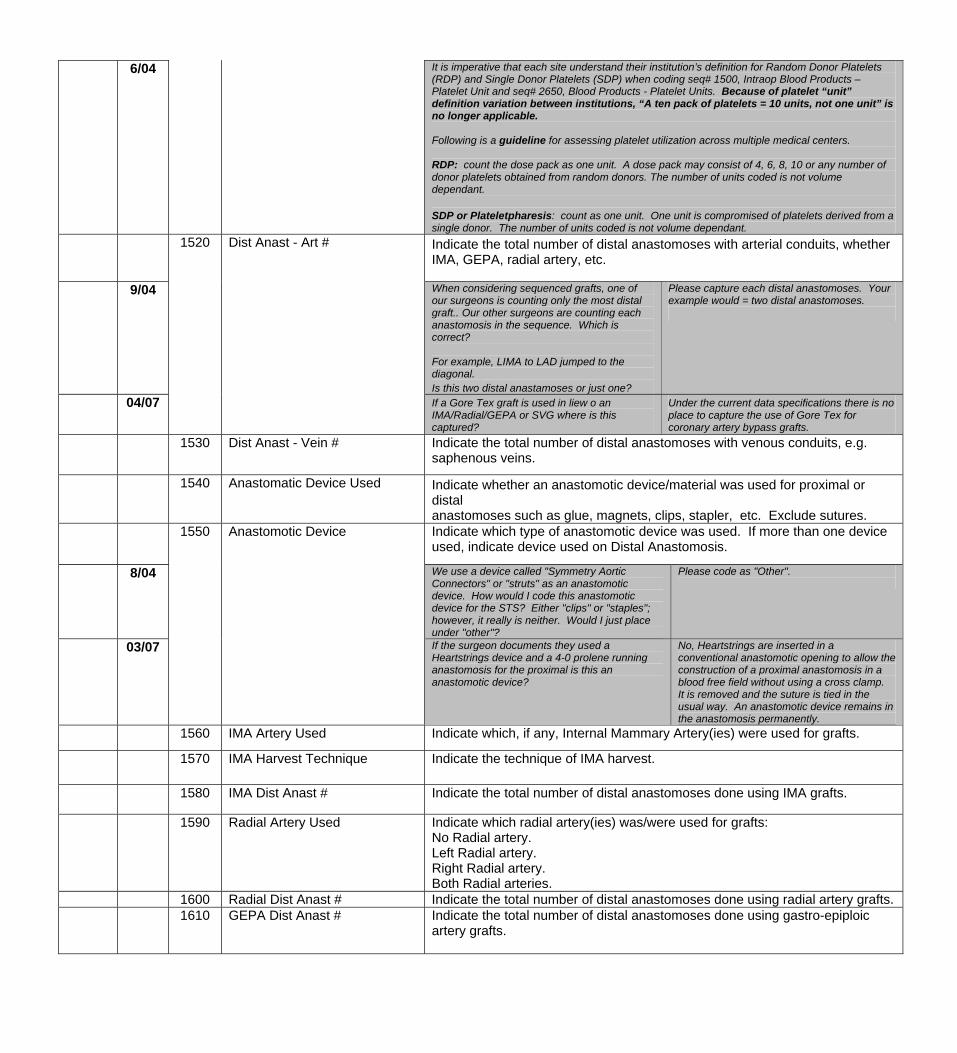
6/04 It is imperative that each site understand their institution’s definition for Random Donor Platelets (RDP) and Single Donor Platelets (SDP) when coding seq# 1500, Intraop Blood Products – Platelet Unit and seq# 2650, Blood Products - Platelet Units. Because of platelet “unit” definition variation between institutions, “A ten pack of platelets = 10 units, not one unit” is no longer applicable. Following is a guideline for assessing platelet utilization across multiple medical centers. RDP: count the dose pack as one unit. A dose pack may consist of 4, 6, 8, 10 or any number of donor platelets obtained from random donors. The number of units coded is not volume dependant. SDP or Plateletpharesis: count as one unit. One unit is compromised of platelets derived from a single donor. The number of units coded is not volume dependant.
Indicate the total number of distal anastomoses with arterial conduits, whether IMA, GEPA, radial artery, etc.
9/04 When considering sequenced grafts, one of our surgeons is counting only the most distal graft.. Our other surgeons are counting each anastomosis in the sequence. Which is correct? For example, LIMA to LAD jumped to the diagonal. Is this two distal anastamoses or just one?
Please capture each distal anastomoses. Your example would = two distal anastomoses.
04/07
1520
Dist Anast - Art #
If a Gore Tex graft is used in liew o an IMA/Radial/GEPA or SVG where is this captured?
Under the current data specifications there is no place to capture the use of Gore Tex for coronary artery bypass grafts.
1530 Dist Anast - Vein # Indicate the total number of distal anastomoses with venous conduits, e.g. saphenous veins.
1540
Anastomatic Device Used
Indicate whether an anastomotic device/material was used for proximal or distal anastomoses such as glue, magnets, clips, stapler, etc. Exclude sutures.
1550 Anastomotic Device Indicate which type of anastomotic device was used. If more than one device used, indicate device used on Distal Anastomosis.
8/04 We use a device called "Symmetry Aortic Connectors" or "struts" as an anastomotic device. How would I code this anastomotic device for the STS? Either "clips" or "staples"; however, it really is neither. Would I just place under "other"?
Please code as "Other".
03/07
If the surgeon documents they used a Heartstrings device and a 4-0 prolene running anastomosis for the proximal is this an anastomotic device?
No, Heartstrings are inserted in a conventional anastomotic opening to allow the construction of a proximal anastomosis in a blood free field without using a cross clamp. It is removed and the suture is tied in the usual way. An anastomotic device remains in the anastomosis permanently.
1560 IMA Artery Used Indicate which, if any, Internal Mammary Artery(ies) were used for grafts.
1570 IMA Harvest Technique Indicate the technique of IMA harvest.
1580 IMA Dist Anast # Indicate the total number of distal anastomoses done using IMA grafts.
1590
Radial Artery Used
Indicate which radial artery(ies) was/were used for grafts: No Radial artery. Left Radial artery. Right Radial artery. Both Radial arteries.
1600 Radial Dist Anast # Indicate the total number of distal anastomoses done using radial artery grafts. 1610
GEPA Dist Anast #
Indicate the total number of distal anastomoses done using gastro-epiploic artery grafts.
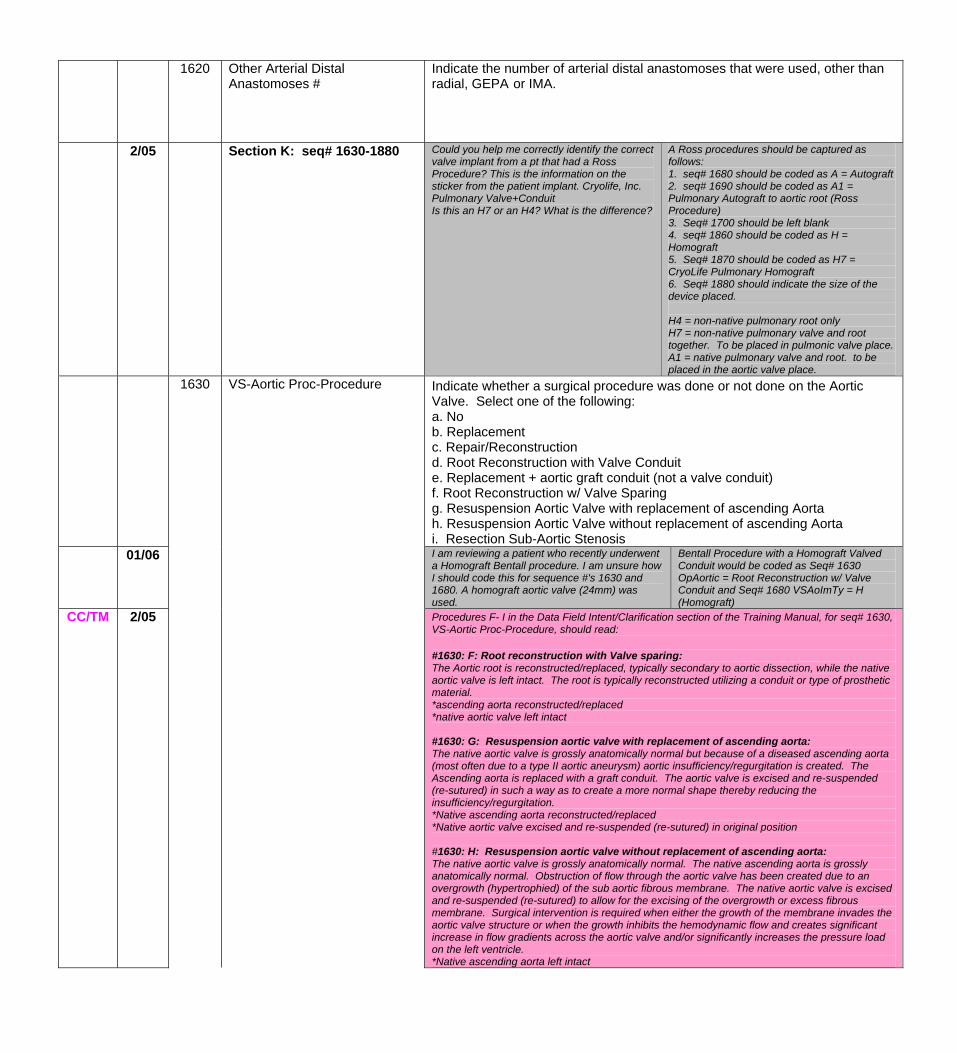
1620 Other Arterial Distal Anastomoses #
Indicate the number of arterial distal anastomoses that were used, other than radial, GEPA or IMA.
2/05 Section K: seq# 1630-1880 Could you help me correctly identify the correct valve implant from a pt that had a Ross Procedure? This is the information on the sticker from the patient implant. Cryolife, Inc. Pulmonary Valve+Conduit Is this an H7 or an H4? What is the difference?
A Ross procedures should be captured as follows: 1. seq# 1680 should be coded as A = Autograft 2. seq# 1690 should be coded as A1 = Pulmonary Autograft to aortic root (Ross Procedure) 3. Seq# 1700 should be left blank 4. seq# 1860 should be coded as H = Homograft 5. Seq# 1870 should be coded as H7 = CryoLife Pulmonary Homograft 6. Seq# 1880 should indicate the size of the device placed. H4 = non-native pulmonary root only H7 = non-native pulmonary valve and root together. To be placed in pulmonic valve place. A1 = native pulmonary valve and root. to be placed in the aortic valve place.
1630 VS-Aortic Proc-Procedure Indicate whether a surgical procedure was done or not done on the Aortic Valve. Select one of the following: a. No b. Replacement c. Repair/Reconstruction d. Root Reconstruction with Valve Conduit e. Replacement + aortic graft conduit (not a valve conduit) f. Root Reconstruction w/ Valve Sparing g. Resuspension Aortic Valve with replacement of ascending Aorta h. Resuspension Aortic Valve without replacement of ascending Aorta i. Resection Sub-Aortic Stenosis
01/06 I am reviewing a patient who recently underwent a Homograft Bentall procedure. I am unsure how I should code this for sequence #'s 1630 and 1680. A homograft aortic valve (24mm) was used.
Bentall Procedure with a Homograft Valved Conduit would be coded as Seq# 1630 OpAortic = Root Reconstruction w/ Valve Conduit and Seq# 1680 VSAoImTy = H (Homograft)
CC/TM 2/05 Procedures F- I in the Data Field Intent/Clarification section of the Training Manual, for seq# 1630, VS-Aortic Proc-Procedure, should read: #1630: F: Root reconstruction with Valve sparing: The Aortic root is reconstructed/replaced, typically secondary to aortic dissection, while the native aortic valve is left intact. The root is typically reconstructed utilizing a conduit or type of prosthetic material. *ascending aorta reconstructed/replaced *native aortic valve left intact #1630: G: Resuspension aortic valve with replacement of ascending aorta: The native aortic valve is grossly anatomically normal but because of a diseased ascending aorta (most often due to a type II aortic aneurysm) aortic insufficiency/regurgitation is created. The Ascending aorta is replaced with a graft conduit. The aortic valve is excised and re-suspended (re-sutured) in such a way as to create a more normal shape thereby reducing the insufficiency/regurgitation. *Native ascending aorta reconstructed/replaced *Native aortic valve excised and re-suspended (re-sutured) in original position #1630: H: Resuspension aortic valve without replacement of ascending aorta: The native aortic valve is grossly anatomically normal. The native ascending aorta is grossly anatomically normal. Obstruction of flow through the aortic valve has been created due to an overgrowth (hypertrophied) of the sub aortic fibrous membrane. The native aortic valve is excised and re-suspended (re-sutured) to allow for the excising of the overgrowth or excess fibrous membrane. Surgical intervention is required when either the growth of the membrane invades the aortic valve structure or when the growth inhibits the hemodynamic flow and creates significant increase in flow gradients across the aortic valve and/or significantly increases the pressure load on the left ventricle. *Native ascending aorta left intact
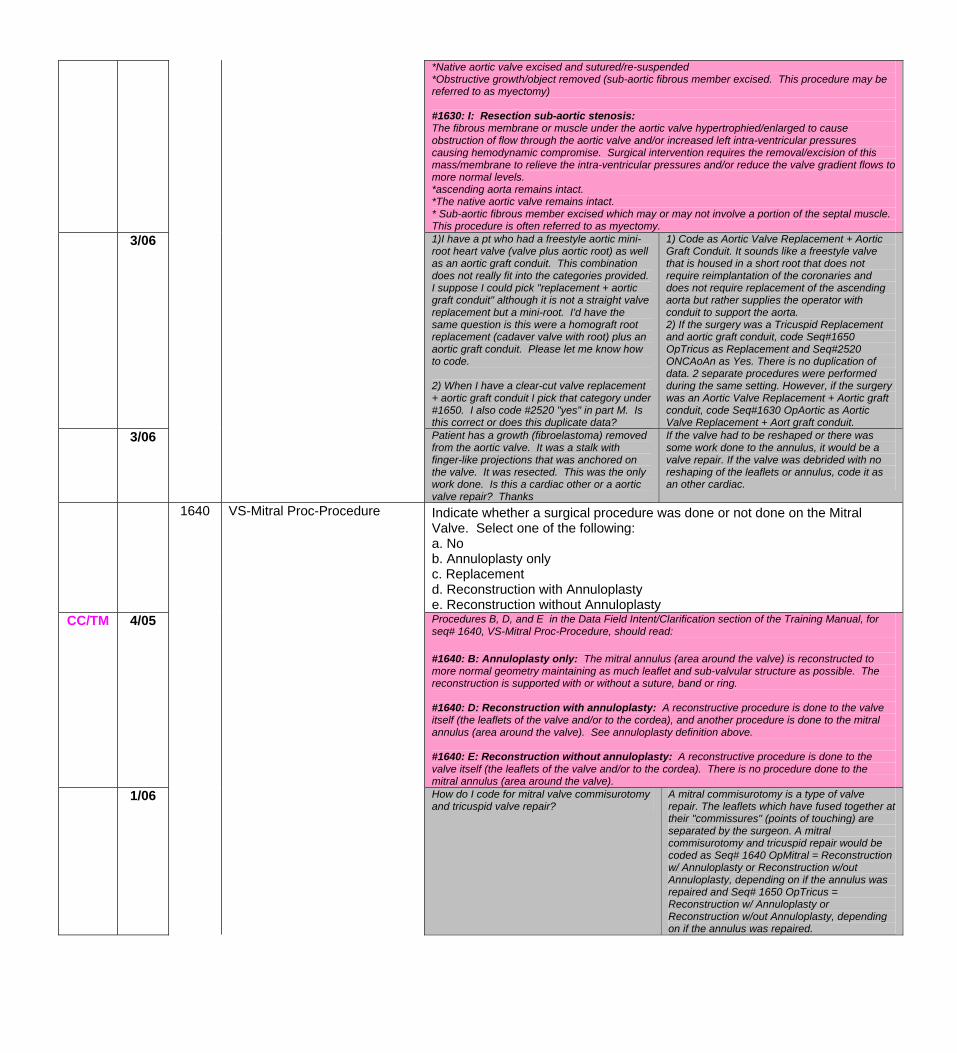
*Native aortic valve excised and sutured/re-suspended *Obstructive growth/object removed (sub-aortic fibrous member excised. This procedure may be referred to as myectomy) #1630: I: Resection sub-aortic stenosis: The fibrous membrane or muscle under the aortic valve hypertrophied/enlarged to cause obstruction of flow through the aortic valve and/or increased left intra-ventricular pressures causing hemodynamic compromise. Surgical intervention requires the removal/excision of this mass/membrane to relieve the intra-ventricular pressures and/or reduce the valve gradient flows to more normal levels. *ascending aorta remains intact. *The native aortic valve remains intact. * Sub-aortic fibrous member excised which may or may not involve a portion of the septal muscle. This procedure is often referred to as myectomy.
3/06 1)I have a pt who had a freestyle aortic mini-root heart valve (valve plus aortic root) as well as an aortic graft conduit. This combination does not really fit into the categories provided. I suppose I could pick "replacement + aortic graft conduit" although it is not a straight valve replacement but a mini-root. I'd have the same question is this were a homograft root replacement (cadaver valve with root) plus an aortic graft conduit. Please let me know how to code. 2) When I have a clear-cut valve replacement + aortic graft conduit I pick that category under #1650. I also code #2520 "yes" in part M. Is this correct or does this duplicate data?
1) Code as Aortic Valve Replacement + Aortic Graft Conduit. It sounds like a freestyle valve that is housed in a short root that does not require reimplantation of the coronaries and does not require replacement of the ascending aorta but rather supplies the operator with conduit to support the aorta. 2) If the surgery was a Tricuspid Replacement and aortic graft conduit, code Seq#1650 OpTricus as Replacement and Seq#2520 ONCAoAn as Yes. There is no duplication of data. 2 separate procedures were performed during the same setting. However, if the surgery was an Aortic Valve Replacement + Aortic graft conduit, code Seq#1630 OpAortic as Aortic Valve Replacement + Aort graft conduit.
3/06 Patient has a growth (fibroelastoma) removed from the aortic valve. It was a stalk with finger-like projections that was anchored on the valve. It was resected. This was the only work done. Is this a cardiac other or a aortic valve repair? Thanks
If the valve had to be reshaped or there was some work done to the annulus, it would be a valve repair. If the valve was debrided with no reshaping of the leaflets or annulus, code it as an other cardiac.
1640 VS-Mitral Proc-Procedure Indicate whether a surgical procedure was done or not done on the Mitral Valve. Select one of the following: a. No b. Annuloplasty only c. Replacement d. Reconstruction with Annuloplasty e. Reconstruction without Annuloplasty
CC/TM 4/05 Procedures B, D, and E in the Data Field Intent/Clarification section of the Training Manual, for seq# 1640, VS-Mitral Proc-Procedure, should read: #1640: B: Annuloplasty only: The mitral annulus (area around the valve) is reconstructed to more normal geometry maintaining as much leaflet and sub-valvular structure as possible. The reconstruction is supported with or without a suture, band or ring. #1640: D: Reconstruction with annuloplasty: A reconstructive procedure is done to the valve itself (the leaflets of the valve and/or to the cordea), and another procedure is done to the mitral annulus (area around the valve). See annuloplasty definition above. #1640: E: Reconstruction without annuloplasty: A reconstructive procedure is done to the valve itself (the leaflets of the valve and/or to the cordea). There is no procedure done to the mitral annulus (area around the valve).
1/06 How do I code for mitral valve commisurotomy and tricuspid valve repair?
A mitral commisurotomy is a type of valve repair. The leaflets which have fused together at their "commissures" (points of touching) are separated by the surgeon. A mitral commisurotomy and tricuspid repair would be coded as Seq# 1640 OpMitral = Reconstruction w/ Annuloplasty or Reconstruction w/out Annuloplasty, depending on if the annulus was repaired and Seq# 1650 OpTricus = Reconstruction w/ Annuloplasty or Reconstruction w/out Annuloplasty, depending on if the annulus was repaired.
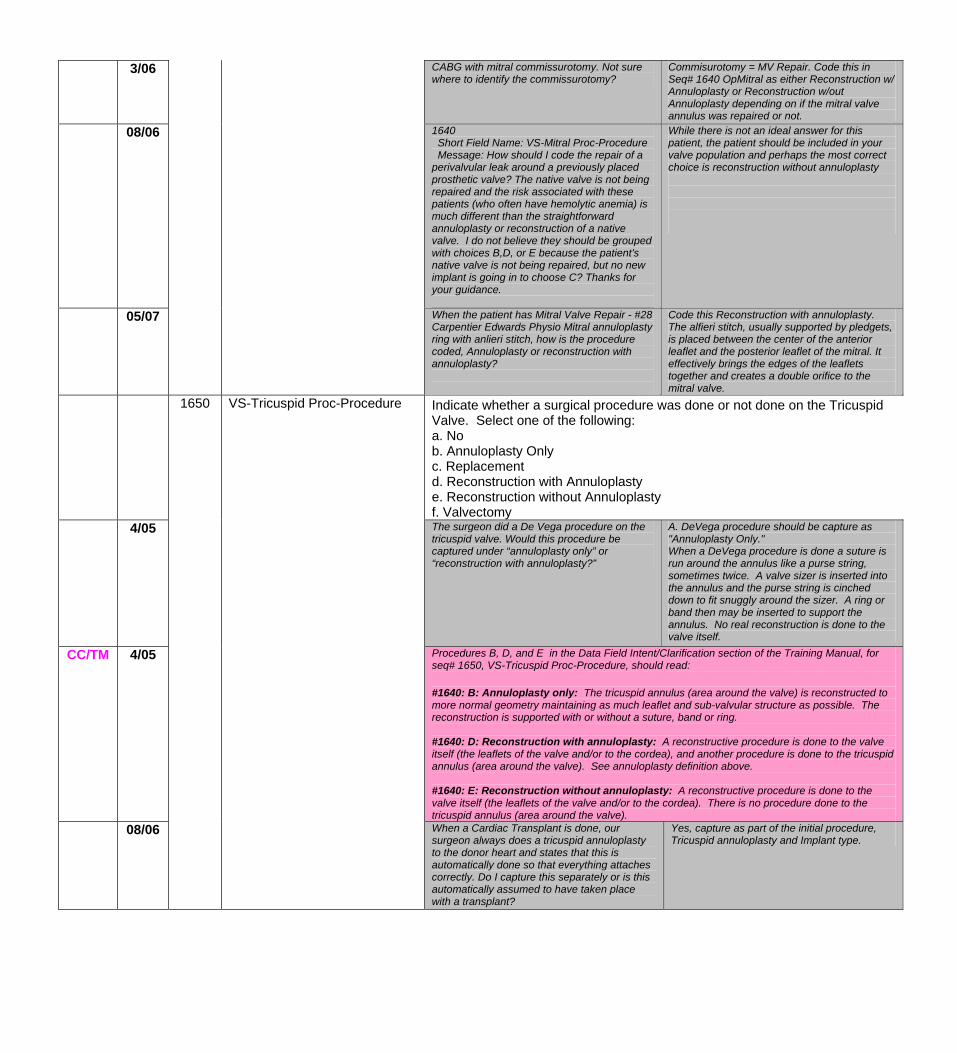
3/06 CABG with mitral commissurotomy. Not sure where to identify the commissurotomy?
Commisurotomy = MV Repair. Code this in Seq# 1640 OpMitral as either Reconstruction w/ Annuloplasty or Reconstruction w/out Annuloplasty depending on if the mitral valve annulus was repaired or not.
08/06 1640 Short Field Name: VS-Mitral Proc-Procedure Message: How should I code the repair of a perivalvular leak around a previously placed prosthetic valve? The native valve is not being repaired and the risk associated with these patients (who often have hemolytic anemia) is much different than the straightforward annuloplasty or reconstruction of a native valve. I do not believe they should be grouped with choices B,D, or E because the patient's native valve is not being repaired, but no new implant is going in to choose C? Thanks for your guidance.
While there is not an ideal answer for this patient, the patient should be included in your valve population and perhaps the most correct choice is reconstruction without annuloplasty
05/07
When the patient has Mitral Valve Repair - #28 Carpentier Edwards Physio Mitral annuloplasty ring with anlieri stitch, how is the procedure coded, Annuloplasty or reconstruction with annuloplasty?
Code this Reconstruction with annuloplasty. The alfieri stitch, usually supported by pledgets, is placed between the center of the anterior leaflet and the posterior leaflet of the mitral. It effectively brings the edges of the leaflets together and creates a double orifice to the mitral valve.
Indicate whether a surgical procedure was done or not done on the Tricuspid Valve. Select one of the following: a. No b. Annuloplasty Only c. Replacement d. Reconstruction with Annuloplasty e. Reconstruction without Annuloplasty f. Valvectomy
4/05
1650 VS-Tricuspid Proc-Procedure
The surgeon did a De Vega procedure on the tricuspid valve. Would this procedure be captured under “annuloplasty only” or “reconstruction with annuloplasty?”
A. DeVega procedure should be capture as "Annuloplasty Only." When a DeVega procedure is done a suture is run around the annulus like a purse string, sometimes twice. A valve sizer is inserted into the annulus and the purse string is cinched down to fit snuggly around the sizer. A ring or band then may be inserted to support the annulus. No real reconstruction is done to the valve itself.
CC/TM 4/05 Procedures B, D, and E in the Data Field Intent/Clarification section of the Training Manual, for seq# 1650, VS-Tricuspid Proc-Procedure, should read: #1640: B: Annuloplasty only: The tricuspid annulus (area around the valve) is reconstructed to more normal geometry maintaining as much leaflet and sub-valvular structure as possible. The reconstruction is supported with or without a suture, band or ring. #1640: D: Reconstruction with annuloplasty: A reconstructive procedure is done to the valve itself (the leaflets of the valve and/or to the cordea), and another procedure is done to the tricuspid annulus (area around the valve). See annuloplasty definition above. #1640: E: Reconstruction without annuloplasty: A reconstructive procedure is done to the valve itself (the leaflets of the valve and/or to the cordea). There is no procedure done to the tricuspid annulus (area around the valve).
08/06
When a Cardiac Transplant is done, our surgeon always does a tricuspid annuloplasty to the donor heart and states that this is automatically done so that everything attaches correctly. Do I capture this separately or is this automatically assumed to have taken place with a transplant?
Yes, capture as part of the initial procedure, Tricuspid annuloplasty and Implant type.
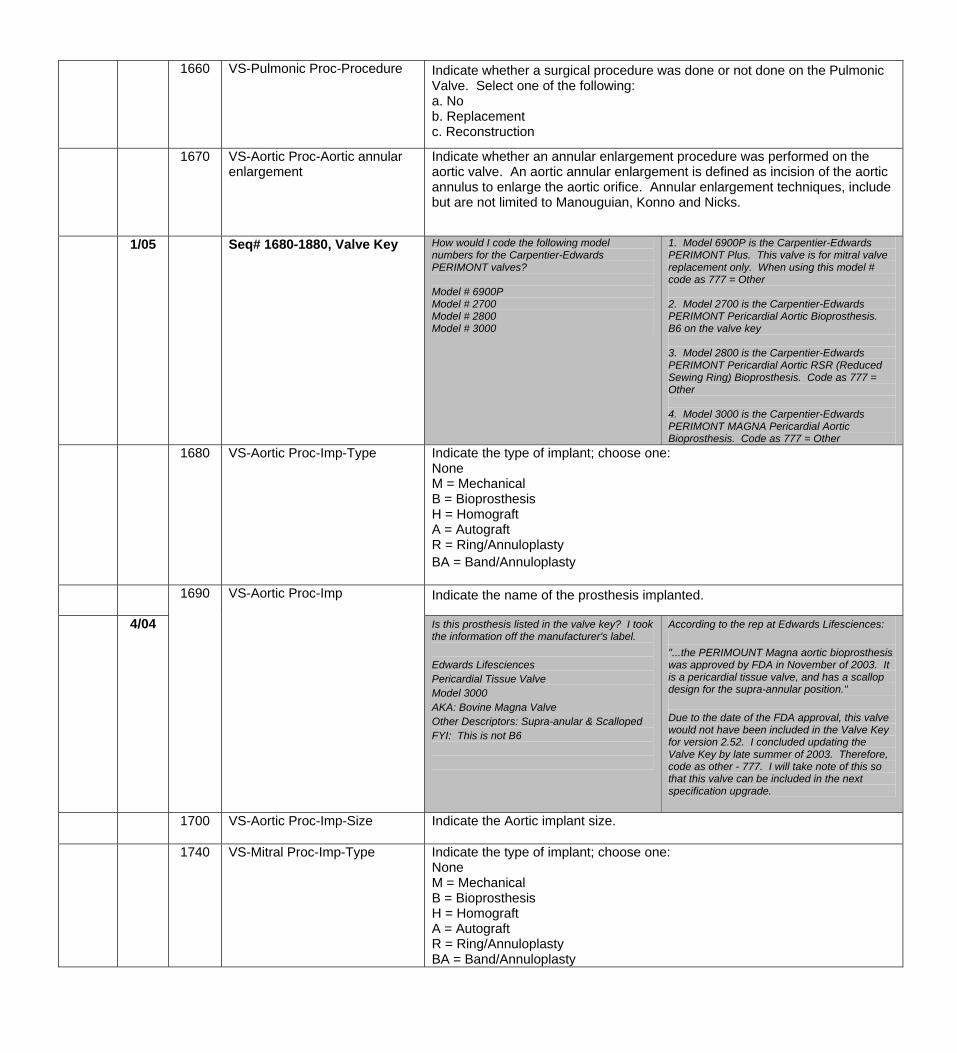
1660 VS-Pulmonic Proc-Procedure Indicate whether a surgical procedure was done or not done on the Pulmonic Valve. Select one of the following: a. No b. Replacement c. Reconstruction
1670 VS-Aortic Proc-Aortic annular enlargement
Indicate whether an annular enlargement procedure was performed on the aortic valve. An aortic annular enlargement is defined as incision of the aortic annulus to enlarge the aortic orifice. Annular enlargement techniques, include but are not limited to Manouguian, Konno and Nicks.
1/05 Seq# 1680-1880, Valve Key
How would I code the following model numbers for the Carpentier-Edwards PERIMONT valves? Model # 6900P Model # 2700 Model # 2800 Model # 3000
1. Model 6900P is the Carpentier-Edwards PERIMONT Plus. This valve is for mitral valve replacement only. When using this model # code as 777 = Other 2. Model 2700 is the Carpentier-Edwards PERIMONT Pericardial Aortic Bioprosthesis. B6 on the valve key 3. Model 2800 is the Carpentier-Edwards PERIMONT Pericardial Aortic RSR (Reduced Sewing Ring) Bioprosthesis. Code as 777 = Other 4. Model 3000 is the Carpentier-Edwards PERIMONT MAGNA Pericardial Aortic Bioprosthesis. Code as 777 = Other
1680 VS-Aortic Proc-Imp-Type
Indicate the type of implant; choose one: None M = Mechanical B = Bioprosthesis H = Homograft A = Autograft R = Ring/Annuloplasty BA = Band/Annuloplasty
1690 VS-Aortic Proc-Imp Indicate the name of the prosthesis implanted.
4/04 Is this prosthesis listed in the valve key? I took the information off the manufacturer's label. Edwards Lifesciences Pericardial Tissue Valve Model 3000 AKA: Bovine Magna Valve Other Descriptors: Supra-anular & Scalloped FYI: This is not B6
According to the rep at Edwards Lifesciences: "...the PERIMOUNT Magna aortic bioprosthesis was approved by FDA in November of 2003. It is a pericardial tissue valve, and has a scallop design for the supra-annular position." Due to the date of the FDA approval, this valve would not have been included in the Valve Key for version 2.52. I concluded updating the Valve Key by late summer of 2003. Therefore, code as other - 777. I will take note of this so that this valve can be included in the next specification upgrade.
1700
VS-Aortic Proc-Imp-Size
Indicate the Aortic implant size.
1740 VS-Mitral Proc-Imp-Type Indicate the type of implant; choose one: None M = Mechanical B = Bioprosthesis H = Homograft A = Autograft R = Ring/Annuloplasty BA = Band/Annuloplasty
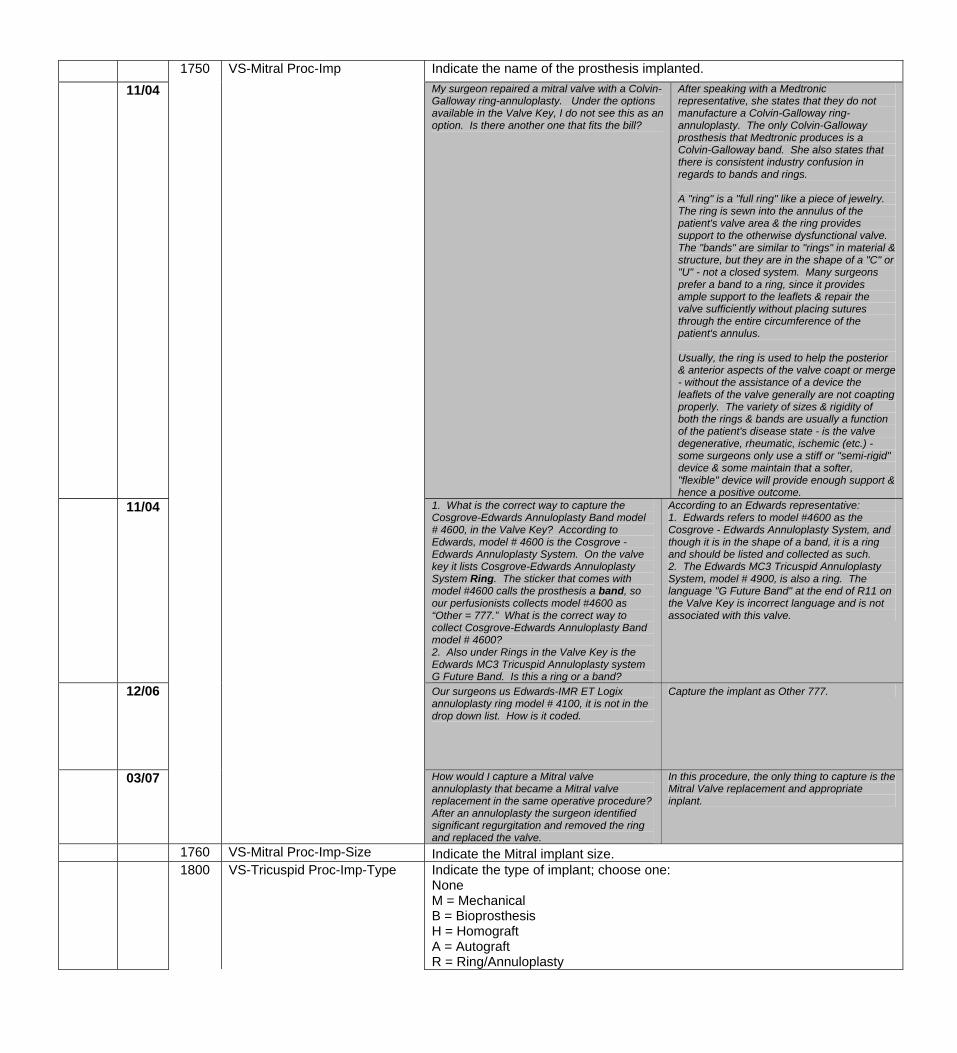
1750 VS-Mitral Proc-Imp Indicate the name of the prosthesis implanted. 11/04 My surgeon repaired a mitral valve with a Colvin-
Galloway ring-annuloplasty. Under the options available in the Valve Key, I do not see this as an option. Is there another one that fits the bill?
After speaking with a Medtronic representative, she states that they do not manufacture a Colvin-Galloway ring-annuloplasty. The only Colvin-Galloway prosthesis that Medtronic produces is a Colvin-Galloway band. She also states that there is consistent industry confusion in regards to bands and rings. A "ring" is a "full ring" like a piece of jewelry. The ring is sewn into the annulus of the patient's valve area & the ring provides support to the otherwise dysfunctional valve. The "bands" are similar to "rings" in material & structure, but they are in the shape of a "C" or "U" - not a closed system. Many surgeons prefer a band to a ring, since it provides ample support to the leaflets & repair the valve sufficiently without placing sutures through the entire circumference of the patient's annulus. Usually, the ring is used to help the posterior & anterior aspects of the valve coapt or merge - without the assistance of a device the leaflets of the valve generally are not coapting properly. The variety of sizes & rigidity of both the rings & bands are usually a function of the patient's disease state - is the valve degenerative, rheumatic, ischemic (etc.) - some surgeons only use a stiff or "semi-rigid" device & some maintain that a softer, "flexible" device will provide enough support & hence a positive outcome.
11/04
1. What is the correct way to capture the Cosgrove-Edwards Annuloplasty Band model # 4600, in the Valve Key? According to Edwards, model # 4600 is the Cosgrove - Edwards Annuloplasty System. On the valve key it lists Cosgrove-Edwards Annuloplasty System Ring. The sticker that comes with model #4600 calls the prosthesis a band, so our perfusionists collects model #4600 as “Other = 777.” What is the correct way to collect Cosgrove-Edwards Annuloplasty Band model # 4600? 2. Also under Rings in the Valve Key is the Edwards MC3 Tricuspid Annuloplasty system G Future Band. Is this a ring or a band?
According to an Edwards representative: 1. Edwards refers to model #4600 as the Cosgrove - Edwards Annuloplasty System, and though it is in the shape of a band, it is a ring and should be listed and collected as such. 2. The Edwards MC3 Tricuspid Annuloplasty System, model # 4900, is also a ring. The language "G Future Band" at the end of R11 on the Valve Key is incorrect language and is not associated with this valve.
12/06
Our surgeons us Edwards-IMR ET Logix annuloplasty ring model # 4100, it is not in the drop down list. How is it coded.
Capture the implant as Other 777.
03/07
How would I capture a Mitral valve annuloplasty that became a Mitral valve replacement in the same operative procedure? After an annuloplasty the surgeon identified significant regurgitation and removed the ring and replaced the valve.
In this procedure, the only thing to capture is the Mitral Valve replacement and appropriate inplant.
1760 VS-Mitral Proc-Imp-Size Indicate the Mitral implant size. 1800
VS-Tricuspid Proc-Imp-Type
Indicate the type of implant; choose one: None M = Mechanical B = Bioprosthesis H = Homograft A = Autograft R = Ring/Annuloplasty
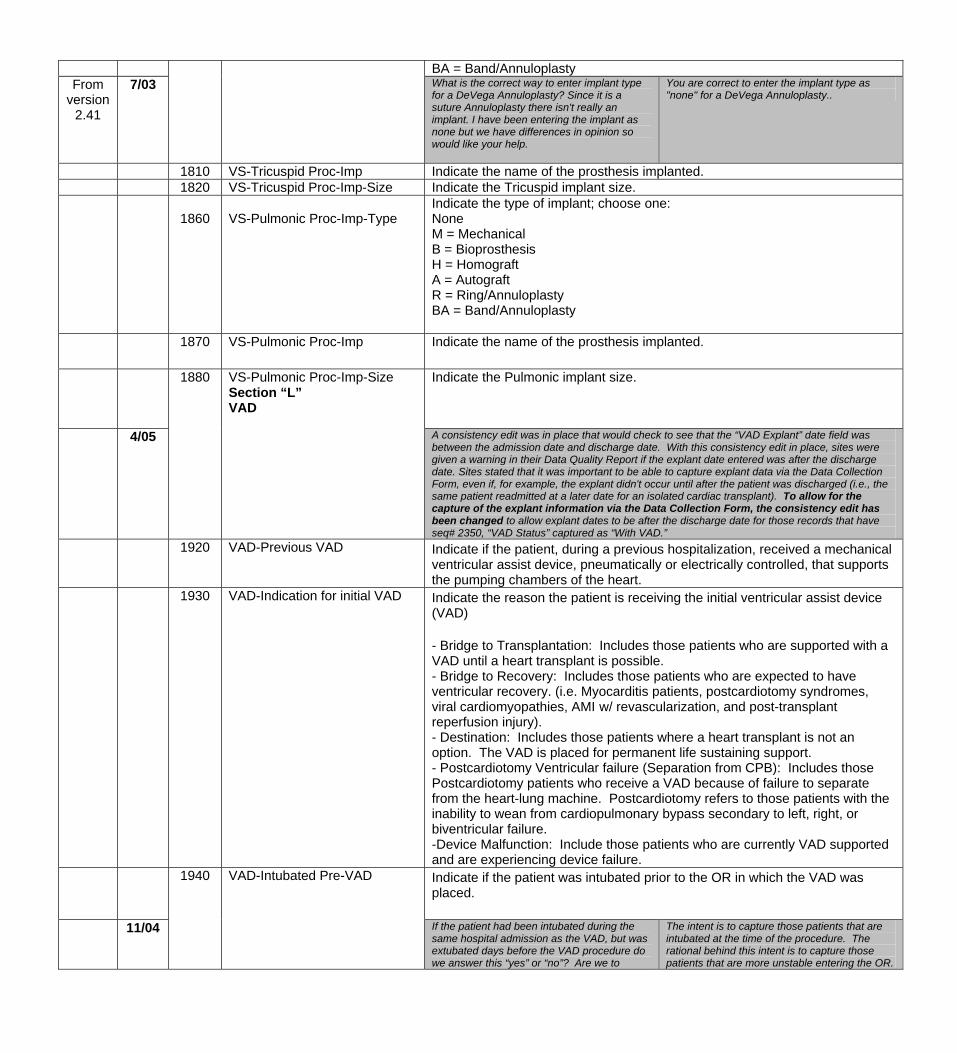
BA = Band/Annuloplasty From
version 2.41
7/03 What is the correct way to enter implant type for a DeVega Annuloplasty? Since it is a suture Annuloplasty there isn't really an implant. I have been entering the implant as none but we have differences in opinion so would like your help.
You are correct to enter the implant type as "none" for a DeVega Annuloplasty..
1810 VS-Tricuspid Proc-Imp Indicate the name of the prosthesis implanted. 1820 VS-Tricuspid Proc-Imp-Size Indicate the Tricuspid implant size.
1860 VS-Pulmonic Proc-Imp-Type
Indicate the type of implant; choose one: None M = Mechanical B = Bioprosthesis H = Homograft A = Autograft R = Ring/Annuloplasty BA = Band/Annuloplasty
1870 VS-Pulmonic Proc-Imp Indicate the name of the prosthesis implanted.
1880
VS-Pulmonic Proc-Imp-Size Section “L” VAD
Indicate the Pulmonic implant size.
4/05 A consistency edit was in place that would check to see that the “VAD Explant” date field was between the admission date and discharge date. With this consistency edit in place, sites were given a warning in their Data Quality Report if the explant date entered was after the discharge date. Sites stated that it was important to be able to capture explant data via the Data Collection Form, even if, for example, the explant didn't occur until after the patient was discharged (i.e., the same patient readmitted at a later date for an isolated cardiac transplant). To allow for the capture of the explant information via the Data Collection Form, the consistency edit has been changed to allow explant dates to be after the discharge date for those records that have seq# 2350, “VAD Status” captured as “With VAD.”
1920 VAD-Previous VAD Indicate if the patient, during a previous hospitalization, received a mechanical ventricular assist device, pneumatically or electrically controlled, that supports the pumping chambers of the heart.
1930 VAD-Indication for initial VAD Indicate the reason the patient is receiving the initial ventricular assist device (VAD) - Bridge to Transplantation: Includes those patients who are supported with a VAD until a heart transplant is possible. - Bridge to Recovery: Includes those patients who are expected to have ventricular recovery. (i.e. Myocarditis patients, postcardiotomy syndromes, viral cardiomyopathies, AMI w/ revascularization, and post-transplant reperfusion injury). - Destination: Includes those patients where a heart transplant is not an option. The VAD is placed for permanent life sustaining support. - Postcardiotomy Ventricular failure (Separation from CPB): Includes those Postcardiotomy patients who receive a VAD because of failure to separate from the heart-lung machine. Postcardiotomy refers to those patients with the inability to wean from cardiopulmonary bypass secondary to left, right, or biventricular failure. -Device Malfunction: Include those patients who are currently VAD supported and are experiencing device failure.
1940 VAD-Intubated Pre-VAD Indicate if the patient was intubated prior to the OR in which the VAD was placed.
11/04 If the patient had been intubated during the same hospital admission as the VAD, but was extubated days before the VAD procedure do we answer this “yes” or “no”? Are we to
The intent is to capture those patients that are intubated at the time of the procedure. The rational behind this intent is to capture those patients that are more unstable entering the OR.
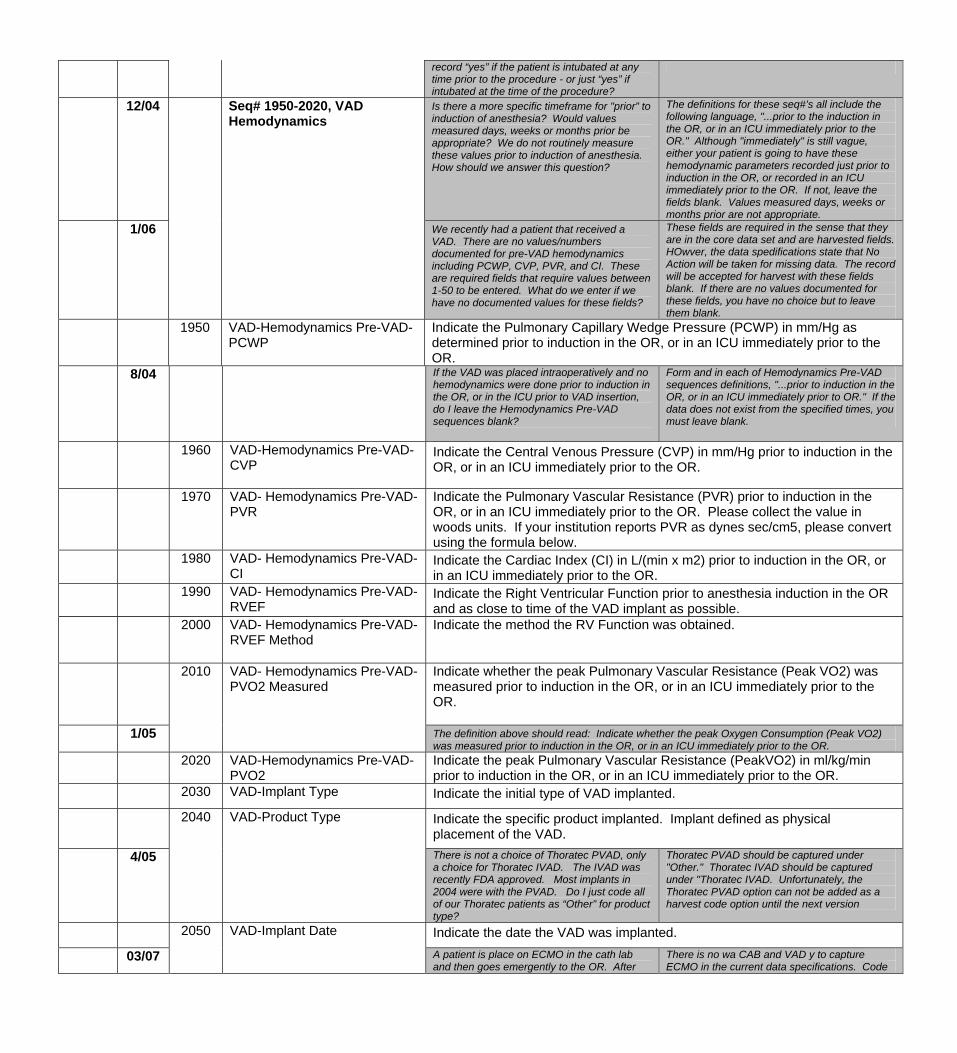
record “yes” if the patient is intubated at any time prior to the procedure - or just “yes” if intubated at the time of the procedure?
12/04 Seq# 1950-2020, VAD Hemodynamics
Is there a more specific timeframe for "prior” to induction of anesthesia? Would values measured days, weeks or months prior be appropriate? We do not routinely measure these values prior to induction of anesthesia. How should we answer this question?
The definitions for these seq#’s all include the following language, "...prior to the induction in the OR, or in an ICU immediately prior to the OR." Although "immediately" is still vague, either your patient is going to have these hemodynamic parameters recorded just prior to induction in the OR, or recorded in an ICU immediately prior to the OR. If not, leave the fields blank. Values measured days, weeks or months prior are not appropriate.
1/06 We recently had a patient that received a VAD. There are no values/numbers documented for pre-VAD hemodynamics including PCWP, CVP, PVR, and CI. These are required fields that require values between 1-50 to be entered. What do we enter if we have no documented values for these fields?
These fields are required in the sense that they are in the core data set and are harvested fields. HOwver, the data spedifications state that No Action will be taken for missing data. The record will be accepted for harvest with these fields blank. If there are no values documented for these fields, you have no choice but to leave them blank.
1950 VAD-Hemodynamics Pre-VAD-PCWP
Indicate the Pulmonary Capillary Wedge Pressure (PCWP) in mm/Hg as determined prior to induction in the OR, or in an ICU immediately prior to the OR.
8/04 If the VAD was placed intraoperatively and no hemodynamics were done prior to induction in the OR, or in the ICU prior to VAD insertion, do I leave the Hemodynamics Pre-VAD sequences blank?
Form and in each of Hemodynamics Pre-VAD sequences definitions, "...prior to induction in the OR, or in an ICU immediately prior to OR." If the data does not exist from the specified times, you must leave blank.
1960
VAD-Hemodynamics Pre-VAD-CVP
Indicate the Central Venous Pressure (CVP) in mm/Hg prior to induction in the OR, or in an ICU immediately prior to the OR.
1970 VAD- Hemodynamics Pre-VAD-PVR
Indicate the Pulmonary Vascular Resistance (PVR) prior to induction in the OR, or in an ICU immediately prior to the OR. Please collect the value in woods units. If your institution reports PVR as dynes sec/cm5, please convert using the formula below.
1980
VAD- Hemodynamics Pre-VAD-CI
Indicate the Cardiac Index (CI) in L/(min x m2) prior to induction in the OR, or in an ICU immediately prior to the OR.
1990 VAD- Hemodynamics Pre-VAD-RVEF
Indicate the Right Ventricular Function prior to anesthesia induction in the OR and as close to time of the VAD implant as possible.
2000
VAD- Hemodynamics Pre-VAD-RVEF Method
Indicate the method the RV Function was obtained.
2010 VAD- Hemodynamics Pre-VAD-PVO2 Measured
Indicate whether the peak Pulmonary Vascular Resistance (Peak VO2) was measured prior to induction in the OR, or in an ICU immediately prior to the OR.
1/05 The definition above should read: Indicate whether the peak Oxygen Consumption (Peak VO2) was measured prior to induction in the OR, or in an ICU immediately prior to the OR.
2020 VAD-Hemodynamics Pre-VAD-PVO2
Indicate the peak Pulmonary Vascular Resistance (PeakVO2) in ml/kg/min prior to induction in the OR, or in an ICU immediately prior to the OR.
2030 VAD-Implant Type Indicate the initial type of VAD implanted. 2040 VAD-Product Type Indicate the specific product implanted. Implant defined as physical
placement of the VAD. 4/05
There is not a choice of Thoratec PVAD, only a choice for Thoratec IVAD. The IVAD was recently FDA approved. Most implants in 2004 were with the PVAD. Do I just code all of our Thoratec patients as “Other” for product type?
Thoratec PVAD should be captured under "Other." Thoratec IVAD should be captured under "Thoratec IVAD. Unfortunately, the Thoratec PVAD option can not be added as a harvest code option until the next version
2050 VAD-Implant Date Indicate the date the VAD was implanted.
03/07 A patient is place on ECMO in the cath lab and then goes emergently to the OR. After
There is no wa CAB and VAD y to capture ECMO in the current data specifications. Code
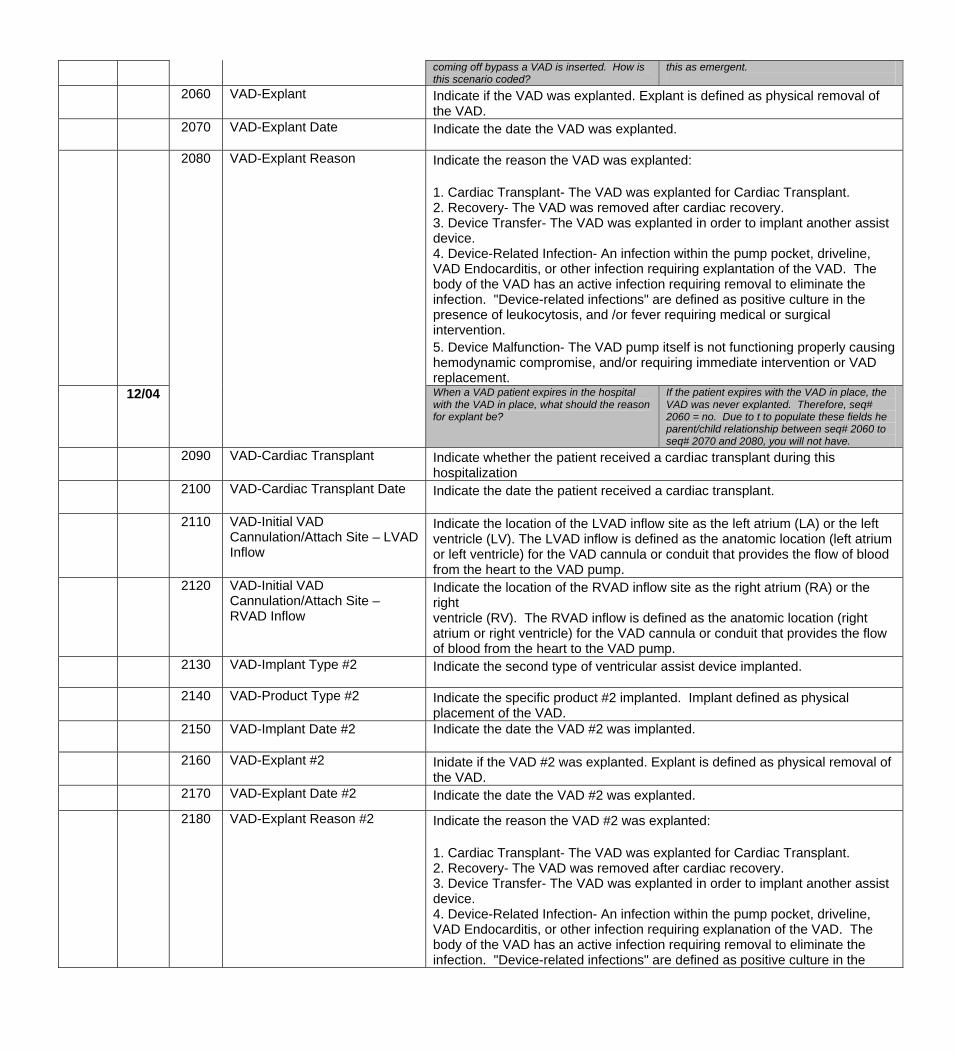
coming off bypass a VAD is inserted. How is this scenario coded?
this as emergent.
2060 VAD-Explant Indicate if the VAD was explanted. Explant is defined as physical removal of the VAD.
2070
VAD-Explant Date
Indicate the date the VAD was explanted.
2080 VAD-Explant Reason Indicate the reason the VAD was explanted: 1. Cardiac Transplant- The VAD was explanted for Cardiac Transplant. 2. Recovery- The VAD was removed after cardiac recovery. 3. Device Transfer- The VAD was explanted in order to implant another assist device. 4. Device-Related Infection- An infection within the pump pocket, driveline, VAD Endocarditis, or other infection requiring explantation of the VAD. The body of the VAD has an active infection requiring removal to eliminate the infection. "Device-related infections" are defined as positive culture in the presence of leukocytosis, and /or fever requiring medical or surgical intervention. 5. Device Malfunction- The VAD pump itself is not functioning properly causing hemodynamic compromise, and/or requiring immediate intervention or VAD replacement.
12/04 When a VAD patient expires in the hospital with the VAD in place, what should the reason for explant be?
If the patient expires with the VAD in place, the VAD was never explanted. Therefore, seq# 2060 = no. Due to t to populate these fields he parent/child relationship between seq# 2060 to seq# 2070 and 2080, you will not have.
2090 VAD-Cardiac Transplant
Indicate whether the patient received a cardiac transplant during this hospitalization
2100 VAD-Cardiac Transplant Date Indicate the date the patient received a cardiac transplant.
2110 VAD-Initial VAD Cannulation/Attach Site – LVAD Inflow
Indicate the location of the LVAD inflow site as the left atrium (LA) or the left ventricle (LV). The LVAD inflow is defined as the anatomic location (left atrium or left ventricle) for the VAD cannula or conduit that provides the flow of blood from the heart to the VAD pump.
2120 VAD-Initial VAD Cannulation/Attach Site – RVAD Inflow
Indicate the location of the RVAD inflow site as the right atrium (RA) or the right ventricle (RV). The RVAD inflow is defined as the anatomic location (right atrium or right ventricle) for the VAD cannula or conduit that provides the flow of blood from the heart to the VAD pump.
2130
VAD-Implant Type #2
Indicate the second type of ventricular assist device implanted.
2140 VAD-Product Type #2 Indicate the specific product #2 implanted. Implant defined as physical placement of the VAD.
2150
VAD-Implant Date #2
Indicate the date the VAD #2 was implanted.
2160 VAD-Explant #2 Inidate if the VAD #2 was explanted. Explant is defined as physical removal of the VAD.
2170 VAD-Explant Date #2 Indicate the date the VAD #2 was explanted. 2180 VAD-Explant Reason #2 Indicate the reason the VAD #2 was explanted:
1. Cardiac Transplant- The VAD was explanted for Cardiac Transplant. 2. Recovery- The VAD was removed after cardiac recovery. 3. Device Transfer- The VAD was explanted in order to implant another assist device. 4. Device-Related Infection- An infection within the pump pocket, driveline, VAD Endocarditis, or other infection requiring explanation of the VAD. The body of the VAD has an active infection requiring removal to eliminate the infection. "Device-related infections" are defined as positive culture in the
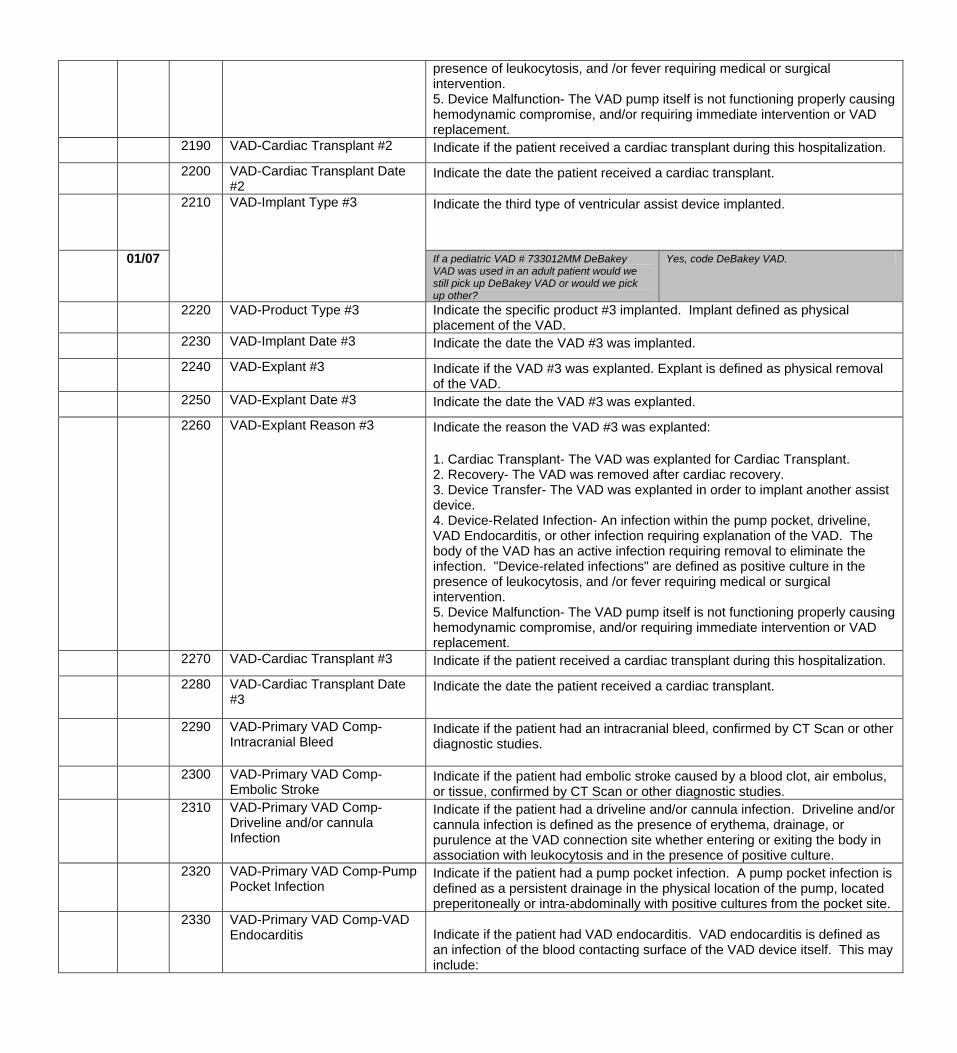
presence of leukocytosis, and /or fever requiring medical or surgical intervention. 5. Device Malfunction- The VAD pump itself is not functioning properly causing hemodynamic compromise, and/or requiring immediate intervention or VAD replacement.
2190 VAD-Cardiac Transplant #2 Indicate if the patient received a cardiac transplant during this hospitalization. 2200 VAD-Cardiac Transplant Date
#2 Indicate the date the patient received a cardiac transplant.
2210 VAD-Implant Type #3 Indicate the third type of ventricular assist device implanted.
01/07 If a pediatric VAD # 733012MM DeBakey VAD was used in an adult patient would we still pick up DeBakey VAD or would we pick up other?
Yes, code DeBakey VAD.
2220 VAD-Product Type #3 Indicate the specific product #3 implanted. Implant defined as physical placement of the VAD.
2230 VAD-Implant Date #3 Indicate the date the VAD #3 was implanted. 2240 VAD-Explant #3 Indicate if the VAD #3 was explanted. Explant is defined as physical removal
of the VAD. 2250 VAD-Explant Date #3 Indicate the date the VAD #3 was explanted. 2260 VAD-Explant Reason #3 Indicate the reason the VAD #3 was explanted:
1. Cardiac Transplant- The VAD was explanted for Cardiac Transplant. 2. Recovery- The VAD was removed after cardiac recovery. 3. Device Transfer- The VAD was explanted in order to implant another assist device. 4. Device-Related Infection- An infection within the pump pocket, driveline, VAD Endocarditis, or other infection requiring explanation of the VAD. The body of the VAD has an active infection requiring removal to eliminate the infection. "Device-related infections" are defined as positive culture in the presence of leukocytosis, and /or fever requiring medical or surgical intervention. 5. Device Malfunction- The VAD pump itself is not functioning properly causing hemodynamic compromise, and/or requiring immediate intervention or VAD replacement.
2270 VAD-Cardiac Transplant #3 Indicate if the patient received a cardiac transplant during this hospitalization. 2280 VAD-Cardiac Transplant Date
#3 Indicate the date the patient received a cardiac transplant.
2290 VAD-Primary VAD Comp-Intracranial Bleed
Indicate if the patient had an intracranial bleed, confirmed by CT Scan or other diagnostic studies.
2300 VAD-Primary VAD Comp-Embolic Stroke
Indicate if the patient had embolic stroke caused by a blood clot, air embolus, or tissue, confirmed by CT Scan or other diagnostic studies.
2310 VAD-Primary VAD Comp-Driveline and/or cannula Infection
Indicate if the patient had a driveline and/or cannula infection. Driveline and/or cannula infection is defined as the presence of erythema, drainage, or purulence at the VAD connection site whether entering or exiting the body in association with leukocytosis and in the presence of positive culture.
2320 VAD-Primary VAD Comp-Pump Pocket Infection
Indicate if the patient had a pump pocket infection. A pump pocket infection is defined as a persistent drainage in the physical location of the pump, located preperitoneally or intra-abdominally with positive cultures from the pocket site.
2330 VAD-Primary VAD Comp-VAD Endocarditis Indicate if the patient had VAD endocarditis. VAD endocarditis is defined as
an infection of the blood contacting surface of the VAD device itself. This may include:
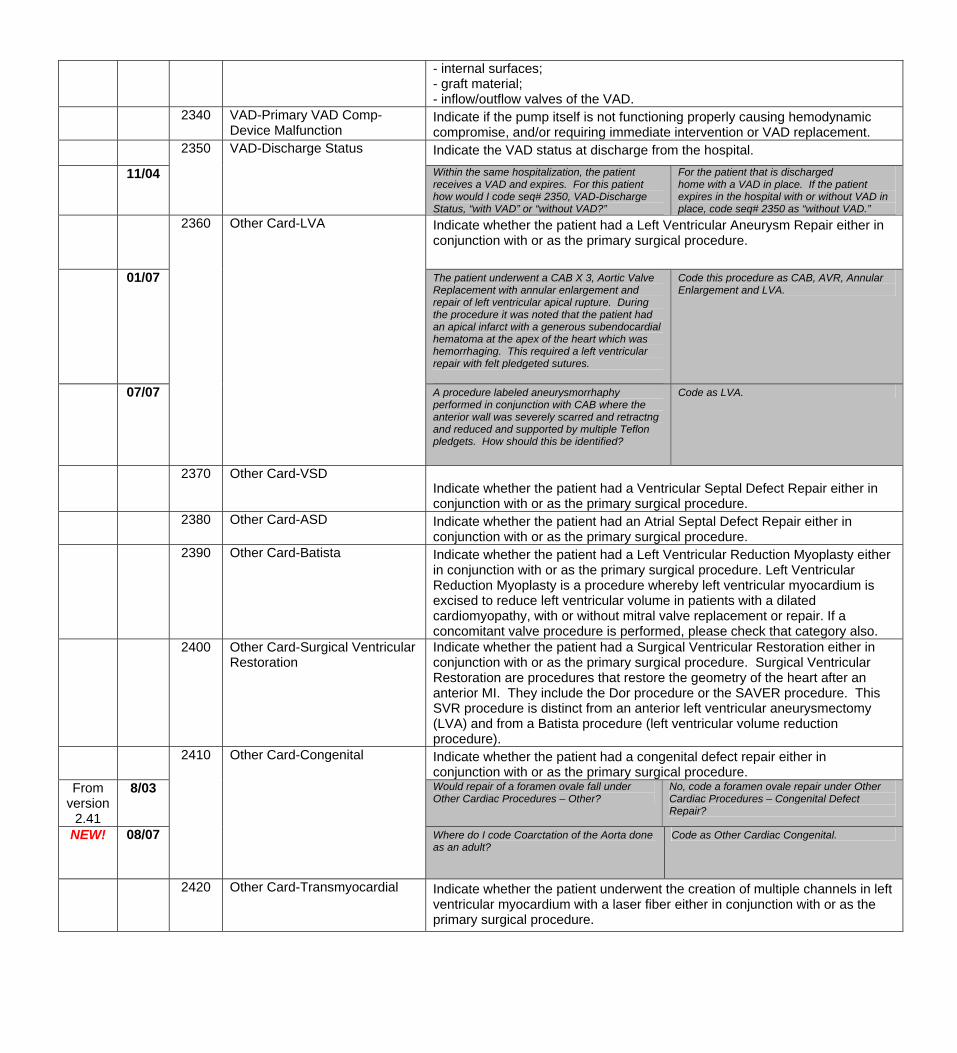
- internal surfaces; - graft material; - inflow/outflow valves of the VAD.
2340 VAD-Primary VAD Comp-Device Malfunction
Indicate if the pump itself is not functioning properly causing hemodynamic compromise, and/or requiring immediate intervention or VAD replacement.
2350 VAD-Discharge Status Indicate the VAD status at discharge from the hospital. 11/04 Within the same hospitalization, the patient
receives a VAD and expires. For this patient how would I code seq# 2350, VAD-Discharge Status, “with VAD” or “without VAD?”
For the patient that is discharged home with a VAD in place. If the patient expires in the hospital with or without VAD in place, code seq# 2350 as “without VAD.”
2360 Other Card-LVA Indicate whether the patient had a Left Ventricular Aneurysm Repair either in conjunction with or as the primary surgical procedure.
01/07 The patient underwent a CAB X 3, Aortic Valve Replacement with annular enlargement and repair of left ventricular apical rupture. During the procedure it was noted that the patient had an apical infarct with a generous subendocardial hematoma at the apex of the heart which was hemorrhaging. This required a left ventricular repair with felt pledgeted sutures.
Code this procedure as CAB, AVR, Annular Enlargement and LVA.
07/07 A procedure labeled aneurysmorrhaphy performed in conjunction with CAB where the anterior wall was severely scarred and retractng and reduced and supported by multiple Teflon pledgets. How should this be identified?
Code as LVA.
2370 Other Card-VSD Indicate whether the patient had a Ventricular Septal Defect Repair either in conjunction with or as the primary surgical procedure.
2380 Other Card-ASD Indicate whether the patient had an Atrial Septal Defect Repair either in conjunction with or as the primary surgical procedure.
2390
Other Card-Batista
Indicate whether the patient had a Left Ventricular Reduction Myoplasty either in conjunction with or as the primary surgical procedure. Left Ventricular Reduction Myoplasty is a procedure whereby left ventricular myocardium is excised to reduce left ventricular volume in patients with a dilated cardiomyopathy, with or without mitral valve replacement or repair. If a concomitant valve procedure is performed, please check that category also.
2400 Other Card-Surgical Ventricular Restoration
Indicate whether the patient had a Surgical Ventricular Restoration either in conjunction with or as the primary surgical procedure. Surgical Ventricular Restoration are procedures that restore the geometry of the heart after an anterior MI. They include the Dor procedure or the SAVER procedure. This SVR procedure is distinct from an anterior left ventricular aneurysmectomy (LVA) and from a Batista procedure (left ventricular volume reduction procedure).
Indicate whether the patient had a congenital defect repair either in conjunction with or as the primary surgical procedure.
From version
2.41
8/03
2410
Other Card-Congenital
Would repair of a foramen ovale fall under Other Cardiac Procedures – Other?
No, code a foramen ovale repair under Other Cardiac Procedures – Congenital Defect Repair?
NEW!
08/07
Where do I code Coarctation of the Aorta done as an adult?
Code as Other Cardiac Congenital.
2420 Other Card-Transmyocardial Indicate whether the patient underwent the creation of multiple channels in left ventricular myocardium with a laser fiber either in conjunction with or as the primary surgical procedure.
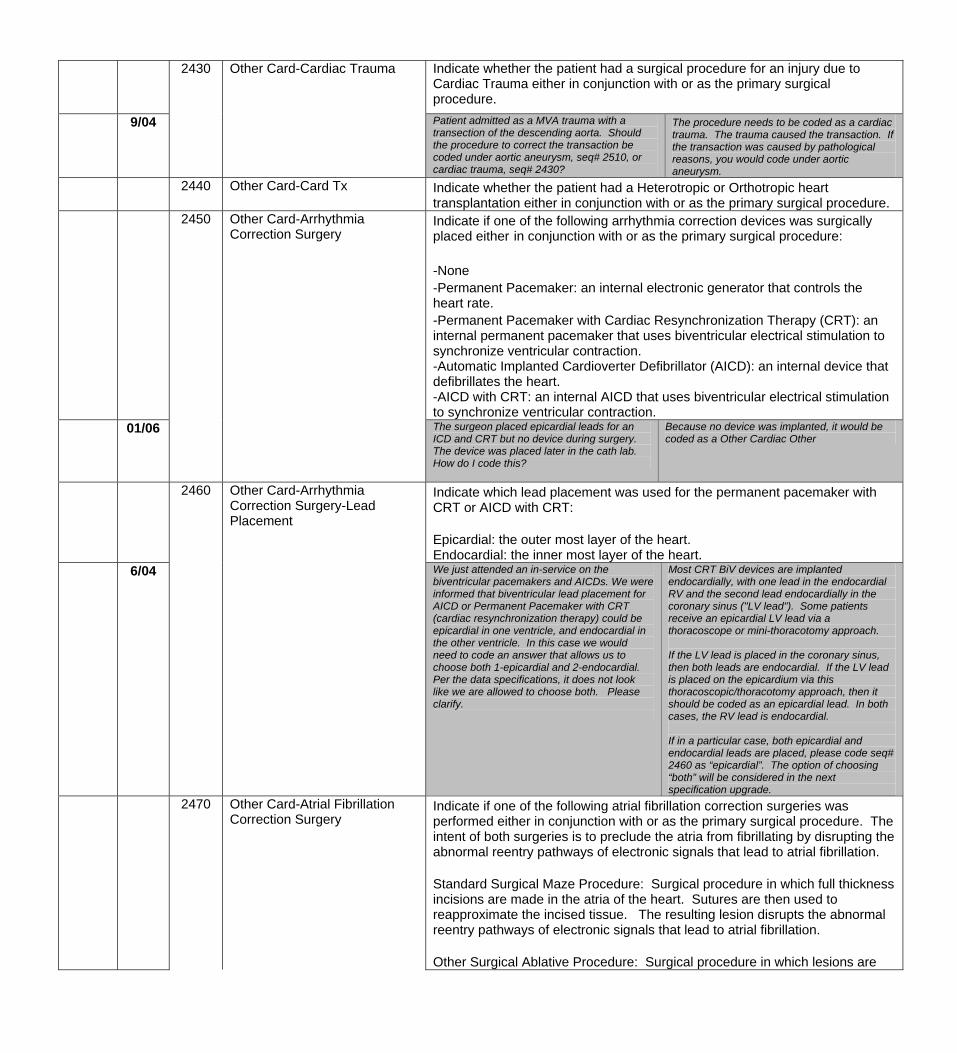
2430 Other Card-Cardiac Trauma Indicate whether the patient had a surgical procedure for an injury due to Cardiac Trauma either in conjunction with or as the primary surgical procedure.
9/04 Patient admitted as a MVA trauma with a transection of the descending aorta. Should the procedure to correct the transaction be coded under aortic aneurysm, seq# 2510, or cardiac trauma, seq# 2430?
The procedure needs to be coded as a cardiac trauma. The trauma caused the transaction. If the transaction was caused by pathological reasons, you would code under aortic aneurysm.
2440 Other Card-Card Tx Indicate whether the patient had a Heterotropic or Orthotropic heart transplantation either in conjunction with or as the primary surgical procedure.
2450 Other Card-Arrhythmia Correction Surgery
Indicate if one of the following arrhythmia correction devices was surgically placed either in conjunction with or as the primary surgical procedure: -None -Permanent Pacemaker: an internal electronic generator that controls the heart rate. -Permanent Pacemaker with Cardiac Resynchronization Therapy (CRT): an internal permanent pacemaker that uses biventricular electrical stimulation to synchronize ventricular contraction. -Automatic Implanted Cardioverter Defibrillator (AICD): an internal device that defibrillates the heart. -AICD with CRT: an internal AICD that uses biventricular electrical stimulation to synchronize ventricular contraction.
01/06 The surgeon placed epicardial leads for an ICD and CRT but no device during surgery. The device was placed later in the cath lab. How do I code this?
Because no device was implanted, it would be coded as a Other Cardiac Other
Indicate which lead placement was used for the permanent pacemaker with CRT or AICD with CRT: Epicardial: the outer most layer of the heart. Endocardial: the inner most layer of the heart.
6/04
2460
Other Card-Arrhythmia Correction Surgery-Lead Placement
We just attended an in-service on the biventricular pacemakers and AICDs. We were informed that biventricular lead placement for AICD or Permanent Pacemaker with CRT (cardiac resynchronization therapy) could be epicardial in one ventricle, and endocardial in the other ventricle. In this case we would need to code an answer that allows us to choose both 1-epicardial and 2-endocardial. Per the data specifications, it does not look like we are allowed to choose both. Please clarify.
Most CRT BiV devices are implanted endocardially, with one lead in the endocardial RV and the second lead endocardially in the coronary sinus ("LV lead"). Some patients receive an epicardial LV lead via a thoracoscope or mini-thoracotomy approach. If the LV lead is placed in the coronary sinus, then both leads are endocardial. If the LV lead is placed on the epicardium via this thoracoscopic/thoracotomy approach, then it should be coded as an epicardial lead. In both cases, the RV lead is endocardial. If in a particular case, both epicardial and endocardial leads are placed, please code seq# 2460 as “epicardial”. The option of choosing “both” will be considered in the next specification upgrade.
2470 Other Card-Atrial Fibrillation Correction Surgery
Indicate if one of the following atrial fibrillation correction surgeries was performed either in conjunction with or as the primary surgical procedure. The intent of both surgeries is to preclude the atria from fibrillating by disrupting the abnormal reentry pathways of electronic signals that lead to atrial fibrillation. Standard Surgical Maze Procedure: Surgical procedure in which full thickness incisions are made in the atria of the heart. Sutures are then used to reapproximate the incised tissue. The resulting lesion disrupts the abnormal reentry pathways of electronic signals that lead to atrial fibrillation. Other Surgical Ablative Procedure: Surgical procedure in which lesions are
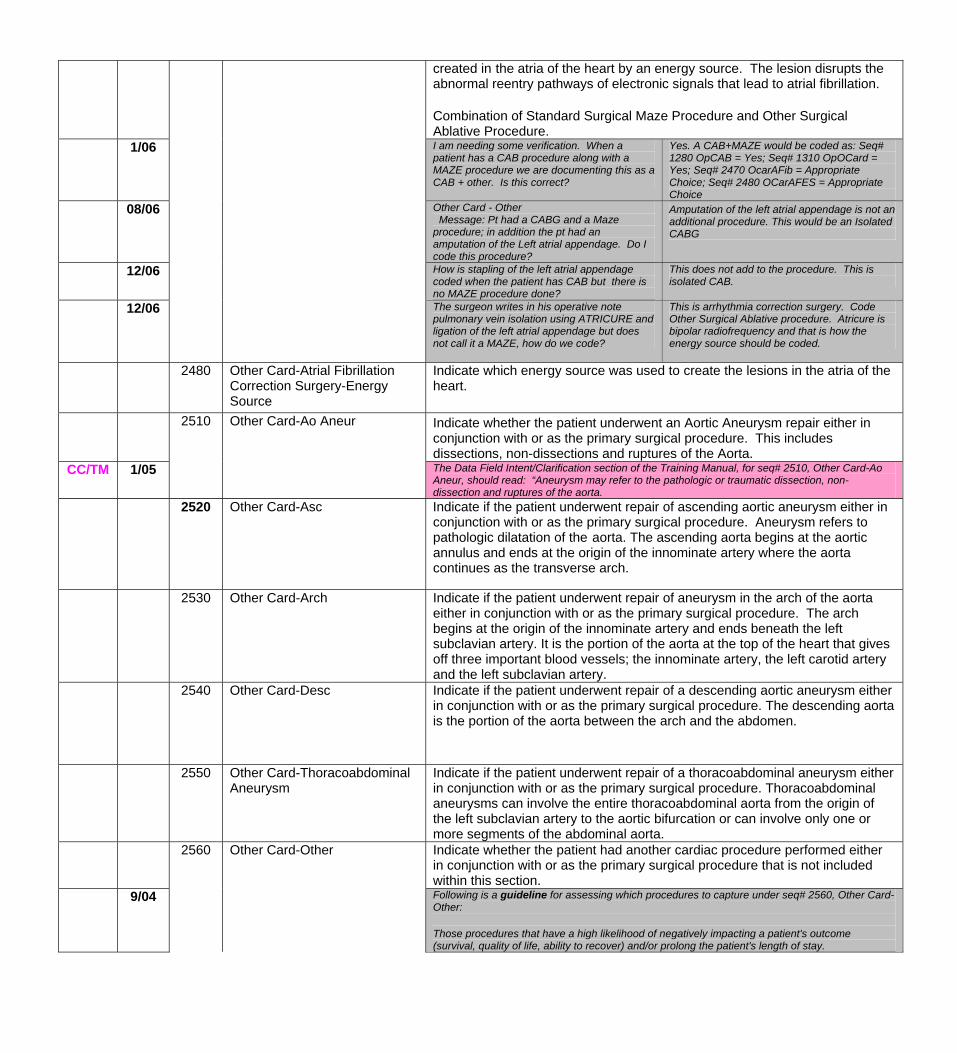
created in the atria of the heart by an energy source. The lesion disrupts the abnormal reentry pathways of electronic signals that lead to atrial fibrillation. Combination of Standard Surgical Maze Procedure and Other Surgical Ablative Procedure.
1/06 I am needing some verification. When a patient has a CAB procedure along with a MAZE procedure we are documenting this as a CAB + other. Is this correct?
Yes. A CAB+MAZE would be coded as: Seq# 1280 OpCAB = Yes; Seq# 1310 OpOCard = Yes; Seq# 2470 OcarAFib = Appropriate Choice; Seq# 2480 OCarAFES = Appropriate Choice
08/06
Other Card - Other Message: Pt had a CABG and a Maze procedure; in addition the pt had an amputation of the Left atrial appendage. Do I code this procedure?
Amputation of the left atrial appendage is not an additional procedure. This would be an Isolated CABG
12/06 How is stapling of the left atrial appendage coded when the patient has CAB but there is no MAZE procedure done?
This does not add to the procedure. This is isolated CAB.
12/06 The surgeon writes in his operative note pulmonary vein isolation using ATRICURE and ligation of the left atrial appendage but does not call it a MAZE, how do we code?
This is arrhythmia correction surgery. Code Other Surgical Ablative procedure. Atricure is bipolar radiofrequency and that is how the energy source should be coded.
2480 Other Card-Atrial Fibrillation Correction Surgery-Energy Source
Indicate which energy source was used to create the lesions in the atria of the heart.
Indicate whether the patient underwent an Aortic Aneurysm repair either in conjunction with or as the primary surgical procedure. This includes dissections, non-dissections and ruptures of the Aorta.
CC/TM 1/05
2510
Other Card-Ao Aneur
The Data Field Intent/Clarification section of the Training Manual, for seq# 2510, Other Card-Ao Aneur, should read: “Aneurysm may refer to the pathologic or traumatic dissection, non-dissection and ruptures of the aorta.
2520 Other Card-Asc Indicate if the patient underwent repair of ascending aortic aneurysm either in conjunction with or as the primary surgical procedure. Aneurysm refers to pathologic dilatation of the aorta. The ascending aorta begins at the aortic annulus and ends at the origin of the innominate artery where the aorta continues as the transverse arch.
2530
Other Card-Arch
Indicate if the patient underwent repair of aneurysm in the arch of the aorta either in conjunction with or as the primary surgical procedure. The arch begins at the origin of the innominate artery and ends beneath the left subclavian artery. It is the portion of the aorta at the top of the heart that gives off three important blood vessels; the innominate artery, the left carotid artery and the left subclavian artery.
2540 Other Card-Desc Indicate if the patient underwent repair of a descending aortic aneurysm either in conjunction with or as the primary surgical procedure. The descending aorta is the portion of the aorta between the arch and the abdomen.
2550 Other Card-Thoracoabdominal Aneurysm
Indicate if the patient underwent repair of a thoracoabdominal aneurysm either in conjunction with or as the primary surgical procedure. Thoracoabdominal aneurysms can involve the entire thoracoabdominal aorta from the origin of the left subclavian artery to the aortic bifurcation or can involve only one or more segments of the abdominal aorta.
2560 Other Card-Other Indicate whether the patient had another cardiac procedure performed either in conjunction with or as the primary surgical procedure that is not included within this section.
9/04 Following is a guideline for assessing which procedures to capture under seq# 2560, Other Card-Other: Those procedures that have a high likelihood of negatively impacting a patient's outcome (survival, quality of life, ability to recover) and/or prolong the patient's length of stay.
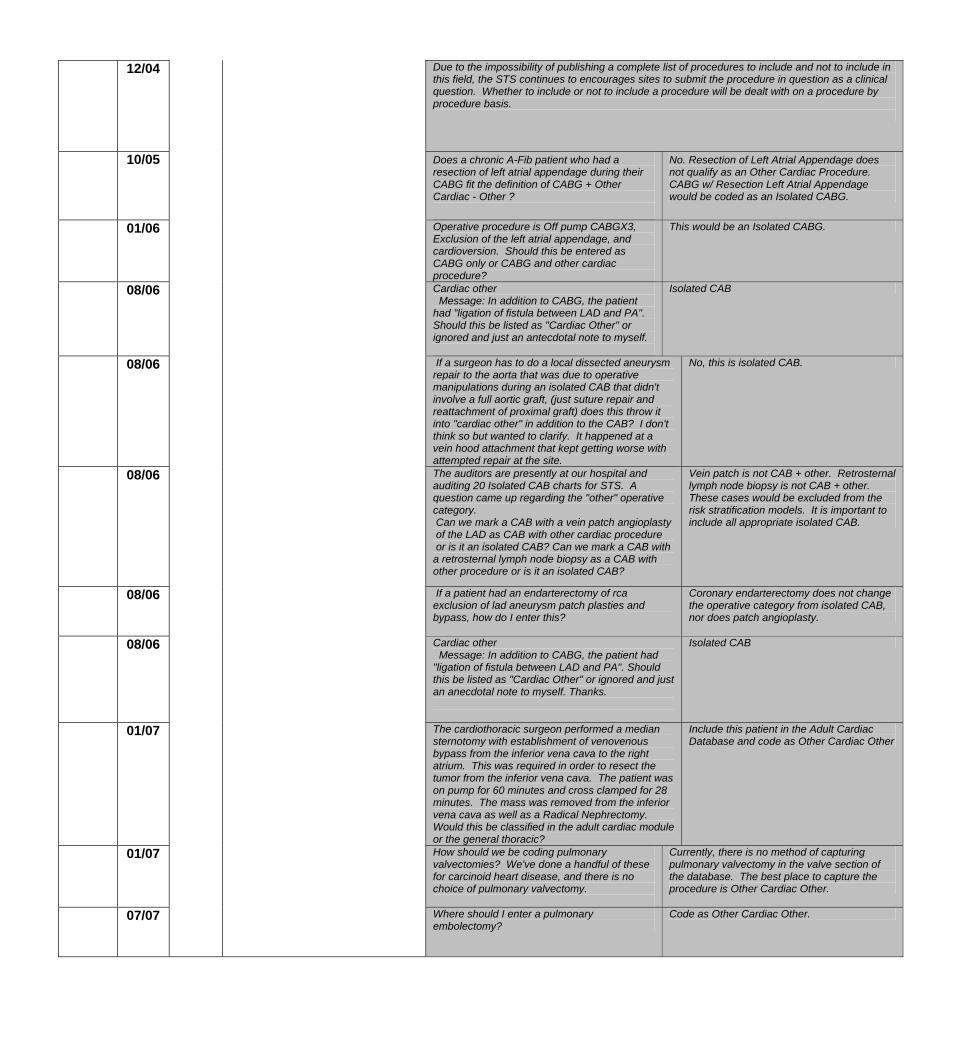
12/04 Due to the impossibility of publishing a complete list of procedures to include and not to include in this field, the STS continues to encourages sites to submit the procedure in question as a clinical question. Whether to include or not to include a procedure will be dealt with on a procedure by procedure basis.
10/05
Does a chronic A-Fib patient who had a resection of left atrial appendage during their CABG fit the definition of CABG + Other Cardiac - Other ?
No. Resection of Left Atrial Appendage does not qualify as an Other Cardiac Procedure. CABG w/ Resection Left Atrial Appendage would be coded as an Isolated CABG.
01/06 Operative procedure is Off pump CABGX3, Exclusion of the left atrial appendage, and cardioversion. Should this be entered as CABG only or CABG and other cardiac procedure?
This would be an Isolated CABG.
08/06 Cardiac other Message: In addition to CABG, the patient had "ligation of fistula between LAD and PA". Should this be listed as "Cardiac Other" or ignored and just an antecdotal note to myself.
Isolated CAB
08/06 If a surgeon has to do a local dissected aneurysm repair to the aorta that was due to operative manipulations during an isolated CAB that didn't involve a full aortic graft, (just suture repair and reattachment of proximal graft) does this throw it into "cardiac other" in addition to the CAB? I don't think so but wanted to clarify. It happened at a vein hood attachment that kept getting worse with attempted repair at the site.
No, this is isolated CAB.
08/06 The auditors are presently at our hospital and auditing 20 Isolated CAB charts for STS. A question came up regarding the "other" operative category. Can we mark a CAB with a vein patch angioplasty of the LAD as CAB with other cardiac procedure or is it an isolated CAB? Can we mark a CAB with a retrosternal lymph node biopsy as a CAB with other procedure or is it an isolated CAB?
Vein patch is not CAB + other. Retrosternal lymph node biopsy is not CAB + other. These cases would be excluded from the risk stratification models. It is important to include all appropriate isolated CAB.
08/06
If a patient had an endarterectomy of rca exclusion of lad aneurysm patch plasties and bypass, how do I enter this?
Coronary endarterectomy does not change the operative category from isolated CAB, nor does patch angioplasty.
08/06
Cardiac other Message: In addition to CABG, the patient had "ligation of fistula between LAD and PA". Should this be listed as "Cardiac Other" or ignored and just an anecdotal note to myself. Thanks.
Isolated CAB
01/07
The cardiothoracic surgeon performed a median sternotomy with establishment of venovenous bypass from the inferior vena cava to the right atrium. This was required in order to resect the tumor from the inferior vena cava. The patient was on pump for 60 minutes and cross clamped for 28 minutes. The mass was removed from the inferior vena cava as well as a Radical Nephrectomy. Would this be classified in the adult cardiac module or the general thoracic?
Include this patient in the Adult Cardiac Database and code as Other Cardiac Other
01/07 How should we be coding pulmonary valvectomies? We've done a handful of these for carcinoid heart disease, and there is no choice of pulmonary valvectomy.
Currently, there is no method of capturing pulmonary valvectomy in the valve section of the database. The best place to capture the procedure is Other Cardiac Other.
07/07 Where should I enter a pulmonary embolectomy?
Code as Other Cardiac Other.
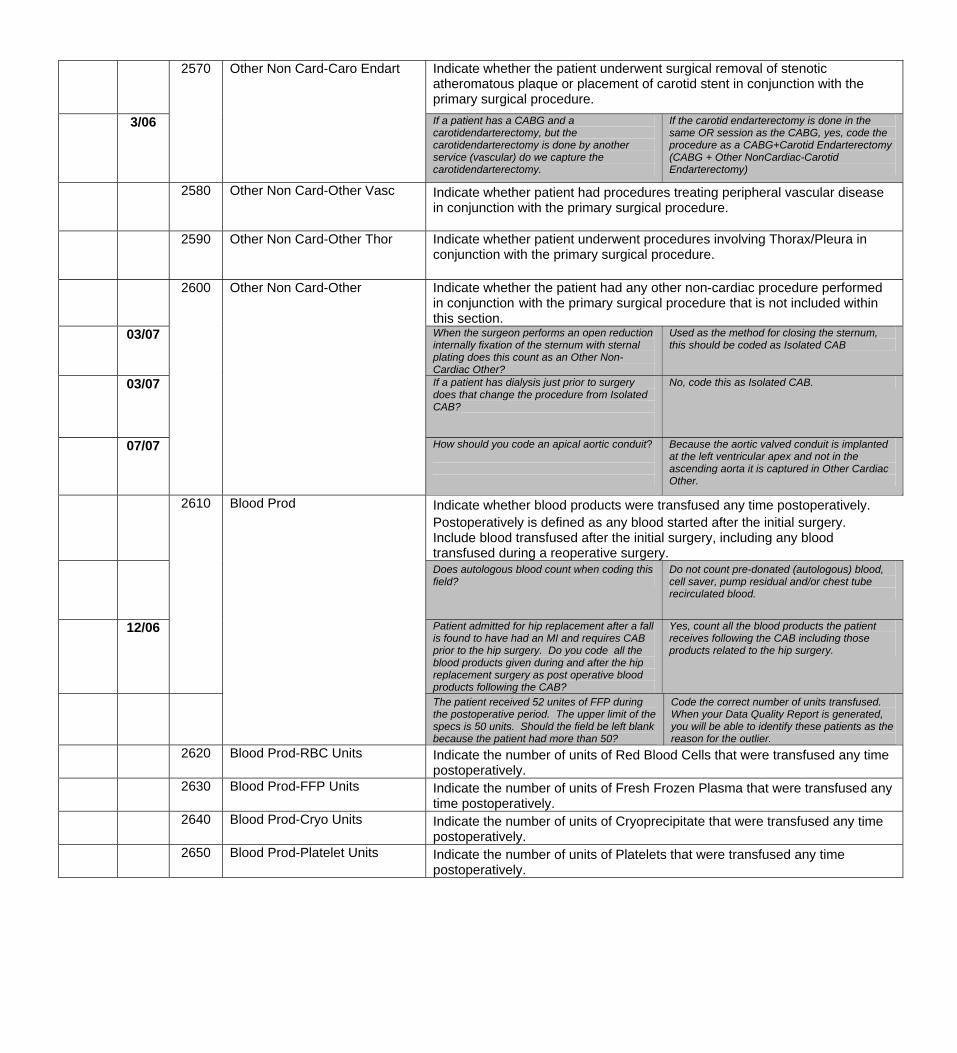
Indicate whether the patient underwent surgical removal of stenotic atheromatous plaque or placement of carotid stent in conjunction with the primary surgical procedure.
3/06
2570
Other Non Card-Caro Endart
If a patient has a CABG and a carotidendarterectomy, but the carotidendarterectomy is done by another service (vascular) do we capture the carotidendarterectomy.
If the carotid endarterectomy is done in the same OR session as the CABG, yes, code the procedure as a CABG+Carotid Endarterectomy (CABG + Other NonCardiac-Carotid Endarterectomy)
2580 Other Non Card-Other Vasc Indicate whether patient had procedures treating peripheral vascular disease in conjunction with the primary surgical procedure.
2590 Other Non Card-Other Thor Indicate whether patient underwent procedures involving Thorax/Pleura in conjunction with the primary surgical procedure.
2600 Other Non Card-Other Indicate whether the patient had any other non-cardiac procedure performed in conjunction with the primary surgical procedure that is not included within this section.
03/07 When the surgeon performs an open reduction internally fixation of the sternum with sternal plating does this count as an Other Non-Cardiac Other?
Used as the method for closing the sternum, this should be coded as Isolated CAB
03/07 If a patient has dialysis just prior to surgery does that change the procedure from Isolated CAB?
No, code this as Isolated CAB.
07/07 How should you code an apical aortic conduit?
Because the aortic valved conduit is implanted at the left ventricular apex and not in the ascending aorta it is captured in Other Cardiac Other.
2610 Blood Prod Indicate whether blood products were transfused any time postoperatively. Postoperatively is defined as any blood started after the initial surgery. Include blood transfused after the initial surgery, including any blood transfused during a reoperative surgery.
Does autologous blood count when coding this field?
Do not count pre-donated (autologous) blood, cell saver, pump residual and/or chest tube recirculated blood.
12/06 Patient admitted for hip replacement after a fall is found to have had an MI and requires CAB prior to the hip surgery. Do you code all the blood products given during and after the hip replacement surgery as post operative blood products following the CAB?
Yes, count all the blood products the patient receives following the CAB including those products related to the hip surgery.
The patient received 52 unites of FFP during the postoperative period. The upper limit of the specs is 50 units. Should the field be left blank because the patient had more than 50?
Code the correct number of units transfused. When your Data Quality Report is generated, you will be able to identify these patients as the reason for the outlier.
2620 Blood Prod-RBC Units Indicate the number of units of Red Blood Cells that were transfused any time postoperatively.
2630 Blood Prod-FFP Units Indicate the number of units of Fresh Frozen Plasma that were transfused any time postoperatively.
2640
Blood Prod-Cryo Units
Indicate the number of units of Cryoprecipitate that were transfused any time postoperatively.
2650 Blood Prod-Platelet Units Indicate the number of units of Platelets that were transfused any time postoperatively.
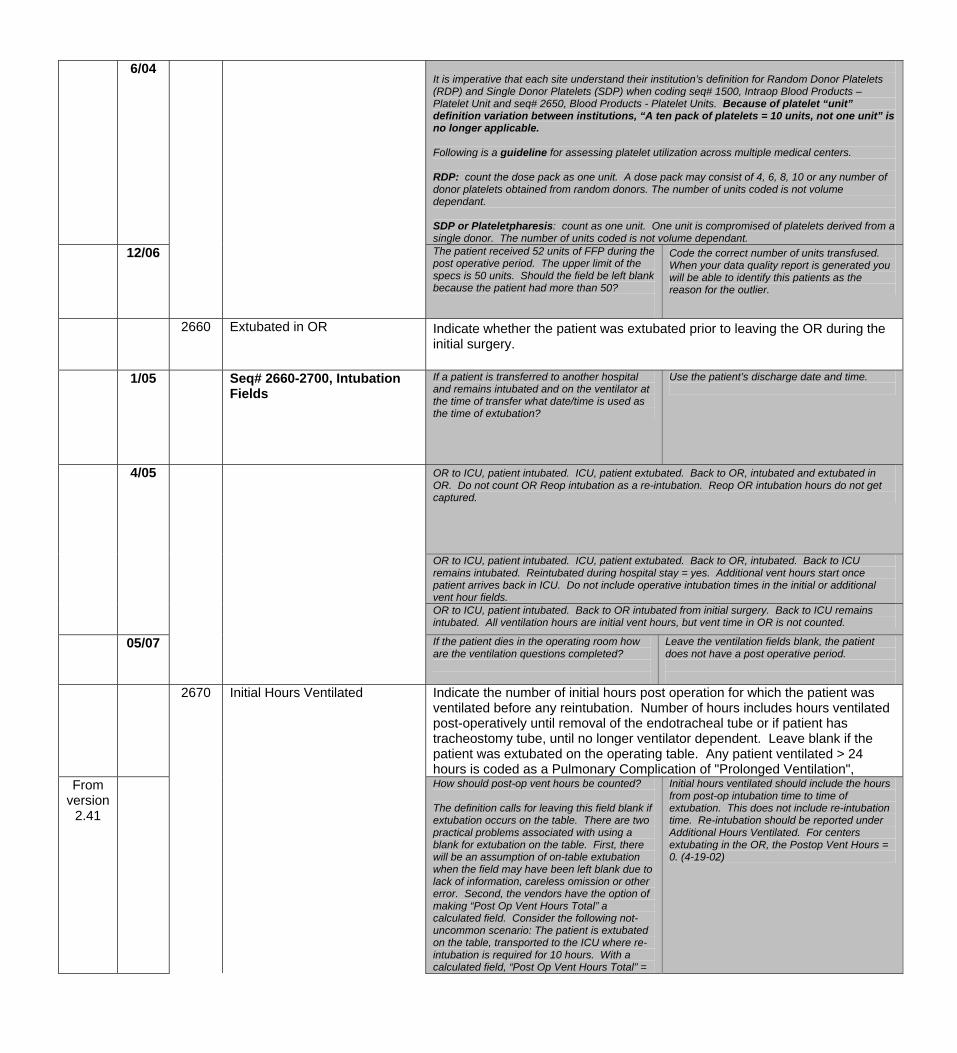
6/04 It is imperative that each site understand their institution’s definition for Random Donor Platelets (RDP) and Single Donor Platelets (SDP) when coding seq# 1500, Intraop Blood Products – Platelet Unit and seq# 2650, Blood Products - Platelet Units. Because of platelet “unit” definition variation between institutions, “A ten pack of platelets = 10 units, not one unit” is no longer applicable. Following is a guideline for assessing platelet utilization across multiple medical centers. RDP: count the dose pack as one unit. A dose pack may consist of 4, 6, 8, 10 or any number of donor platelets obtained from random donors. The number of units coded is not volume dependant. SDP or Plateletpharesis: count as one unit. One unit is compromised of platelets derived from a single donor. The number of units coded is not volume dependant.
12/06 The patient received 52 units of FFP during the post operative period. The upper limit of the specs is 50 units. Should the field be left blank because the patient had more than 50?
Code the correct number of units transfused. When your data quality report is generated you will be able to identify this patients as the reason for the outlier.
2660 Extubated in OR Indicate whether the patient was extubated prior to leaving the OR during the initial surgery.
1/05 Seq# 2660-2700, Intubation Fields
If a patient is transferred to another hospital and remains intubated and on the ventilator at the time of transfer what date/time is used as the time of extubation?
Use the patient’s discharge date and time.
4/05 OR to ICU, patient intubated. ICU, patient extubated. Back to OR, intubated and extubated in OR. Do not count OR Reop intubation as a re-intubation. Reop OR intubation hours do not get captured.
OR to ICU, patient intubated. ICU, patient extubated. Back to OR, intubated. Back to ICU remains intubated. Reintubated during hospital stay = yes. Additional vent hours start once patient arrives back in ICU. Do not include operative intubation times in the initial or additional vent hour fields.
OR to ICU, patient intubated. Back to OR intubated from initial surgery. Back to ICU remains intubated. All ventilation hours are initial vent hours, but vent time in OR is not counted.
05/07 If the patient dies in the operating room how are the ventilation questions completed?
Leave the ventilation fields blank, the patient does not have a post operative period.
2670
Initial Hours Ventilated
Indicate the number of initial hours post operation for which the patient was ventilated before any reintubation. Number of hours includes hours ventilated post-operatively until removal of the endotracheal tube or if patient has tracheostomy tube, until no longer ventilator dependent. Leave blank if the patient was extubated on the operating table. Any patient ventilated > 24 hours is coded as a Pulmonary Complication of "Prolonged Ventilation",
From version
2.41
How should post-op vent hours be counted? The definition calls for leaving this field blank if extubation occurs on the table. There are two practical problems associated with using a blank for extubation on the table. First, there will be an assumption of on-table extubation when the field may have been left blank due to lack of information, careless omission or other error. Second, the vendors have the option of making “Post Op Vent Hours Total” a calculated field. Consider the following not-uncommon scenario: The patient is extubated on the table, transported to the ICU where re-intubation is required for 10 hours. With a calculated field, “Post Op Vent Hours Total” =
Initial hours ventilated should include the hours from post-op intubation time to time of extubation. This does not include re-intubation time. Re-intubation should be reported under Additional Hours Ventilated. For centers extubating in the OR, the Postop Vent Hours = 0. (4-19-02)
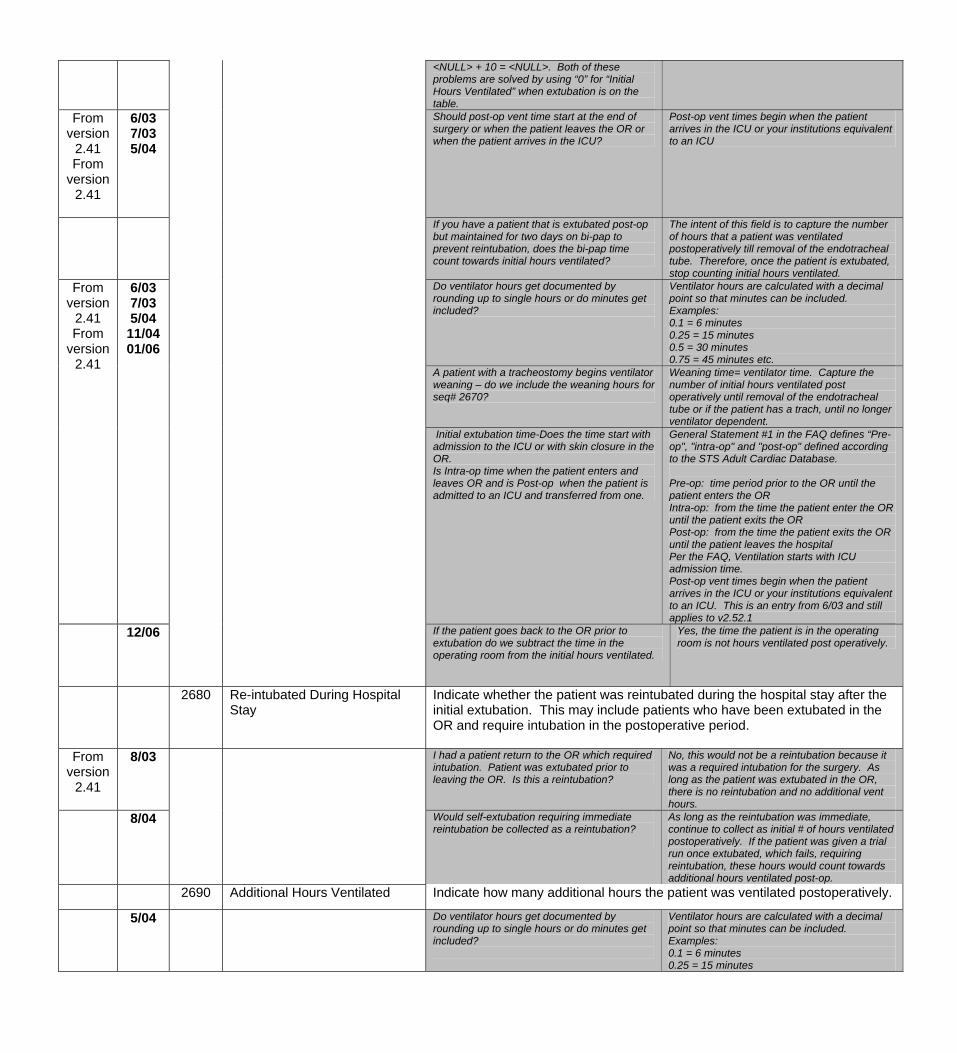
<NULL> + 10 = <NULL>. Both of these problems are solved by using “0” for “Initial Hours Ventilated” when extubation is on the table.
From version
2.41 From
version 2.41
6/03 7/03 5/04
Should post-op vent time start at the end of surgery or when the patient leaves the OR or when the patient arrives in the ICU?
Post-op vent times begin when the patient arrives in the ICU or your institutions equivalent to an ICU
If you have a patient that is extubated post-op but maintained for two days on bi-pap to prevent reintubation, does the bi-pap time count towards initial hours ventilated?
The intent of this field is to capture the number of hours that a patient was ventilated postoperatively till removal of the endotracheal tube. Therefore, once the patient is extubated, stop counting initial hours ventilated.
Do ventilator hours get documented by rounding up to single hours or do minutes get included?
Ventilator hours are calculated with a decimal point so that minutes can be included. Examples: 0.1 = 6 minutes 0.25 = 15 minutes 0.5 = 30 minutes 0.75 = 45 minutes etc.
A patient with a tracheostomy begins ventilator weaning – do we include the weaning hours for seq# 2670?
Weaning time= ventilator time. Capture the number of initial hours ventilated post operatively until removal of the endotracheal tube or if the patient has a trach, until no longer ventilator dependent.
From version
2.41 From
version 2.41
6/03 7/03 5/04
11/04 01/06
Initial extubation time-Does the time start with admission to the ICU or with skin closure in the OR. Is Intra-op time when the patient enters and leaves OR and is Post-op when the patient is admitted to an ICU and transferred from one.
General Statement #1 in the FAQ defines “Pre-op", "intra-op" and "post-op" defined according to the STS Adult Cardiac Database. Pre-op: time period prior to the OR until the patient enters the OR Intra-op: from the time the patient enter the OR until the patient exits the OR Post-op: from the time the patient exits the OR until the patient leaves the hospital Per the FAQ, Ventilation starts with ICU admission time. Post-op vent times begin when the patient arrives in the ICU or your institutions equivalent to an ICU. This is an entry from 6/03 and still applies to v2.52.1
12/06 If the patient goes back to the OR prior to extubation do we subtract the time in the operating room from the initial hours ventilated.
Yes, the time the patient is in the operating room is not hours ventilated post operatively.
2680
Re-intubated During Hospital Stay
Indicate whether the patient was reintubated during the hospital stay after the initial extubation. This may include patients who have been extubated in the OR and require intubation in the postoperative period.
From version
2.41
8/03 I had a patient return to the OR which required intubation. Patient was extubated prior to leaving the OR. Is this a reintubation?
No, this would not be a reintubation because it was a required intubation for the surgery. As long as the patient was extubated in the OR, there is no reintubation and no additional vent hours.
8/04
Would self-extubation requiring immediate reintubation be collected as a reintubation?
As long as the reintubation was immediate, continue to collect as initial # of hours ventilated postoperatively. If the patient was given a trial run once extubated, which fails, requiring reintubation, these hours would count towards additional hours ventilated post-op.
2690 Additional Hours Ventilated Indicate how many additional hours the patient was ventilated postoperatively.
5/04 Do ventilator hours get documented by rounding up to single hours or do minutes get included?
Ventilator hours are calculated with a decimal point so that minutes can be included. Examples: 0.1 = 6 minutes 0.25 = 15 minutes
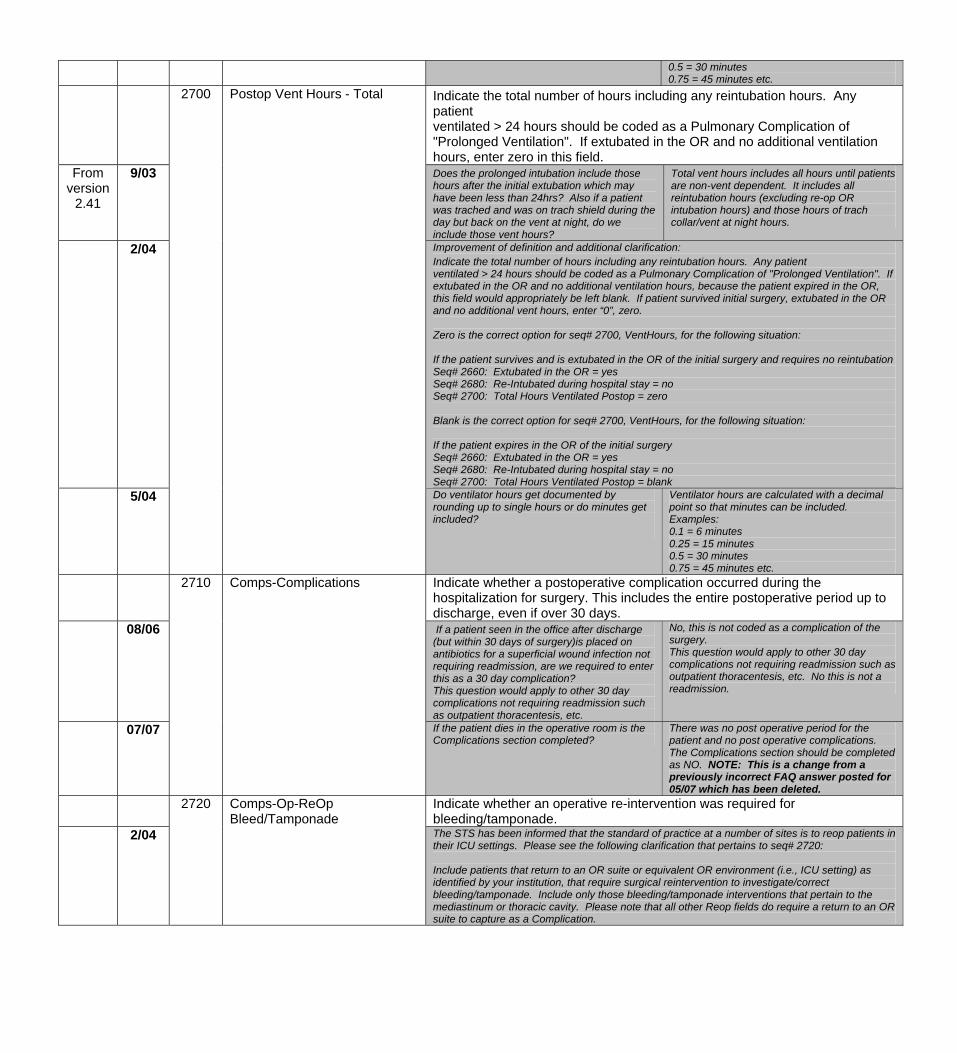
0.5 = 30 minutes 0.75 = 45 minutes etc.
Indicate the total number of hours including any reintubation hours. Any patient ventilated > 24 hours should be coded as a Pulmonary Complication of "Prolonged Ventilation". If extubated in the OR and no additional ventilation hours, enter zero in this field.
From version
2.41
9/03
2700 Postop Vent Hours - Total
Does the prolonged intubation include those hours after the initial extubation which may have been less than 24hrs? Also if a patient was trached and was on trach shield during the day but back on the vent at night, do we include those vent hours?
Total vent hours includes all hours until patients are non-vent dependent. It includes all reintubation hours (excluding re-op OR intubation hours) and those hours of trach collar/vent at night hours.
2/04 Improvement of definition and additional clarification: Indicate the total number of hours including any reintubation hours. Any patient ventilated > 24 hours should be coded as a Pulmonary Complication of "Prolonged Ventilation". If extubated in the OR and no additional ventilation hours, because the patient expired in the OR, this field would appropriately be left blank. If patient survived initial surgery, extubated in the OR and no additional vent hours, enter “0”, zero. Zero is the correct option for seq# 2700, VentHours, for the following situation: If the patient survives and is extubated in the OR of the initial surgery and requires no reintubation Seq# 2660: Extubated in the OR = yes Seq# 2680: Re-Intubated during hospital stay = no Seq# 2700: Total Hours Ventilated Postop = zero Blank is the correct option for seq# 2700, VentHours, for the following situation: If the patient expires in the OR of the initial surgery Seq# 2660: Extubated in the OR = yes Seq# 2680: Re-Intubated during hospital stay = no Seq# 2700: Total Hours Ventilated Postop = blank
5/04 Do ventilator hours get documented by rounding up to single hours or do minutes get included?
Ventilator hours are calculated with a decimal point so that minutes can be included. Examples: 0.1 = 6 minutes 0.25 = 15 minutes 0.5 = 30 minutes 0.75 = 45 minutes etc.
Indicate whether a postoperative complication occurred during the hospitalization for surgery. This includes the entire postoperative period up to discharge, even if over 30 days.
08/06
2710 Comps-Complications
If a patient seen in the office after discharge (but within 30 days of surgery)is placed on antibiotics for a superficial wound infection not requiring readmission, are we required to enter this as a 30 day complication? This question would apply to other 30 day complications not requiring readmission such as outpatient thoracentesis, etc.
No, this is not coded as a complication of the surgery. This question would apply to other 30 day complications not requiring readmission such as outpatient thoracentesis, etc. No this is not a readmission.
07/07
If the patient dies in the operative room is the Complications section completed?
There was no post operative period for the patient and no post operative complications. The Complications section should be completed as NO. NOTE: This is a change from a previously incorrect FAQ answer posted for 05/07 which has been deleted.
2720 Comps-Op-ReOp Bleed/Tamponade
Indicate whether an operative re-intervention was required for bleeding/tamponade.
2/04 The STS has been informed that the standard of practice at a number of sites is to reop patients in their ICU settings. Please see the following clarification that pertains to seq# 2720: Include patients that return to an OR suite or equivalent OR environment (i.e., ICU setting) as identified by your institution, that require surgical reintervention to investigate/correct bleeding/tamponade. Include only those bleeding/tamponade interventions that pertain to the mediastinum or thoracic cavity. Please note that all other Reop fields do require a return to an OR suite to capture as a Complication.
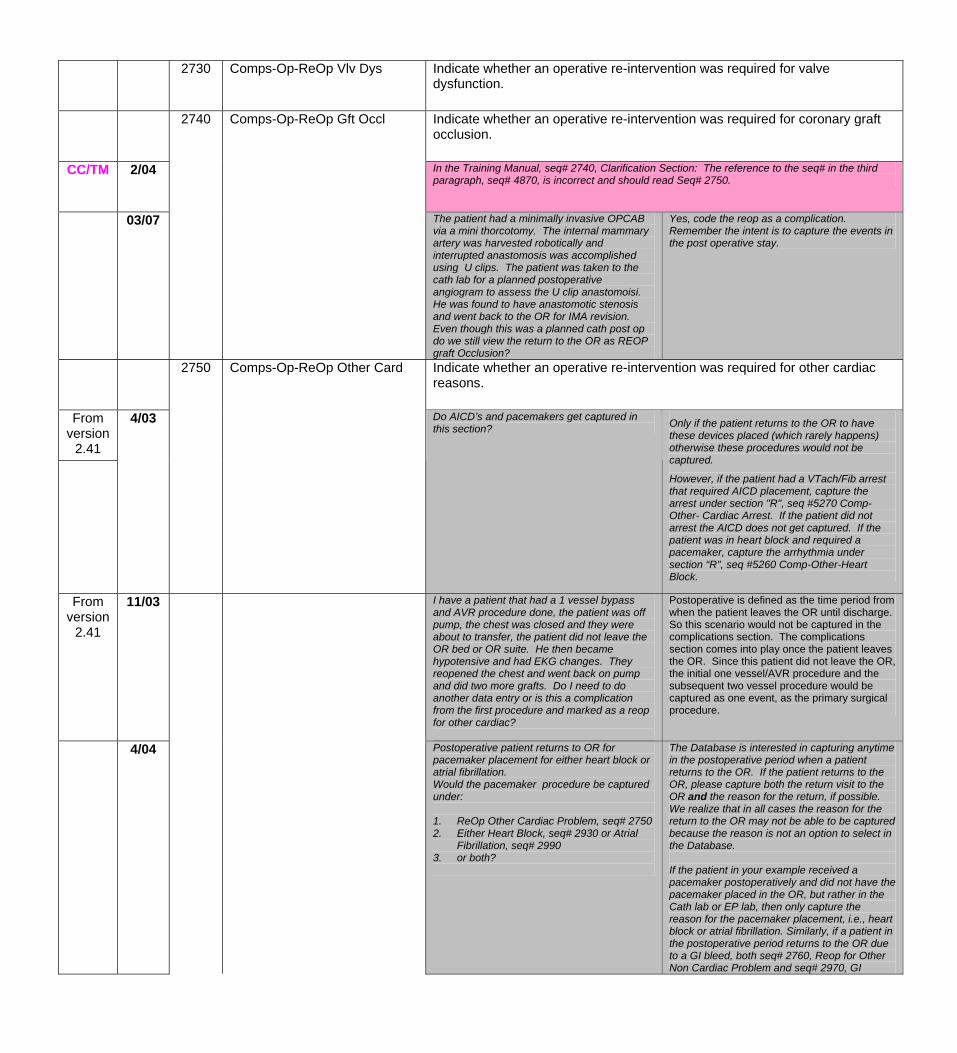
2730 Comps-Op-ReOp Vlv Dys Indicate whether an operative re-intervention was required for valve dysfunction.
2740 Comps-Op-ReOp Gft Occl Indicate whether an operative re-intervention was required for coronary graft occlusion.
CC/TM 2/04
In the Training Manual, seq# 2740, Clarification Section: The reference to the seq# in the third paragraph, seq# 4870, is incorrect and should read Seq# 2750.
03/07
The patient had a minimally invasive OPCAB via a mini thorcotomy. The internal mammary artery was harvested robotically and interrupted anastomosis was accomplished using U clips. The patient was taken to the cath lab for a planned postoperative angiogram to assess the U clip anastomoisi. He was found to have anastomotic stenosis and went back to the OR for IMA revision. Even though this was a planned cath post op do we still view the return to the OR as REOP graft Occlusion?
Yes, code the reop as a complication. Remember the intent is to capture the events in the post operative stay.
2750 Comps-Op-ReOp Other Card Indicate whether an operative re-intervention was required for other cardiac reasons.
From version
2.41
4/03 Do AICD’s and pacemakers get captured in this section? Only if the patient returns to the OR to have
these devices placed (which rarely happens) otherwise these procedures would not be captured.
However, if the patient had a VTach/Fib arrest that required AICD placement, capture the arrest under section "R", seq #5270 Comp-Other- Cardiac Arrest. If the patient did not arrest the AICD does not get captured. If the patient was in heart block and required a pacemaker, capture the arrhythmia under section “R”, seq #5260 Comp-Other-Heart Block.
From version
2.41
11/03 I have a patient that had a 1 vessel bypass and AVR procedure done, the patient was off pump, the chest was closed and they were about to transfer, the patient did not leave the OR bed or OR suite. He then became hypotensive and had EKG changes. They reopened the chest and went back on pump and did two more grafts. Do I need to do another data entry or is this a complication from the first procedure and marked as a reop for other cardiac?
Postoperative is defined as the time period from when the patient leaves the OR until discharge. So this scenario would not be captured in the complications section. The complications section comes into play once the patient leaves the OR. Since this patient did not leave the OR, the initial one vessel/AVR procedure and the subsequent two vessel procedure would be captured as one event, as the primary surgical procedure.
4/04
Postoperative patient returns to OR for pacemaker placement for either heart block or atrial fibrillation. Would the pacemaker procedure be captured under: 1. ReOp Other Cardiac Problem, seq# 2750 2. Either Heart Block, seq# 2930 or Atrial
Fibrillation, seq# 2990 3. or both?
The Database is interested in capturing anytime in the postoperative period when a patient returns to the OR. If the patient returns to the OR, please capture both the return visit to the OR and the reason for the return, if possible. We realize that in all cases the reason for the return to the OR may not be able to be captured because the reason is not an option to select in the Database. If the patient in your example received a pacemaker postoperatively and did not have the pacemaker placed in the OR, but rather in the Cath lab or EP lab, then only capture the reason for the pacemaker placement, i.e., heart block or atrial fibrillation. Similarly, if a patient in the postoperative period returns to the OR due to a GI bleed, both seq# 2760, Reop for Other Non Cardiac Problem and seq# 2970, GI
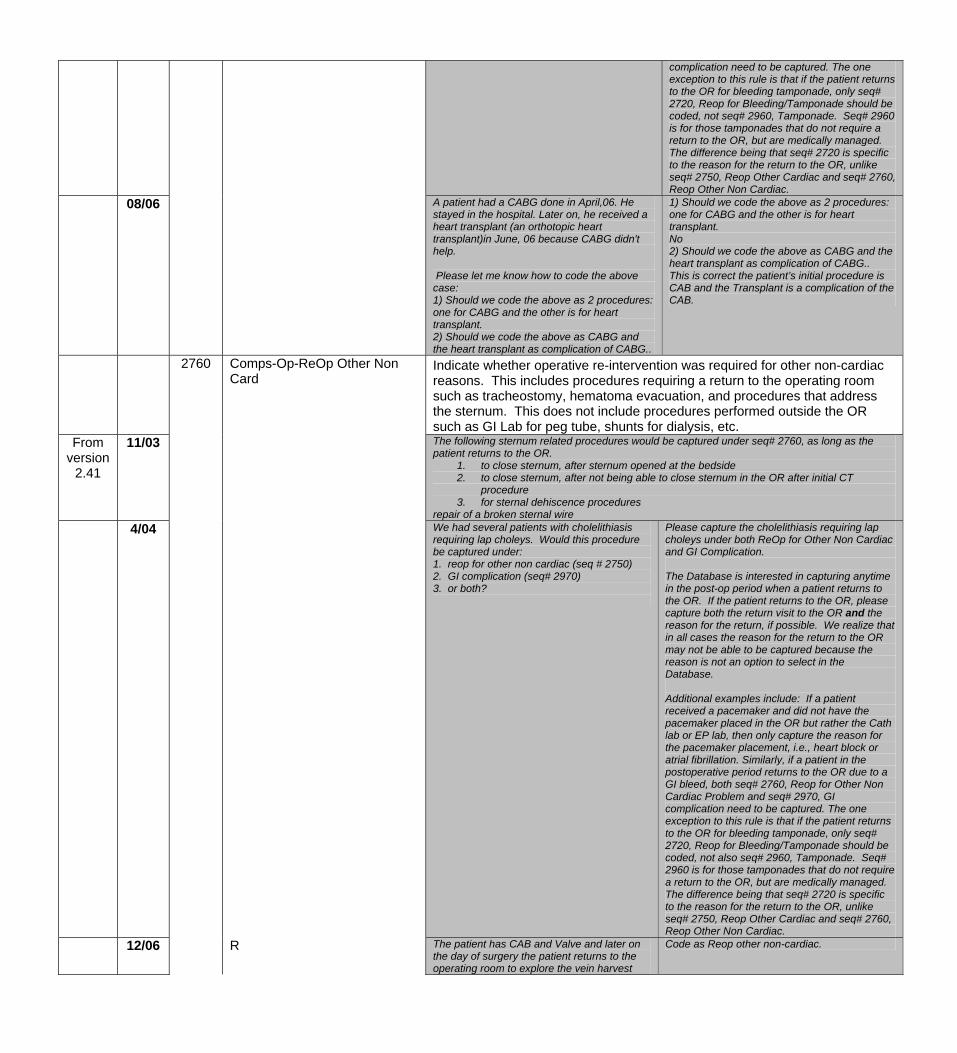
complication need to be captured. The one exception to this rule is that if the patient returns to the OR for bleeding tamponade, only seq# 2720, Reop for Bleeding/Tamponade should be coded, not seq# 2960, Tamponade. Seq# 2960 is for those tamponades that do not require a return to the OR, but are medically managed. The difference being that seq# 2720 is specific to the reason for the return to the OR, unlike seq# 2750, Reop Other Cardiac and seq# 2760, Reop Other Non Cardiac.
08/06 A patient had a CABG done in April,06. He stayed in the hospital. Later on, he received a heart transplant (an orthotopic heart transplant)in June, 06 because CABG didn't help. Please let me know how to code the above case: 1) Should we code the above as 2 procedures: one for CABG and the other is for heart transplant. 2) Should we code the above as CABG and the heart transplant as complication of CABG..
1) Should we code the above as 2 procedures: one for CABG and the other is for heart transplant. No 2) Should we code the above as CABG and the heart transplant as complication of CABG.. This is correct the patient’s initial procedure is CAB and the Transplant is a complication of the CAB.
Indicate whether operative re-intervention was required for other non-cardiac reasons. This includes procedures requiring a return to the operating room such as tracheostomy, hematoma evacuation, and procedures that address the sternum. This does not include procedures performed outside the OR such as GI Lab for peg tube, shunts for dialysis, etc.
From version
2.41
11/03
2760
Comps-Op-ReOp Other Non Card
The following sternum related procedures would be captured under seq# 2760, as long as the patient returns to the OR.
1. to close sternum, after sternum opened at the bedside 2. to close sternum, after not being able to close sternum in the OR after initial CT
procedure 3. for sternal dehiscence procedures
repair of a broken sternal wire 4/04 We had several patients with cholelithiasis
requiring lap choleys. Would this procedure be captured under: 1. reop for other non cardiac (seq # 2750) 2. GI complication (seq# 2970) 3. or both?
Please capture the cholelithiasis requiring lap choleys under both ReOp for Other Non Cardiac and GI Complication. The Database is interested in capturing anytime in the post-op period when a patient returns to the OR. If the patient returns to the OR, please capture both the return visit to the OR and the reason for the return, if possible. We realize that in all cases the reason for the return to the OR may not be able to be captured because the reason is not an option to select in the Database. Additional examples include: If a patient received a pacemaker and did not have the pacemaker placed in the OR but rather the Cath lab or EP lab, then only capture the reason for the pacemaker placement, i.e., heart block or atrial fibrillation. Similarly, if a patient in the postoperative period returns to the OR due to a GI bleed, both seq# 2760, Reop for Other Non Cardiac Problem and seq# 2970, GI complication need to be captured. The one exception to this rule is that if the patient returns to the OR for bleeding tamponade, only seq# 2720, Reop for Bleeding/Tamponade should be coded, not also seq# 2960, Tamponade. Seq# 2960 is for those tamponades that do not require a return to the OR, but are medically managed. The difference being that seq# 2720 is specific to the reason for the return to the OR, unlike seq# 2750, Reop Other Cardiac and seq# 2760, Reop Other Non Cardiac.
12/06 R The patient has CAB and Valve and later on the day of surgery the patient returns to the operating room to explore the vein harvest
Code as Reop other non-cardiac.
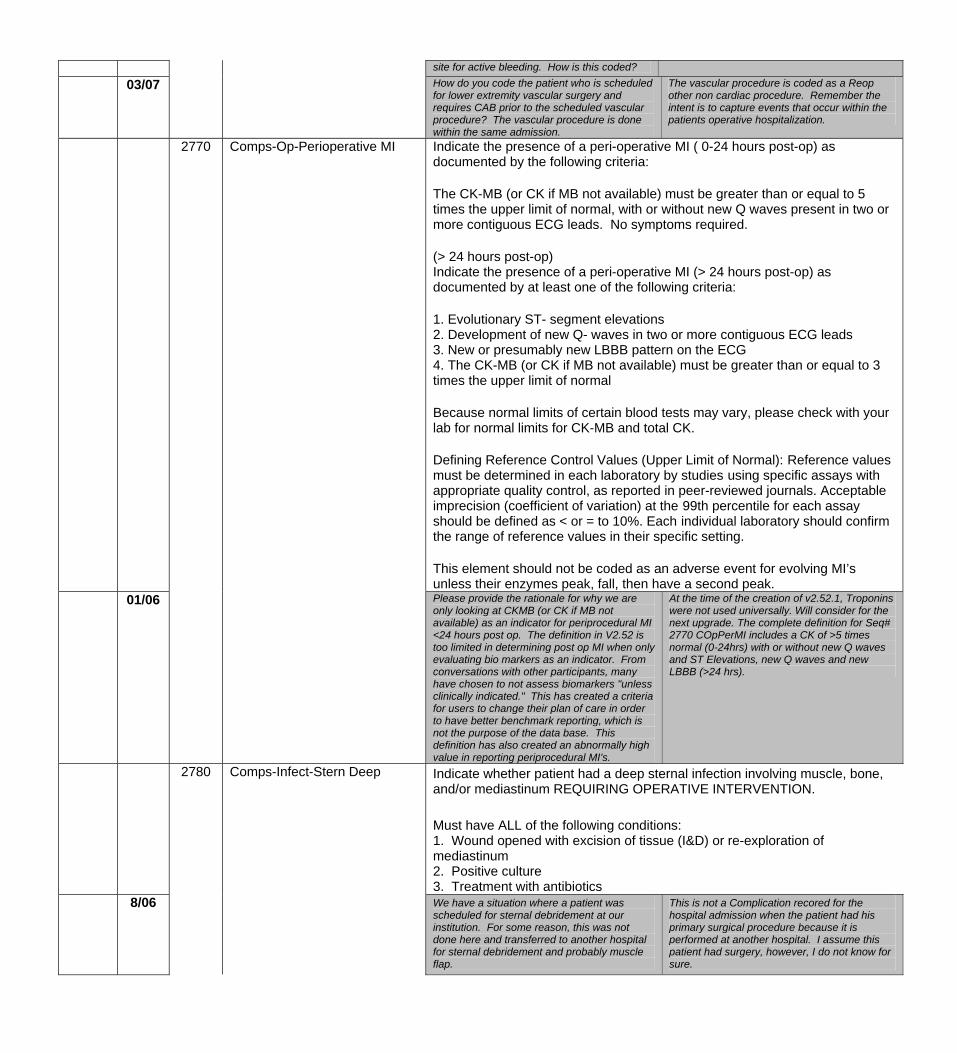
site for active bleeding. How is this coded?
03/07 How do you code the patient who is scheduled for lower extremity vascular surgery and requires CAB prior to the scheduled vascular procedure? The vascular procedure is done within the same admission.
The vascular procedure is coded as a Reop other non cardiac procedure. Remember the intent is to capture events that occur within the patients operative hospitalization.
Indicate the presence of a peri-operative MI ( 0-24 hours post-op) as documented by the following criteria: The CK-MB (or CK if MB not available) must be greater than or equal to 5 times the upper limit of normal, with or without new Q waves present in two or more contiguous ECG leads. No symptoms required. (> 24 hours post-op) Indicate the presence of a peri-operative MI (> 24 hours post-op) as documented by at least one of the following criteria: 1. Evolutionary ST- segment elevations 2. Development of new Q- waves in two or more contiguous ECG leads 3. New or presumably new LBBB pattern on the ECG 4. The CK-MB (or CK if MB not available) must be greater than or equal to 3 times the upper limit of normal Because normal limits of certain blood tests may vary, please check with your lab for normal limits for CK-MB and total CK. Defining Reference Control Values (Upper Limit of Normal): Reference values must be determined in each laboratory by studies using specific assays with appropriate quality control, as reported in peer-reviewed journals. Acceptable imprecision (coefficient of variation) at the 99th percentile for each assay should be defined as < or = to 10%. Each individual laboratory should confirm the range of reference values in their specific setting. This element should not be coded as an adverse event for evolving MI’s unless their enzymes peak, fall, then have a second peak.
01/06
2770 Comps-Op-Perioperative MI
Please provide the rationale for why we are only looking at CKMB (or CK if MB not available) as an indicator for periprocedural MI <24 hours post op. The definition in V2.52 is too limited in determining post op MI when only evaluating bio markers as an indicator. From conversations with other participants, many have chosen to not assess biomarkers "unless clinically indicated." This has created a criteria for users to change their plan of care in order to have better benchmark reporting, which is not the purpose of the data base. This definition has also created an abnormally high value in reporting periprocedural MI's.
At the time of the creation of v2.52.1, Troponins were not used universally. Will consider for the next upgrade. The complete definition for Seq# 2770 COpPerMI includes a CK of >5 times normal (0-24hrs) with or without new Q waves and ST Elevations, new Q waves and new LBBB (>24 hrs).
2780 Comps-Infect-Stern Deep Indicate whether patient had a deep sternal infection involving muscle, bone, and/or mediastinum REQUIRING OPERATIVE INTERVENTION. Must have ALL of the following conditions: 1. Wound opened with excision of tissue (I&D) or re-exploration of mediastinum 2. Positive culture 3. Treatment with antibiotics
8/06 We have a situation where a patient was scheduled for sternal debridement at our institution. For some reason, this was not done here and transferred to another hospital for sternal debridement and probably muscle flap.
This is not a Complication recored for the hospital admission when the patient had his primary surgical procedure because it is performed at another hospital. I assume this patient had surgery, however, I do not know for sure.
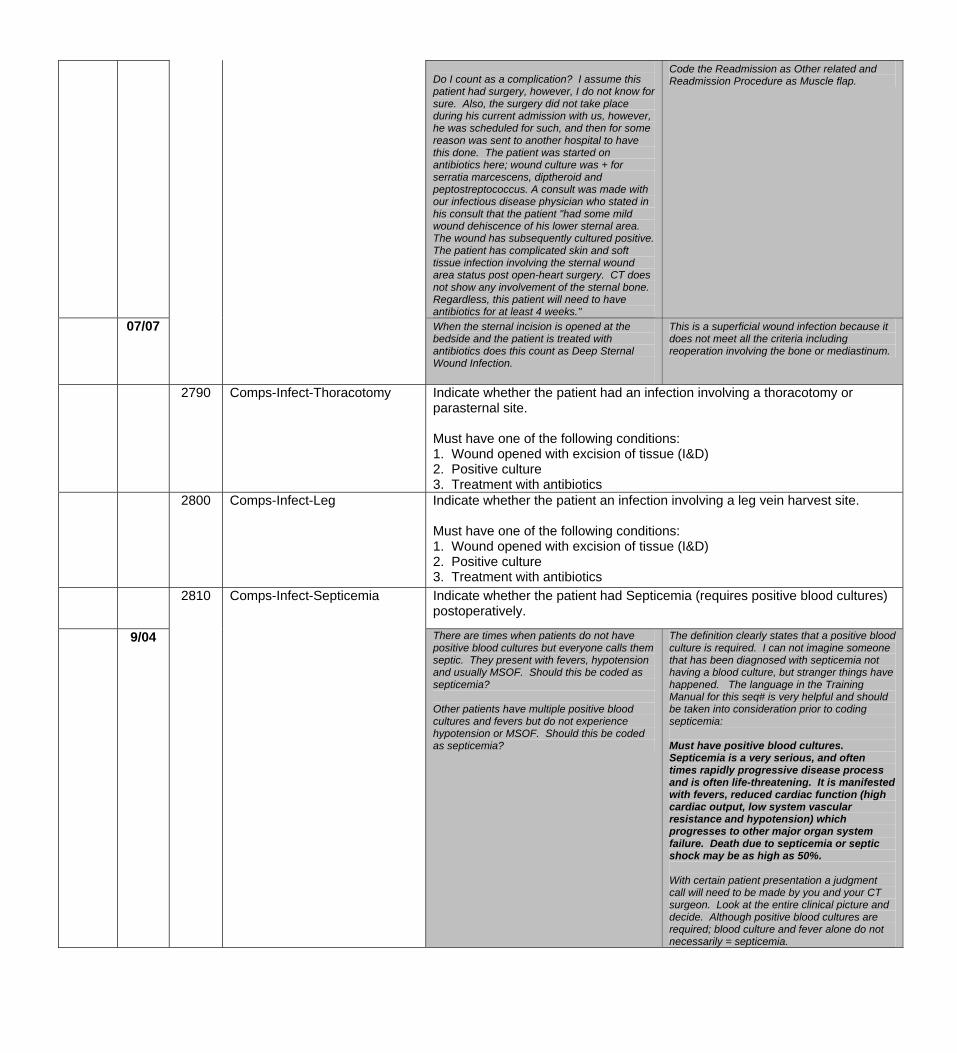
Do I count as a complication? I assume this patient had surgery, however, I do not know for sure. Also, the surgery did not take place during his current admission with us, however, he was scheduled for such, and then for some reason was sent to another hospital to have this done. The patient was started on antibiotics here; wound culture was + for serratia marcescens, diptheroid and peptostreptococcus. A consult was made with our infectious disease physician who stated in his consult that the patient "had some mild wound dehiscence of his lower sternal area. The wound has subsequently cultured positive. The patient has complicated skin and soft tissue infection involving the sternal wound area status post open-heart surgery. CT does not show any involvement of the sternal bone. Regardless, this patient will need to have antibiotics for at least 4 weeks."
Code the Readmission as Other related and Readmission Procedure as Muscle flap.
07/07 When the sternal incision is opened at the bedside and the patient is treated with antibiotics does this count as Deep Sternal Wound Infection.
This is a superficial wound infection because it does not meet all the criteria including reoperation involving the bone or mediastinum.
2790 Comps-Infect-Thoracotomy Indicate whether the patient had an infection involving a thoracotomy or parasternal site. Must have one of the following conditions: 1. Wound opened with excision of tissue (I&D) 2. Positive culture 3. Treatment with antibiotics
2800 Comps-Infect-Leg Indicate whether the patient an infection involving a leg vein harvest site. Must have one of the following conditions: 1. Wound opened with excision of tissue (I&D) 2. Positive culture 3. Treatment with antibiotics
2810 Comps-Infect-Septicemia Indicate whether the patient had Septicemia (requires positive blood cultures) postoperatively.
9/04 There are times when patients do not have positive blood cultures but everyone calls them septic. They present with fevers, hypotension and usually MSOF. Should this be coded as septicemia? Other patients have multiple positive blood cultures and fevers but do not experience hypotension or MSOF. Should this be coded as septicemia?
The definition clearly states that a positive blood culture is required. I can not imagine someone that has been diagnosed with septicemia not having a blood culture, but stranger things have happened. The language in the Training Manual for this seq# is very helpful and should be taken into consideration prior to coding septicemia: Must have positive blood cultures. Septicemia is a very serious, and often times rapidly progressive disease process and is often life-threatening. It is manifested with fevers, reduced cardiac function (high cardiac output, low system vascular resistance and hypotension) which progresses to other major organ system failure. Death due to septicemia or septic shock may be as high as 50%. With certain patient presentation a judgment call will need to be made by you and your CT surgeon. Look at the entire clinical picture and decide. Although positive blood cultures are required; blood culture and fever alone do not necessarily = septicemia.
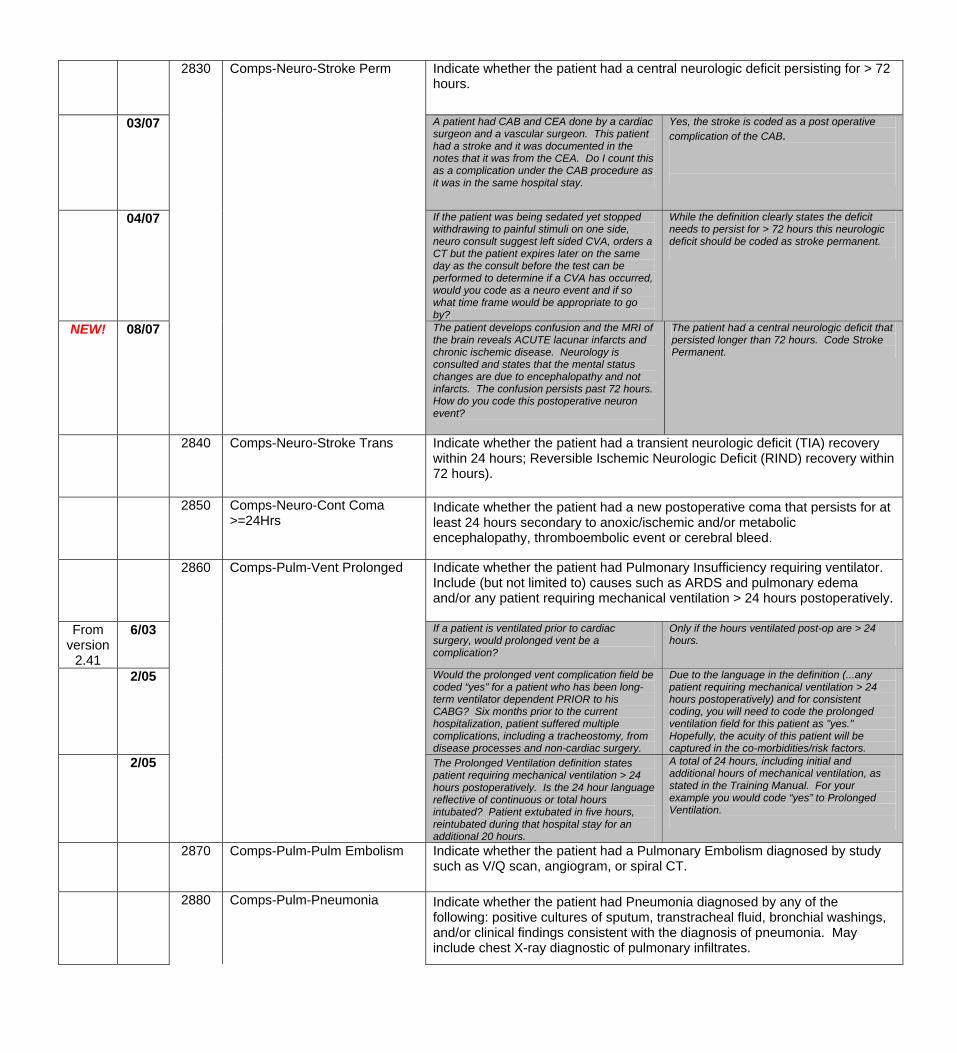
Indicate whether the patient had a central neurologic deficit persisting for > 72 hours.
03/07
2830
Comps-Neuro-Stroke Perm
A patient had CAB and CEA done by a cardiac surgeon and a vascular surgeon. This patient had a stroke and it was documented in the notes that it was from the CEA. Do I count this as a complication under the CAB procedure as it was in the same hospital stay.
Yes, the stroke is coded as a post operative complication of the CAB.
04/07 If the patient was being sedated yet stopped withdrawing to painful stimuli on one side, neuro consult suggest left sided CVA, orders a CT but the patient expires later on the same day as the consult before the test can be performed to determine if a CVA has occurred, would you code as a neuro event and if so what time frame would be appropriate to go by?
While the definition clearly states the deficit needs to persist for > 72 hours this neurologic deficit should be coded as stroke permanent.
NEW! 08/07 The patient develops confusion and the MRI of the brain reveals ACUTE lacunar infarcts and chronic ischemic disease. Neurology is consulted and states that the mental status changes are due to encephalopathy and not infarcts. The confusion persists past 72 hours. How do you code this postoperative neuron event?
The patient had a central neurologic deficit that persisted longer than 72 hours. Code Stroke Permanent.
2840 Comps-Neuro-Stroke Trans Indicate whether the patient had a transient neurologic deficit (TIA) recovery within 24 hours; Reversible Ischemic Neurologic Deficit (RIND) recovery within 72 hours).
2850
Comps-Neuro-Cont Coma >=24Hrs
Indicate whether the patient had a new postoperative coma that persists for at least 24 hours secondary to anoxic/ischemic and/or metabolic encephalopathy, thromboembolic event or cerebral bleed.
2860 Comps-Pulm-Vent Prolonged Indicate whether the patient had Pulmonary Insufficiency requiring ventilator. Include (but not limited to) causes such as ARDS and pulmonary edema and/or any patient requiring mechanical ventilation > 24 hours postoperatively.
From version
2.41
6/03 If a patient is ventilated prior to cardiac surgery, would prolonged vent be a complication?
Only if the hours ventilated post-op are > 24 hours.
2/05
Would the prolonged vent complication field be coded “yes” for a patient who has been long-term ventilator dependent PRIOR to his CABG? Six months prior to the current hospitalization, patient suffered multiple complications, including a tracheostomy, from disease processes and non-cardiac surgery.
Due to the language in the definition (...any patient requiring mechanical ventilation > 24 hours postoperatively) and for consistent coding, you will need to code the prolonged ventilation field for this patient as "yes." Hopefully, the acuity of this patient will be captured in the co-morbidities/risk factors.
2/05 The Prolonged Ventilation definition states patient requiring mechanical ventilation > 24 hours postoperatively. Is the 24 hour language reflective of continuous or total hours intubated? Patient extubated in five hours, reintubated during that hospital stay for an additional 20 hours.
A total of 24 hours, including initial and additional hours of mechanical ventilation, as stated in the Training Manual. For your example you would code “yes” to Prolonged Ventilation.
2870 Comps-Pulm-Pulm Embolism Indicate whether the patient had a Pulmonary Embolism diagnosed by study such as V/Q scan, angiogram, or spiral CT.
2880 Comps-Pulm-Pneumonia Indicate whether the patient had Pneumonia diagnosed by any of the following: positive cultures of sputum, transtracheal fluid, bronchial washings, and/or clinical findings consistent with the diagnosis of pneumonia. May include chest X-ray diagnostic of pulmonary infiltrates.
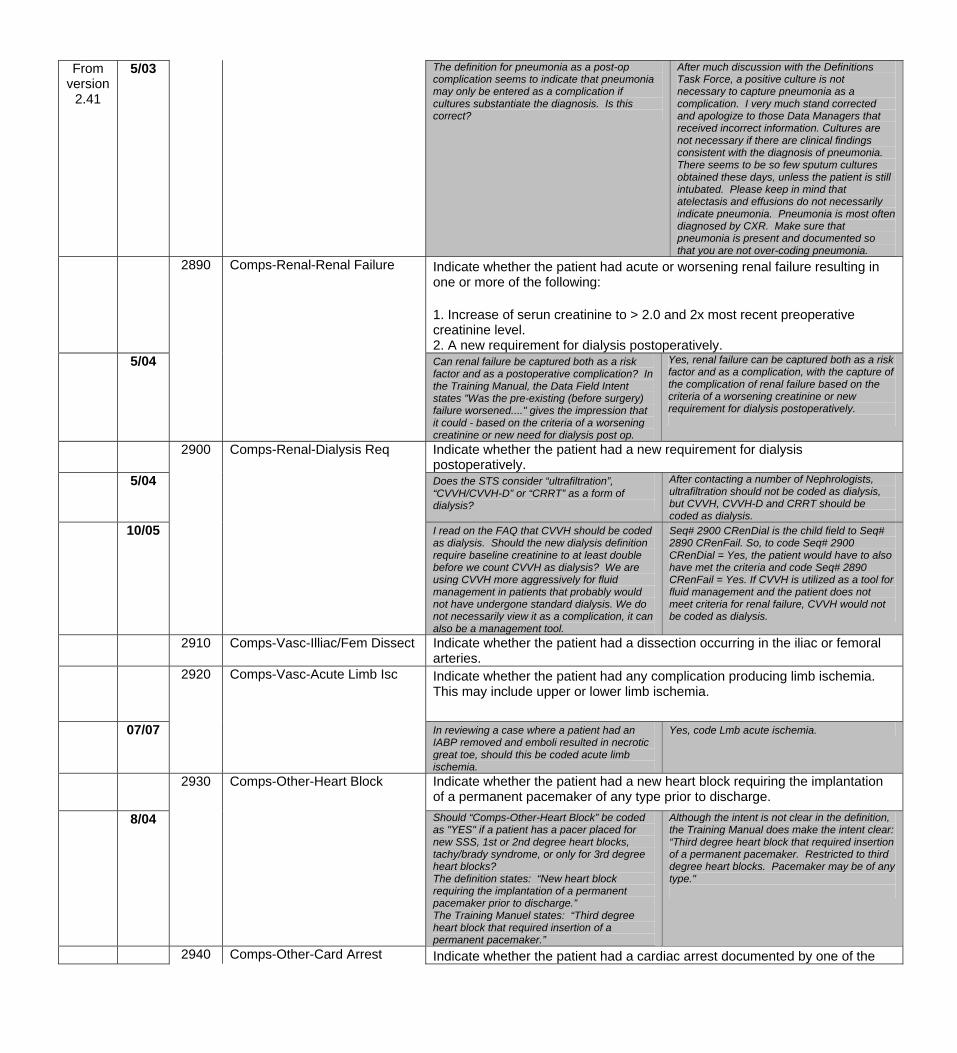
From version
2.41
5/03
The definition for pneumonia as a post-op complication seems to indicate that pneumonia may only be entered as a complication if cultures substantiate the diagnosis. Is this correct?
After much discussion with the Definitions Task Force, a positive culture is not necessary to capture pneumonia as a complication. I very much stand corrected and apologize to those Data Managers that received incorrect information. Cultures are not necessary if there are clinical findings consistent with the diagnosis of pneumonia. There seems to be so few sputum cultures obtained these days, unless the patient is still intubated. Please keep in mind that atelectasis and effusions do not necessarily indicate pneumonia. Pneumonia is most often diagnosed by CXR. Make sure that pneumonia is present and documented so that you are not over-coding pneumonia.
2890 Comps-Renal-Renal Failure
Indicate whether the patient had acute or worsening renal failure resulting in one or more of the following: 1. Increase of serun creatinine to > 2.0 and 2x most recent preoperative creatinine level. 2. A new requirement for dialysis postoperatively.
5/04 Can renal failure be captured both as a risk factor and as a postoperative complication? In the Training Manual, the Data Field Intent states "Was the pre-existing (before surgery) failure worsened...." gives the impression that it could - based on the criteria of a worsening creatinine or new need for dialysis post op.
Yes, renal failure can be captured both as a risk factor and as a complication, with the capture of the complication of renal failure based on the criteria of a worsening creatinine or new requirement for dialysis postoperatively.
2900 Comps-Renal-Dialysis Req Indicate whether the patient had a new requirement for dialysis postoperatively.
5/04 Does the STS consider “ultrafiltration”, “CVVH/CVVH-D” or “CRRT” as a form of dialysis?
After contacting a number of Nephrologists, ultrafiltration should not be coded as dialysis, but CVVH, CVVH-D and CRRT should be coded as dialysis.
10/05
I read on the FAQ that CVVH should be coded as dialysis. Should the new dialysis definition require baseline creatinine to at least double before we count CVVH as dialysis? We are using CVVH more aggressively for fluid management in patients that probably would not have undergone standard dialysis. We do not necessarily view it as a complication, it can also be a management tool.
Seq# 2900 CRenDial is the child field to Seq# 2890 CRenFail. So, to code Seq# 2900 CRenDial = Yes, the patient would have to also have met the criteria and code Seq# 2890 CRenFail = Yes. If CVVH is utilized as a tool for fluid management and the patient does not meet criteria for renal failure, CVVH would not be coded as dialysis.
2910 Comps-Vasc-Illiac/Fem Dissect Indicate whether the patient had a dissection occurring in the iliac or femoral arteries.
2920
Comps-Vasc-Acute Limb Isc
Indicate whether the patient had any complication producing limb ischemia. This may include upper or lower limb ischemia.
07/07 In reviewing a case where a patient had an IABP removed and emboli resulted in necrotic great toe, should this be coded acute limb ischemia.
Yes, code Lmb acute ischemia.
2930 Comps-Other-Heart Block Indicate whether the patient had a new heart block requiring the implantation of a permanent pacemaker of any type prior to discharge.
8/04 Should “Comps-Other-Heart Block” be coded as "YES" if a patient has a pacer placed for new SSS, 1st or 2nd degree heart blocks, tachy/brady syndrome, or only for 3rd degree heart blocks? The definition states: “New heart block requiring the implantation of a permanent pacemaker prior to discharge.” The Training Manuel states: “Third degree heart block that required insertion of a permanent pacemaker.”
Although the intent is not clear in the definition, the Training Manual does make the intent clear: “Third degree heart block that required insertion of a permanent pacemaker. Restricted to third degree heart blocks. Pacemaker may be of any type."
2940 Comps-Other-Card Arrest Indicate whether the patient had a cardiac arrest documented by one of the
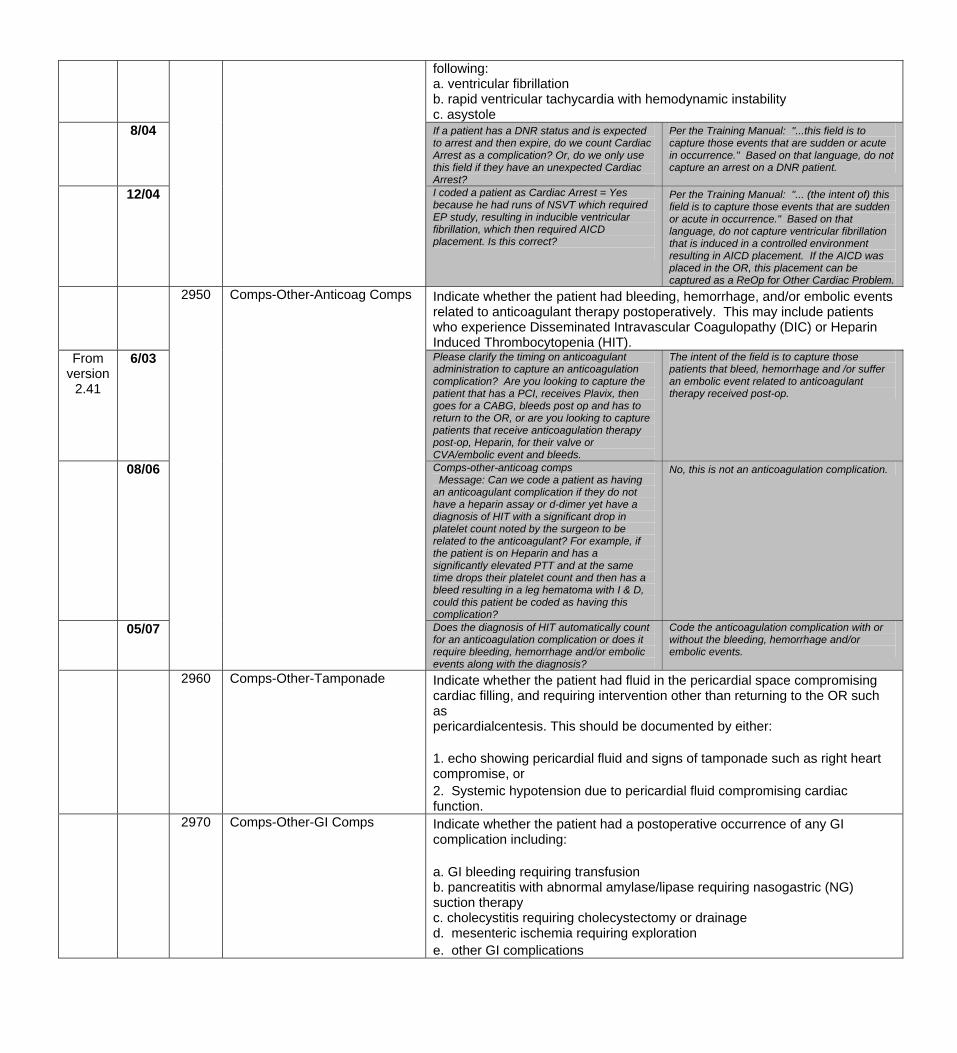
following: a. ventricular fibrillation b. rapid ventricular tachycardia with hemodynamic instability c. asystole
8/04 If a patient has a DNR status and is expected to arrest and then expire, do we count Cardiac Arrest as a complication? Or, do we only use this field if they have an unexpected Cardiac Arrest?
Per the Training Manual: "...this field is to capture those events that are sudden or acute in occurrence." Based on that language, do not capture an arrest on a DNR patient.
12/04
I coded a patient as Cardiac Arrest = Yes because he had runs of NSVT which required EP study, resulting in inducible ventricular fibrillation, which then required AICD placement. Is this correct?
Per the Training Manual: "... (the intent of) this field is to capture those events that are sudden or acute in occurrence." Based on that language, do not capture ventricular fibrillation that is induced in a controlled environment resulting in AICD placement. If the AICD was placed in the OR, this placement can be captured as a ReOp for Other Cardiac Problem.
2950 Comps-Other-Anticoag Comps Indicate whether the patient had bleeding, hemorrhage, and/or embolic events related to anticoagulant therapy postoperatively. This may include patients who experience Disseminated Intravascular Coagulopathy (DIC) or Heparin Induced Thrombocytopenia (HIT).
From version
2.41
6/03 Please clarify the timing on anticoagulant administration to capture an anticoagulation complication? Are you looking to capture the patient that has a PCI, receives Plavix, then goes for a CABG, bleeds post op and has to return to the OR, or are you looking to capture patients that receive anticoagulation therapy post-op, Heparin, for their valve or CVA/embolic event and bleeds.
The intent of the field is to capture those patients that bleed, hemorrhage and /or suffer an embolic event related to anticoagulant therapy received post-op.
08/06 Comps-other-anticoag comps Message: Can we code a patient as having an anticoagulant complication if they do not have a heparin assay or d-dimer yet have a diagnosis of HIT with a significant drop in platelet count noted by the surgeon to be related to the anticoagulant? For example, if the patient is on Heparin and has a significantly elevated PTT and at the same time drops their platelet count and then has a bleed resulting in a leg hematoma with I & D, could this patient be coded as having this complication?
No, this is not an anticoagulation complication.
05/07 Does the diagnosis of HIT automatically count for an anticoagulation complication or does it require bleeding, hemorrhage and/or embolic events along with the diagnosis?
Code the anticoagulation complication with or without the bleeding, hemorrhage and/or embolic events.
2960
Comps-Other-Tamponade Indicate whether the patient had fluid in the pericardial space compromising cardiac filling, and requiring intervention other than returning to the OR such as pericardialcentesis. This should be documented by either: 1. echo showing pericardial fluid and signs of tamponade such as right heart compromise, or 2. Systemic hypotension due to pericardial fluid compromising cardiac function.
2970
Comps-Other-GI Comps
Indicate whether the patient had a postoperative occurrence of any GI complication including: a. GI bleeding requiring transfusion b. pancreatitis with abnormal amylase/lipase requiring nasogastric (NG) suction therapy c. cholecystitis requiring cholecystectomy or drainage d. mesenteric ischemia requiring exploration e. other GI complications
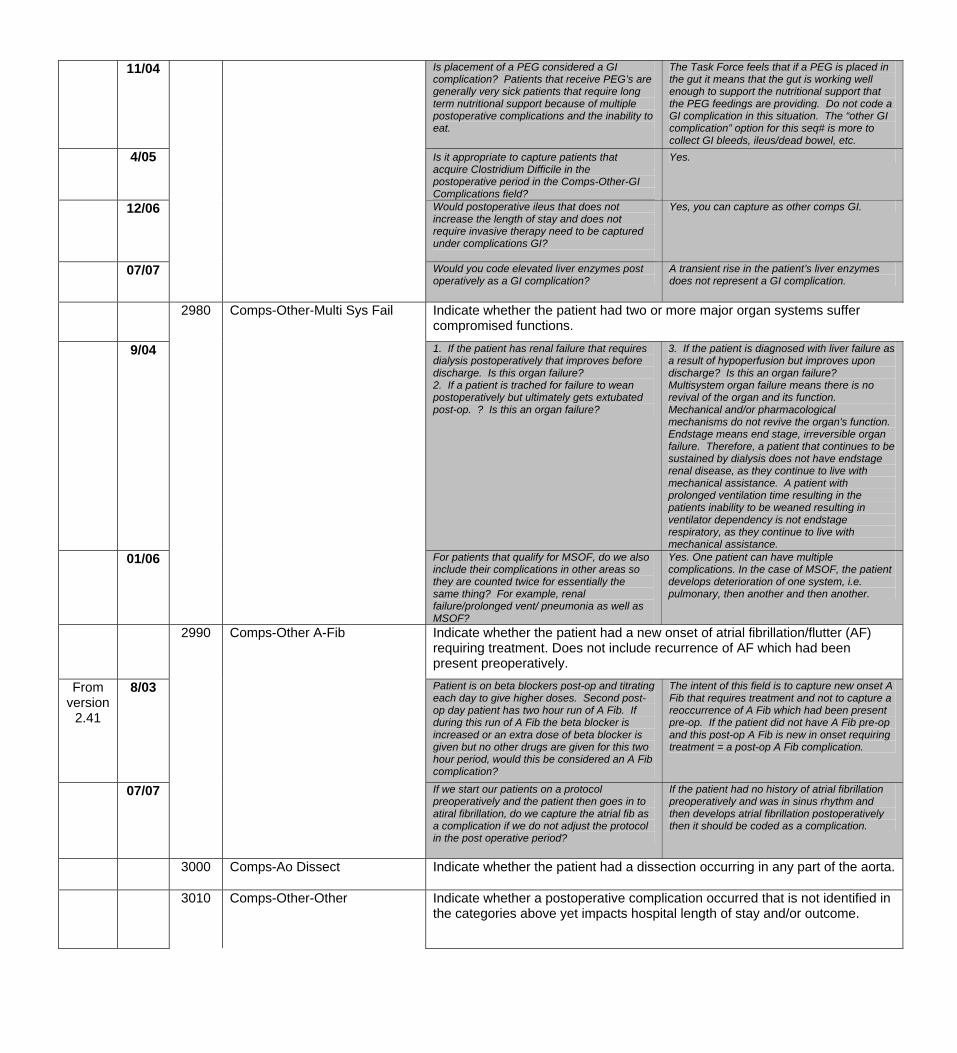
11/04 Is placement of a PEG considered a GI complication? Patients that receive PEG’s are generally very sick patients that require long term nutritional support because of multiple postoperative complications and the inability to eat.
The Task Force feels that if a PEG is placed in the gut it means that the gut is working well enough to support the nutritional support that the PEG feedings are providing. Do not code a GI complication in this situation. The “other GI complication” option for this seq# is more to collect GI bleeds, ileus/dead bowel, etc.
4/05 Is it appropriate to capture patients that acquire Clostridium Difficile in the postoperative period in the Comps-Other-GI Complications field?
Yes.
12/06
Would postoperative ileus that does not increase the length of stay and does not require invasive therapy need to be captured under complications GI?
Yes, you can capture as other comps GI.
07/07 Would you code elevated liver enzymes post operatively as a GI complication?
A transient rise in the patient’s liver enzymes does not represent a GI complication.
Indicate whether the patient had two or more major organ systems suffer compromised functions.
9/04
2980
Comps-Other-Multi Sys Fail
1. If the patient has renal failure that requires dialysis postoperatively that improves before discharge. Is this organ failure? 2. If a patient is trached for failure to wean postoperatively but ultimately gets extubated post-op. ? Is this an organ failure?
3. If the patient is diagnosed with liver failure as a result of hypoperfusion but improves upon discharge? Is this an organ failure? Multisystem organ failure means there is no revival of the organ and its function. Mechanical and/or pharmacological mechanisms do not revive the organ's function. Endstage means end stage, irreversible organ failure. Therefore, a patient that continues to be sustained by dialysis does not have endstage renal disease, as they continue to live with mechanical assistance. A patient with prolonged ventilation time resulting in the patients inability to be weaned resulting in ventilator dependency is not endstage respiratory, as they continue to live with mechanical assistance.
01/06 For patients that qualify for MSOF, do we also include their complications in other areas so they are counted twice for essentially the same thing? For example, renal failure/prolonged vent/ pneumonia as well as MSOF?
Yes. One patient can have multiple complications. In the case of MSOF, the patient develops deterioration of one system, i.e. pulmonary, then another and then another.
2990 Comps-Other A-Fib Indicate whether the patient had a new onset of atrial fibrillation/flutter (AF) requiring treatment. Does not include recurrence of AF which had been present preoperatively.
From version
2.41
8/03 Patient is on beta blockers post-op and titrating each day to give higher doses. Second post-op day patient has two hour run of A Fib. If during this run of A Fib the beta blocker is increased or an extra dose of beta blocker is given but no other drugs are given for this two hour period, would this be considered an A Fib complication?
The intent of this field is to capture new onset A Fib that requires treatment and not to capture a reoccurrence of A Fib which had been present pre-op. If the patient did not have A Fib pre-op and this post-op A Fib is new in onset requiring treatment = a post-op A Fib complication.
07/07 If we start our patients on a protocol preoperatively and the patient then goes in to atiral fibrillation, do we capture the atrial fib as a complication if we do not adjust the protocol in the post operative period?
If the patient had no history of atrial fibrillation preoperatively and was in sinus rhythm and then develops atrial fibrillation postoperatively then it should be coded as a complication.
3000
Comps-Ao Dissect
Indicate whether the patient had a dissection occurring in any part of the aorta.
3010 Comps-Other-Other Indicate whether a postoperative complication occurred that is not identified in the categories above yet impacts hospital length of stay and/or outcome.
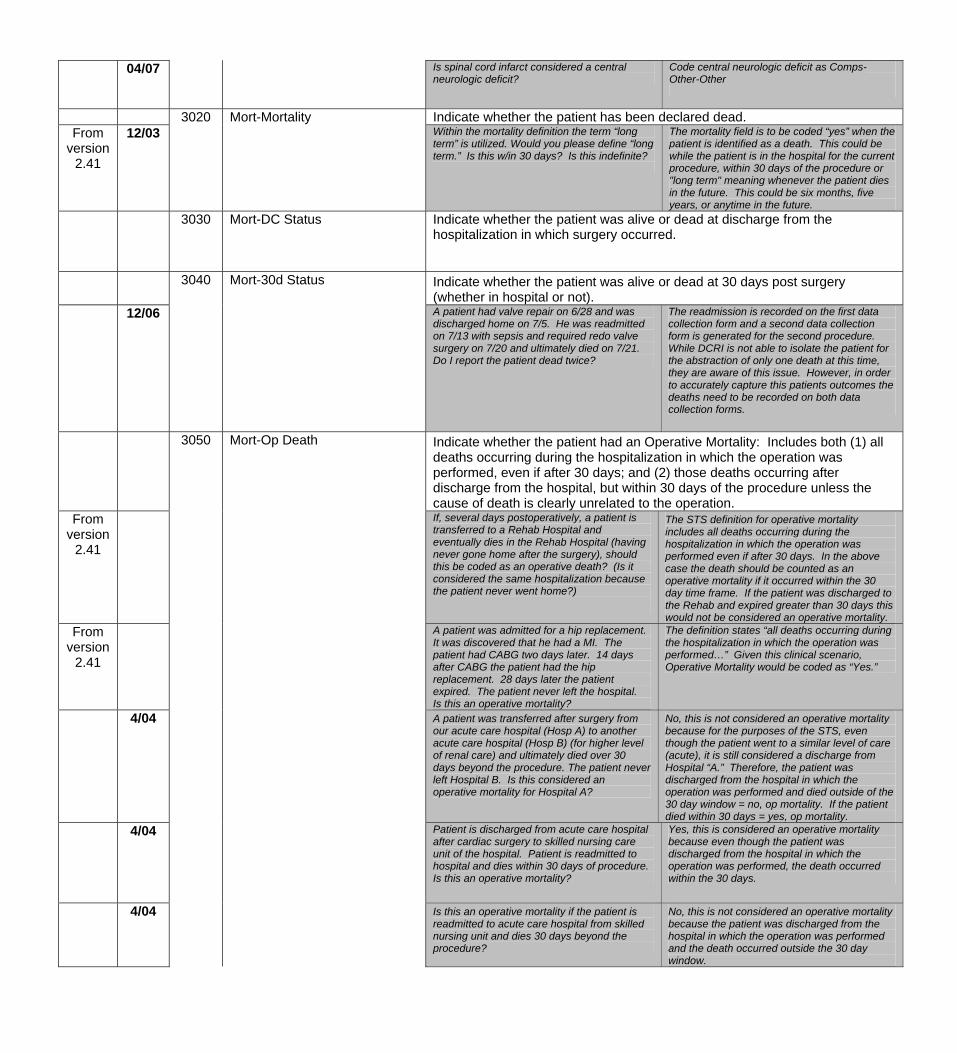
04/07 Is spinal cord infarct considered a central neurologic deficit?
Code central neurologic deficit as Comps-Other-Other
3020 Mort-Mortality Indicate whether the patient has been declared dead. From
version 2.41
12/03 Within the mortality definition the term “long term” is utilized. Would you please define “long term.” Is this w/in 30 days? Is this indefinite?
The mortality field is to be coded “yes” when the patient is identified as a death. This could be while the patient is in the hospital for the current procedure, within 30 days of the procedure or "long term" meaning whenever the patient dies in the future. This could be six months, five years, or anytime in the future.
3030 Mort-DC Status Indicate whether the patient was alive or dead at discharge from the hospitalization in which surgery occurred.
3040
Mort-30d Status
Indicate whether the patient was alive or dead at 30 days post surgery (whether in hospital or not).
12/06 A patient had valve repair on 6/28 and was discharged home on 7/5. He was readmitted on 7/13 with sepsis and required redo valve surgery on 7/20 and ultimately died on 7/21. Do I report the patient dead twice?
The readmission is recorded on the first data collection form and a second data collection form is generated for the second procedure. While DCRI is not able to isolate the patient for the abstraction of only one death at this time, they are aware of this issue. However, in order to accurately capture this patients outcomes the deaths need to be recorded on both data collection forms.
3050 Mort-Op Death Indicate whether the patient had an Operative Mortality: Includes both (1) all deaths occurring during the hospitalization in which the operation was performed, even if after 30 days; and (2) those deaths occurring after discharge from the hospital, but within 30 days of the procedure unless the cause of death is clearly unrelated to the operation.
From version
2.41
If, several days postoperatively, a patient is transferred to a Rehab Hospital and eventually dies in the Rehab Hospital (having never gone home after the surgery), should this be coded as an operative death? (Is it considered the same hospitalization because the patient never went home?)
The STS definition for operative mortality includes all deaths occurring during the hospitalization in which the operation was performed even if after 30 days. In the above case the death should be counted as an operative mortality if it occurred within the 30 day time frame. If the patient was discharged to the Rehab and expired greater than 30 days this would not be considered an operative mortality.
From version
2.41
A patient was admitted for a hip replacement. It was discovered that he had a MI. The patient had CABG two days later. 14 days after CABG the patient had the hip replacement. 28 days later the patient expired. The patient never left the hospital. Is this an operative mortality?
The definition states “all deaths occurring during the hospitalization in which the operation was performed…” Given this clinical scenario, Operative Mortality would be coded as “Yes.”
4/04 A patient was transferred after surgery from our acute care hospital (Hosp A) to another acute care hospital (Hosp B) (for higher level of renal care) and ultimately died over 30 days beyond the procedure. The patient never left Hospital B. Is this considered an operative mortality for Hospital A?
No, this is not considered an operative mortality because for the purposes of the STS, even though the patient went to a similar level of care (acute), it is still considered a discharge from Hospital “A.” Therefore, the patient was discharged from the hospital in which the operation was performed and died outside of the 30 day window = no, op mortality. If the patient died within 30 days = yes, op mortality.
4/04
Patient is discharged from acute care hospital after cardiac surgery to skilled nursing care unit of the hospital. Patient is readmitted to hospital and dies within 30 days of procedure. Is this an operative mortality?
Yes, this is considered an operative mortality because even though the patient was discharged from the hospital in which the operation was performed, the death occurred within the 30 days.
4/04 Is this an operative mortality if the patient is readmitted to acute care hospital from skilled nursing unit and dies 30 days beyond the procedure?
No, this is not considered an operative mortality because the patient was discharged from the hospital in which the operation was performed and the death occurred outside the 30 day window.
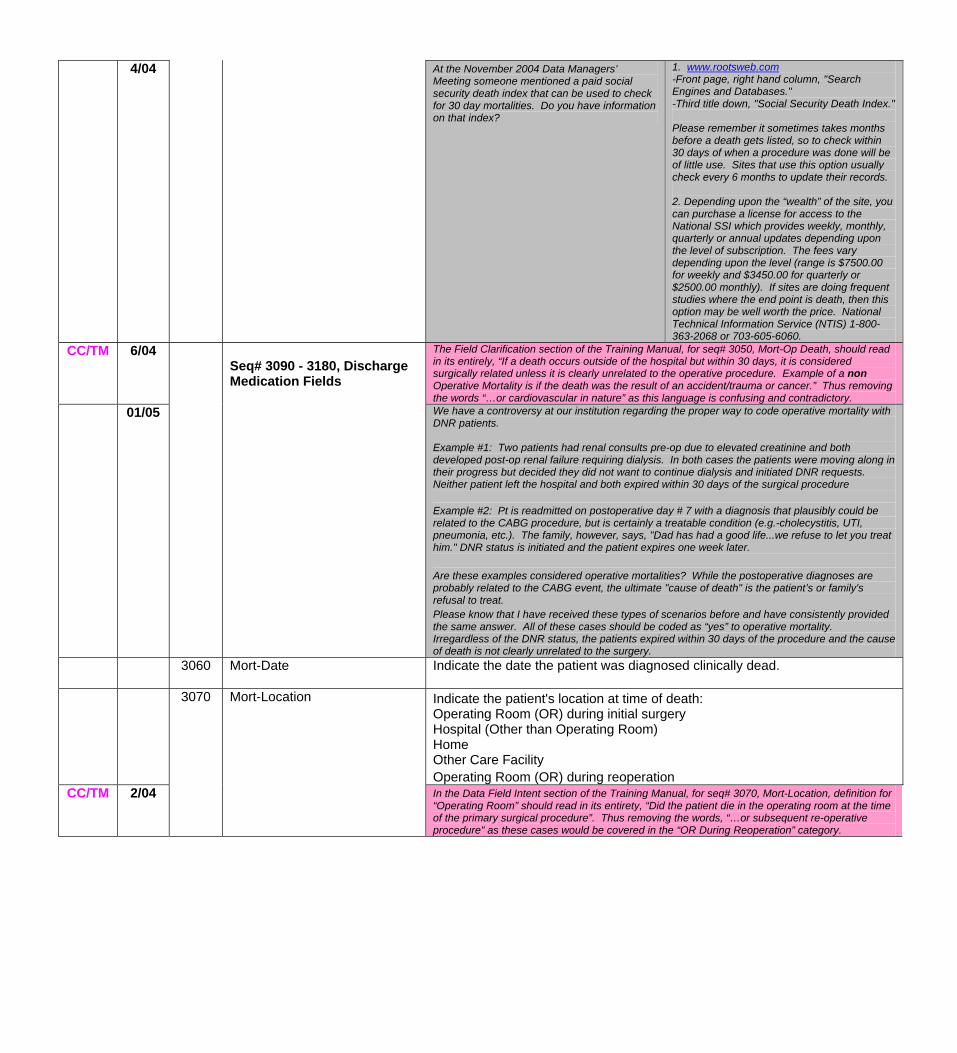
4/04 At the November 2004 Data Managers’ Meeting someone mentioned a paid social security death index that can be used to check for 30 day mortalities. Do you have information on that index?
1. www.rootsweb.com -Front page, right hand column, "Search Engines and Databases." -Third title down, "Social Security Death Index." Please remember it sometimes takes months before a death gets listed, so to check within 30 days of when a procedure was done will be of little use. Sites that use this option usually check every 6 months to update their records. 2. Depending upon the “wealth” of the site, you can purchase a license for access to the National SSI which provides weekly, monthly, quarterly or annual updates depending upon the level of subscription. The fees vary depending upon the level (range is $7500.00 for weekly and $3450.00 for quarterly or $2500.00 monthly). If sites are doing frequent studies where the end point is death, then this option may be well worth the price. National Technical Information Service (NTIS) 1-800-363-2068 or 703-605-6060.
CC/TM 6/04 Seq# 3090 - 3180, Discharge Medication Fields
The Field Clarification section of the Training Manual, for seq# 3050, Mort-Op Death, should read in its entirely, “If a death occurs outside of the hospital but within 30 days, it is considered surgically related unless it is clearly unrelated to the operative procedure. Example of a non Operative Mortality is if the death was the result of an accident/trauma or cancer.” Thus removing the words “…or cardiovascular in nature” as this language is confusing and contradictory.
01/05 We have a controversy at our institution regarding the proper way to code operative mortality with DNR patients. Example #1: Two patients had renal consults pre-op due to elevated creatinine and both developed post-op renal failure requiring dialysis. In both cases the patients were moving along in their progress but decided they did not want to continue dialysis and initiated DNR requests. Neither patient left the hospital and both expired within 30 days of the surgical procedure Example #2: Pt is readmitted on postoperative day # 7 with a diagnosis that plausibly could be related to the CABG procedure, but is certainly a treatable condition (e.g.-cholecystitis, UTI, pneumonia, etc.). The family, however, says, "Dad has had a good life...we refuse to let you treat him." DNR status is initiated and the patient expires one week later. Are these examples considered operative mortalities? While the postoperative diagnoses are probably related to the CABG event, the ultimate "cause of death" is the patient’s or family's refusal to treat. Please know that I have received these types of scenarios before and have consistently provided the same answer. All of these cases should be coded as “yes” to operative mortality. Irregardless of the DNR status, the patients expired within 30 days of the procedure and the cause of death is not clearly unrelated to the surgery.
3060 Mort-Date
Indicate the date the patient was diagnosed clinically dead.
Indicate the patient's location at time of death: Operating Room (OR) during initial surgery Hospital (Other than Operating Room) Home Other Care Facility Operating Room (OR) during reoperation
CC/TM 2/04
3070 Mort-Location
In the Data Field Intent section of the Training Manual, for seq# 3070, Mort-Location, definition for “Operating Room” should read in its entirety, “Did the patient die in the operating room at the time of the primary surgical procedure”. Thus removing the words, “…or subsequent re-operative procedure” as these cases would be covered in the “OR During Reoperation” category.
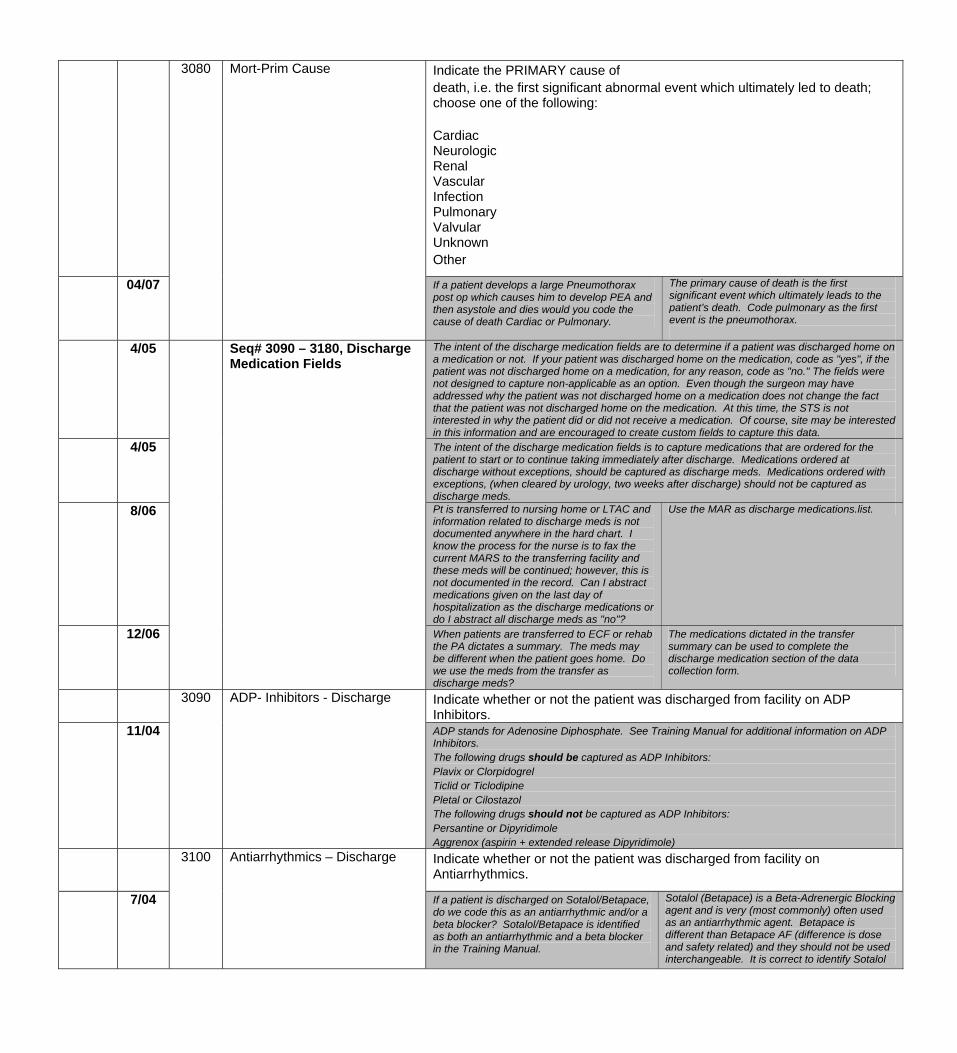
Indicate the PRIMARY cause of death, i.e. the first significant abnormal event which ultimately led to death; choose one of the following: Cardiac Neurologic Renal Vascular Infection Pulmonary Valvular Unknown Other
04/07
3080 Mort-Prim Cause
If a patient develops a large Pneumothorax post op which causes him to develop PEA and then asystole and dies would you code the cause of death Cardiac or Pulmonary.
The primary cause of death is the first significant event which ultimately leads to the patient’s death. Code pulmonary as the first event is the pneumothorax.
4/05 Seq# 3090 – 3180, Discharge Medication Fields
The intent of the discharge medication fields are to determine if a patient was discharged home on a medication or not. If your patient was discharged home on the medication, code as "yes", if the patient was not discharged home on a medication, for any reason, code as "no." The fields were not designed to capture non-applicable as an option. Even though the surgeon may have addressed why the patient was not discharged home on a medication does not change the fact that the patient was not discharged home on the medication. At this time, the STS is not interested in why the patient did or did not receive a medication. Of course, site may be interested in this information and are encouraged to create custom fields to capture this data.
4/05 The intent of the discharge medication fields is to capture medications that are ordered for the patient to start or to continue taking immediately after discharge. Medications ordered at discharge without exceptions, should be captured as discharge meds. Medications ordered with exceptions, (when cleared by urology, two weeks after discharge) should not be captured as discharge meds.
8/06 Pt is transferred to nursing home or LTAC and information related to discharge meds is not documented anywhere in the hard chart. I know the process for the nurse is to fax the current MARS to the transferring facility and these meds will be continued; however, this is not documented in the record. Can I abstract medications given on the last day of hospitalization as the discharge medications or do I abstract all discharge meds as "no"?
Use the MAR as discharge medications.list.
12/06 When patients are transferred to ECF or rehab the PA dictates a summary. The meds may be different when the patient goes home. Do we use the meds from the transfer as discharge meds?
The medications dictated in the transfer summary can be used to complete the discharge medication section of the data collection form.
Indicate whether or not the patient was discharged from facility on ADP Inhibitors.
11/04
3090
ADP- Inhibitors - Discharge
ADP stands for Adenosine Diphosphate. See Training Manual for additional information on ADP Inhibitors. The following drugs should be captured as ADP Inhibitors: Plavix or Clorpidogrel Ticlid or Ticlodipine Pletal or Cilostazol The following drugs should not be captured as ADP Inhibitors: Persantine or Dipyridimole Aggrenox (aspirin + extended release Dipyridimole)
3100
Antiarrhythmics – Discharge
Indicate whether or not the patient was discharged from facility on Antiarrhythmics.
7/04 If a patient is discharged on Sotalol/Betapace, do we code this as an antiarrhythmic and/or a beta blocker? Sotalol/Betapace is identified as both an antiarrhythmic and a beta blocker in the Training Manual.
Sotalol (Betapace) is a Beta-Adrenergic Blocking agent and is very (most commonly) often used as an antiarrhythmic agent. Betapace is different than Betapace AF (difference is dose and safety related) and they should not be used interchangeable. It is correct to identify Sotalol
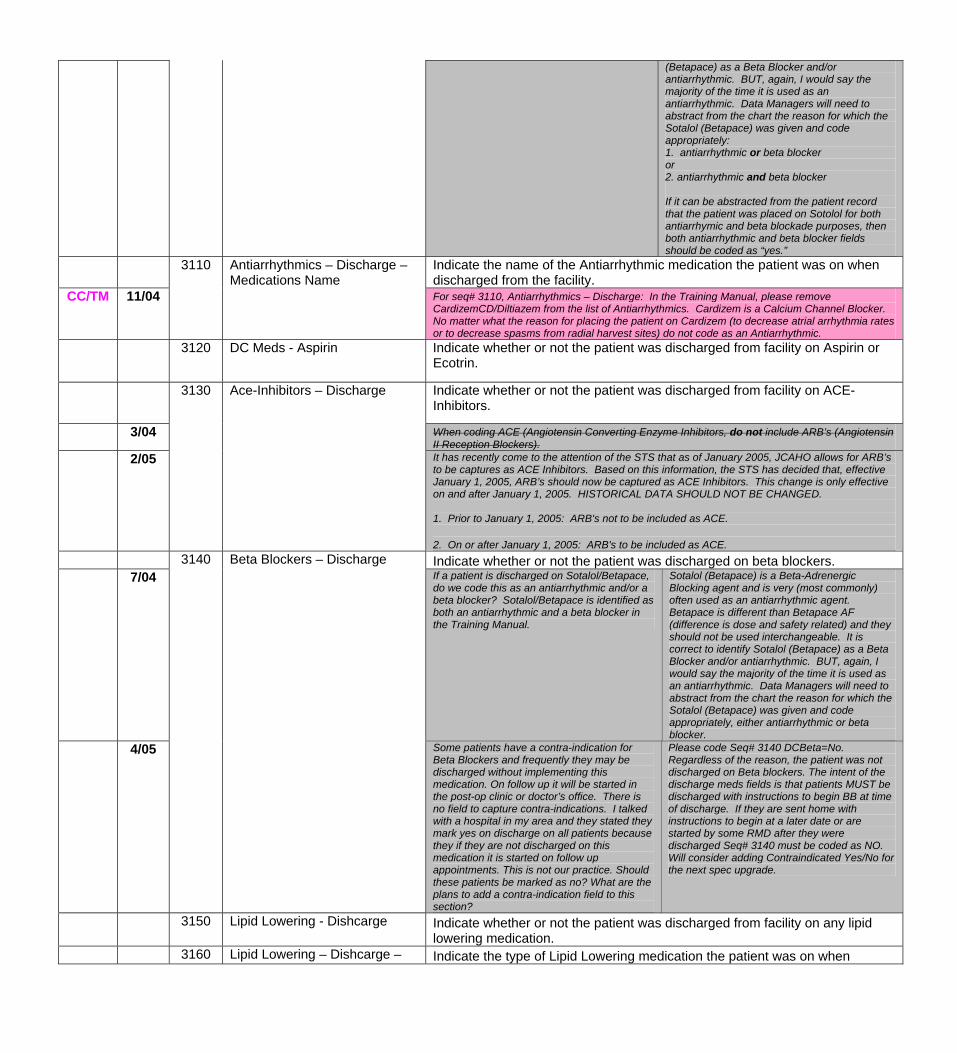
(Betapace) as a Beta Blocker and/or antiarrhythmic. BUT, again, I would say the majority of the time it is used as an antiarrhythmic. Data Managers will need to abstract from the chart the reason for which the Sotalol (Betapace) was given and code appropriately: 1. antiarrhythmic or beta blocker or 2. antiarrhythmic and beta blocker If it can be abstracted from the patient record that the patient was placed on Sotolol for both antiarrhymic and beta blockade purposes, then both antiarrhythmic and beta blocker fields should be coded as “yes.”
Indicate the name of the Antiarrhythmic medication the patient was on when discharged from the facility.
CC/TM 11/04
3110
Antiarrhythmics – Discharge – Medications Name For seq# 3110, Antiarrhythmics – Discharge: In the Training Manual, please remove
CardizemCD/Diltiazem from the list of Antiarrhythmics. Cardizem is a Calcium Channel Blocker. No matter what the reason for placing the patient on Cardizem (to decrease atrial arrhythmia rates or to decrease spasms from radial harvest sites) do not code as an Antiarrhythmic.
3120 DC Meds - Aspirin Indicate whether or not the patient was discharged from facility on Aspirin or Ecotrin.
3130 Ace-Inhibitors – Discharge Indicate whether or not the patient was discharged from facility on ACE- Inhibitors.
3/04 When coding ACE (Angiotensin Converting Enzyme Inhibitors, do not include ARB’s (Angiotensin II Reception Blockers).
2/05
It has recently come to the attention of the STS that as of January 2005, JCAHO allows for ARB’s to be captures as ACE Inhibitors. Based on this information, the STS has decided that, effective January 1, 2005, ARB’s should now be captured as ACE Inhibitors. This change is only effective on and after January 1, 2005. HISTORICAL DATA SHOULD NOT BE CHANGED. 1. Prior to January 1, 2005: ARB's not to be included as ACE. 2. On or after January 1, 2005: ARB's to be included as ACE.
3140 Beta Blockers – Discharge Indicate whether or not the patient was discharged on beta blockers. 7/04
If a patient is discharged on Sotalol/Betapace,
do we code this as an antiarrhythmic and/or a beta blocker? Sotalol/Betapace is identified as both an antiarrhythmic and a beta blocker in the Training Manual.
Sotalol (Betapace) is a Beta-Adrenergic Blocking agent and is very (most commonly) often used as an antiarrhythmic agent. Betapace is different than Betapace AF (difference is dose and safety related) and they should not be used interchangeable. It is correct to identify Sotalol (Betapace) as a Beta Blocker and/or antiarrhythmic. BUT, again, I would say the majority of the time it is used as an antiarrhythmic. Data Managers will need to abstract from the chart the reason for which the Sotalol (Betapace) was given and code appropriately, either antiarrhythmic or beta blocker.
4/05
Some patients have a contra-indication for Beta Blockers and frequently they may be discharged without implementing this medication. On follow up it will be started in the post-op clinic or doctor’s office. There is no field to capture contra-indications. I talked with a hospital in my area and they stated they mark yes on discharge on all patients because they if they are not discharged on this medication it is started on follow up appointments. This is not our practice. Should these patients be marked as no? What are the plans to add a contra-indication field to this section?
Please code Seq# 3140 DCBeta=No. Regardless of the reason, the patient was not discharged on Beta blockers. The intent of the discharge meds fields is that patients MUST be discharged with instructions to begin BB at time of discharge. If they are sent home with instructions to begin at a later date or are started by some RMD after they were discharged Seq# 3140 must be coded as NO. Will consider adding Contraindicated Yes/No for the next spec upgrade.
3150 Lipid Lowering - Dishcarge
Indicate whether or not the patient was discharged from facility on any lipid lowering medication.
3160 Lipid Lowering – Dishcarge – Indicate the type of Lipid Lowering medication the patient was on when
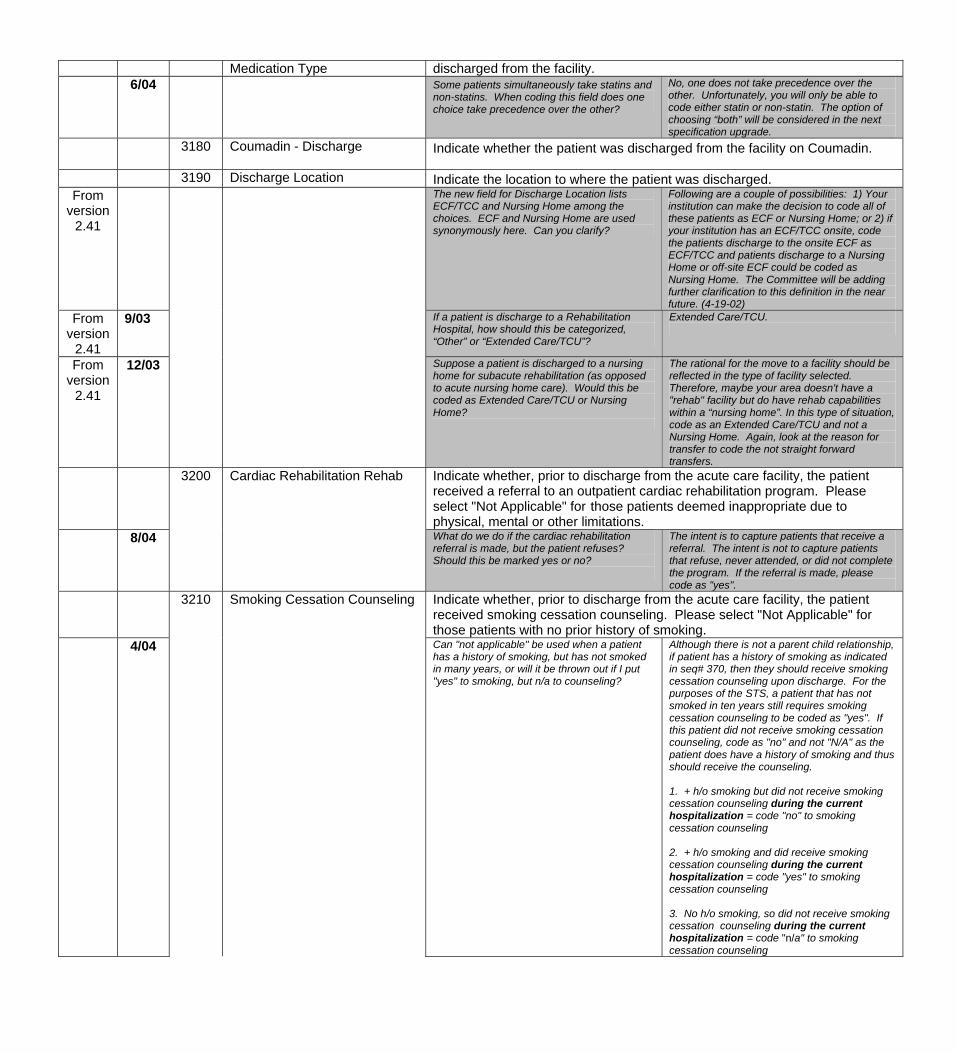
Medication Type discharged from the facility. 6/04
Some patients simultaneously take statins and non-statins. When coding this field does one choice take precedence over the other?
No, one does not take precedence over the other. Unfortunately, you will only be able to code either statin or non-statin. The option of choosing “both” will be considered in the next specification upgrade.
3180 Coumadin - Discharge
Indicate whether the patient was discharged from the facility on Coumadin.
3190 Discharge Location Indicate the location to where the patient was discharged. From
version 2.41
The new field for Discharge Location lists ECF/TCC and Nursing Home among the choices. ECF and Nursing Home are used synonymously here. Can you clarify?
Following are a couple of possibilities: 1) Your institution can make the decision to code all of these patients as ECF or Nursing Home; or 2) if your institution has an ECF/TCC onsite, code the patients discharge to the onsite ECF as ECF/TCC and patients discharge to a Nursing Home or off-site ECF could be coded as Nursing Home. The Committee will be adding further clarification to this definition in the near future. (4-19-02)
From version
2.41
9/03
If a patient is discharge to a Rehabilitation Hospital, how should this be categorized, “Other” or “Extended Care/TCU”?
Extended Care/TCU.
From version
2.41
12/03
Suppose a patient is discharged to a nursing home for subacute rehabilitation (as opposed to acute nursing home care). Would this be coded as Extended Care/TCU or Nursing Home?
The rational for the move to a facility should be reflected in the type of facility selected. Therefore, maybe your area doesn't have a "rehab" facility but do have rehab capabilities within a “nursing home”. In this type of situation, code as an Extended Care/TCU and not a Nursing Home. Again, look at the reason for transfer to code the not straight forward transfers.
3200 Cardiac Rehabilitation Rehab Indicate whether, prior to discharge from the acute care facility, the patient received a referral to an outpatient cardiac rehabilitation program. Please select "Not Applicable" for those patients deemed inappropriate due to physical, mental or other limitations.
8/04
What do we do if the cardiac rehabilitation referral is made, but the patient refuses? Should this be marked yes or no?
The intent is to capture patients that receive a referral. The intent is not to capture patients that refuse, never attended, or did not complete the program. If the referral is made, please code as "yes".
3210 Smoking Cessation Counseling Indicate whether, prior to discharge from the acute care facility, the patient received smoking cessation counseling. Please select "Not Applicable" for those patients with no prior history of smoking.
4/04 Can "not applicable" be used when a patient has a history of smoking, but has not smoked in many years, or will it be thrown out if I put "yes" to smoking, but n/a to counseling?
Although there is not a parent child relationship, if patient has a history of smoking as indicated in seq# 370, then they should receive smoking cessation counseling upon discharge. For the purposes of the STS, a patient that has not smoked in ten years still requires smoking cessation counseling to be coded as "yes". If this patient did not receive smoking cessation counseling, code as "no" and not "N/A" as the patient does have a history of smoking and thus should receive the counseling. 1. + h/o smoking but did not receive smoking cessation counseling during the current hospitalization = code "no" to smoking cessation counseling 2. + h/o smoking and did receive smoking cessation counseling during the current hospitalization = code "yes" to smoking cessation counseling 3. No h/o smoking, so did not receive smoking cessation counseling during the current hospitalization = code "n/a" to smoking cessation counseling
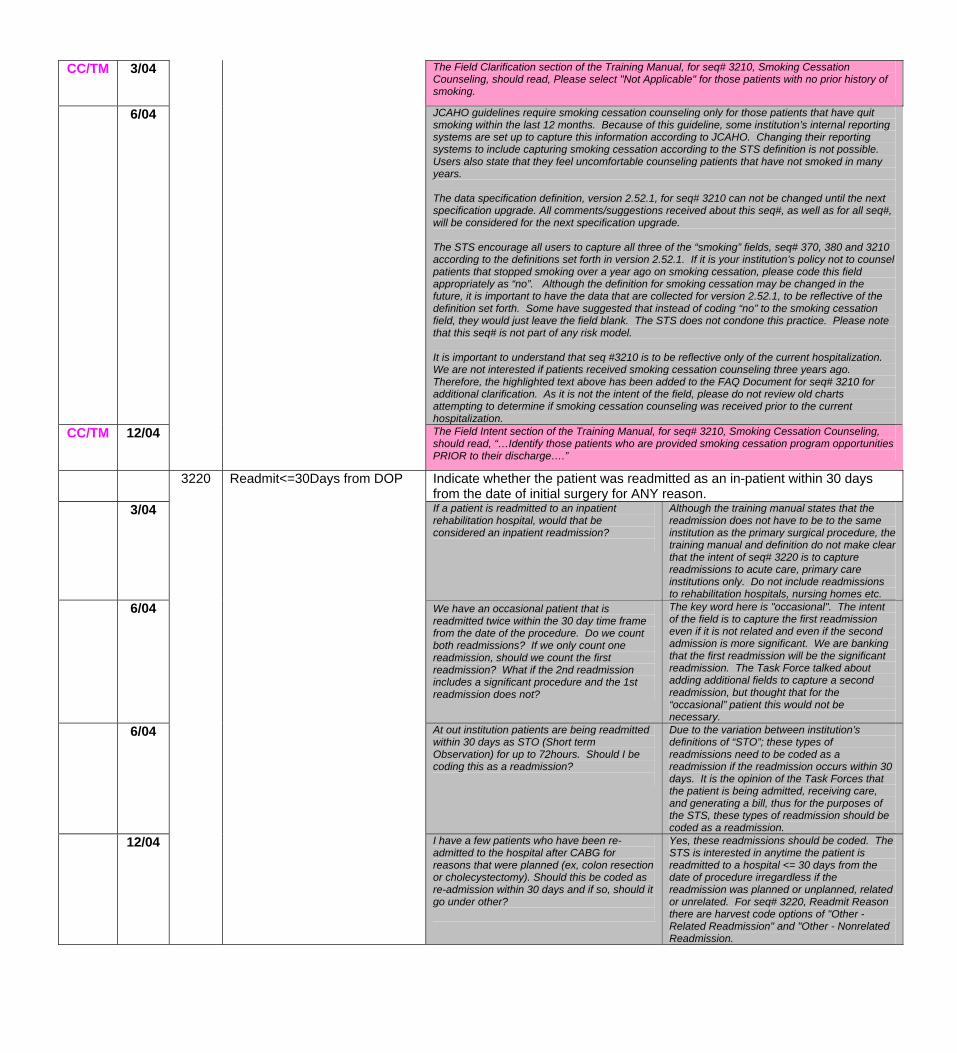
CC/TM 3/04 The Field Clarification section of the Training Manual, for seq# 3210, Smoking Cessation Counseling, should read, Please select "Not Applicable" for those patients with no prior history of smoking.
6/04 JCAHO guidelines require smoking cessation counseling only for those patients that have quit smoking within the last 12 months. Because of this guideline, some institution’s internal reporting systems are set up to capture this information according to JCAHO. Changing their reporting systems to include capturing smoking cessation according to the STS definition is not possible. Users also state that they feel uncomfortable counseling patients that have not smoked in many years. The data specification definition, version 2.52.1, for seq# 3210 can not be changed until the next specification upgrade. All comments/suggestions received about this seq#, as well as for all seq#, will be considered for the next specification upgrade. The STS encourage all users to capture all three of the “smoking” fields, seq# 370, 380 and 3210 according to the definitions set forth in version 2.52.1. If it is your institution’s policy not to counsel patients that stopped smoking over a year ago on smoking cessation, please code this field appropriately as “no”. Although the definition for smoking cessation may be changed in the future, it is important to have the data that are collected for version 2.52.1, to be reflective of the definition set forth. Some have suggested that instead of coding “no” to the smoking cessation field, they would just leave the field blank. The STS does not condone this practice. Please note that this seq# is not part of any risk model. It is important to understand that seq #3210 is to be reflective only of the current hospitalization. We are not interested if patients received smoking cessation counseling three years ago. Therefore, the highlighted text above has been added to the FAQ Document for seq# 3210 for additional clarification. As it is not the intent of the field, please do not review old charts attempting to determine if smoking cessation counseling was received prior to the current hospitalization.
CC/TM 12/04 The Field Intent section of the Training Manual, for seq# 3210, Smoking Cessation Counseling, should read, “…Identify those patients who are provided smoking cessation program opportunities PRIOR to their discharge….”
3220 Readmit<=30Days from DOP Indicate whether the patient was readmitted as an in-patient within 30 days from the date of initial surgery for ANY reason.
3/04 If a patient is readmitted to an inpatient rehabilitation hospital, would that be considered an inpatient readmission?
Although the training manual states that the readmission does not have to be to the same institution as the primary surgical procedure, the training manual and definition do not make clear that the intent of seq# 3220 is to capture readmissions to acute care, primary care institutions only. Do not include readmissions to rehabilitation hospitals, nursing homes etc.
6/04
We have an occasional patient that is readmitted twice within the 30 day time frame from the date of the procedure. Do we count both readmissions? If we only count one readmission, should we count the first readmission? What if the 2nd readmission includes a significant procedure and the 1st readmission does not?
The key word here is "occasional". The intent of the field is to capture the first readmission even if it is not related and even if the second admission is more significant. We are banking that the first readmission will be the significant readmission. The Task Force talked about adding additional fields to capture a second readmission, but thought that for the “occasional” patient this would not be necessary.
6/04 At out institution patients are being readmitted within 30 days as STO (Short term Observation) for up to 72hours. Should I be coding this as a readmission?
Due to the variation between institution’s definitions of “STO”; these types of readmissions need to be coded as a readmission if the readmission occurs within 30 days. It is the opinion of the Task Forces that the patient is being admitted, receiving care, and generating a bill, thus for the purposes of the STS, these types of readmission should be coded as a readmission.
12/04
I have a few patients who have been re-admitted to the hospital after CABG for reasons that were planned (ex, colon resection or cholecystectomy). Should this be coded as re-admission within 30 days and if so, should it go under other?
Yes, these readmissions should be coded. The STS is interested in anytime the patient is readmitted to a hospital <= 30 days from the date of procedure irregardless if the readmission was planned or unplanned, related or unrelated. For seq# 3220, Readmit Reason there are harvest code options of "Other - Related Readmission" and "Other - Nonrelated Readmission.
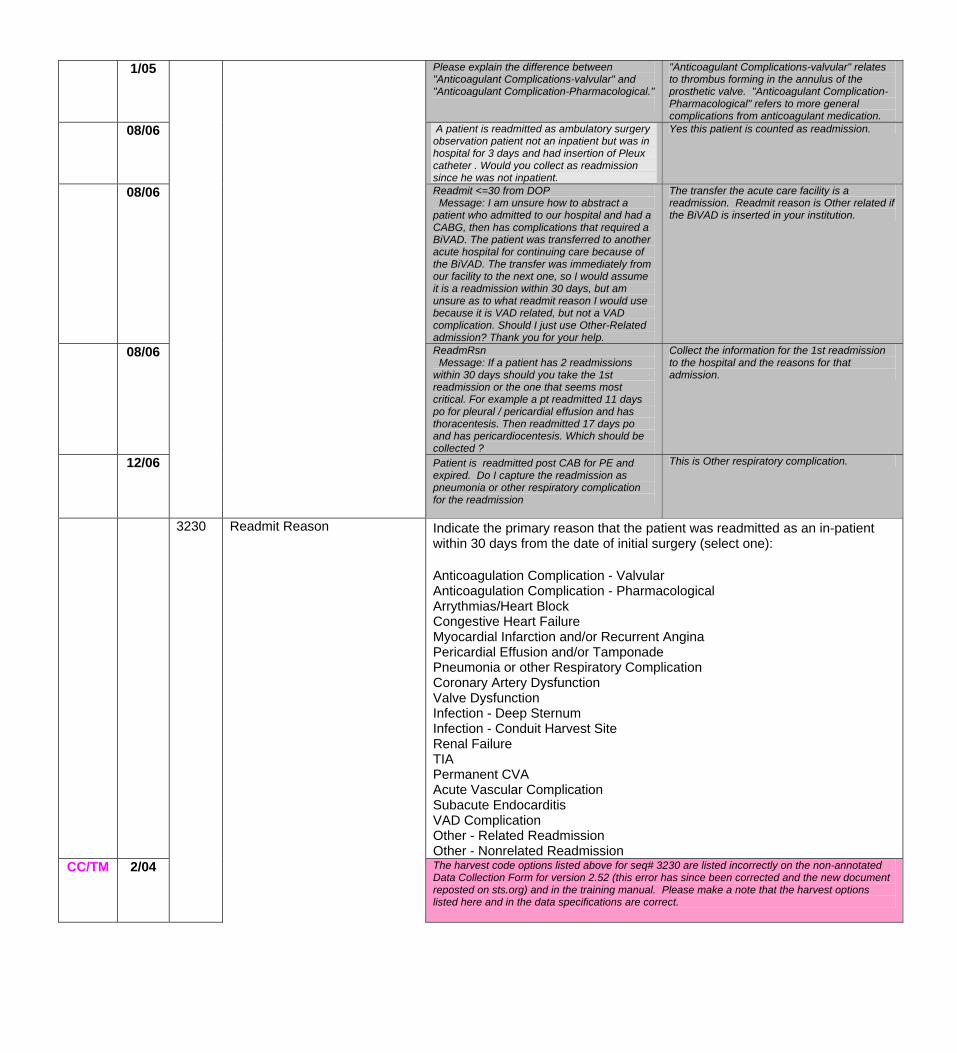
1/05 Please explain the difference between "Anticoagulant Complications-valvular" and "Anticoagulant Complication-Pharmacological."
"Anticoagulant Complications-valvular" relates to thrombus forming in the annulus of the prosthetic valve. "Anticoagulant Complication-Pharmacological" refers to more general complications from anticoagulant medication.
08/06 A patient is readmitted as ambulatory surgery observation patient not an inpatient but was in hospital for 3 days and had insertion of Pleux catheter . Would you collect as readmission since he was not inpatient.
Yes this patient is counted as readmission.
08/06 Readmit <=30 from DOP Message: I am unsure how to abstract a patient who admitted to our hospital and had a CABG, then has complications that required a BiVAD. The patient was transferred to another acute hospital for continuing care because of the BiVAD. The transfer was immediately from our facility to the next one, so I would assume it is a readmission within 30 days, but am unsure as to what readmit reason I would use because it is VAD related, but not a VAD complication. Should I just use Other-Related admission? Thank you for your help.
The transfer the acute care facility is a readmission. Readmit reason is Other related if the BiVAD is inserted in your institution.
08/06 ReadmRsn Message: If a patient has 2 readmissions within 30 days should you take the 1st readmission or the one that seems most critical. For example a pt readmitted 11 days po for pleural / pericardial effusion and has thoracentesis. Then readmitted 17 days po and has pericardiocentesis. Which should be collected ?
Collect the information for the 1st readmission to the hospital and the reasons for that admission.
12/06
Patient is readmitted post CAB for PE and expired. Do I capture the readmission as pneumonia or other respiratory complication for the readmission
This is Other respiratory complication.
Indicate the primary reason that the patient was readmitted as an in-patient within 30 days from the date of initial surgery (select one): Anticoagulation Complication - Valvular Anticoagulation Complication - Pharmacological Arrythmias/Heart Block Congestive Heart Failure Myocardial Infarction and/or Recurrent Angina Pericardial Effusion and/or Tamponade Pneumonia or other Respiratory Complication Coronary Artery Dysfunction Valve Dysfunction Infection - Deep Sternum Infection - Conduit Harvest Site Renal Failure TIA Permanent CVA Acute Vascular Complication Subacute Endocarditis VAD Complication Other - Related Readmission Other - Nonrelated Readmission
CC/TM 2/04
3230 Readmit Reason
The harvest code options listed above for seq# 3230 are listed incorrectly on the non-annotated Data Collection Form for version 2.52 (this error has since been corrected and the new document reposted on sts.org) and in the training manual. Please make a note that the harvest options listed here and in the data specifications are correct.
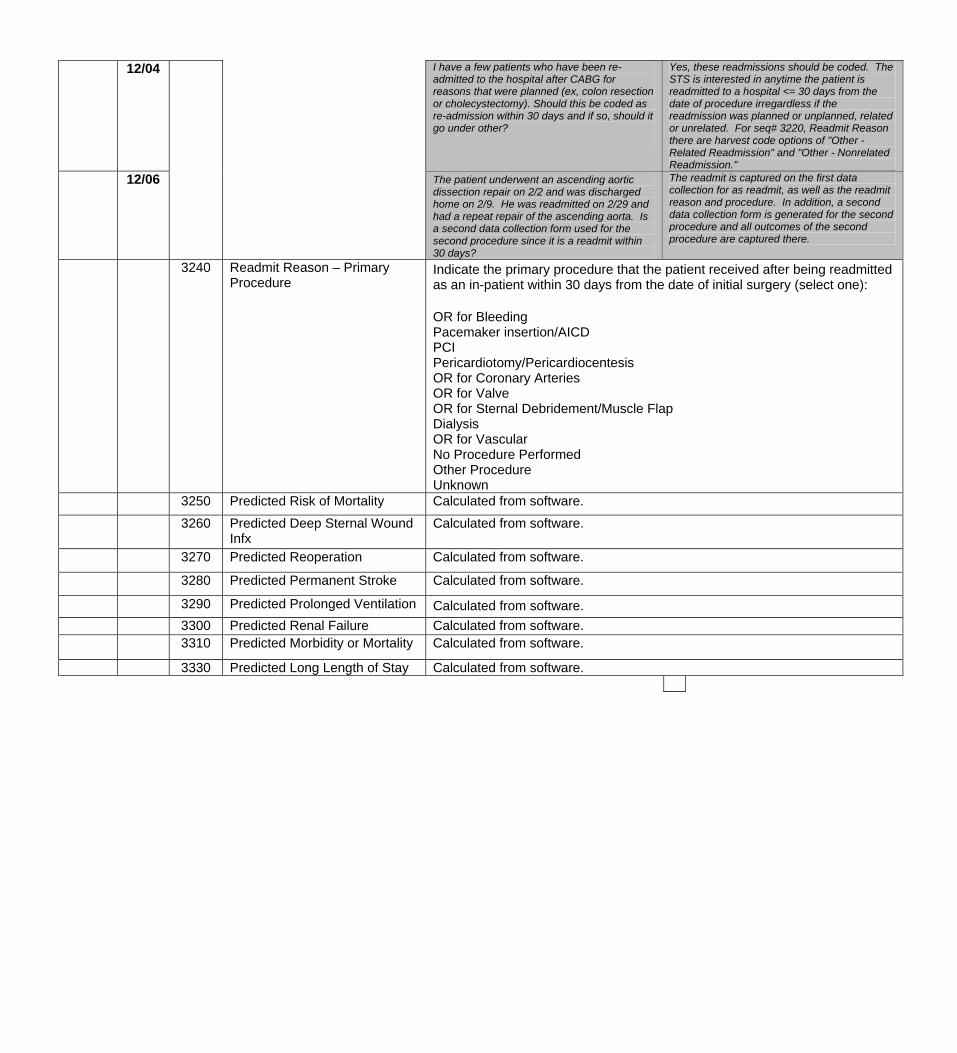
12/04 I have a few patients who have been re-admitted to the hospital after CABG for reasons that were planned (ex, colon resection or cholecystectomy). Should this be coded as re-admission within 30 days and if so, should it go under other?
Yes, these readmissions should be coded. The STS is interested in anytime the patient is readmitted to a hospital <= 30 days from the date of procedure irregardless if the readmission was planned or unplanned, related or unrelated. For seq# 3220, Readmit Reason there are harvest code options of "Other - Related Readmission" and "Other - Nonrelated Readmission."
12/06 The patient underwent an ascending aortic dissection repair on 2/2 and was discharged home on 2/9. He was readmitted on 2/29 and had a repeat repair of the ascending aorta. Is a second data collection form used for the second procedure since it is a readmit within 30 days?
The readmit is captured on the first data collection for as readmit, as well as the readmit reason and procedure. In addition, a second data collection form is generated for the second procedure and all outcomes of the second procedure are captured there.
3240 Readmit Reason – Primary Procedure
Indicate the primary procedure that the patient received after being readmitted as an in-patient within 30 days from the date of initial surgery (select one): OR for Bleeding Pacemaker insertion/AICD PCI Pericardiotomy/Pericardiocentesis OR for Coronary Arteries OR for Valve OR for Sternal Debridement/Muscle Flap Dialysis OR for Vascular No Procedure Performed Other Procedure Unknown
3250 Predicted Risk of Mortality Calculated from software.
3260 Predicted Deep Sternal Wound Infx
Calculated from software.
3270 Predicted Reoperation Calculated from software.
3280 Predicted Permanent Stroke Calculated from software.
3290 Predicted Prolonged Ventilation Calculated from software. 3300 Predicted Renal Failure Calculated from software. 3310 Predicted Morbidity or Mortality Calculated from software.
3330 Predicted Long Length of Stay Calculated from software.