Embed Size (px)
Citation preview
Cardiovascular Alterations
NUR 264Pediatrics
Angela J. Jackson, RN, MSN
Cardiovascular Alterations:Developmental Differences
Heart sounds are higher pitchedPulse rate is higherChest wall is thinner because of lack of subcutaneous tissue and muscleCardiac output is dependent on heart rate until 5 years oldSystolic murmur maybe present with fever and anemia without heart disease
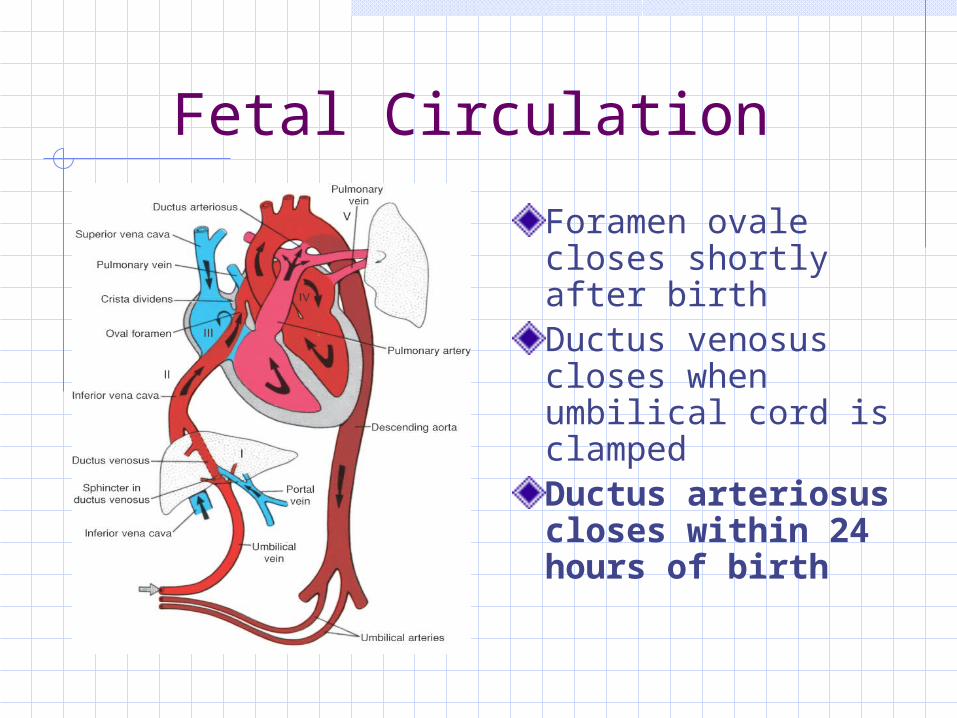
Fetal Circulation
Foramen ovale closes shortly after birthDuctus venosus closes when umbilical cord is clampedDuctus arteriosus closes within 24 hours of birth
Congenital Heart Defects:Acyanotic Disorders
Acyanotic: oxygenated blood shunts from left to right where it mixes with unoxygenated blood Atrial septal defect Ventricular septal defect Patent ductus arteriosus Atrioventricular canal Coarctation of the aorta Aortic stenosis Pulmonic stenosis
Congenital Heart Defects: Cyanotic Disorders
Cyanotic: unoxygenated blood shunts from right to left where it mixes with oxygenated blood. Blood pumped through aorta to peripheral tissues has decrease oxygen resulting in cyanosis Tetralogy of Fallot Tricuspid atresia Transposition of great arteries Truncus arteriosus Hypoplastic left heart syndrome
Congenital Heart Defects:General Clinical Manifestations
Chest enlargement or asymmetryAbnormal heart sounds: murmursAbnormal B/P readingsIncreased pulse and respirationsWeak, muffled cry in infantsPoor exercise tolerance, especially with feedingsPosturing dyspnea with activity or stressCyanosis: mucous membranes, nail beds, lips, extremities, decreased cap refill, doesn’t pink with O2 administration
Congenital Heart Defects:General Clinical Manifestations
Clubbing of fingers and toes @ 1-2 years of age in response to hypoxiaCHF: early signs – tachypnea, dyspnea, retractions, grunting, tachycardia, diaphoresis on upper lip and forehead late signs – hepatomegaly, edema. Risk of left-sided heart failure PolycythemiaPoor feeding, poor growthSquatting Frequent respiratory infections
Congenital Heart Defects:Nursing Care
Monitor vital signsProvide O2 to keep saturations at prescribed levelAdequate nutrition: Infants: small frequent feedings, burp
frequently, provide extra calories (24 calories /oz), soft nipple for bottle feeding, bottle for 20 minutes then tube feed rest of formula, feed before hungry to avoid crying.
Children: avoid empty calorie foods, well-balanced meals, healthy snacks
Congenital Heart Defects:Nursing Care
Prevent cold stressDecrease energy expenditure: plan nursing care to allow for rest, prevent cryingSkin care: decreased blood flow to peripheryMedication administration: cardiac drugs, diuretics, anticoagulants, antibiotic prophylaxisPosition: knee-chest, DO NOT interfere with squattingPrepare family and client for diagnostic studies, surgeryPromote growth and developmentTeach parents to treat child normally, use discipline, don’t overprotect
Congenital Heart Defects:Nursing Care
Cardiac Catheterization Care: Cardiac Cath may be performed to obtain
pressure gradients, O2 concentrations Pre-op: NPO 4-6 hours prior to procedure,
obtain consent, check pulse strength, educate parents/child about procedure
Post-op care: keep extremity straight, check pressure dressing on site, check pulse distal to site, NO BP on extremity, do neurovascular checks on extremity, monitor for dysrhythmias, hematoma, thrombus formation, infection. Monitor I&O as contrast medium may cause diuresis
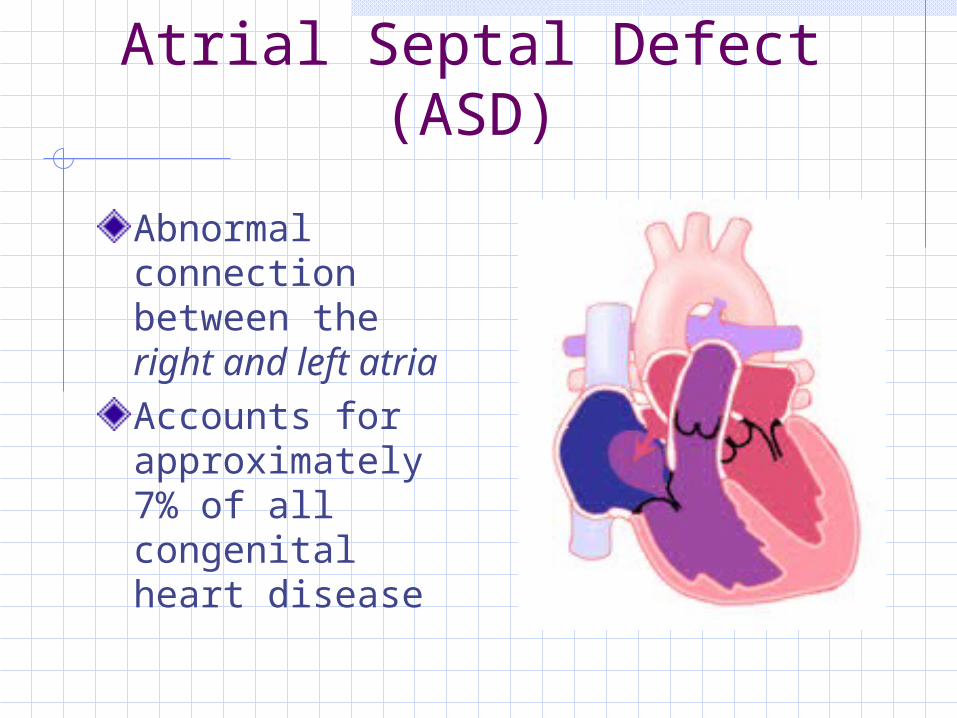
Cardiovascular Alterations:Atrial Septal Defect (ASD)
Abnormal connection between the right and left atriaAccounts for approximately 7% of all congenital heart disease
ASD: Pathophysiology
Normal increased pressure on the left side of the heart causes blood to flow from left to right through the ASDLeads to increased volume on the right side of the heartIncrease in right atrial, right ventricular and pulmonary artery size
ASD: Clinical Manifestations
Usually asymptomaticMay have a soft systolic murmur May have a widely split S2, unaffected by respiratory pattern (increased blood flow prolongs right ventricular emptying, causing a delay in pulmonic valve closure)
ASD: Diagnosis
Physical exam (detection of a murmur)Chest x-ray (increased heart size)Echocardiogram identifies the location and size of the defect
ASD: Treatment
Diuretics may be given preoperatively for symptoms of CHFThe defect may close spontaneously during the first 2 years of lifeSurgery is performed in the preschool age child Defect is stitched closed or patched Insertion of an implantable umbrella through a
large femoral vessel may also be an option Main complications of repair are atrial
arrhythmias or heart block
Ventricular Septal Defect (VSD)
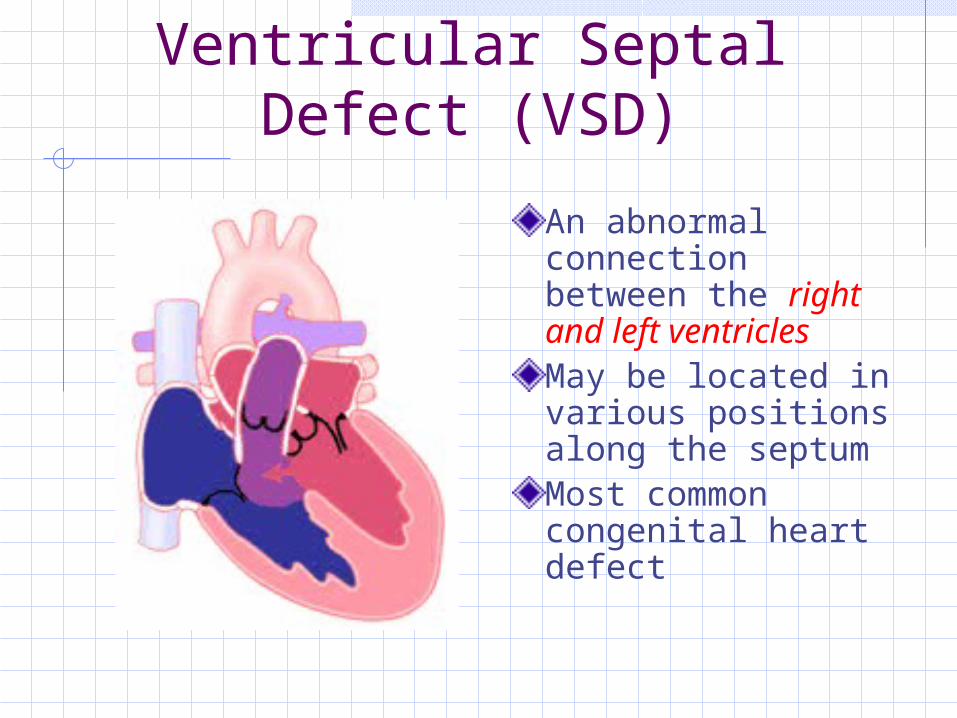
An abnormal connection between the right and left ventriclesMay be located in various positions along the septumMost common congenital heart defect
VSD: Pathophysiology
Normally increased pressure on the left side of the heart causes blood shunt from left to right through the VSDThe blood recirculates through the pulmonary artery to the lungsIncreased pulmonary blood flow leads to left heart enlargement and pulmonary venous congestionThe degree of shunting depends on the size of the defect and pulmonary resistance

VSD: Clinical Manifestations
An infant with a small VSD may be asymptomaticModerate to large defects result in CHF Tachypneic Diaphoretic Easily fatigued Underweight for age Poor feeding (tires before a feeding is
completed)
VSD: Diagnosis
Physical examLoud, harsh pansystolic murmur heard best at the left lower sternal borderChest x-ray reveals cardiomegaly with an increase in pulmonary blood flowEchocardiogram identifies the size and location of the defect
VSD: Treatment
75-80% of small VSD close in the first two years of lifeLarge defects are unlikely to close
Treated medically for first few months Digoxin and diuretics for symptoms of CHF High calorie formula for growth May need NGT feedings
Surgical repair Performed between 3 and 12 months of life Earlier in infants with failure to thrive Defect is closed with a patch of the child’s own
pericardium
Patent Ductus Arteriosus (PDA)
The ductus arteriosus remains open Incidence in preterm infants: 45%Incidence in term infants: 5-10&
PDA: Pathophysiology
Left to right shunt Blood from high pressure aorta flows
directly to low pressure pulmonary artery
Degree of shunting depends on size of defect, as well as pulmonary vascular resistanceIncreased pulmonary blood flow can contribute to CHF
PDA: Clinical Manifestations and
Diagnosis
Clinical manifestations Small PDA: asymptomatic Large PDA: signs and symptoms of
CHF
Diagnosis Continuous murmur best heard below
the left clavicle Normal chest x-ray Diagnosed with echocardiogram
PDA: Treatment
May be closed with infusion of indomethacin in preterm infantsSurgical closure in full-term, symptomatic infantsElective closure in older, asymptomatic children before age 5
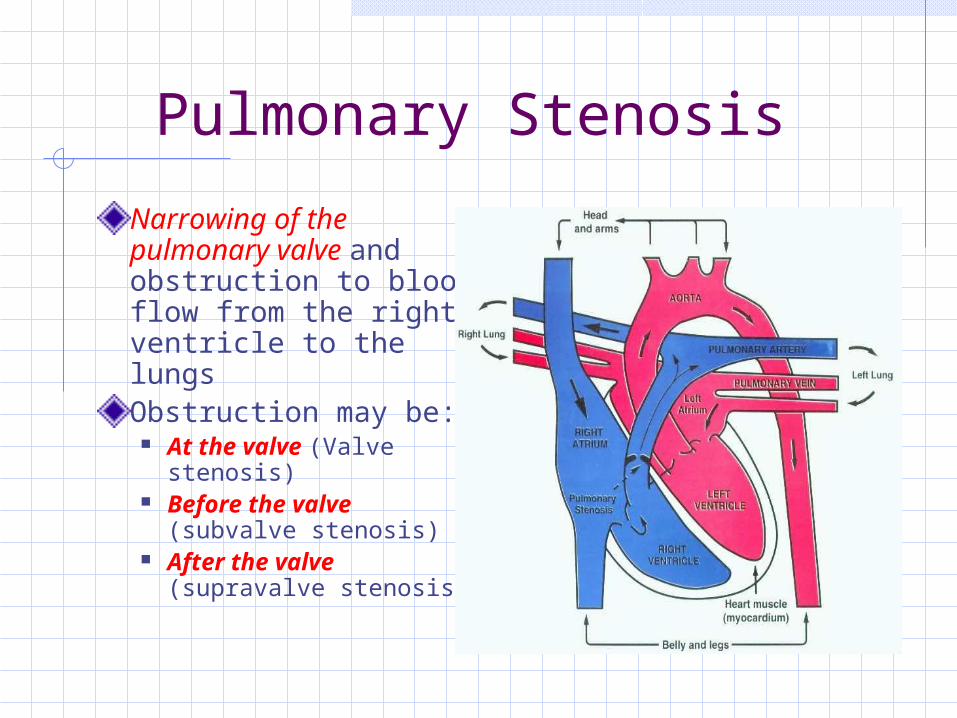
Pulmonary Stenosis
Narrowing of the pulmonary valve and obstruction to blood flow from the right ventricle to the lungsObstruction may be:
At the valve (Valve stenosis)
Before the valve (subvalve stenosis)
After the valve (supravalve stenosis)
Pulmonary Stenosis: Pathophysiology
Right ventricular pressure increases because of obstruction of blood flow from the RV to the pulmonary artery. This may result in RV failureDecreased amount of blood flow is able to get to the lungsIncreased exertion may result in cyanosis
Pulmonary Stenosis: Clinical Manifestations and
Diagnosis
Clinical Manifestations Mild to moderate PS may be asymptomatic Severe PS: dyspnea upon exertion, fatigue,
cyanosis Murmur discovered on physical exam
Diagnosis Physical exam Chest x-ray normal (severe PS may have
cardiomegaly) Echocardiogram demonstrates size and
function of RV and anatomy of pulmonary valve
Pulmonary Stenosis: Treatment
Neonates with critical PS require infusion of prostaglandins to maintain patency of the ductus arteriosus in order to provide adequate blood flow to the lungs until surgery can be performedSurgical repair Balloon valvuloplasty performed in the
cardiac catheterization lab Surgical valvotomy
Tetralogy of Fallot
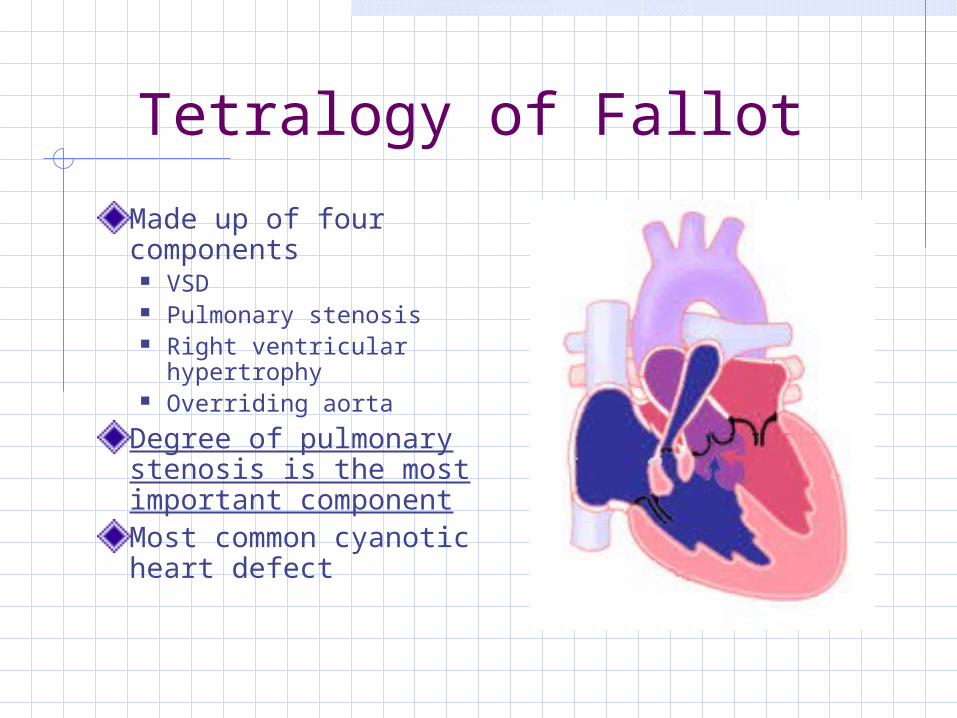
Made up of four components
VSD Pulmonary stenosis Right ventricular
hypertrophy Overriding aorta
Degree of pulmonary stenosis is the most important componentMost common cyanotic heart defect
Tetralogy of Fallot: Pathophysiology
Large VSD leads to equal pressures in right and left ventriclesAmount of pulmonary blood flow and the amount of cyanosis is dependant on the degree of pulmonary stenosis

Tetralogy of Fallot: Clinical Manifestations and
Diagnosis
Clinical Manifestations Dependant upon degree of PS, may be
mildly or profoundly cyanotic Loud systolic murmur noted at birth Hypercyanotic spells (“tet spells”) may be
brought on by crying, feeding or defecating
Diagnosis Echocardiogram Chest x-ray often normal. May exhibit boot-
shaped heart
Tetralogy of Fallot: Treatment
Preoperative management of hypercyanotic spells: Place infant in knee-chest position. (Older children will squat)
this decreases systemic venous return of unoxygenated blood and increases systemic vascular resistance, reducing right to left shunting and allowing more blood flow to the lungs
Children in the hospital may be treated with morphine to relieve symptoms of agitation and break the cycle of hyperpnea. Other treatment includes: IV fluids to decrease blood viscosity, supplemental O2, IV phenylephrine to increase systemic vascular resistance.
Infants with multiple hypercyanotic spells may need a palliative modified Blalock-Taussing (BT) shunt to assure pulmonary blood flow until complete surgical repair is performed
Tetralogy of Fallot: Treatment
Surgery: Performed between 6 and 12 months
of age The pulmonary artery is widened and
the VSD is closed If a BT shunt is in place, it is taken
down or occluded at the time of the definitive repair
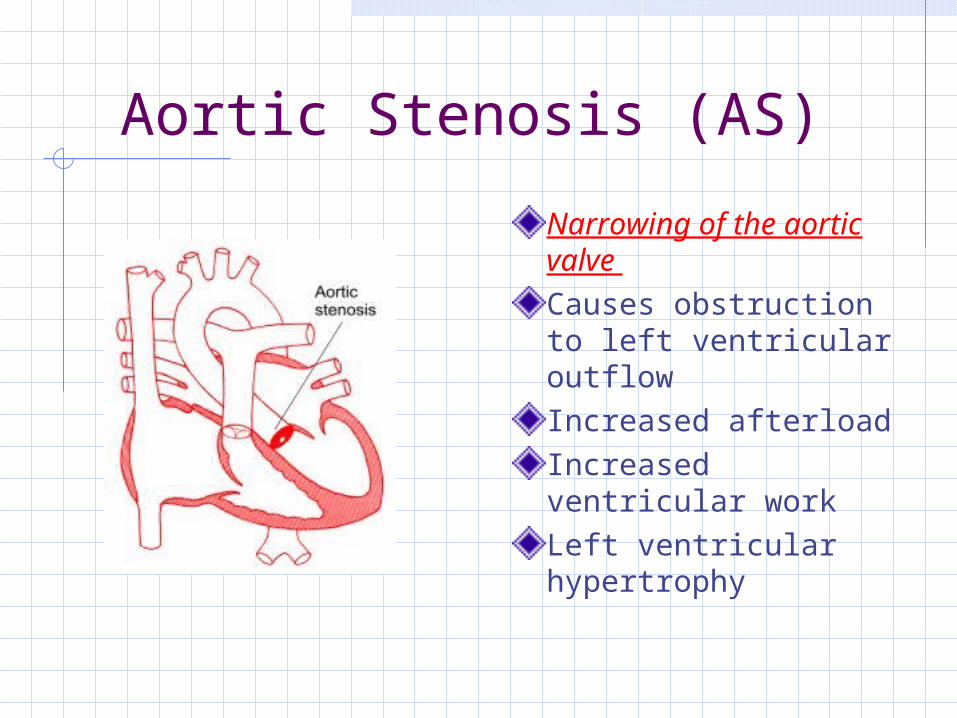
Aortic Stenosis (AS)
Narrowing of the aortic valve Causes obstruction to left ventricular outflowIncreased afterload Increased ventricular workLeft ventricular hypertrophy
AS: Clinical Manifestations and Diagnosis
Clinical Manifestations Infants usually grow normally, diagnosis made when
older child is referred for evaluation of a murmur. Older children may also have:
Exertional fatigue Dyspnea Angina Syncope with severe AS
Diagnosis Physical exam Echocardiogram LV and aorta pressure gradients (less than 25 mm
Hg are considered mild)
Aortic Stenosis: Treatment
Infants: administration of prostaglandins
to keep the ductus arteriosus open
Aortic valvotomy
Children: Balloon valvuloplasty Valve replacement

Hypoplastic Left Heart Syndrome (HLHS)
Lack of development of the left ventricle secondary to mitral valve atresia or aortic atresiaSmall, hypoplastic left ventricle not capable of any cardiac function
HLHS: Clinical Manifestations and Diagnosis
Clinical Manifestations Cyanosis develops within hours of
birth Hypotension, tachycardia, cyanosis,
tachypnea One-third will present in
cardiovascular collapseDiagnosis Physical exam Echocardiogram

HLHS: Treatment
Three treatment options No intervention Cardiac transplantation Palliative surgery
Acute Rheumatic Fever
Autoimmune reaction to an untreated or partially treated group A streptococcal pharyngitisDevelops 2-6 weeks after infectionThree organ systems affected: heart, central nervous system and the joints
Acute Rheumatic Fever:Clinical Manifestations
Valvulitis: inflammation of the heart valves – one of the most significant clinical features. New systolic murmur reflects mitral regurgitationPolyarthritis: most frequent benign major manifestation. Arthritis is migratory, there is tenderness, pain, swelling, heat and limitation of movement in the affected jointsErythema marginatum: fine, pink rash noted on the trunk and extremities, becomes more pronounced with heat. Always seen with carditis or polyarthritisSubcutaneous nodules: firm, painless nodules over the extensor surfaces of the elbows, knees and wrists. Always accompany carditis
Acute Rheumatic Fever: Diagnosis
Physical examinationLaboratory findings Elevated sed rate and C-reactive protein
(inflammation) ASO titers, anti-DNAse B (detects strep
infection)
EKGECHO: most sensitive tool for diagnosis of valvar disease
Acute Rheumatic Fever: Treatment
Penicillin for eradication of strep bacteriaAspirin as an anti-inflammatory agent Bedrest until inflammation has resolvedRepeat ECHOAntibiotic prophylaxisFrequent follow-up
Kawasaki Disease(Acute Systemic Vasculitis)
Vasculitis of multiple systems in the body, especially the coronary arteriesFirst 10 days of the disease: infiltration of vessel walls with inflammatory cells causing inflammation and hypertrophy of blood vessels. Day 10 to day 40, decrease in inflammation. Vessels have undergone destructive changes. Coronary artery aneurysm can developAfter 40 days, progressive fibrosis and healing of coronary artery abnormalities occurs. Aneurysms and dilation usually regress in one to two years
Kawasaki Disease: Clinical Manifestations
Abrupt onset of high fever lasting more than 5 daysConjunctival infection, photophobiaDiffuse red rashRed strawberry tongue, cracked red lipsHands and feet swollen, palms and soles red, tips of fingers and toes peel, progressing to palms and solesCervical lymphadenopathyTachycardia, gallop rhythm, CHFIrritabilityPainful joints, aseptic meningitis, sterile pyuria, diarrhea

Kawasaki Disease: Diagnosis
Physical examElevated WBC, sed rate, platelet countPyuriaElevated liver function testsECHO for coronary aneurysms
Kawasaki Disease: Treatment
IV immune globulin: 2gm/kg IV over 10-12 hours, may repeat with 1gm/kg)Aspirin 100mg/kg/day in 4 divided doses until fever subsides, then 3-5mg/dg daily for 6-8 weeksSolu-medrol may be used with IVIGCoumadin if aneurysms >8mmThrombolytics for vessel occlusionCoronary angioplasty, coronary artery bypass and graft or heart transplant for severe coronary artery disease
Kawasaki Disease: Nursing Considerations
VS, I%O, daily weightSupportive treatment – analgesics, fever reduction, soft foods, fluids, monitor caloriesAssess for S/S of CHFIVIG administration, monitor VS and side effectsParental involvementDischarge planning for medication administration, follow-up with cardiologist
Questions?