Embed Size (px)
Citation preview

Cardiovascular diseasesCardiovascular diseases
John C. Stevenson

Risk factors forRisk factors forcoronary heart disease (CHD)coronary heart disease (CHD)
• Genetic– Family history– Ethnic origin
• Metabolic– Diabetes mellitus– Hypertension– Obesity
• Lifestyle– Diet– Exercise– Smoking
• Socioeconomic status
• Menopause status

Prevalence of coronary vascular Prevalence of coronary vascular disease (CVD) and some risk factorsdisease (CVD) and some risk factors
USA females 2004USA females 2004
0
25
50
75
Total
CVD
CHD
Stroke
Hyper
tens
ion
Smok
ers
Hyper
chole
ster
olem
ia
Ove
rwei
ght
Obe
se
Diabe
tes
% o
f P
op
ula
tio
n
www.americanheart.org

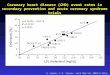
CVD and menopausal statusCVD and menopausal status
0
1
2
3
4
5
6
7
40 40–44 45–49 50–54
Age (years)
CV
D in
cid
en
ce
pe
r 1
00
0 w
om
en
Premenopausal
Postmenopausal
Adapted from the Framingham Study, DHEW No 74, 1974

CVD risk factorsCVD risk factors
• Lipids and lipoproteins
• Glucose and insulin metabolism
• Body fat distribution
• Coagulation and fibrinolysis
• Homocysteine
• Inflammatory markers
• Blood pressure
• Arterial function

Metabolic syndromeMetabolic syndrome
Insulin resistance
Central obesity
Impaired GTDyslipidemia
CoagulationHypertension
CHD

CHD: metabolic changesCHD: metabolic changes
• Lower HDL and HDL2
• Lower apolipoprotein AI
• Higher triglycerides
• Higher insulin response
• Lower insulin sensitivity
• Lower tissue plasminogen activator (tPA)
• Higher PAI-1
• Higher systolic blood pressure
• Greater android fat Ley et al. J Am Coll Cardiol 1994;23:377–83

Lipoproteins and CHDLipoproteins and CHD
• Increased total cholesterol
• Increased LDL cholesterol
• Decreased HDL and HDL2 cholesterol
• Increased triglycerides
• Increased lipoprotein(a)
• Increased small dense LDL cholesterol
• Decreased postprandial lipid clearance
• Increased LDL oxidation

Menopause and lipidsMenopause and lipids
-30 -20 -10 0 10 20 30
% Change
Cholesterol
Triglycerides
LDL
HDL
HDL2
HDL3
Apo B
Apo AI
Lipoprotein(a)
Stevenson et al. Atherosclerosis 1993;98:83–90

Glucose/insulin and CHDGlucose/insulin and CHD
• Impaired glucose tolerance
• Hyperinsulinemia
• Increased insulin response to glucose
• Increased insulin resistance
• Increased uric acid

Insulin metabolismInsulin metabolism
*
*
Menopause Menopause
*p < 0.001
Incremental pancreatic Insulin secretion
Insulin half-life
Walton, et al. Eur J Clin Invest 1993;23:466–73
0
0.5
1
1.5
2
2.5
Pre Post
nm
ol/m
l.min
0
2
4
6
8
10
12
Pre Post
min

Glucose Insulin C-peptide
r = 0.20 r = 0.49 r = 0.28
Menopausal age ns p < 0.05 ns
Chronological age ns ns ns
Body mass index ns p < 0.001 ns
Insulin metabolismInsulin metabolism
0
1
2
3
4
5
< 50 < 55 > 55
Age range (years)
Si (
μU
.ml-
1)
Insulin sensitivity
IVGTT incremental areas
Walton, et al. Eur J Clin Invest 1993;23:466–73; Proudler, et al. Clin Sci 1992;83:489–94

Seige K, et al. 6th Symposium of the German Endocrinological Society: Modern Developments in Progestagenic Hormones in Veterinary Medicine; 1959, 1960; Kiel: Springer Verlag; 1959. p. 274–9
Menopause and diabetesMenopause and diabetes
Nu
mb
er o
f w
om
en n
ewly
d
iag
no
sed
wit
h d
iab
etes
Years from menopause
Premenopause Postmenopause120
100
80
60
40
20
0 -10 -8 -6 -4 -2 0 2 4 6 8 10 12 14 16

Body compositionBody composition
30
40
50
60
Pre Post
% A
nd
roid
fa
t
30
40
50
60
Pre Post
% G
yn
oid
fa
t
Menopause Menopause
* *
*p < 0.001Ley, et al. Am J Clin Nutr 1992;55:950–54

Menopause and hemostasisMenopause and hemostasis
• Increased fibrinogen
• Increased factor VII
• Increased plasminogen activator inhibitor-1 (PAI-1)
• Increased antithrombin
• ? Increased protein C
• Increased tissue plasminogen activator (tPA)
Bonithon-Kopp, et al. Int J Epidemiol 1990;19:42–8; Heinrich, et al. Clin Chem 1991;37:1950–4

Endothelial functionEndothelial function
Menopausal
Flow-mediated dilatation (FMD)
*p < 0.01Arrowood, et al. Circulation 2000;A514
0
2
4
6
8
10
12
Pre Post
%In
cre
as
e in
FM
D
*

CHD assessmentsCHD assessments
• Ischemia– Exercise ECG– Stress thallium scan
• Imaging– Coronary angiography– Multi-slice CT scanning– MRI scanning– Ultrasound IMT
• Risk factors– Fasting lipids/lipoproteins– Fasting glucose/insulin– C-reactive protein– Homocysteine

CHD preventionCHD prevention
• Lipid-lowering drugs
• Antihypertensives
• Weight reduction
• Physical activity
• Smoking cessation
• ? HRT

HRT and CHDHRT and CHD
• Lipids and lipoproteins
• Glucose and insulin metabolism
• Body fat distribution
• Coagulation and fibrinolysis
• Homocysteine
• Inflammatory markers
• Blood pressure
• Arterial function

Epidemiology: CHD and HRT Epidemiology: CHD and HRT
21.510.50
RR
Hospital case-control
Population case-control
Prospective internal control
Cross-sectional
Prospective external control
All studies combined
Prospective internal control
and cross-sectional
Stampfer and Grodstein. Raven Press, 1994

HRT and CHDHRT and CHD
• HRT is beneficial to CVS– Primary prevention– Secondary prevention
• Women start HRT around menopause
• Studies are not randomized– Healthy user bias (applies
to other outcomes, e.g. osteoporosis)
– Data can be adjusted for potential biases
• HRT is not beneficial to CVS– Primary prevention– Secondary prevention
• Women start HRT at later ages
• Problem lies with HRT– Dose and type of
estrogen– Dose and type of
progestogen– Harm is due to increased
thrombogenesis– Harm is due to adverse
vascular remodelling
Observational studies Randomized trials

Adapted from Grodstein F, et al. J Women’s Health 2006;15:35–44
Postmenopausal hormone use and CHDPostmenopausal hormone use and CHDNurses Health Study 1976-2000Nurses Health Study 1976-2000
Timing of hormone initiation with respect to ageTiming of hormone initiation with respect to age
Adjusted for age, body mass index, hypercholesterolemia, hypertension, parental coronary heart disease, diabetes, cigarette smoking, dietary data, husband’s education, alcohol intake, physical activity, vitamin E or multivitamin supplementation, aspirin use
50–59 years
60+ years
RR (95% CI)
0 0.2 0.4 0.6 0.6 1.0 1.2 1.2
Excluding postmenopausal women with prevalent CHDExcluding postmenopausal women with prevalent CHD

IMS Position Statement, Climacteric 2004;7:333–7
Effect of HRT-ERT on CHD in PMWEffect of HRT-ERT on CHD in PMWTiming of initiation, data from WHITiming of initiation, data from WHI
CEE
CEE + MPA
Haz
ard
ra
tio
s
Yea
rs s
ince
men
op
aus
e
< 10
10–19
> 20
< 10
10–19
> 20
0.56
0.92
1.04
0.89
1.22
1.71
0 0.5 1.0 1.5 2.0 2.5
0 0.5 1.0 1.5 2.0 2.5
Hazard ratio(95% CI)
Hazard ratio(95% CI)
LEVEL 1

Hsia J, et al. Arch Intern Med 2006;166:357–65
WHI: coronary events withWHI: coronary events withET or placebo by age at baselineET or placebo by age at baseline
Hazard ratio (95% CI)
Coronary event
CHD (MI or coronary death)
CABG or PCI
MI, coronary death CABG, and PCI
MI, coronary death CABG, PCI and
confirmed angina
0 0.5 1 1.5 2
p = 0.07
p = 0.09
p = 0.09
p = 0.11
50–5960–6970–79

WHI: coronary heart diseaseWHI: coronary heart diseaseHRT and CHD: absolute risk by ageHRT and CHD: absolute risk by age
p-value for trend = 0.16n = 27,347
Taken from Rossouw, et al. J Am Med Assoc 2007;297:1465–77
-2-1
19
-10-8-6-4-202468
101214161820
Age at randomisation (years)
Ab
so
lute
ex
ce
ss
ris
k o
f C
HD
pe
r 1
00
00
pe
rso
n-y
ea
rs
50–59 60–69 70–79

Adapted from Rossouw, et al. J Am Med Assoc 2007;297:1465–77
WHI: HT and WHI: HT and absolute riskabsolute risk of cardiovascular of cardiovascular disease by disease by years since menopauseyears since menopause
Years since menopause Hazard ratio CI Absolute excess risk
(per 10,000person-years)
< 10 0.76 0.50–1.16 –6
10–19 1.10 0.84–1.45 4
> 20 1.28 1.03–1.58 17
p for trend = 0.02

ERT and atheroma preventionERT and atheroma prevention
• 222 healthy postmenopausal women
• 17β-estradiol 1 mg daily vs. placebo
• Study duration 2 years
• Carotid artery intima-media thickness by ultrasound scan
0
0.002
0.004
mm
/ye
ar
Placebo
ERT
I/M thickness
Progression
Hodis, et al. Ann Intern Med 2001;135:939–53

ERA studyERA study
-0.12
-0.07
Ch
an
ge
in M
LD
(m
m)
Placebo
CEE
CE-MPA
Progression
p = NSHerrington DM, et al. N Engl J Med 2000

HRT and CHD eventsHRT and CHD events
• Increased CHD events in elderly women– ? Increased
thrombogenesis/adverse remodelling
– ? Estrogen dose too high
MI / death
CABG / PCI
0 21
50–59 years
70–79 years
HR
composite
Hsai, et al. Arch Intern Med 2006;166:357–65

Estradiol and myocardial ichemiaEstradiol and myocardial ichemia
0
200
400
600
800
0
200
400
600
800
Tim
e (s
ec)
Time to 1 mm ST depression
Total exercise time
Placebo Estradiol Placebo Estradiol
*p = 0.01; **p < 0.01 Rosano, et al. Lancet 1993;342:133–6
*
**
Tim
e (s
ec)

CHD treatmentCHD treatment
• Anti-anginal drugs
• Statins
• Angioplasty + stenting
• CABG
• ? HRT

HERS trialHERS trial
• 2763 women
• Mean age 66.7 years
• > 6 months from cardiac event
• Conjugated equine estrogens 0.625 mg + MPA 2.5 mg
• Event rate 3.3%(estimated 5%)
• Mean follow-up 4.1 years (estimated 4.75 years)
• No overall benefit seen
0
0.4
0.8
1.2
1.6
0 1 2 3 4
Years
RH
CHD events
Trend p = 0.009
Hulley, et al. J Am Med Assoc 1998;260:605–13

HERS trialHERS trial
2
2.5
3
3.5
4
4.5
5
1 2 3 4
Ca
rdio
va
sc
ula
r e
ve
nts
(%
)
Placebo
HRT
Hulley, et al. J Am Med Assoc 1998;260:605–13

WHISPWHISP
• 100 postmenopausal women followed up to 12 months
• Acute coronary syndrome (majority MI)
• Randomized to placebo or HRT 2–28 days post-event
• 17β-estradiol 1 mg/NETA 0.5 mg daily
• Efficacy– Lipid parameters– (Clinical events)
• Safety– Hemostatic parameters
0
5
10
15
20
25
30
35
40
45
CVA
Death M
I
CVA/dea
th/M
I
CV adm
issio
n
Ev
en
t ra
te (
%)
HRT
Placebo
RH 0.68 (CI 0.32–1.46)
Collins, et al. Eur Heart J 2006;27:2046–53

Time
Premenopausal years Postmenopausal years
OvariectomyPlaque area
(% of placebo)
Healthy diet CEE + atherogenic diet1.1. 70%1,2
Atherogenic diet CEE + atherogenic diet2.2. 50%3
Healthy diet Atherogenic diet
Healthy diet+ CEE3.3. 0%4
~ 6-year human equivalent
Timing of HRT interventionTiming of HRT interventionEffect of estrogens on atherogenesis
in non-human primates
1Clarkson, et al. J Clin Endocrinol Metab 1998;83:721; 2Adams, et al. Arterioscler Thromb Vase Biol 1997;17:217; 3Clarkson, et al. J Clin Endocrinol Metab 2001;86:41; 4Williams, et al. Arterioscler Thromb
Vase Biol 1995;15:827

The window of opportunity: The window of opportunity: hypothetical pathogenetic sequencehypothetical pathogenetic sequence

Age distribution in WHI population and Age distribution in WHI population and stage of atherosclerosis progressionstage of atherosclerosis progression
0% 10% 20% 45% 25%
< 50 yrs 50–54 yrs 55–59 yrs 60–69 yrs 70–79 yrs
Endothelial dysfunction
Foam Fatty Intermendiate Atheroma Fibrous Complicatedcells streak lesion plaque lesion/rupture
HRTObs. Studies
Clinical practice HT
RCT
WHIMS
35–45 yrs 45–55 yrs 55–65yrs > 65 yrs
Endothelial injury Lipid accumulation Inflammation
Estrogens’ preventive action requires healthy tissue

Conclusions: generalConclusions: general
• CVD is major cause of death in women
• Similar risk factors for males and females
• Menopause gives additional risk
• Prevention and treatment similar for males and females
• HRT potentially gives additional benefit

Conclusions: HRTConclusions: HRT• Biological plausibility for beneficial CVD effects of HRT
– Metabolic processes– Arterial function
• Clinical studies– Benefit for myocardial ischemia– Benefit for atheroma prevention in healthy women
• Population studies– Concordance of benefit in primary prevention– Event studies suggest benefit for secondary prevention
• Randomized clinical trials– Early harm followed by later benefit– More benefit seen in younger women – ? therapeutic window
of opportunity– More benefit seen with lower dose ± different/no progestogen

HRT and CHD:HRT and CHD:MisperceptionsMisperceptions
• HRT increases CHD risk throughout the whole postmenopausal period
• HRT causes an increase in coronary events in the first 1–2 years in all women
IMS Global Summit 2008. Climacteric 2008;11:267–72

HRT and CHD:HRT and CHD:EvidenceEvidence
• HRT in women aged 50–59 years does not increase CHD risk in healthy women and may even decrease the risk in this age group
• Estrogen-alone therapy in the age group 50–59 years was associated with significantly less coronary calcification (equivalent to a smaller plaque burden), which is consistent with findings of a lower coronary intervention score in women of this age in the WHI study
IMS Global Summit 2008. Climacteric 2008;11:267–72

HRT and CHD:HRT and CHD:EvidenceEvidence
• Early harm (more coronary events during the first 2 years of HRT) was not observed in the early postmenopausal period. The number of CHD events decreased with duration of HRT in both WHI clinical trials
• Data derived from randomized controlled trials in the age group 50–59 years are similar to the older observational data, suggesting a protective effect of HRT on coronary disease
IMS Global Summit 2008. Climacteric 2008;11:267–72

HRT and CHD:HRT and CHD:EvidenceEvidence
• Late starters of standard-dose HRT may have a transient, slightly increased risk for coronary events
IMS Global Summit 2008. Climacteric 2008;11:267–72