Embed Size (px)
Citation preview
CARDIOVASCULAR
EVALUATION UNIT
Presentation
by Laurie Lambert, PhD
November 28, 2016
MULTIDISCIPLINARY TEAM
Coordinator and
administrative support
DSSET Director
Scientific Professionnals
Medical/ Scientific Advisor
Web site Programmer
DSSET Scientific Advisor
Economist
Graphic Artist
Medical Archivists
Biostatistician

Our goal is to help the health care system provide equal
access to high quality and timely care to the population
of Québec.
Literature review
Field evaluation
Quality standards
Support improvement
EVALUATION FRAMEWORK
ST-Segment Elevation Myocardial Infarction
(STEMI)
5
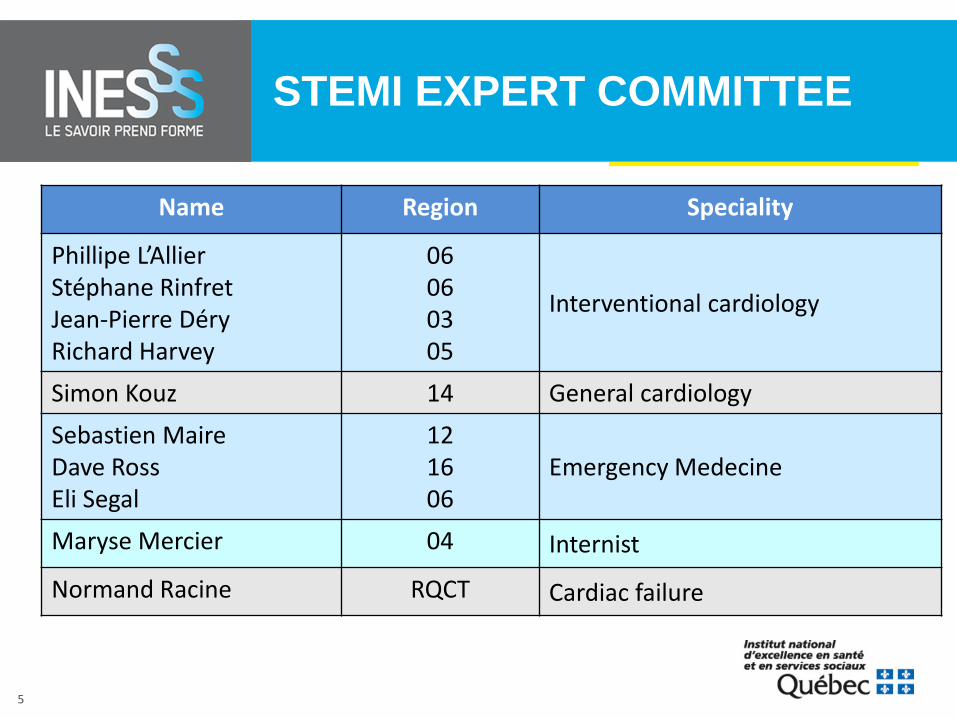
STEMI EXPERT COMMITTEE
Name Region Speciality
Phillipe L’Allier Stéphane Rinfret Jean-Pierre Déry Richard Harvey
06 06 03 05
Interventional cardiology
Simon Kouz 14 General cardiology Sebastien Maire Dave Ross Eli Segal
12 16 06
Emergency Medecine
Maryse Mercier 04 Internist
Normand Racine RQCT Cardiac failure
6
PREVIOUS SCIENTIFIC PRODUCTS
• Comparison of efficacy, effectiveness and safety of fibrinolysis and PPCI for care of STEMI (2008)
• Care of STEMI : Systematic review of organizational and economics Issues (2008)
• Province-wide field evaluations (2006-7 ; 2008-9)
*UECT: Unité d’évaluation en cardiologie tertiaire
7
ACTIONS TO SUPPORT CHANGE
• Ministerial Action Plan on continuum care for patients with STEMI;
• Individualized results by region and by center ;
• Oral presentations by INESSS with ministerial representatives in many regions across Québec
• Creation of interdisciplinary committees within various hospitals or regions with a goal of improving of processes of care
8
RE-EVALUATE
• Update of literature review
• Establishment of quality standards
• Third field evaluation – 83 Hospitals across Québec ; – Standardized and objective review of medical charts by
UECV’s medical archivists ; – Centralized website with automatic data checks – Linkage with medicoadministrative data in order
to measure short and long term clinical results
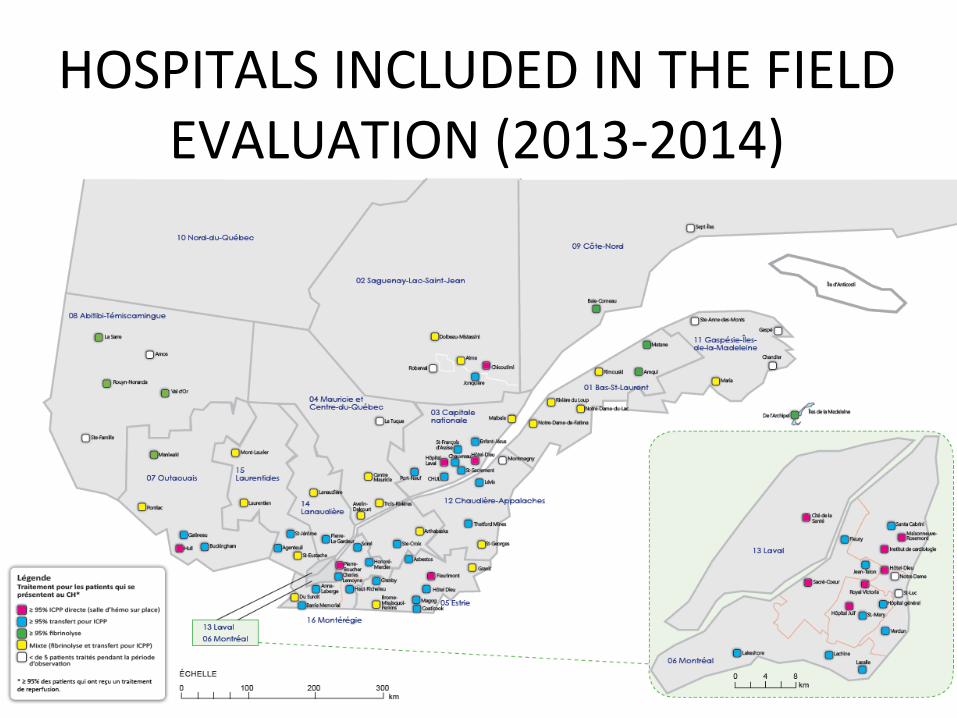
HOSPITALS INCLUDED IN THE FIELD EVALUATION (2013-2014)

PPCI WITH DIRECT ADMISSION: DELAY (MINUTES) FIRST MEDICAL CONTACT TO DEVICE BY REGION
79 7981
8487 88 88
91 91
9598
50
60
70
80
90
100
110
120
130
14 16 12 02 QC 05 07 03 15 06 13
% ≤90 min for all Québec ETIAMEST I/II = 42 % ETIAMEST III = 54 %
n 56 140 29 30 768 67 51 99 30 202 57

PPCI WITH DIRECT ADMISSION: IMPACT OF PREHOSPITAL CARE ON DELAY FROM DOOR TO DEVICE
79
70
52
33
24
10
30
50
70
90
110
Sans ambulance Ambulance sansECGPh
Ambulance avecECGPh et ECG
intrahospitalier
Ambulance avecECGPh, sans ECG
intrahospitalier etdirigés en salle
d'urgence
Ambulance avecECGPh, sans ECG
intrahospitalier etdirigés directementen Hémodynamie
High degree of interdependance between various systems involved in the process of care:
• Prehospitalier • Emergency room • Cath lab
n=116 n=37 n=471 n=62 n=81

STEPS TO SUPPORT IMPROVEMENT ?
• How can we support collaborative change ?
• How can we engage and assist stakeholders to achieve the established quality standards ? – individual feedback
– tool kit
– site visits / audit ?
– public reporting ?
LEFT VENTRICULAR ASSIST DEVICES
LVAD
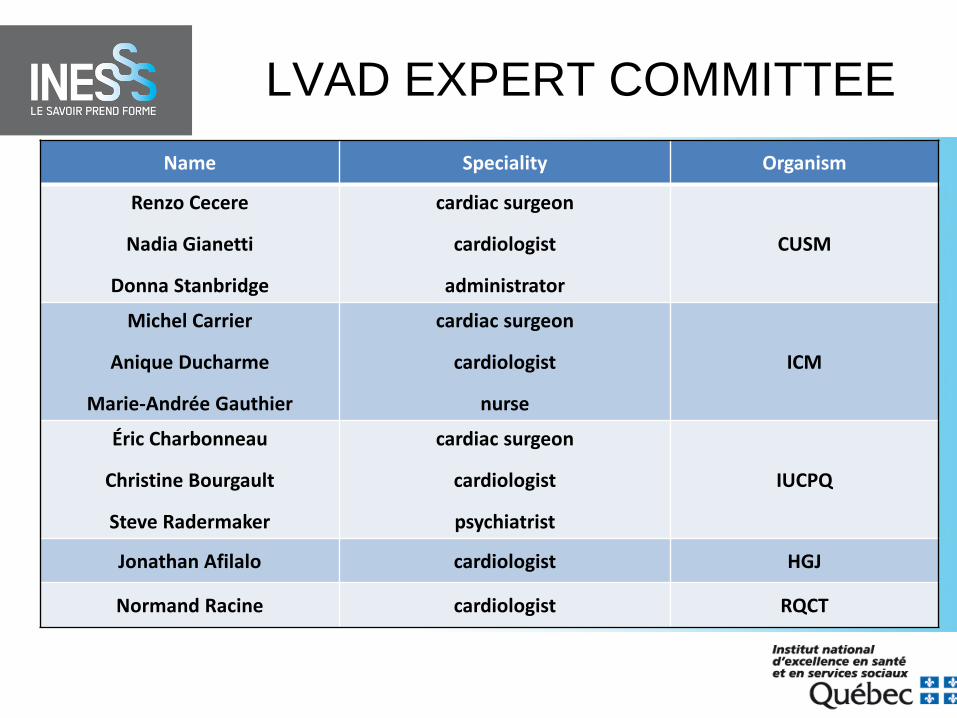
LVAD EXPERT COMMITTEE Name Speciality Organism
Renzo Cecere
Nadia Gianetti
Donna Stanbridge
cardiac surgeon
cardiologist
administrator
CUSM
Michel Carrier
Anique Ducharme
Marie-Andrée Gauthier
cardiac surgeon
cardiologist
nurse
ICM
Éric Charbonneau
Christine Bourgault
Steve Radermaker
cardiac surgeon
cardiologist
psychiatrist
IUCPQ
Jonathan Afilalo cardiologist HGJ
Normand Racine cardiologist RQCT

16
RECOMMENDATIONS
• being eligible for a heart transplant should not be an essential criterion for patient selection
• LVAD should be offered to those patients who are the most likely to benefit in terms of survival and quality of life
• clear and applicable selection criteria should be established and applied uniformly across the centers
• a mandatory provincial registry of LVAD should be created to : – monitor patient selection and clinical outcomes – to aid decision-making concerning the organization of care
FIELD EVALUATION

Treatment strategy according to INTERMACS definitions
Quebec (2013-2015)
N=53 %
INTERMACS (2012-2015)
N= 10436 %
BTT Bridge to transplant 34.0 25.9
BTC Bridge to candidacy - Likely 30.1 17.2
BTC Bridge to candidacy - Moderate 11.3 8.9
BTC Bridge to candidacy - Unlikely 3.8 2.6
DT Destination therapy 15.1 44.3
RT Rescue therapy 3.8 0.4
BTR Bridge to recovery 1.9 0.3

QUALITY STANDARDS
Literature review
Field evaluation
Quality standards
Support improvement
-Development of QI -Toolkit -Site visits -Shared-decision making ?
Transcatheter Aortic Valve Implantation
(TAVI)
TAVI ADVISORY COMMITTEE
Cardiac surgeons Interventional cardiologists
Michel Carrier (ICM) Benoit Daneault (CHUS)
Yoan Lamarche (HSCM/ICM) Réda Ibrahim (ICM)
Benoit de Varennes (CUSM) Philippe Généreux (HSCM)
Éric Dumont (IUCPQ) Giuseppe Martucci (CUSM)
General Cardiologists Josep Rodés-Cabau (IUCPQ)
Jonathan Afilalo (HGJ) Anita Asgar (ICM)
Normand Racine (RQCT) Brian Potter (CHUM)
Geriatrician Nicolo Piazza (CUSM)
Jean-Pierre Beauchemin (IUCPQ)

FIELD EVALUATION

MORTALITY : QUEBEC (2013-2014) VS NATIONAL REGISTRY DATA
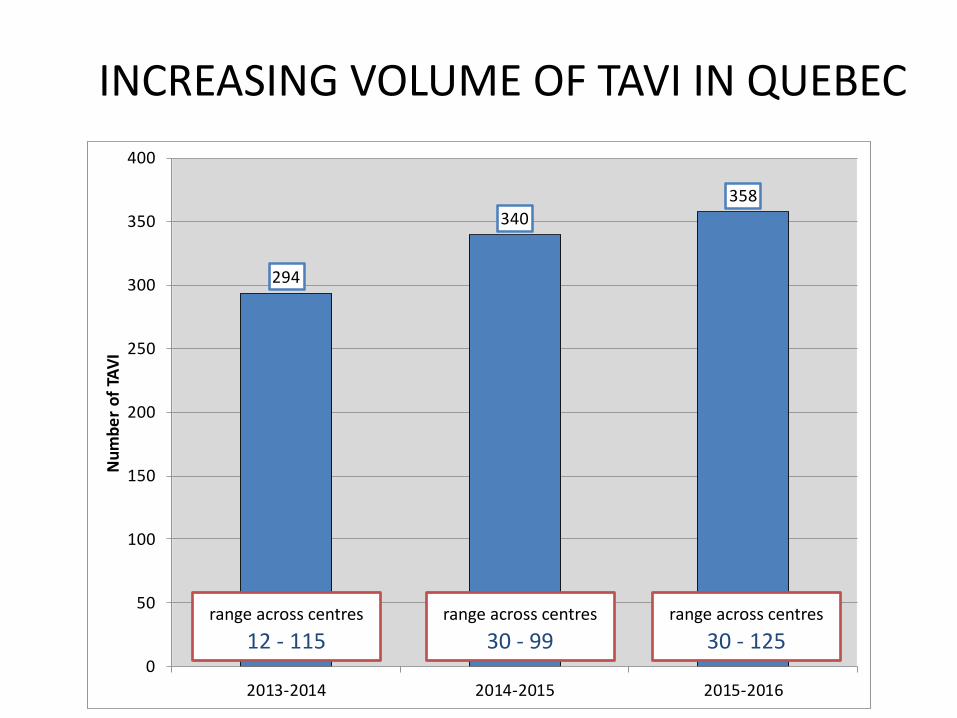
INCREASING VOLUME OF TAVI IN QUEBEC
294
340358
0
50
100
150
200
250
300
350
400
2013-2014 2014-2015 2015-2016
Num
ber o
f TAV
I
range across centres 12 - 115
range across centres 30 - 99
range across centres 30 - 125
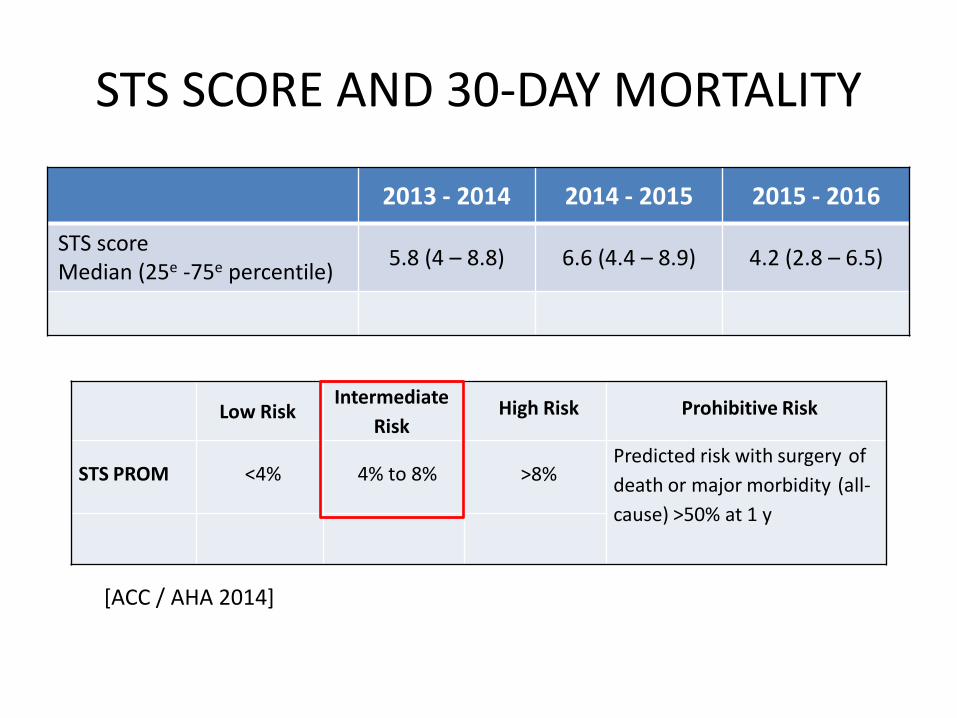
STS SCORE AND 30-DAY MORTALITY
2013 - 2014 2014 - 2015 2015 - 2016
STS score Median (25e -75e percentile) 5.8 (4 – 8.8) 6.6 (4.4 – 8.9) 4.2 (2.8 – 6.5)
Low Risk
Intermediate Risk
High Risk Prohibitive Risk
STS PROM
<4%
4% to 8%
>8% Predicted risk with surgery of death or major morbidity (all-cause) >50% at 1 y
[ACC / AHA 2014]
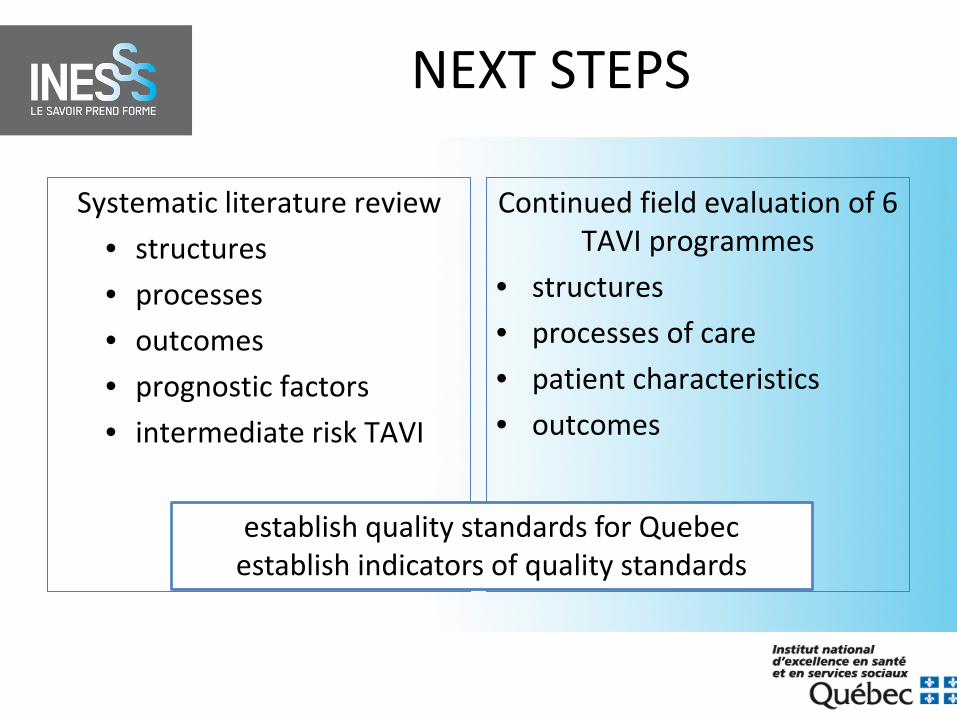
NEXT STEPS
Systematic literature review • structures • processes • outcomes • prognostic factors • intermediate risk TAVI
Continued field evaluation of 6 TAVI programmes
• structures • processes of care • patient characteristics • outcomes
establish quality standards for Quebec establish indicators of quality standards
29
THROMBECTOMY
Literature review
Field evaluation
Quality standards
Support improvement
• Characteristics of patients • Processes of care • Clinical outcomes
Impact of a new technology on the system of care for ischemic stroke ?
IMPLANTABLE CARDIAC DEFIBRILLATORS
(ICD)

ICD ADVISORY COMMITTEE
Name Speciality Organism
François Philippon Electrophysiologist IUCPQ
Marc Dubuc Electrophysiologist ICM
Vidal Essebag Electrophysiologist CUSM
Felix-Alejandro Ayala-Paredes Electrophysiologist CHUS
Paolo Costi Electrophysiologist CHUM
Miguel Barrero-Garcia Cardiologist Trois-Rivières
Dominique Grandmont Cardiologist Hôpital de St-Hyacinthe
Paul Farand Cardiologist /administration CHUS
Christine Villemaire ICD Technician ICM
Marianne Dompierre Nurse – coordinator ICM
Marie-Andrée Gauthier Nurse – informed decision Hôpital Lasalle
Normand Racine Cardiologist – heart failure RQCT
WHAT IS THE QUESTION ?
“…. estimating the ICD benefit through risk scores promotes honest communication and evidence-based decision making between patients and physicians to achieve the most appropriate therapy that is consistent with the patient’s values and preferences regarding their quantity and quality of life.” CCS Guidelines 2016
CHOICE OF ICD THERAPY REPLACEMENT? UPGRADE? DEACTIVATION?
• Systematical literature review
• Field evaluation – Characteristics of patients – Processes of care – Clinical outcomes
• Creation of patient committee to integrate the patient perspective
ANALYSIS OF MEDICOADMINISTRATIVE DATA
Siège social : 1195, avenue Lavigerie 1er étage, bureau 60 Québec (Québec) G1V 4N3
Bureau de Montréal : 2021, avenue Union bureau 10,083 Montréal (Québec) H3A 2S9
Questions?
Institut national d’excellence en santé et en services sociaux