Embed Size (px)
Citation preview

CARE & HEALTH . APPLICATION FORM 2
@@@
CARE & HEALTH
Application Form
CARE & HEALTH . APPLICATION FORM 1
Last name ______________________________________ First name ________________________________
Date of birth ___ / ____ / ________ (dd/mm/yyyy) Nationality ______________________ Gender (M/F) ________
Residential address(1)______________________________ _________________________________________
City _________________________ Country ______________________ Postcode _____________________
Mailing address (if different from above) ____________________________________________________________
City _________________________ Country _______________________ Postcode _____________________
Phone number ____________________ Mobile(2) ______________ E-mail(2) ____________________________
Occupation _______________________________________________________________________________
______________ _____________ _______________ ___ / ____ /_____ _________ ______________
______________ _____________ _______________ ___ / ____ /_____ _________ ______________
______________ _____________ _______________ ___ / ____ /_____ _________ ______________
______________ _____________ _______________ ___ / ____ /_____ _________ ______________
(1) Any country in which you and your dependants will reside for at least 6 months of the year is called Country of Usual Residence. (2)We can send you confirmation by SMS of any hospital guarantee we issue if you provide us with your mobile phone number. An email address, however, must be provided as we will send invoices and claim statements by email.
How would you like to pay your premium?
Annually Semi-annually Quarterly
(Semi-annual and Quarterly premiums are subject to a 3% loading)
Select your method of payment:
Visa / MasterCard
Bank Transfer
When would you like your cover to start?
______ / _____ / _______
Your membership and that of your dependants are effective on the date indicated on your Certificate of Enrollment, and at the earliest on the day after we receive the Application Form and Health Declaration Form duly filled and signed, along with all requested additional information, subject to approval by HENNER - GMC Medical Advisory Board and payment of first premium.
Your details
Dependants to be included in the plan
Relationship (eg: Spouse, Child)
Last name First name Date of birth (dd/mm/yyyy)
Gender (M/F)
Country of Usual
Residence(1)
Payment
(For payment by credit card, upon receipt of your invoice, go to www.henner.com, log into your secure personal access page and register your credit card details online)
(Account details for transfer will be provided with your invoice)
Effective date of coverage
dd mm yyyy

CARE & HEALTH . APPLICATION FORM 2
Choose your Area of Coverage
Area 1 Area 2 Area 3 Area 4 Area 5
Choose your Plan
Primary Vitality Serenity Prestige
1 Choose your Maximum Annual Limit:
US$ 200,000 US$ 300,000
US$ 500,000 US$ 4,500,000
2 Choose your level of coverage for Outpatient benefits: (it will also apply to Maternity, Dental & Vision of chosen)
80% of usual 90% of usual 100% of usual benefits benefits benefits
Choose your Options
Maternity
Dental
Vision
Choose your Life Insurance
Death (all causes) or Permanent Total Disability
Select your lump sum benefit:
US$ 25,000 US$ 50,000 US$ 100,000 US$ 250 000 Optional double benefit when death is caused by accident
(1)
Brazil, Hong Kong, Mainland China, Switzerland + countries in areas 2, 3, 4, and 5.
Argentina, Australia, Belarus, Bosnia, Canada, Colombia, Ireland, Israel, Italy, Japan, Macao, Mexico, Monaco, Russia, Singapore, South Korea, Spain, United Kingdom, Venezuela + countries in areas 3,4,and 5.
Belgium, Chile, Denmark, Finland, France, Germany, Greece, Hungary, Iceland, New Caledonia, New Zealand, Portugal, South Africa, Sweden, Rest of Latin America, Rest of Europe + countries in areas 4,and 5.
Bahrain, Egypt, Iran, Iraq, Jordan, Kuwait, Lebanon, Morocco, Oman, Qatar, Saudi Arabia, Syria, Tunisia, Turkey, United Arab Emirates, Yemen Rest of Middle East + countries in area 5.
Rest of Africa, Rest of Asia (Bangladesh, Cambodia, India, Indonesia, Laos, Malaysia, Mongolia, Myanmar, North Korea, Philippines, Sri Lanka, Thailand, Vietnam, etc).
You will be covered outside your chosen Area of cover for unexpected illnesses and accidents only. Assistance Companies evacuate to “the nearest place of suitable care” so make certain the country to which you might be evacuated to is in your chosen Area of
Cover so that hospitalization costs are covered after any evacuation.
Emergency Assistance, Repatriation & Evacuation and Personal Liability* are included. * Not available in every country.
US$ _________________
* Not available with
Primary
* Not available with
Primary
* Not available
with Primary
or Vitality Only available if Dental is also chosen
US$ _________________
US$ _________________
US$ _________________
Your Death (all causes) or Permanent Total Disability lump sum multiplied by 2.
(1)Only available if Death (all causes) or Permanent Total Disability is chosen.
US$ _________________
US$ _________________
TOTAL US$ ______________ / year Total annual premium
including all dependants
PREMIUMS

CARE & HEALTH . APPLICATION FORM 1
I, the undersigned, certify that the information filled in the present Application Form, as well as in the Health Declaration Form,
is correct and sincere, and certify not having declared or withheld any information which might affect the risk assessment.
I understand and have taken note that any false declaration or non-disclosure will void coverage under this policy, that in this
case the insurer would retain paid premiums as civil damages and that me and my dependants shall have to reimburse
perceived benefits.
I hereby request to become a member of La Garantie Médicale et Chirurgicale (GMC), under the Care & Health insurance
plan designed by HENNER and underwritten by La GMC.
I acknowledge that I have read and understood the guarantees described in the table of benefits and the General Conditions
of the Care & Health Policy provided with this Application Form.
I have duly noted that my enrollment under the Care & Health Policy shall be effective subject to:
Approval by the HENNER - GMC Medical Advisory Board of the enclosed health declaration duly filled out by myself and
all my dependants who have reached majority
Payment of premium
In the event of my death, I appoint as beneficiary my surviving spouse unless legally separated; otherwise in equal shares my
children born or to be born, the share of a deceased child going to his/her own children or to his/her brothers and sisters if
he/she has no children; otherwise in equal shares my surviving parents; or in their absence, my heirs.
I further note that should I wish to change beneficiaries at any time, I shall write formally to HENNER - GMC with details of the
requested changes and clearly identify any new beneficiaries.
Signed in (city; country) _____________________________ Policy holder’s signature, precede by « read and agreed » :
On (date) ____ / ___ / ______ (dd/mm/yyyy)
To apply for cover, you need to complete this Application Form and the Health Declaration Form. We would like to draw your attention to the fact that the health declaration has to be sent directly to our Medical Board (by email or by post using a separated envelope) at the following address:
Medical board (Care & Health Application) GMC Services Asia Pacific
20 Cecil Street, #05-04/05/08 Equity Plaza Singapore 049705
Email: [email protected]
For the other documents, you can scan your signed forms and email them to us at [email protected]
When submitting, remember also to include:
Your bank account details, for reimbursement of claims
A copy of your ID or passport
The Certificate of Insurance from your last insurer, if you would like us to consider waiving some of the usual waiting
periods
If your Application is accepted we will send you a Premium Invoice and your Policy will not be in force until that premium is paid. Please make sure to answer all questions and to sign the forms. We look forward to being of service.
Your declaration
Your declaration
R.C
.S.
PA
RIS
B 3
23
37
7 7
39
- r
ef
GM
CG
12
47
4 -
05
/20
13
HENNER - Simplified private joint stock company - Registered capital of € 8,212,500 - RCS Paris B 323 377 739 - TVA intra communautaire FR48323377739 - ORIAS No. 07.002.039 (available at www.orias.fr) - Regulated by the ACP (Prudential Supervisory Authority) - ISO 9001 certified by Bureau Veritas Certification Certificate No. 122190 - Headquarters: 10 rue Henner 75459 Paris Cedex 09 France - www.henner.com
Hauteville Insurance Company Limited, Harbour Court - Les Amballes, St. Peter Port, GUERNSEY GY1 4QA - CHANNEL ISLANDS Licensed by the Guernsey Financial Services Commission Registered Number : 24676
La Garantie Médicale et Chirurgicale Association constituted in accordance with the 1901 French law regarding non-profitable organizations - 10, rue Henner - 75459 PARIS Cedex 09 France.
1
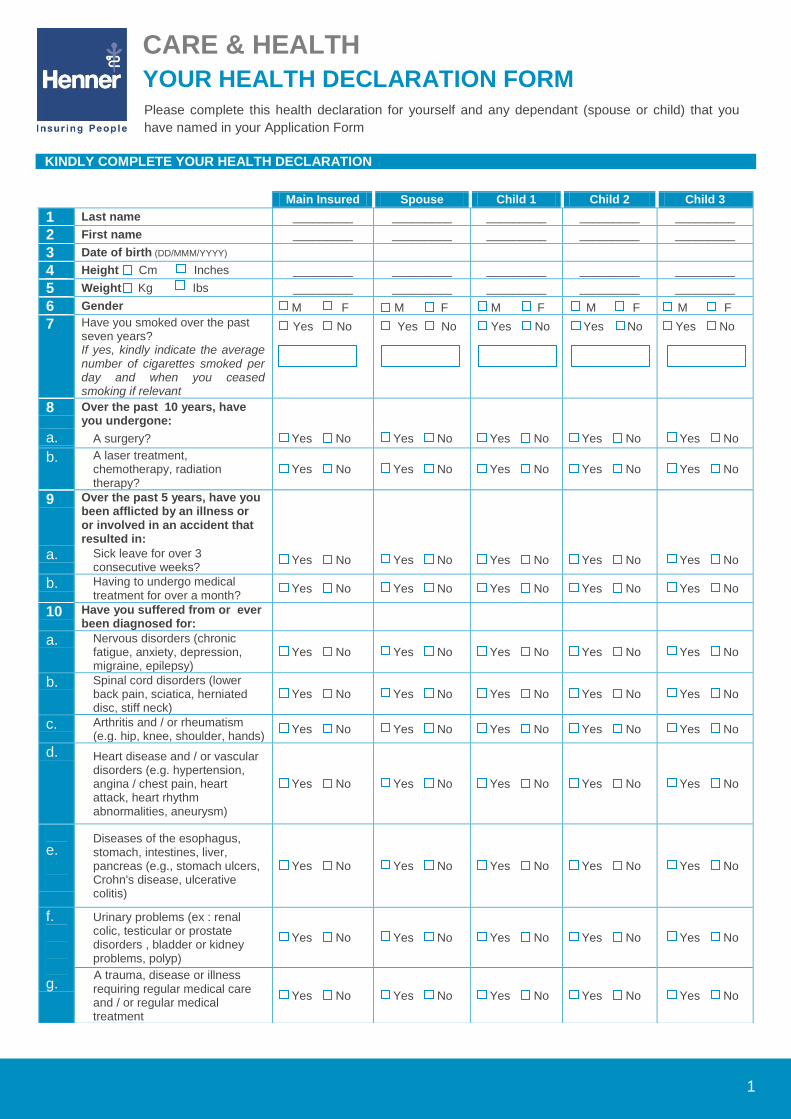
KINDLY COMPLETE YOUR HEALTH DECLARATION
Main Insured Spouse Child 1 Child 2 Child 3
1 Last name _________ _________ _________ _________ _________
2 First name _________ _________ _________ _________ _________
3 Date of birth (DD/MMM/YYYY)
4 Height Cm Inches _________ _________ _________ _________ _________
5 Weight Kg Ibs _________ _________ _________ _________ _________
6 Gender M F M F M F M F M F
7 Have you smoked over the past seven years? If yes, kindly indicate the average number of cigarettes smoked per day and when you ceased smoking if relevant
Yes No Yes No Yes No Yes No Yes No
8 Over the past 10 years, have you undergone:
a. A surgery? Yes No Yes No Yes No Yes No Yes No
b. A laser treatment, chemotherapy, radiation therapy?
Yes No Yes No Yes No Yes No Yes No
9 Over the past 5 years, have you been afflicted by an illness or or involved in an accident that resulted in:
a. Sick leave for over 3 consecutive weeks?
Yes No Yes No Yes No Yes No Yes No
b. Having to undergo medical treatment for over a month?
Yes No Yes No Yes No Yes No Yes No
10 Have you suffered from or ever been diagnosed for:
a. Nervous disorders (chronic fatigue, anxiety, depression, migraine, epilepsy)
Yes No Yes No Yes No Yes No Yes No
b. Spinal cord disorders (lower back pain, sciatica, herniated disc, stiff neck)
Yes No Yes No Yes No Yes No Yes No
c. Arthritis and / or rheumatism (e.g. hip, knee, shoulder, hands)
Yes No Yes No Yes No Yes No Yes No
d. Heart disease and / or vascular disorders (e.g. hypertension, angina / chest pain, heart attack, heart rhythm abnormalities, aneurysm)
Yes No Yes No Yes No Yes No Yes No
e.
Diseases of the esophagus, stomach, intestines, liver, pancreas (e.g., stomach ulcers, Crohn's disease, ulcerative colitis)
Yes No Yes No Yes No Yes No Yes No
f. g.
Urinary problems (ex : renal colic, testicular or prostate disorders , bladder or kidney problems, polyp)
Yes No Yes No Yes No Yes No Yes No
A trauma, disease or illness requiring regular medical care and / or regular medical treatment
Yes No Yes No Yes No Yes No Yes No
CARE & HEALTH
YOUR HEALTH DECLARATION FORM Please complete this health declaration for yourself and any dependant (spouse or child) that you
have named in your Application Form

2
11 Have you ever performed a serological screening test as follows: If yes, kindly specify the result in the table below
a. Hepatitis B virus(HBV) ? Yes No Yes No Yes No Yes No Yes No
b. Hepatitis C (HCV) ? Yes No Yes No Yes No Yes No Yes No
c. HIV (AIDS) ? Yes No Yes No Yes No Yes No Yes No
12 Have you ever had addiction problems related to alcohol and / or drugs?
Yes No Yes No Yes No Yes No Yes No
13 Within the next 6 months following the effective date of your contract, do you think you may :
a. Go to see a doctor or require any medical test (e.g. laboratory, imaging, endoscopy) and / or see a specialist and / or seek medical or surgical treatment?
Yes No Yes No Yes No Yes No Yes No
b. Receive hospital treatment? (e.g. removal of tonsils, removal of a cyst, removal of a mole)
Yes No Yes No Yes No Yes No Yes No
Main Insured
14 Do you suffer from a handicap, disability or chronic illness?
Yes No
15 In the 12 months preceding the effective date of your contract, have you taken sick leave more than 3 times?
Yes No
16 Do you or anyone in your family have a history of the following diseases? Heart disease, vascular, neurological, psychiatric, cancer, diabetes?
Yes No
17 Are you currently on sick leave? Yes No
18 Have you been declared disabled? Yes No
Are you in the process of being declared disabled?
Yes No
19 Are you currently insured for health or Life insurance?
Yes No
Have you ever been refused, restricted or received a premium loading for a previous insurance policy?
Yes No
20 Do you fly in a private or aviation club aircraft as a passenger or pilot (excluding
regular commercial aircrafts)? Yes No
21 Have you suffered any medical condition other than those mentioned above?
Yes No
22 Please add any other information regarding your health status that we should know.
CARE & HEALTH
YOUR LIFE INSURANCE DECLARATION FORM
Please complete this health declaration for yourself if you suscribe to the Life Insurance coverage.

3
If you answered "yes" to any of the above questions, kindly clarify the details in the table below.
Question number
Date of declaration of the first symptoms
Date of the last
symptoms Treatments, tests and results
Complementary precisions
Main insured
Spouse
Child 1
Child 2
Child 3
CARE & HEALTH
HEALTH DECLARATION

4
DECLARATION AND AUTHORISATION
1. To ensure medical confidentiality, you must submit this questionnaire and any medical documents sealed and marked
confidential, addressed to the attention of the medical board of HENNER – GMC:
Medical board (Care & Health Application) Email: [email protected]
2. Please provide your answer on a separate piece of paper and attached it to this Declaration when sending if you need more
space to provide your response. If you are applying with more than 3 children, please complete a second form for the
additional children.
3. I certify that the statements above are complete, accurate and truthful and agree to provide the medical board of HENNER -
GMC all the medical information that they need. Any misrepresentation or omission shall render the policy null and void and
the premiums paid will be retained by the insurer as damages. The Insured and his dependants will have to refund the
benefits they have received.
Your email (compulsory): …………………………………………………………...
(This is necessary for our medical board to contact you in regards to this health declaration).
Signed in (City, Country): ……………………………………………………………
Date (dd/mm/yy): …………………………………………………………………......
Signature(s) of the Insured and all dependants who have reached majority with the mention "read and approved":
HENNER - Simplified private joint stock company - Registered
capital of € 8,212,500 - RCS Paris B 323 377 739 TVA intra
communautaire FR48323377739 - ORIAS No. 07.002.039
(available at www.orias.fr) - Regulated by the ACP (Prudential
Supervisory Authority) - ISO 9001 certified by Bureau Veritas
Certification - Certificate No. 122190 Headquarters: 10 rue
Henner 75459 Paris Cedex 09 - France www.henner.com
Hauteville Insurance Company Limited - Harbour House - Les Amballes - St Peter Port Guernsey GY1 4QA - Channel Islands - Licenced by the Guernsey Financial Services Commission - Register number: 24676
La Garantie Médicale et Chirurgicale - Association
constituted in accordance with the 1901 French law
regarding non-profitable organizations - 10, rue
Henner - 75459 PARIS Cedex 09 France
Care
& H
ealth
-
QM
- O
ffsho
re -
G
MC
G12
41
9 -
AN
G -
04/2
01
3






![Pakistan: Afghan Refugees and Undocumented Afghans … · 2020-04-30 · Pakistan: Afghan Refugees and Undocumented Afghans Repatriation [Subject] (as of XX Mmm YYYY) (01 Jan to 01](https://img.pdfslide.net/doc/110x75/5f5f76443bf2be22eb7ffb86/pakistan-afghan-refugees-and-undocumented-afghans-2020-04-30-pakistan-afghan.jpg)













![0...yyyy Z t yyyy G¯ Íz Î Í yyyy G¯ ¤ Íz Î ¤ Í o ] ¢ o z - ~ . £ yyyy o ïù·ï» yyyy G¯ . z Î . yyyyhTq . z Î - \ 6] ¢ \ 6 £ yyyy $ { yyyy· T¿ yyyy \ 6 « w](https://img.pdfslide.net/doc/110x75/6084e787fc18b9237345786a/0-yyyy-z-t-yyyy-g-z-yyyy-g-z-o-o-z-.jpg)








