Embed Size (px)
Citation preview
Care of the Post-Op Foot Surgery Patient
By Anne Eby, RN, ONC, BSNNursing made Incredibly Easy! November/December 20082.0 ANCC/AACN contact hoursOnline: www.nursingcenter.com
© 2008 by Lippincott Williams & Wilkins. All world rights reserved.
Foot Surgery
Includes a variety of procedures:
Removal of a growth Amputation of part or all of the foot Elective or emergent procedures for
musculoskeletal disorders
Nonsurgical management remains the treatment of choice for chronic foot disorders
When these options fail, surgical treatment may be necessary
Anatomy of the Foot
The foot contains: 26 bones 33 joints More than 100 ligaments, tendons, and muscles
Joints and muscles of the foot allow for a wide range of motion
Components prone to injury: Achilles tendon Plantar fascia ligament
Two most commonly discussed arteries: Dorsalis pedis Posterior tibial
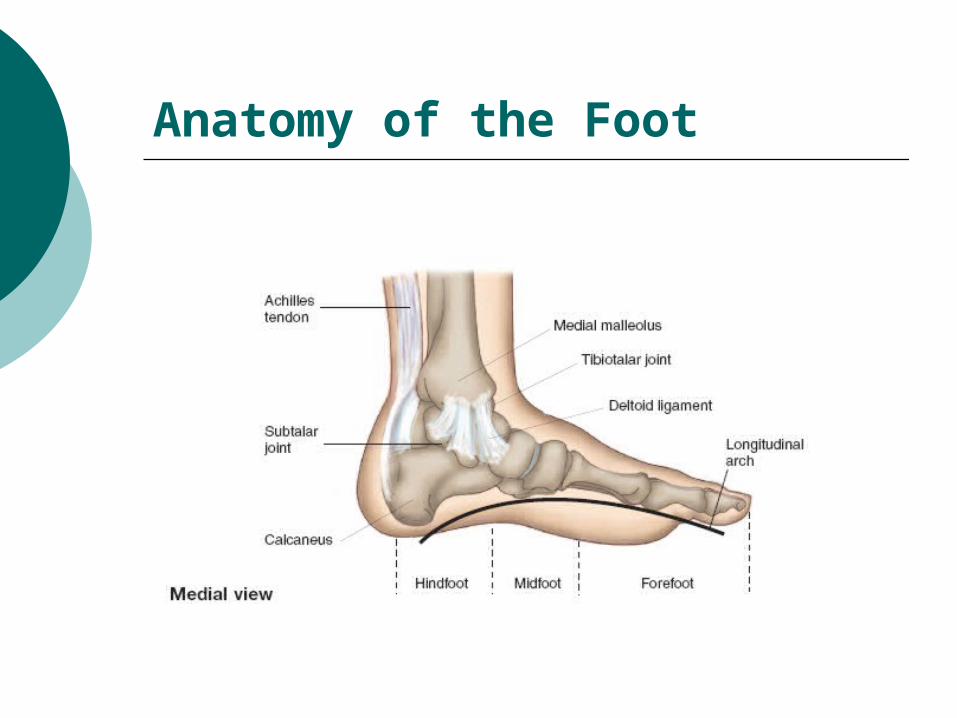
Anatomy of the Foot
Common Foot Deformities
Bunions—a local painful swelling caused by misalignment of a joint
Clawfoot—an abnormally high arch and a fixed equinus deformity of the forefoot; Charcot foot deformity is a common cause
Clubfoot—one or both of the feet turn inward; effects 1 in 1,000 newborns
Flatfoot—progressive disorder in which the arch of the foot is diminished; four times more likely in women; causes: congenital abnormalities, injury, muscle fatigue, obesity, hypertension, diabetes, or arthritis
Common Foot Deformities
Hammer toe—flexion deformity of the interphalangeal joint
Heel pain—usually related to inflammation of the plantar fascia or entrapment of the medial calcaneal nerve or the first branch of the lateral plantar nerve
Morton’s neuroma—swelling of the third branch of the median plantar nerve caused by ischemia of the nerve from compression or trauma
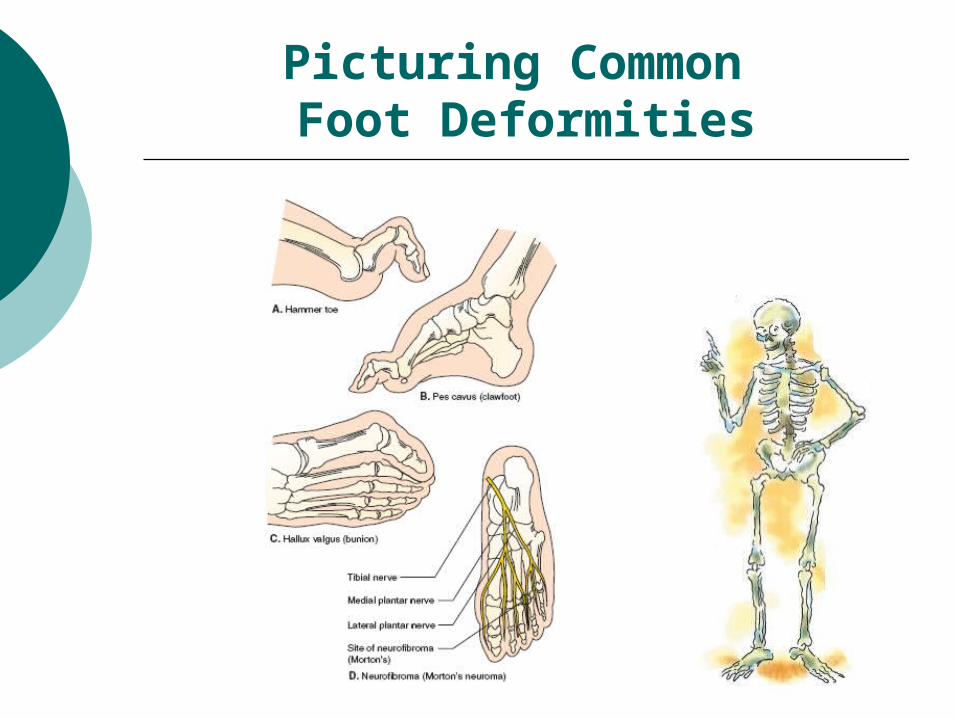
Picturing Common Foot Deformities
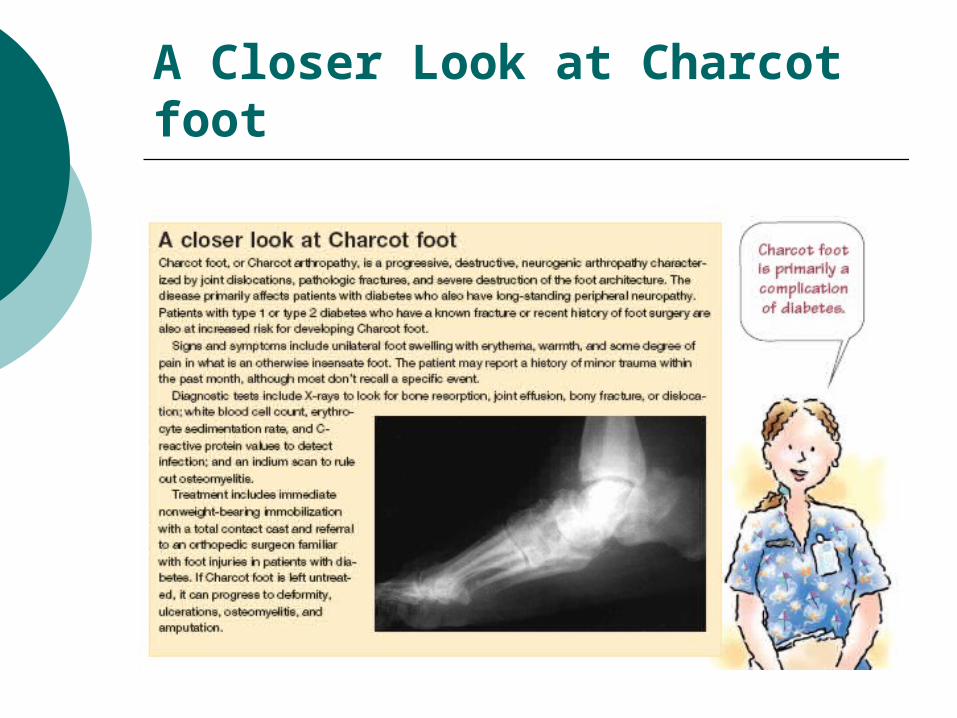
A Closer Look at Charcot foot
Treatment
Bunions X-rays to determine the extent of deformity Ranges from no treatment to orthoses or night
splints
Clawfoot Exercises and bracing
Clubfoot Managed exclusively with the Ponseti technique,
which involves stretching the foot, casting, and tenotomy, followed by wearing braces
Treatment
Flatfoot Exercises and orthoses, surgery if necessary
Hammer toe Wearing open-toed sandals and performing
manipulation exercises; osteotomy may be required
Heel pain Corticosteroid injections, taping ,and casting;
surgery when conservative treatment fails after 6 to 12 months
Morton’s neuroma Inner soles and metatarsal pads to balance foot
posture, local hydrocortisone injections
Post-Operative Care
Depends on type of injury and procedure
Nursing care focuses on:
Promoting tissue perfusion Pain management Preventing complications Improving mobility
Promoting Tissue Perfusion
Assess the neurovascular status of the affected extremity every 1 to 2 hours for the first 24 hours, including:
Color Edema Temperature Pain Capillary refill time Sensation Pulses Motion
Indicators of Neurovascular Dysfunction
Circulation Pale, cyanotic, or mottled color Cool temperature Capillary refill time of more than 3 seconds
Motion Weakness Paralysis
Sensation Paresthesia Unrelenting pain Pain on passive stretch Absence of feeling
Pain Management
Related to inflammation
Elevation and ice
Oral or I.V. pain medications
Assess your patient’s pain by asking her to identify its location, describe its quality, and rate its intensity
Preventing Complications
Most significant are infection and deep vein thrombosis
Prophylactic antibiotics
Pin care (if applicable) with stringent standard precautions
Early mobilization, compression devices, and anticoagulants as appropriate
Improving Mobility
Weight bearing as tolerated/ordered
Use of assistive devices, such as crutches or a walker
Patient teaching in safe use of these devices
Teaching Crutch Maneuvering Techniques
To sit down Grasp the crutches at the hand pieces for control Bend forward slightly while assuming a sitting
position Place your affected leg forward to prevent weigh
bearing and flexion
To stand up Move forward to the edge of the chair with your
strong leg slightly under the seat Place both crutches in your hand on the side of the
affected leg Push down on the hand piece while raising your
body to a standing position
Teaching Crutch Maneuvering Techniques
To go down stairs Walk forward as far as possible on the step Advance the crutches to the lower step, advancing
your weaker leg first and then the stronger one
To go up stairs Advance your stronger leg first up to the next step. Advance the crutches and then the affected leg A helpful memory device for your patient is: Up with
the good, down with the bad
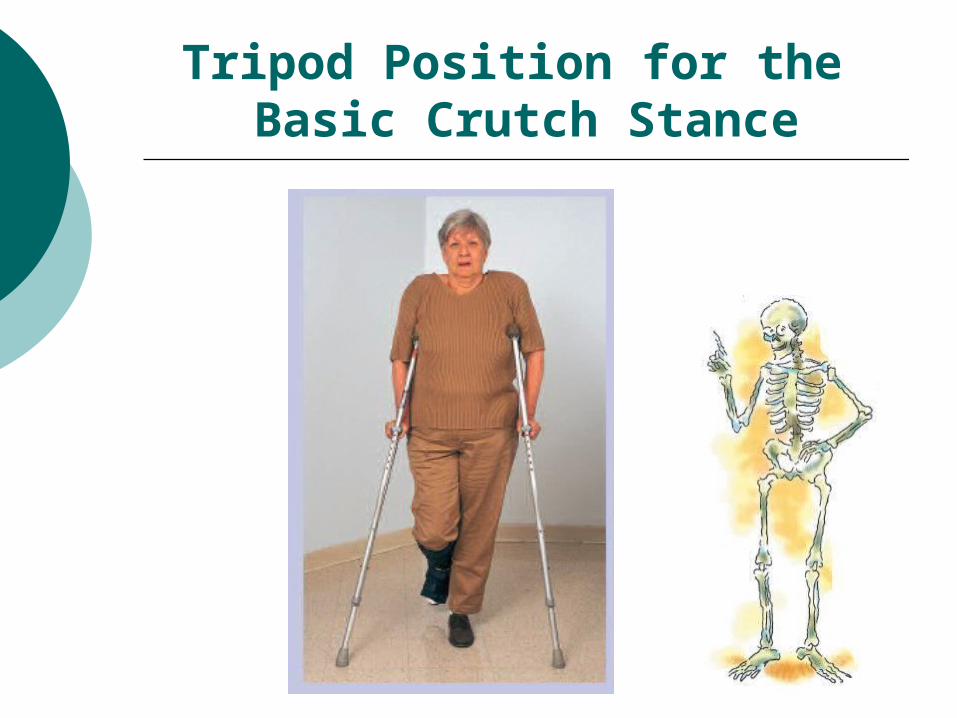
Tripod Position for the Basic Crutch Stance
Self Care After Foot Surgery
Signs and symptoms to report
Change in sensation Inability to move your
toes Toes or foot cool to the
touch Color changes
Pain management Elevate your foot to
heart level Apply ice as prescribed Use analgesics as
prescribed Report unrelieved pain
Mobility Use assistive devices
safely Comply with prescribed
weight-bearing limits Wear a special
protective shoe over the dressing
Wound care Keep the dressing or
cast clean and dry Report signs of
infection, such as pain, drainage, or fever, immediately
Follow the prescribed antibiotic regimen
Keep your appointment with the surgeon for the initial dressing change