Embed Size (px)
Citation preview

Volume 89 No. 12 December 2006
�Care of the Uninsured
and UnderservedPart 2


387VOLUME 89 NO. 12 DECEMBER 2006
Medicine and Health/Rhode Island (USPS 464-820), a monthly publication, is owned and published by the Rhode Island Medical Society, 235Promenade St., Suite 500, Providence, RI 02908, Phone: (401) 331-3207. Single copies $5.00, individual subscriptions $50.00 per year, and $100per year for institutional subscriptions. Published articles represent opinions of the authors and do not necessarily reflect the official policy of the Rhode IslandMedical Society, unless clearly specified. Advertisements do not imply sponsorship or endorsement by the Rhode Island Medical Society. Periodicals postagepaid at Providence, Rhode Island. ISSN 1086-5462. POSTMASTER: Send address changes to Medicine and Health/Rhode Island, 235 Promenade St.,Suite 500, Providence, RI 02908. Classified Information: RI Medical Journal Marketing Department, P.O. Box 91055, Johnston, RI 02919,phone: (401) 383-4711, fax: (401) 383-4477, e-mail: [email protected]. Production/Layout Design: John Teehan, e-mail: [email protected].
UNDER THE JOINTEDITORIAL SPONSORSHIP OF:
Brown Medical SchoolEli Y. Adashi, MD, Dean of Medicine& Biological Science
Rhode Island Department of HealthDavid R. Gifford, MD, MPH, Director
Quality Partners of Rhode IslandRichard W. Besdine, MD, ChiefMedical Officer
Rhode Island Medical SocietyBarry W. Wall, MD, President
EDITORIAL STAFFJoseph H. Friedman, MD
Editor-in-ChiefJoan M. Retsinas, PhD
Managing EditorStanley M. Aronson, MD, MPH
Editor Emeritus
EDITORIAL BOARDStanley M. Aronson, MD, MPHJay S. Buechner, PhDJohn J. Cronan, MDJames P. Crowley, MDEdward R. Feller, MDJohn P. Fulton, PhDPeter A. Hollmann, MDSharon L. Marable, MD, MPHAnthony E. Mega, MDMarguerite A. Neill, MDFrank J. Schaberg, Jr., MDLawrence W. Vernaglia, JD, MPHNewell E. Warde, PhD
OFFICERSBarry W. Wall, MD
PresidentK. Nicholas Tsiongas, MD, MPH
President-ElectDiane R. Siedlecki, MD
Vice PresidentMargaret A. Sun, MD
SecretaryMark S. Ridlen, MD
TreasurerKathleen Fitzgerald, MD
Immediate Past President
DISTRICT & COUNTY PRESIDENTSGeoffrey R. Hamilton, MD
Bristol County Medical SocietyHerbert J. Brennan, DO
Kent County Medical SocietyRafael E. Padilla, MD
Pawtucket Medical AssociationPatrick J. Sweeney, MD, MPH, PhD
Providence Medical AssociationNitin S. Damle, MD
Washington County Medical SocietyJacques L. Bonnet-Eymard, MD
Woonsocket District Medical Society
RHODE ISLANDPUBLICATION OF THE RHODE ISLAND MEDICAL SOCIETY
Medicine � Health VOLUME 89 NO. 12 December 2006
COMMENTARIES
388 Dreams In Neurological DiseasesJoseph H. Friedman, MD
389 Profiling and Genetic Destiny
Stanley M. Aronson, MD
CONTRIBUTIONS
CARE OF THE UNINSURED AND UNDERSERVED, PART 2Guest Editor: L. McTyeire Johnston, MD
390 Improving the Poor Outcomes of Today’s Health CareL. McTyeire Johnston, MD
391 RIte Care: Rhode Island’s Success In Improving the Health of Children andFamilies
Tricia Leddy, MS
397 Serving the Spectrum of Needs In Community Health CentersDennis Roy
400 Opportunities For Improved Quality and Access In the Office SettingChris Campanile, MD, PhD
407 Is Health Reform In Massachusetts a Model For Rhode Island?David A. Rochefort, PhD
411 What Would It Take?Christopher F Koller, MPPM, MA
COLUMNS
415 HEALTH BY NUMBERS – Utilization of Hospital Emergency Departments, RhodeIsland 2005Karen A. Williams, MPH, and Jay S. Buechner, PhD
417 PUBLIC HEALTH BRIEFING – Rhode Island Public Health Training Program: MarketSurvey FindingsKarine Tolentino, PhD, and Robert Marshall, PhD
419 IMAGES IN MEDICINE – Colonic Intussusception in an AdultJohn A. Pezzullo, MD
420 PHYSICIAN’S LEXICON – The Vocabulary of DisasterStanley M. Aronson, MD
420 Vital Statistics
422 December Heritage
Cover: “Snowed In,” oil, by MeredithThayer, an East Providence-based art-ist who has exhibited at the ProvidenceArt Club, the Spring Bull Gallery, theWickford Art Association, the RhodeIsland Water Color Society, and theCape Cod Art Association.E-mail: [email protected]
ERRATUM: The November 2006 issue (volume 89, number 11) mistakenly in-cluded L. McTyeire Johnston, MD, among the authors of the ACP abstract: “Recur-rent Clozapine Induced Cardiac Tamponade.”

388MEDICINE & HEALTH/RHODE ISLAND
Dreams In Neurological Diseases�
Commentaries
“YOU’RE DREAMING,” IS A COMMONCOMMENT. It usually means that you arewishing, or overly optimistic. It used tobe used routinely for the Red Sox’s hopesto win a World Series; or these days tohope that your medical insurance rateswon’t rise as your coverage plummets.
“Maybe I’ll win the lottery.”“Dream on…”As best I can tell, the study of dreams
has not advanced much. While dreamsplayed a huge role in the development ofpsychoanalysis, they seem not have beenstudied much in the past few decades. Bythis I mean the study of dream content.Understanding of the physiology of dreamshas advanced greatly but what dreams “do”and what they “mean” has not.
In my field, Parkinson’s disease(PD), dreams play a very important role.For one thing PD patients often developvivid dreams when they start taking theirPD medications. Sometimes the dreamsare so realistic that if they have that sortof dream they may wake up thinking thatit happened. When the family hears,“Did the fire department get everyoneout of the burning house down thestreet?” after what seemed to them a nor-mal, uneventful night, they will oftenbecome worried about confusion andimpending dementia.
Nightmares too occur in PD, as theydo throughout the population. Some-times they occur because of the medica-tions, and sometimes they simply becomemore vivid, hence more terrifying, abet-ted by the medications.
About one-third of men (about 1/15 of women) with PD develop REMsleep behavior disorder. In normal REM(rapid eye movement) sleep, we are para-lyzed except for our eye and breathingmovements. This is when the bulk of ourdreaming occurs. People with REM sleepbehavior disorder maintain their normalawake muscle tone during dream sleep.During certain types of dreams, typically
violent, they act out their dreams: kick-ing, punching and strangling theirbedmates, punching furniture, jumpingout of bed, causing the type of havoc you’dexpect if you acted out a violent dream.Interestingly the dreams in which theyhit their wives usually accompany dreamsin which they are fighting people or ani-mals which are attacking the wife. Whilethe psychoanalytic meaning of this maybe clear, its pathophysiology is not. It of-ten precedes the onset of the motor dys-function in PD and is unrelated to themedications used to treat it.
Post-traumatic stress disorder is an-other condition in which dreams are anintegral part of the illness. People experi-ence the same terrifying nightmare re-peatedly, making sleep another battle-field in life.
An observation by a patient got meinterested in another aspect of sleep. I gavea talk on non-motor aspects of Machado-Joseph Disease, an inherited spinocerebel-lar ataxia, at the annual meeting of the Na-tional Ataxia Foundation. During thequestion and answer session, a patientasked me why he was always normal in hisdreams, meaning that he hadn’t yet devel-oped his motor symptoms. These usuallybegin in the fourth or fifth decade. I toldhim that I had no idea about this, havingnever heard it before; and then I got theinspiration to ask the audience, full ofpeople with a variety of ataxic disorders,almost all of adult onset, whether they toowere only normal in their dreams. The re-sponse was about 30:1. Only a single per-son had dreams in which she was afflicted.The rest were normal.
That was interesting. I wondered ifthis was true with other adult onset dis-orders, so I asked the next 100 patients Isaw with PD about their dreams. Many,of course, didn’t recall their dreams (weall dream although many think they don’t)but of those who did, only a small frac-tion dreamt they had PD.
In my way of thinking, these werenot wish fulfillment dreams, with a singleexception. In a wish fulfillment dream,there is great relief or joy in some dreamoutcome. Your lost dog is found, yourfriend’s cancer is miraculously cured, youget the job you’ve been wanting, etc. Inmy patients’ dreams they experiencethemselves as normal, not hampered byPD. There is so sense of relief, of beingrestored. The one wish fulfillment dreamwas of a person who dreamt he had PD!The PD got him out of the army, whichallowed him to go home, with great joy.
I love making these sorts of observa-tions. While I am not very creative, I thinkthat I’m intellectually curious. So whensomeone, like the ataxic person in the audi-ence, asks me a question about somethingI’ve never thought about, especially some-thing a little bit oddball, I wonder about it.In this case the first question, which theataxic patients answered was, “is it a gen-eral observation?” The next question waswhether or not it extended to another dis-order, which it did. I don’t know, of course,whether it is true of all adult-onset disor-ders, that the dreamers are normal in theirdreams, but I assume that it is, although toinduce from only two disorders, both neu-rological, is not a solid foundation.
The more interesting question is: doesthis mean anything? I don’t know. For onething we don’t know if the observation re-flects the dream or the recall mechanism.Maybe patients only recall particular typesof dreams, just as the PD patients only en-act certain dreams. Perhaps there is an in-nate censor that restricts recall.
Perhaps these are wish-fulfillmentdreams. Perhaps the wish is not to be mi-raculously healed and restored, but sim-ply to have a normal life, a life nevertouched by disease, not a “going back,”but a “never was,” a much better wish tohave fulfilled.
– JOSEPH H. FRIEDMAN, MD

389VOLUME 89 NO. 12 DECEMBER 2006
Profiling and Genetic Destiny�
THE RICH VOCABULARY OF ANCIENT ROME included a word todescribe the process of sketching or otherwise displaying thelateral outlines of some person or object. The word was profileand as a form of art it confined itself to the peripheral contoursof the face, rather that its full portrait. Addison in 1702, forexample, declared that the classical Roman art had decayed tosuch a degree that by the Third Century, its emperors wereportrayed solely in profile.
A new art form eventually arose called silhouetting [namedafter Etienne de Silhouette, 18th Century French Minister ofFinance]. It embodied the skillful representation of a person’sfacial profile incised from black paper and then placed againsta contrasting white background. The American theater dur-ing the 1930s was blessed with the presence of three hugelytalented siblings, the Barrymores: Ethel, Lionel and John.Newspapers often referred to John Barrymore, an extraordi-narily handsome man, as “the great profile;” indeed. his noblefacial contours richly deserved such a title.
A silhouetted profile becomes high art when people canreadily recognize it as Napoleon or Elvis Presley or even UnclePhilbert. Accuracy and predictability became the criteria ofperfection in graphic profiling. If a profile, which is little morethan a hint of the full truth, can allow the observer to identifythe subject with a high level of probability, the profile can becalled successful.
Demographers, geologists and even economists graduallyexpanded the definition of a profile to include non-facial out-lines; and, inevitably, it came to define the shape, artistic ornot, individual, populational or even meteorological. Thus,gradually, the word profile was taken to mean a hazy outlineevocative of fuller realities. In this altered sense sociologists,physicians and even police departments now employ the wordprofile.
Profiling of criminal behavior, or the potential for crimi-nal behavior, is centuries old. It is tempting, if also naïve, tocontemplate a list of visible characteristics which police mightuse to identify criminals, even potential criminals who havenot as yet undertaken a life of crime. Jurisdictions have strivento create such a forensic profile for centuries. In 17th CenturyEngland, for example, Michael Dalton, a jurist, prepared a listof characteristics; e.g., whether the suspect’s parents “werewicked,” the suspect’s nature [whether a “quarreler, a pilfereror bloody-minded”], whether idle or vagrant, his companions,and “whether he be of evil fame or report.” Thus earlier profil-ing placed much responsibility on the intuitive judgment ofthe enforcers of law and tacitly accepted such guiding prin-ciples as guilt by association, the heritability of criminals andthe association of unemployment with unlawful acts.
The 19th Century witnessed the first serious attempts toidentify a genetic basis for criminal behavior. Cesare Lombroso,one of the founders of criminology, was convinced that certainfacial characteristics predisposed an individual to crime, alco-holism and feeblemindedness. Advocates of phrenology, thepseudoscience which attempts to associate cranial contour with
behavior, also believed that certain cranial bumps signifiedcertain altered cognitive faculties and character traits.
In 1985 the Drug Enforcement Administration [DEA]issued guidelines for the identification of possible drug couri-ers. The profile included the age and ethnic characteristics ofthe probable contraband drivers. As a result, a disproportion-ate number of black and Hispanic drivers were stopped foralleged traffic violations as a means of ascertaining whetherthe vehicle was carrying drugs. This widespread practice, nowcalled racial profiling, led to increased tensions between thepolice and communities of color. Racial profiling is now de-fined as the discriminatory police practice of suspecting indi-viduals of criminal behavior based principally on their ethnicity,race or nation of origin.
The most egregious example of racial profiling on Ameri-can territory took place in 1942 when 109,650 west coast resi-dents of Japanese ancestry [70,000 of whom were Americancitizens] were forcibly removed from their homes and internedin “preventive detention” for the duration of the conflict withJapan. These actions were undertaken to abort acts of sabo-tage or espionage. Records of the Federal Bureau of Investiga-tion, incidentally, contain no substantiated instances of veri-fied espionage or sabotage by Japanese-Americans before orduring World War II.
Medical profiling, on the other hand, would seem to be asafe practice since the only victims of potential bias in profilingmight be the diseases themselves. Certainly triage profilingfor diabetes would seem to be an ennobling effort. Thus, if apatient were to exhibit the triad of great thirst [polydipsia],excessive urination [polyuria] and unexplained weight loss,urgent steps should then be taken to determine the presenceor absence or diabetes. Not everyone with these signs will be adiabetic, but sufficient numbers will indeed be in the earlystages of the disease to justify the continued use of this profile.
In 1961 a genetic study of an otherwise normal 44 year-old male revealed him to possess an extra Y chromosome [themale sex chromosome]. This curious anomaly was then de-tected in about one in every thousand newborn males. Stud-ies have since determined that such individuals – called super-males by the tabloids – are taller than normal, slower learners,more prone to facial acne and more easily frustrated than thosewith a normal complement of sex chromosomes. Still othersocial scientists have detected an increased aggressive tendencyin the XYY syndrome males, and some people have even specu-lated that such individuals are more prone to engage in violentcrime. More recent and more comprehensive studies havedisputed this alleged association.
Science-fiction writers have envisioned a brave new worldwhere each newborn’s capabilities and destiny will be readilyavailable to its parents on a computer-generated profile. Butothers believe that man, like Jacob Marley, has no destiny onthis earth save the one he contrives for himself.
– STANLEY M. ARONSON, MD

390MEDICINE & HEALTH/RHODE ISLAND
Knowing is not enough; we must apply.Willing is not enough; we must do.
– Goethe
Goethe prefaces the findings of the Institute of Medicine,in their studies to improve safety and outcomes for patients.His words are likewise applicable to these two Medicine &Health/Rhode Island issues.
October’s issue focused on shortcomings in our deliveryof health services. Starting with the adverse impacts of lack ofinsurance, articles spotlighted that many Rhode Islanders re-ceive fragmented care, in a system with shallow understandingand application of patients’ personal and cultural needs, withresultant outcomes in quality, access, and customer satisfactionthat would embarrass any industry.
This issue’s topics are more hopeful. The authors high-light successes:
• Tricia Leddy reviews the progress of RIte Care in improv-ing access and outcomes for Rhode Islanders. Critical tothese successes was the concrete vision at RIte Care’s cre-ation, and the political will to construct that vision.
• Dennis Roy discusses the multi-disciplinary model ofCommunity Health centers, which have built systems ofcare reaching beyond office visits to address the spec-trum of patients’ needs. These successes should be nosurprise—the Community Health Centers are governedby community-driven Boards of Directors.
• Reflecting the critical work on the front lines of patientcare, Chris Campanile, MD, discusses changes in of-fice operations to improve access and quality. Thereare lessons here about vision (what are we trying to do?),about teamwork (and the critical role of non-physicians),and about using measurement (are we doing what wewant?).
• David Rochefort, PhD, analyzes health reform in Mas-sachusetts. Noting that we best evaluate Massachusetts’individual design components and Rhode Island’s estab-lished agency environment, he points out the public andpolitical partnerships necessary to drive the innovationin policy.
• Christopher Koller, the state’s Health Insurance Com-missioner, asks “What Would It Take?” He challenges usto define the principles and make a plan, and names thenecessary support from all constituencies—patients, pro-viders, and policymakers.
These articles present strong rays of light that penetratethe otherwise bleak horizons of our health care system. There
is no doubt—the forces impeding a comprehensive system ofcomprehensive services are winning. As individuals, as em-ployers, as policymakers, and as a State, we are losing the battleto control health care costs; as costs rise, purchasers respond bylimiting coverage. As the situation gets more desperate, werisk making bad decisions that could lead to a more fragmentedsystem serving fewer Rhode Islanders.
As background and understanding for facing these chal-lenges, we need to appreciate the forces at work.
Impact of Unit CostsThe total costs of services are the simple product of unit cost
and volume. Unit costs are increasingly uncontrollable—infla-tion, new technology, costs of new infrastructure (e.g.,, capitalexpansions at hospitals). More and more, unit cost growth con-sumes all the expense growth our system can tolerate. The re-sult: the burden of cost control falls to the control of volume, ofutilization—fewer services become the only answer to rising costs.
Competition as a double-edged swordCompetition can drive improvement and efficiency. How-
ever, a competitive system is also a fragmented one, losing the ne-gotiating leverage that comes with all-or-nothing contracting. Com-petition also relieves us as a society of the responsibility to answer,“What product do we want?” To date, the enthusiasm for compe-tition risks blocking a clear vision and concrete system delivery:
• In the commercial world, plans present variable cost-shift-ing strategies and therefore different barriers for patientsto negotiate (the choice made, by the way, by employers,not patients);
• In the world of publicly financed health care, some ap-proaches would foster a multi-model system without tak-ing advantage of the leverage (in contracting and in per-formance outcomes) provided by a centralized approach.
Meeting the cost challenge by reducing coverage In the face of overwhelming cost and limited vision, we
miss the point (and responsibility):
• What in our system has value, and what does not?
• What should we spend our money on?
• Where is the tradeoff between cost-shifting and access?
Increasingly, we are at risk of consciously limiting access asthe strategy to moderating health system costs. We are alreadyseeing new trends emerge:
• employers no longer purchase insurance for their workers;
Improving the Poor Outcomes of Today’s Health CareL. McTyeire Johnston, MD
�

391VOLUME 89 NO. 12 DECEMBER 2006
• Medicaid solutions are sought in reducing eligibility;
• The percentage of uninsured Rhode Island children hasrisen from 4.3% (2002) to 6.8% (2005). 1
These are daunting problems—daunting, but not hope-less. The authors in this issue cite successes. These successes oc-cur at the front lines of the provider office, in the design of andcommitment to comprehensive services as named by the com-munity, in the State-level planning and implementation that hasbrought health care and quality outcomes to Rhode Island’s chil-dren, and in the active struggles for vision at our State policylevel. There are solutions, solutions that require us all to give alot, solutions that will bring our patients better care.
REFERENCES1. Rhode Island Kids’ Count, August 29, 2006.
L. McTyeire Johnston, MD, is Chief Medical Officer, Neigh-borhood Health Plan of Rhode Island.
CORRESPONDENCEL. McTyeire Johnston, MDNeighborhood Health Plan of RI299 Promenade St.Providence, RI 02908Phone: (401) 459-6086e-mail: [email protected]
RIte Care: Rhode Island’s Success In Improving theHealth of Children and Families
Tricia Leddy, MS
“Universal comprehensive cov-erage for all Rhode Islanders isa goal to be achieved over thecourse of several years.”
Thus began a new Rhode Island lawauthorizing the RIte Care Program.Implemented in 1994 under a Medic-aid 1115 Research and DemonstrationWaiver, RIte Care had three goals:
Goal 1: To improve access andquality of care, health status,and health outcomes.
RIte Care established specific mea-sures as markers of improvement in ac-cess and quality: lengthen the intervalsbetween pregnancies, increase prenatalcare, improve birth outcomes, improvechildhood immunization/well child visitrates, decrease lead poisoning, and im-prove oral health. In 1994, there was asignificant gap in these measures betweenindividuals in Medicaid-enrolled familiesand individuals enrolled in employer-sponsored health insurance coverage in RI.
Goal 2: To reduce uninsuranceamong low-income children andfamilies in Rhode Island.
The marker of success would be thenumber of uninsured children in RI, aswell as RI’s level of uninsurance overall.In 1995, Rhode Island ranked 25th inthe country in uninsured children, with12.5% of Rhode Island children with-out coverage.1
�Goal 3: To control the rate of growth inhealth care expenditures for enrollees inRhode Island’s Medicaid Program.
The marker would be the annual rateof increase in costs for RIte Care families,compared to the annual increase in thecost of commercial insurance coverage inthe state. At that time, the state’s cost for achild or family enrolled in Medicaid wasincreasing at twice the rate as that of fami-lies with commercial coverage.
THE BEGINNINGIn 1993, a federal Medicaid Re-
search and Demonstration waiver al-lowed Rhode Island to enroll all of thestate’s AFDC 2 families into licensed man-aged care health plans. The waiverbrought in new federal Medicaid dol-lars to expand coverage to uninsured,low-income working families.
RIte Care began with 70,000 indi-viduals - children and parents in singleparent families, receiving cash assistanceunder the AFDC program. BetweenAugust 1994 and August 1995, all fami-lies enrolled in AFDC were enrolled intheir choice of Health Plans. Initially, fiveplans participated: NeighborhoodHealth Plan of Rhode Island (NHPRI),a new health plan formed by the networkof the state’s community health centers;United Healthcare of New England(UHCNE); Blue Chip, Blue Cross ofRhode Island’s HMO; Harvard HealthPlan; and Pilgrim Health Care.
The state contracted with theseplans, all accredited by the National Com-mittee for Quality Assurance (NCQA),for a comprehensive set of benefits, fo-cusing on primary and preventive care.Contracts specified quality and accessstandards which the state defined andmonitored. The contracts provided finan-cial incentives for meeting or exceedingperformance standards in areas of qual-ity and access, primarily using NCQAmeasures. Most significantly, the state re-quired that each enrollee have a primarycare physician, responsible for coordinat-ing all his/her care.
The state would meet the goals ofthe RIte Care program through two ba-sic components of the federal waiver:
• The 70,000 enrollees in AFDC,who had Medicaid coverage buthad difficulty obtaining services,were transitioned from Medicaidfee-for-service to a RIte Care plan.
• RIte Care’s waiver allowed the stateto expand coverage to the state’s un-insured, low-income working fami-lies.
THE FIRST TEN YEARSIn 1994, RIte Care began with preg-
nant women and preschool children en-rolled in Medicaid. By 1999, through aseries of incremental expansions ap-proved by the federal government, thestate legislature and the governor, eligi-bility expanded to cover all uninsured

392MEDICINE & HEALTH/RHODE ISLAND
RIte Care covers126,000 enrollees—
12% of RhodeIsland’s population.
children and parents in low-income,working families. By 2000, an additional35,000 children and parents, who werepreviously uninsured, had enrolled inRIte Care.
At the same time, federal welfare re-form changed the rules for AFDC: thenumber of Rhode Islanders receivingcash assistance dwindled from 70,000 toless than 35,000. Maintaining health in-surance coverage through RIte Care en-abled families to move to employment,since these jobs rarely offered health cov-erage.
Between 2001 and 2004, 5000children with special health care needs,including children in state foster care,were transitioned from Medicaid fee-for-service to RIte Care. These children re-ceived care management services, whichwere not available in fee-for-service Med-icaid.
RITE CARE NOWRIte Care covers 126,000 enroll-
ees—12% of Rhode Island’s popula-tion. More than 70,000 are children -one third of all children in Rhode Is-land. While almost all of RIte Care’s ini-tial 70,000 enrollees in 1994 receivedcash assistance, now more than threequarters are working families, living ator near the poverty level, who are notoffered health insurance coverage atwork, for whom RIte Care coverage is
their only “public” benefit, and who, ifnot for RIte Care, would be without in-surance.
As the nature of the enrollees haschanged—from families primarily oncash assistance to families who are prima-rily working—RIte care instituted co-payments:
• Working families above 150% ofthe federal poverty level ($24,900for a family of three) are requiredto pay a monthly premium be-tween $61 and $92. A total of12,000 enrollees, less than 10% ofthe program’s enrollment, areabove 150% of the poverty leveland are required to pay thismonthly premium.
• Any family eligible for RIte Carewho is offered health coverage atwork is required to enroll in thatcoverage. Through the creation of“RIte Share” in 2001, state andfederal funds under the RIte Carewaiver can be used to help eligiblefamilies pay the monthly premium
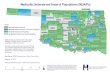
Percent of Women who Received Adequate/Adequate+Prenatal Care by Insurance
Status 1993-2003
charged by their employer. Thereare currently 6000 RIte Share en-rollees – these families are enrolledin insurance at work, receive helppaying their monthly premium in-stead of enrolling in RIte Care, andthe state saves approximately $2.2million annually.
The state and federal government, theenrolled families, and often the family’semployer now share responsibility forhealth insurance. These changes haveslowed RIte Care’s enrollment growth,while ensuring that families with access toemployer-sponsored coverage can remainin or enroll in coverage at work.
Fundamental Changes toMedicaid’s Health Care DeliverySystem
Although the program requiredhealth plans to include traditional safetynet providers in their networks, the pro-gram expsnded to include all the provid-ers in the plans’ networks, and ensuredthat each individual had a primary carephysician. RIte Care plans increased phy-sician reimbursement from the fee-for-service Medicaid rates, and tripled pri-mary care provider participation (from350 physicians pre-RIte Care to over 900physicians post-RIte Care). Within RIteCare’s first year, the number of physicianvisits went from an average of two peryear per enrollee to almost five visits peryear.
With the increase in care providedby community-based physicians came areduction in both inpatient hospitaldays and emergency department (ED)visits. The federal waiver requires RIteCare to limit program expenditures tono more than a 6% increase annuallyper enrollee, using pre-waiver Medic-aid expenditures for the AFDC popu-lation as the baseline. In fact, when bothphysician reimbursement rates and phy-sician visits increased significantly in RIteCare’s first year, the total program ex-penditures remained within the pre-scribed limit of the waiver. The dramaticreductions in both ED use and prevent-able inpatient stays essentially “funded”the increased investment in communitybased physician services. This was theprogram’s intent.

393VOLUME 89 NO. 12 DECEMBER 2006
Pay for Performance results in”America’s Best Health Plans”recognition
In 2005, US News and World Re-port (”America’s Best Health Plans”)ranked Medicaid health plans, usingNCQA HEDIS scores. All three ofRhode Island’s RIte Care Health Plansplaced among the top six among allhealth plans in the nation participatingin Medicaid managed care.3 In 2006,they placed in the top four.
Since 1998, health plan contractshave had a pay-for-performance com-ponent based on improvements inHEDIS and other performance mea-sures (e.g., member services, preven-tive services, clinical care, and chroniccare management). Because RIte Care-participating plans are NCQA-accred-ited, the State has access to theHEDIS® data for the plans’ RIte Carepopulation, as well as for their commer-cial population, and uses these andother measures to track, measure, andreward exemplary performance. Therehas been significant and steady im-provement over the seven years that theperformance measures have been inplace in virtually every measure for allthree plans.4
The Commonwealth Fund5 high-lighted RIte Care: “Rhode Island’s ex-perience illustrates that much can bedone to improve quality as well as effi-ciency through relatively modest qualityimprovement initiatives.”
NATIONAL RECOGNITIONMany articles have cited RIte Care’s
success in expanding access to the unin-sured, improving access and quality ofcare, while maintaining the per personannual rate of inflation at about half theinflation rate for commercial insurance.5
• In 2001, DHS received a Pur-chaser Award from the NationalHealth Care Purchasing Institutefor the program to recognize DHS’“value purchasing” managementphilosophy.
• In 2003, the National Health PolicyForum at The George Washington
University reviewed RIte Care andRIte Share: Doing It RIte: Explor-ing a Decade of Health Care Inno-vation. They reported:7
“The RIte Care program has beenwidely heralded as a success andan illustration that not all man-aged care is alike. Ongoing evalu-ations of the program have foundincreased enrollee access to pri-mary care, specialty services, andimproved health outcomes. And97% of enrollees indicate thatthey are satisfied with RIte Care.”
ENROLLEE SATISFACTION• Since 1996, between 95% and
97% of enrollees reported that theywere very satisfied or satisfied withthe services of their “regular doc-tor”;
• During that same time, between 96%and 98% of RIte Care enrollees re-ported that, overall, they were verysatisfied or satisfied with RIte Care;
In the 2004 enrollee survey:• Almost 82% of respondents report
that they (or their child) saw theirdoctor the same day they called foran appointment when sick;
• 97% of respondents said they wereseen either the same day or the nextday;
• 93% of respondents reported that
Annual Well Child VisitsRIte Care vs. US Medicaid vs. US Commercial Insurance
Ages 3 to 6
US Commcerial
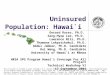
Rhode Island’s Postneonatal Mortality Rate Declines forPublicly Funded Births Rhode Island Postneonatal Mortality
by Insurance Status1990-1999

394MEDICINE & HEALTH/RHODE ISLAND
they had seen their regular doctorwithin the past 12 months;
• Almost 92% of respondents saidthey were either very satisfied orsatisfied with reaching their regu-lar doctor during evenings, nights,weekends, and holidays; and
• Nearly 95% of respondents saidthey were very satisfied or satisfiedwith getting a referral to a special-ist.
SUCCESS IN ACHIEVING ALLTHREE PROGRAM GOALSGoal 1: RIte Care has ImprovedAccess, Quality and HealthOutcomes
“Rhode Island has the bestrecord in the country at pro-viding women with prenatalcare. Credit goes to its RIteCare program, which has im-proved children’s health gener-ally. The key to this managed
care effort comes in setting stan-dards for provider performanceand then following up to see thatthey are met. Attention to pre-and post-natal care results inlower infant mortality.”
– Governing Magazine6
RIte Care has improvedprenatal care
• Adequacy of prenatal care im-proved for pregnant women onMedicaid/RIte Care, from 70% in1993 (pre-RIte Care) to 82% in2003 (RIte Care), narrowing thegap between women with publicand with private health coverage inRhode Island.
• The percentage of pregnantwomen on Medicaid who smokedduring pregnancy decreasedfrom 33% in 1993 to 20% in2003.
• Short interbirth interval (i.e., lessthan 18 months) is associated withlow birth weight. The number ofwomen on Medicaid waiting at least18 months between births increasedfrom 58% of pre-RIte Care (1993)to 72% post-RIte Care (2003), clos-ing the gap between women withpublic and with private health cov-erage in Rhode Island.
Percent Uninsured Rhode Island Children (under 18) 1995-2005
Lead Poisoning Rates Decline as Lead Screening RatesImprove In RIte Care Two Year Olds
1997 vs. 2003

395VOLUME 89 NO. 12 DECEMBER 2006
Numbers of well-child visits also in-creased. In 2004, 79% of the childrenbetween the ages of 3 and 6 enrolled inRIte Care had timely well child visits. Thiscompares favorably to the rates for Med-icaid-enrolled children nationally (58%)as well as to the rate for children enrolledin commercial health plans across thenation (58%).
Infant Mortality Rate ReducedSignificantly
Infant mortality data point to RIteCare’s success.7 From 1990 to 1999, theinfant mortality rate declined 36% for in-fants born in RI with public insurance,from 10.7 deaths per thousand births to6.8 deaths per thousand births. The gapbetween the publicly insured infant mor-tality rate and privately insured infantmortality rate was reduced, from a gap of4.3 deaths per thousand births in 1990to 1.5 deaths per thousand births in 1999.
The infant mortality rate combinesneonatal mortality, deaths within the first28 days after birth, and post neonatal mor-tality, deaths from 29 days to one year. Theneonatal mortality rate can be influencedby access to specialized neonatal intensivecare. In fact, technology and other im-proved access to such care have served toimprove neonatal infant mortality ratesacross the nation over the last decade.
Neonatal mortality for Rhode Islandinfants with public insurance decreased23%, from 6.2 deaths per thousandbirths in 1990 to 4.8 deaths per thou-sand births in 1999.
Postneonatal mortality is considereda measure of access to pediatric care.8
The postneonatal mortality rate forRhode Island infants with public insurancedecreased more sharply, by 57%, from 4.5deaths per thousand births in 1990 to 1.9deaths per thousand births in 1999.
This sharp decline in postneonatalinfant mortality is not reflected in the restof the nation, and can be assumed to bedue to improvements in access to pediat-ric care. The causes of death includeSIDS, congential anomalies, infections,and prematurity.
Lead Poisoning is ReducedSignificantly
In 1997 Brown University research-ers studied two year-olds enrolled in RiteCare: 79% received timely screening for
lead poisoning, a rate dramatically higherthan those published in national surveys.9
The study also showed an alarming re-sult: 29% of the children screened hadblood lead levels that were consideredlead-poisoned by the Centers for DiseaseControl and Prevention (CDC), a ratethat was significantly higher than nationalreported rates of childhood lead poison-ing (at 8.6%).11
Today RIte Care children with leadpoisoning are enrolled in “Lead Cen-ters.” Located in urban areas, Lead Cen-ters ensure that the family receives helpin creating and maintaining a lead-safeenvironment in their home. In 2003,Brown University researchers conducteda new study on RIte Care two year olds.The already high timely lead screeningrate of 79% increased to 88%. The rateof lead poisoning plummeted from 29%to 17% .
Goal 2: RIte Care ReducedUninsurance in Rhode Island
By 2000, RIte Care had reduceduninsurance among Rhode Island chil-dren and families. In 2002 Rhode Islandhad the second lowest rate of uninsuredin the nation, surpassed only by Vermont.
Since 2000, as health care costs haverisen, the level of uninsurance across all stateshas risen. Uninsurance among all Rhode Is-landers had dropped from 12.9% in 1995to 5.9% in 2000, the lowest in the nation. By2005, level of uninsurance in RI was 11.8%.Uninsurance among children dropped from12.5 % in 1995 to 2.5% in 2000, the lowestin the nation. By 2005, the rate ofuninsurance in children had crept up to 7.7%,12th in the nation. Without RIte Care,
Rhode Island’s rate of uninsurance would berising even more quickly.
Goal 3: To contain the growthof health care costs forMedicaid/RIte Care enrolledfamilies
RIte Care has limited the annualgrowth in expenditures to no more than6 % for each enrollee over the past 8years, as required under the federalwaiver. This 6% growth is less than halfthe double digit rate of growth experi-enced during this time by commercialhealth insurers. In the early 1990s, preRIte Care, the situation was the oppo-site—the cost of covering Medicaid fami-lies was increasing at 8%, twice the rateof growth in the commercial market,which was then 4%. Among the waysRIte Care has limited expenditures:
• The newly created RIte Share off-sets public costs by requiring eligiblefamilies to enroll in employer spon-sored coverage whenever available,
• Monthly premiums paid by fami-lies over 150% of the poverty level
• Ensuring that RIte Care is alwaysthe “last payor,” by identifying allopportunities for enrollees to becovered by commercial insurance,Medicare, etc.
But the most effective way that RIteCare has limited expenditure growth isthe same method the program has usedto improve access, quality and health out-comes—by following these basic prin-ciples of an efficient, high-performinghealth system:
• Ensure access to primary and pre-ventive care, including timely accessto community-based urgent care,
• Ensure that enrollees with chronicdisease or other health conditionsare identified promptly and receiveongoing chronic care management,
• Ensure that all care provided is evi-dence-based, and
• Ensure that all care is provided inthe most appropriate, least restric-tive setting.
Governing Magzine10 noted, in a ref-erence to RIte Care:
“A few states have revamped theirorganization and managementsystems to ensure better access to
The dramaticreductions in both
ED use andpreventable
inpatient staysessentially “funded”
the increasedinvestment in
community basedphysician services.

396MEDICINE & HEALTH/RHODE ISLAND
medical care and by keeping costsin control. Rhode Island standsout in this respect.”
FUTURE CHALLENGES AND PLANSRIte Care has plans for thefuture
Oral health care was not part of thehealth plan’s contract, and remained infee-for-service Medicaid—until now. Be-ginning September first, children are en-rolling in RIte Smiles. Like RIte Care,children enroll in a dental plan, whichwill provide access to care through itsprovider network, focusing on primaryand preventive care. United Healthcare’sdental plan is enrolling RIte Care chil-dren under a contract with the state, be-ginning with 35,000 children age 6 andunder.
Births to teens in Rhode Island out-paces every other New England state.11
Of the 1200 teenagers each year whogive birth, two- thirds enroll in RIte Carefor themselves and their infants. Address-ing this issue would help control RIteCare costs by controlling the program’sgrowth.
The biggest challenge to RIte Careis beyond the scope and control of theprogram –the continuing escalation inthe cost of health care.
Escalating health care costs hits RIteCare in two ways:
• With the limits imposed by the fed-eral waiver and the state budget,health care costs that are increas-ing beyond the rate of inflation willcreate a structural deficit that hasto be addressed each year by find-ing additional ways to offset pro-gram costs.
• The continued erosion of em-ployer-sponsored health coveragewill create a continual demand forRIte Care.
Addressing the escalation in the costof health care will be critical for RIteCare’s sustainability.
REFERENCES1. US Bureau of the Census, Current Population
Survey, 19952. Aid to Families with Dependent Children3. http://www.usnews.com/usnews/health/best-
health-insurance/rankings/medicaid.htm.4. http://www.ritecareresearch.org/reportspubs/
RIteCare/RCPerfIncentiveProgram-Oct03.pdf5. Silow-Carroll S. Building Quality Into RIte Care:
How Rhode Island Is Improving Health Care forIts Low-Income Populations: Field Report, TheCommonwealth Fund, January 2003:p21.
6. h t t p : / / w w w. r i t e c a r e r e s e a r c h . o r g /nationalpubs.html
7. National Health Policy Forum. Doing It RIte:Exploring a Decade of Health Coverage Innova-tion, The George Washington University, May27-29, 2003.
8. Children’s care. Governing February 2004.9. http://www.ritecareresearch.org/reportspubs/
RIteCare/RI_InfantMortal_90-99_2002.pdf10. Centers for Disease Control. “Postneonatal mor-
tality surveillance – US 1980 – 1994. MMWR1998; 47 (15).
11. Kaufmann RB, et.al. Elevated blood lead levelsand blood lead screening among US children agedone to five years: 1988 – 1994. Pediatrics 2000;106(6).
Tricia Leddy, administrator of RIteCare from 1994-2006, is Chief of Staffand Associate Director of the Rhode IslandDepartment of Mental Health Retarda-tion and Hospitals.
CORRESPONDENCETricia LeddyRhode Island Department of MHRH14 Harrington RdCranston, RI 02920Phone: (401) 462-6005e-mail: [email protected]

397VOLUME 89 NO. 12 DECEMBER 2006
Serving the Spectrum of Needs in CommunityHealth Centers
Dennis Roy�RHODE ISLAND’S COMMUNITY HEALTHCENTERS have served as a safety net forour residents for close to forty years. TheHealth Centers’ collective mission is toprovide comprehensive health care topatients regardless of their ability to pay,thereby reducing dispairties in care.
HISTORYWhat is today a movement of over
1,000 health centers serving 15 millionpeople began in December, 1965, in asmall office in Boston’s Columbia PointHousing Project, as a project of the TuftsMedical School. A rural health center inMississippi along with urban centers inChicago, Denver, Los Angeles and Provi-dence, Rhode Island, (1968) followed. From the beginning health centers werededicated to providing accessible and af-fordable quality health care.. Located inlow income neighborhoods, the Centersinvolved patients not only in their healthcare but in the governing structure of thehealth center.
The Public Health Services Act es-tablished the community health centerprogram. There are two types of commu-nity health centers, those that meet thequalifications for coverage and paymentthrough Medicaid and Medicare, andthose which also receive funding underSection 330 of the PHSA. Currently thereare 1018 Section 330 health centers and97 “look-a-likes” who received enhancedrates but no federal funding. All healthcenters must meet four basic standards tobe deemed federally qualified:
1. They must be located in or serve a
medically underserved commu-nity; one with a high proportion oflow-income persons as well as acommunity with demonstrably el-evated levels of death and disabil-ity from preventable causes.
2. They must offer a comprehensiverange of primary health services aswell as supportive services includ-ing translation and transportation.
3. They must adjust fees on a pub-lished sliding fee schedule andmust provide services without re-gard for the patient’s ability to pay.
4. They must be governed by a Boardof Directors, a majority of whosemembers are center patients. Thisgoverning structure makes eachhealth center unique, allowing fordirect patient feedback regardingthe quality of care.
The Rhode Island Health CenterAssociation (RIHCA) is the PrimaryCare Association for all CommunityHealth Centers statewide. Our organi-zation represents 10 Federally QualifiedHealth Centers, the state’s Health Carefor the Homeless program and one is-land-based medical center, incorporating33 locations including school basedhealth centers and one mobile van.
WHO ARE THE PATIENTS?In 2004 our centers served over
103,000 unduplicated patients. This isnearly 10% of the total state population.Our Health centers serve patients fromevery city and town in Rhode Island. Inaddition, they serve patients from thePawcatuck/Stonington area in southeast-ern Connecticut, the Blackstone/Bellingham area in Massachusetts andthe Attleboro/Seekonk area in SouthernMassachusetts. Over 20% of our patientsare uninsured; the number of center-patients without insurance rose by morethan 3,500 in 2004 from the previousyear. According to the 2004 UniformData System of the Bureau of PrimaryHealth Care, 37% Health Center pa-tients are best served by a language otherthan English. In Rhode Island, 35% ofthe health center population is reportedas Hispanic, four times the percentageof the state’s Hispanic population. Ninepercent of the health center patients arereported as African-American, twice thestate rate.
CHALLENGES: POVERTY,DISPARITIES
One in five Rhode Island childrenlives in poverty. According to the US cen-sus, childhood poverty in Rhode Islandincreased from 16.7% in 22000 to 21%in 2004, above the national rate of18.4%. In parallel, the number of unin-sured children in Rhode Island is also ris-ing. According to the Rhode Island KidsCount Fact Book (2006 Rhode IslandKids Count Factbook) 5.8% of RhodeIsland’s children under age 18 are unin-sured. This number has been increasingin the last few years.
The percantage of uninsured adultsis 10.8%; this number is also rising.One reason for the increase in the un-insured rate is the institution of RiteCare/Share premiums. Another con-tributor is the decline in employer-spon-sored insurance. According to the 2003Behavioral Risk Factor SurveillanceSystem, (BRFSS) the number of unin-sured working Rhode Islanders rosefrom 7.6% to 8.3% between 2002 and2003. This 1% increase represents4,415 newly uninsured employedRhode Islanders.
The Rhode Island Public Expendi-ture Council’s (RIPEC) FY 2006 Medic-aid Report, A RX for Reform, forecaststhat Medicaid’s growth will continue tocreate large structural problem in the state’sbudget unless a vigorous program of en-titlement reform and cost containment ispursued. The projected national budgetcuts will cut 10 million dollars in federalMedicaid funding to Rhode Island. InRhode Island 10% of the population re-ceive their health care at community healthcenters. Of the over 100,000 that receiveservices, 30,000 are uninsured; there is areal threat, to patients and to the solvencyof Health Centers, that those numbers willgrow.
COMBATING HEALTH DISPARITIESEliminating health disparities by
2010 is an important stated goal for thenation and the state. The Rhode Island

398MEDICINE & HEALTH/RHODE ISLAND
BRFSS has identified nine risk indicatorsfor which significant racial and ethnic dis-parities exist: firearms in the home, bingedrinking, lack of physical activity, obesity,tobacco use, unable to afford a doctor, noregular provider, fair or poor generalhealth, and lack of health insurance. InRhode Island the percentage of blacks,Hispanics and Asian and Pacific Islanderswith no health insurance is more thantwice the rate for whites. The 2004 BRFSSreports 20% of males and 9% of femaleshave no regular provider. According toBRFSS, Rhode Island has one of the high-est adult asthma prevalence rates in thecountry. Rhode Island Department ofHealth reports that Rhode Island ranksfifth in the nation in the prevalence ofasthma among adults (9.6% as comparedto 7.7% nationally). Asthma is the num-ber one chronic condition in children andthe third ranked cause of hospitalizationin children under fifteen. African Ameri-can children are more likely than whitechildren to suffer from asthma. RhodeIsland Department of Health dischargedatabase reports that the rate for asthmarelated hospitalizations was 7.8% for Af-rican American children vs. 2.9% forwhite children. Because the healthcenter’s African American population istwice the state rate, the need for asthmaeducation for health center patients andstaff is great.
The prevalence of diabetes in RhodeIsland increased by 52% from 1996through 2001. This increase was great-est among Hispanics/Latinos and people45-64 years of age. Rhode Island’s in-crease was reflected in an increase in dia-betic patients at the health centers. In2001 diabetes contributed to the deathof 759 residents of Rhode Island.
WHAT ARE THE SERVICES?Rhode Island’s Community Health
Centers provide a wide spectrum of ser-vices, including:
Adult MedicinePediatric and AdolescentMedicineFamily MedicineOB/GYNLab servicesRadiologyPharmacySubstance Abuse CounselingHearing Screening
Mental Health CounselingVision ScreeningHealth EducationNutrition CounselingDental CareFamily PlanningHealthcare for the HomelessHIV: Primary Care and Support
ServicesSchool Based ProgramFood PantryTransportation AssistanceCase Management/Disease
Management
Within this set, Community HealthCenters put special focus on those aspectsof care often under-represented in tradi-tional service systems: Oral Health, Men-tal Health, and Social Service.
ORAL HEALTH NEEDSIn Rhode Island, a number of fac-
tors contribute to the shortage of den-tists. Many dentists are aging and fewindividuals are establishing new practicesin Rhode Island; this in part is due to thefact that Rhode Island has no dentalschool. Those who are practicing limittheir number of Medicaid patients, inpart because of the low Medicaid reim-bursement rate. In addition, Medicaidin Rhode Island does not cover all oralhealth care services. This dental challengeis greatest for Rhode Island’s nursinghome residents. Annually there are ap-proximately 11,750 Medicaid recipientsin Rhode Island nursing homes but in atwo year period from 2001-2002, only29% received any dental services. Lowreimbursement is a primary reason. Oralhealth disease is the top chronic diseasefacing children. Rhode Island HealthCenters have acted as a safety net by es-tablishing full service practices through-out the state and by establishing school-based portable dental operations. In ad-dition, three health centers havepartnered, (East Bay Community ActionProgram, Comprehensive CommunityAction Program, Thundermist) to create“The Molar Express” in conjunction withRonald McDonald House Charities tobring a fully operational mobile dentalvehicle to local elementary schools this fallto provide comprehensive oral health ser-vices..
Eight centers in our network pro-
vided over 27,500 visits for over 11,600Rhode Islanders in 2005. We are readyto continue our critical role in providingaccess as the State of Rhode Island un-folds its new dental benefits manager pro-gram. In fact, Community Health Cen-ters will be a critical element in the suc-cess of this program as they have been inthe success of Rite Care.
Community Health Centers are cre-ating solutions to the lack of oral healthaccess for nursing home residents. A con-sortium of health centers includingEBCAP has replied to the Departmentof Human Services request for dental ser-vices for nursing home residents.
MENTAL HEALTH NEEDSThe Rhode Island Department of
Health’s BRFSS (2004) states that 34.6%of adults in Rhode Island report havingpoor mental health. In 2004, RhodeIsland’s health centers treated 4,000 pa-tients for depression, with an average ageof 38 years. Some Rhode Island HealthCenters have co-located mental healthproviders within their practices, a servicethat shows promise for the future in con-centrating patient care under one roof.At EBCAP, we are working closely withEast Bay Mental Health and NewportCounty Mental Health. Our providers,using a screening tool for mental healthconcerns, can refer patients to on-site cli-nicians for further diagnosis and follow-up. EBCAP uses federal health centergrant funds to support screening andtreatment.
SOCIAL SERVICES FOR PATIENTSIn 1991 the Department of Health
began the Family Resource Counselorprogram at health centers and some hos-pitals to screen pregnant women for pub-lic benefits. In 1998 the Department ofHealth and the Department of HumanServices collaborated to expand the Fam-ily Resource Counselor (FRC) Networkto include assisting with the Rite Care ap-plication.
In 2006, the network consists of al-most 60 individuals located at all healthcenters including school based health cen-ter sites, most hospitals and one commu-nity based organization. The network ismanaged by the Rhode Island Health Cen-ter Association through a contract with theDepartment of Human Services. The Family

399VOLUME 89 NO. 12 DECEMBER 2006
Resource Counselors screen and refer pa-tients to public benefit programs and assistpatients with the RIte Care/Share (RhodeIsland’s Medicaid program) application.
Family Resource Counselors areavailable for all health center patients aswell as the general public. They receivereferrals from the Department of HumanServices, the Department of Health andthe three health plans. They speak six lan-guages, in addition to English; Spanish,Portuguese, Cambodian, Creole, French,and Cape Verdean.
Community Health Centers employsocial workers. For example, EBCAP pro-vides a full array of social services rangingfrom Head Start for children, Women, In-fants and Children Program (WIC), assis-tance with heating bills in the winter andcase management services for seniors, thehomeless and teens. Community HealthCenters are experienced in combining pri-mary health, oral health, mental health andsocial services to the patient at one site.
OUTCOMES/PERFORMACEMEASUREMENT
All Health Centers have achievedJoint Commission on Accreditation forHealth Care Organizations (JCAHO)accreditation and are committed to pa-tient safety and quality improvement, asevidenced by participation in state andnational quality collaboratives.
To address the needs of patients withchronic diseases, 80% of our centers par-ticipated in Health DisparitiesCollaboratives for asthma, diabetes and de-pression. These Health DisparitiesCollaboratives, initiated in 1999, are in-tended to address the reality that racial andethnic minorities suffer disproportionatelyfrom health problems, including infantmortality, asthma, cancer, HIV/AIDS, anddiabetes. The Collaboratives bring to-gether health center teams for 12 to 16months, under the guidance of nationalexperts, to effect rapid improvements incare for patients with chronic conditions.
Goals include improving the skills of clini-cal staff, ensuring that care is comprehen-sive and proactive, and effectively educat-ing patients on self-management of theirconditions.
Health Disparities Collaboratives andJCAHO accreditation mark CommunityHealth Centers’ drive to integrate qualitygoals and performance measurement intodaily work. 2005 HEDIS rates indicatethat the Health Centers surpass others inthe provider network of NHPRI for child-hood immunization and testing andscreening for patients with diabetes. Ninehealth center sites have re-worked theirappointment systems to deliver OpenAccess. Yearly the CHCs assess the satis-faction of our patients with our services.
As state lawmakers think about howto provide services to Rhode Island’s in-creasingly diverse communities, communityhealth centers are poised to lead the way.Health centers are experts in deliveringhigh quality health care, but they also knowtheir patients and have developed provenmethods of managing the chronic diseaseswhich affect their patients’ lives.
A COMMUNITY RESOURCEAll health centers are engaged with
the Department of Health Center forEmergency Response and Preparedness.Since 2004 all 12 health center organiza-tions meet with HEALTH under RIHCAleadership to develop emergency pre-paredness plans that include surge capac-ity, and meeting the needs of clients whohave both medical and behavioral needs.Rhode Island Health Centers have aprominent place in State planning forpandemic flu. All the health centers areactively engaged in training their clinicaland non clinical staff to address responseand each is organizing their own incidentresponse teams. Examples of communityservice during past health crises follows:
• In October 1996 when a true out-break of meningococcal disease oc-curred in Northern Rhode Island,
health centers were an integral partof the mass vaccination campaigntargeting 2-29 year olds. This masscampaign assisted in stopping theoutbreak.
• In February of 2003 Rhode Islandexperienced its worse fire in history,the Station nightclub fire. HealthCenter directories were delivered tothe Department of Human Service’scommand center for DHS staff toassist in making referrals to healthcenters. Many Family ResourceCounselors volunteered to help. In2005 when hurricane Katrinaevacuees were moved from the GulfCoast to Middletown, health cen-ters provided medical and dentalcare as well as prescription needsand food pantry services for thesedisplaced individuals. Again, theFamily Resource Counselors volun-teered. All the evacuees (200+) weremanaged by staff of East Bay Com-munity Action Program.
Because health centers are in 28 lo-cations across the state, we are positionedto be an effective and efficient system tomeet the daily needs as well as the emer-gency needs of Rhode Islanders.
Since 1965, Community HealthCenters have provided care for peoplewho are uninsured, under insured orparticipating in Medicaid-based pro-grams.
ACKNOWLEDGEMENT:Thanks to the staff of the Rhode Is-
land Health Center Association, who pro-vided significant support for this article.
Dennis Roy is the Chief Executive Of-ficer of East Bay Community Action Pro-gram, a full service health, dental and socialservice organization with Health Centerslocated in East Providence and Newport.
CORRESPONDENCEDennis RoyEast Bay Community Action Program19 BroadwayNewport, RI 02840Phone: (401) 848-6697,x301E-mail: [email protected]
RHODE ISLAND’S COMMUNITY HEALTH CENTERS:Blackstone Valley Community Health Center, Thundermist Health Centers ,Providence Community Health Centers, Wood River Health Services, North-west Health Center, CCAP/Family Health, Crossroads Rhode Island, East BayCAP, Tri Town Health Center, Chad Brown Health Center, Block IslandHealth Services and Bayside Family Healthcare.

400MEDICINE & HEALTH/RHODE ISLAND
Opportunities For Improved Quality and AccessIn the Office Setting
Chris Campanile MD, PhD
QUALITY IMPROVEMENT 101 WAS NOT OF-FERED after Pathology in our second yearof medical school or as a fourth-year elec-tive. Nor was it part of our residency cur-riculum. Physicians are trained to elicit ahistory, examine, assess and plan, patientby patient. We know the course and out-come of individual patients, but we sel-dom know how we’re doing caring forthe entire population of patients we see.We strive to implement evidence-basedguidelines for our individual patients butare generally not aware of our perfor-mance in satisfying such measures for ourentire patient-population.. We are not ac-customed to practicing Population-BasedMedicine.
OUTSIDE OF OUR OFFICES: THEBROADER CONTEXT FOR QUALITYIMPROVEMENT
In the hospital setting, accreditationorganizations such as the JCAHO (JointCommission on Accreditation ofHealthcare Organizations) are strongoutside motivating forces. To overseephysician performance, the Federal gov-ernment created Professional Stan-dards Review Organizations (PSRO),established by the Social SecurityAmendments of 1972. The Health CareFinancing Administration (HCFA) ad-ministered Peer Review Organizations(PRO), whose stated purpose was to“curb the growth in expenditures forhealth care” and “assure the quality ofcare delivered.” The law allowed sanc-tions, including lack of payment for ser-vices. These approaches often dismayedphysicians, who complained of: inaccu-rate and incomplete data, differences injudgment regarding individual patientcare, limited evidence-based data onwhich to set performance targets, andinadequate tools to achieve these targets.The measures also were viewed aslargely about cost containment and astaking a punitive rather than support-ive approach to quality.
The Centers for Medicaid andMedicare Services (CMS) replaced
PROs with Quality Improvement Orga-nizations (QIO) to promote care in theMedicare and Medicaid populations.The physician office setting is one of fourareas of focus, along with home health,nursing homes, and hospitals. Statewidequality organizations compete for theQIO contract for their state. A contractruns for 3 years and is termed a Scope ofWork (SOW). Quality Partners of RI isthe QIO for Rhode Island. We are cur-rently in the 8th Scope of Work, whichemphasizes health information technol-ogy (HIT), chronic illness care, and cul-tural competency in providing care todiverse populations.
In the outpatient setting Commu-nity Health Centers (CHCs) wereamong the first practices to adopt for-mal QI programs. CHCs fall under theBureau of Primary Health Care/HealthResources and Services Administration(HRSA) of the Department of Healthand Human Services. Those CHCswhich are ‘federally qualified’ regularlysubmit a grant to receive funds to offsetcare given to un- and underinsured pa-tients. The clinical portion of thesegrants requires the submission of dataon a number of health measures and theCHC’s plan for improvement. In addi-tion, CHCs have been required to par-ticipate in Health DisparitiesCollaboratives, a HRSA initiative begin-ning in 1998 with involvement from theInstitute for Healthcare Improvement(IHI). These Collaboratives seek to im-prove chronic illness care for diabetes,depression, asthma, and cardiovasculardisease.
THE FRAMEWORK FOR IMPROVINGQUALITY
The RI Department of Health(RIDOH), and in particular, the Dia-betes Prevention and Control Program(DPCP), have been instrumental inbringing the Health Disparities Col-laborative model to a wider array ofpractice settings in Rhode Island. Foryears the DPCP ran a Collaborative-like
QI diabetes program called CHIP(Community Health ImprovementProgram) for CHCs and some hospital-based clinics. Driven by a desire tospread this model of chronic care im-provement and collaborative learning,the RI Chronic Care Collaborative(RICCC) started in the spring of 2003.This program is based on the nationalHealth Disparities Collaboratives thathad previously been run only withCHCs. This included adopting theChronic Care Model (CCM) developedby Dr. Ed Wagner and colleagues at theMacColl Institute for Healthcare Inno-vation2 as well as the rapid cycle Im-provement Model and the IHI’s Learn-ing Model. What the RICCC created,for the first time, was a Collaborativecomposed of CHCs, hospital-based clin-ics, and private practices. By doing this,the RICCC promoted the spread of achronic illness care program from CHCsto private practices.
Dr. Don Berwick and the Institutefor Healthcare Improvement developedThe Collaborative Learning Model. Itis composed of four conferences thattake place over the course of a year: 3Learning Sessions and an OutcomesCongress. In the original CHC HealthDisparities Collaboratives these Learn-ing Sessions might take place over 2 to3 days. The RICCC, in deference to thesmaller private practices now participat-ing, has modified these conferences totake place during evening and half daysessions. The Outcomes Congress occursat the end of the yearlong cycle of train-ing. Government, health, academic andbusiness leaders are invited to the Out-comes Congress. The Learning Sessionsare supplemented by monthly confer-ence calls, an email listserve, , and sitevisits by RICCC faculty. The time in-tervals between Learning Sessions aretermed Action Periods. During this timepractice teams innovate, test, and imple-ment improvements into their model ofcare.
�

401VOLUME 89 NO. 12 DECEMBER 2006
BEYOND THE FRAMEWORK: DOINGTHE WORK
The Improvement Model is basedon the work of Shewart and Demings,1
(the Plan, Do, Study, Act (PDSA) cycle):
• Planning refers to identifying anarea that needs improvement. Withdiscussion among staff who are fa-miliar with the related process(es),reasons for poor performance arelisted. Based on these, a specific in-novation is planned. An examplefrom the RICCC involves the goalof having patients with diabetes re-move their shoes and socks beforetheir provider enters the examroom.
• The innovation (Do) is as follows:signs will be posted in the examrooms of Dr. E; starting tomorrow,Dr. E. will note whether the nextten diabetes patients she sees hasshoes and socks off. Dr. E. does thisand notes that the sign was not par-ticularly prominent and also wasnot in the appropriate language forsome patients.
• The group met again for twentyminutes a few days later to review(Study) the data. Four out of 10 pa-tients had shoes and socks off whenDr. E. entered the exam room. Dr.E. passed along her observationsabout the signs.
• Act involves one of three options:toss out the idea because it appearsto have no merit, modify the ideaand test again, or implement theidea because it appears optimal ornearly so. This group decides tochange the signs, making themmore prominent, with Spanish andPortuguese versions.
The cycle continues. The next roundof testing resulted in 7 or 10 patients withshoes and socks off. The next innovationwas to have the medical assistant verballyremind the diabetes patients to take offshoes and socks (this depended on thesuccess of some parallel testing which en-sured that the M.A. knew the reason foreach patient’s visit). This round of test-ing resulted in 10 out of 10 patients withshoes and socks off by the time Dr. E.entered the exam room.
The Chronic Care Model (CCM)has as its premise the need to redesignone’s approach to chronic illness care toeffect significant improvement. TheCCM began as a pilot at Group HealthCooperative in Puget Sound and grew toinvolve over 70 ‘best practices.’ The ulti-mate goal of the Model is a productiveinteraction between an ‘informed, acti-vated patient’ and a ‘prepared, proactivepractice team..”3,4 Six components com-prise this Model:
1. Health System – Organization ofHealth Care. All levels of the orga-nization beginning with medicaland administrative leadership mustsupport this model. Ideally this vi-sion is reflected in the mission state-ment of the practice and incentivesare based on quality of care.
2. Delivery System Design. Physi-cians are encouraged to work withancillary staff and mid-level provid-ers as a team, each member havinga defined role. More complex pa-tients may require a case manage-ment style that incorporates otherprofessionals (e.g., nutritionists,mental health providers, socialworkers). In addition, alternativeformats for the patient encounter,such as group visits, should be con-sidered.. Increasingly, physiciansmust be cognizant of patients’ cul-tural backgrounds.
3. Clinical Information Systems.Data-driven improvement allows aphysician to know which patientsneed follow-up appointments,laboratory studies or visits to otherspecialists,. and to have a snapshotsummary of the patient’s clinicalstatus at the time of the visit.
4. Decision Support entails embed-ding this information into dailyclinical practice. It also means shar-ing these evidence-based guidelineswith patients as well as integratingspecialist expertise into the primarycare of the patient.
5. Self-Management Support refersto preparing and empowering pa-tients to manage their health care.Emphasis is placed on the patient’scentral role in disease-manage-
ment. Physicians must becomeskilled in brief clinical interventions; e.g., motivational interviewingand facilitating the patient’s passagethru the 5 A’s: Ask, Assess, Advise,Assist, and Arrange, originally de-veloped as part of smoking cessa-tion programs.6-8 This componentof the model sets it apart from rou-tine care of chronic conditions.
6. Community Resources makesphysicians aware of potentiallyhelpful resources in the commu-nity. For key programs the physi-cian or practice is encouraged tocreate a more formal partnership.For example, a physician mightpartner with a senior center whichhas exercise classes. The practicemight create a ‘referral’ form thatis given to the patient with infor-mation on the senior center.
The CCM has been implementedin Rhode Island through the ChronicCare Collaborative. The RICCC has nowcompleted two full cycles of the Learn-ing Model and began the 3rd year lastMay. This has involved 30 practice sitescomposed of a mixture of private prac-tices, community health centers, and hos-pital-based outpatient clinics and a totalof over 2500 patients. The average A1cfor the entire population is 7.6% whilethe proportion of patients with bloodpressure at goal (<130/80) is 41% andLDL-cholesterol at goal (<100) is 63%.These comprise the outcome measures.Some of the process measure perfor-mance are as follows: proportion withdocumented retinal eye exam: 27%, an-nual renal function screening via urinemicroalbumin/creatinine ratio: 50%, andpneumovax administration: 61%. Eightof nine measures showed improved overthe past two years.
Though the Chronic Care Modelassists with improving outcomes relatedto visits for chronic illness, a more basicquestion is: How easy is it for patients tobe seen when they want, especially if thatentails a same-day visit? Many practicesare implementing Open Access Sched-uling.,10,11 (also called “advanced access”or “same-day scheduling”) Patients withsame-day access usually make fewer emer-gency room visits and after-hours phone

402MEDICINE & HEALTH/RHODE ISLAND
calls. Patient satisfaction surveys indicatethat patients appreciate this model. Sev-eral practices in Rhode Island have imple-mented Open Access Scheduling and anopen access ‘collaborative’ run throughQuality Partners of RI has completed itsfirst year.
Two measures used to gauge the suc-cess of Open Access Scheduling are no-show rates and 3rd next available appoint-ment. The “third next available” appoint-ment is used rather than the “next avail-able” appointment since it is a more sen-sitive reflection of true appointmentavailability. Capitol Hill Health Center,a participant in the QPRI Open AccessCollaborative, reduced the no-show ratein its pediatric clinic from 24% to 8%over a nine month period. The numberof calendar days until the 3rd next avail-able appointment dropped from sixty tozero.
Health Information Technology is socritical to quality improvement that itbears further mention. The need for al-most real time reporting of data on largegroups of patients makes an electronichealth record (EHR) essential. An EHRmust not only facilitate documentationand transmission of information but alsoact as an interactive database able to pro-vide customized reports instantly. InRhode Island, a grant from the Agencyfor Healthcare Research and Quality(AHRQ) is funding the effort to create aCommunity Health Information Ex-change through which health data willbe shared by approved entities. The con-struction of this network has spurredother groups such as RI Primary CarePhysicians Corporation and EHR RhodeIsland to assist physicians in selecting andpurchasing EHRs which are compatiblewith the larger connectivity work occur-ring through the AHRQ grant. In addi-tion, QPRI administers DOQ-IT(Doctor’s Office Quality InformationTechnology), a CMS program designedto assist practices in choosing an EHR.Most importantly, health plans have be-gun to demonstrate that they also valuethe implementation of EHRs in doctors’offices: BCBSRI recently initiated Qual-ity Counts, a four year program whichrewards physicians first for using an EHRthat produces clinical reports and ulti-mately for demonstrating improvementin 10 health measures.
PRACTICAL SUGGESTIONS: THEHILLSIDE QUALITY IMPROVEMENTPROGRAM
Creating a quality improvement pro-gram in a practice requires less financialresources than sheer will. The needed in-gredients are: a clinical champion, a QIassistant, an administrative representativesuch as an office manager, an electronichealth record or a stand alone patient reg-istry or at least an electronic scheduling/billing module that includes diagnosiscodes, a forum to share results with otherphysicians and staff, and regular meet-ings of the quality group. At Hillside Av-enue Family & Community Medicine,the quality improvement group consistsof 4 people: myself, the physician oper-ating officer, a QI assistant, and the op-erations manager. Our QI assistant hasgenerally been a college graduate inter-ested in a career in health who is in a tran-sition year.
The major components of the QIprogram at Hillside divide into two cat-egories: a chronic care QI program whichoperates as part of the RICCC as de-scribed above, and a system to contactpatients who are due for chronic illnessfollow-up visits or for regular preventivecare visits. The RICCC QI program fo-cuses on diabetes and uses a standaloneregistry written in Microsoft Access calledCDEMS (Chronic Disease ElectronicManagement System). Once a diabetesvisit has occurred, an email is sent to theQI assistant. She takes the updated in-formation from the patient’s diabetessummary table in the EHR and enters itinto the CDEMS program, located on anetwork drive available to all Hillside us-ers. The QI assistant also generates themonthly data reports and Excel graphsrequired by the RICCC and posts thisinformation in a common area so that allstaff can view the results.
Importantly, for measures that arenot showing improvement, the QI assis-tant will generate a list of patients wholacked the marked activity; e.g., annualretinal eye exam, and contact these pa-tients. Measures that continue to fail toimprove are discussed at QI meetings.Out of that discussion comes an agree-ment to test an innovation that is pre-dicted to improve outcomes. For ex-ample, the PCP may fax a memo to theeye care specialist to facilitate documen-
tation of eye exams.In this type of disease-based QI
work it is essential to report performancedata monthly. To ascribe an outcome toa given intervention, regular measure-ment will provide data directly beforeand after that intervention. The trendover time will make up for what mightotherwise be a statistically insignificantchange.
The addition of a nutritionist to ourdiabetes care team has been integral tothe success of this program. We have en-couraged our nutritionist to attend col-laborative learning sessions and to be-come skilled in motivational interviewingtechniques.
I believe that if we are to improvethe care of patients with chronic illnesswe need a ‘chronic disease educator’ onthe health care team. This person wouldhave basic knowledge of several of themost common chronic illnesses and alsohave extensive training in the techniquesof motivational interviewing. Such a per-son would spend 30 to 60 minutes withthe patient, right before or after the phy-sician-visit. This person’s training wouldbe part of a nationally accredited pro-gram and their services would have anICD-9 or CPT code that would be re-imbursed by payers.
The other major thrust of the Hill-side QI program consists of contactingpatients who have CHF, COPD, DM,HTN, or asthma, and have not been seenin the previous four months. We also tar-get pediatric and adult patients who havenot been seen for an annual physical examwithin the past year. To generate thesereports we use our scheduling/billingsoftware. Our front desk staff will maketwo phone calls and mail one letter.
At Hillside we also use this work togenerate volume especially during a rela-tively slow season such as the summer andearly Fall. We have estimated the returnon our investment in this work by tabu-lating the cost of the staff doing the workagainst the projected collections for theappointments generated and have foundthat this work easily pays for itself. Regu-lar meetings are essential if a QI programis going to produce results. There shouldbe a regular time every one to two weeks.At Hillside the four of us meet for 30-60minutes most Tuesday mornings.

403VOLUME 89 NO. 12 DECEMBER 2006
MOVING FORWARDIf physicians undertake the task of
establishing a quality improvement pro-gram in their practice, the most difficultpart of this work will not be discoveringmore efficient and satisfying ways of do-ing things in your office. These improve-ments will be self-evident after sufficienttesting. Much more daunting is the Dif-fusion of Innovation,12 i.e., convincingyour fellow clinicians and support staffthat any new method is worth imple-menting throughout the practice.
Many professional societies offer as-sistance to physicians interested in start-ing a quality improvement program.. TheAmerican Academy of Family Physicians’website has a section on quality improve-ment.13 The seven year cycle of recertifi-cation of the American Board of FamilyPractice now requires that all physicianscomplete a Performance in Practice Mod-ule which is in essence a quality improve-ment project.
I urge all physicians to add a qualityimprovement program to their practicesto be well positioned for the time whenperformance data will be expected andrewarded.
REFERENCES1. The W. Edwards Deming Institute
www.deming.org2. www.improvingchroniccare.org/3. Bodenheimer T, Wagner EH, Grumbach K. Im-
proving primary care for patients with chronicillness. JAMA 2002;288:1775-9.
4. Bodenheimer T,Wagner EH, , Grumbach K. Im-proving primary care for patients with chronicillness Part 2 JAMA 2002;288:1909-14.
5. UK Prospective Diabetes Study. http://www.dtu.ox.ac.uk/index.html?maindoc=/ukpds/
6. Fiore MC, Bailey WC, et al. Treating TobaccoUse and Dependence. Quick Reference Guidefor Clinicians [monograph on the Internet].Rockville: U.S. Department of Health and Hu-man Services. Public Health Service; 2000 [cited2005 Feb 1]. Available from: http://www.surgeongeneral.gov/tobacco/tobaqrg.htm
7. Fisher EB, Brownson CA, et al. Ecological ap-proaches to self-management: the case of diabe-tes. Am J Public Health 2005;95:1523-35.
8. Glasgow R, Goldstein Mm et al. Translating whatwe have learned into practice.Am J Prev Med 2004; Aug;27(2 Suppl):88-101.
9. http://www.improvingchroniccare.org/research/randevaluation.htm
10. Murray M, Tantau C. Must patients wait? JtComm J Qual Improv 1998;24:423-5.
11. Murray M, Tantau C. Redefining open access toprimary care. Manag Care Q 1999;7(3):45-55.
12. Rogers EM. Diffusion of Innovations. The FreePress, 1995.
13. http://www.aafp.org/online/en/home/practicemgt/quality.html
Chris Campanile MD, PhD, is Clini-cal Coordinator, Quality Partners of RI,and Chair, RI Chronic Care Collabora-tive.
CORRESPONDENCEChris Campanile MD, PhDHillside Avenue Family & CommunityMedicine727 East AvenuePawtucket, RI 02860Phone: (401) 725-6160e-mail: [email protected]

404MEDICINE & HEALTH/RHODE ISLAND

405VOLUME 89 NO. 12 DECEMBER 2006

406MEDICINE & HEALTH/RHODE ISLAND

407VOLUME 89 NO. 12 DECEMBER 2006
Is Health Reform In Massachusetts a ModelFor Rhode Island?
David A. Rochefort, PhD�WHEN GOVERNOR CARCIERI ANNOUNCEDhis fiscal year 2007 budget in February,health care cuts figured prominently inthe plan to control expenditures. Recom-mended reductions in RIte Care andMedicaid, Rhode Island’s primary publicprograms for providing health insurancefor low-income families, amounted to $43million. Nearly 7,000 enrollees wouldhave become ineligible for continued cov-erage. Reacting to the governor’s proposal,an eclectic group of community, labor,health, and mental health groups joinedforces to block the changes.1 Ultimately,the General Assembly rejected most pro-posed cuts, but the episode dramatized theseverity of the state’s health care financingproblems while highlighting the programchanges that loom on the horizon.2
Against this backdrop, Massachusettshas adopted major new health insurancelegislation. Len Nichols of the NewAmerica Foundation has written, “Every-one interested in solutions to our healthsystem’s problems (and who isn’t?) is look-ing to Massachusetts in the wake of its re-cent landmark legislation.”3 According tosupporters, the new law will bring Massa-chusetts close to universal coverage by acombination of new requirements on busi-nesses and expanded government involve-ment in the insurance marketplace.
To what extent does the Massachu-setts approach present useful strategiesfor policymakers and health reform ad-vocates in Rhode Island? This article ad-dresses that question.
HEALTH INSURANCE PROBLEMS INRHODE ISLAND
According to the Robert WoodJohnson Foundation, “No one report cardexists on how the United States is faringon health insurance coverage. However,one thing is certain: the number of unin-sured is rising.”4 Latest estimates by the USCensus Bureau put the total number ofuninsured in the country at 46.6 millionfor 2005, up from 45.3 million in 2004.5
This figure represents 15.9% of the popu-lation. An increase in health insurance
costs, the decline of employment-basedcoverage, and eligibility limitations withinpublic programs have all contributed togrowth of the uninsured.
Although the situation in Rhode Is-land looks better than in many states, a par-allel reduction in health insurance cover-age has taken place here. In 2004-05, theuninsured reached 11.4% of the Rhode Is-land population.6 This statistic, the highestpercentage since the mid-1990s, caps aworsening trend that began after the state’suninsured bottomed out at 6.2% in 2000.Whereas Rhode Island had the lowestuninsurance rate in the nation that year, by2004-05 it was tied for eleventh place; Mas-sachusetts, at 10.7%, held seventh position
Not all population groups in RhodeIsland are equally likely to face coverageproblems. Males, residents between theages of 18 and 34, low- and middle-in-come earners, the unemployed, Hispan-ics, and those living in core cities are dis-proportionately affected.7 The compara-tively favorable insurance status of chil-dren and women reflects, in large part,
the RIte Care Medicaid managed careprogram, Rhode Island’s State Children’sHealth Insurance Program (SCHIP), andRIte Share, a premium assistance pro-gram to help low-income working fami-lies obtain coverage through their jobs.
Although most Rhode Islanders stillreceive health insurance through employ-ment, there have been extensive reductionsin coverage of this type similar to changesnationally. The share of the Rhode Islandpopulation covered by employment-basedhealth insurance fell from 70% in 2000 to62% in 2004.8 The most rapid decline oc-curred within the small business commu-nity. In addition, enrollees are facing higherpremiums, deductibles, and copayments.9
Health care costs in the UnitedStates are the highest in the world andcontinue to rise, raising questions aboutthe sustainability of the current system.In Rhode Island, health care spending,climbing steadily over recent decades,is higher on a per capita basis than forthe US as a whole. In 2004, Rhode Is-landers’ personal health care expendi-
Figure 1Uninsured as Percentage
of Total Population2004-05

408MEDICINE & HEALTH/RHODE ISLAND
tures accounted for 16% of Gross StateProduct; the share is 13% nationally.10
Rhode Island’s spending level resultsfrom an annual growth rate of 8.5% be-tween 1980 and 2004. Family premi-ums for people insured through theirjobs now average more than $10,000in Rhode Island.
Spending for Medicaid, which is pro-jected to reach $63.5 million next year,now absorbs more than 20% of the statebudget. In September, Governor Carcieri,working with the Rhode Island Expendi-ture Council, charged a new Study Groupwith improving the efficiency and effec-tiveness of the program.2
In November 2002, researchers fromthe Boston University Health Reform Pro-gram concluded there was already enoughspending on health care in Rhode Islandto make coverage available to all, if only theexisting system would be reformed.11 Yetthere has been little agreement on the bestdirection for change. Proposals have in-cluded malpractice litigation, single-payerhealth care, and employer mandates. A“Fair Share Health Care Act” requiring largecompanies either to contribute a minimum
amount to their employees’ health insur-ance or pay into a state fund did not passthe legislature this year, despite supportfrom the Lieutenant-Governor.
One bill that did pass, The HealthCare Affordability Act of 2006, is meantto reduce the cost of insurance for low- tomoderate-income individuals, small busi-nesses, and the self-employed, but the lawfalls far short of comprehensive reform.Significantly, lawmakers inserted a provi-sion creating a Task Force to study “the ap-plicability of the Massachusetts HealthCare Reform Plan to Rhode Island” witha reporting date no later than June of2007.12
UNDERSTANDING THE MASSACHUSETTSHEALTH REFORM LAW
The Massachusetts health reform re-sulted from a combination of problems,pressures, and possibilities.13 Althoughfederal and state estimates differ, bothagree on a sharp increase in the numberof uninsured in the Commonwealth dur-ing the early part of this decade. Healthinsurance costs in Massachusetts are alsoamong the highest in the nation: yearly
premium increases of 10% or more inprivate health plans are the norm.
Massachusetts’ governor, with Presi-dential aspirations, was intent on establish-ing a reputation for domestic policy suc-cesses. Legislative leaders also recognizedhealth coverage as a priority. An initiativeby the Blue Cross Blue Shield Foundationof Massachusetts, Roadmap to Coverage,maintained focus on the uninsured.
Yet these conditions alone might havebeen insufficient to elicit a legislative solu-tion were it not for two additional forces.The federal government threatened towithdraw $385 million annually under thestate’s Medicaid waiver unless Massachu-setts came up with a new way to financeservices for its uninsured.14 And a coalitionof religious and community groups intro-duced a ballot initiative to put the healthcoverage issue before voters. The implica-tions were clear: if Massachusettspolicymakers failed to adopt meaningfulreform, there would be serious conse-quences.
Contentious debate characterized dis-cussions of the new legislation. Powerfulgroups representing business, the healthindustry, and consumers monitored devel-opments while competing to influence thespecification of benefits and responsibili-ties. Wisely, however, major stakeholdersavoided the legislative stalemate that couldhave arisen had they approached the law-making process as a zero-sum contest be-tween their interests and those of other par-ticipants. By November 2005, four mainoptions from Governor Romney, theHouse, the Senate, and the MassachusettsAffordable Care Today! campaign heldthe spotlight.15 Their provisions differedwith respect to program size, mandatedemployer costs, individual coverage re-quirements, and the role of Medicaid.Even as the legislative endgame was un-derway in spring of 2006, the Governorand legislative leaders remained at oddsover state funding for the new programand proposed business costs.
The final package that emerged inApril embodied a compromise of govern-ment interventionism and market-basedincentives.13 A new “Health InsuranceConnector” was established to make low-cost insurance products available to smallbusinesses and individuals. Employerswith more than 10 employees who fail toprovide coverage will be subject to an as-
Figure 2Personal Health Expenditures (2004)and State Health Expenditures (2003)as Percentage of Gross State Product

409VOLUME 89 NO. 12 DECEMBER 2006
sessment of $295 per employee per year.Eligibility changes in MassHealth, thestate’s Medicaid program, expanded cov-erage for children up to 300% percent ofthe poverty level. For low-income individu-als and families falling in the gap betweenpublic and private sources, policymakerscreated the “Commonwealth Care HealthInsurance Program,” providing sliding-scale subsidies for the purchase of insur-ance. Plans offered through Common-wealth Care will be without deductibles,and enrollees below the poverty level willnot pay premiums. A new requirementalso expands availability of “cafeteria plans”enabling the purchase of health insurancewith pre-tax dollars.
One of the most innovative—andwidely discussed—elements of the Massa-chusetts health reform is an “individualmandate.” Beginning in July 2007, all resi-dents must acquire coverage through eitheran employer, MassHealth, or self-purchase.For the latter group, the Health InsuranceConnector will define affordability stan-dards as well as the features of health plansthat will be offered for sale to the uninsured.The penalty for not complying with thisindividual mandate, if “affordable cover-age” is made available, will be an increasein state income taxes equal to loss of thepersonal exemption in 2007, and one-halfthe cost of the lowest available insuranceplan premium after that.
The Massachusetts law also revampsthe state’s Free Care Pool, increases reim-bursements for hospitals and physicians,and merges the non-group and small-group insurance markets. The most note-worthy part of the new program, how-ever, will be its impact in expanding cov-erage. Once fully in place within threeyears, the plan is projected to cover515,000 of the currently uninsured,bringing the uninsured population inMassachusetts to below 1%.16
When Governor Romney signed thehealth care bill into law, the Boston Globedescribed it as a moment “widely praisedas historic for the state and seen as a bigboost to Romney’s presidential aspira-tions.”17 Health policy expert PaulGinsburg (in the New York Times ) pre-dicted: “It’s definitely going to be inspir-ing to other states…They found a way toget to a major expansion of coverage thatpeople could agree on.”16
Less than a month after the signing ofthe bill, Rhode Island lawmakers scheduleda special hearing to begin reviewing the les-sons of the Massachusetts experience.
A SOLUTION WITH STRENGTHS ANDWEAKNESSESPolitics, Not Policy
Conflicting views and interests not-withstanding, health care reform in Mas-sachusetts was made possible by a sharedbipartisant commitment from Democraticlegislative leaders and a Republican gov-ernor. At the same time, the process ofpolicymaking was, in important respects,an open one, in which business, labor, hos-pital, professional, and consumer groupswere consulted. The final legislative pack-age combined new mandates on employ-ers as well as individuals.
When John McDonough, executivedirector of the Boston-based advocacy groupHealth Care For All, spoke with Rhode Is-land lawmakers last May, he stressed com-promise as the major lesson of the Massa-chusetts reform.18 Writing subsequently inHealth Affairs, McDonough emphasizedthat the Massachusetts experience is valuable“more as a political blueprint and less as apolicy blueprint.”13
For Rhode Island, in which the healthpolicy process has often been marked by acombative relationship between the Demo-cratic legislature and Republican governor,this point is essential. Finding a successfulpath to reform will depend on mutual ac-commodation and inclusiveness.
The Cost QuestionAt the root of unease about the Mas-
sachusetts plan is a fear that costs will soonoutdistance revenues, making it necessaryfor policymakers either to retrench on theprogram’s objectives or find additionalfunding via higher taxes, higher employerassessments, and/or increased consumercontributions.17 Already, the state’s finan-cial commitment under the law is targetedat $125 million annually in general rev-enues. A large proportion of remainingcosts is to be covered by the special Med-icaid waiver monies obtained by Massa-chusetts. For Rhode Island, which has ahigher level of uninsurance than Massa-chusetts and no equivalent supplementalfederal Medicaid payments, the fundingrequirements of a program with this de-
sign would be daunting. One answer is tofashion a bill that couples coverage expan-sion with tough cost-containment provi-sions—something the Massachusetts lawdoes not do—but this will increase thepolitical obstacles to reform.
Finding the Right AdministrativeModel
The central administrative mecha-nism of the Massachusetts health reformis the Commonwealth Health InsuranceConnector, a new authority whose func-tions range from helping to rewrite theregulation of private insurance plans, toapproval of new low-cost low-benefit prod-ucts for young adults, to supervising thepurchase of insurance by individuals eli-gible for public subsidies. It is too early toassess the Connector’s complex work. Asignificant effort at transparency seems tobe underway through regular public no-tices and open meetings. As expected,staffing demands, internal organization,basic data-gathering and analysis, anddrafting of rules have dominated theConnector’s first few months.
A current controversy, however, con-cerns the affordability of rates announcedby the Connector for enrollees between100 and 300% of the poverty line. Com-mented one health policy analyst from TuftsUniversity, “for too many people, the num-bers just don’t add up.”19 This worrisomedevelopment has occurred closely in tan-dem with Governor Romney’s weakeningof the enforcement of the $295 assessmenton businesses that don’t pay a “fair and rea-sonable” contribution to their employees’coverage.20 Now there is discussion as towhether the state’s insurance mandate willrequire parents to buy plans that cover theirchildren.21 Taken together, decisions onthese matters could limit the scope of cov-erage achieved in Massachusetts.
The lesson to be underscored here isthat administrative operations as well aspolicy design are pivotal in maintainingthe balance of interests within health re-form. Rhode Islanders need to considercarefully which bureaucratic model—theMassachusetts example, or some other al-location of implementation responsibil-ity—would prove most advantageous inview of this state’s established agency envi-ronment. Creating specialized bureaucra-cies is a tempting strategy for concentrat-

410MEDICINE & HEALTH/RHODE ISLAND
ing expertise and authority in executingnew public functions. Yet the risks includehigh start-up costs, problems of coordina-tion with other government departments,and capture by outside groups.
W(h)ither Employment-BasedCoverage?
According to the Boston Globe, pre-mium increases for the four major privatehealth insurers in Massachusetts are ex-pected to exceed 10% for 2007—the sev-enth straight year of double-digit inflationin health insurance costs.22 Many employ-ers are likely to restrict benefits and/or im-pose higher deductibles, copayments, andpremiums on employees.
This same scenario has been playingout in Rhode Island. Small wonder, then,that Governor Carcieri identified haltingthe “continued erosion of employer-spon-sored health insurance” as a primary goalof his current health policy agenda.23
However, the Massachusetts health plandoes little to address this problem. On theone hand, the Connector will help makelower-cost insurance products available forsmall businesses, but on the other themerger of small-group and nongroupmarkets is expected to raise small-grouppremiums.13 Further, the $295 employerassessment could prove too meager to pre-vent a disinsurance movement amongbusiness-owners who direct employees tothe Connector rather than continue toprovide coverage on their own.24
Nor does the Massachusetts plan haltthe cost-sharing increases in private insur-ance. It may even exacerbate the trend bylimiting benefits in the nonsubsidized plansoffered through the Connector. The basicdilemma of our market-based health systemremains: those lowest on the political andeconomic totem pole are expected to absorbthe burden of cost-shifting. The result hasbeen increasing levels of “underinsurance.”To the extent that Rhode Island addressesthis problem through regulation and othermeans—the emphasis in the state’s 2006health law on prevention and wellness is apossible contribution—it would have lessonsof its own to export.
CONCLUSIONWould the Massachusetts model work
in Rhode Island? The question is difficultto answer, not least because it is still farfrom clear how well the program will work
in Massachusetts. As health care advocateJohn McDonough and his associates havewritten, “Give Massachusetts time toimplement, and revisit what we haveachieved by 2009. Then let’s talk.”13
Yet Rhode Island may not have theluxury of waiting for results elsewhere be-fore having to act. As measured by keycoverage and spending indicators, RhodeIsland’s health system faces a predicamenteven worse than the one in Massachu-setts, and major cuts in public programsare under consideration. The Massachu-setts example may be very useful now forits inspirational value.
As to whether the structure of theMassachusetts approach should beadopted in this state, it seems a questionbest answered through evaluation of indi-vidual design components, rather than asa thumbs-up-or-down for the program asa whole. The Massachusetts health plan isa social experiment, and its pieces are notso closely interlocked they can’t be tam-pered with. Once Rhode Islanders decideon what they want to accomplish—interms of such aims as universality, cost-con-tainment, and market intervention—thehow should come more plainly into view.
REFERENCES1. MacKay S. Coalition protests cuts to uninsured.
Providence Journal, May 9, 2006, p. B1.2. Lord PB. Panel formed to corral Medicaid spend-
ing. Providence Journal, September 12, 2006, p. B1.3. Nichols LM. Health Reform Massachusetts Style:
Ink Blot Test and Example for Us All. Washing-ton, DC: New America Foundation, May 2006.
4. Robert Wood Johnson Foundation, State Cover-age Initiative. Uninsurance in America. http://www.statecoverage.net/stateofthestates/uninsurance.html. 2006.
5. US Census Bureau. Income, Poverty, and HealthInsurance in the United States, 2005. CurrentPopulation Reports, P60-231. US GovernmentPrinting Office, Washington, DC, 2006.
6. Ibid., Table 10, p. 27.7. Lebel RA. Annual Report on the Department of
Human Services’ Implementation of Programs toAddress Uninsurance among Rhode Islanders.Submitted to Permanent Joint Committee onHealth Care Oversight. February 15, 2006.
8. RI State Planning Grant on Access to Health Insur-ance. HRSA Final Report. RI Department of Hu-man Services, September 2005, Figure 10, p. 24.
9. Landis B. Employers found cutting back onhealth-care coverage. Providence Journal, Novem-ber 16, 2005, p. A1.
10. Kaiser Family Foundation, StateHealthFacts.Org.Health Costs & Budgets. http://www.statehealthfacts.org/cgi-bin/healthfacts.cgi. 2006.
11. Sager A et al. Rhode Island Can Afford HealthCare for All: A Report to the Rhode Island Gen-eral Assembly. Boston University Health ReformProgram. November 25, 2002.
12. The Rhode Island Health Care Affordability Actof 2006. Public Laws, Chapter 307, Part V.
13. McDonough JE, Rosman B, et al. The ThirdWave of Massachusetts Health Care Access Re-form. Health Affairs, Web Exclusive, http://content.healthaffairs.org/cgi/content/full/hlthaff.25.w420/DC1.September 14, 2006.
14. Massachusetts Medicaid Policy Institute. TheMassHealth Waiver. Issue Brief. Boston, April2005.
15. Helman S. Mending the healthcare system: Theproblem, the action, the options. Boston Globe,November 6, 2005, p. B1.
16. Belluck P. Massachusetts sets health plan for nearlyall. New York Times, April 5, p. A1.
17. Helman S, Kowalczyk L. Joy, worries onhealthcare. Boston Globe, April 13, 2006, p. A1.
18. Rhode Island General Assembly. Permanent JointLegislative Committee on Health Care Oversight.May 9, 2006.
19. Quoted in McNamara E. Unrealistic health plan.Boston Globe, September 13, 2006, p. B1.
20. Massachusetts Division of Health Care Financeand Policy. Determination of Employer Fair ShareContribution. 114.5 CMR 16.00. Final Adop-tion, September 8, 2006.
21. Kowalczyk L. Coverage of children not requiredin health law. Boston Globe, October 2, 2006, p.A1.
22. Krasner J. Medical insurance hikes loom in Mass.Boston Globe, September 10, 2006, p. A1.
23. RI Office of the Governor. Toward a More Af-fordable Health Care System for Rhode Island:Governor Carcieri’s Agenda. October, 2005.
24. Holahan J, Blumberg L. Massachusetts HealthCare Reform. Health Affairs, Web Exclusive, http://content.healthaffairs.org/cgi/content/full/hlthaff.25.w432v1/DC1. September 14, 2006,w440-w441.
ACKNOWLEDGMENTSMarie Ganim, PhD, Policy Director
for Health and Human Services, RhodeIsland Senate, and Kaitlyn Kenney, PhDcandidate in Public and InternationalAffairs, Northeastern University, com-mented on this article.
David A. Rochefort, PhD, is Arts andSciences Distinguished Professor of Politi-cal Science, Northeastern University, andVisiting Professor, Taubman Public PolicyCenter, Brown University.
CORRESPONDENCEDavid A. Rochefort, PhDPolitcal Science Department303 Meserve HallNortheastern UniversityBoston, MA 02115(617) 373-4399e-mail:[email protected]

411VOLUME 89 NO. 12 DECEMBER 2006
What Would It Take?Christopher F. Koller, MPPM, MA�
IN THE PARABLE OF THE BOILED FROG, thecold-blooded amphibian sits in a pot ofhot water on the stove, ignorant of therising temperature until it is too late.
Many observers maintain our medi-cal care system is bobbing in a pot of ris-ing costs and the resulting increased num-ber of uninsured citizens - similarly un-aware of the dangers that are rising.When, they ask, will the pot boil over andour system collapse?
Even if the imagery is overheated—after all, there are states with uninsuredrates that are double Rhode Island’s—thenumber of uninsured here is twice what itwas five years ago and there seems to berenewed interest in tackling this persistentissue: how can a country as wealthy as oursnot insure everybody? The passage of am-bitious legislation in Massachusetts raises thequestion for Rhode Island: What would ittake to guarantee for all Rhode Islanderssome basic health care and a protectionagainst medical catastrophes? What wouldit take to include all the Rhode Islanderswho are outside the health insurance poolbut are the ones getting soaked?
IT WOULD HAVE TO PRIORITIZE THEPROBLEM
Appeals to cover the uninsured canbe made on justice: it is unfair for a moralsociety to live with so much inequity. Af-ter all, uninsured people are sicker thanthose with insurance, they postpone medi-cal care and presumably suffer more,and—if uninsured long enough—die ear-lier.1 Medicaid and Medicare were estab-lished based on this principle; and, accord-ing to this thinking, it is time to updategovernmental programs to reflect today’ssocial reality of more uninsured.
Appeals to social justice often havelimited effect in the US. Culturally we tol-erate a fair amount of inequity in exchangefor freedom and the hope of hitting it big.The second approach is more utilitarian:a large uninsured population imposesgreat social and economic costs on the restof us - treatment costs borne by the in-sured and economic costs in lost produc-tivity.2 These costs are real but elusive todocument: capturing and applying them
to finance an effort cover the uninsured isdifficult. Maine’s Dirigo Health Plan isbuilt on such on effort, and its success isby no means assured.
If the costs are hard to capture, thenthe appeal to justice is probably stronger.Rhode Island, with its traditionally strongsense of cultural and social solidarity, is ame-nable to this appeal. Affordable health in-surance is becoming a middle class prob-lem. Massachusetts’ legislation could inspiresome productive sibling rivalry and collabo-ration. Yet even with the prioritization ofhealth insurance for all, how would this beaccomplished in a socially, politically andeconomically feasible fashion?
IT WOULD HAVE TO TARGET THEUNINSURED POPULATION.
Rhode Islanders’ uninsured popula-tion resembles that in other states.3 Theuninsured in RI are most likely to be:4
• Young (57% are between the agesof 18 and 34)
• Working (63% work for wages)and
• Poor (50% have incomes less than$25,000)
While the number of Rhode Islandcompanies offering health insurance has noteroded much over the last six years (smallercompanies are consistently less likely to of-fer it), the number of employees able to af-ford their employers’ offering has. 5
The implications are that any effortstargeting these people will have to takeinto account their limited ability to pay,their relatively young (and healthy) sta-tus, and the inability of the privatelyfunded, employer-based system to givethem affordable, useful options.
IT WOULD TAKE A VISIONImagine a set of rules for health in-
surance with a commitment to universalcoverage. That sounds like an expansionof what works—Medicare. That belea-guered program has provided medicalsecurity for all elders, balanced a com-mon set of benefits with the ability to buyup to a more comprehensive package—
with administrative costs 80% less thanthose of commercial health plans.
Applied to the commercial and un-insured population, a Medicare-for-allplan would replace (at least for some) em-ployer-based health insurance with Fed-eral financing, paid for by payroll andemployer taxes with means-testing forlower income populations. Like Medi-care it would offer a choice of plans, withthe ability to buy supplemental coverage.By eliminating the tie to employer-basedhealth care, it would acknowledge thereality of a mobile workforce and createa level playing field for employers.
Such a vision has its limits. Patientscurrently with private health insurancewould surrender a choice of benefit plansfor the certainties of health coverage anda government bureaucracy. Employerswould be either invited or commandedto throw in the towel on buying healthcare benefits and trust that the governmentcould do it better. Providers would acceptbroader Medicare-like fee setting in ex-change for administrative simplicity. Stateswould have to wait for change to emergefrom Washington—a daunting prospect.6
An accommodation to this visionwould capitalize on rather than refute therise of consumerism and individualism inour culture. Commercial health insur-ance would look a lot like auto insurance.Individual purchasers empowered by theInternet and shrewd benefit plans, andgoaded by an obligation to buy healthinsurance, would make informed choices,based on the cost and quality of their op-tions. Patients would take more responsi-bility for the preventive equivalent of oilchanges. Providers would respond to con-sumer pressures by offering specialization,cheap pricing and better service for com-modity items—patients would come to“Trust the Midas touch.” Rare and ex-pensive high-end services, like collisionwork, would be negotiated between in-surers and regulated providers.
There are limits to this accommoda-tion as well. Unlike auto insurance, soci-ety would insist on public subsidizationof the purchase of health insurance or aset of publicly funded providers for low

412MEDICINE & HEALTH/RHODE ISLAND
income citizens. Also, the moral and epi-demiological consequences of neglectingpreventive health services are a lot higherthan not changing your oil: we find iteasier to junk someone’s house or car thantheir body. But our cultural schizophre-nia demands both maximum benefitscoverage and maximum treatmentchoice, with little consideration of price.
IT WOULD TAKE SOME PRINCIPLESAny policies to expand health insur-
ance would start with some collectivecommitments. In Rhode Island, theymight look like the following:
1.Universal right: as obvious as itsounds, any proposal must beginwith a fundamental social commit-ment to the requirement of univer-sal coverage for every citizen.
2.Universal obligation: everyone con-tributes—at the point of care, atthe premium level and in taxes.There is no free loading for eitherindividuals or employers. Individu-als have some cost sharing at thepoint of care so cost-sensitive deci-sions are made.
3.Limited right: As with Medicare,everyone would have to buy into acore benefit package. This packagewould have to be cheap enough foryoung, healthy and lower incomepeople: built on primary and pre-ventive care, generic drugs andcatastrophic hospitalization. Every-one could buy more coverage ifthey could afford it, but the socialcommitment would be to the con-ditions to promote a healthy life,not a guarantee of coverage to treatany condition or to sustain anyhope for physical survival.
4.Mercy trumps responsibility. As ap-pealing as it may be to penalize ev-ery bad habit through insurancepremiums, that road ends witholder and sicker people paying a lotmore—thus defeating the poolingeffects of insurance. We do chargemore for sixteen year olds to driveand for sky divers to buy life insur-ance and we should probablycharge you more if you smoke andchoose not to exercise, but insur-ance is also about randomness: bad
things happening for no good rea-son. Health insurance in particu-lar is about spreading the financialburden of ill health: no matter howmuch you smoke your diseaseshould not render you destitute.Besides, public health measures likepublic smoking laws and directconsumption taxes have provenmore effective at reducing smok-ing incidence than an indiscrimi-nate premium surcharge.
5. Lots of choice: Americans have con-sistently shown a willingness to paymore, and accept more inequality,in exchange for more choices ofdoctor and of health plan. Anydesign would have to allow for this.
6. Let the Government do (more of ) it.Employer-based health insurancecontinues to erode in the face ofrising costs. Without requiring it,there would need to be a mecha-nism for employers to meet theirobligations by ceding money andresponsibility to the Government,to avoid instances like large retailfirms where employees flock toMedicaid. By evolution and intent,as it purchases more, the Govern-ment assumes a greater role inregulating the medical care system.
Similarly, advocates of universalcoverage must acknowledge that tobe politically feasible the deliverysystem and at least some of the fi-nancing system must stay private—at least initially—and thus morefragmented and more costly.
7. Fix the tax code. Employee healthcare benefits are not taxed; employ-ers reduce their tax liability with ev-ery dollar of insurance coveragepurchased. But when individualsbuy health insurance for them-selves, they do it with after tax dol-lars. These incentives need to becorrected.
8. Let the states try it. National reformswill be glacial in pace. Political con-sensus is easier to reach at the locallevel. States, citing Oliver WendellHolmes, can be “the laboratories ofinnovation” and Rhode Island—with its RIte Care program, and his-tory of provider quality report-
ing—has shown an appetite for in-novation in health policy. In a uni-versal coverage model, states wouldhave to be:
• Rule-makers – to level the play-ing field for individuals, employ-ers and providers.
• Market-makers – to negotiatewith private health plans on be-half of others without that lever-age.
• Financiers – to maximize federalMedicaid payments and use tax-ing authority to subsidize care forthose who cannot afford it.
9. Underlying costs must be addressedand the delivery system changed. Ourfragmented, specialty-heavy medi-cal delivery system is partially re-sponsible for poor quality and highcosts. Any reforms should promotebetter information exchange to re-duce duplication, more cost aware-ness for ambulatory services, moreconsumer responsibility and stron-ger primary and preventive care.
10.Most importantly: don’t let the per-fect be the enemy of the good. Thegreatest challenge would be the de-termination of a basic benefit.There remains a huge gap betweenthe health benefits we want andwhat we can afford. Economiststypically suggest that it is unsustain-able for a family to spend muchmore than 10% of gross income onmedical care expenses. For themarket rate of $1100/month for afamily policy and an employer con-tribution of 50%, that would re-quire an annual income of$66,000. If more money is notfound, the cost of the package mustbe reduced; part of that must comefrom reduced benefits. No budgetis unlimited.
IT WOULD TAKE A PLANVisions, by their nature, are great
leaps forward. Any variant of the visionsarticulated here could involve a massivereallocation of funding from employersto individuals and the state or federal gov-ernment. It would signify an acceptanceby the public that health care is a public

413VOLUME 89 NO. 12 DECEMBER 2006
good and entrust more of its financingto a political process and public adminis-tration—neither of which enjoy greatpopularity today.
So it would take pragmatism to getfrom here to there. That is why the planpassed this spring by the Massachusettslegislature has attracted such attention.It consists of the following elements:7
1. Employer mandate (Vetoed by Gov-ernor Romney but over-ridden by thelegislature) Businesses would be re-quired to insure employees or paya contribution to the state for thosewho do not purchase health insur-ance. The state, through a newagency, will take a stronger handin negotiating benefits and priceswith private health plans on behalfof small employers.
2. Individual mandate. When theprogram is fully implemented, ev-ery Massachusetts resident wouldhave to show—on their tax filing—proof of insurance coverage.
a. Low income families would haveaccess to an expanded Medicaidprogram, possibly with a morelimited set of benefits than cur-rently.
b.Young residents could stay ontheir parents’ coverage until age25, or purchase special, reducedbenefit packages through thestate purchasing agency.
c. Employed individuals could pur-chase their benefit through thesame agency using pre-tax dol-lars, with a subsidy if their in-come was low.
This program’s success will hinge onmoney. Under threats of federal cuts,Massachusetts is moving large amountsof Medicaid money which previouslywent directly to providers into insurancesubsidies. Even if the money “works” ini-tially, will this program create a largerbudgetary obligation for the state, withno ability to control medical cost trendsin the future?
A second success factor will be theeffect on small businesses. Will the“Commonwealth Connector”—thestate’s new purchasing entity –succeed innegotiating with health plans, reducing
the rate of medical inflation and forginga consensus on the balance between ex-panded benefits and cost?
Finally, the legislative artfully avoidsdefining what constitutes affordablehealth insurance in terms of price andcomprehensiveness. It remains to be seenhow consensus will be developed.
A program such as Massachusetts’could be developed in Rhode Island. Keyelements might include:
1. Employer and individual obliga-tions—in a voluntary market, wewill not achieve full insurance. Asizeable group of people buy autoinsurance only because they must.
2. Requirement of a basic benefitpackage—less comprehensivethan the current commercial stan-dard.
3. Increasing the age of covered de-pendents.
4. An active Government purchas-ing and regulatory role for thosewho can’t negotiate with healthplans themselves, building on thesuccess of RIte Care and historyof small employer group regula-tion.
5. Subsidies for low income popula-tions who cannot afford even thebasic plan, funded as much as pos-sible through Medicaid.
6. Building a common platform onthe foundations of RIte Care andour existing small group and in-dividual regulations. This wouldpermit some standardization ofmarketing and enrollment in cer-tain markets to reduce adminis-trative costs.
IT WOULD TAKE CAREFUL THOUGHTTO OVERCOME OBSTACLES
Not surprisingly, there would be con-ditions to such a program.
The money. Covering Rhode Island’s110,000 uninsured is a $500 million an-nual challenge at commercial rates of cov-erage and payment. Financing is a greaterconcern than in Massachusetts, becausethere is no bolus of existing Medicaidfunds. Sources include Federal paymentsfor new Medicaid eligibles, existing pay-ments for uncompensated care, savings
from benefit limitations and design, andmore payments from the currently-unin-sured, their employers, and the taxpayers.
Sustainability. With medical trendrates at two-three times inflation, any newprogram should dampen the trend, notaccelerate it, particularly since the statewould be liable for future expense in-creases for the subsidized portion of theprogram. The tools used by large pur-chasers—aggressive plan negotiation tolimit administrative costs and profit, andbenefits redesign that demands morepatient responsibility—should be em-ployed. The state would have to negoti-ate aggressively with large health planson behalf of those who can’t, set standardsfor information and quality, and possiblyeven negotiate provider rates. Health in-formation technology would have to de-liver on its promise of reduced duplica-tion and administrative costs.
Political Resistance. The establish-ment of a program like this would de-pend upon a political mandate that winsover the voices of resistance – those whobelieve they would lose in the new sys-tem. The line of putative losers would belarge: patients fearing loss of choice; ad-vocates fearing the loss of consumer pro-tections and benefit coverage; tax payersand employers fearing new financial ob-ligations; providers and insurance brokersfearing loss of autonomy and revenue,insurance companies fearing loss of prof-its. At the core would be institutional re-sistance to the unknown: the unforeseenoutcomes could be worse than the statusquo.
Who would advocate for such a pro-gram? Certainly the uninsured them-selves—but poor young people have notbeen bases of great political power. Un-compensated care providers—hospitals,community health centers and other phy-sicians—would see their burden greatlylightened. Employers who struggle toprovide health insurance should wel-come both the increased options avail-able to them, and a set of common rulesto eliminate unfair advantages enjoyed bysome businesses that pay for less healthcare. Absent leadership, a viable plan andskillful advocacy, this may not be enoughto overcome resistance. The linchpin mayend up being people obligated and acti-vated to purchase health insurance un-der an individual mandate—who would

414MEDICINE & HEALTH/RHODE ISLAND
exert a strong force for reform andchange. Any calls for mere subsidizationof our current unaffordable structureshould be resisted.
The inequities posed by the unin-sured exert a moral claim on the com-munity. Moral claims in a civil society aretranslated and prioritized through thepolitical process. “In the end”, saysPrinceton economist Uwe Reinhardt,“Efforts at health care reform are exer-cises in the economics of sharing.”8 Shar-ing is hard to do, even harder to legis-late. However, Rhode Island has assets.Our small size is an advantage: there is astrong fabric of social solidarity resultingfrom our sometimes-too-intimate-sense ofcommunity; and as visiting policy mak-ers repeatedly tell us, it is possible to de-velop “line of sight trust” on issues ofcommon importance.
The number of uninsured will in-crease until we believe it is in our indi-vidual and collective interests to act—even at the risk of the unknown, of fail-ure and certainly with compromises and,yes, sharing. Has that time come in
The views in this article are those ofthe author, not those of the Office ofthe Health Insurance Commissioner,or of the State of Rhode Island.
Rhode Island? The almost one in eightRhode Islanders without insurance be-lieve it is past time. The workers whowatch the rising costs of their health ben-efits eat up their wages believe that some-thing must be done. Legislators whostruggle to balance a budget in the faceof rising Medicaid and personnel healthcosts believe that something must be done.
Like the number of uninsured, thetemperature in the frog’s pot is increas-ing—and the number of people willingto act on the challenge of the uninsuredmay well be too.
REFERENCES1. Kaiser Family Foundation: http://www.kff.org/
uninsured/upload/7451.pdf2. Vladeck B. Paying for hospitals’ community ser-
vice. Health Affairs 2006; 25:34-43.3. As of 2004, at a point in time 12.3 % of RI’s
citizens were without health insurance vs. 17.8nationally. Henry J. Kaiser Family Foundationanalysis of Current Population Survey Statistics.(http://www.kff.org/uninsured/upload/7451.pdf )
4. Rhode Island Department of Health. BehavioralRisk Factor Surveillance System. 2004.
5. 2005 Survey of RI Employers.
6. Krugman W. The healthcare crisis and what to doabout it. NY Review of Books, March 23, 2006.
7. Conference Committee Report, April 3, 2006,8. Reinhardt UE, Hussey PS, Anderson GF. US
health care spending in an international context.Health Affairs 2004; 23: 10-25.
Christopher F. Koller, MPPM, MA isHealth Insurance Commissioner, State ofRhode Island.
CORRESPONDENCEChristopher F. Koller, MPPM, MAOffice of the Health InsuranceCommissioner233 Richmond StProvidence, RI 02903Phone: (401) 222-2246E-mail: [email protected]

415VOLUME 89 NO. 12 DECEMBER 2006
Utilization of Hospital Emergency Departments,Rhode Island 2005
Karen A. Williams, MPH, and Jay S. Buechner, PhD
RECENT CHANGES TO LICENSURE REGULATIONS IN RHODE ISLANDrequired hospitals to report emergency department (ED) visitand observation data to the Department of Health routinelybeginning in 2005. ED data in particular provide a wealth ofinformation on special populations (e.g., the uninsured) andconditions seen primarily in the outpatient setting. Preliminarydata on ED utilization are presented here, with special focus onthe disparities between the insured and uninsured populations.
METHODSUnder licensure regulations, the eleven acute-care general hos-
pitals and two psychiatric facilities in Rhode Island report to theDepartment of Health a defined set of data items on each emer-gency department visit beginning with visits occurring January 1,2005. The data include patient-level demographic and clinical in-formation. This analysis covers ED visits occurring January 1 - De-cember 31, 2005 and is limited to ED visits not resulting in admis-sion to the hospital. ED data reported by the two psychiatric hospi-tals consist of visit data for patients receiving an unscheduled psychi-atric evaluation that did not result in an inpatient stay. Due to com-plexities in the manner in which hospitals record ED data, the datapresented here are subject to change as methods to distinguish EDvisits that result in inpatient admission at acute-care facilities fromthose that do not are improved. Diagnoses are coded in ICD-9-CM,1 and were grouped as for published national data.2 Expectedsource of payment reported as “self-pay” was used as a proxy foruninsured in this analysis. Comparative data for inpatient stays were
produced by analyzing the data on inpatient discharges also reportedby the state’s acute-care hospitals.
RESULTSIn 2005, there were 382,243 ED visits not resulting in an
inpatient stay to Rhode Island’s acute-care general and psychiatrichospitals. Of these, the highest proportion of visits was to RhodeIsland Hospital (26.1%), followed by Kent County MemorialHospital (12.3%). (Table 1) The two psychiatric hospitals reportedthe lowest volume, together comprising less than 1%.
Females accounted for more than one-half (55.4%) of allED visits and for the majority of visits within each age groupexcept 0-14 years, where males comprised 54.1% of the visits.For both males and females, approximately one-half of the vis-its were among those ages 15-44, a younger pattern than theinpatient population, where 41.1% of admissions are of per-sons ages 65 years and older.
The largest proportion of ED visits were covered by pri-vate insurance, with Blue Cross comprising the largest propor-tion overall. (Figure 1) Medicaid managed care, primarily RIteCare, was the second leading payer, with 19.1% of visits. Ex-pected source of payment among ED visits was distributed dif-ferently than among hospital inpatients. For example, Medi-care, which accounts for the largest proportion of inpatientadmissions (45.4% in 2004), accounted for only 15.2% of EDvisits. Additionally, 14.4% of ED visits were uninsured, com-pared to only 3.1% of inpatient stays and 4.9% of inpatientsadmitted through the emergency room.
Insurance status varied by age group and sex. ED visits forthose ages 15-44 accounted for the greatest proportion of visitsby far, with 48.3% of ED visits among the insured and overthree-fourths (76.1%) of the uninsured visits. For both malesand females, the youngest (ages 0-14) and oldest (ages 65+) agegroups had the lowest proportion of uninsured visits. The differ-
RHODE ISLAND DEPARTMENT OF HEALTH • DAVID GIFFORD, MD, MPH, DIRECTOR OF HEALTH EDITED BY JAY S. BUECHNER, PHD
Figure 1. Emergency department utilization as percent of all visits,by expected source of payment, Rhode Island, 2005

416MEDICINE & HEALTH/RHODE ISLAND
ence in insurance status by sex is greatest for those ages 15-44.Overall, one in five visits in this age group are uninsured, but30.1% of males are uninsured compared to 14.4% of females.(Figure 2) Overall, 19.1% of visits by males were uninsured,compared to only 10.6% of visits by females. (Figure 2)
Among ED visits, insurance status also varied by race andethnicity. Seventy-four percent of ED visits were by White Non-Hispanic persons. The next largest race/ethnic group was BlackNon-Hispanic, accounting for 9.1% of all ED visits. Persons iden-tified as White non-Hispanic had the lowest proportion of visitswithout insurance (12.9%). (Figure 2) The proportion withoutinsurance was much higher for minority groups—19.5% for Blacknon-Hispanic, 17.9% for Hispanic, and 17.9% for Asian.
Injury and poisoning was the leading first-listed diagnosis cat-egory overall for both the insured and uninsured, comprising al-most a third (29.9%) of all ED visits. (Figure 3) The second lead-ing diagnosis category was symptoms, signs, and ill-defined condi-tions, which accounted for 18.5% of all visits, followed by diseasesof the respiratory system (9.0%). The most notable differences byinsurance status were for mental disorders and for complications
of pregnancy, childbirth and the puerperium. Mental disorderswas the third leading category among the uninsured ED visits(9.9%), but ranked only seventh for those insured (4.8%). Com-plications of pregnancy, childbirth, and the puerperium accountedfor 4.9% of insured ED visits, but only 1.4% of uninsured visits.
DISCUSSIONEmergency department data are a rich data source for ex-
amining trends among the uninsured and disease conditionsspecific to outpatient settings. Utilization patterns in the EDdiffer from patterns seen for inpatients with regards to patientcharacteristics, health insurance and disease conditions.
A significant proportion of ED visits by both genders areuninsured. Not surprisingly, lack of insurance is highest for malesage 15-44, where the uninsured represent almost one-third ofvisits. This disparity in insurance status by age and sex highlightsthe need for improving insurance coverage among this group.
Few differences in disease conditions between the insuredand uninsured populations were identified based on broad di-agnosis categories. However, the proportion of persons seekingcare in hospital EDs who are uninsured is much higher than theproportion uninsured among inpatients, including those admit-ted through the ED, giving rise to the question of whether theuninsured may be using the ED largely for non-emergent con-ditions. More detailed analyses of the diagnostic information inthe ED database are planned to investigate the use of emergencydepartments for such conditions, with particular regard to in-surance status. In the longer term, linking ED data to aggregatepopulation-based survey data on access to primary care and usualsources of care will be pursued, with the expectation that theadditional information may help to explain the utilization pat-terns identified from the ED database.
Karen A. Williams, MPH, is Public Health Epidemiologist,Center for Health Data and Analysis.
Jay S. Buechner, PhD, is Chief, Center for Health Data andAnalysis, and Assistant Professor of Community Health, BrownMedical School.
Figure 2. Emergency department visits as percent uninsured, byage group, sex and select race/ethnicity groups, Rhode Island, 2005
Figure 3. Emergency department utilization as percent of all visits, by first-listeddiagnosis category, Rhode Island, 2005
REFERENCES1. Public Health Service and Health Care Financing Ad-
ministration. International Classification of Diseases, 9th
Revision, Clinical Modification, 6th ed. Washington:Public Health Service, 1996.
2. McCaig LF, Nawar EN. National Hospital AmbulatoryMedical Care Survey: 2004 Emergency DepartmentSummary. Advance Data from Vital and Health Statis-tics; No 372. Hyattsville, MD: National Center forHealth Statistics.

417VOLUME 89 NO. 12 DECEMBER 2006
IN MARCH 2001 THE ROBERT WOOD JOHNSON FOUNDATIONasked the Institute of Medicine to develop recommendationsfor how public health education, training, and research couldbe strengthened to meet the future needs to improve popula-tion-level health. Because of the ecological approach to publichealth and the numerous institutions and agencies that playimportant roles, the IOM report, Who will keep the publichealthy, (2002), addresses its recommendations widely to a va-riety of public health-related sectors. It seems a reasonablestep to extend that framework to professionals in the many com-munity-based organizations that carry out critical roles in stateand local public health activities.
Brown University Program in Public Health and the RhodeIsland Department of Health (HEALTH) received an educa-tional grant from Pfizer, Inc. in December 2005 to develop aPublic Health Training Program (PHTP) for professional staffin the business, government and not-for-profit sectors of RhodeIsland. To assure project success, it is important to minimizebarriers to participation among the target audiences by identify-ing and addressing concerns; by determining their high prioritytraining topics; and by noting preferences for scheduling, train-ing “credit” and cost. One of the first steps in this process in-volved conducting a market survey and using those results toinform the design and implementation of the PHTP activities.This paper summarizes the key findings of the survey.
BACKGROUNDOnly the Brown University Master in Public Health
(MPH) offers accredited, graduate public health training inRhode Island. Yet, due to various reasons, such as workdayclass schedules, this program may not meet the needs of manyfull-time employed health-related professionals in Rhode Is-land. Both Brown and HEALTH believe that public healthtraining can lead professionals and other community leadersto a better understanding of the dynamics of population-basedhealth issues in the state.
The PHTP is a collaborative project established to improvecollaboration and promote training experiences in public healthtopics for personnel in the state and local government, busi-ness, non-profit community organizations and healthcare. Asone of the first tasks during the planning phase, the PHTPsurveyed key informants, including executives and administra-tors in each of the target sectors in order to determine the spe-cific interest of the intended audience.
METHODSThe investigators selected 46 executives and administra-
tors in major Rhode Island community organizations duringFebruary-March 2006. These included business executives(Vice President-level) in banking, insurance and manufactur-
ing firms, Executive Directors of community human serviceagencies (including those serving minority populations), senior-level hospital administrators (Presidents, Department Direc-tors, state and municipal agency officials (Division Directors,Human Resource Executives) and representatives of profes-sional organizations (Presidents, Executive Directors, etc.). Thesource information for key informants came from the PublicHealth Directory—the Department of Health’s electronic database for routine and emergency communication with key con-tacts in minority agencies, hospitals, businesses involved in theworksite wellness program, members of licensed health profes-sional boards, occupational safety groups and municipal offi-cials (water, sewage, public works), in addition to others. TheDirectory contains 160,000 contacts (including all licensedhealth professionals) in 200 categories. Department of Healthprogram staff recommended prospective respondents fromwithin categories of interest to ensure broad participation at ahigh level across all the target organizations. Investigatorsmailed personal requests to selected respondents and followedup by telephone.
While some of these organizations and professions, espe-cially the health-related ones, may be required to offer or un-dergo certain public health related training, such as universalprecautions, food safety or hospital incident command, thereis no requirement, per se, for training in broad-based publichealth subjects, such as epidemiology or economics of healthcare, which are addressed here.
The data collection instrument included four main sec-tions: the responding executive’s own personal interest in pub-lic health training (“self assessment”); the respondent’s assess-ment of whether or not the organization’s policies and prac-tices would encourage participation by employees in publichealth training (“organizational assessment”); an assessment ofthe perceived interest of professional employees within the or-ganization, based on the executives’ own experience (“employ-ees assessment”); and, finally, general information about theorganization and its workforce. Investigators used Epi-Info(version 3.3.2) and STATA 8.0 for data analysis.
RESULTSA total of 43 executives and administrators responded to
requests for interviews (completion rate of 93%). Overall, themajority of participants (67.4%, n = 29) had a graduate de-gree while (27.9%, n = 12) had an undergraduate degree.Organizations’ size ranged from less than 50 to more than 500employees.
Table 1 shows the level of interest in public health train-ing, preferences for training scheduled, type of credit and thewillingness to pay for training—according to the self, organi-zational and employee assessments. Respondents said that they,
Rhode Island Public Health Training Program:Market Survey Findings
Karine Tolentino, MPH, and Robert Marshall, PhD
DAVID GIFFORD, MD, MPH, DIRECTOR OF HEALTH
RHODE ISLAND DEPARTMENT OF HEALTH EDITED BY JOHN P. FULTON, PHD

418MEDICINE & HEALTH/RHODE ISLAND
individually, their organizations and their professional employeesare interested in public health training. Preferred topics rangedwidely from health economics to environmental health, obe-sity and emergency preparedness. When asked about theirown personal interest, 83.7% of respondents valued publichealth training. Nearly all of the respondents (95.4%) indi-cated that their organization would promote or encourage par-ticipation, by employees, in public health training. Most re-spondents (69.8%) thought that professional employees withintheir organization have a moderate interest in public healthtraining, while 16.3 % and 14.0% reported high and very highinterest, respectively.
Workday is the preferred schedule of training for bothrespondents (55.6%,) and organizations (80.5%). Only a fewpreferred multi-day trainings. Approximately 30% of respon-dents prefer continuing education (CME/CEU) credits, while27.8% are interested in public health training not requiringcertification. According to respondents, continuing educationis the preferred type of credit for both organizations (51.2%)and professional employees (48.8%), with some preference forgraduate and undergraduate credit. Only about 1 in 5 wantedcertificates or letters of completion.
The largest percentages of individual respondents (72.3%),organizations (41.5%) and professional employees (86.1%) arewilling to pay only $100 or less for training. This finding isconsistent with responses from 40 participants in other PHTP
trainings held during August 2006concerning access to RI publichealth data. Ninety percent of re-spondents (mostly from commu-nity-based organizations) were onlywilling to pay up to $20 for courseregistration fees. In this studyabout 40% of companies (mostlylarger ones) have tuition assistanceavailable. In an average year, 44%of organizations devote less than$10,000 for professional develop-ment or continuing educationtraining.
DISCUSSIONResults indicate a high level
but diverse pattern of interest inpublic health training topicsamong professional employees inthe government, business and not-for-profit sectors. Most key infor-mants identified access to continu-ing education as an important in-centive for their professional em-ployees and the organization forwhich they work. There is a stronginterest in making undergraduateand graduate public health train-ing more available to professionalsand other employees. Executivesexpressed strong personal interest
in public health training mostly to enhance their knowledgeand work performance, not necessarily requiring incentives orcertification.
Based on these preliminary findings, we conclude that thereare two key markets for public health training in Rhode Island:1) undergraduate and graduate public health training for em-ployees of business, government, community-based organiza-tions and 2) continuing education for public-health relatedprofessionals. Over the next few months, the PHTP plans toexplore these various markets further and collaborate with part-ner organizations to promote opportunities for public healthtraining throughout the state.
REFERENCESMarshall R. Public Health Training Program and Integrative Planning. 2005. Un-
publishedMarshall R. Public Health Training Program: Summary report of Activity. 2006.
UnpublishedInstitute of Medicine. Who will keep the public healthy: educating public health profes-
sionals for the 21st century. National Academies Press, November 4, 2002.

419VOLUME 89 NO. 12 DECEMBER 2006
Colonic Intussusception in an AdultJohn A. Pezzullo, MD
Images In Medicine
A 37 year-old man presented to the emergency department withintermittent colicky mid-abdominal pain, episodes of nauseaand vomiting, and bright red blood per rectum. Laboratoryanalysis was unrevealing, and the patient was normotensive andafebrile. On physical examination, there was tenderness to pal-pation in the mid abdomen and the left upper quadrant with-out rebound. The abdomen was otherwise soft and non-ten-der. Past medical history was benign, and there was no signifi-cant family history. A computed tomographic (CT) study ofthe abdomen revealed a 5 cm mid-colonic mass with intussus-ception of the hepatic flexure suspicious for primary bowelcarcinoma. The remainder of the CT examination was nega-tive. The patient was admitted to the surgical service for ex-ploratory laparotomy, which confirmed the colo-colonic intus-susception due to a large intraluminal and partially intramuralmass. A right hemicolectomy was performed. On histology, themass was revealed to be a large benign colonic fibroma withmild intramural invasion.
Adult intussusception is rare, accounting for 5% ofall intussusceptions, and nearly equally involves the small boweland colon. In contradistinction to the pediatric population,90% of adult cases have a demonstrable cause, and 65% ofthese cases are due to neoplasia. Malignant tumors are morecommon than benign tumors in the colon; the reverse is truein the small bowel. Isolated colonic fibromatosis in the adult isextraordinarily rare with less than 15 case reports in the medi-cal literature. Extracolonic and enteric fibromatosis may be seenin cases of Gardner’s Syndrome, which was not present in thiscase.
John A. Pezzullo, MD, is Assistant Professor of DiagnosticImaging, Brown Medical School.
REFERENCESChoi SH, Han JK, et al. Intussusception in adults. AJR 2004; 183: 691-8.
CORRESPONDENCE:John A. Pezzullo, MDe-mail: [email protected]
BC/BE Primary CareBC/BE Primary CareBC/BE Primary CareBC/BE Primary CareBC/BE Primary CarePhysician with an interestPhysician with an interestPhysician with an interestPhysician with an interestPhysician with an interest
in Medical Dermatologyin Medical Dermatologyin Medical Dermatologyin Medical Dermatologyin Medical Dermatologyneeded for busyneeded for busyneeded for busyneeded for busyneeded for busy
dermatology practice.dermatology practice.dermatology practice.dermatology practice.dermatology practice.SoutheasternSoutheasternSoutheasternSoutheasternSoutheastern
Massachusetts &Massachusetts &Massachusetts &Massachusetts &Massachusetts &Rhode Island.Rhode Island.Rhode Island.Rhode Island.Rhode Island.
CompeCompeCompeCompeCompetitivtitivtitivtitivtitive salare salare salare salare salaryyyyy.....
For details call508-226-9619
BC/BE PRIMARY CAREBC/BE PRIMARY CAREBC/BE PRIMARY CAREBC/BE PRIMARY CAREBC/BE PRIMARY CARE

420MEDICINE & HEALTH/RHODE ISLAND
The Vocabulary of Disaster�
Physician’s Lexicon
MEDICINE, IN ITS INFINITE FLEXIBILITY, con-tends with small problems, medium-sizedproblems and even crises. The lexicons of di-saster, however, are rarely unique to the pro-fession. Physicians and lay folks alike tend touse the same words when confronted withoverwhelming calamities.
The word, disaster, for example, is a de-scendant of the Italian, disastrato, meaningfrom a star but interpreted as meaning bornunder an ill-fated star. The Italian word, inturn, is derived from the Latin, astrum, mean-ing star; and the prefix, dis-, means deprivedof or something negative.
Crisis is from a Greek word meaning aputting apart or sometimes a judgment. TheLatin, criticus, means to understand or tojudge. In medicine, the word has come tomean an abrupt change in the progress ofan acute disease and thus we have a malarialcrisis, an Addisonian crisis, a febrile crisis and,of course, an identity crisis.
Catastrophe is derived from a Greekword meaning a twisting downward or anoverturning. The prefix, cata- , is Greek sig-nifying a downward or disintegrating qual-ity as in words such as catabolism, cataclysm,catalyst, catatonia, cataract [a waterfall,, andlater, a waterfall-like opacity descending overthe human ocular lens], catamenia and evencatalog [a breakdown of many words.] Theroot, strophe, means a twisting or turning,as in words such as apostrophe, Dystrophy,on the other hand, is from a Greek root,trophe, meaning growth.
Pestilence is derived from the Latin, pes-tis, meaning plague-like. The psalmist wrote:“Thou shall not be afraid for the terror bynight; nor for the arrow that flieth by day;nor for the pestilence that walketh in dark-ness.” The word, pest, has come to mean anannoyance, a bane, even a scourge.
Plague comes indirectly from the Latin,plaga, meaning to strike or to wound. De-
rivative English words include apoplexy,paraplegia and complain.
Influenza is from the Latin, influentia,meaning the capacity to affect other thingsby intangible means; and inferentially, it re-fers to the ability of the stars to control hu-man destiny. The Italian phrase, influenciadi freddo, meaning of the cold, is the originof the English name given to the respiratoryinfection.
And finally, the word, apocalypse. Theword is derived from the Greek meaning toreveal or to uncover as it is used in the final,apocalyptic book of the New Testament, TheRevelation. The Greek root, calypsus, meansto cover, to hide. In Greek mythology, Ca-lypso, the sea nymph, was daughter of Atlaswho lived on the island of Ogygia. It was shewho captured Odysseus and hid him as pris-oner of love for seven years.
– STANLEY M. ARONSON, MD
Diseases of the HeartMalignant Neoplasms
Cerebrovascular DiseasesInjuries (Accidents/Suicide/Homicde)
COPD
Number (a)285205
384532
Number (a) Rates (b) YPLL (c)2,971 277.7 4603.02,324 217.3 6,206.5**
482 45.1 780.0433 40.5 6,212.0535 50.0 482.5
Reporting Period
12 Months Ending with December 2005December
2005
UnderlyingCause of Death
Live BirthsDeaths
Infant DeathsNeonatal Deaths
MarriagesDivorces
Induced TerminationsSpontaneous Fetal Deaths
Under 20 weeks gestation20+ weeks gestation
Number Number Rates1,116 13,145 12.3*
736 9,708 9.1*(6) (99) 7.5#(4) (81) 6.2#
776 7,155 6.7*225 3,141 2.9*434 4,827 367.2#
43 1,027 78.1#(41) (962) 73.2#
(2) (65) 4.9#
Reporting Period12 Months Ending with
June 2006June2006
Vital Events
Rhode Island MonthlyVital Statistics Report
Provisional OccurrenceData from the
Division of Vital Records
(a) Cause of death statistics were derived fromthe underlying cause of death reported byphysicians on death certificates.
(b) Rates per 100,000 estimated population of1,069,725
(c) Years of Potential Life Lost (YPLL)
Note: Totals represent vital events which occurred in RhodeIsland for the reporting periods listed above. Monthly pro-visional totals should be analyzed with caution because thenumbers may be small and subject to seasonal variation.
* Rates per 1,000 estimated population# Rates per 1,000 live births** Excludes 1 death of unknown age
RHODE ISLAND DEPARTMENT OF HEALTH
DAVID GIFFORD, MD, MPHDIRECTOR OF HEALTH EDITED BY COLLEEN FONTANA, STATE REGISTRAR
V ITAL STATISTICS

421VOLUME 89 NO. 12 DECEMBER 2006
a d v e r t i s e m e n t

422MEDICINE & HEALTH/RHODE ISLAND
NINETY YEARS AGO, DECEMBER 1916An Editorial, “The AMA Organizer in Rhode Island,”
reported that Dr. L.P. Van Dusen, the “official organizer” ofthe AMA, had spent the past six weeks calling on individualphysicians, urging them to join.
A second Editorial, “Board of Health,” commended theState Board of Health for: “…the efficiency and sanity of theirattitude towards the epidemic of infantile paralysis which hasstruck terror to hearts of the parents of children throughoutthe areas afflicted. The sensible investigation of …visitors tothe state and their subsequent observation at their point ofdemarcation is in pleasing contrast to the rigid and thereforeinefficient quarantine and uncertain control as instituted inneighboring states.” The Editorial urged Rhode Island to hirea “trained sanitarian of the type exemplified by Gorgas of thePanama Canal.”
A third Editorial, “Think it Over,” urged members to con-sider merging the Providence and Pawtucket Medical Societ-ies.
A fourth editorial, “Medical Meetings,” recounted the lastmeeting, held at the School for the Feeble-Minded in Exeter,with an ex tempore talk by Dr. Ladd.
FIFTY YEARS AGO, DECEMBER 1956Laurence A. Senseman, MD, discussed “Tranquilizing
Drugs – Uses and Abuses for the Nervous Patient;” e.g.,chlorprimanzine, rauwolfa, serpasil, reserpine, azacyclonal,ritalin.
John E. Verna, MA, the Charles V. Chapin Fellow for Con-tagious Diseases at the Charles V. Chapin Hospital, contrib-uted “Estimation of VI Antigen by a Direct Hemagglutina-tion Test.” He decsribed the new test as “more sensitive forantigen detection than conventional hemagglutination.”
Warren W. Francis, MD, and Robert R. Baldridge, MD,in “Arterial Grafting: Report of an Interesting Case,” describedthe case of a 52 year-old woman admitted to Rhode IslandHospital “with a one year history of increasing bilateral claudi-cation,” primarily in the left leg. She was not diabetic. The firstgraft was found to be “occluded with thrombus.” Another ar-terial hemograft shunt was inserted successfully.
An Editorial, “Doctor Draft,” reported that the draft, whichhad been on the statutes for 6 years, would end in June. “…itwill expire if the Congress amends the regular Selective Servicelaws to permit the service to make special calls for persons whoseskills are needed by the armed forces. Such a special call wouldencompass physicians, but would not be limited to them. Suchan amendment is now in process of drafting, but with the recentEuropean and Near East strife a movement might get underwayearly in 1957 to continue the draft…”
TWENTY-FIVE YEARS AGO, DECEMBER 1981The Journal printed “Reversible Neuropsychiatric Disease
Related to Folate Deficiency,” the first of a series of positionpapers in Neurology which will appear in the Medical Jour-nal, produced by the Division of Neurology, Roger WilliamsGeneral Hospital, and the Brown University Program in Medi-cine. The article concluded: “It is essential that folate levels bemeasured in the patient with diffuse cerebral dysfunction.”
Edward A. Iannuccilli, MD, FACP, and Peter P. Yu, MD,discussed the 5 reported cases in “Adult Fibropolycystic LiverDisease and Symptomatic Portal Hypertension.”
Frederick S. Fish, MD, and Francis H. Scola, MD, con-tributed “The Breast Cancer Detection Demonstration Projectat Rhode Island Hospital,” The authors analyzed the resultsfrom 1973 to 1979: of 700 patients screened, 95 were foundto have biopsy-proved breast cancer.
Donald C. Williams, from the Rhode Island Departmentof Health, contributed “Assessment of Physician Supplies inRhode Island in light of GMENAC Report.” The GraduateMedical Education National Advisory Committee report sug-gested that the state would need more family practitioners,fewer general surgeons.
�
�
�
�VOLUME 1 PER YEAR $2.00NUMBER 1 SINGLE COPY, 25 CENTSPROVIDENCE, R.I., JANUARY, 1917
The Official Organ of the Rhode Island Medical SocietyIssued Monthly under the direction of the Publications Committee
To find out more, or to speak to an Army Health CareRecruiter, call 800-784-8867 or visithealthcare.goarmy.com/hct/50


(800) 652-1051 ● www.norcalmutual.com
Whatever it is that sustains you through the daily challengesof your profession, know that you have an ally in NORCAL.
integrity
whatdrivesyou?
Call RIMS Insurance Brokerage Corporation at (401) 272-1050 to purchase NORCAL coverage.