Embed Size (px)
Citation preview
Inside:Special IssueSpecial IssueSpecial IssueSpecial IssueSpecial Issue
Jeanette Ives Erickson: Nurse
Week Presentation .............. 22222
Strengthening Patient- and
Family-Centered Care ......... 55555
Health Disparities: Nursing’s
Voice in Practice ................. 66666
Pioneers of Healing in
the Sudan ............................ 77777
Family-Centered Care ............. 88888
Family Presence During
Resuscitation ....................... 99999
Yvonne L. Munn Nursing
Research Lecture ............. 1111111111
PICU Reflects on Past
Ten Years .......................... 1212121212
Yvonne L. Munn Nursing
Research Awards ............. 1313131313
CaringCaringMay 19, 2005
H E A D L I N E S
MGHWorking together to shape the future
Patient Care ServicesPatient Care Services
Nurse Week 2005Nurse Week 2005
Staff nurse, Bonnie Eidens, RN, with patient,Sohrab Hashmi, on the Dialysis Unit
Bonnie EidensBonnie Eidens

Page 2
May 19, 2005May 19, 2005Jeanette Ives EricksonJeanette Ives EricksonMGH Nursing today:
healing, leadership, and global action“There exists a fleeting and deliriously exciting
moment in the life of an idea when it teeters betweenwhat one person suspects and what everyone accepts.
In that moment, months or years before it exerts anypractical influence, the idea holds the greatest potential
to inspire and incite. Opportunities, implications,and related discoveries open up from it in all
directions like a hall of mirrors.”
—“Introduction to the year’s Best Innovations”Harvard Business Review, February 2005
“Leadership is much more an art, a belief,a condition of the heart, than a set of things to do.
The visible signs of artful leadership areexpressed ultimately, in its practice.”
—Max De Pree
t started with afast-paced, up-beat,rock-’n’-roll re-cap
of the past ten yearsof nursing at MGH.
And for those of you whomissed it, it was quite aride! In her signatureNurse Week address (set tothe tune of Jefferson Star-ship’s, We Built this Cityon Rock ’n’ Roll), seniorvice president for PatientCare and chief nurse, Jean-ette Ives Erickson, RN,opened with a video retro-spective of some of themost memorable momentsof the past decade, includ-ing implementation of col-laborative governance,development of the Clini-cial Recognition Program,achieving Magnet Hospitalstatus, the introduction ofnew technology, the open-ing of many new units, thefilling of key leadershippositions, and of course, thelegendary march to nation-al championships for herbeloved Patriots and RedSox. Said Ives Erickson,“We may not have builtthis city on rock ’n’ roll,but for me, our work to-gether has been just asmuch fun.”
Focusing on the tri-logy of healing, leadership,and global action first arti-culated by Florence Night-ingale, Ives Erickson fram-ed our agenda for the nextten years. Too long to beincluded in its entirity,what follows is an abridg-ed version of Ives Erick-son’s presentation.
I
This week is an oppor-tunity to honor the impor-tant work of nurses andthank those who supportour practice. Let us beginwith a discussion of ourvision, values, successes...and a few of our failures.
As members of the heal-ing community, our workflows from a rich history ofresearch and intimate ex-periences with patients.
Some of us have stud-ied Florence Nightingale’svision of contemporarynursing and global well-ness. Her work gives us aframework for the past andhelps set the stage for thefuture.
When I first came toMGH and found a need tocreate systems that sup-port patient care delivery,Nightingale became myrole model. Her book,Notes on Nursing, speaksto the environment of careand of nurses’ responsibili-ty for that environment andthe systems that keep pa-tients safe.
Nightingale was influ-ential in the communityand in the world, like manyMGH nurses who left the
comforts of home to servein harsh conditions (inIran, the Sudan, southeastAsia, and Ground Zero inNew York City) to try tobring comfort to countlesspeople with waning hope.Our humanitarian effortshave helped many of to-day’s forgotten people inforgotten lands, many trap-ped behind closed borders,suffering under brutal re-gimes.
I was humbled andprivileged this past Febru-ary to visit our staff caringfor tsunami survivors inBanda Aceh, Indonesia.What had been a bleak andcomfortless existence, wastransformed into a place ofhope by the skilled andcompassionate cliniciansof MGH.
And of course, everyday, thousands of patientsreceive exceptional careright here on Fruit Streetand in our health centers in
Charlestown, Revere, Ev-erett, Chelsea, the BackBay, and the North End.MGH nurses are a symbolof what’s right in the worldand in the profession ofnursing. And none of thiswould be possible withoutthe support of everyonehere at MGH.
Nightingale’s achieve-ments, like our own, in-clude contributions to nurs-ing theory, research, statis-tics, public health, andhealthcare reform. Herlegacy is relevant becausethe journey ahead holdsmany challenges:
The nursing shortageThe building of the newKnight Nursing Centerfor Clinical & Profes-sional Development.Advancing our researchagendaOvercrowding will leadus to build a new inpa-tient facility. Perhapsthis new building willhave universal roomswhere patients don’ttravel—we doPerhaps all operatingrooms will be ORs of thefutureOur commitment to the
future means an increasedcommitment to teachingthe next generation ofnurses. There will be astrong push to control ex-
penses due to shortfalls inMedicaid and Medicarereimbursement. Changes inour demographics andworkforce will lead us tobe more culturally compe-tent. And hopefully thosechanges will include moremen, Latino, Black andAsian nurses.
Advancements in tech-nology will help us. (Witha nod to Ed Coakley) Therobots are coming! Com-bining the art and scienceof holistic nursing practice,education, and research isthe way of the future.
We are the nurses Flo-rence Nightingale envis-ioned. Every day, we deep-en our understanding ofthe nurse as an instrumentof healing. We create totalhealing environments andsacred spaces in our hos-pital and in the world.
In her book, Notes onNursing, Nightingale iden-tified concepts related tothe nurse, the patient’shealth, and the environ-ment. She emphasized thatspiritual, social, and phys-ical support, along with acomfortable and healingenvironment, influence allfactors in healing. Theactive participation of thenurse is part of the healingprocess. So, if healing oc-curs both inward and out-ward, we as nurses haveseveral responsibilities.
We need to develop ourinner selves—develop anability to be present to ourpatients and colleagues,and feel good about whowe are as people and mem-bers of this community.
Nurses are responsiblefor creating a healing en-vironment. In the comingmonths, we will talk more
Page 3
May 19, 2005May 19, 2005
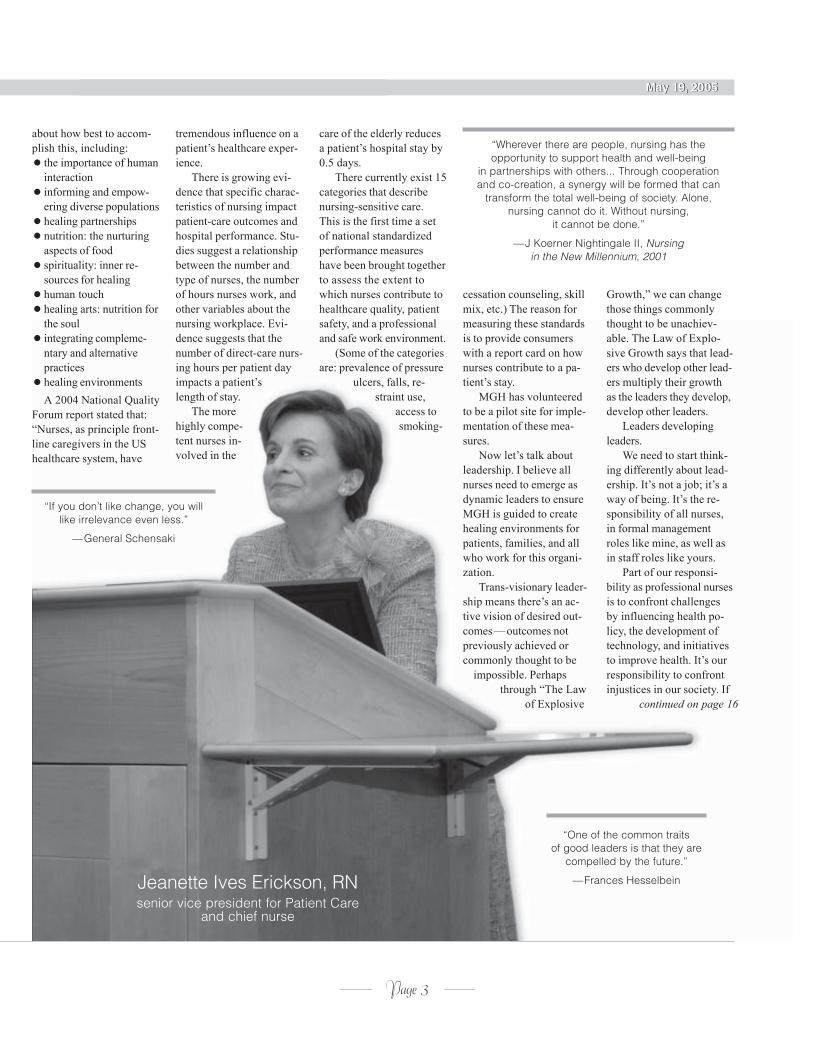
Jeanette Ives Erickson, RNsenior vice president for Patient Care
and chief nurse
“If you don’t like change, you willlike irrelevance even less.”
—General Schensaki
“Wherever there are people, nursing has theopportunity to support health and well-being
in partnerships with others... Through cooperationand co-creation, a synergy will be formed that can
transform the total well-being of society. Alone,nursing cannot do it. Without nursing,
it cannot be done.”
—J Koerner Nightingale II, Nursingin the New Millennium, 2001
continued on page 16
“One of the common traitsof good leaders is that they are
compelled by the future.”
—Frances Hesselbein
about how best to accom-plish this, including:
the importance of humaninteractioninforming and empow-ering diverse populationshealing partnershipsnutrition: the nurturingaspects of foodspirituality: inner re-sources for healinghuman touchhealing arts: nutrition forthe soulintegrating compleme-ntary and alternativepracticeshealing environmentsA 2004 National Quality
Forum report stated that:“Nurses, as principle front-line caregivers in the UShealthcare system, have
tremendous influence on apatient’s healthcare exper-ience.
There is growing evi-dence that specific charac-teristics of nursing impactpatient-care outcomes andhospital performance. Stu-dies suggest a relationshipbetween the number andtype of nurses, the numberof hours nurses work, andother variables about thenursing workplace. Evi-dence suggests that thenumber of direct-care nurs-ing hours per patient dayimpacts a patient’slength of stay.
The morehighly compe-tent nurses in-volved in the
care of the elderly reducesa patient’s hospital stay by0.5 days.
There currently exist 15categories that describenursing-sensitive care.This is the first time a setof national standardizedperformance measureshave been brought togetherto assess the extent towhich nurses contribute tohealthcare quality, patientsafety, and a professionaland safe work environment.
(Some of the categoriesare: prevalence of pressure
ulcers, falls, re-straint use,
access tosmoking-
cessation counseling, skillmix, etc.) The reason formeasuring these standardsis to provide consumerswith a report card on hownurses contribute to a pa-tient’s stay.
MGH has volunteeredto be a pilot site for imple-mentation of these mea-sures.
Now let’s talk aboutleadership. I believe allnurses need to emerge asdynamic leaders to ensureMGH is guided to createhealing environments forpatients, families, and allwho work for this organi-zation.
Trans-visionary leader-ship means there’s an ac-tive vision of desired out-comes—outcomes notpreviously achieved orcommonly thought to be
impossible. Perhapsthrough “The Law
of Explosive
Growth,” we can changethose things commonlythought to be unachiev-able. The Law of Explo-sive Growth says that lead-ers who develop other lead-ers multiply their growthas the leaders they develop,develop other leaders.
Leaders developingleaders.
We need to start think-ing differently about lead-ership. It’s not a job; it’s away of being. It’s the re-sponsibility of all nurses,in formal managementroles like mine, as well asin staff roles like yours.
Part of our responsi-bility as professional nursesis to confront challengesby influencing health po-licy, the development oftechnology, and initiativesto improve health. It’s ourresponsibility to confrontinjustices in our society. If
Page 4
May 19, 2005May 19, 2005
May 19, 2005
Staff nurse, Mary Lowe, RN, with patient, EmilFleischaker, in the Respiratory Intensive Care Unit
Mary LoweMary Lowe

Page 5
May 19, 2005May 19, 2005PresentationPresentationStrengthening patient- and
family-centered careicking off Nurse
Week, executivedirector for theJohn D. Stoeckle
Center forPrimary Care Innova-tion, Susan Edgman-Levitan, PA, presented,“Strengthening patient-and family-centered care:strategies that work,” onMonday, May 2, 2005, inO’Keeffe Auditorium.
Stressing the impor-tance of listening to pa-tients, Edgman-Levitanreminded listeners thatsimply documentinginformation in patients’records doesn’t tell uswhether or not patientsunderstand a particularintervention or instruc-tion. Patients are theonly ones in a position tojudge certain aspects ofcare. What they tell us isinvaluable.
“Bad news travelsfast,” said Edgman-Lev-itan. Customer satisfac-tion is ‘lived’ in the com-munity where good orbad news can make orbreak a hospital’s repu-tation. Public accounta-bility is stronger thanever. Engaging patientsand families in decision-making, care-planning,discharge planning, andpatient-education is cru-cial.
Edgman-Levitanspoke about a patient-centered ‘aptitude,’ andhow our hiring practicesshould target individualswho embody that apti-tude. She shared this
K quote from The Custom-er Comes Second: “Youcan’t teach people to benice... Caring must beinherent to their natures—they have to feel it intheir hearts. And if theydo, their clients will feelit, too.”
First impressions arethe most important—forpatients and staff alike.When staff experience ameaningful, comprehen-sive orientation programit conveys an attitude ofpride in oneself and inthe organization; it in-stills a feeling of self-worth; creates a sense ofbelonging; and enhancesthe working relationshipbetween staff and theorganization. When every-one is aligned around thesame mission, vision,and philosophy, there isa low tolerance for be-havior that doesn’t sup-port that mission.
When patients comeinto a hospital and ex-perience good businesspractices, a positive careenvironment, and feel asense of community, aconnection is made. Loy-alty is born. Edgman-Levitan suggests thatloyalty can be nourishedthrough subsequent hos-pitalizations with con-sistency of staffing, re-admission to the same‘team,’ and primary care-givers for patients whoreturn frequently.
Doing what we can tomaximize a patient’ssense of control over his/
her surroundings instillstrust and confidence.Even when their activi-ties and abilities are lim-ited, we can give themchoices about what theycan do. Do they wanttheir curtains open orclosed? Do they want thebed at a certain angle?Would they like to keepa journal or notebook?
Sharing informationis another way to givepatients a sense of con-trol when they may feelthey’re in a ‘helpless’situation. Informed pa-tients and families arepartners in the healthcareexperience. Sharing laband test results, informa-tion in medical records,patient-education
materials, and the rea-soning behind why wedo interventions andprocedures are all thingspatients want, and have aright, to know. Let thephrase, “Know it, tell it,”be your guide.
Checking a patient’sunderstanding of home-care and follow-up in-structions by way of adischarge ‘quiz’ is moreeffective than simplyreciting information orgiving a patient a writtensheet of information.Asking, “Mr. Smith, howlong should you waitbefore taking a bathwhen you get home?”ensures that Mr. Smithunderstands the in-structions and ismore likely tocomply.
Edgman-Levitan be-lieves that walking a milein our patients shoes is agood way to ensure we’reproviding the best pos-sible care. Do periodicwalk-throughs of yourunit to look for ways toimprove care and services.
In closing, Edgman-Levitan shared this quotefrom Cedar-Sinai MedicalCenter clinical specialist,Marilyn Shirk, RN: “Talk-ing with patients is oftenviewed as ‘not working.’We have to start viewingthis as our most importantwork.”
Susan Edgman-Levitan, PA,executive director, John D. StoeckleCenter for Primary Care Innovation
Susan Edgman-Levitan, PA,executive director, John D. StoeckleCenter for Primary Care Innovation

Page 6
May 19, 2005May 19, 2005PresentationPresentationHealth disparities: Nursing’s
voice in practice
W hen a cauca-sion persongoes into a
hospital securein the knowledge
that he’ll receive thehighest quality care, anda minority individualgoes into the same hos-pital worried he’ll re-ceive less than adequatecare, something is seri-ously wrong with thehealthcare system. Thatwas the topic addressedby director of the PCSDiversity Program, Deb-orah Washington, RN, inher Nurse Week presen-tation, “Health dispari-ties: Nursing’s voice inpractice.”
Washington looked atthe past five decadeschronicling various stu-dies conducted on mino-rity health and healthcare, but it wasn’t untilthe 1990s that a focus ondisparity and inequalityreally emerged as a de-monstrable area of studyamong researchers. Sheshared the National In-stitutes of Health’s defi-nition of health dispari-ties as: “Differences inthe incidence, preva-lence, mortality, andburden of disease andother adverse health con-ditions that exist amongspecific populations inthe United States, in-cluding African Amer-ican, Asian and PacificIslander, Hispanic orLatino, Native Amer-ican, and Native Alas-kan.”
Said Washington, “Ifwe have our guard up,we’re not hearing, we’renot listening. If we’re notlistening to our patients,we’re not providinggood care. The first andmost important thing wemust bring to the bedsideis an open mind.”
Good nursing care,said Washington, in-volves advocacy (cham-pioning causes on behalfof our patients); explain-ing procedures (in a waythat is meaningful andunderstandable to all);following up on issues(discussing options withother disciplines andinvolving the patient);and collaborating withpatients and families(letting everyone knowwhy a particular test orprocedure is being per-formed).
Speaking as an Afri-can American, Washing-ton explained that trust(or lack thereof) is one ofthe biggest obstacles inthe African Americancommunity. For reasonswell documented in ournation’s history, there isa prevailing lack of trustamong people of colorwhen it comes to seekingcare. “We must remem-ber,” said Washington,“that health disparitiesoccur within a socialcontext.”
By way of demon-stration, Washingtonasked a series of ques-tions (from the Develop-ment and Testing of the
Health Care System Dis-trust Scale) designed togauge the level of trust inthe healthcare systemamong African Americanpatients. Questions suchas:
Do you think there is acure for AIDS that isnot being shared withthe public?Do you think medicalexperiments will beperformed on youwithout your know-ledge?Do you think peoplehave access to yourmedical record withoutyour consent?It was startling to see
the percentage of AfricanAmericans polled whoagreed with those state-ments. Are those beliefsvalid? They are to theindividuals who hold
them. We cannot dismissa lack of trust as ‘some-one else’s problem. ‘It’sup to us as clinicians toearn the trust of our pa-tients, and we shouldn’tneed an ‘invitation’ to dothat.
Racism, said Wash-ington, is not always apre-meditated outcome. Awhite caregiver doesn’thave to treat a minoritypatient badly for racialdisparity to exist. Simplytreating a white patientmore favorably has thesame effect. Puttingan end to healthdisparitiesrequires
work on two fronts: im-proving our care at thepolicy level (national,state, and local), andestablishing trustingrelationships with allpatients at the bedside.
We need to take thetime. We need to beaware. We need to payattention to the verbaland non-verbal cues ourpatients give us. A seem-ingly simple questioncould be a patient’s wayof assessing whether ornot we are ‘worthy’ ofher trust. We need to be
courageous enoughto enter into
those relation-ships with oureyes and ourhearts wideopen.
Deborah Washington, RNdirector, Patient Care Services Diversity Program
Deborah Washington, RNdirector, Patient Care Services Diversity Program

Page 7
May 19, 2005May 19, 2005PresentationPresentationGrace Deveney and Kate Fallon:pioneers of healing in the Sudan
Grace Deveney, RN (left)and Kate Fallon, RN
Thomas S. Durant refugee medicine fellows
Grace Deveney, RN (left)and Kate Fallon, RN
Thomas S. Durant refugee medicine fellows
n two separatepresentations,Thomas S. Dur-
ante refugee medi-cine fellows, Grace
Deveney, RN, and KateFallon, RN, shared theirexperiences bringinghumanitarian aid andnursing care to the peo-ple of Sudan, one of themost drought-ridden,politically unstable areasin the world.
Deveney, whose fel-lowship was affiliatedwith Concern World-wide, began with a briefhistory of the social andpolitical conflicts thathave left much of thatregion of Africa withoutfood, running water,shelter, security, or healthcare. To date, 180,000people have been killedand more than two mil-lion displaced, living inrefugee camps under themost dire conditions.
Deveney workedprimarily as part of anutrition program in ElGeniena, in northwesternDarfur. The programused a community-bas-ed, therapeutic care mo-del that brought treat-ment and services intothe community ratherthan making families goto therapeutic feedingcenters as had been thepractice. Many familieswere unable, or unwill-ing, to seek care for theirmalnourished childrenbecause spending pro-longed periods of time atfeeding centers (children
I were required to be ac-companied by a care-taker at all times) tookthem away from theirother children and otherresponsibilities.
The therapeutic careprogram targeted child-ren under five, since thatpopulation was deemedmost susceptible to mal-nutrition. In addition tomalnutrition, Deveneyand her internationalcolleagues treated indi-viduals with malaria,diarrhea, eye infections,chest infections, infesta-tions, and many otherchronic and acute con-ditions.
Part of Deveney’swork involved train-ing community care-givers so the pro-gram could con-tinue after sheand her col-leagues left.
Fallon’s fellowshipwas connected with theAmerican Refugee Com-mittee (ARC) and in-volved establishing andrunning mobile healthclinics in the Nyala-Girayda ‘corridor,’ anarea still at the center ofmuch political unrest.
Said Fallon, “We hadno guidance, no model tofollow; we were essen-
tially giventhis task
and toldto godo it!”
Fallon and her col-leagues consulted otherNGOs (non-governmentorganizations), visited anumber of villages toassess the health needsof the people, obtainedbasic medical suppliesfrom UNICEF and othersources, and put a plantogether to operate amobile clinic.
The small group ofcaregivers learned quick-ly through trial-and-error, solving problemsas they went, and soon
became acohesive
team
of clinicians in the field.At the peak of their
learning curve, Fallon’steam was visiting fivevillages a week providingassessment, consultation,treatment and medicationto hundreds of ‘benefici-aries.’ They saw gun-shotwounds, knife wounds,skin ulcers, infections,malaria, and burns.
One of the unplannedinterventions they intro-duced was a health edu-cation workshop for child-ren to teach basic hy-giene, tooth-brushing,hand-washing, etc., which,said Fallon, isn’t easywhen there’s no runningwater.
Deveney and Fallonboth lived in crude, pri-mitive, dangerous con-ditions for the duration oftheir fellowship. Theyprovided life-saving careto hundreds of Sudaneserefugees.
Said Fallon, “I cameto know and under-stand the people ofSudan on a much
deeper level. It wasthe hardest work
I’ve ever done.And I loved
every min-ute.”

Page 8
May 19, 2005May 19, 2005
Family-centered care at theMassGeneral Hospital for Children:
how are we doing, how important is it?
Mary Lou Kelleher, RNPediatric clinical nurse specialistMary Lou Kelleher, RN
Pediatric clinical nurse specialist
Scientific SessionScientific Session
uilding on thepresentationof Susan Edg-man-Levitan
earlier in the week(“Strengthening Patient-and Family-CenteredCare”), Mary Lou Kelle-her, RN, pediatric clini-cal nurse specialist, pre-sented the results of herresearch study, “Family-centered care at the Mass-General Hospital forChildren: how are wedoing and how importantis it?”
She began with abrief history of the evo-lution of family-centeredcare, which today in-cludes four key elements:
dignity and respectinformation-sharingparticipationcollaborationTo successfully de-
liver patient- and family-centered care, said Kel-leher, we must first agreeon what a family is. Sheput forth the followingdefinition: “Families arebig, small, extended,nuclear, multi-genera-tional, with one parent,two parents, grandpar-ents, aunts, uncles (byblood or friendship) andsiblings. Families liveunder one roof or many.You become part of afamily by birth, adop-tion, marriage, or from adesire to be of mutualsupport—friendship. Afamily is a culture untoitself with different val-
B ues and unique ways ofrealizing its dreams. To-gether, families are thebest source of our richcultural heritage andspiritual diversity. It isthe family that createsneighborhoods, commu-nities, states and na-tions.”
In 2000, the MGHPediatric Service formal-ly adopted family-cen-tered care as its model ofpractice, rewriting itsmission statement andguiding principles toreflect the shift in focus,and renaming the ser-vice, the MassGeneralHospital for Children.
Providing a concep-tual framework for herresearch, Kelleher de-scribed the paradigmshift toward family-cen-tered care as a movementfrom a medical approachto a family-inclusiveapproach; from an indi-vidual focus to a patientand family focus; fromefficiency-based care tonurturing care; from re-stricting information tofreely sharing informa-tion; and from medical-acuity-based practice tovalue-based practice.
In an effort to gaugethe success of MassGen-eral Hospital for Child-ren’s conversion to afamily-centered caremodel, Kelleher craftedthe research question:“What are the similari-ties and differences in
the way parents (fami-lies) and clinical staffrate the performance andimportance of key com-ponents of family-center-ed care at MassGeneralHospital for Children?”
From July throughSeptember, 2004, cus-tomer satisfaction sur-veys were given to fam-ily members and health-care providers in thePediatric Service. Seven-ty statements were putforth that fell into ninecategories, and respond-ents were asked to rateeach statement accordingto performance and im-portance. The rating scaleincluded options rangingfrom ‘Very Unimportant,’to ‘Very Important,’ andregarding performance,‘Unacceptable’ to ‘Ex-ceptional.’
Overall, there weresome significant ‘stati-stical’ differences be-tween the responses re-turned by family mem-
bers and those returnedby care providers, but,said Kelleher, only a fewof those differences wouldbe considered ‘clinically’significant.
In general, familiesrated performance slight-ly lower than care pro-viders rated perform-ance; and when it cameto importance, familiesrated items slightly high-er in importance or thesame as care providers.Results indicated a needto focus more on collab-oration between familiesand healthcare providers;sharing infor-mation;and
developing and usingsupport groups and net-working opportunities.
The study has alreadyprompted action regard-ing patient-education,signage, discharge plan-ning, and a pilot programto assess the feasibilityof including familiesduring patient rounds.Kelleher plans to repeatthe Family-CenteredCare Customer Satisfac-tion Survey next year.
Following Kelleher’spresentation, JeanetteIves Erickson, RN, se-nior vice president forPatient Care, challengedresearchers to study fam-ily-centered care through-out the entire hospital,not just Pediatrics. SaidIves Erickson, “Family-centered care is an im-
portant paradigm shift,one we should
support on everyunit, in everypractice and
setting in thehospital.

Page 9
May 19, 2005May 19, 2005
The impact of a multi-facetedintervention on nurse and physician attitudes
and behaviors toward family presenceduring resuscitation
Susan Warchal, RN, (left),and Patricia Mian, RN
ED staff nurse and psychiatric clinical nurse specialist
Susan Warchal, RN, (left),and Patricia Mian, RN
ED staff nurse and psychiatric clinical nurse specialist
Scientific SessionScientific Session
mergency De-partment psych-iatric clinical
nurse specialist, Patricia Mian,
RN, and staff nurse,Susan Warchal, RN,presented research theyconducted along withSusan Whitney, RN;Joan Fitzmaurice, RN;and David Tancredi,MD, on “The impact of amulti-faceted interven-tion on nurse and physi-cian attitudes and beha-viors toward family pre-sence during resuscita-tion.”
Interest in conductingthe study grew out ofobservations that thepresence of family mem-bers during resuscitationcontinues to be contro-versial among caregiv-ers; there are mixed opi-nions among nurses andphysicians about thispractice; there is po-tential for ethical con-flicts among members ofthe resuscitation team;and there is a dearth ofprotocols and education-al materials to guidepractice in this matter.
Concerns among staffranged from fear thatfamily presence wouldinterfere with patientcare, be traumatic forfamily members, inter-fere with teaching op-portunities, cause anxi-ety over clinical perfor-mance, and have reper-
E cussions related to liabi-lity and confidentiality.
Even in light of thoseconcerns, some thoughtthat having family mem-bers present during re-suscitation could helpincrease families’ under-standing of their lovedone’s condition, actuallyreduce fear and anxiety,provide greater comfortand support for patients,and help facilitate thegrieving process.
So the purpose of thisstudy was to design andimplement a Family-Presence During Resus-citation Program, andevaluate nurse and phy-sician attitudes and be-haviors before and afterprogram implementation.
Approval to conductthe pilot program in theED came in January of2002, and the initialbaseline survey was con-ducted shortly thereafter.Following the initialsurvey, there were edu-cational forums and im-plementation strategysessions that includedrole-modeling; supportand feedback; education-al posters; primary nurs-ing rounds; and attend-ing an ethics conference.
The follow-up surveywas conducted in May of2003. Some of the ques-tions included on thesurvey (both pre- andpost-implementation)
were:If I were being resus-citated, I would wantmy family to have theoption of being presentI would want to bepresent during theresuscitation of a closefamily memberPatients have a right tohave family memberspresent during resusci-tationFamily presence dur-ing resuscitation wouldmake healthcare work-ers more liable to mal-practice suitsIn the presence of fam-ily members, medi-cal staff willchange theirdecisions dur-ing resuscita-tionFamily mem-bers may beupset
watching residentsbeing taught duringresuscitationThe presence of familymembers during resus-citation would makeme anxiousRespondents were
asked if they thought anyof the educational mater-ials/forums influencedtheir attitude on havingfamily members presentduring resuscitation, andwhether their change inattitude could be charac-terized as positive ornegative (or no change).
As a result of this re-
search, the Family Pre-sence Program has beensuccessfully adopted asthe standard of practicein the ED.
One staff nurse wrote,“I had a critically ill pa-tient who died. His sonwas present during life-saving efforts. After hisfather died, the son gaveme a hug and thanked mefor letting him spend thattime with his dad. Thatexperience convinced methat both the patient andson benefited from beingtogether. Had I waited fora ‘good’ time to allow theson into the room, therewouldn’t have been one.”
Said a family member,It was the hardest thingI’ve ever done, but I hadto be there... no ques-tion.”
Page 10
May 19, 2005May 19, 2005
May 19, 2005
Staff nurse, Cheryl Joseph, RN, with patient,John Brogan, in the Post Anesthesia Care Unit
Cheryl JosephCheryl Joseph

Page 11
May 19, 2005May 19, 2005PresentationPresentationYvonne L. Munn Nursing Research
Lecture: “From the bedside to researchand back again”
Ruth McCorkle, RNprofessor, director, Center for Excellence
in Chronic Illness Care, Yale University Schoolof Nursing
Ruth McCorkle, RNprofessor, director, Center for Excellence
in Chronic Illness Care, Yale University Schoolof Nursing
uest lecturer,Ruth McCorkle,RN, professorand director of
the Center forExcellence in ChronicIllness Care at Yale Uni-versity School of Nurs-ing, delivered this year’sYvonne L. Munn Nurs-ing Research Lecture,“From the bedside toresearch and back again:the journey of a nurseresearcher,” on Wednes-day, May 4, 2005.
McCorkle began bysharing how she ‘backedin’ to her career in On-cology nursing in the1960s, when she was anAir Force nurse. “I choseOncology because noone else volunteered,”she said.
By way of encapsul-ating her life’s work,McCorkle reported on anumber of studies sheand others conductedover the years that haveimpacted patient andcaregiver outcomes. In1973, she embarked on astudy of acute symptomsassociated with breastcancer. It became appar-ent through her researchthat pain, immobility,and other symptomswere important aspectsof the cancer experience.
In 1979, her team ofresearchers proposed astudy to test and developa battery of instrumentsto identify ways in whichpatients cope (or fail tocope) with certain psy-
G chosocial variables as-sociated with advancedcancer. It was in thecourse of this study thatthe Symptom DistressScale (SDS) was devel-oped. The SDS was a13-item tool designed tomeasure the degree ofdiscomfort experiencedby patients based onspecific symptoms theyreported.
In 1980, McCorkleand her team developedthe ESDS (EnforcedSocial DependencyScale), a tool to helpidentify the state in whichadult patients requirehelp or assistance fromothers in performingactivities that under or-dinary circumstancesthey could perform them-selves.
McCorklewas involvedin a study thatlooked at theanxiety levelsof patients withcancer, andhow their an-xiety levelschanged asthey passedthrough thevarious stagesof their illness(diagnosis, tocrisis, acute,stable, chronic,unstable, andultimately, end-stage). Theyfound that evenwhen a pa-
tient’s condition did notchange significantly, thepatient’s anxiety (relatedto the disease) declinedover time.
McCorkle reportedon her “Series of Inter-vention Studies,” con-ducted in 1983. This wasa study to test the effectsof home nursing care onpatients with progressivelung cancer. Patients inthree groups were fol-lowed for eight months.One group received of-fice care only; one groupreceived office care plusstandard home care; andone group received officecare plus oncology homecare.
It was concluded thathome nursing care assist-ed patients with mini-mizing distress from
symptoms and maintain-ing independence longerthan those who receivedno home nursing care.Nurses were also able tohelp patients come togrips with the reality oftheir disease.
McCorkle shared theresults of a number ofother studies she andothers conducted, includ-ing, “The effects of home-care nursing during ter-minal illness on the be-reaved’s psycho-logical distresslevel;” andstudies thatfocused onstandardizednursing inter-ventionprotocols
(SNIPs) on patients andfamily caregivers. Thesestudies led to the imple-mentation of the FamilyLeave Bill (in 1992) andthe Family CaregiversEducation Program (in1993).
In closing, McCorkleadvised that one of themost important inter-ventions caregivers canperform is determiningwhether patients haveadequate home care whenthey’re discharged fromthe hospital. Studiesshow that patients thrivebetter on their own, evenpost-surgically, than theydo when discharged into
situations where theircaregiver is ill or
severely burden-ed by the need
to care for aloved one.

Page 12
May 19, 2005May 19, 2005Pediatric Intensive CarePediatric Intensive CareYou’ve come a long way, babies!
PICU staff reflects on past ten years
I n her Nurse Week presen-tation, senior vice presi-dent for Patient Care,
Jeanette Ives Erickson,spotlighted many of the ac-
complishments and milestonesachieved by MGH nurses overthe past ten years. Inspired toreflect on their own practiceover the past decade, PediatricIntensive Care Unit nurses real-ized they have much to cele-brate, as well. Following is a listof some of the accomplishmentsand innovations achieved in thePICU since 1995.
1995 Increased focus on pri-mary nursing
1995 Pediatric BereavementProgram is held for thefifth consecutive year.
1996 Brenda Miller, RN, ap-pointed nurse manager
1996 Family-Centered Care for-mally adopted as philoso-phy of care, though fam-ily input and presencewas always highly valued
1997 Dawn McLaughlin, RN,first PICU staff nurse torun in the Boston mara-thon to benefit PediatricHematology Oncology
1997 MGH is formally recog-nized as Pediatric LevelOne Trauma Center
1997 Pediatric Cardiac Surgicalprogram revitalized withinflux of increasinglyhigh-acuity patients
1998 Continuous VenovenousHemofiltration (CVVH)begins in Pediatrics aspediatric liver transplantprogram continues to grow(CVVH is an extremelycomplex form of dialysisadministered by nurses)
1999 Kathryn Beauchamp, RN,joins staff as clinical nursespecialist
1999 First family members pre-sent during cardiac arrestof their child; family-cen-tered care moves to newlevel
1999 Pediatric Conscious Sed-ation and Infusion Pro-gram opens in the PICU
1999 Nurse Partners, the pedi-atric after-hours telephonetriage system, moves tothe PICU for the summerprior to restructuring
1999 Louise Sethmann, RN,receives Stephanie Maca-luso Award for Excellencein Nursing Practice
1999 Saint Teresa Benedicta iscanonized in Rome. Oneof the miracles for whichshe is credited occurred inthe PICU; several PICU
nursing staff attend thecanonization
1999 PICU temporarily movesto Bigelow 12 during El-lison 3 renovations; en-hancements include in-stallation of Omnicell,new security system, andadditional family sleeprooms to enhance family-centered care; art workadded to reflect diversityof patients and families.
2000 Technology continues toimprove; new monitorsinstalled with introduc-tion of end-tidal CO2
monitoring (the measure-ment of carbon dioxide atthe end of exhalation)
2001 Heidi Simpson, RN, andBeth Robbins, RN, grad-uate from first New Grad-uate in Critical Care Pro-gram. (Since then, fournew grads have been hir-ed each year with a mini-mum of two preceptorsmentoring each)
continued on next page
PICU staff and their families at SummerFun outing at Houghton’s Pond

Page 13
2002 Pediatric Advance LifeSupport Program is re-vamped in accordancewith new American HeartAssociation guidelines
2002 First PICU retreat heldresulting in first PICUConference for Commu-nity Affiliates. Confer-ence titled, “The RockyRoad to Adolescence”
2003 Music therapy introducedwith harpists volunteeringas part of the HOPESProgram
2003 Debra Burke, RN, ap-pointed associate chiefnurse for Women andChildren’s Nursing
2004 Pediatric nursing leaders(with representation fromMGHf C, North ShoreMedical Center, and New-ton Wellesley), begin tomeet regarding standard-izing care across Partners
2004 First PICU staff recogniz-ed in PCS Clinical Rec-ognition Program (SarahBuck, RN, advanced clin-ician, and Dawn McLaugh-lin, RN, clinical scholar)
2004 PICU team receives Fam-ily-Centered Care Award,highest honor given atMGH for exemplary fam-ily-centered care
2004 Summer Fun grant (alongwith money donated by agrateful family) used tohost picnic at Houghton’sPond for staff, family, andfriends. (Dawn McLaugh-lin, RN, planned the event,which was fun and reju-venating for all)
2004 Second Partners AffiliatesConference held entitled,“Primer in Pediatric LiverTransplantation”
2005 In a comprehensive, col-laborative undertaking toimprove patient safety,the medication distribu-tion system for Pediatricsis redesigned. (The Ruleof Six, a method used to
calculate pediatric medi-cation dosages, is elimin-ated more than three yearsprior to JCAHO’s man-date to do so)
2005 Technological analysis of‘smart’ syringe pumpsand a pediatric drug lib-rary is completed in effortto further enhance patientsafety in the area of pedi-atric medication manage-ment (represents secondmajor project of 2005where Pediatric Nursing,Pharmacy, and Bio-Medi-cal Engineering collabor-ate to improve care)
2005 PICU team receives Ex-cellence in Action Awardpresented by Peter Slavinfor exemplary, collabora-tive patient care (BethRobbins, RN, and PhoebeYager, MD, cited in awarddescription)
2005 PICU nurse, Heidi Simp-son, RN, travels to south-east Asia with MGH andProject HOPE to care forsurvivors of the tsunamidisaster
The next ten yearsPICU staff look forward tomoving into larger quarterssome time in the near future,an ICU with private rooms,each with enough sleepingspace for family members tostay in rooms with their child-ren.
They foresee technologicaladvances that will make pedi-atric procedures less invasive;a greater life expectancy forchildren with pediatric diseasesas nursing and medical exper-tise continues to expand.
Says Brenda Miller, RN,PICU nurse manager, “Thefuture will mirror the past aswe continue to acquire newskills and greater knowledge.Adapting to a changing clin-ical practice requires flexibilityand collaboration, two attri-butes that have been the hall-mark of PICU nursing for thelast decade.”
PICU Nursingcontinued from previous page
May 19, 2005May 19, 2005ResearchResearchRecipients of the 2005 Yvonne L.Munn Nursing Research Awards
Recipients of the 2005 Yvonne L. MunnNursing Research Awards are (at left, l-r):Whitney Foster, RN; Anastasia Michaelidis,RN; Alyona Runyans, RN; Diane Carroll, RN;Marion Phipps, RN; (and Jennifer O’Neill, RN,not pictured) for their study, “Music as aTherapeutic Intervention in the Care ofNeuromuscular and Neurosurgical Patients”(Above l-r): Virginia Capasso, RN, and MaryLarkin, RN, for their study, “PsychologicalInsulin Resistance: a Study of Patients’Attitudes, Perceptions and Fears.”
NursingNursingMay 19, 2005
Page 14
at MGHat MGHat MGHat MGHat MGHat MGHat MGHat MGHat MGHat MGH

May 19, 2005
Page 15
Fun,Fulfilling,
Formidable,Fantastic!
Fun,Fulfilling,
Formidable,Fantastic!
SimplytheBest

Page 16
May 19, 2005May 19, 2005
leadership is about ad-vocating and empower-ing, I want to hear fromyou. That’s what today isall about!
Let’s move on to glo-bal action. Global actionmeans more than takingcare of those in needduring a crisis. What isour role in government?In the debate over end-of-life care? In teachingwellness to the under-served? In understandingand interpreting the is-sues of the day?
The death of TerriSchiavo generated in-tensely polarized debateabout the sanctity andquality of life. At MGH,we have our own debatesabout brain damage, therights of families to deter-mine their fate, and whe-ther dying of dehydra-tion is humane.
On one issue we canbe clear. It is not up topoliticians to determine apatient’s course of treat-ment. It may seem anobvious thing, but know-ing our patients is whatshould guide us in doingthe right thing for eachpatient at the end of life.This is nursing’s work.Don’t ever let anyonetake that away.
We are serious peo-ple, living in serioustimes. In our country,three million children goto bed hungry every day.Five and a half millionpeople between the agesof 16 and 24 are home-less, hungry, and hope-less. Creating a visionfor the next ten years
must take these statisticsinto consideration.
What about thosedays when our Emer-gency Department is ondivert. Emergency De-partment diversion is afailure to create a healing
environment, to take aleadership position, andto act globally for ourcommunity.
If we are to remainthe nursing service ofchoice, we need to askourselves what our prio-rities are for the next tenyears.
(At this point, IvesErickson posed severalquestions, asking parti-cipants to respond usingan electronic, hand-heldkey pad. Four responsesranging from StronglyAgree, to Tend to Agree,to Tend to Disagree, toStrongly Disagree, weretabulated immediatelyand displayed on a videoscreen)
Some of the ques-tions were:
The nursing executiveteam (chief nurse, as-sociate chiefs, nursingdirectors, nurse mana-gers) emphasizes pa-tient safety as much asfinancial and product-ivity goals
Scheduling and workassignments are de-signed to promotesafetyThis organization en-courages error-report-ing, analysis, and feed-back without blameOur organizationalculture continuouslystrengthens patientsafety.
We train and rewardemployees for safetyThe quality of the dis-charge process on yourunit is very goodOver the past year, thequality of the dischargeprocess on your unithas improvedYou play a major rolein ensuring that theEmergency Depart-ment stays off divertHaving patients onstretchers in the Emer-gency Departmentcorridors is a problemyou should be asked tohelp fixYou have an idea thatwould help to keep theEmergency Departmentoff divert.It is important to posi-tion every nurse as aleaderInterdisciplinary col-laboration, includinginterdisciplinary pa-tient care rounds, is thenorm at MGHYou have ample op-portunity to participate
in the decision-makingprocess about nursingpracticeYou influence the qua-lity of nursing practiceon your unitBy this time next year,
we will have a new stra-tegic plan to help usshape the next ten years.
With your help, wewill advance Nightin-
gale’s philosophy andbring nursing practice toa new level locally, re-gionally, and globally. Inthe next decade, we willhave an opportunity tocreate change—to createa revolution in nursing.
What will differen-tiate us will be our rela-tionships with our pa-tients, our collaborationwith our colleagues, andour influence locally,nationally, and interna-tionally.
The most notablework we will do will bein the arena of expertpractice, the develop-ment of the next genera-tion of nurses, and inoutcomes associatedwith nursing researchconducted right here onFruit Street.
These are the meansto an end—not the endof our vision.
We will set the barhigh for advancing clin-icians through the Clin-ical Recognition Pro-
gram. We will re-examineour collaborative gover-nance program. We willlook at launching moreadvisory committees.
If, in fact, robots arecoming, we need to pre-pare for these advancesin technology. I lookforward to the day whenevery nurse has a hand-held device to supportclinical decision-makingand document patientcare.
In the coming year,we will advance the workof a new committee toimplement an acute-caredocumentation system.Our goals: electronicflow sheets, electronicpatient assessment tools,electronic progress notes.But before we automate,we need to review ourpractice and establish aculture where verbal andwritten communicationare embraced.
In the coming year,we will advance our qua-lity and safety agenda.Disclosure of errors andidentification of poten-tial errors will be a prio-rity. Our responsibility isto create an environmentwhere it’s safe to dis-close and discuss errors.
We will continue toidentify and acquire tech-nology that enhancespatient- and employee-safety. Smart pumps arejust one example.
We will address ca-pacity management. Wewill study, gain under-standing, and eliminatedelays in care. We willdesign new facilitieswith enhanced structuresto eliminate chaos. Andwe will partner with
Jeanette Ives Ericksoncontinued from page 3
continued on next page
“May we hope that, when we are all dead and
gone, leaders will arise who have been personally
experienced in the hard, practical work, the difficulties
and the joy of organizing nursing reforms, and who will
lead far beyond anything we have done!”
—Florence Nightingale

May 19, 2005
Page 17
May 19, 2005
Next Publication Date:June 2, 2005
Published by:Caring Headlines is published twice eachmonth by the department of Patient Care
Services at Massachusetts General Hospital.
PublisherJeanette Ives Erickson RN, MS,
senior vice president for Patient Careand chief nurse
Managing EditorSusan Sabia
Editorial Advisory BoardChaplaincy (interim)
Marianne Ditomassi, RN, MSN, MBA
Development & Public Affairs LiaisonVictoria Brady
Editorial SupportMarianne Ditomassi, RN, MSN, MBAMary Ellin Smith, RN, MS
Materials ManagementEdward Raeke
Nutrition & Food ServicesMartha Lynch, MS, RD, CNSD
Office of Patient AdvocacySally Millar, RN, MBA
Orthotics & ProstheticsMark Tlumacki
Patient Care Services, DiversityDeborah Washington, RN, MSN
Physical TherapyOccupational Therapy
Michael G. Sullivan, PT, MBA
Police & SecurityJoe Crowley
Reading Language DisordersCarolyn Horn, MEd
Respiratory CareEd Burns, RRT
Social ServicesEllen Forman, LICSW
Speech-Language PathologyCarmen Vega-Barachowitz, MS, SLP
Volunteer, Medical Interpreter, Ambassadorand LVC Retail Services
Pat Rowell
DistributionPlease contact Ursula Hoehl at 726-9057 for
all issues related to distribution
Submission of ArticlesWritten contributions should be
submitted directly to Susan Sabiaas far in advance as possible.
Caring Headlines cannot guarantee theinclusion of any article.
Articles/ideas should be submittedin writing by fax: 617-726-8594or e-mail: [email protected]
For more information, call: 617-724-1746.
Please recycle
industry to do this work.We will address quality and
safety; clinical business devel-opment; clinical innovations;communication; informationsystems; new business opportu-nities; and process improve-ment.
We will do everything in ourpower to fill vacant nursingpositions. We will be known asa learning organization as ournurses are recognized as world-
renowned preceptorsand educators.
We will do ev-erything in our pow-
er to end the nursing shortage.Staffing ratios, scholarshipprograms, and mandates willnot solve the problem. We neednew answers.
I take full responsibility forarticulating a vision for thefuture—one that has not previ-ously been achieved or is com-monly considered impossible.
Through my trust in you asindividuals, my commitment toour patients, my passion for
our profession, and my beliefin the need for everyone tohave meaningful employment,I promise that MGH will be abeacon for professional nurs-ing.
In the coming months, youwill have an opportunity toinfluence the work ahead. I’llkeep you apprised of this im-portant work in future issues ofCaring Headlines. It has beena pleasure to work with you forthe past nine years. I know theyears ahead are going to beincredible.
Courtney Craig, RN, with mom-to-be, DanaFiore, during pre-natal examination
Courtney CraigCourtney Craig
Jeanette Ives Ericksoncontinued from previous page

Page 18
May 19, 2005May 19, 2005
May 19, 2005
IV nurse, Deb Guthrie, RN, with patient,Sydney Parlow, on the Ellison 16 Medical Unit
Deb GuthrieDeb Guthrie
Page 19
May 19, 2005May 19, 2005
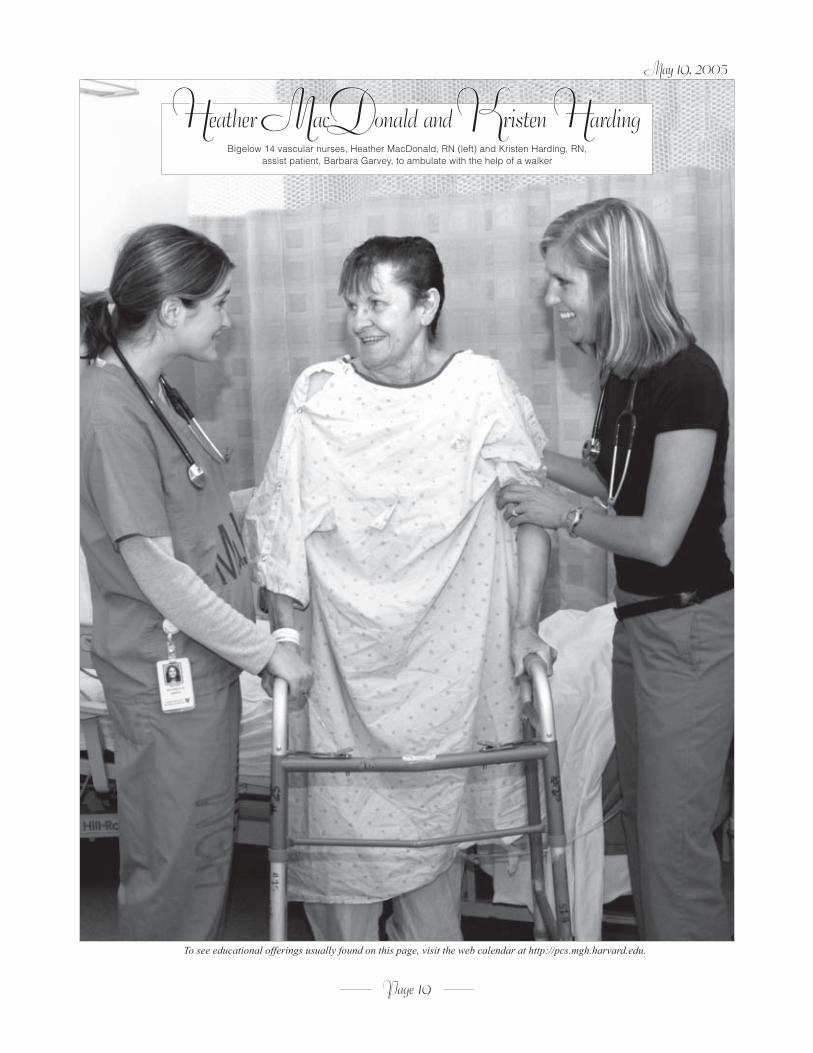
Bigelow 14 vascular nurses, Heather MacDonald, RN (left) and Kristen Harding, RN,assist patient, Barbara Garvey, to ambulate with the help of a walker
Heather MacDonald and Kristen HardingHeather MacDonald and Kristen Harding
May 19, 2005
To see educational offerings usually found on this page, visit the web calendar at http://pcs.mgh.harvard.edu.

Page 20
May 19, 2005May 19, 2005
CaringCaringH E A D L I N E S
Send returns only to Bigelow 10Nursing Office, MGH
55 Fruit StreetBoston, MA 02114-2696
First ClassUS Postage Paid
Permit #57416Boston MA
May 19, 2005
Staff nurse, Katharina Ikels, RN, with patientin the Burn Intensive Care Unit
Katharina IkelsKatharina Ikels





























