Embed Size (px)
Citation preview

CONSUMER PERCEPTION OF CULTURALLY COMPETENT COMMUNITY SERVICES & TREATMENT OUTCOMES
Carol Carstens, PhD, Scott Wingenfeld, MPA, Kwok Tam, MSocSciOhio Department of Mental Health Office of Research & Evaluation
First Meeting on Patient Reported Outcomes in Mental Health
September 30, 2012 Washington DC

2
ABSTRACTObjective: To look at the relationship between patient self-reported experience of care and measures of clinical care.
Data Source/Collection: Data were collected in a mail survey of minority consumers (N = 311).
Design/Methods: In this cross-sectional study, Likert-type scales were used to collect information on client perception of providers’ cultural competence and self-report measures of functioning, quality of life, and social connectedness. Hierarchical regression was used to examine the relationship between cultural competence and the independent variables.
Principal Findings: After controlling for subject-related factors, consumer perception of provider cultural competence was significantly related to self-reported outcome measures.
Conclusions: Cultural competence is a specific approach to patient centered care that can improve the outcomes of mental health services.
Ohio Department of Mental Health Office of Research & Evaluation
3
OVERVIEW
Research Question What is Cultural Competence? Measuring Cultural Competence Measuring Self-Reported
Outcomes Adult Consumer Sample Linear Regression Models Limitations & Sources Cited
Ohio Department of Mental Health Office of Research & Evaluation

4
RESEARCH QUESTION
Does consumer perception of the service providers’ cultural competence have any association with self-reported treatment outcomes?
Ohio Department of Mental Health Office of Research & Evaluation

5
WHY IS CULTURAL PERSPECTIVE IMPORTANT?
Culture falls under the umbrella of person-centered care. It provides a framework for understanding human experience.
Personal & Group IdentityBeliefs & ValuesCustoms & TraditionsLanguage & HistoryOtherness: Minority versus Majority
Ohio Department of Mental Health Office of Research & Evaluation

6
CROSS-CULTURAL BARRIERS TO TREATMENT
Ignorance Indifference Mistrust Fear Discrimination Difference
Beliefs & ValuesLanguageCommunication patterns
Ohio Department of Mental Health Office of Research & Evaluation
7
DSM IV-TR GUIDELINES Inquire about cultural identity — race,
ethnicity, gender, sexual orientation, religion, spirituality, disability status & other self-defining characteristics
Explore cultural explanations of the problem
Consider cultural factors in psychosocial environment and level of functioning
Examine cultural elements in the client-provider relationship
Overall cultural assessment goes into diagnosis and individual treatment plan
Ohio Department of Mental Health Office of Research & Evaluation
8
THE KNOWLEDGE BASE
Very little research looks at the relationship between
provider’s cultural competence & the patient’s symptoms, functioning or social support (Griner & Smith, 2006)
evaluates cultural competence from the consumer perspective (Cornelius et al, 2004)
Ohio Department of Mental Health Office of Research & Evaluation

9
CONSUMER BASED CULTURAL COMPETENCE INVENTORY (CBCCI)
Experimental 52-item Inventory developed by L.J. Cornelius & others in Maryland in 2002.
Awareness of patient culture Respectful behaviors Language interpreters Understanding indigenous practices Consumer involvement Acceptance of cultural differences Community outreach Patient-provider-organization interactions
Ohio Department of Mental Health Office of Research & Evaluation
10
FOR STUDY PURPOSES
20 items from CBCCI tested & analyzed by ODMH-ORE staff in 2012 Ohio administration
Reduced administrative burden Conceptual & statistical considerations
10 items from CBCC survey adopted to analyze consumer-reported treatment outcomes
Factor loadings > .4Two factor solution explains 59.4% s²
Staff level (8 items)Organizational level (2 items)
Cronbach’s α = .91
Ohio Department of Mental Health Office of Research & Evaluation

11
Survey Item #
QuestionFacto
r 1Facto
r 2
2 The staff listen to me and my family when we talk to them. .706
3
The staff who work directly with me on my mental health needs respect my belief in God, a supreme being, or higher power.
.709
4Some of the staff at my agency understand the difference between their culture and mine.
.755
5Staff understand that people of my racial or ethnic group are not all alike.
.739
7When I first called or came to the agency, it was easy to talk to the staff.
.532
8Most of the time, I feel I can trust the staff who work with me.
.707
10
Staff understand some of the different ideas that I, my family, and others from my minority group may have about mental illness.
.743
11
Staff are willing to be flexible and provide alternative approaches or services to my cultural/ethnic treatment needs.
.737
16The agency waiting room has pictures or reading material that show people from my minority group.
.962
17The agency’s reading materials and handouts are in other languages as well as English.
.603
Ohio Department of Mental Health Office of Research & Evaluation

12
MHSIP ADULT CONSUMER SURVEY
Self-rated Perception of Care
General Satisfaction (3 items)Access to Care (4 items)Quality & Appropriateness (8 items)Participation in Treatment (2 items)
Outcomes (8 items) Functioning (5 items) Social Connectedness (4 items)
http://www.nri-inc.org/projects/SDICC/TA/Ganju.Smith_1.pdf
Ohio Department of Mental Health Office of Research & Evaluation

13
MHSIP CLIENT-REPORTED OUTCOMESAS A DIRECT RESULT OF THE SERVICES I RECEIVED:
Domain Items
Outcomes of Services
• I deal more effectively with daily problems
• I am better able to control my life
• I am better able to deal with crisis
• I get along better with family
• I do better in social situations
• I do better in school and/or work
• My housing situation has improved
• My symptoms don’t bother me as much
Ohio Department of Mental Health Office of Research & Evaluation

14
MHSIP CLIENT-REPORTED OUTCOMESAS A DIRECT RESULT OF THE SERVICES I RECEIVED:
Domain Items
Functioning
• I am able to do things that are more meaningful to me
• My symptoms don’t bother as much
• I am better able to take care of my needs
• I am better able to handle things when they go wrong
• I am better able to do things I want to do
Social Connected-ness
• I am happy with the friendships I have
• I have people with whom I can do enjoyable things
• I feel I belong in community
• In a crisis, I would have the support I need from family or friends
Ohio Department of Mental Health Office of Research & Evaluation
15
SAMPLING
Adult survey: 4,740 randomly selected adult consumers with serious mental illness (SMI)
Minority subsample: 1,325 consumers selected if race code indicated person of color OR ethnicity code indicated hispanic origin
175 individuals selected where race = White without hispanic qualifier
Total subsample = 37% of adult consumer sample received cultural competence survey
Ohio Department of Mental Health Office of Research & Evaluation
16
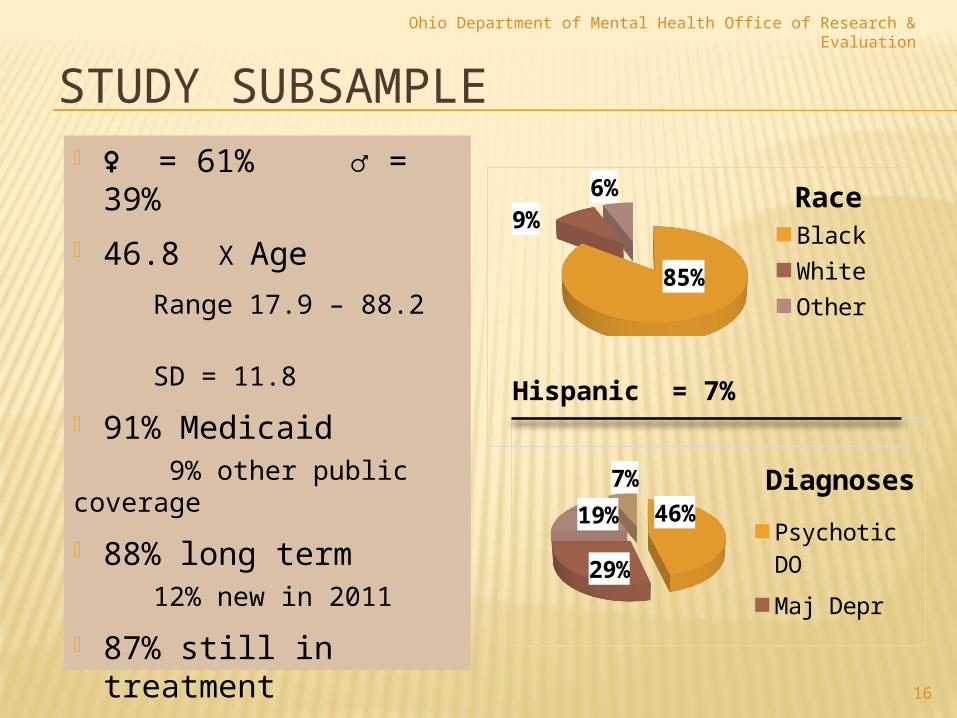
STUDY SUBSAMPLE ♀ = 61% ♂ = 39%
46.8 X Age
Range 17.9 – 88.2
SD = 11.8
91% Medicaid 9% other public coverage
88% long term 12% new in 2011
87% still in treatment
6.5% terminated
7% unknown status
85%
9%6% Race
BlackWhiteOther
Hispanic = 7%
Ohio Department of Mental Health Office of Research & Evaluation
46%
29%
19%7% Diagnoses
Psychotic DOMaj DeprBipolar DO
17
CBCC SURVEY LEADING QUESTION
Some people belong to minority groups because their race, country of origin, history, language, religion, or sexual orientation is different than most people. Do you consider yourself a cultural, racial, ethnic, religious, or sexual minority group member?
Yes No
If you answered YES, what is your minority group? (Specify cultural, racial, ethnic, religious and/or sexual identity)______________________
Ohio Department of Mental Health Office of Research & Evaluation

18
MINORITY STATUS
About 37% of the sample who were people of color or hispanic ethnicity said No to the question about minority status. The US is becoming more racially and
ethnically diverse. Many people in the sample do not appear
to see themselves as “other” or set apart from mainstream society because of race or ethnicity.
Ohio Department of Mental Health Office of Research & Evaluation

19
13 INDEPENDENT VARIABLESENTERED INTO REGRESSION MODELS
Age Race Gender Ethnicity Geographic Profile Diagnosis Service Longevity Service Continuity
Perception of Care General Satisfaction Access Quality &
Appropriateness Participation in
Treatment* Cultural Competence
Ohio Department of Mental Health Office of Research & Evaluation

20
DV: TREATMENT OUTCOMES (N = 311; 13 INDEPENDENT VARIABLES)
Significant Variables β t pBipolar DO -.108 -2.157 .032Major Depression -.176 -3.487 .001Small City Geo Type .177 3.853 .000Participation in Tx .277 4.080 .000Cultural Competence .187 2.970 .003
Ohio Department of Mental Health Office of Research & Evaluation
R² = .422, F = 11.9018,293, p < .000

21
DV: FUNCTIONING(N = 317; 13 INDEPENDENT VARIABLES)
Significant Variables β t pBipolar DO -.212 -2.365 .019Major Depression -.220 -4.261 .001Small City Geo Type .146 3.093 .000Participation in Tx .242 3.462 .001Cultural Competence .183 2.834 .005
Ohio Department of Mental Health Office of Research & Evaluation
R² = .381, F = 10.2218,299, p < .000
22
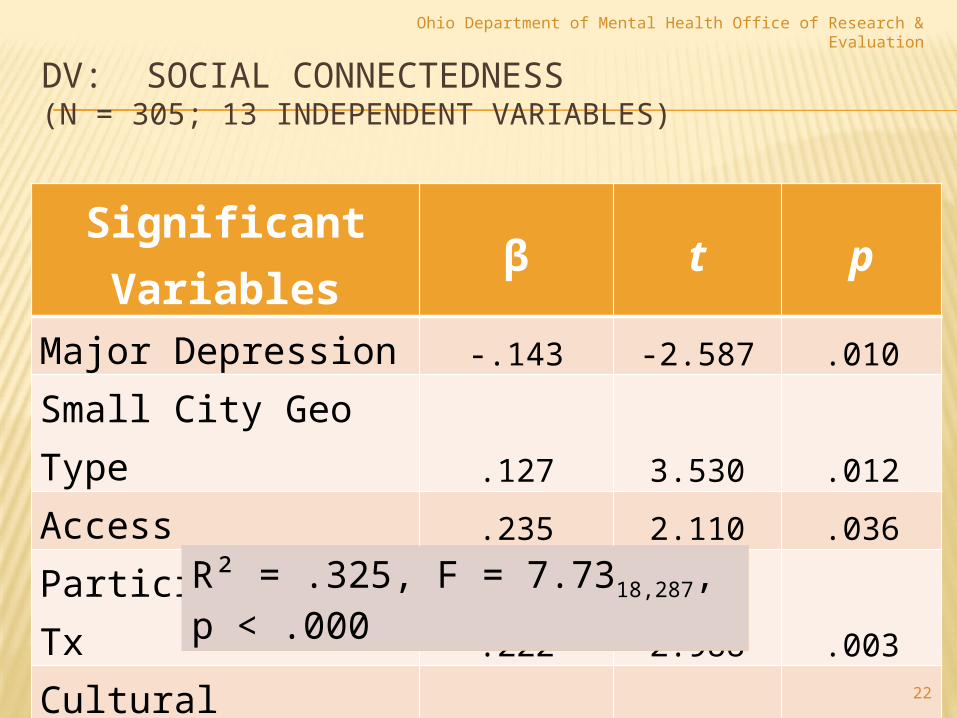
DV: SOCIAL CONNECTEDNESS(N = 305; 13 INDEPENDENT VARIABLES)
Significant Variables β t pMajor Depression -.143 -2.587 .010Small City Geo Type .127 3.530 .012Access .235 2.110 .036Participation in Tx .222 2.988 .003Cultural Competence .427 6.217 .000
Ohio Department of Mental Health Office of Research & Evaluation
R² = .325, F = 7.7318,287, p < .000

23
LIMITATIONS
Cultural Competence: Confounded Construct Minority status Race & Ethnicity Group vs Individual
identity Scale Development:
Limited psychometric testing on CBCC
Dependent Vars: Post-hoc outcome
measures Diversity of Service
Population Unknown: Sample
religious/spiritual identification = 8%
Sample GLBT identification = 2%
Ohio Department of Mental Health Office of Research & Evaluation

SOURCES CITED
Griner, D, & Smith, TB. 2006. Culturally Adapted Mental Health Interventions: A meta-analytic review. Psychotherapy: Theory, Research, Practice, Training 43(4): 531-548.
Cornelius LJ, Booker NC, Arthur TE, Reeves I & Morgan O. 2004. The Validity and Reliability Testing of a Consumer-Based Cultural Competency Inventory. Research on Social Work Practice 14(3): 201-209.
24
Ohio Department of Mental Health Office of Research & Evaluation