Embed Size (px)
Citation preview

Letters to the Editor
enlarged. Brain MRI showed haemorrhagicinfarction in both thalami, extending to theinternal capsule on the right and in theperipheral posterior left parietal lobe.Carotid angiography showed occlusion ofthe vein of Galen, inferior sagittal sinus,and straight sinus consistent with thrombo-sis.
Routine biochemical and haematologicalscreens were normal. Lupus anticoagulantand cardiolipin antibodies were notdetected. The international normalised ratiowas 1-0 (normal range < 1-2) and the acti-vated partial thromboplastin time (APTT)was 30 seconds (normal range 20-34 sec-onds). Antithrombin III and protein C andS concentrations were normal. The activatedprotein C resistance ratio (a ratio of theAPTT measured in the presence of addedactivated protein C to the APTT measuredin its absence) was 1-27 (normal > 2-5).Genetic testing disclosed homozygosity forthe factor V mutation (using the methoddescribed by Bertina et al,3 after amplifica-tion of the factor V cDNA by the poly-merase chain reaction, the cDNA fragmentwas enzymatically digested and hybridisedwith the bioatinylated oligonucleotide spe-cific for the allele of interest). Anti-coagulation was started with intravenousheparin and dexamethasone was given. Herconscious level deteriorated over the next 24hours despite continued therapeutic antico-agulation. She developed fixed dilatedpupils, impaired reflex ocular movements,and exhibited extensor posturing in responseto painful stimuli. Anticoagulation was con-tinued throughout, and two weeks afteradmission further MRI showed progressionof thrombus into the lateral sinus and leftjugular bulb. Over the next four weeks herconscious state improved. She began to fol-low commands appropriately; ocular move-ments returned to normal, but she remainedmute with an asymmetric spastic tetrapare-sis, left worse than right. Over the subse-quent seven months, speech retumed tonear normal with corresponding improve-ment in upper and lower limb function. Sheis now independent in all daily activitiesdespite bilateral upper motor neuron signsand a mild trunkal ataxia. Progress of thecerebral venous thrombosis will be followedup by MRI and it is intended to continueanticoagulation indefinitely.
Activated protein C is a natural inhibitorof blood coagulation which acts by inactivat-ing plasma cofactors Va and VIIIa.Activated protein C resistance is known tooccur in up to 50% of people with a per-sonal and family history of deep venousthrombosis4 compared with a prevalence ofabout 5% in the general population. Thegenetic defect responsible for most cases ofactivated protein C resistance is now knownto be a single point mutation in the factor Vgene on chromosome 1.3 This codes for adefective factor V molecule which is notproperly inactivated by activated protein C.Women taking the oral contraceptive pill
who also have activated protein C resistanceare considered to have a higher risk ofvenous thrombosis than women withactivated protein C resistance alone.'Qestrogens in replacement doses have notbeen shown to increase the risk of thrombo-sis but were stopped in the present case.There are no clear guidelines to the durationof anticoagulation after cerebral venousthrombosis, with or without activated pro-tein C resistance. The decision to continuelifelong anticoagulation in this patient was
based on the catastrophic nature of thevenous thrombosis and on the increased riskof future thrombosis as a result of homozy-gosity for the factor V mutation.Of the patient's family, her mother and
one brother are heterozygous for the factorV mutation and another brother is homozy-gous. They have been advised that theyshould receive standard prophylaxis againstvenous thrombosis for procedures withthrombotic risk but that full anticoagulationwould only be indicated for a proved throm-bosis.
TE KIMBERDepartments ofMedicine and Neurology
JV LLOYDHaematology Unit
BP BROPHYNeurosurgery UnitPD THOMPSON
Departments ofMedicine and Neurology, RoyalAdelaide Hospital, Adelaide, Australia.
Correspondence to: Dr T E Kimber, NeurologyUnit, Royal Adelaide Hospital, North Terrace,Adelaide SA 5000, Australia.
1 Svensson PJ, Diihlback B. Resistance to acti-vated protein C as a basis for venous throm-bosis. Lancet 1994;330:517-22.
2 Bridey F, Wolff M, Laissy JP, Morin V,Lefebvre M, de Prost D. Fatal cerebralvenous sinus thrombosis associated with theFactor V Leiden Mutation and the useof oral contraceptives. Thrombostasis andHaemostasis 1995;74: 1382.
3 Bertina R, Koeleman B, Koster T, et al.Mutation in blood coagulation factor V asso-ciated with resistance to activated protein C.Nature 1994;369:64-7.
4 Griffin JH, Evatt B, Wideman C, FernandezJA. Anticoagulant C pathway defective inmajority of thrombophilic patients. Blood1993;82: 1989-93.
5 Vandenbroucke J, Koster T, Briet E, ReitsmaP, Bertina R, Rosendaal F. Increased risk ofvenous thrombosis in oral contraceptiveusers who are carriers of factor V Leidenmutation. Lancet 1994;344:1453-6.
Isolated dysarthria caused by a rightparavermal infarction
Information on the topography of speechdisorders in cerebellar disease is lacking. '
The few reports agree that the paravermalzone of the rostral cerebellum is the mostfrequent site of damage in patients withdysarthria and focal cerebellar disorders. 1-3However, it is not clear if there is a cerebel-lar hemispheric dominance. In fact, topo-graphical study of the cerebellar speechcentre is difficult because most speech disor-ders in cerebellar lesions result from involve-ment of brain stem or occipitotemporalstructures.We report details of a patient with a single
infarct in the right paravermal zone who pre-sented with an isolated dysarthria.The patient was a 78 year old right
handed man (Edinburgh handedness inven-tory: 16) with an abrupt onset of dysarthriawithout other symptoms.On admission he was alert and oriented.
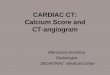
There was severe dysarthria, consisting ofslurred articulation and exaggerated conso-nants. The rest of the neurological examina-tion was normal, without gait disturbance,disequilibrium or limb ataxia, or dysphagia.His gag reflex was normal. Initial CT wasnormal. Brain MRI showed an ischaemiclesion located in the paravermal zone of theright rostral cerebellar hemisphere, in theterritory of the medial branch of the superiorcerebellar artery (figure).The patient had a good clinical outcome,
and recovered completely from the speechdisorder within 10 days.The patient presented with a pure cere-
bellar dysarthria after a right superior cere-bellar artery infarction involving the rightrostral cerebellar hemisphere. This area cor-responds with that delineated by previousstudies' I but in the opposite cerebellarhemisphere. Thus the present case is thefirst report of isolated dysarthria caused by aright paravermal infarct in a right handedpatient.
Dysarthria is common in superior cerebel-lar artery infarcts, being a characteristic signof involvement of the medial branch of thesuperior cerebellar artery.' 1 4 In fact,dysarthria may be the only distinguishingclinical feature between lateral posteriorinferior cerebellar artery infarcts and supe-rior cerebellar artery infarcts.4 However,
(A) AxialMRI T2 weighted scan and (B) Coronal MRI Tl weighted scan showing an infarct inthe superior portion of the right paravermal zone (medial branch of the superior cerebellar artery).
205

Letters to the Editor
dysarthria is usually associated with othersymptoms, such as vomiting, limb ataxia, oraxial lateropulsion.
In posterior inferior cerebellar artery andanterior inferior cerebellar artery territoryinfarcts dysarthria is an unusual symptom.4There were no detailed phonetic descrip-tions in the cases reported, and brain stemsigns were present as well. So, it might besuspected that his speech impairmentresulted from an involvement of brain stemstructures.
Lechtenberg and Gilman2 first noted thatdysarthria developed most often after dam-age extending into the superior paravermalsegments of the left cerebellar hemisphere.Amarenco et al3 confirmed this finding in apatient with an isolated cerebellar dysarthriaafter a small infarction in the left paravermalzone; but they considered a minute mirrorimage lesion to be of no importance, thepatient's hand dominance was not reported,and MRI was not performed. Nevertheless,both studies strongly implicated the leftcerebellar hemisphere in the development ofdysarthria. Ackermann et al I did not corrob-orate the notion of an exclusive left sidedparavermal cerebellar speech cortex; three ofthe four dysarthric patients in their studyhad unilateral right sided ischaemia due toocclusion of the superior cerebellar artery;all of them were right handed. The fourthhad a bilateral cerebellar infarction.More recently, increasing evidence sug-
gests a role for the cerebellum in cognitivefunctions such as language. Silveri et allreported a patient with agrammatical speechafter a posterior inferior cerebellar arteryinfarction, suggesting a right cerebellarhemispheric dominance for language func-tion. It is not clear if that hemispheric domi-nance exists for speech function.The well delineated lesion in our patient
agrees with the hypothesis that the rightcerebellar hemisphere is the most likely sitefor cerebellar speech function as cerebro-cerebellar connections are predominantlycontralateral and the left cerebral hemi-sphere is dominant for speech function inright handed people. However, it may alsobe possible that the site of the infarct (theparavermal zone) is more important than theside.
In conclusion, as well as describing anexceedingly uncommon clinical presentationof a superior cerebellar artery infarction, ourreport suggests the superior right paravermalzone as the possible site of the cerebellarspeech centre, and supports the hypothesisof functional interrelation between supraten-torial structures and cerebellum in func-tional domains outside the motor system.
A GIRONELLDepartment ofNeurology,
Hospital de la Santa Creu i Sant Pau,A ARBOIX
Department ofNeurology,Hospital Central-La Alianfa,
JL MARTI-VILALTADepartment ofNeurology,
Hospital de la Santa Creu i Sant Pau,Auwnomous University ofBarcelona,
Barcelona, Catalonia, Spain
Correspondence to: Dr A Gironell.
1 Ackermann H, Vogel M, Petersen D, PorembaM. Speech deficits in ischaemic cerebellarlesions. JNeurol 1992;239:223-7.
2 Lechtenberg R, Gihnan S. Speech disordersin cerebellar disease. Ann Neurol 1978;3:285-90.
3 Amarenco P, Chevrie-Muller C, Roullet E,Bousser MG. Paravermal infarct and isolatedcerebellar dysarthria. Ann Neurol 1991;30:211-3.
4 Barth A, Bogousslavsky J, Regli F. The clinicaland topographic spectrum of cerebellar
infarcts: a clinical-magnetic resonance imag-ing correlation study. Ann Neurol 1993;33:451-6.
5 Silveri MC, Leggio MG, Molinari M. Thecerebellum contributes to linguistic produc-tion: a case of agrammatic speech following aright cerebellar lesion. Neurology 1994;44:2047-50.
Bilateral internal carotid artery agene-sis
Bilateral internal carotid artery agenesis isextremely rare. Agenesis of the internalcarotid artery may cause cerebrovasculardiseases such as subarachnoid haemorrhageor cerebral ischaemia. We describe a patientwith bilateral internal carotid artery agenesismanifesting as intracerebellar haemorrhage.A 57 year old woman suddenly developed
vertigo and vomiting with severe headache,and was brought to our hospital by ambu-lance on 19 November 1993. She was alertwith slight ataxia on the right side. Brain CTshowed a haematoma 2 cm in diameter in
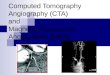
the subcortical region of the right cerebellarhemisphere. Brain MRI showed no vascularmalformation near the haematoma, but anMR angiogram (base view) showed abnor-mal dilatation of the basilar artery andabsence of the internal carotid arteries. Bothanterior cerebral arteries and middle cere-bral arteries were filled from the enlargedposterior communicating arteries. Trans-femoral cerebral angiography showed nobifurcation of either common carotid arteryand absence of bilateral internal carotidarteries. The ophthalmic arteries were sup-plied through the middle meningeal artery.Left vertebral angiography showed anenlarged and tortuous basilar artery. A highresolution CT of the skull base showed com-plete absence of the carotid canals on bothsides, indicating bilateral internal carotidartery agenesis.The patient gradually improved with con-
servative medical treatment and was dis-charged on 13 December with noneurological deficit. She died suddenly athome of heart failure on 30 January, 1994.
Congenital internal carotid artery agenesisis a very rare anomaly, with only about 100
Figure 1 Left: CT showing a haematoma in the subcortical region of the right cerebellar hemisphere.Right: High resolution skull base CT showing complete absence of the carotid canals on both sides.
Figure 2 MR angiogram (base view) showing abnormal dilatation of the basilar artery (largearrow) and absence of the bilateral ICAs. Both anterior cerebral arteries (small arrow heads) andmiddle cerebral arteries (large arrow heads) were filledfrom the enlarged posterior communicatingarteries (small arrows).
206