Embed Size (px)
Citation preview

PERIPHERAL VASCULAR DISEASE (M SHISHEHBOR, SECTION EDITOR)
Carotid Artery Stenting Versus Carotid Endarterectomy:Post CREST
Michael Buschur & Hitinder S. Gurm
Published online: 5 February 2012# Springer Science+Business Media, LLC 2012
Abstract The risk of stroke associated with carotid arterystenosis can be reduced with carotid endarterectomy orcarotid artery stenting in carefully selected patients. Whilesurgery has been the traditional treatment there have beenmany trials comparing carotid endarterectomy with carotidartery stenting, and stenting has shown promising results forcertain patient populations. This article reviews the naturalhistory of carotid artery stenosis, the data supporting carotidendarterectomy, trials directly comparing surgery to stent-ing, and current recommendations for each modality.
Keywords Carotid artery disease . Carotid artery angioplastyand stenting . Carotid endarterectomy
Clinical Trial AcronymsACAS Asymptomatic Carotid Atherosclerosis StudyACST Asymptomatic Carotid Surgery TrialCAVATAS Carotid and Vertebral Artery Transluminal
Angioplasty StudyCREST Carotid Revascularization Endarterectomy
Versus Stenting TrialECST European Carotid Surgery Trial
EVA-3S Endarterectomy Versus Stenting in Patientswith Symptomatic Severe Carotid Stenosis
ICSS International Carotid Stenting StudyNASCET North American Symptomatic Carotid
Endarterectomy TrialSAPPHIRE Stenting and Angioplasty with Protection in
Patients at High Risk for EndarterectomyTrial
SPACE Stent Protected Angioplasty Versus CarotidEndarterectomy in Symptomatic Patients
Introduction
Carotid artery stenosis was first described in 1951 as athero-sclerotic disease at the carotid bifurcation leading to ischemicsymptoms in the ipsilateral eye and brain [1]. Carotid plaquesincrease the risk of stroke and cerebral infarction in asymp-tomatic patients [2]. In addition, carotid plaque burden is anindependent predictor of all-cause and cardiovascular mortal-ity [3]. Treatment of carotid artery stenosis can reduce the riskof stroke and related deaths [4]. Treatment options includemedical management, carotid endarterectomy (CEA), andcarotid artery stenting (CAS) (Fig. 1).
Carotid Endarterectomy
CEA has long been the mainstay of treatment for carotidstenosis as it has been shown to be superior to medicaltherapy in patients with and without symptoms [5]. Severallarge studies have proven that CEA is beneficial for asymp-tomatic patients with severe coronary stenosis (60% to 99%)[6–8].
M. Buschur :H. S. Gurm (*)University of Michigan Cardiovascular Center,2A 394, 1500 East Medical Center Drive,Ann Arbor, MI 48109, USAe-mail: [email protected]
M. Buschure-mail: [email protected]
M. Buschur :H. S. GurmVeterans Affairs Ann Arbor Healthcare System,Ann Arbor, MI, USA
Curr Cardiol Rep (2012) 14:135–141DOI 10.1007/s11886-012-0250-5

The Veterans Affairs (VA) trial assigned 444 men at 11VA centers, with 50% to 99% asymptomatic carotid steno-sis, to aspirin alone or aspirin plus CEA. The end point wasthe combined incidence of transient ischemic attack (TIA),transient monocular blindness, and stroke at 48 months. Theincidence of ipsilateral neurologic events was 8% in thesurgical group and 20.6% in the medical group. The inci-dence of ipsilateral stroke alone was 4.7% in the surgicalgroup and 9.4% in the medical group. An analysis of strokeand death combined within the first 30 postoperative daysshowed no significant differences. CEA reduced the overallincidence of ipsilateral neurologic events in a selected groupof male patients with asymptomatic carotid stenosis [6]. TheACAS study randomized 1662 adults with 60% to 99%carotid stenosis, to CEA and aspirin 325 mg daily, or aspirintherapy alone. The primary end point was cerebral infarctionor any stroke or death occurring in the perioperative period.After a median follow-up of 2.7 years, the incidence ofipsilateral stroke and any perioperative stroke or death ratewas significantly lower in the surgical group than withaspirin alone (5% vs 11%) for a relative risk reduction of0.53 (95% CI, 0.22–0.72) [7]. The ACST trial is the largestmulticenter study of asymptomatic carotid surgery thatfound a significant benefit for CEA. This study randomized3120 asymptomatic patients with ≥60% carotid stenosis toimmediate CEA or deferral of CEA until a definite indica-tion. The end points were perioperative (within 30 days of
surgery) stroke and myocardial infarction (MI) and non-perioperative stroke. The 5-year risk in the immediateCEA group was significantly lower than the CEA deferralgroup (6.4% vs 11.8%; 95% CI, 2.96–7.75). A similar resultwas found for fatal or disabling stroke (3.5% vs 6.1%) andfor fatal stroke alone (2.1% vs 4.2%). The trial concludedthat the benefit of CEA is delayed, as the asymptomaticpatients had a poor outcome after CEA for up to 2 yearsbecause of perioperative morbidity. Significant benefit didnot begin until 2 years after surgery [8].
A meta-analysis including the VA, ACAS, and ACSTtrials showed that despite a 3% perioperative stroke or deathrate, CEA for asymptomatic patients reduced the risk of anystroke by 30% over 3 years. The absolute risk reduction wasonly 1% per year, but may have been higher with longerfollow-up [5].
CEA Indications in Symptomatic Patients
Symptomatic carotid disease describes focal neurologicsymptoms that are sudden in onset and attributable to spe-cific carotid artery distributions. This includes one or moreTIAs characterized by focal neurologic symptoms, transientmonocular blindness, or one or more minor ischemic strokeswithin the previous 6 months [9]. Multiple large trials haveshown dramatic benefit for CEA in patients with symptomaticcarotid artery stenosis [9–11].
NASCET
This randomized controlled trial (RCT) compared CEAversus medical treatment alone in patients with symptomaticcarotid stenosis. Fifty centers enrolled 1,212 patients with aTIA or nondisabling stroke within 120 days prior to entryand carotid stenosis of 70% to 99%. The risk of stroke anddeath was higher at 30 days in the patients treated with CEA(5.8%) versus those treated with medical therapy (3.3%).However, at 2 years of follow-up, CEA had a lower risk ofany stroke or death (15.8% vs 32.3%), any ipsilateral stroke(9% vs 26%), major or fatal ipsilateral stroke (2.5% vs13.1%), and any major stroke or death (8.0% vs 19.1%).Therefore, CEA was found to be highly beneficial forpatients with recent TIAs or nondisabling strokes with ste-nosis of 70% to 99% [10].
ECST
This multicenter, prospective trial randomly assigned 2,518patients with a nondisabling ischemic stroke, TIA, or retinalinfarct to medical therapy with aspirin or to CEA. At 3 years,
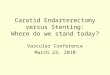
Fig. 1 A 71-year-old female was discovered to have severe asymp-tomatic left internal carotid artery (LICA) stenosis (arrow) as part ofher evaluation for transcatheter aortic valve replacement. a She hadcritical aortic stenosis (valve area 0.6 cm2), morbid obesity (body massindex 51.7 kg/m2), and severe chronic obstructive pulmonary diseasethat made her a high risk surgical candidate. b She underwent success-ful protected stenting of her LICAwith a 6–8/40 tapered Acculink Stent(Abbott Vascular, Abbott Park, IL) (arrow) and the use of an NAVEmboshield (Abbott Vascular) emboli protection device.
136 Curr Cardiol Rep (2012) 14:135–141

patients treated with CEA had significant reductions in theincidence of ipsilateral ischemic stroke compared to aspirinalone (2.8% vs 16.8%) and in the total risk of surgical death,surgical stroke, ipsilateral ischemic stroke, or any otherstroke (12.3% vs 21.9%). The risk varied with age andsex, with less benefit in women and younger patients. Afollow-up report from the same authors after 6 years con-firmed that CEA was beneficial for symptomatic carotidstenosis of 80% to 99% [11].
Criticism of CEA Trials
Critics have pointed out that the above trials had experi-enced surgeons working at expert hospitals. One studyexamined the perioperative mortality among Medicarepatients undergoing CEA in nonfederal institutional settings[12]. This trial showed that the perioperative mortality wassignificantly higher than that what was reported in NASCETand ACAS. Patients undergoing their procedures at trialhospitals had a mortality risk reduction of 15% (95% CI,0% to 31%) compared with high-volume non-trial hospitals;a risk reduction of 25% (95% CI, 7% to 40%) compared toaverage-volume hospitals; and a risk reduction of 43% (95%CI, 25% to 56%) compared with low-volume hospitals.Furthermore, surgeons who only performed less than threeCEAs every 2 years had the highest mortality (2%) andmajor morbidity (9.2%) [13].
Carotid Artery Stenting
CAS has been shown to be safe and effective and is beingincreasingly used to treat carotid stenosis in symptomatic andasymptomatic patients. A number of studies have comparedthe two treatment strategies.
Comparison of CEAVersus CAS in AsymptomaticPatients
No high-quality RCTs comparing CEA with CAS havefocused exclusively on patients with asymptomatic carotiddisease.
Cochrane Review
This large review included a subanalysis looking at two trialswith 136 symptomatic patients. This found no differencebetween CEA and CAS for the combined end point of anystroke or death within 30 days. During long-term follow-up,the analysis found no significant difference between CEA and
CAS in the risk of stroke or death. CAS had significantreductions in cranial nerve injury and MI, but significantincrease in 30-day death and stroke rates [5]. There wasno difference in the 24-month end point of death or stroke[14].
SAPPHIRE
This RCT assigned 334 patients to CAS with the use of anembolic protection device (EPD) or CEA. The study en-rolled both symptomatic patients with ≥50% carotid stenosisand asymptomatic patients with ≥80% carotid stenosis.More than 70% of patients had asymptomatic carotid dis-ease. The primary end point was the incidence of a majorcardiovascular event at 1 year including the following:death, stroke, and MI within 30 days after the intervention;and death or ipsilateral stroke between 31 days and 1 year.The study was designed to test the hypothesis that CAS wasnot inferior to CEA. The primary end point occurred in 20patients in the CAS group (12.2%) and in 32 patients in theCEA group (20.1%). CAS was not inferior to CEA inpatients with symptomatic or asymptomatic severe carotidstenosis who were at high surgical risk.
A common criticism of this study is that more than 20%of the patients in each group had recurrent carotid arterystenosis, which favors CAS as there are more complicationswith redo CEA than primary CEA. The better outcomes at1 year for CAS were mostly due to higher perioperative MIin the CEA group. Finally, outcomes for both groups werepoor compared to NASCET and had higher than 3% rate ofperiprocedural complications in both groups [15]. A follow-up report at 3 years on the SAPPHIRE patients showed nosignificant differences in long-term outcomes in patientstreated with CEA or CAS with severe carotid stenosis andincreased surgical risk [16].
Comparison of CEAVersus CAS in SymptomaticPatients
CEA remains the preferred treatment for most patients withsymptomatic carotid atherosclerosis. One of the initial head-to-head comparisons reported that CAS and CEA had similarrates of adverse outcomes. This study was an RCT in acommunity hospital enrolling 104 patients with symptomaticcarotid stenosis greater than 70% and assigning them to CASor CEA. One death occurred in the CEA group (1/51) and oneTIA occurred in the CAS group, with no patients having astroke. While it had a small sample size, this study concludedthat CAS is equivalent to CEA in reducing carotid stenosiswithout increased risk for major complications of death orstroke [17].
Curr Cardiol Rep (2012) 14:135–141 137

CAVATAS
This was the first major multicenter trial comparing CEA toendovascular therapy. A total of 253 patients underwent CEAand 251 underwent an endovascular procedure. Approximately90% of the patients were symptomatic. The combined strokeand death rate at 30 days post procedure was 9.9% for the CEAarm and 10% for the endovascular arm. Death or disablingstrokes was 5.9% in the CEA arm compared to 6.4% in theendovascular arm. However, only 55 of the 251 patients in theendovascular group were treated with a stent and an EPD wasnot used. Endovascular treatment had similar major risks andeffectiveness at prevention of stroke during 3 years comparedwith CEA and less minor complications [18]. Long-termCAVATAS follow-up looked at 8-year results and found thatthe incidence for ipsilateral and perioperative stroke was notsignificantly different, 11.3% in the endovascular arm and8.6% in the CEA arm [19].
In another follow-up, severe carotid restenosis (> 70%)occurred significantly more in patients in the endovasculararm than the CEA arm over 5 years; 30.7% versus 10.5%(hazard ratio [HR], 3.17; 95% CI, 1.89–5.32; P<0.0001).However, patients who had a stent placed had lower rate ofrestenosis compared to those treated with angioplasty alone,16.6% versus 36.2% (HR, 0.43; 95% CI, 0.19–0.97; P00.04). This finding may be of limited significance in con-temporary practice since stenting is universally used as partof the endovascular therapy of carotid disease [20].
ICSS
This study looked at 1,713 patients over the age of 40 yearswith symptomatic carotid artery stenosis greater than 50%and randomly assigned them to CEA or CAS. At 120 days,8.5% of CAS patients versus 5.2% of CEA patients reachedthe combined end point of stroke, death, or MI. Comparedto the CEA arm, the CAS arm had higher rates of any stroke(7.7% vs 4.1%), any stroke or death (8.5% vs 4.7%), and all-cause death (2.3% vs 0.8%). There was no significant dif-ference between the groups in disabling stroke or death [21].
SPACE
This multicenter European study enrolled 1,200 patientswith symptomatic carotid artery stenosis and randomlyassigned them within 180 days of TIA or moderate stroketo CAS or CEA. The primary end point was ipsilateralischemic stroke or death at 30 days after the procedure.The primary end point occurred 6.84% with CAS and6.34% with CEA (absolute difference, 0.51%; 90% CI,1.89–2.91). SPACE failed to prove noninferiority of CAS
compared with CEA [22]. A 2-year follow-up on theSPACE trial revealed no significant difference betweenCAS and CEA in periprocedural stroke or death and ipsilat-eral ischemic stroke (9.5% vs 8.8%). However, recurrentcarotid stenosis ≥70% was significantly more frequent in theCAS group (10.7% vs 4.6%) [23].
EVA-3S
This French multicenter study enrolled 537 patients withsevere symptomatic carotid stenosis (> 60%) to either CASor CEA. Similar to SPACE, it evaluated the hypothesis thatCAS is not inferior to CEA for the treatment of severesymptomatic carotid stenosis. The primary outcome of theincidence of any stroke or death at 30 days was significantlyhigher in the CAS group than in the CEA group (9.6% vs3.9%; relative risk, 2.5; 95% CI, 1.2–5). At 6 months, theincidence of any stroke or death was 6.1% after CEA and11.7% after CAS (P00.02). The trial was stopped prema-turely due to an excess number of deaths in the CAS group[24].
A follow-up showed that the prespecified secondary out-come (periprocedural stroke or death and non-periproceduralipsilateral stroke occurring by 4 years) was significantlyhigher with CAS than with CEA (11.1% vs 6.2%; HR,1.97; 95% CI, 1.06–3.67). This follow-up concluded thatCAS is as effective as CEA for middle-term prevention ofipsilateral stroke. However, in patients with symptomaticcarotid stenosis, CAS needs to be safer before it can be analternative to CEA [25••]. Of note, EPDs in the CAS armwere optional early in the trial, and the 30-day outcome ofany stroke or death was significantly lower in patients treatedwith an EPD than in those treated without the device (7.9%and 25%) [26].
Meta-Analyses
A large meta-analysis included ICSS, EVA-3S, and SPACEdata in comparing CEA to CAS. In the first 120 days afterrandomization, any stroke or death occurred significantlymore often in the CAS group (8.9%) than in the CEA group(5.8%; RR, 1.53; 95% CI, 1.20–1.95; P00.0006). Only agesignificantly modified the treatment effect. Patients youngerthan 70 years old had an estimated 120-day risk of stroke ordeath of 5.8% in the CAS group and 5.7% in the CEAgroup. In patients 70 years of age or older, the estimatedrisk with CAS was twice that with CEA, 12.0% versus5.9%. This analysis concluded that CAS for symptomaticcarotid stenosis should be avoided in older patients(≥70 years of age), but might be as safe as CEA in patientsyounger than 70 years of age [27].
138 Curr Cardiol Rep (2012) 14:135–141

CREST
This RCT is the largest and most comprehensive trial com-paring contemporary CAS to CEA in both symptomatic andasymptomatic patients. The primary composite end pointwas stroke, MI, or death from any cause during the peri-procedural period or any ipsilateral stroke within 4 yearsafter randomization. A total of 2,502 patients were enrolled,of which 47% were asymptomatic. Periprocedural rate ofdeath was 0.7% in the CAS group versus 0.3% in the CEAgroup (P00.18), rate of stroke 4.1% versus 2.3% (P00.01),and rate of MI 1.1% versus 2.3% (P00.03). In addition theincidences of ipsilateral stroke with CAS and CEA weresimilarly low (2.0% vs 2.4%; P00.85). Over 2.5 years, therewas no significant difference in the primary end point be-tween the CAS group and the CEA group (7.2% and 6.8%;HR, 1.1; 95% CI, 0.81–1.51.) The 4-year rate of stroke ordeath was 6.4% with CAS and 4.7% with CEA (HR, 1.50;P00.03); among symptomatic patients the rate was 8.0%with CAS and 6.4% with CEA (HR, 1.37; P00.14), and therate among asymptomatic patients was 4.5% with CAS and2.7% with CEA (HR, 1.86; P00.07) [25••].
The overall effectiveness and safety of the two proce-dures were similar, and the benefits were equal for men andwomen and for patients with asymptomatic and symptom-atic carotid disease. During the periprocedural period, therewas a higher risk of stroke with CAS and a higher risk of MIwith CEA. Of interest, at 1 year after the procedure, qualityof life was significantly diminished for patients who had anystroke, even minor, compared with those patients who hadan MI. For patients age 70 years and older, CEA had lowerrates of the primary end point and less adverse events thanCAS. CAS tended to have greater benefit at younger ages,while CEA tended to have greater benefit at older ages[25••].
A subanalysis on the CREST trial examined the primaryend point in symptomatic versus asymptomatic patients.Upon examining 1,321 symptomatic and 1,181 asymptom-atic patients, the periprocedural composite end point ofstroke, MI, and death did not differ between the CAS andCEA arms (5.2% vs 4.5%; HR, 1.18; 95% CI, 0.82–1.68;P00.38). The stroke and death rate was higher for CASversus CEA (4.4% vs 2.3%; HR, 1.90; 95% CI, 1.21–2.98;P00.005). For symptomatic patients, the periproceduralstroke and death rates were 6.0% for CAS and 3.2% forCEA (HR, 1.89; 95% CI, 1.11–3.21; P00.02). For asymp-tomatic patients, the stroke and death rates were 2.5% forCAS and 1.4% for CEA (HR, 1.88; 95% CI, 0.79–4.42; P00.15). There were no significant differences between CASversus CEA by symptomatic status for the primary endpoint. Periprocedural stroke and death rates were signifi-cantly lower for CEA in symptomatic patients. For both theCAS and CEA arms, the stroke and death rates were below
or comparable to prior RCTs and were within the rangessuggested in current guidelines [28].
Recent Publications
Since the publication of CREST, many meta-analyses havebeen published as well as new guidelines from both theAmerican Heart Association (AHA) and the AmericanStroke Association (ASA).
Recent trials have continued to show that CAS is com-parable to CEA in stroke rates even though the CAS patientshave more comorbidities [29, 30]. The first of these studiesexamined late outcomes in CAS versus CEA. This studylooked at 836 patients in each group with the primaryoutcome of death, MI, or stroke. CAS was comparable toCEA and was better in elderly and symptomatic patients[31]. Examining only the Medicare population, another trialdemonstrated that the in-hospital stroke and mortality rateswere similar between CAS and CEA patients. At 1 year offollow-up, the stroke rates were still similar but all-causemortality was higher in CAS patients, likely because theyhad higher baseline risks [30].
Several large meta-analyses included CREST data andfound similar high rates of MI in patients assigned to CEAand higher risks of stroke with CAS [31, 32]. In the largestand most comprehensive meta-analysis to date, 13 RCTsand 7,477 patients were examined. In the short term, CAShad higher risk of stroke and death while CEA was associ-ated with higher rates of MI and cranial nerve injury. Overthe long term, CAS had significantly higher risks of stroke(OR, 1.27; 95% CI, 1.13–1.65) and death or stroke (OR,1.25; 95% CI, 1.06–1.48). These differences were not sig-nificant in patients younger than 69 years of age. The overalloutcomes of CEA are superior to CAS, but are less sizablein younger patients [32].
A recent article examined the 30-day mortality in olderpatients undergoing CAS looking at the role of operatorexperience. Similar to prior CEA data, experience plays animportant role in outcomes [14, 15]. Patients treated by low-volume operators had an increased risk of 30-day mortalitycompared to patients treated by high-volume operators(adjusted OR, 1.9; 95% CI, 1.4–2.7; P<0.001) [33].
AHA and ASA Guidelines
The most significant publication on carotid stenosis sinceCREST has been the new AHA and ASA guidelines. In1995, prior guidelines had included recommending CEAonly in symptomatic patients in whom morbidity and mor-tality rates are less than 6% and in asymptomatic patientswhen the rate is less than 3% [34]. Guidelines from 2006
Curr Cardiol Rep (2012) 14:135–141 139

have stated that CAS is a reasonable strategy for selectpatients when performed by operators with established peri-procedural morbidity and mortality rates of 4% to 6% [35].In the 2011 guidelines, CEA is recommended for symptom-atic patients with moderate (50% to 69%) and severe (70%to 99%) disease, but only if the perioperative morbidity andmortality risk is estimated to be less than 6%. There is noindication for revascularization in patients with less than50% stenosis [36•].
CAS is indicated as an alternative to CEA for symptomaticpatients at average or low risk of complications associatedwith endovascular intervention when the diameter of thelumen of the internal carotid artery is reduced by more than70% by noninvasive imaging or more than 50% by catheterangiography. CAS may be considered among patients withsymptomatic severe stenosis (> 70%) in whom the stenosis isdifficult to access surgically, medical conditions are presentthat greatly increase surgical risk, or when other specificcircumstances exist, such as radiation-induced stenosis orrestenosis after CEA. In the above settings, CAS is onlyreasonable when performed by operators with establishedperiprocedural morbidity and mortality rates of 4% to 6%[36•].
A collaboration of organizations also released guidelinesin 2011 for CEA and CAS in carotid artery stenosis. Similarto the AHA/ASA recommendations, elderly (age 70 yearsand older) symptomatic patients with 70% to 99% stenosisare recommended to have CEA instead of CAS as theperioperative risk of stroke or death for these patients isapproximately twofold higher with CAS compared withCEA. For these patients, CAS is recommended if the lesionis not suitable for surgical access, there is radiation-inducedstenosis, or the patient has clinically significant cardiac,pulmonary, or other disease that increases the risk of anes-thesia and surgery [37].
To summarize the multiple sets of guidelines, CAS andCEA provide similar long-term outcomes for both symp-tomatic and asymptomatic patients. However, CAS isassociated with a higher periprocedural risk of strokeand death. CEA continues to be recommended overCAS for symptomatic patients with 60% to 99% stenosis[38, 39]. However, there is a much weaker benefit forasymptomatic patients and CEA in these patients shouldbe considered a long-term investment as the benefit onlybegins after 2 years [37, 38]. CAS should not be consid-ered for asymptomatic patients unless the center has aless than 3% risk for combined stroke and death. Finally,CAS is recommended over CEA in symptomatic patientswith severe disease if the carotid lesion is not suitable forsurgical access, is from radiation-induced stenosis orrestenosis after CEA, or if the patient has significantdisease placing them at an unacceptably high surgical risk[36•, 37].
Conclusions
The CREST trial was one of the largest randomized trialscomparing CAS to CEA and established the comparativesafety and efficacy of the two revascularization strategies.This trial has influenced guideline changes and has beenfollowed by large outcome studies that have highlighted therole of operator experience. With all of this new informa-tion, CEA remains first-line treatment as it has better peri-procedural outcomes specifically in terms of preventingstroke and death. Whereas CEA has a higher periproceduralMI rate, strokes have been shown to be more debilitatingafter 1 year than MIs. And although CEA remains thetreatment option of choice, CAS does offer benefits forpatients younger than 70 years of age. CAS is less invasivethen CEA and has a place in patients who are too high riskto undergo CEA. In addition, further refinements in tech-nology will enhance its safety and make it an increasinglyappealing treatment option for carotid artery stenosis.
Disclosure No potential conflicts of interest relevant to this articlewere reported.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. Fisher, Miller C. AMA Arch Neurol Psychiat. 1951;65:346.2. HollanderM, BotsML, Del Sol AI, et al. Carotid plaques increase the
risk of stroke and subtypes of cerebral infarction in asymptomaticelderly: the Rotterdam study. Circulation. 2002;105:2872.
3. Störk S, Van Den Beld AW, Von Schacky C, et al. Carotid arteryplaque burden, stiffness, and mortality risk in elderly men: aprospective, population-based cohort study. Circulation.2004;110:344.
4. Van der Vaart MG, Meerwaldt R, Reijnen MM, Tio RA, ZeebregtsCJ. Endarterectomy or carotid artery stenting: the quest continues.Am J Surg. 2008;195:259.
5. Chambers BR, Donnan GA. Carotid endarterectomy for asymp-tomatic carotid stenosis. Cochrane database. Syst Rev. 2005.
6. Hobson 2nd RW, Weiss DG, Fields WS, et al. Efficacy of carotidendarterectomy for asymptomatic carotid stenosis. The veteransaffairs cooperative study group. N Engl J Med. 1993;328:221.
7. Executive Committee for the Asymptomatic Carotid AtherosclerosisStudy. Endarterectomy for asymptomatic carotid artery stenosis.JAMA. 1995;273:1421.
8. Halliday A, Mansfield A, Marro J, et al. Prevention of disablingand fatal strokes by successful carotid endarterectomy in patientswithout recent neurological symptoms: randomised controlled trial.Lancet. 2004;363:1491.
9. Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarter-ectomy in patients with symptomatic moderate or severe stenosis.North American symptomatic carotid endarterectomy trial collabora-tors. N Engl J Med. 1998;33:1415.
140 Curr Cardiol Rep (2012) 14:135–141

10. North American Symptomatic Carotid Endarterectomy Trial Col-laborators. Beneficial effect of carotid endarterectomy in symp-tomatic patients with high-grade carotid stenosis. N Engl J Med.1991;325:445.
11. European Carotid Surgery Trialists’ Collaborative Group. MRCEuropean carotid surgery trial: interim results for symptomaticpatients with severe (70–99%) or with mild (0–29%) carotid stenosis.Lancet. 1991;337:1235.
12. Wennberg DE, Lucas FL, Birkmeyer JD, et al. Variation in carotidendarterectomy mortality in the Medicare population: trial hospitals,volume, and patient characteristics. JAMA. 1998;279:1278.
13. O’Neill L, Lanska DJ, Hartz A. Surgeon characteristics associatedwith mortality and morbidity following carotid endarterectomy.Neurology. 2000;55:773.
14. Ederle J, Featherstone RL, BrownMM. Randomized controlled trialscomparing endarterectomy and endovascular treatment for carotidartery stenosis: a Cochrane systematic review. Stroke. 2009;40:1373.
15. Yadav JS, Wholey MH, Kuntz RE, et al. Protected carotid-arterystenting versus endarterectomy in high-risk patients. N Engl JMed. 2004;351:1493.
16. Gurm HS, Yadav JS, Fayad P, et al. Long- term results of carotidstenting versus endarterectomy in high-risk patients. N Engl JMed. 2008;358:1572.
17. Brooks WH, McClure RR, Jones MR, et al. Carotid angioplastyand stenting versus carotid endarterectomy: randomized trial in acommunity hospital. J Am Coll Cardiol. 2001;38:1589.
18. Brown MM, Rogers J, Bland JM, et al. CAVATAS investigators.Endovascular versus surgical treatment in patients with carotid ste-nosis in the Carotid and Vertebral Artery Transluminal AngioplastyStudy (CAVATAS): a randomized trial. Lancet. 2001;357:1729.
19. Ederle J, Bonati LH, Dobson J, et al. Endovascular treatment withangioplasty or stenting versus endarterectomy in patients withcarotid artery stenosis in the Carotid and Vertebral Artery Trans-luminal Angioplasty Study (CAVATAS): longterm follow-up of arandomized trial. Lancet Neurol. 2009;8:898.
20. Bonati LH, Ederle J, McCabe DL, et al. Long-term risk of carotidrestenosis in patients randomly assigned to endovascular treatment orendarterectomy in the Carotid and Vertebral Artery TransluminalAngioplasty Study (CAVATAS): long-term follow-up of a randomizedtrial. Lancet Neurol. 2009;9:908.
21. Ederle J, Dobson J, Featherstone RL, et al. Carotid artery stentingcompared with endarterectomy in patients with symptomatic ca-rotid stenosis (International Carotid Stenting Study): an interimanalysis of a randomised controlled trial. Lancet. 2010;375:985.
22. Ringleb PA, Allenberg J, Brückmann H, et al. 30 day results fromthe SPACE trial of stent-protected angioplasty versus carotid end-arterectomy in symptomatic patients: a randomised non-inferioritytrial. Lancet. 2006;368:1239.
23. Eckstein HH, Ringleb P, Allenberg JR, et al. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE)study to treat symptomatic stenoses at 2 years: a multinational,prospective, randomised trial. Lancet Neurol. 2008;7:893.
24. Mas JL, Chatellier G, Beyssen B, et al. Endarterectomy versusstenting in patients with symptomatic severe carotid stenosis. NEngl J Med. 2006;355:1660.
25. •• Brott TG, Hobson RW 2nd, Howard G, et al.: Stenting versusendarterectomy for treatment of carotid-artery stenosis. N Engl JMed 2010, 363(1):11–23. This was the largest RCT comparingCEA to carotid artery stenosis.
26. Mas JL, Trinquart L, Leys D, et al. Endarterectomy Versus Angio-plasty in Patients with Symptomatic Severe Carotid Stenosis (EVA-3S) trial: results up to 4 years from a randomised, multicentre trial.Lancet Neurol. 2008;7:885.
27. Bonati LH, Dobson J, Algra A, et al. Short-term outcome afterstenting versus endarterectomy for symptomatic carotid stenosis: apreplanned meta-analysis of individual patient data. Lancet.2010;376:1062.
28. Silver FL, Mackey A, Clark WM, et al. Safety of stenting andendarterectomy by symptomatic status in the carotid Revasculari-zation Endarterectomy Versus Stenting Trial (CREST). Stroke.2011;42:675.
29. Bangalore S, Bhatt DL, Rother L, et al. Late outcomes after carotidartery stenting versus carotid endarterectomy: insights from apropensity-matched analysis of the Reduction of Atherthrombosisfor Continued health (REACH) Registry. Circulation. 2010;122:1092.
30. Wang FW, Esterbrooks D, Kuo YF, et al. Outcomes after carotidartery stenting and endarterectomy in the Medicare population.Stroke. 2019;2011:42.
31. Bangalore S, Kumar S, Wetterskev J, et al. Carotid artery stentingvs carotid endarterectomy. Arch Neurol. 2011;68:172.
32. Economopoulos KP, Sergentanis TN, Tsuvgoulis G, et al. Carotidartery stenting versus carotid endarterectomy: a comprehensivemeta-analysis of short-term and long-term outcomes. Stroke.2011;42:687.
33. Nallamothu BK, Gurm HS, Ting HH, et al. Operator experienceand carotid stenting outcomes in medicare beneficiaries. JAMA.2011;306:1338.
34. Moore WS, Barnett HJ, Beebe HG, et al. Guidelines for carotidendarterectomy. A multidisciplinary consensus statement from theAd Hoc committee, American heart association. Circulation.1995;91:566.
35. Sacco RL, Adams R, Albers G, et al. Guidelines for prevention ofstroke in patients with ischemic stroke or transient ischemic attack:a statement for healthcare professionals from the American heartassociation/American stroke association council on stroke: co-sponsored by the council on cardiovascular radiology and inter-vention: the American academy of neurology affirms the value ofthis guideline. Stroke. 2006;37:577.
36. • Furie KL, Kasner SE, Adams RJ, et al.: Guidelines for the preven-tion of stroke in patients with stroke or transient ischemic attack: aguideline for healthcare professionals from the American HeartAssociation/American Stroke Association. American Heart Associa-tion Stroke Council, Council on Cardiovascular Nursing, Council onClinical Cardiology, and Interdisciplinary Council on Quality of Careand Outcomes Research. Stroke 2011, 42:227. These were the firstguidelines published after results of the CREST trial.
37. Brott TG, Halperin JL, Abbara S, et al. 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With ExtracranialCarotid and Vertebral Artery Disease: A Report of the AmericanCollege of Cardiology Foundation/American Heart AssociationTask Force on Practice Guidelines, and the American Stroke As-sociation, American Association of Neuroscience Nurses, Ameri-can Association of Neurological Surgeons, American College ofRadiology, American Society of Neuroradiology, Congress ofNeurological Surgeons, Society of Atherosclerosis Imaging andPrevention, Society for Cardiovascular Angiography and Interven-tions, Society of Interventional Radiology, Society of NeuroInter-ventional Surgery, Society for Vascular Medicine, and Society forVascular Surgery. Circulation. 2011;124:489.
38. National Institute for Health and Clinical Excellence; Carotidartery stent placement for asymptomatic extracranial carotid stenosis.April 2011.
39. National Institute for Health and Clinical Excellence; Carotidartery stent placement for symptomatic extracranial carotid stenosis.April 2011.
Curr Cardiol Rep (2012) 14:135–141 141