Embed Size (px)
Citation preview

JOSEPH GLENMULLEN, MD 1770 M assachusetts A venue, No. 263
C am bridge, M A 02140
Septem ber 22, 2014
Mr. M atthew Leckm an Pogus Braslow & M illrood 8 Tow er Bridge, Suite 1520 161 W ashington Street Conshohocken, PA 19428
D ear Mr. Leckman:
It is m y opinion, based on a reasonable degree of m edical certainty and based on m y education, train ing , and clinical experience, as w ell as m y review of the m aterial referenced in this rep o rt and listed in the attached appendices, th a t evidence from m ultip le sources p roves stopp ing C ym balta causes w ithd raw al reactions in a h igh percentage of patien ts and tha t C ym balta w ithd raw al can be severe, debilitating, and even life-threatening. Four d ifferent types of scientific evidence su p p o rt th is conclusion: Lilly 's double-blind, placebo-controlled, random ized C ym balta studies; da ta from w orld-w ide post-m arketing surveillance; published , peer-rev iew ed scientific studies of an tidepressan t w ithdraw al; and C ym balta 's m echanism of action.
In Lilly's studies, 40% to 50% of depressed patien ts stopp ing C ym balta reported w ithd raw al side effects, and u p to 17% w ere severe. In Lilly's short-term (eight to n ine w eek) studies, s topp ing C ym balta m ore th an doubled the risk of w ithd raw al side effects by com parison w ith s topp ing placebo: the o dds ratio w as 2.68. In the com pany 's longer-term (34-week) studies, s topp ing C ym balta again m ore th an doubled the risk of w ithd raw al sym ptom s: the odds ratio w as 4.95.The risk of specific w ithd raw al sy m p to m s—nausea, dizziness, abnorm al sensations, irritability, n ightm ares, headaches, and v o m itin g —w as elevated as m uch as 23-fold. All of these e levated risks w ere statistically significant, m aking them strong scientific evidence stopp ing C ym balta causes w ithd raw al reactions th a t can be severe in a h igh percentage of patients. A s tudy of the FD A 's postm arketing adverse event database found reports of C ym balta w ithdraw al ou tnum bered reports of w ithd raw al for all o ther d rugs including narcotics and V alium -type antianxiety agents and sleeping pills, p rov id ing confirm atory evidence C ym balta causes w ithd raw al reactions in a h igh percentage of patients.
1
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 21 of 246 PageID# 8251

Published scientific studies have established th a t the frequency of an tidepressan t w ithd raw al reactions directly correlates w ith a d ru g 's half-life, a m easure of how quickly it w ashes ou t of the body w hen stopped. W ithdraw al sym ptom s are evidence of abnorm al b ra in cell functioning in response to w ithd raw al of an an tidepressan t w hen there is n o t enough tim e for the b ra in cells to adapt. Lilly's pharm acodynam ic studies found C ym balta has an extrem ely short half-life, about 12 hours, exiting the body precipitously. C ym balta 's precip itous d rop explains w hy it is one of the w orst offenders w hen it comes to an tidepressan t w ithdraw al. Patients w ho inadverten tly m iss just one dose can experience C ym balta w ithdraw al. Severe an tidepressan t w ithd raw al can be incapacitating, require hospitalization, and be life-threatening. Even w ith a slow taper, patien ts can experience severe w ithd raw al reactions. S topping C ym balta can be so difficult it takes seven m onths or m ore.
Since C ym balta 's in troduction in 2004, in every version of the d ru g 's label, Lilly has m isrepresen ted or failed to adequately inform doctors and patien ts about the frequency, severity, and du ra tio n of C ym balta w ithd raw al reactions. Lilly 's m isleading inform ation m ake it im possible for any patien t or physician to m ake an inform ed decision about the app ropria teness of taking or prescrib ing Cym balta.
Q ualifications
A gradua te of H arvard M edical School, I am a Clinical Instructor in Psychiatry at H arv ard M edical School, w as a staff psychiatrist at the H arv ard Law School H ealth Services for tw en ty years, and have a p rivate practice in H arv ard Square. I am Board Certified in psychiatry by the A m erican Board of Psychiatry and N eurology.
I am the au tho r of tw o books on the side effects of psychiatric m edications: P r o z a c
B a c k la sh : O v e r c o m in g th e D a n g e r s o f P r o z a c , Z o lo f t , P a x i l , a n d O th e r A n t id e p r e s s a n t s w i th
S a fe , E f fe c t iv e A l t e r n a t i v e s pub lished in 2000 by Sim on & Schuster and T h e A n t i d e p r e s s a n t
S o lu t io n : A S t e p - b y - S t e p G u id e to O v e r c o m in g A n t i d e p r e s s a n t W i th d r a w a l , D e p e n d e n c e , a n d
"A d d ic t i o n " pub lished by Sim on & Schuster's Free Press d ivision in January 2005.1
P r o z a c B a c k la sh includes a chapter on an tidepressan t w ithd raw al an d is anno tated w ith over 600 footnotes from m edical journals, books, and o ther sources. T h e A n t i d e p r e s s a n t
S o lu t io n is devo ted to an tidepressan t w ithd raw al and anno tated w ith over 350 footnotes. In the title P r o z a c B a c k la sh , I use the w o rd "Prozac" generically to refer to the g roup of an tidepressan ts know n as SSRIs (selective sero tonin reup take inhibitors).
2
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 22 of 246 PageID# 8252

Prozac w as the first of the new er an tidepressan ts in troduced in th is country in the 1990s and is the best know n. C ym balta is a closely-related SNRI (selective sero tonin and norep inephrine reup take inhibitor).
I am a m oderate in the debate over the risks and benefits of an tidepressants. I prescribe the m edications for patien ts w hose conditions are serious enough to w arran t them and have h ad num erous patien ts rep o rt their beneficial effects. But, I am a critic of the d rugs being over-prescribed for m ild conditions and of doctors and patien ts n o t being adequately w arn ed of their side effects. I testified at the FDA's February 2004 and D ecem ber 2006 hearings on an tidepressan t-induced suicidality.
I have becom e a national spokesperson for the appropria te , m easured use of psychiatric m edications. I have been in terv iew ed on num ero u s national television an d radio show s including NBC's The Today Show, ABC N ew s’ 20/20, ABC's G ood M orning Am erica, A B C s W orld N ew s Tonight, ABC's P rim etim e Live, CN N, Fox N ew s, PBS, C ourt TV, and N ational Public Radio for m y expertise on antidepressants. M y w ork has been the subject of m any review s and articles includ ing in the N e w Y o r k T im e s and T h e N e w
Y o r k e r m agazine.2 A m ong the honors I have received for w riting P r o z a c B a c k la sh is the A m erican College for A dvancem ent in M edicine's (ACAM's) A nnual A chievem ent A w ard in M edicine in M ay 2001.1 received the aw ard at ACAM 's 2001 annual convention and delivered the convention 's keynote address, the Linus Pauling Lecture. M y c u r r i c u lu m v i ta e is enclosed w ith this rep o rt as Exhibit 1.
M aterials R eview ed for th is R eport
In p reparing this general causation report, I have d raw n on m y extensive know ledge of an tidepressan t w ithd raw al based on m y education, training, and experience. I have researched the m edical literature on an tidepressan t w ithd raw al sym ptom s. As detailed in m y books, I have trea ted num erous patien ts suffering from an tidepressan t w ithdraw al. In addition , a ttached hereto as Exhibit 2 is a list of Lilly and other docum ents I rev iew ed or considered in form ing m y opinions and /o r w hich relate to m y opinions. D iscovery in th is case is ongoing. M y u n d ers tan d in g is th a t Lilly has no t yet p roduced a num b er of docum ents I in tend to review . For exam ple, all of the Lilly C ym balta stud ies d iscussed in th is rep o rt w ere studies of patien ts w ith m ajor depressive d isorders. Lilly subsequen tly obtained FDA approval for C ym balta for add itional indications including generalized anxiety d iso rder (GAD), diabetic periphera l neuropa thy , fibrom yalgia, and chronic m usculoskeletal pa in .3 Lilly 's studies of these conditions are the subject of ongoing discovery. I anticipate supplem enting this rep o rt once additional docum ents becom e available.
3
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 23 of 246 PageID# 8253

For m y tim e doing telephone conferences, research, review ing docum ents, and w riting th is report, I am com pensated at the rate of $650 per hour. For travel and testim ony, I am reim bursed at the rate of $650 p er hour, w ith 10 hou rs fee for a full day and 5 hours fee for a half day. In the last four years, I have given testim ony in the follow ing cases: State of Texas ex rel. A llen Jones v Janssen on January 31, 2011, M arch 22, 2011, D ecem ber 1, 2011, and January 18, 2012; C allahan v Jellinek on June 13, 2011; B arth v N etolicky on July 20, 2011; In re Chantix (varenicline) P roducts Liability L itigation on A pril 4, 2012, A pril 5, 2012, June 26, 2012, and D ecem ber 13, 2012; Berry v K inast on January 22, 2013; B row n v Forest Labs et al on M arch 11, 2013 and M ay 14, 2013; H enry v K ahnert on July 10, 2013; Elm ore v Janssen on A ugust 12, 2013; Teters v Bristol-M yers Squibb on O ctober 25, 2013; D elahoussaye v Concepcion on N ovem ber 22, 2013; A m edia v U nited States of A m erica on A pril 15, 2014; and M uzichuck v Forest Labs on July 1, 2014.
This rep o rt is d iv ided in to eight parts:
• Section 1 discusses the evidence in Lilly 's p re -approval studies tha t stopp ing C ym balta causes w ithd raw al sym ptom s th a t can be severe.
• Section 2 discusses the FD A 's post-approval adverse event reports (AERs) of C ym balta causing w ithd raw al sym ptom s th a t can be severe.
• Section 3 review s the evidence in pub lished scientific stud ies of an tidepressan t w ithdraw al.
• Section 4 discusses the biological m echanism of C ym balta w ithdraw al.• Section 5 is a B radford Hill causality assessm ent of C ym balta 's w ithdraw al
effects.• Section 6 explains w hy Lilly 's label is inadequate and m isleading w ith
regard to C ym balta w ithdraw al.• Section 7 discusses Lilly 's conduct.
4
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 24 of 246 PageID# 8254

S ection 1: L illy 's C y m b a lta S tu d ie s
In Lilly's placebo-controlled studies of depressed patients, s topp ing C ym balta m ore th an doub led the risk of an tidepressan t w ithd raw al reactions by com parison w ith stopp ing placebo. The increased risk w as statistically significant.
T h e G o ld S ta n d a r d f o r E f f ic a c y
The FDA requires pharm aceutical com panies to conduct w ell-controlled, double-blind, random ized stud ies to dem onstrate a new d ru g 's efficacy for its p roposed use. "C ontrolled" m eans the studies com pare a g roup of patien ts receiving the test d ru g to a g roup receiving placebo (inactive) pills and /o r a g roup receiving an established com parator d ru g already on the m arket. The FDA prefers placebo-controlled studies w hen feasible. "D ouble-blind" m eans the patien ts all receive identical pills and neither the patien ts no r the researchers are supposed to know w ho is receiving the test d ru g versus placebo. "R andom ized" m eans a pool of sim ilar patien ts are random ly assigned to the different trea tm en t groups. These features are in tended to rem ove potential bias in the studies. Pharm aceutical com pany studies th a t m eet these requ irem ents are called R andom ized Clinical Trials, or RCT.
R andom ized clinical trials are prospectively designed to have enough statistical pow er,i.e. a large enough sam ple size (enough patients), to detect differences in efficacybetw een the trea tm en t groups. In addition, the studies are requ ired to assess the d ru g 'seffectiveness using valida ted m easurem ent scales. To m easure C ym balta 's efficacy,Lilly evaluated patien ts w eekly du rin g trea tm en t w ith C ym balta or placebo to assessw hether or no t their condition im proved, using detailed sym ptom checklist ratingscales including the 17-item H am ilton D epression R ating Scale (HAM D 17),M ontgom ery A sberg D epression R ating Scale (MADRS), Clinical Global Im pressions ofIm provem ent scale (CG I-Im provem ent), Patien t's Global Im pressions of Im provem entscale (PG I-Im provem ent), H am ilton A nxiety R ating Scale (HAMA), and the quality oflife 36-item Short Form H ealth Survey (SF-36).4
W hen the studies of a new d ru g are com pleted, the resu lts are analyzed statistically. In o rder for a new d ru g to be deem ed efficacious, it no t only has to outperform placebo, the difference m ust be statistically significant, show ing th a t the difference w as unlikely to have occurred by chance. W ell-designed placebo-controlled studies are w idely regarded as the gold s tan d ard for establishing a d ru g 's efficacy. M y evaluation of C ym balta 's efficacy in Lilly's studies —an im p o rtan t p a rt of a risks benefits analysis —is n o t com plete since I am aw aiting docum ents th a t are the subject of ongoing discovery.
5
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 25 of 246 PageID# 8255

L im i ta t io n s f o r A s s e s s i n g S id e E ffe c ts
R andom ized clinical trials, w hile the gold s tan d ard for assessing efficacy, often have substantial w eaknesses for assessing side effects. The studies m ay n o t be able to detect in frequen t side effects, because they are no t pow ered (i.e. they do n o t have enough patients) to detect differences betw een the d ru g versus placebo. W hile the d ru g 's efficacy can be assessed in all the patients, an in frequen t side effect m ay occur in just a few and the difference betw een the d ru g and placebo m ay n o t be apparen t.
The problem can be com pounded by the m ethods u sed to assess side effects. In m any pharm aceutical com pany studies, detailed ra ting scales are n o t u sed to system atically assess potential side effects.5 Instead, side effects are only recorded if patien ts recognize and vo lun teer them .6 This unsystem atic approach is called "non-probing" because the patien ts are no t specifically asked about side effects and "spontaneous" because the patien ts m ust spon taneously vo lun teer them . Such spontaneous reporting is well- know n to resu lt in significant un d errep o rtin g of side effects.7
Lilly 's C ym balta stud ies suffered from this shortcom ing. W hile Lilly rigorously m onito red efficacy in its C ym balta studies, w ithd raw al side effects w ere no t system atically m onito red w ith ra ting scales w hen patien ts stopped the d rug . Instead, according to Lilly w ithd raw al side effects w ere only assessed in a "nonprob ing" m anner "by m eans of spon taneous reports ra ther th an a [w ithdraw al] sym ptom checklist."8 In o ther w ords, w ithd raw al side effects w ere recorded only if the researcher recognized the patien t w as hav ing a side effect or if the patien t recognized a side effect as such and considered it significant enough to volunteer. L illy-funded researchers h ad prev iously developed rating scales for system atically m onitoring an tidepressan t w ithd raw al side effects.9 Indeed, the ra ting scales w ere u sed in earlier L illy-funded research on Prozac, w hich causes low er rates of w ithdraw al reactions th an m any other an tidepressan ts.10 But Lilly d id no t use the ra ting scales in its C ym balta stud ies.11 C ym balta has an extrem ely short half-life, m eaning it w ashes o u t of the body precip itously w hen the d ru g is s to p p ed .12 Therefore, C ym balta w ou ld be expected to cause an tidepressan t w ithd raw al sym ptom s in a h igh percentage of pa tien ts.13 Lilly has acknow ledged th a t the com pany 's no t system atically m onitoring C ym balta side effects w as one of the "m ain lim itations" of its stud ies.14 System atically m onito ring w ithd raw al side effects w ith a sym ptom checklist ra ting scale w ou ld be expected to detect h igher rates of C ym balta w ithd raw al.15
W hen pharm aceutical com pany stud ies are com pleted, statistical analyses can be conducted to com pare the num ber and rate of side effects in patien ts w ho received the
6
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 26 of 246 PageID# 8256

d ru g versus placebo. W hen despite the stud ies ' lim itations, a d ru g statistically significantly increases the risk of a side effect, the findings are particu larly com pelling.16 Indeed, the FDA has stated th a t statistically significant findings establish a d ru g causes side effects.17 A t a July 10, 2008 FDA hearing on m edication-induced psychiatric side effects, the FD A 's Dr. Russell Katz, the d irector of the agency 's D ivision of N europharm acological D rugs, explained:18
This is how w e determ ine causality ....If it's statistically significantly d ifferent from placebo, w e say the d ru g caused i t . .. .1 th ink in controlled trials, yo u see a signal, [if] it is statistically significantly d ifferent from placebo, tha t is operationally defined as causality.
In add ition to statistically significant findings, there are o ther w idely u sed m easures for assessing causality including the B radford H ill criteria d iscussed below .
W h a t L i l l y 's S h o r t - T e r m , P la c e b o -C o n tr o l le d
C y m b a l ta S tu d ie s F o u n d
D espite their lim itations, Lilly 's random ized , double-blind, placebo-controlled studies of depressed patien ts dem onstrated th a t C ym balta m ore th an doub led the risk of w ithd raw al reactions w hen the d ru g w as s topped .19 The elevated risk w as statistically significant.20 To w in FDA approval for Cym balta, Lilly conducted a num b er of shortterm (eight to n ine w eek) stud ies of patien ts w ith m ajor depressive d iso rder (MDD), com paring trea tm en t w ith C ym balta to trea tm en t w ith placebo. In Table 1, w hich rep roduces a table from a Lilly article pub lished in 2005 in the J o u r n a l o f A f f e c t i v e
D is o r d e r s , the first six studies are short-term , placebo-controlled studies.21 A to tal of 870 patien ts partic ipa ted in the six studies; 490 received C ym balta w hile 380 received placebo.
7
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 27 of 246 PageID# 8257

Table 1Sum m ary of Lilly 's M DD C ym balta Studies
T able 1S u m m ary o f c lin ica l tria ls
S tudy S tu d y d e sig n T rea tm e n ts (Al) W eek s o f trea tm en t
1 P a ra lle l, d o u b le -b lin d , p la c e b o -c o n tro lle d ,
ra n d o m iz e d , f lu o x e tin e -c o n tro l le dP la c e b o (7 0 )D u lo x e tin e 2 0 - 6 0 m g B 1D ‘ (7 0 ) F lu o x e tin e 2 0 m g Q D (3 3 )
T o ta l (1 7 3 )
8
2 P a ra lle l, d o u b le -b lin d , p la c e b o -c o n tro lle d , ra n d o m iz e d , f lu o x e tin e -c o n tro l le d
P la c e b o (7 5 )D u lo x e tin e 2 0 - 6 0 m g B ID " (8 2 ) F lu o x e tin e 2 0 m g Q D (3 7 )T otal (1 9 4 )
8
3 P a ra lle l, d o u b le -b lin d , p la c e b o -c o n tro lle d , ran d o m ized
P la c e b o (1 2 2 )D u lo x e tin e 6 0 m g Q D (1 2 3 ) T o tal (2 4 5 )
9
4 P a ra lle l, d o u b le -b lin d , p la c c b o -c o n tro lle d , ra n d o m iz e d
P la c e b o (1 3 9 )D u lo x e tin e 6 0 m g Q D (1 2 8 ) T o ta l (2 6 7 )
9
5 P a ra lle l, d o u b le -b lin d , p la c e b o -c o n tro lle d , ra n d o m iz e d , p a ro x e tin e -c o n tro lle d
P la c e b o (9 0 )D u lo x e tin e 2 0 m g B ID (9 1 ) D u lo x e tin e 4 0 m g B ID (8 4 ) P a ro x e tin e 2 0 m g Q D (8 9 ) T o ta l (3 5 4 )
8
6 P ara lle l, d o u b le -b lin d , p la c e b o -c o n tro lle d , ra n d o m iz e d , p a ro x e tin e -c o n tro lle d
P la c e b o (8 9 )D u lo x e tin e 2 0 m g B ID (8 6 ) D u lo x e tin e 4 0 m g B ID (91 ) P a ro x e tin e 2 0 m g Q D (8 7 ) T o tal (3 5 3 )
8
7 P a ra lle l, d o u b le -b lin d , p la c e b o -c o n tro lle d , ra n d o m iz e d , p a ro x e tin e -c o n tro lle d
P la c e b o (9 3 )
D u to x c lin c 4 0 m g B ID (9 3 ) D u lo x e tin e 6 0 m g B ID (9 5 ) P a ro x e tin e 2 0 m g Q D (8 6 ) T o tal (3 6 7 )
8 ; + 2 6 -w c c k e x te n sio n p h a se
8 P a ra lle l, d o u b le -b lin d , p la c e b o -c o n tro lle d , ra n d o m iz e d , p a ro x e tin e -c o n tro lle d
P la c e b o (99 )
D u lo x e tin e 4 0 m g B ID (9 3 ) D u lo x e tin e 6 0 m g B ID (1 0 3 ) P a ro x e tin e 2 0 m g Q D (9 7 ) T o tal (3 9 2 )
8 ; + 2 6 -w e e k ex te n sio n p h a se
9 O p e n -la b e l D u lo x e tin e 4 0 - 6 0 m g B ID (1 2 7 9 ) 52
In all th e se s tu d ie s , th e o b s e rv a tio n p e r io d fo r D E A E s is 2 w e ek s ; B I D - tw ic e d a ily ; Q D - o n c e da ily . * F o rced titra tio n to 120 rn g /day .
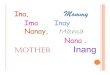
As seen in Table 1, som e of the six short-term studies also h ad active com parators, including Prozac (fluoxetine) and Paxil (paroxetine). A t the end of the eight to n ine w eek studies, pa tien ts ' active d rugs (Cym balta, Prozac, or Paxil) w ere stopped w ith double-blind placebo substitu tion for one to tw o add itional w eeks in w h a t Lilly called a "placebo lead-out" phase, also know n as a placebo w ash-ou t phase.22 The placebo group sim ply continued on placebo du rin g this post-active trea tm en t phase. Table 2 rep roduces ano ther Lilly table, listing the m ost com m on w ithd raw al side effects repo rted by at least 2% of patien ts w hose C ym balta w as s topped .23 In Table 2, "d iscontinuation-em ergent adverse effects" is Lilly's te rm for sym ptom s of an tidepressan t w ithdraw al.
8
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 28 of 246 PageID# 8258

Table 2A ntidepressan t W ithdraw al Side
Effects in Lilly 's C ym balta S tudies
Table 2Discontinuation-emergent adverse events after acute treatment reported by at least 2% o f duloxetine-treated patients who entered the lead-out phase o f studies 1, 2, 3, 4, 5 and 6_________________
Event Placebo(/V=380; n (%))
Duloxetine (N = 490 ; n (%))
Patients with > 1 event 87 (22.9) 217 (44.3)*Dizziness 3 (0.8) 61 (12.4)*Nausea 1 (0.3) 29 (5.9)*Headache NOS 3 (0.8) 26 (5.3)*Paraesthesia 1 (0.3) 14 (2.9)*Diarrhea NOS 3 (0.8) 11 (2.2)Vomiting NOS 2 (0.5) 12 (2.4)*Irritability 1 (0.3) 12 (2.4)*Insomnia 2 (0.5) 10 (2.0)Nightmare 0 (0.0) 10 (2.0)*
NOS = not otherwise specified.* /><0.05 vs. placebo, F isher’s Exact Test.
As seen in Table 2, in Lilly's stud ies C ym balta w ithdraw al reactions w ere com m on: 44% of patien ts stopp ing the d ru g experienced one or m ore characteristic sym ptom s of an tidepressan t w ithdraw al. Since Lilly d id no t system atically assess C ym balta w ithd raw al side effects in the studies, system atic m onitoring w ould be expected to detect even h igher rates.24
The m ost com m on w ithdraw al sym ptom s w ere dizziness, nausea, headaches, paraesthesias (abnorm al sensations such as electric shock-like sensations in the brain), d iarrhea, vom iting, irritability, and nightm ares, all classic sym ptom s of an tidepressan t w ithdraw al. M any of the w ithd raw al sym ptom s w ere reported w ith in a day of stopping C ym balta.25
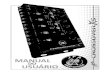
Table 3 analyzes Lilly's C ym balta da ta in Table 2, p rov id ing the odds ratios, confidence intervals, and p-values for the risk of patien ts experiencing w ithd raw al sym ptom s w hen stopp ing C ym balta versus placebo.26
9
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 29 of 246 PageID# 8259

Table 3Statistical Significance Calculations
Based on Lilly's D ata in Table 2WithdrawalSymptoms
PlaceboN=380
CymbaltaN=490
OR p-Value Cl
Patients with >1 symptom
87 (22.9%) 217 (44.3%) 2.68 <0.001 1.98 - 3.65
Dizziness 3 (0.8%) 61 (12.4%) 17.87 <0.001 5.74-89.59Nausea 1 (0.3%) 29 (5.9%) 23.84 <0.001 3.91 - 976.20Headache NOS 3 (0.8%) 26 (5.3%) 7.04 <0.001 2.13-36.57Paraesthia 1 (0.3%) 14 (2.9%) 11.15 0.004 1.68 - 472.60Vomiting NOS 2 (0.5%) 12 (2.4%) 4.75 0.041 1.05 - 43.84Irritability 1 (0.3%) 12 (2.4%) 9.51 0.012 1.39 - 406.7Nightmares 0 (0.0%) 10 (2.0%) 8.71 0.020 1.25-376.00
As seen in Table 3, s topp ing C ym balta m ore th an doub led the risk of w ithdraw al sym ptom s by com parison w ith stopp ing placebo: the odds ratio w as 2.68.27 The increased risk w as statistically significant: the p-value w as less th an 0.001.28 The risk of ind iv idual w ithd raw al sym ptom s w as elevated even m ore: By com parison w ith stopp ing placebo, stopp ing C ym balta statistically significantly e levated the risk of nausea 23-fold, d izziness 17-fold, paraesth ias 11-fold, irritability 9-fold, n igh tm ares 8fold, headaches 7-fold, and vom iting 4-fold.
These statistically significant findings in Lilly 's short-term , placebo-controlled, random ized stud ies of depressed patien ts constitute strong scientific evidence tha t stopp ing C ym balta causes w ithd raw al reactions in a h igh percentage of patients. The findings for m ultip le, classic sym ptom s of an tidepressan t w ithd raw al p rov ide evidence of a b road range of C ym balta w ithd raw al reactions.
C o n f i r m a to r y E v id e n c e f r o m L i l l y 's
3 4 - W e e k S tu d ie s
The findings in Lilly 's short-term studies w ere confirm ed by tw o 34-week placebo- controlled studies the com pany conducted, studies 7 an d 8 in Table l .29 These tw o longer term studies consisted of initial 8-week studies follow ed by 26-week extension phases, for a total of 34 weeks. A to tal of 343 patien ts in the stud ies w ere trea ted w ith either 80 m illigram s a day of C ym balta (118 patients); 120 m illigram s a day of C ym balta (124 patients); or placebo (101 patients). A t the end of active treatm ent, the patien ts ' C ym balta w as stopped w ith double-b lind placebo substitu tion in a tw o w eek placebo lead-ou t phase.30 The placebo g roup continued on placebo for tw o additional w eeks.
10
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 30 of 246 PageID# 8260

Lilly again d id no t system atically m onitor w ithd raw al side effects in these studies, only record ing them if patien ts spon taneously rep o rted them .31 N evertheless, in the longer- te rm studies, s topp ing C ym balta again m ore th an doub led the risk of an tidepressan t w ithd raw al reactions by com parison w ith stopp ing placebo: the odds ratio w as 4.95.32 The increased risk w as statistically significant: the p-value w as 0.023.33 Thus, in Lilly's longer-term placebo-controlled studies, s topp ing C ym balta significantly increased the risk of w ithd raw al reactions alm ost 5-fold by com parison w ith stopp ing placebo.
C o n f i r m a to r y E v id e n c e f r o m
L i l l y 's 5 2 - W e e k L o n g e r - T e r m S t u d y
Lilly also conducted a longer-term , 52-week s tudy of C ym balta for depressed patients, s tudy 9 in Table 1. This s tudy w as n o t placebo-controlled; it w as open label. A to tal of 553 patien ts partic ipa ted in the study. In th is longer-term study, too, Lilly d id no t system atically m onitor C ym balta w ithdraw al side effects, only record ing them if patien ts spon taneously rep o rted them .34 N otw ith stand ing the absence of system atic m onitoring, 50.8% of C ym balta patien ts s t i l l rep o rted an tidepressan t w ithdraw al reactions u p o n d iscontinuing the d ru g .35 H ad Lilly u sed system atic m onitoring, one w ou ld expect the ra te to be even h igher.36 Table 4 rep roduces ano ther Lilly table listing the w ithd raw al side effects rep o rted by patien ts after a year of trea tm en t w ith C ym balta.37
11
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 31 of 246 PageID# 8261

Table 4C ym balta W ithdraw al Side Effects
in Lilly 's Longer-Term 52-W eek StudyTable 4Discontinuation-emergent adverse events after long-term treatment for which the incidence was at least 2%
Event Duloxetine (iV=553; n (%))
Patients with > 1 DEAE 281 (50.8)Dizziness (excluding vertigo) 106 (19.2)Anxiety NEC 55 (9.9)Nausea 54 (9.8)Headache NOS 40 (7.2)Insomnia 37 (6.7)Irritability 33 (6.0)Vomiting NOS 24 (4.3)Nightmare 16(2.9)Parses thesia 16 (2.9)Tinnitus 16 (2.9)Crying 15 (2.7)Depressed mood 15 (2.7)Depression NOS 15 (2.7)Anorexia 14 (2.5)Diarrhea NOS 14 (2.5)Myalgia 13 (2.4)Tremor 12 (2.2)Nervousness 11 (2.0)
NEC=not elsewhere classified; NOS:=not otherwise specified.
As seen in Lilly 's list in Table 4, the side effects of an tidepressan t w ithdraw al include characteristic physical side effects (such as dizziness, nausea, headaches, vom iting, parathesias [abnorm al sensations such as electric shock-like sensations in the brain], d iarrhea, and trem ors) as w ell as characteristic psychiatric side effects (including anxiety, depression, insom nia, irritability , n ightm ares, an d crying).
12
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 32 of 246 PageID# 8262

S ection 2: P o s t-M a rk e tin g A d v e rse E v en t R ep o rts (A ERs) o f C y m b a lta W ith d ra w a l
Once a d ru g is on the m arket and prescribed to m illions of patients, postm arketing surveillance adds add itional safety inform ation to w h a t w as learned in p re-approval pharm aceutical com pany stud ies.38 In this country, the FD A 's system for postm arketing surveillance is called the A dverse Event R eporting System, or AERS. H ealthcare professionals know the system by the nam e M edW atch. H ealthcare professionals and consum ers can rep o rt side effects to the FDA or the pharm aceutical com pany, w hich collects the inform ation, w rites the case reports, and subm its them to the FDA. Pharm aceutical com panies w rite 94% of the reports and fo rw ard them to the FDA.39 The FDA relies on postm arketing surveillance for its regu la to ry decisions. The system is vo luntary , or spontaneous, n o t m andatory . The FDA receives abou t 500,000 side effect repo rts a year, w hich are estim ated to rep resen t 1% to 10% of all side effects tha t actually occur.40 The rep o rt rate for any particu lar side effect m ay vary by drug , side effect, and over time.
The technical term for these side effect reports is adverse event reports or adverse d ru g even t reports (ADERs). A ccording to the FDA and pharm acoepidem iology textbooks, adverse d ru g reports are the essential, core da ta of postm arketing surveillance.41 The consensus in the field is th a t the reports im ply the d ru g caused the side effect—the healthcare p rov ider or consum er w ho repo rted the event th o u g h t it w as re la ted to the d rug .42 The reports can include details such as the pa tien t's age, gender, diagnosis, concom itant m edications, dates of exposure, and the dates of the d ru g reaction. They also include a narra tive section in w hich the repo rte r can describe in som e detail w hat the patien t experienced. The narra tives p rov ide a descriptive p ictu re of the side effect th a t com plem ents m ore m atter-of-fact inform ation.
The im portan t role of postm arketing surveillance has been sum m arized in an article by Dr. Janet W oodcock, the d irector of the FD A 's C enter for D rug Evaluation and Research, and tw o of her colleagues at the agency. The article, en titled the "Role of Postm arketing Surveillance in C ontem porary M edicine," w as pub lished in the A ugust 2010 issue of the A n n u a l R e v i e w o f M e d ic in e .43 A ccording to W oodcock:44
Even w ell-controlled random ized controlled clinical trials cannot uncover every safety problem , no r are they expected to do so. In m ost cases, clinical trials are n o t large enough, diverse enough, or long enough in d u ra tion to p rov ide all the inform ation on a p ro d u c t's perform ance and safety. A dditionally , clinical trials of the size an d scope typically
13
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 33 of 246 PageID# 8263

su p p o rted by ou r curren t system are unlikely to reliably detect serious adverse events [side effects] th a t are rare, th a t occur w ith long latency, or th a t h a p p en in subpopulations w ho have no t partic ipa ted (or h ad sm all representation) in clinical studies.
Once a n ew m edical p ro d u c t en ters the m arket, it can be expected to be u sed in a pa tien t p o p u la tion th a t is m uch larger an d m ore heterogeneous th an those s tud ied in p reapp roval clinical trials. The real-w orld popu la tion has a b roader range of com orbidities, uses a w ide variety of concom itant m edications, has genetic d iversity th a t can affect d ru g m etabolism , an d m ay be trea ted for conditions th a t have n o t been studied. For all these reasons, postm arketing surveillance p lays a critical role in identify ing m edication risks th a t w ere p reviously unknow n.
For the p ast 40 years, spon taneous reporting has been the cornerstone of FD A 's postm arketing d ru g safety m onitoring. The spontaneous reporting system is based on the p u b lic—bo th healthcare professionals and their p a tien ts—volun tarily reporting adverse events, errors, and quality p roblem s they observe du rin g the use of a p ro d u c t to either m anufacturers or FD A .... Substantial u n d errep o rtin g of adverse events is w idely acknow ledged. M oreover, the reports subm itted are a h ighly selective sam ple of the events observed in practice. D espite these lim itations, w ell-docum ented observations m ade at the po in t of care — repo rted either to m anufacturers, w ho are requ ired by law to rep o rt to FDA, or directly to FDA — are an invaluable com ponent of the d ru g safety surveillance system .
The FDA m akes postm arketing surveillance da ta publicly available for research, so in d ep en d en t scientists can also exam ine and evaluate the data. So do m any foreign d ru g regulators. Personal in form ation th a t m igh t reveal the pa tien t's iden tity is redacted. The FDA m akes adverse event rep o rt da ta publicly available four tim es a year, on a quarterly basis, for in d ep en d en t scientists to exam ine and analyze.
The Institu te for Safe M edication Practices is one such g roup of indep en d en t scientists w ho evaluate an d analyze adverse event reports to the FDA.45 The Institu te is a nonprofit o rganization ded icated to educating the healthcare com m unity and patien ts about safe m edication practices.46 Four tim es a year, the Institu te publishes an analysis of adverse event reports called Q u a r te r W a tc h : M o n i t o r i n g F D A M e d W a t c h R e p o r t s .47
A ccording to the Institu te:48
14
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 34 of 246 PageID# 8264

Q uarter W atch ... m onitors all dom estic, serious adverse d ru g events repo rted to the FDA. We analyze com puter excerpts from the FDA A dverse Event R eporting System. These vo lun tary reports (best know n as M ed W atch reports) are a cornerstone of the na tio n 's system for m onitoring the safety of p rescrip tion d rugs after FDA m arketing approval.
The O ctober 3, 2012 issue of Q u a r te r W a tc h rep o rted th a t in the first q u arte r of 2012 reports to the FDA of C ym balta w ithdraw al ou tnum bered reports of w ithd raw al for all o ther d rugs:49
We observed a signal for serious d ru g w ithd raw al sym ptom s associated w ith C ym balta, a w idely u sed an tidepressan t th a t is also ap p roved to treat arthritis and back pain , anxiety, and fibrom yalg ia....C ym balta w as notable in the first q u arte r of 2012 because reports of serious d ru g w ithd raw al effects (n=48) ou tnum bered all o ther regu larly m onito red d rugs, including an opioid trea tm en t for narcotics addiction, buprenorph ine-naloxone (Suboxone) (n=43) and the p o ten t synthetic opioid fentanyl (Duragesic) (n=34)....The specific sym ptom s spanned a w ide range of d isorders. They included physical and neurological sym ptom s such as dizziness, paresthesia, an d abnorm al sw eating. But psychiatric sym ptom s w ere also repo rted such as crying, anger, suicidal ideation, hallucinations, and personality change.
Thus, the reports to Lilly an d the FDA included severe, life th reaten ing cases of C ym balta w ithdraw al. Indeed, according to Q u a r te r W a tc h : 50
Several cases involved hosp ita liza tion ... .[and] all of th e .. .cases w ere coded as se rio u s....
The FDA defines serious side effects as those th a t resu lt in death , inpatien t hosp italization or p ro longation of a hospitalization, significant or persisten t incapacity, or b irth defects.51 Q u a r te r W a tc h described C ym balta w ithdraw al as a "m ajor d ru g safety issue":52
We docum ent a serious lapse in the system th a t ough t to be p rov id ing com plete inform ation and clear w arn ings for patien ts and health professionals about the extensive w ithd raw al effects of the an tidepressan t Cym balta. The M edication G uide for patien ts gives no h in t th a t w ithd raw al sym ptom s can affect half of those d iscontinuing Cym balta,
15
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 35 of 246 PageID# 8265

and th a t m any cases m ay be severe, persistent, or both. The prescribing inform ation for physicians and pharm acists does n o t p rov ide realistic schedules for dose tapering or a clear p icture of the likely incidence of these reactions....Excessive and unnecessary long-term use [of an tidepressants] is ano ther likely consequence of serious w ithd raw al effects w ith o u t adequate w arnings. Patients try to d iscontinue, encounter severe sym ptom s, and discover th a t these problem s d isappear quickly if they resum e the drug . W hile an tidepressan ts are n o t classified as d rugs of abuse, they share the risk of w ithd raw al sym ptom s w ith the opio ids and benzodiazepines [V alium -type drugs]. G iven th a t an tidepressan t d rugs w ere tested p rim arily in short-term trials of six to n ine w eeks, the fact th a t th a t 60% of the large popu la tion tak ing an tidepressan ts h ad done so for tw o years or m ore m oves th is issue onto the short list of m ajor d ru g safety issues.
The strong signal of serious C ym balta w ithd raw al reactions seen in post-m arketing adverse event reports to the FDA —a larger num ber of reports th an for any o ther d rugs includ ing opiates or V alium -type m edications —prov ides strong supporting evidence C ym balta causes w ithd raw al reactions th a t can be severe. As discussed later in this report, I agree w ith the Q u a r te r W a tc h scientists th a t the inform ation Lilly p rov ides doctors an d patien ts in its C ym balta label is inadequate and th a t C ym balta w ithdraw al is a serious d ru g safety issue.
16
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 36 of 246 PageID# 8266

S ection 3: T he E v id en ce in P u b lish e d S cientific S tu d ie s of A n tid e p re s s a n t W ith d ra w a l
Published stud ies have established th a t an tidepressan ts cause w ithd raw al reactions.53 Indeed, a s tudy and review s calling atten tion to w ithd raw al w ith new er SSRI an tidepressan ts w ere fu nded an d published by Eli Lilly w hen the com pany w as m arketing its earlier an tidepressan t, Prozac.54 In the study, L illy-funded researchers system atically m onito red w ithd raw al side effects using checklist ra ting scales to com pare the frequency of w ithdraw al reactions in patien ts stopp ing Prozac, Zoloft and Paxil.55 The s tudy w as conducted in the mid-1990s before Lilly began m arketing C ym balta in 2004. A subsequent s tudy by som e of the sam e researchers evaluated w ithd raw al reactions in patien ts stopp ing the SNRI-type an tidepressan t Effexor.56 Table 5 sum m arizes the resu lts of the studies.57
Table 5Lrequency of A ntidepressan t
W ithdraw al ReactionsAntidepressant Half-Life Frequency of
Withdrawal ReactionsEffexor 5 hou rs 78%
Paxil 21 hours 66%Zoloft 26 hours 60%Prozac 4-6 days 14%
As seen in Table 5, 78% of patien ts stopp ing Effexor, 66% of patien ts stopp ing Paxil, 60% of patien ts stopp ing Zoloft, and 14% of patien ts s topp ing Prozac experienced w ithd raw al sym ptom s in the studies.
T h e R o le o f a n
A n t i d e p r e s s a n t 's H a l f - L i fe
As show n in Table 5, the frequency of w ithd raw al reactions directly correlates w ith an an tidep ressan t's half-life, a m easure of how quickly the an tidepressan t w ashes o u t of the body. A m edication 's half-life is the length of tim e it takes for half the d ru g to be excreted from the body after a pa tien t stops taking it. If an an tidep ressan t's half-life is tw enty-four hours, then tw enty-four h o u rs after the last d o se —the next d a y —half the an tidepressan t is elim inated. A nother tw enty-four h ou rs later, half ag a in —a total of 75% of the d ru g —has been elim inated. By contrast, if the an tidep ressan t's half-life is seven days, then it takes a w e ek —instead of a d a y —for half of it to be gone, and tw o
17
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 37 of 246 PageID# 8267

w eek s—instead of tw o d a y s—for th ree quarters of it to be gone. O bviously, this is a significant difference in h o w precip itously or g radually the level of the an tidepressan t d rops and therefore how m uch tim e b ra in cells have to ad ap t to the change.W ithdraw al reactions are evidence of abnorm al b ra in cell functioning in response to insufficient tim e for the cells to g radually ad ap t to w ithd raw al of the drug . Even after an an tidepressan t is gone, w ithd raw al reactions can persist because the b ra in cells are still d istressed, try ing to cope w ith the d ro p in the d ru g 's level.
A nother s tan d ard m easure of how quickly an tidepressan ts w ash ou t of the body is the tim e it takes for 90% of the d ru g to be elim inated, w hich is about five half-lives. W ith its extrem ely short half-life, Effexor w ashes ou t of the body in about a day. W ith their short half-lives, Paxil and Zoloft are elim inated w ith in about four to five days. By contrast, Prozac takes about 25 days to be elim inated, p rov id ing an autom atic, g radual taper.Like Effexor, C ym balta h as an extrem ely short half-life of about 12 hou rs.58 Thus, C ym balta w ashes o u t of the body precip itously in abou t tw o and a half days. Because C ym balta 's half-life (12 hours) is be tw een Effexor's (5 hours) and Paxil's (21 hours), if Lilly h ad system atically m onito red w ithd raw al side effects in its C ym balta studies, one w ou ld expect to find betw een 66% and 78% of patien ts experienced C ym balta w ithdraw al.
W o r s t O f fe n d e r s
Table 6 lists the half-lives, 90% elim ination tim es, and typical tim e of onset of w ithd raw al side effects of SSRIs, SNRIs, and o ther new er an tidepressan ts.59 In Table 6, the an tidepressan ts are listed from those w ith the shortest half-lives—Effexor and C ym balta—to those w ith the longest half-lives—Rem eron, Celexa, and Prozac. The halflives of the an tidepressan ts span a w ide range from five hou rs to four to six days. As seen in Table 6, tw o of the w orst offenders are C ym balta and Effexor w ith their extrem ely short half-lives. Because of their extrem ely short half-lives, patien ts on C ym balta or Effexor can experience w ithd raw al side effects if they inadverten tly m iss just one dose.60
18
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 38 of 246 PageID# 8268

Table 6The Half-Lives, E lim ination Times, and Typical O nset
of W ithdraw al Sym ptom s after S topping A ntidepressan tsAntidepressant Half-Life 90% Eliminated Typical Onset of
WithdrawalEffexor, Effexor XR 5 hours 1 day D ay 1-2
C ym balta 12 h ou rs 2.5 days D ay 2-3Luvox 15.6 h ou rs 3.3 days D ay 2-3
Serzone 11-24 hours 3.6 days D ay 2-3Paxil CR 15-20 hours 3.6 days D ay 2-3
Paxil 21 h ou rs 4.4 days D ay 2-3W ellbutrin,
W ellbutrin SR, W ellbutrin XL
21 h ou rs 4.4 days D ay 2-3
Zoloft 26 h ou rs 5.4 days D ay 3-4Lexapro 27-32 hours 6.1 days D ay 3-5R em eron 20-40 hours 6.3 days D ay 3-5
Celexa 35 h ou rs 7.3 days D ay 3-6Prozac 4-6 days 25 days 2-3 w eeks
C h a r a c te r is t ic S y m p to m s o f
A n t i d e p r e s s a n t W i th d r a w a l
M ore th an 50 sym ptom s of an tidepressan t w ithd raw al have been repo rted .61 W ithdraw al sym ptom s are b road ly d iv ided in to tw o m ain categories: psychiatric sym ptom s an d physical sym ptom s.62 The psychiatric sym ptom s of an tidepressan t w ithd raw al include depressed m ood, anxiety, insom nia, n ightm ares, irritability, agitation, im pulsiv ity , or suicidal and violent urges. The characteristic physical sym ptom s include d izziness th a t can be disabling, im balance, flu-like aches and pains, nausea, vom iting, headaches, trem ors, tingling sensations, and electric shock-like "zaps" in the brain. Table 7 rep roduces the checklist of w ithd raw al sym ptom s used in the L illy-funded Prozac s tudy .63 Thus, Table 7 is the Lilly-sponsored list of side effects characteristic of an tidepressan t w ithdraw al.
19
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 39 of 246 PageID# 8269

Table 7A ntidepressan t
W ithdraw al Side Effects
A ppendix. D iscontinuation-Em ergent Signs and Symptoms
Symptom
1. Nervousness or anxiety2. Elevated mood, feeling high3. Irritability4. Sudden worsening of mood5. Sudden outbursts o f anger ("anger attacks")6. Sudden panic or anxiety attacks7. Bouts of crying or tearfulness8. Agitation9. Feeling unreal or detached
ID. Confusion or trouble concentrating 11. Forgetfulness or problems with memory 12- Mood swings13. Trouble sleeping, insomnia14. Increased dreaming or nightmares15. Sweating more than usual16. Shaking, trembling17. Muscle tension or stiffness18. Muscle aches or pains19. Restless feeling in lega20. Muscle cramps, ipasms, or Iwitching21. Fatigue, tiredness22. Unsteady gait or incoordination .23. Dlurrcd vision24. Sore eyes25. Uncontrollable mouth’tonguc movements26. Problems with speech or speaking clearly27. Headache26, Increased saliva in mouth29. Distiness, lightheadedness, or sensation of spinning (vertigo)30. Nose running3 1. Shortness of breath, gasping for air32. Chills33. Fever34. Vomiting35. Nausea36. Dianhca37. Stomach cramps 36. Stomach bloating39. Unusual visual sensations (lights, colon, geometne shapes, etc.)40. Burning, numbness, tingling sensations41. Unusual sensitivity to sound42. Ringing or noises in the ears43. Unusual tastes or smells
Patient *M asked, "During the past 7 days, hove you csperieacod any changes in the following symptoms.,” Patient chose one of four response* (new symptom, old symptom, but worse; old symptom, but improved; old symptom, but unehanjed or symptom not ptosent).
20
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 40 of 246 PageID# 8270

Similar side effects were seen in Lilly's later Cymbalta studies (compare Table 7 from Lilly's Prozac study to Table 4 from Lilly's Cymbalta studies). Table 4 is a shorter list than Table 7 because Lilly did not systematically monitor withdrawal side effects in its Cymbalta studies, as was done in the Prozac study. In addition, Table 4 does not list all of the Cymbalta withdrawal side effects spontaneously reported by patients; it only lists side effects that were reported by two percent or more of patients.
Table 8 reproduces another table of characteristic symptoms of antidepressant withdrawal from T h e A n t i d e p r e s s a n t S o lu t io n : A S t e p - b y - S t e p G u id e to S a fe ly O v e r c o m in g
A n t i d e p r e s s a n t W i th d r a w a l D e p e n d e n c e , a n d " A d d i c t i o n " .M Table 8 lists a total of 58 side effects characteristic of antidepressant withdrawal that have been reported in the medical literature. Table 8 breaks this large number of withdrawal side effects down into smaller, easier to recognize clusters of characteristic side effects of antidepressant withdrawal. The characteristic psychiatric side effects are divided into depressive symptoms, anxiety symptoms, irritability and aggression, confusion and memory problems, mood swings, hallucinations, and dissociation. The characteristic physical side effects are divided into flu-like symptoms, gastrointestinal symptoms, dizziness, headache, tremor, and abnormal sensations.
21
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 41 of 246 PageID# 8271

Table 8Symptoms of
Antidepressant WithdrawalPsychiatric Symptoms Medical Symptoms
D e p re ss iv e S y m p to m s F lu -L ik e S y m p to m s
1. Crying spells 29. Flu-like aches and pains2. Worsened mood 30. Fever3. Low energy (fatigue, lethargy, malaise) 31. Sweats4. Trouble concentrating 32. Chills5. Insomnia or trouble sleeping 33. Runny nose6. Change in appetite 34. Sore eyes7. Suicidal thoughts8. Suicide attempts G a s tr o in te s tin a l S y m p to m s
35. NauseaA n x ie t y S y m p to m s 36. Vomiting
9. Anxious, nervous, tense 37. Diarrhea10. Panic attacks (racing heart, breathless) 38. Abdominal pain or cramps11. Chest pain 39. Stomach bloating12. Trembling, jittery, or shaking
D iz z in e s s
Ir r i ta b il i ty a n d A g g re s s io n 40. Disequilibrium13. Irritability14. Agitation (restlessness, hyperactivity)15. Impulsivity16. Aggressiveness17. Self-harm18. Homicidal thoughts or urges
41. Spinning, swaying, lightheaded42. Hung over or waterlogged feeling43. Unsteady gait, poor coordination44. Motion sickness
H ea d a ch e
45. HeadacheC o n fu s io n a n d M e m o r y P ro b lem s
19. Confusion or cognitive difficulties20. Memory problems or forgetfulness
46. Tremor
M o o d S w in g s
21. Elevated mood (feeling high)22. Mood swings23. Manic-like reactions
S e n so r y A b n o r m a lit ie s
47. Numbness, burning, or tingling48. Electric zap-like sensations in the brain49. Electric shock-like sensations in the body50. Abnormal visual sensations
H a llu c in a tio n s 51. Ringing or other noises in the ears24. Auditory hallucinations 52. Abnormal smells or tastes25. Visual hallucinations
O th e r
D isso c ia tio n
26. Feeling detached or unreal
53. Drooling or excessive saliva54. Slurred speech55. Blurred vision
O th e r
27. Excessive or intense dreaming28. Nightmares
56. Muscle cramps, stiffness, twitches57. Feeling of restless legs58. Uncontrollable twitching of mouth
22
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 42 of 246 PageID# 8272

T h e C h a r a c te r is t ic T im e C o u r s e
o f A n t i d e p r e s s a n t W i th d r a w a l
In addition to characteristic symptoms, antidepressant withdrawal typically follows a characteristic time course. Patients stopping antidepressants with short half-lives like Cymbalta typically develop withdrawal side effects within one to five days after stopping the drugs.65 Indeed, in Lilly's Cymbalta studies, many patients reported withdrawal side effects within one to two days.66 Because of Cymbalta's extremely short half-life, patients who inadvertently miss just one dose can experience withdrawal reactions.67 The close temporal relationship between lowering the dose of Cymbalta and the abrupt development of symptoms is characteristic of antidepressant withdrawal.68 By contrast, depressive relapse (a return of the patient's original depression) occurs gradually, one to two months or more after stopping an antidepressant.69
M ild , M o d e r a te , a n d S e v e r e
W ith d r a w a l R e a c t io n s
Antidepressant withdrawal side effects can be categorized as mild, moderate, or severe.70 This is a global, or overall, assessment based on the patient's worst symptoms and their effect on the patient's ability to function. Mild withdrawal side effects are noticeable but not terribly uncomfortable and do not affect the patient's ability to function. Moderate withdrawal is sufficiently uncomfortable that it negatively affects the patient's ability to think clearly and/or function normally. Severe withdrawal reactions are characterized by one or more debilitating side effects that:
• include suicidal thoughts, suicidal behavior, harm to the patient or others, hallucinations, or manic-like symptoms
• make it impossible for the patient to function normally for all or part of the day
• necessitate resuming the antidepressant or putting the dose back up to stop the withdrawal symptoms
• require tapering the antidepressant so painstakingly slowly that it takes more than four months to safely discontinue the drug
According to Lilly, in the company's short-term, placebo-controlled Cymbalta studies of depressed patients, 9.6% of Cymbalta withdrawal side effects were severe.71 In the company's year-long study, 17.2% of withdrawal side effects were severe.72
23
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 43 of 246 PageID# 8273

Severe withdrawal reactions can be incapacitating, leaving patients bedridden and unable to work.73 Because antidepressant withdrawal reactions can be severe and even life-threatening, antidepressants should not be stopped abruptly, with rare exceptions such as modest doses of Prozac with its automatic, slow, built-in taper. Instead, the drugs should be tapered, i.e. the dose should be lowered gradually over an extended period of time. How long it takes a patient to taper off an antidepressant depends on a number of factors including the particular drug, how long the patient has been on it, the dose, and the patient's vulnerability to withdrawal symptoms. Some patients are extremely sensitive to antidepressant withdrawal reactions. There are reports of people who could not stop using their antidepressant because of severe withdrawal reactions.74
Antidepressant tapering schedules need to be individualized for patients.75 When a patient has severe withdrawal reactions, one tries to adjust the reductions until they are small enough that the patient can tolerate them relatively comfortably. One aims for the patient to only have mild to moderate withdrawal side effects that typically peak within seven to ten days and subside over the course of two to three weeks. If this pattern has been achieved, the patient's dose can be lowered about once a month. But especially with worst offenders like Cymbalta and Effexor, even when the drug is tapered slowly, patients may experience severe withdrawal reactions and require seven or more months to get off the drug. Unfortunately, many doctors are unaware of antidepressant withdrawal and how slowly antidepressants need to be tapered for some patients.
P h y s ic a l D e p e n d e n c y
In medicine, physical dependency is the term for when patients are forced to go back on a drug that has been stopped (or back up on the dose that has been lowered) in order to suppress intolerable or debilitating withdrawal side effects. Thus, when patients experience moderate to severe antidepressant withdrawal and are forced to resume taking the drug and/or take longer to taper off, they are physically dependent on the antidepressant to prevent unpleasant or debilitating withdrawal reactions.
D if fe r e n t ia t in g W i th d r a w a l
f r o m R e la p s e
When doctors and patients are misinformed about antidepressant withdrawal, there is a danger that they will mistake withdrawal side effects for a return of the patients' underlying psychiatric condition. On the other hand, when doctors and patients know what to look for, in most instances it can become easier for the physician to distinguish withdrawal from relapse. The characteristics that typically set withdrawal apart from
24
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 44 of 246 PageID# 8274

depressive relapse are: the timing of the onset of symptoms; the presence of physical symptoms of withdrawal; the characteristic time course for withdrawal side effects to peak and fade; and the dramatic disappearance of withdrawal side effects if they are intolerable and the prior antidepressant dose is reinstated.
Unfortunately, when doctors and patients are misinformed about antidepressant withdrawal they can mistake withdrawal for relapse of the patients' original psychiatric condition. In this antidepressant catch-22, the drug may be reinstated —often for years — needlessly exposing patients to the side effects and long-term risks of antidepressants.In many instances, not only is the drug restarted, the dose is increased and additional drugs—additional antidepressants, mood stabilizers, antianxiety agents, and sleeping pills—are added to "treat" withdrawal that has been misdiagnosed as a relapse of the patients' prior psychiatric condition. In the process, patients get the false impression their psychiatric conditions and prognoses are far worse than they really are.
25
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 45 of 246 PageID# 8275

Section 4: The Biological Mechanismof Cymbalta Withdrawal
Stopping C ym balta or low ering the dose can cause w ithd raw al reactions because of the d ru g 's m echanism of action. W hen the C ym balta dose is low ered, b ra in cells m ay n o t have sufficient tim e to ad ap t to the su d d en change. W ithdraw al sym ptom s are evidence of abnorm al b ra in cell functioning in response to precip itous w ithd raw al of an an tidepressan t, no t enough tim e for the cells to g radually adjust.
Brain cells are n o t passive, in response to m edications including an tidepressan ts like Cym balta. Instead, b ra in cells actively adap t, or change, in response to drugs. The adap ta tions are typically in the direction of reversing or counteracting the effects of drugs. Lilly p rom otes C ym balta as increasing sero tonin and norep inephrine levels in the b ra in .76 Serotonin and norep inephrine are tw o of the chemical signals b ra in cells use to com m unicate w ith one another. These chem icals ta rget sero tonin and norep inephrine receptors on the surfaces of bra in cells. In response to increased sero tonin and norep inephrine signals, b ra in cells decrease the sensitivity of their receptors to the signals in a process called "d o w n regu la tion ."77 Since the serotonin and norep inephrine receptors are m ade of proteins, w ith in the cells changes occur in p ro te in synthesis, w hich involves changes in the instructions g iven by the cells' DNA, the m aster code regu lating cellular function.78 The process takes w eeks or m onths. Some of the changes the cells m ake are believed to be responsible for the d ru g s ' therapeutic effects. W hen doctors prescribe an tidepressan ts like Cym balta, w e often tell patien ts the d ru g s take about a m onth to w ork, because the changes in b ra in cells take tim e to occur. O ther changes in the b ra in cells are believed to be responsible for the side effects of an tidepressants.
W hen patien ts low er the dose or stop taking Cym balta, b ra in cells need sufficient tim e to u n d o the adap ta tions they m ade to living w ith the d rug . The cells need to read ap t to living w ith less C ym balta or to living w ith o u t the drug . W hereas the cells dow n regu la ted in response to C ym balta, n o w they need to "u p regu late" in response to less of the drug . Once again, the process takes w eeks or m onths. W hen the C ym balta dose is low ered, the b ra in cells m ay no t have sufficient tim e to adapt. The stress on the cells p roduces abnorm al b ra in cell activity, resu lting in the sym ptom s of C ym balta w ithdraw al.
Low ering the dose of C ym balta too ab rup tly is like d riv ing a car at sixty m iles per h o u r and sudden ly p u ttin g it in reverse. Instead, one needs to slow the car d ow n gradually ,
26
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 46 of 246 PageID# 8276

and only put it in reverse once it has stopped. Similarly, one needs to gradually taper Cymbalta to allow the brain cells sufficient time to adjust.
This biological model explains why putting the dose of Cymbalta back up suppresses withdrawal symptoms: If the brain cells have not had enough time to readapt to a drop in Cymbalta levels, putting the dose back up reestablishes the level with which the brain cells are comfortable.
This biological model also explains why an antidepressant's half-life correlates with the frequency of withdrawal reactions. The shorter an antidepressant's half-life, the more quickly it washes out of the body and the more likely patients are to experience withdrawal reactions. Even before Lilly studied Cymbalta in patients, the company knew from pharmacodynamic studies Cymbalta had an extremely short half-life and would be expected to cause withdrawal reactions in a high percentage of patients. This biological mechanism explains the high rate of Cymbalta withdrawal reactions seen in patients in Lilly's studies.
27
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 47 of 246 PageID# 8277

Section 5: Bradford Hill Causality AssessmentCymbalta Withdrawal
Taken together as a w hole, the available evidence satisfies the B radford Hill criteria for concluding th a t stopp ing C ym balta can cause characteristic w ithd raw al reactions tha t can be severe. In troduced in 1965 by B radford Hill, the criteria have becom e w idely u sed in m edicine to p rov ide a form al structu re for evaluating causality; for exam ple, for evaluating w hether or n o t a d ru g causes specific side effects.79 The n ine B radford Hill criteria for evaluating causality are: experim ent, streng th of association, consistency, tem porality , biological gradient, specificity, plausibility, coherence, and analogy.80 N ot all of the criteria n eed to be satisfied to conclude a d ru g causes a side effect; instead, the criteria p rov ide a fram ew ork for com prehensively evaluating the available evidence.
E x p e r im e n t
A ccording to the B radford Hill criteria, "experim ental evidence is the m ost com pelling evidence of causation."81 In the case of C ym balta w ithdraw al, th is criteria is met: In Lilly 's short-term , placebo-controlled studies stopp ing C ym balta m ore th an doub led the risk of w ithd raw al sym ptom s by com parison w ith stopp ing placebo: the odds ratio w as 2.68.82 The increased risk w as statistically significant: the p-value w as less th an 0.001.83 The risk of specific w ithd raw al side effects w as elevated even more: By com parison w ith stopp ing placebo, stopp ing C ym balta significantly elevated the risk of nausea 23fold, dizziness 17-fold, parasth ias 11-fold, irritability 9-fold, n igh tm ares 8-fold, headaches 7-fold, and vom iting 4-fold.84 A m ong the C ym balta w ithd raw al side effects, 50.6% w ere m oderate an d 9.6% w ere severe.85
These resu lts w ere confirm ed in Lilly 's longer-term , 34-week placebo-controlled studies. In the longer-term studies, s topp ing C ym balta again m ore th an doubled the risk of an tidepressan t w ithd raw al reactions by com parison w ith stopp ing placebo: the odds ratio w as 4.95.86 The elevated risk w as statistically significant: the p-value w as 0.023.87
The resu lts of Lilly 's short and longer-term placebo-controlled studies w ere confirm ed by the com pany 's 52-week open label s tudy in w hich about 51% of patien ts reported w ithd raw al reactions w hen stopp ing C ym balta after one year of trea tm en t.88 A m ong the C ym balta w ithd raw al side effects, 46.3% w ere m odera te and 17.2% w ere severe.89
The evidence from Lilly 's C ym balta studies has also been confirm ed and elaborated u p o n by the FD A 's post-m arketing adverse event surveillance data. In the first quarter of 2012, reports of serious C ym balta w ithd raw al reactions ou tnum bered repo rts for all
28
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 48 of 246 PageID# 8278

other regu larly m onito red d rugs including narcotic (opiate-type) d ru g s and V alium - type (benzodiazepine) d rugs.90
The evidence from Lilly 's C ym balta studies is also su p p o rted by Lilly's earlier Prozac s tudy investigating the com parative rates of w ithd raw al reactions in patien ts stopp ing Prozac, Paxil, and Zoloft. In th a t study , w ith their short half-lives, s topp ing Paxil and Zoloft caused w ithd raw al reactions in 66% an d 60% of patien ts respectively.91 W ith its long half-life, s topp ing Prozac caused w ithd raw al reactions in a low er percentage of patients, 14%.
Supporting evidence also com es from Lilly's pharm acokinetic stud ies of Cym balta. C ym balta 's extrem ely short 12 h o u r half-life is consistent w ith C ym balta causing w ithd raw al reactions in a h igh percentage of patien ts stopp ing the d rug: 40 to 50% in Lilly 's studies.92
Taken together, this substantial body of experim ental resu lts p rov ides convincing scientific evidence th a t s topp ing C ym balta can cause w ithd raw al reactions in a h igh percentage of patien ts and th a t the w ithd raw al reactions can be severe.
S t r e n g t h o f A s s o c ia t io n
Strength of association refers to the degree to w hich a d ru g is associated w ith side effects. A statistically significant association is a strong association. In Lilly 's studies, C ym balta statistically significantly increased the risk of w ithd raw al reactions. In Lilly's short-term , placebo-controlled studies, C ym balta increased the risk of w ithdraw al reactions 2.68-fold.93 In Lilly's longer-term , 34-w eek placebo-controlled studies, C ym balta increased the risk of w ithd raw al reactions 4.95-fold.94 The risk of specific w ithd raw al sym ptom s w as e levated as m uch as 23-fold.95 These statistically significantly elevated risks dem onstrate a strong association betw een C ym balta and w ithd raw al side effects.
C o n s is t e n c y
C onsistency refers to w hether or no t additional studies have rep licated or confirm ed a d ru g 's association w ith side effects. Lilly 's short-term , placebo-controlled studies; Lilly's longer-term , 34-week placebo-controlled studies; and Lilly 's 52-week open label s tudy have consistency dem onstrated C ym balta increases the risk of w ithd raw al side effects in a h igh percentage of patients. Lilly 's pharm acodynam ic stud ies of C ym balta 's short
29
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 49 of 246 PageID# 8279

half-life and the FD A 's postm arketing adverse event surveillance da ta are also consistent w ith h igh ra tes of C ym balta w ithd raw al reactions.
T e m p o r a l i ty
Tem porality refers to the tem poral relationship betw een a d ru g and its side effects. A ccording to the B radford Hill criteria, in o rder to conclude th a t A causes B, A m ust occur before B. This criteria is m et in the case of C ym balta w ithdraw al side effects because in pharm aceutical com pany studies, the FDA requires th a t only trea tm en t em ergen t signs an d sym ptom s can be recorded as side effects.96 Side effects are only recorded after the baseline, w hen p atien ts begin trea tm en t w ith the s tudy d ru g or, as in the case of w ithd raw al side effects, in the phase of the s tudy m onitoring side effects after active trea tm en t has stopped. Thus, all the incidents of C ym balta w ithd raw al side effects in Lilly 's stud ies occurred in the first w eek or tw o after the patien ts stopped tak ing C ym balta, hav ing taken the d ru g for at least tw o m onths.
B io lo g ic a l G r a d ie n t
A biological g rad ien t refers to a dose-dependen t relationship betw een a d ru g and side effect: th a t is, the h igher the dose, the m ore frequen t the side effect. A dose-dependen t relationship p rov ides add itional evidence a d ru g causes a side effect. In Lilly 's sho rtterm , placebo-controlled studies, the patien ts on C ym balta received 40, 60, 80, or 120 m illigram s a day .97 The rates of w ithdraw al reactions w hen patien ts stopped the d ifferent doses w ere 42.4%, 39.2%, 36.9%, and 62.1% respectively. Thus, a h igher ra te of C ym balta w ithd raw al reactions w as seen in patien ts w ho h ad taken 120 m illigram s a day by com parison w ith the low er doses. A m ong the three low er doses, the dose- response relationship w as no t linear; the low er doses h ad sim ilar ra tes of C ym balta w ithd raw al reactions. In L illy 's longer-term 34-week placebo-controlled studies, a h igher percentage of the patien ts w ho h ad taken 120 m illigram s a day of C ym balta experienced w ithd raw al reactions th an those w ho h ad taken 80 m illigram s a d a y .98 Thus, in L illy 's stud ies the h ighest C ym balta dose resu lted in the h ighest ra tes of w ithd raw al side effects, p rov id ing su p p o rt for a biological g rad ien t, a lthough the low er doses d id no t have a linear relationship. It is im p o rtan t to note th a t pa tien ts vary w idely in their sensitivity to an tidepressan t w ithdraw al. Some patien ts experience severe w ithd raw al after stopp ing low doses of an tidepressan ts w hile o ther patien ts experience m ilder w ithd raw al side effects after s topp ing h igher doses of an tidepressants.
30
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 50 of 246 PageID# 8280

S p e c i f i c i t y
B radford Hill defines tw o types of specificity: (1) agents p roducing a specific resu lt n o t caused by o ther agents or conditions, or caused by few others, or (2) specificity in the m agn itude of the association. O ne of C ym balta 's w ithd raw al side effects satisfies the first definition: electric shock-like sensations in the brain. These b ra in "zaps" are characteristic of an tidepressan t w ithdraw al. C ym balta 's o ther w ithdraw al side effects do no t satisfy the first definition, since side effects like dizziness, nausea, vom iting, headaches, irritability, and n igh tm ares can be caused by a w ide range of d rugs and m edical conditions. But, C ym balta 's w ithd raw al side effects satisfy the second definition: based on the m agn itude of the association. In Lilly 's placebo controlled studies, C ym balta increased the risk of w ithd raw al side effects be tw een 2.86-fold and 23-fold by com parison w ith placebo, a very strong association. The m agn itude of the association suggests a Cym balta-specific effect, despite the fact th a t o ther d rugs or conditions can cause sim ilar sym ptom s. The m agn itude of the association satisfies the B radford Hill criteria for specificity.
P la u s ib i l i t y
Plausibility refers to a p lausible biological hypothesis for how C ym balta can cause w ithd raw al side effects. Lilly 's studies da ting back to the com pany 's Prozac s tudy com paring Prozac to Paxil an d Zoloft have dem onstrated stopp ing an tidepressan ts can cause w ithd raw al reactions, and an tidepressan ts w ith short half-lives can cause particu larly h igh rates of w ithd raw al in 40%-50% of patien ts or m ore. C ym balta has an extrem ely short half-life of about 12 hours. W hen the C ym balta dose is low ered, b ra in cells need sufficient tim e to re-adapt, for exam ple th ro u g h a process called "dow n regulation," w hich takes w eeks to m onths. W hen the dose is low ered, the b ra in cells m ay no t have sufficient tim e to ad ap t to the su d d en change. The stress on the cells p roduces abnorm al b ra in cell activity, resu lting in the sym ptom s of C ym balta w ithdraw al. W ith its extrem ely short half-life C ym balta is one of the w orst offenders: its precip itous exit from the body and the stress on b ra in cells try ing to ad ap t to the su d d en change in their env ironm ent is a plausible biological m echanism for C ym balta w ithdraw al.
C o h e r e n c e
Coherence refers to w hether or n o t ou r know ledge of C ym balta w ithd raw al is consistent w ith p rev ious know ledge. O ther classes of d rugs acting on the central nervous system including opiates, V alium -type (benzodiazepine) antianxiety agents and sleeping pills are also know n to cause w ithd raw al reactions w hen stopped. Earlier
31
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 51 of 246 PageID# 8281

classes of an tidepressan ts such as tricyclic an tidepressan ts have also been show n to cause w ithd raw al reactions. A nd stud ies of earlier SSRI and SNRI-type an tidepressan ts includ ing Prozac, Zoloft, Paxil and Effexor have dem onstrated th a t these so-called "new er" an tidepressan ts can cause w ithd raw al reactions. Thus, ou r cu rren t know ledge of C ym balta 's w ithd raw al side effects is consistent w ith p rev ious know ledge of these o ther drugs.
A n a l o g y
A nalogy is sim ilar to coherence and refers to w hether or no t C ym balta 's w ithdraw al side effects are analogous to those of o ther d rugs or conditions. C ym balta 's w ithdraw al side effects are analogous to the sim ilar side effects of d rugs such as Prozac, Zoloft, Paxil, and Effexor th a t are also p rom oted as increasing sero tonin or norep inephrine signals in the brain. Like C ym balta, these d rugs can also cause w ithd raw al reactions w hen stopped. C ym balta being one of the w orst offenders is analogous to Effexor, w hich also has an extrem ely short half-life.
S u m m a r y
In conclusion, the available da ta dem onstrates th a t the B radford Hill criteria for establishing causality are m et in the case of C ym balta w ithd raw al side effects. The B radford Hill criteria p rov ide a structu re for analyzing causality in m edicine. The resu lts of the above B radford Hill analysis su p p o rt m y op in ion th a t C ym balta frequently causes w ithd raw al reactions tha t can be severe.
32
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 52 of 246 PageID# 8282

S ection 6: L illy 's L ab e l is In a d e q u a te a n d M is le a d in g w ith R eg a rd to C y m b a lta W ith d ra w a l
For prescrib ing doctors like m yself and for patien ts, an an tidep ressan t's likelihood of causing w ithd raw al sym ptom s and, ultim ately , physical dependency is an im portan t factor in deciding w hether to prescribe or take a particu lar an tidepressan t versus an alternative m edication. The degree of risk of w ithd raw al sym ptom s associated w ith a particu lar an tidepressan t m ust be considered by any doctor w ho m igh t prescribe the d rug , and any patien t w ho m igh t take it.
D octors like m yself prescribe m edicines such as C ym balta rely ing on the accuracy of the d ru g 's label (i.e., the prescrib ing inform ation contained in the package insert and pub lished in the Physicians' D esk Reference, the so-called "PDR"). Rarely do w e perform our ow n clinical studies or have tim e to research w h a t o ther studies have been perform ed on a particu lar m edication. A lthough w e have access to o ther sources of inform ation, such as pharm aceutical represen tative detailing, recom m endations by fellow physicians, and m edical journal publications, treating physicians rely on the label as an u ltim ate au thority of a d ru g 's safety and efficacy.
The original 2004 C ym balta label stated:99
D iscontinuation of T reatm ent w ith C ym balta - D iscontinuation sym ptom s have been system atically evaluated in patien ts tak ing Cym balta. Follow ing ab ru p t d iscontinuation in placebo-controlled clinical trials of u p to 9-weeks dura tion , the follow ing sym ptom s occurred at a rate greater th an or equal to 2% and at a significantly h igher ra te in du loxetine-treated patien ts com pared to those d iscontinuing from placebo: dizziness; nausea; headache; paresthesia; vom iting; irritability; and n ightm are.
Lilly 's list of w ithd raw al side effects th a t occurred in significantly m ore C ym balta patien ts is the sam e as the list in Table 3 in th is rep o rt of the side effects th a t occurred at significantly h igher rates in Lilly 's original short-term studies of depressed patients. In 2005, Lilly ad d ed "M DD" before "placebo-controlled clinical trials" so the label read (the change is h igh ligh ted in bold):100
D iscontinuation of T reatm ent w ith C ym balta - D iscontinuation sym ptom s have been system atically evaluated in patien ts tak ing Cym balta.Follow ing ab ru p t d iscon tinuation in M D D placebo-controlled clinical
33
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 53 of 246 PageID# 8283

trials of u p to 9-weeks dura tion , the follow ing sym ptom s occurred at a rate greater th an or equal to 2% and at a significantly h igher rate in C ym balta-treated patien ts com pared to those d iscontinuing from placebo: dizziness; nausea; headache; paresthesia; vom iting; irritability; and nightm are.
A fter that, the label stayed essentially the sam e for several years until 2008. In 2008,Lilly took o u t "trials of u p to 9-w eeks dura tion ," changed the percentage w ithdraw al ra te from 2% to 1%, and ad d ed add itional w ithd raw al sym ptom s tha t occurred at significantly h igher rates in Lilly 's la ter C ym balta studies:101
D iscontinuation of T reatm ent w ith C ym balta - D iscontinuation sym ptom s have been system atically evaluated in patien ts tak ing duloxetine. Follow ing ab ru p t d iscon tinuation in placebo-controlled clinical trials, the follow ing sym ptom s occurred at a ra te greater th an or equal to 1% and at a significantly h igher rate in du loxetine-treated patien ts com pared to those d iscontinuing from placebo dizziness; nausea; headache; paresthesia; vom iting; irritability; n ightm ares; insomnia, diarrhea, anxiety, hyperhidrosis and vertigo.
In 2009, Lilly ad d ed "or tapered" to the label and "fatigue" to the list of C ym balta 's w ithd raw al side effects:102
D iscontinuation of T reatm ent w ith C ym balta - D iscontinuation sym ptom s have been system atically evaluated in patien ts taking duloxetine. Follow ing ab ru p t or tapered discon tinuation in placebo-controlled clinical trials of u p to 9-weeks dura tion , the follow ing sym ptom s occurred at a rate greater th an or equal to 1% and at a significantly h igher rate in du loxetine-treated patien ts com pared to those d iscontinuing from placebo: dizziness; nausea; headache; fatigue; paresthesia; vom iting; irritability; n ightm ares; insom nia, d iarrhea, anxiety, hyperh id rosis and vertigo.
In 2012, Lilly changed "at a ra te greater th an or equal to 1%" to "at 1% or greater," a ltered the sequence of the w ithd raw al side effects and rem oved "n igh tm ares" so the label read :103
D iscontinuation of T reatm ent w ith C ym balta - D iscontinuation sym ptom s have been system atically evaluated in patien ts tak ing duloxetine. Follow ing ab ru p t or tapered d iscontinuation in
34
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 54 of 246 PageID# 8284

placebo-controlled clinical trials, the follow ing sym ptom s occurred at 1% or greater and at a significantly h igher ra te in duloxetine- trea ted patien ts com pared to those d iscontinuing from placebo: dizziness; nausea, headache, paresthesia, fatigue, vom iting, irritability, insom nia, d iarrhea, anxiety, and hyperhidrosis.
Since en tering the m arket, Lilly's label for C ym balta has failed to p rov ide accurate and /o r sufficient inform ation about the frequency, severity, and du ra tio n of those sym ptom s caused by stopp ing C ym balta, i.e., C ym balta w ithdraw al.
Lilly 's label uses the phrases "D iscontinuation of T reatm ent w ith C ym balta" and "d iscon tinuation sym ptom s," euphem ism s for C ym balta w ithdraw al. In m y opinion, Lilly 's label shou ld use the p la in English phrases "C ym balta W ithdraw al" and "w ithd raw al sym ptom s" so doctors and patien ts readily u n d e rs tan d C ym balta can cause w ithd raw al reactions. In contrast to Lilly 's C ym balta label in the U nited States, in Europe Lilly's C ym balta label explicitly uses the phraseology "w ithd raw al sym ptom s," instead of the euphem ism discon tinuation sym ptom s.104
Lilly 's label asserts w ithd raw al "sym ptom s have been system atically evaluated in patien ts tak ing C ym balta" in the com pany 's studies. But, as d iscussed earlier in this report, in its C ym balta stud ies Lilly d id n o t system atically m onitor w ithdraw al reactions w ith the sym ptom checklist ra ting scale u sed in the earlier L illy-sponsored s tudy com paring stopp ing Prozac w ith s topp ing Paxil or Zoloft.105 Instead, in Lilly's C ym balta studies, w ithd raw al side effects w ere only recorded if patien ts recognized and vo lun teered them .106 Lilly's unsystem atic approach is called "non-probing" because the patien ts w ere n o t specifically asked about side effects.107 This unsystem atic approach is also called "spontaneous" reporting because patien ts m ust spontaneously vo lun teer the side effects.108 Spontaneous reporting of side effects is w ell-know n to resu lt in significant und errep o rtin g .109 Lilly 's C ym balta label m isleadingly suggests w ithd raw al side effects w ere m ore rigorously and sensitively evaluated in the com pany 's studies th an w as the case.
W ith regard to the frequency of C ym balta w ithd raw al reactions, L illy 's C ym balta label gives the m isim pression th a t the frequency of w ithd raw al reactions is low, approxim ately 1% to 2% of patients. These percentages suggest th a t w hen it com es to w ithd raw al reactions, C ym balta is one of the b e s t an tidepressan ts w ith a low rate of w ithd raw al side effects and therefore relatively little difficulty getting off the d ru g w hen, in fact, the opposite is true: C ym balta is one of the w o r s t . This language in C ym balta 's label m isrepresents Lilly 's ow n clinical data. As described in Section 1 of th is report, in Lilly's six short-term , double-blind placebo controlled C ym balta studies,
35
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 55 of 246 PageID# 8285

involving a com bined total of 870 patients, 44% of patien ts stopp ing C ym balta experienced w ithd raw al side effects.110 In Lilly 's year-long, open label s tudy involving 1,279 patients, about 51% of patien ts experienced C ym balta w ithd raw al sym ptom s.111 As explained earlier in this report, the true percentage is likely m uch h igher since Lilly d id no t system atically assess C ym balta w ithd raw al side effects in the studies. C ym balta increased the risk of som e w ithdraw al sym ptom s, for exam ple nausea, as m uch as 23fold by com parison w ith placebo. The 1% to 2% figures in Lilly 's C ym balta label fail to convey the m agn itude and seriousness of the p rob lem of C ym balta w ithdraw al. In contrast to Lilly 's C ym balta label in the U nited States, in Europe, Lilly 's C ym balta label inform s doctors and patien ts th a t in the com pany 's studies "approx im ately 45% of patien ts trea ted w ith C ym balta" repo rted w ithd raw al side effects.112 Lilly 's U nited States label fails to inform doctors in th is country tha t C ym balta is one of the w orst an tidepressan ts w ith h igh rates of w ithd raw al reactions docum ented in Lilly 's ow n studies, one of the m ost difficult an tidepressan ts to com fortably and safely taper off.
W ith regard to the severity of C ym balta w ithdraw al, C ym balta 's labeling fails to indicate h o w severe C ym balta w ithdraw al can be. Specifically, in L illy 's six short-term , placebo-controlled C ym balta studies, am ong the 44% of patien ts w ho experienced w ithd raw al sym ptom s, 50.6% of w ithd raw al side effects w ere m odera te and 9.6% w ere severe.113 In Lilly 's larger year-long, open-label study , am ong the rough ly 51% of patien ts experiencing w ithd raw al side effects, approxim ately 46% of the side effects w ere m oderate and 17% w ere severe.114 It is im portan t to note th a t the FD A 's black box and accom panying w arn ings regard ing an tidepressan t-induced suicidality state tha t dosage changes, including tapering or stopp ing the d rugs, are am ong the m ost vulnerable tim es for an tidepressan ts to induce suicidal th ink ing an d behavior. Physical sym ptom s of w ithdraw al, such as severe nausea, vom iting, disequilibrium , or electric shock-like sensations in the b ra in can be incapacitating and m ake patien ts bed-ridden . Lilly 's label fails to explain th a t severe w ithd raw al reactions can be debilita ting or even life-threatening .
R egarding the du ra tio n of C ym balta w ithdraw al, C ym balta 's labeling does n o t p rovide any indication of the d u ra tio n patien ts can expect to experience w ithd raw al sym ptom s follow ing the d iscontinuation of Cym balta. In Lilly 's short-term , placebo-controlled C ym balta studies, 53.7% of patien ts w ho rep o rted w ithd raw al sym ptom s continued to experience w ithd raw al reactions after tw o w eeks.115 In Lilly 's longer-term , 34-week studies, 64.7% of the patien ts w ho rep o rted w ithd raw al sym ptom s continued to experience sym ptom s after tw o w eeks.116 In the year-long, open-label study , 55.2% of the patien ts w ho rep o rted w ithdraw al sym ptom s continued to experience sym ptom s after tw o w eeks.117 Since Lilly d id no t m onitor or record w ithd raw al sym ptom s beyond tw o w eeks in any of these studies, there is no indication of how long the patien ts
36
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 56 of 246 PageID# 8286

continued to experience w ithdraw al sym ptom s. W hen patien ts a ttem p t to go off an tidepressan ts w ith extrem ely short half-lives like C ym balta, seven or m ore m onths m ay be requ ired to painstak ingly taper off the drug . Lilly's label fails to inform doctors and patien ts it can be so difficult to d iscontinue Cym balta. In contrast to Lilly's C ym balta label in the U nited States, in Europe Lilly 's label acknow ledges C ym balta w ithd raw al reactions "m ay be p ro longed (2-3 m onths or m ore)."118
T hroughou t the years, the C ym balta label also stated tha t:119
D uring m arketing of o th e r SSRIs and SNRIs (Serotonin and N orep inephrine R euptake Inhibitors), there have been s p o n ta n e o u s
reports of adverse events occurring u p o n d iscon tinuation of these d rugs, particu larly w hen abrup t, including the following: dysphoric m ood, irritability, agitation, dizziness, sensory d isturbances (e.g., paresthesias such as electric shock sensations), anxiety, confusion, headache, lethargy, em otional lability, insom nia, hypom ania , tinn itus, and seizures. A l t h o u g h th e s e e v e n t s
a re g e n e r a l l y s e l f - l im i t in g , s o m e h a v e b e e n r e p o r te d to be se v e re .
Patients shou ld be m onito red for these sym ptom s w hen d iscontinuing trea tm en t w ith Cym balta. A g radua l reduction in the dose ra th e r th an ab ru p t cessation is recom m ended w henever possible. If intolerable sym ptom s occur follow ing a decrease in the dose or u p o n d iscon tinuation of treatm ent, then resum ing the p reviously prescribed dose m ay be considered. Subsequently, the physician m ay continue decreasing the dose b u t at a m ore g radual rate [em phasis added].
Lilly 's use of "o ther SSRIs or SNRIs" is m isleading because it suggests an tidepressan ts are m ore or less the sam e w ith regard to w ithd raw al reactions, and th a t C ym balta is just ano ther typical SSRI or SNRI, w hen this is n o t the case. A n tidepressan ts are no t the same; they vary w idely in their half-lives and likelihood of causing w ithdraw al reactions. W ith its extrem ely short half-life an d h igh rates of w ithd raw al reactions, C ym balta is an outlier, one of the w orst. D octors an d patien ts need to be p roperly inform ed of the risk of C ym balta w ithd raw al so they u n d e rs tan d it is one of the m ost difficult an tidepressan ts to get off. Lilly 's use of "generally self-lim iting" suggests w ithd raw al is uncom m on and th a t severe reactions are rare, ne ither of w hich is true. In addition , Lilly's statem ent th a t there have been "spontaneous" reports u p o n d iscon tinuation "d u rin g m arketing" of these "o ther SSRIs or SNRIs" m isleadingly obscures the m ore specific da ta from Lilly 's ow n C ym balta studies. In add ition to the
37
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 57 of 246 PageID# 8287

high rates of patien ts w ho rep o rted w ithd raw al side effects in L illy 's C ym balta studies, a h igh percentage w ere severe.
Lilly 's inform ation on gradually reducing the dose is also inadequate. Lilly fails to m ention th a t patien ts w ho inadverten tly m iss just one dose of C ym balta m ay experience w ithd raw al reactions (w hich Lilly 's E uropean label again discloses); fails to p rov ide recom m ended dosage reductions; fails to explain dosage reductions need to be custom ized to the ind iv idual patien t; fails to m ention th a t even w ith a g radua l taper, patien ts m ay experience severe w ithd raw al reactions because of C ym balta 's extrem ely short half-life; and again fails to inform doctors an d patien ts tha t C ym balta is one of the w orst offenders.120 W hile Lilly's label recom m ends g radually tapering Cym balta, Lilly only m anufactures an d m akes available 20, 30, and 60 m illigram delayed release capsules.121 Lilly 's label explicitly instructs patients: "C ym balta shou ld be sw allow ed w hole and should n o t be chew ed or crushed no r should the contents be sprink led on food or m ixed w ith liqu ids."122 So, for a pa tien t com plying w ith the p ro d u c t labeling, the only available taper reg im en w ou ld involve a m in im um dose of 20 m illigram s a day, w ith no sm aller doses available. In add ition to a lim ited selection of C ym balta dosages, Lilly has never given physicians or consum ers any specific instructions on the appropria te tap er reg im en and has never w arn ed th a t a pa tien t m igh t still experience severe w ithd raw al even w ith a painstak ing ly g radual taper regim en. Lilly 's pill design and its generalized w arnings, especially in ligh t of the com pany 's clinical trial da ta on C ym balta, is grossly inadequate.
Since C ym balta 's en try onto the U nited States m arket, in each and every version of the d ru g 's label, Lilly m isrepresen ted or failed to adequately inform prescrib ing physicians and patien ts in th is country about the frequency, severity, and d u ra tio n of w ithdraw al sym ptom s th a t can be caused by the d iscon tinuation of Cym balta. Lilly's label contains m aterial m isstatem ents re la ted to the frequency, severity, and d u ra tio n of Cym balta w ithdraw al. Lilly 's m isrepresen tations and om issions m ake it im possible for any patien t or physician to m ake an in form ed decision abou t the appropria teness of taking or prescrib ing Cym balta.
38
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 58 of 246 PageID# 8288

S ection 7: L illy 's c o n d u c t
Lilly 's label m inim izing the risk of C ym balta w ithdraw al is particu larly egregious given th a t in the mid-1990s, w hile m arketing Prozac, Lilly m oun ted a cam paign to call a tten tion to Paxil, in particu lar, as one of the w orst offenders w hen it comes to an tidepressan t w ith d raw al.123 In the late 1980s, Lilly in troduced Prozac as the first of the new er an tidepressan ts in th is country. By the mid-1990s, Paxil and Zoloft h a d entered the m arket and w ere a th rea t to Prozac sales. W ith its cam paign to call a tten tion to an tidepressan t w ithdraw al, Lilly sough t a m arket advan tage for Prozac as an an tidepressan t w ith a long half-life and therefore a relatively low frequency of w ithd raw al reactions. Then in 2004, Lilly d id an about face, m inim izing and obscuring the risk w ith its new an tidepressan t w ith an extrem ely short half-life, Cym balta.
In the 1990s, Lilly fu n d ed the s tudy d iscussed earlier in th is rep o rt com paring w ithd raw al reactions in patien ts tak ing Prozac against its com petitors at the tim e, Paxil and Zoloft.124 The s tudy w as h eaded by Dr. Jerold Rosenbaum , a p a id Lilly consultan t.125 In the study, the patien ts ' an tidepressan ts w ere stopped ab rup tly for five to eight days and w ithd raw al side effects w ere system atically m onito red using a sym ptom checklist ra ting scale.126 R osenbaum and one of his colleagues pub lished the s tudy w ith three Lilly em ployees in 1998 in the journal B io lo g ic a l P s y c h ia t r y .127 The conclusion of the study w as th a t Paxil h ad the h ighest level of w ithdraw al, Zoloft to a lesser degree, and there w ere "few sym ptom s seen w ith Prozac."128 The au thors reasoned tha t Prozac d id no t cause as frequen t or severe w ithd raw al reactions as Paxil and Zoloft because Prozac h ad a substantially longer half-life th an the o ther drugs. R osenbaum subsequently becam e a public spokesperson com m enting on an tidep ressan t w ithdraw al w ith SSRI-type an tidepressan ts.129
Also in the mid-1990s, Lilly p a id for a g roup of key opin ion leader psychiatrists, so- called KOLs, to m eet at a resort in Phoenix, A rizona to d iscuss an tidepressan t w ithd raw al.130 A fter the m eeting, Lilly p rov ided financial assistance for the opin ion leaders, m any of them p rom inen t academ ic psychiatrists like R osenbaum , to publish eight papers on an tidepressan t w ithd raw al.131 The eight papers w ere pub lished in 1997 as a supp lem ent to the J o u r n a l o f C l in ic a l P s y c h ia t r y .132 The b o u n d supp lem ent w as m ailed free of charge to doctors across the country. As is typical of journal supplem ents, the papers w ere n o t peer review ed. Instead, they w ere effectively L illy-funded infom ercials w hen the com pany w as try ing to p rom ote Prozac as causing less w ithd raw al th an its com petitors.
39
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 59 of 246 PageID# 8289

In ano ther article by R osenbaum and Dr. A lan Schatzberg (both pa id Lilly consultants), the au thors po in t ou t that, in patien ts s topp ing Effexor (w hich has an extrem ely short half-life like Cym balta), w ithd raw al reactions "occur dram atically and com m only ."133
Internal GlaxoSmithKline m em os and sales tra in ing m aterials docum ent Lilly's cam paign .134 A M ay 1, 1997 GlaxoSm ithKline m em o states: "Lilly has in itiated a new cam paign focused on d iscon tinuation sym ptom s associated w ith cessation of SSRI" an tidepressan ts.135 A nother rep o rt suggests: Lilly has created a "m arketing cam paign focusing on the h igher incidence of w ithd raw al sym ptom s associated w ith Paxil com pared to Prozac" because "Lilly has seen a precip itous d ro p in their m arket share over the p ast tw o years w hile Paxil m arket share has been soaring ."136 A nd a June 5, 1997 m em o from G laxoSm ithK line's public relations firm , R uder Finn, describes the steps it is tak ing on behalf of the pharm aceutical g iant to refute "w hat R osenbaum [the pa id Lilly consultant] et al. state or allege."137 Indeed, in the late 1990s, GlaxoSmithKline w en t to considerable effort to tra in its sales force to counter L illy 's cam paign po in ting a finger at Paxil as one of the w orst offenders.138
Thus, Lilly w as aw are of the risks associated w ith an tidepressan t w ithd raw al and its relationship to a d ru g 's half-life. A nd, Lilly w as m aking an issue of an tidepressan ts w ith short half-lives being the w orst offenders w hen th is w as to the com pany 's advan tage p rom oting Prozac. Since C ym balta 's half-life is considerably shorter th an P ax il's—indeed, C ym balta 's is the second shortest after E ffexor's—Lilly m u st have recognized the risk of C ym balta w ithd raw al w as substantial com pared to o ther new er an tidepressants, as confirm ed by its ow n clinical data. H ow ever, ra ther th an being forthcom ing abou t the degree of the C ym balta risk, Lilly chose to obscure the degree of risk by using m isleading language in C ym balta 's label once the com pany w as m arketing its ow n an tidepressan t w ith an extrem ely short half-life.
In 2005, Lilly pub lished the resu lts of its C ym balta studies in the J o u r n a l o f A f f e c t i v e
D is o r d e r s in an article en titled "Sym ptom s Follow ing A b ru p t D iscontinuation of D uloxetine T reatm ent in Patients w ith M ajor D epressive D iso rder."139 The article disclosed th a t 40%-50% of patien ts s topp ing C ym balta repo rted w ithd raw al side effects.140 W hile the article acknow ledged C ym balta caused statistically significantly m ore w ithd raw al side effects th an placebo, Lilly failed to p rov ide the odds ratios and p- values show ing th a t C ym balta increased the risk of w ithd raw al side effects as m uch as 23-fold.141
A t the tim e of its publication, like m any psychiatrists, I w as n o t a subscriber to the J o u r n a l o f A f f e c t i v e D is o r d e r s (nor am I a subscriber now ) an d only becam e aw are of the article once I began to m ore closely investigate the C ym balta risk at issue in this
40
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 60 of 246 PageID# 8290

litigation. The J o u r n a l o f A f f e c t i v e D is o r d e r s is pub lished ou t of the N etherlands. A ccording to a search of the Scientific Journal Research m edical journal ranking database, in 2005 w hen Lilly pub lished the Perahia article, the J o u r n a l o f A f f e c t i v e
D is o r d e r s w as no t on the list of 87 journals ranked in the U nited States in psych iatry and m ental health , in o ther w ords, it appears readersh ip in the U nited States w as too low to m ake it onto th is list.142 Like myself, m any A m erican doctors w ou ld have been unaw are of the article, w hereas doctors are aw are of and rely on a d ru g 's label. Indeed, doctors generally rely on a d ru g 's label as the u ltim ate au thority on a d ru g 's safety and efficacy. In fact, in an instance such as this, w here a m edical journal article gives a very different im pression from a d ru g 's label, physicians generally w ou ld consider the label m ore au thorita tive th an the publication since the label is FDA approved.
In the 1990s, Lilly tried to use an tidepressan t w ithd raw al to its advan tage w hen m arketing Prozac. But since 2004, Lilly has m inim ized and obscured C ym balta w ithd raw al in its label. Lilly's C ym balta label m isleads doctors and patien ts in this country, and seriously sets back the effort to p roperly inform patien ts and the m edical com m unity of the risks of an tidepressan t w ithdraw al. It is m y u n d ers tan d in g tha t Lilly's Prozac prom otional and sales tra in ing m aterial ta rgeting Paxil and other an tidepressan ts is the subject of forthcom ing discovery. W hen I review these docum ents, I reserve the righ t to supp lem ent m y report.
All of the opinions in th is rep o rt are expressed to a reasonable degree of m edical certainty. O f course, m y opinions are subject to change based on additional discovery.
Sincerely yours,
A ttachm ents:Joseph G lenm ullen, MD
Exhibit 1 (CV)Exhibit 2 (List of D ocum ents Review ed)
1J. Glenmullen, P ro za c B a ckla sh (New York: Simon & Schuster, 2000); J. Glenmullen, T h e A n tid e p r e s s a n t
41
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 61 of 246 PageID# 8291

S o lu t io n (New York: Free Press Division of Simon & Schuster, 2005). Please note that in academic and professional journals, the chemical rather than the commercial names for drugs are typically used.For example, Cymbalta is referred to as duloxetine. When these journals are quoted in the text, for readability the well-recognized commercial names of the drugs have been substituted for their chemical names. In addition, abbreviations and shorthand commonly used in medical records have also been spelled out, again, for readability.
2 J. Maslin, "Exploring a Dark Side of Depression Remedies," T h e N e w Y o r k T im e s , June 29, 2000. Acocella,J. "The Empty Couch: What is lost when psychiatry turns to drugs?" T h e N e w Y o rker , May 8, 2000, pg.112.
3 http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/0225161bl.pdf4 Eli Lilly Clinical Study Synopses, Clinical Trials (CT) Registry ID numbers 3327A, 3327B, 4689A, 4689B,
4091A, 409IB, 4298A, 4298B, 4092.5 J. Glenmullen. P ro za c B a ck la sh . New York, NY: Simon & Schuster, 2000, pp. 119-121.6 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd e rs 2005 Dec; 89(l-3):207-12.
7 J. Glenmullen. P ro za c B a ck la sh . New York, NY: Simon & Schuster, 2000, pp. 119-121.8 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
9 J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitordiscontinuation [withdrawal] syndrome: a randomized clinical trial," B io log ica l P s y c h ia tr y
1998;44(2):77-8710 Ibid.11 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
12 P h y s ic ia n s ’ D e sk R e fe re n ce (59th ed.). Montvale, NJ: Thomson PDR, 2005, pp. 3430-3435.13 J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitor
discontinuation [withdrawal] syndrome: a randomized clinical trial," B io log ica l P s y c h ia tr y
1998;44(2):77-87; M. Fava, R. Mulroy, J. Alpert, A.A. Neirenberg, J.F. Rosenbaum, "Emergence of adverse events following discontinuation [withdrawal] of treatment with extended-release venlafaxine [Effexor]," A m e r ic a n Jo u rn a l o f P s y c h ia tr y 1997; 154(12):1760-2.
14 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation ofduloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
15 T.B. Newman, "A black box warning for antidepressants in children," N e w E n g la n d Jo u rn a l o f M e d ic in e
2004 Oct. 14;351(16):1595-1598.16 Ibid.17 In addition to statistically significant findings, there are other widely used measures for assessing
causality including the Bradford Hill criteria. R. Van Reekum , D.L. Streiner, and D.K. C onn, "Applying Bradford Hill's criteria for causation to neuropsychiatry," T h e J o u rn a l o f N e u r o p s y c h ia tr y &
C lin ic a l N e u ro sc ie n c e s August 2001;13:318-325; Hofler, "The Bradford Hill considerations on causality: a counterfactual perspective," E m e r g in g T h e m e s in E p id e m io lo g y 2005;2(11).
18 Transcript of the Joint Meeting of the Food and Drug Administration's Peripheral and Central NervousSystem Drugs Advisory Committee (PCNS) and the Psychopharmacologic Drugs Advisory Committee (PDAC), July 10, 2008.
19 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
42
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 62 of 246 PageID# 8292

duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd e rs 2005 Dec; 89(l-3):207-12.
20 Report of Dr. Roger Grimson.21 Ibid.22 Eli Lilly Clinical Study Synopses, Clinical Trials (CT) Registry ID numbers 3327A, 3327B, 4689A, 4689B,
4091A, 409IB, 4298A, 4298B, 4092.23 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
24 T.B. Newman, "A black box warning for antidepressants in children," N e w E n g la n d Jo u rn a l o f M e d ic in e
2004 Oct. 14;351(16):1595-1598.25 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
26 Report of Dr. Roger Grimson.27 Ibid.28 Ibid.29 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
30 Eli Lilly Clinical Study Synopses, Clinical Trials (CT) Registry ID numbers 3327A, 3327B, 4689A, 4689B,4091A, 409IB, 4298A, 4298B, 4092.
31 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation ofduloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
32 Report of Dr. Roger Grimson33 Ibid.34 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
35 Ibid.36 T.B. Newman, "A black box warning for antidepressants in children," N e w E n g la n d Jo u rn a l o f M e d ic in e
2004 Oct. 14;351(16):1595-1598.37 Ibid.38 J. Woodcock, R.E. Behrman, and G.J. Dal Pan, "Role of postmarketing surveillance in contemporary
medicine," A n n u a l R e v ie w o f M e d ic in e 2011;62:1-10.39 Ibid.40 B.L. Strom, Ed., P h a rm a c o e p id e m io lo g y 4th ed., England: John Wiley & Sons Ltd., 2005, p. 136; J.
Woodcock, R.E. Behrman, and G.J. Dal Pan, "Role of postmarketing surveillance in contemporary medicine," A n n u a l R e v ie w o f M e d ic in e 2011;62:1-10; D. A. Kessler, "Introducing MedWatch: a new approach to reporting medication and device adverse effects and product problems," Jo u rn a l o f th e
A m e r ic a n M e d ic a l A s s o c ia tio n (JAMA) 1993 June 2;269(21):2765-2768.41 B.L. Strom, Ed., P h a rm a c o e p id e m io lo g y 4th ed., England: John Wiley & Sons Ltd., 2005, p. 153; J.
Woodcock, R.E. Behrman, and G.J. Dal Pan, "Role of postmarketing surveillance in contemporary medicine," A n n u a l R e v ie w o f M e d ic in e 2011;62:1-10.
42 Report of CIOMS Working Group V, C u r r e n t C h a llen g es in P h a rm a co v ig ila n ce : P ra g m a tic A p p ro a c h e s ,
Geneva: Council for International Organizations of Medical Sciences, CIOMS, 2001; FDA Code of Federal Regulations (CRF), Part 21 (g), adverse reactions.
43
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 63 of 246 PageID# 8293

43 J. Woodcock, R.E. Behrman, and G.J. Dal Pan, "Role of postmarketing surveillance in contemporarymedicine," A n n u a l R e v ie w o f M e d ic in e 2011;62:1-10.
44 Ibid.45 http://www.ismp.org/46 Ibid.47 Ibid.48 Ibid.49 Ibid.50 Ibid.51 http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/cfrsearch.cfm7fF314.8052 Eli Lilly Clinical Study Synopses, Clinical Trials (CT) Registry ID numbers 3327A, 3327B, 4689A, 4689B,
4091A, 409IB, 4298A, 4298B, 4092.53 J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitor
discontinuation [withdrawal] syndrome: a randomized clinical trial," B io log ica l P s y c h ia tr y
1998;44(2):77-87; M. Fava, R. Mulroy, J. Alpert, A.A. Neirenberg, J.F. Rosenbaum, "Emergence of adverse events following discontinuation [withdrawal] of treatment with extended-release venlafaxine [Effexor]," A m e r ic a n Jo u rn a l o f P s y c h ia tr y 1997; 154(12):1760-2; A.F. Schatzberg, "Introduction: antidepressant discontinuation [withdrawal] syndrome: an update on serotonin reuptake inhibitors," Jo u rn a l o f C lin ica l P s y c h ia tr y 1997;58(suppl 7):3-4; A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, J.F. Rosenbaum, A.H. Young, J. Zajecka, "Serotonin reuptake inhibitor discontinuation [withdrawal] syndrome: hypothetical definition," Jo u rn a l o f C lin ic a l P s y c h ia tr y
1997;58(suppl 7):5-10; Schatzberg et al., "Serotonin reuptake inhibitor discontinuation [withdrawal] syndrome; M. Lejoyeux and J. Ades, "Antidepressant discontinuation [withdrawal]: a review of the literature," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):11-16; P. Haddad, "Newer antidepressants and the discontinuation [withdrawal] syndrome," J o u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):17-22; A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, J.F. Rosenbaum, A.H. Young, J. Zajecka," Possible biological mechanisms of the serotonin reuptake inhibitor discontinuation [withdrawal] syndrome," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):23-27; A.H. Young and A. Currie, "Physicians' knowledge of antidepressant withdrawal effects: a survey," Jo u rn a l o f C lin ic a l P s y c h ia tr y
1997;58(suppl 7):28-30; E.M. Kaplan, "Antidepressant noncompliance as a factor in the discontinuation [withdrawal] syndrome, Jo u rn a l o f C lin ica l P s y c h ia tr y 1997; 58(suppl 7):31-36; J.F. Rosenbaum and J. Zajecka, "Clinical management of antidepressant discontinuation [withdrawal]," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):37-40. Please note that these citations are a representative sample of studies and articles regarding antidepressant withdrawal in the medical literature. These are not meant to be an exhaustive or complete list of all the studies and articles I am familiar with and have relied upon in forming my opinions.
54 J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitordiscontinuation [withdrawal] syndrome: a randomized clinical trial," B io log ica l P s y c h ia tr y
1998;44(2):77-87; A.F. Schatzberg, "Introduction: antidepressant discontinuation [withdrawal] syndrome: an update on serotonin reuptake inhibitors," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):3-4; A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, J.F. Rosenbaum, A.H. Young, J.Zajecka, "Serotonin reuptake inhibitor discontinuation [withdrawal] syndrome: hypothetical definition," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):5-10; Schatzberg et al., "Serotonin reuptake inhibitor discontinuation [withdrawal] syndrome; M. Lejoyeux and J. Ades, "Antidepressant discontinuation [withdrawal]: a review of the literature," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):11-16; P. Haddad, "Newer antidepressants and the discontinuation [withdrawal] syndrome," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):17-22; A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, J.F. Rosenbaum, A.H. Young, J. Zajecka," Possible biological mechanisms of the serotonin
44
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 64 of 246 PageID# 8294

reuptake inhibitor discontinuation [withdrawal] syndrome," Jo u rn a l o f C lin ic a l P s y c h ia t r y
1997;58(suppl 7):23-27; A.H. Young and A. Currie, "Physicians' knowledge of antidepressant withdrawal effects: a survey," Jo u rn a l o f C lin ic a l P s y c h ia t r y 1997;58(suppl 7):28-30; E.M. Kaplan, "Antidepressant noncompliance as a factor in the discontinuation [withdrawal] syndrome, Jo u rn a l o f
C lin ic a l P s y c h ia t r y 1997; 58(suppl 7):31-36; J.F. Rosenbaum and J. Zajecka, "Clinical management of antidepressant discontinuation [withdrawal]," Jo u rn a l o f C lin ica l P s y c h ia t r y 1997;58(suppl 7):37-40.
55 J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitordiscontinuation [withdrawal] syndrome: a randomized clinical trial," B io log ica l P s y c h ia tr y
1998;44(2):77-8756 M. Fava, R. Mulroy, J. Alpert, A.A. Neirenberg, J.F. Rosenbaum, "Emergence of adverse events
following discontinuation [withdrawal] of treatment with extended-release venlafaxine [Effexor]," A m e r ic a n J o u rn a l o f P s y c h ia tr y 1997; 154(12):1760-2.
57 J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitordiscontinuation [withdrawal] syndrome: a randomized clinical trial," B io log ica l P s y c h ia tr y
1998;44(2):77-87; M. Fava, R. Mulroy, J. Alpert, A.A. Neirenberg, J.F. Rosenbaum, "Emergence of adverse events following discontinuation [withdrawal] of treatment with extended-release venlafaxine [Effexor]," A m e r ic a n J o u rn a l o f P s y c h ia tr y 1997; 154(12):1760-2.
58 P h y s ic ia n s ' D e sk R e fe re n ce (59th ed.). Montvale, NJ: Thomson PDR, 2005, pp. 3430-3435.59 J. Glenmullen, T h e A n tid e p r e s s a n t S o lu tio n (New York: Free Press Division of Simon & Schuster, 2005),
pp. 77-89.60 J. Glenmullen, T h e A n tid e p r e s s a n t S o lu tio n (New York: Free Press Division of Simon & Schuster, 2005);
http://www.ema.europa.eu/docs/en_GB/document_library/EPAR__Product_lntormation/human/000572/WC500036781 .pdf
61 F. Bogetto, S. Bellino, R.B. Revello, L. Patria, "Discontinuation [Withdrawal] syndrome in dysthymicpatients treated with selective serotonin reuptake inhibitors: a clinical investigation," C N S D ru g s
2002;16(4):273-83; P. Haddad, "The SSRI discontinuation [withdrawal] syndrome," Jo u rn a l o f
P sy c h o p h a rm a c o lo g y 1998;12(3):305-13; P.M. Haddad, "Antidepressant discontinuation [withdrawal] syndromes," D r u g S a fe ty 2001;24(3):183-97; P. Haddad, "Newer antidepressants and the discontinuation [withdrawal] syndrome," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):17-21, discussion 22; A u s tr a lia n A d v e r s e D r u g R e a c tio n s B u lle t in , "SSRIs and withdrawal syndrome," 1996;15(1).
62 F. Bogetto, S. Bellino, R.B. Revello, L. Patria, "Discontinuation [withdrawal] syndrome in dysthymicpatients treated with selective serotonin reuptake inhibitors: a clinical investigation," C N S D ru g s
2002;16(4):273-83; M. Lejoyeux, J. Ades, "Antidepressant discontinuation! withdrawal ]: a review of the literature," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(7):ll-5,discussion 16; J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitor discontinuation [withdrawal] syndrome: a randomized clinical trial," B io lo g ica l P s y c h ia tr y 1998;44(2):77-87; A.F. Schatzberg, "Antidepressant discontinuation [withdrawal] syndrome: an update on serotonin reuptake inhibitors," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(7):3-4; J. Zajecka, K.A. Tracy, S. Mitchell, "Discontinuation [Withdrawal] symptoms after treatment with serotonin reuptake inhibitors: a literature review," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(7):291-7.
63 J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitordiscontinuation [withdrawal] syndrome: a randomized clinical trial," B io log ica l P s y c h ia tr y
1998;44(2):77-8764 J. Glenmullen, T h e A n tid e p r e s s a n t S o lu tio n (New York: Free Press Division of Simon & Schuster, 2005).65 Ibid, see p. 3566 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005
45
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 65 of 246 PageID# 8295

Dec; 89(l-3):207-12.67http://www.ema.europa.eu/docs/en_GB/document_library/EPAR__Product_Information/human/000572AVC500036781.pdf68 F. Benazzi, "Venlafaxine [Effexor] withdrawal symptoms," Canadian Journal of Psychiatry
1996;41(7):487.69 J. Glenmullen, P ro za c B ackla sh (New York: Simon & Schuster, 2000)70 J. Glenmullen, T h e A n tid e p r e s s a n t S o lu tio n (New York: Free Press Division of Simon & Schuster, 2005)71 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
72 Ibid.73 Pyke RE, "Paroxetine [Paxil] withdrawal syndrome," A m e r ic a n J o u rn a l o f P s y c h ia tr y 1995; 152:149-50;
N.J. Keuthen, P. Cyr, J.A. Ricciardi, W.E. Minichiello, M.L. Buttolph, M.A. Jenike, "Medication withdrawal symptoms in obsessive-compulsive disorder patients treated with paroxetine [Paxil]," Jo u rn a l o f C lin ic a l P sy c h o p h a rm a c o lo g y 1994;14(3):206-7.
74 A. Farah, T.E. Lauer, "Possible venlafaxine [Effexor] withdrawal syndrome," A m e r ic a n J o u rn a l o f
P s y c h ia tr y 1996;153(4):576.75 J. Glenmullen, T h e A n tid e p r e s s a n t S o lu tio n (New York: Free Press Division of Simon & Schuster, 2005)76 P h y s ic ia n s ' D e sk R e fe re n ce (59th ed.). Montvale, NJ: Thomson PDR, 2005, pp. 3430-3435.77 E. Richelson, "Pharmacology of antidepressants," M a y o C lin ic P ro ceed in g s 2001; 76:511-27; Lane,
"Withdrawal symptoms after discontinuation of selective serotonin reuptake inhibitors (SSRIs)"; A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, J.F. Rosenbaum, A.H. Young, J. Zajecka, "Possible biological mechanisms of the serotonin reuptake inhibitor discontinuation [withdrawal] syndrome. Discontinuation Consensus Panel," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997; 58(suppl 7):23-7.
78 K. P. Lesch, C.S. Aulakh, B.L. Wolozin, T. J. Tolliver, J.L. Hill, D.L. Murphy, "Regional brain expressionof serotonin transporter mRNA and its regulation by reuptake inhibiting antidepressants," M o le c u la r
B ra in R esea rch 1993; 73:31-5; J. Glenmullen, P ro za c B acklash (New York: Simon & Schuster, 2000), p. 94.79 A. B. Hill, "The Environment and Disease: Association or Causation?" P ro ceed in g s o f th e R o y a l S o c ie ty o f
M e d ic in e , Section on Occupational Medicine, January 14,1965 meeting; Van Reekum R, Streiner DL, Conn DK, "Applying Bradford Hill's Criteria for Causation to Neuropsychiatry," T h e J o u rn a l o f
N e u r o p s y c h ia tr y & C lin ica l N e u ro sc ie n c e s , 2001 August;13:318-325; Hofler, "The Bradford Hill Considerations on Causality: A Counterfactual Perspective," E m e r g in g T h e m e s in E p id e m io lo g y 2005; 2( 11)
80 Van Reekum R, Streiner DL, Conn DK, "Applying Bradford Hill's Criteria for Causation toNeuropsychiatry," T h e J o u rn a l o f N e u r o p s y c h ia tr y & C lin ica l N e u ro sc ie n c e s , 13:318-325, August 2001; Hofler, "The Bradford Hill Considerations on Causality: A Counterfactual Perspective," E m e r g in g
T h e m e s in E p id e m io lo g y 2005; 2(11).81 Van Reekum R, Streiner DL, Conn DK, "Applying Bradford Hill's Criteria for Causation to
Neuropsychiatry," T h e J o u rn a l o f N e u r o p s y c h ia tr y & C lin ica l N e u ro sc ie n c e s , 2001 August;13:318-325.82 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12; Report of Dr. Roger Grimson
83 Ibid.84 Ibid.85 Ibid.86 Ibid.87 Ibid.88 Ibid.
46
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 66 of 246 PageID# 8296

89 Ibid.90 http://www.ismp.org/91 J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitor
discontinuation [withdrawal] syndrome: a randomized clinical trial," B io log ica l P s y c h ia tr y
1998;44(2):77-8792 P h y s ic ia n s ' D e sk R e fe re n ce (59th ed.). Montvale, NJ: Thomson PDR, 2005, pp. 3430-3435.93 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
94 Ibid.95 Ibid.96 Center for Drug Evaluation and Research, Food and Drug Administration, Department of Health and
Human Services, "Guideline for the Format and Content of the Clinical and Statistical Sections of an Application," July 1988, pp. 36-38.
97 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation ofduloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
98 Ibid.99 http://www.accessdata.fda.gov/drugsatfda_docsAabel/2004/214271bl.pdf100 P h y s ic ia n s ' D e sk R e fe re n ce (59th ed.). Montvale, NJ: Thomson PDR, 2005, pp. 3430-35.101 P h y s ic ia n s ' D e sk R e fe re n ce (62th ed.). Montvale, NJ: Thomson PDR, 2008, pp. 1791-98.102 P h y s ic ia n s ' D e sk R e fe re n ce (63rd ed.). Montvale, NJ: Thomson PDR, 2009, pp. 1801-810.103 P h y s ic ia n s ' D e sk R e fe re n ce (66th ed.). Montvale, NJ: Thomson PDR, 2012, pp. 1602-612.104 http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-
_Product_Information/human/000572/WC500036781.pdf105 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A f fe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12; J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitor discontinuation [withdrawal] syndrome: a randomized clinical trial," B io log ica l P s y c h ia tr y 1998;44(2):77-87.
106 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation ofduloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
107 Ibid.108 Ibid.109 J. Glenmullen, T h e A n t id e p r e s s a n t S o lu tio n (New York: Free Press Division of Simon & Schuster, 2005).110 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
111 Ibid.112 http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-
_Product_Information/human/000572/WC500036781.pdf113 D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
114 Ibid.115 Ibid.116 Ibid.
47
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 67 of 246 PageID# 8297

117 Ibid.118 http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-
_Product_Information/human/000572/WC500036781.pdf119 P h y s ic ia n s ' D e sk R e fe re n ce (59th ed.). Montvale, NJ: Thomson PDR, 2005, pp. 3430-3435.120 Ibid; http://www.accessdata.fda.gov/drugsatfda_docs/label/2004/214271bl.pdf; P h y s ic ia n s ' D e sk
R e fe re n ce (62th ed.). Montvale, NJ: Thomson PDR, 2008, pp. 1791-98; P h y s ic ia n s ' D e sk R e fe re n ce (63rd ed.). Montvale, NJ: Thomson PDR, 2009, pp. 1801-810; P h y s ic ia n s ' D e sk R e fe re n ce (66th ed.). Montvale, NJ: Thomson PDR, 2012, pp. 1602-612.
121 Ibid.122 Ibid123 J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitor
discontinuation [withdrawal] syndrome: a randomized clinical trial," B io log ica l P s y c h ia tr y
1998;44(2):77-87; A.F. Schatzberg, "Introduction: antidepressant discontinuation [withdrawal] syndrome: an update on serotonin reuptake inhibitors," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):3-4; A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, J.F. Rosenbaum, A.H. Young, J. Zajecka, "Serotonin reuptake inhibitor discontinuation [withdrawal] syndrome: hypothetical definition," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):5-10; Schatzberg et al., "Serotonin reuptake inhibitor discontinuation [withdrawal] syndrome; M. Lejoyeux and J. Ades, "Antidepressant discontinuation [withdrawal]: a review of the literature," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):11-16; P. Haddad, "Newer antidepressants and the discontinuation [withdrawal] syndrome," Jo u rn a l o f C lin ica l P s y c h ia tr y 1997;58(suppl 7):17-22; A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, J.F. Rosenbaum, A.H. Young, J. Zajecka," Possible biological mechanisms of the serotonin reuptake inhibitor discontinuation [withdrawal] syndrome," Jo u rn a l o f C lin ic a l P s y c h ia tr y
1997;58(suppl 7):23-27; A.H. Young and A. Currie, "Physicians' knowledge of antidepressant withdrawal effects: a survey," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):28-30; E.M. Kaplan, "Antidepressant noncompliance as a factor in the discontinuation [withdrawal] syndrome, Jo u rn a l o f
C lin ic a l P s y c h ia tr y 1997; 58(suppl 7):31-36; J.F. Rosenbaum and J. Zajecka, "Clinical management of antidepressant discontinuation [withdrawal]," Jo u rn a l o f C lin ica l P s y c h ia tr y 1997;58(suppl 7):37-40;123 SmithKlineBeecham (which later merged and became GlaxoSmithKline) memo to the Paxil Selling Team entitled "Discontinuation Syndrome," May 1,1997; SmithKlineBeecham "Business Plan Guide: A marketing/sales guide to help you tailor your territory business plan," Cycle 2,1997: December 1, 1997-May 31,1998; Ruder Finn memo entitled "Discontinuation," June 5,1997; SmithKlineBeecham report on Paxil "Safety Review of Discontinuation [Withdrawal] Symptoms" by Lisa Howell, Tamara Pedgrift, Julie Nash, Dr. R.W. Morris, and Dr. R. Kumar, March 1997; SmithKlineBeecham "Business Plan Guide;" SmithKlineBeecham company sales training guide; GlaxoSmithKline, "ACES: A Continuing Education System. Module III. Paxil;" SmithKlineBeecham Report on Paxil "Safety Review of Discontinuation [Withdrawal] Symptoms;" GlaxoSmithKline guide entitled "Central Strategy," 1997.
124 J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitordiscontinuation [withdrawal] syndrome: a randomized clinical trial," B io log ica l P s y c h ia tr y
1998;44(2):77-87125 Ibid; Schatzberg et al., "Serotonin reuptake inhibitor [Prozac-type drug] discontinuation [withdrawal]
syndrome," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7). See the discussion at the end of the paper. This is one of eight papers published by the participants at a Lilly-funded meeting of "experts" to discuss the "antidepressant discontinuation syndrome" at a resort in Phoenix, Arizona. In the discussion following the paper, Rosenbaum announces the Lilly-funded research that was already underway.
126 Ibid.
48
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 68 of 246 PageID# 8298

127 J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs, "Selective serotonin reuptake inhibitordiscontinuation [withdrawal] syndrome: a randomized clinical trial," B io log ica l P s y c h ia tr y
1998;44(2):77-87128 Ibid.129 S. Fried, "Addicted to anti-^depressants? The controversy over a pill millions of us are taking,"
G la m o u r , April 2003, pp. 178-80, 262; M. Duenwald, "Flow to stop depression medications: very slowly," T h e N e w Y o r k T im e s , May 25, 2004, Science section.
130 Jo u rn a l o f C lin ic a l P s y c h ia tr y , 1997;58(suppl 7): see inside cover for statement of Lilly sponsorship.131 A.F. Schatzberg, "Introduction: antidepressant discontinuation [withdrawal] syndrome: an update on
serotonin reuptake inhibitors," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):3-4; A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, J.F. Rosenbaum, A.H. Young, J. Zajecka, "Serotonin reuptake inhibitor discontinuation [withdrawal] syndrome: hypothetical definition," Jo u rn a l o f C lin ica l
P s y c h ia tr y 1997;58(suppl 7):5-10; Schatzberg et al., "Serotonin reuptake inhibitor discontinuation [withdrawal] syndrome; M. Lejoyeux and J. Ades, "Antidepressant discontinuation [withdrawal]: a review of the literature," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):11-16; P. Haddad, "Newer antidepressants and the discontinuation [withdrawal] syndrome," Jo u rn a l o f C lin ic a l P s y c h ia tr y
1997;58(suppl 7):17-22; A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, J.F. Rosenbaum, A.H. Young, J. Zajecka," Possible biological mechanisms of the serotonin reuptake inhibitor discontinuation [withdrawal] syndrome," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):23-27; A.H. Young and A. Currie, "Physicians' knowledge of antidepressant withdrawal effects: a survey,"Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):28-30; E.M. Kaplan, "Antidepressant noncompliance as a factor in the discontinuation [withdrawal] syndrome, Jo u rn a l o f C lin ica l P s y c h ia tr y 1997; 58(suppl 7):31-36; J.F. Rosenbaum and J. Zajecka, "Clinical management of antidepressant discontinuation [withdrawal]," Jo u rn a l o f C lin ic a l P s y c h ia tr y 1997;58(suppl 7):37-40.
132 Ibid.133 Schatzberg et al., "Serotonin reuptake inhibitor discontinuation [withdrawal] syndrome." See
discussion at the end of the paper.134 SmithKlineBeecham (which later merged and became GlaxoSmithKline) memo to the Paxil Selling
Team entitled "Discontinuation Syndrome," May 1,1997; SmithKlineBeecham "Business Plan Guide: A marketing/sales guide to help you tailor your territory business plan," Cycle 2,1997: December 1, 1997-May 31,1998; Ruder Finn memo entitled "Discontinuation," June 5,1997; SmithKlineBeecham report on Paxil "Safety Review of Discontinuation [Withdrawal] Symptoms" by Lisa Howell, Tamara Pedgrift, Julie Nash, Dr. R.W. Morris, and Dr. R. Kumar, March 1997; SmithKlineBeecham "Business Plan Guide;" SmithKlineBeecham company sales training guide; GlaxoSmithKline, "ACES: A Continuing Education System. Module III. Paxil;" SmithKlineBeecham Report on Paxil "Safety Review of Discontinuation [Withdrawal] Symptoms;" GlaxoSmithKline guide entitled "Central Strategy," 1997.
135 SmithKlineBeecham (which later merged and became GlaxoSmithKline) memo to the Paxil SellingTeam entitled "Discontinuation Syndrome," May 1,1997.
136 SmithKlineBeecham (which later merged and became GlaxoSmithKline) "Business Plan Guide: Amarketing/sales guide to help you tailor your territory business plan," Cycle 2,1997: December 1, 1997-May 31,1998.
137 Ruder Finn memo entitled "Discontinuation," June 5,1997.138 SmithKlineBeecham (which later merged and became GlaxoSmithKline) report on Paxil "Safety
Review of Discontinuation [Withdrawal] Symptoms" by Lisa Howell, Tamara Pedgrift, Julie Nash, Dr. R.W. Morris, and Dr. R. Kumar, March 1997; SmithKlineBeecham "Business Plan Guide;" SmithKlineBeecham company sales training guide; GlaxoSmithKline, "ACES: A Continuing Education System. Module III. Paxil;" SmithKlineBeecham Report on Paxil "Safety Review of
49
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 69 of 246 PageID# 8299

139
140
141
142
Discontinuation [Withdrawal] Symptoms;" GlaxoSmithKline guide entitled "Central Strategy," 1997. D.G. Perahia, D.K. Kajdasz, D. Desaiah, P.M. Haddad, "Symptoms following abrupt discontinuation of
duloxetine treatment in patients with major depressive disorder," Jo u rn a l o f A ffe c t iv e D iso rd ers 2005 Dec; 89(l-3):207-12.
Ibid.Ibid.SCImago (2007) SJR - SCImago Journal & Country Rank, Retrieved July 17, 2013 from
http://www.scimagojr.com.
50
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 70 of 246 PageID# 8300

EXHIBIT 1
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 71 of 246 PageID# 8301

JOSEPH GLENMULLEN, M.D. C u rricu lu m V itae
Academic Appointments
1988 to present: Clinical Instructor in Psychiatry, Harvard Medical School, in the Department of Psychiatry, Cambridge Hospital, Cambridge, MA
1988-89: Associate Director, Medical Student Education, Cambridge Hospital/Harvard Medical School, Cambridge, MA
1987-89: Instructor, Psychiatry 700 Course, Harvard Medical School
Clinical Practice
Clinical P ractice
1986 to present: Private practice in Harvard Square, Cambridge, MA1988 to 2008: Psychiatrist, Harvard Law School Health Services, Cambridge, MA
Forensic P ractice
2001 to present: Expert witness and forensic consulting 2002-present: Member, Program in Psychiatry and the Law, Harvard Medical
School
Teaching and Awards
Teaching1988-present: Supervision of social work interns, psychology fellows, and
psychiatry residents at the Cambridge Hospital/Harvard Medical School.
A w ards:
May, 2001: Annual Achievement Award in Medicine, American College forAdvancement in Medicine (ACAM), and delivered the keynote address, the Linus Pauling Lecture, at ACAM's annual convention.
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 72 of 246 PageID# 8302

Education and Training
Education
1984: MD, Harvard Medical School, Boston, MA1972: BA, magna cum laude, Brown University, Providence, RI
P ostdoctoral T ra in in g
1987-88: Psychiatry Fellow, Harvard University Health Services, Cambridge, MA
1987-88: Chief Resident, Outpatient Department, Department of Psychiatry, Cambridge Hospital/Harvard Medical School, Cambridge, MA
1986-88: Residency, Department of Psychiatry, Cambridge Hospital/Harvard Medical School, Cambridge, MA
1984-85: Internship, Department of Medicine, Cambridge Hospital/Harvard Medical School, Cambridge, MA
Board C ertification
1990: Board certified in psychiatry by the American Board of Psychiatry and Neurology
Licensure
1985 to present: Medical License, Massachusetts Board of Registration in Medicine
Board Membership/Professional Organizations
2008-present: Member, Board of Directors, Boston Chapter of the American Foundation for Suicide Prevention
2008-present: Member, American Association of Suicidology
Bibliography
T.J. Moore, C.D. Furberg, J. Glenmullen, J.T. Maltsberger, and S. Singh, Suicidal Behavior and Depression in Smoking Cessation, PLoS O N E Nov 2011;6(11)
Moore TJ, Glenmullen J, Furberg CD, Prescription Drugs Associated withReports of Violence Towards Others, PLoS O ne, 2010 Dec 15;5(12): el5337
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 73 of 246 PageID# 8303

Moore TJ, Glenmullen J, Furberg CD, Thoughts and Acts of Aggression/Violence Toward Others Reported in Association with Varenicline, A n n a ls o f P harm acotherapy, 2010 Sep;44(9):1389-94
Wanzer, Sidney and Glenmullen, Joseph. To D ie W ell: Y ou r R ig h t to Com fort,
Calm , and Choice in the L ast D a ys o f Life. New York: Perseus Books Group, 2007.
Glenmullen, Joseph. The A n tid ep re ssa n t Solution: A S tep -b y -S tep G uide to
O verco m in g A n tid ep re ssa n t W ith draw al, D ependence, and " A d d ic tio n ." New York: Free Press (division of Simon & Schuster), 2005
Glenmullen, Joseph. P rozac Backlash: O vercom in g the D an gers o f P rozac, Zoloft,
P axil and O th er A n tid ep ressa n ts w ith Safe, E ffective A lte rn a tive s . New York: Simon & Schuster, 2000
Glenmullen, Joseph. Sexual M ysteries: Tales o f P sych o th erapy with a Foreword by Robert Coles. New York: Harper Collins, 1993 (hardcover). Cambridge, MA: Orbit Publishing, 2000 (paperback).
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 74 of 246 PageID# 8304

EXHIBIT 2
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 75 of 246 PageID# 8305

REFERENCES:
Approved labeling for Cymbalta:August, 2006June, 2005 (reprinted in the 2006 PDR)June, 2006 (reprinted in the 2007 PDR)June, 2007 (reprinted in the 2008 PDR)June, 2008 (reprinted in the 2009 PDR)February, 2009 (reprinted in the 2010 PDR)March, 2010 (reprinted in the 2011 PDR)May, 20112 (reprinted in the 2012 PDR)
FDA, Approval Package at:http://www.accessdata.fda.gov/drugsatfda docs/nda/2004/021427 sOOO Cymbalta AdminCor res.pdf
FDA, Drug Approval Package for Cymbalta (Duloxetine Hydrochloride) Capsules at: http://www.accessdata.fda.gov/drugsatfda docs/nda/2004/021427 sOOO Cvmbalta.cfm
FDA, Historical Information on Duloxetine hydrochloride (marketed as Cymbalta) at: http://www.fda.gov/Drugs/DrugSafetv/PostmarketDrugSafetvInformationforPatientsandProvid ers/ucml 14970.htm
Lilly Trials, Lilly Clinical Study Results at: http://www.1i11vtrials.com/results/Cvmbalta.pdf
J.F. Rosenbaum, M. Fava, S.L. Hoog, R.C. Ascroft, W.B. Krebs,“Selective serotonin reuptake inhibitor discontinuation [withdrawal] syndrome: a randomized clinical trial,”Biological Psychiatry 1998;44(2):77-87;
A.F. Schatzberg,“Introduction: antidepressant discontinuation [withdrawal] syndrome: an update on serotonin reuptake inhibitors,”Journal of Clinical Psychiatry 1997;58(suppl 7):3-4;
A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, J.F. Rosenbaum, A.H. Young, J. Zajecka,“Serotonin reuptake inhibitor discontinuation [withdrawal] syndrome: hypothetical definition,” Journal of Clinical Psychiatry 1997;58(suppl 7):5—10;
Schatzberg et al., “Serotonin reuptake inhibitor discontinuation [withdrawal] syndrome; M. Lejoyeux and J. Ades, “Antidepressant discontinuation [withdrawal]: a review of the literature,” Journal of Clinical Psychiatry 1997;58(suppl 7): 11-16;
P. Haddad,“Newer antidepressants and the discontinuation [withdrawal] syndrome,”Journal of Clinical Psychiatry 1997;58(suppl 7): 17-22;
A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, J.F. Rosenbaum, A.H. Young, J. Zajecka
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 76 of 246 PageID# 8306

“Possible biological mechanisms of the serotonin reuptake inhibitor discontinuation [withdrawal] syndrome,”Journal of Clinical Psychiatry 1997;58(suppl 7):23-27;
A.H. Young and A. Currie,“Physicians’ knowledge of antidepressant withdrawal effects: a survey,”Journal of Clinical Psychiatry 1997;58(suppl. 7):28-30;
E.M. Kaplan, “Antidepressant noncompliance as a factor in the discontinuation [withdrawal] syndrome”Journal of Clinical Psychiatry 1997; 58(suppl 7):31-36;
J.F. Rosenbaum and J. Zajecka,“Clinical management of antidepressant discontinuation [withdrawal],”Journal of Clinical Psychiatry 1997;58(suppl 7):37-40; 123
SmithKlineBeecham (which later merged and became GlaxoSmithKline) memo to the Paxil Selling Team entitled “Discontinuation Syndrome,”May 1, 1997;
SmithKlineBeecham“Business Plan Guide: A marketing/sales guide to help you tailor your territory business plan,” Cycle 2, 1997: December 1, 1997-May 31, 1998;
Ruder Finn memo entitled “Discontinuation,”June 5, 1997;
SmithKlineBeecham report on Paxil “Safety Review of Discontinuation [Withdrawal] Symptoms” by Fisa Howell, Tamara Pedgrift, Julie Nash, Dr. R.W. Morris, and Dr. R. Kumar, March 1997;
SmithKlineBeecham “Business Plan Guide;” SmithKlineBeecham company sales training guide;
GlaxoSmithKline, “ACES: A Continuing Education System. Module III. Paxil;”
SmithKlineBeecham Report on Paxil “Safety Review of Discontinuation [Withdrawal] Symptoms;” GlaxoSmithKline guide entitled “Central Strategy,”1997.
Medical Literature
J. Acocella “The Empty Couch”The New Yorker, May 8, 2000; 82-88
I. AgellUse of antidepressants by nursing mothers Br J Psychiatry. 2002 Jan; 180:85-6
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 77 of 246 PageID# 8307

K. Adam, I. Oswald“Can a Rapidly-eliminated Hypnotic Cause Daytime Anxiety?” Psychopharmac. 22 (1989) 115-119
D.O. Antonuccio, W.G. Danton, G.Y. DeNelsky, RP. Greenberg, JS. Gordon "Raising questions about antidepressants"Psychother Psychosom. 1999;68(1):3-14. Review
D.K. Ary a"Withdrawal after discontinuation of paroxetine"Aust N Z J Psychiatry. 1996 Oct;30(5):702
F.J. Ayd"Paroxetine withdrawal symptoms" Int Drug Ther NewsL 1994;29:36
Australian Adverse Drug Reactions Bulletin, Vol. 15, no. 1 (February 1996), "SSRIs and withdrawal syndrome"
RJ Baldessarini S. Nassir Ghaemi Adele C. Viguera “Commentary: Tolerance in Antidepressant Treatment”Psychother Psychosom 2002;71:177-179
RJ. Baldessarini"Risks and implications of interrupting maintenance psychotropic drug therapy" Psychother Psychosom. 1995;63(3-4): 137-41
T .C . Barr, W.K. Goodman, L.H. Price"Physical symptoms associated with paroxetine discontinuation" Am J Psychiatry. 1994 Feb; 151(2):289
A.J. Bayer, E. M. Bayer, M.S.J. Pathyl and M.J. StokerA double-blind controlled study of chlormethiazole and triazolam as hypnotics in the elderly Acta psychiatr. Scand. Suppl. 329, Vol. 73. 1986:104-11
J.E. Bekelman, AB, Y. Li, MPhil, C.P Gross, MD“Scope and Impact of Financial Conflicts of Interest in Biomedical Research A Systematic Review”JAMA, January 22/29, 2003 - Vol 289, No. +
N. Bel, F. Artigas"In vivo effects of the simultaneous blockade of serotonin and norepinephrine transporters on serotonergic function. Microdialysis studies."J Pharmacol Exp Ther. 1996 Sep;278(3): 1064-72
L. Belloeuf, e. Le Jeunne, F.e. Hugues "Paroxetine withdrawal syndrome"
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 78 of 246 PageID# 8308

Ann Med Interne (Paris) 2000 Apr; 151 Suppl A:A52-3
F. Benazzi"Nefazodone withdrawal symptoms" Can J Psychiatry. 1998 Mar;43(2): 194-5
F. Benazzi"Sertraline discontinuation syndrome presenting with severe depression and compulsions."Biol Psychiatry. 1998 [un 15;43(12):929-30
F. Benazzi" S S R I discontinuation syndrome related to fluvoxamine." J Psychiatry Neurosci. 1998 Mar;23(2):94
F. Benazzi"Venlafaxine withdrawal symptoms." Can J Psychiatry. 1996 Sep;41(7):487
Serotonin Clearance In Vivo Is Altered to a Greater Extent by Antidepressant-Induced Down regulation of the Serotonin Transporter than by Acute Blockade of this Transporter”S. Benmansour, W.A. Owens, M. Cecchi, D.A. Morilak, A. Frazer The Journal of Neuroscience, August 1, 2002, 22(15):6766-6772
M.J. BerberFINISH: remembering the discontinuation syndrome. Flu-like symptoms, Insomnia, Nausea, Imbalance, Sensory disturbances, and Hyperarousal (anxiety/agitation)J Clin Psychiatry. 1998 May; 59(5):255
C. S. Berlin"Fluoxetine withdrawal symptoms."J Clin Psychiatry. 1996 Feb;57(2):93-4
S. Bhaumik, H.J. Wild gust "Letter to the editor."Human Psychopharmacology 1996;11:337-8 Biological Therapies in Psychiatry "Paroxetine Withdrawal: Behavioral Effects"
D. W. Black, R. Wesner, J. Gabel"The abrupt discontinuation of flu voxamine in patients with panic disorder." J Clin Psychiatry. 1993 Apr;54(4): 146-9
K. Black, C. Shea, S. Dursun, S. Kutcher"Selective serotonin reuptake inhibitor discontinuation syndrome: proposed diagnostic criteria"
J Psychiatry Neurosci. 2000 May;25(3):255-61
M. Bloch, S.V. Stager, A.R Braun, D.R Rubinow"Severe psychiatric symptoms associated with paroxetine withdrawal" Lancet. 1995 Jul 1;346(8966):57
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 79 of 246 PageID# 8309

T. Bodenheimer, M.D.“UNEASY ALLIANCE - Clinical Investigators and the Pharmaceutical Industry”The New England Journal of Medicine, Volume 342 Number 20: 1539-1544
Blomgren"SSRI Dose Interruption Study." New Research Program and Abstracts of the 150th Annual Meeting of the American Psychiatric Association, May 20, 1997 in San Diego, California.
F. Bogetto, S. Bellino, RB. Revello, L. Patria"Discontinuation syndrome in dysthymic patients treated with selective serotonin reuptake inhibitors: a clinical investigation"CNS Drugs. 2002;16(4):273-83
P. Boksa"Antidepressant use during pregnancy"J Psychiatry Neurosci. 2001 Jan;26(l): 17-9
British National Formulary"Section 4.3 - Antidepressant drugs: Withdrawal."
S.A. Bult E.M. Hunkeler, J.Y. Lee, C.R Rowland, T.E. Williamson, J.R Schwab, S.W. Hurt"Discontinuing or switching selective serotonin-reuptake inhibitors" Ann Pharmacother. 2002 Apr;36( 4):578-84
S.A. Bult X.H. Hu, E.M. Hunkeler, J.Y. Lee, E.E. Ming, L.E. Markson, B. Fireman "Discontinuation of use and switching of antidepressants: influence of patient-physician communication"JAMA. 2002 Sep 18;288( 11): 1403-9
V.Choo"Paroxetine and extrapyramidal reactions." Lancet. 1993 Mar 6;341(8845):624
E. F. Cocarro"Central serotonin and impulsive aggression." Br J Psychiatry Suppl. 1989 Dec;(8):52-62
F. H. Coleman, H.D. Christensen, c.L. Gonzalez, W.F. Rayburn"Behavioral changes in developing mice after prenatal exposure to paroxetine (Paxil)" Am J Obstet Gynecol. 1999 Nov;181(5 Pt 1): 1166-71
COMMITTEE ON SAFETY OF MEDICINES “Benzodiazepines, Dependence, and Withdrawal Symptoms” benzo.org.uk : Committee on Safety of Medicines, Benzodiazepines, Jan...
M. Cotterchio, N. Kreiger, G. Darlington, A. Steingart "Antidepressant medication use and breast cancer risk" Am J Epidemiol. 2000 May 15;151(10):951-7
N.J. Coupland, c.t. Bell, J.P. Potokar
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 80 of 246 PageID# 8310

CSMjMCA, Current Problems in Pharmacovigilance, Volume 19, February 1993 "Dystonia and withdrawal symptoms with paroxetine (Seroxat)"
M.L. Dahl, E. Olhager, J. Ahlner"Paroxetine withdrawal syndrome in a neonate" Br J Psychiatry. 1997 Oct;171:391-2
D'Arcy"Dystonia and withdrawal symptoms with paroxetine." International Pharmacology Journal 1993;7:140
D. Davidoff, M.D.,“Sponsorship, Authorship, and Accountability”N Engl 7 Med, Vol. 345, No. 11 • September 13, 2001, 825-827
J. R. Davidson"The long-term treatment of panic disorder"J Clin Psychiatry. 1998;59Suppl8:17-21; discussion 22-3
C. Debattista, A.F. Schatzberg"Physical symptoms associated with paroxetine withdrawal" Am J Psychiatry. 1995 Aug;152(8):1235-4
R. DeRubeis, PhD; S.D. Hollon, PhD; J.D. Amsterdam, MD; R.C. Shelton, MD; P.R. Young, PhD; R.M. Salomon, MD; J.P O'Reardon, MD; M.L Lovett, MEd; M.M Gladis, PhD;L.L. Brown, PhD; R.G., PhD“Cognitive Therapy vs Medications in the Treatment of Moderate to Severe Depression” ARCH GEN PSYCHIATRY/VOl. 62. APR 2005, 409-416
K. Demyttenaere, E. Van Ganse, J. Gregoire, E. Gaens, P. Mesters"Compliance in depressed patients treated with fluoxetine or amitriptyline. Belgian Compliance Study Group."Int Clin Psychopharmacol. 1998 Jan; 13(1): 11-7
K. Demyttenaere, P. Haddad"Compliance with antidepressant therapy and antidepressant discontinuation symptoms"Acta Psychiatr Scand Suppl. 2000; 403:50-6
O. Diav-Citrin, S. Shechtmanl, D. Weinbaum, J. Arnon, E. Di Gianantonio, M. Clementi, A. Ornoyl“Paroxetine and Fluoxetine in Pregnancy: a multicenter, prospective, controlled study” Abstracts/Reproductive Toxicology 20 (2005) 453-491
RS. Diler, L. Tamam, A. Avci"Withdrawal symptoms associated with paroxetine discontinuation in a nine-year-old boy"J. Clin Psychopharmacol. 2000 Oct;20(5):586-7
"Serotonin reuptake inhibitor withdrawal"J Clin Psychopharmacol. 1996 Oct;16(5):356-62
S.C. Dilsaver, J.F. Greden
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 81 of 246 PageID# 8311

Antidepressant withdrawal phenomena." Biol Psychiatry. 1984 Feb;19(2):237-56
S.c. Dilsaver, J.F. Greden, RM. Snider"Antidepressant withdrawal syndromes: phenomenology and pathophysiology" Int Clin Psychopharmacol. 1987 Jan;2(l): 1-19
S.c. Dilsaver, J.F. Greden"Antidepressant withdrawal-induced activation (hypomania and mania): is withdrawal-induced cholinergic overdrive causally significant?"J Clin Psychopharmacol. 1984 Jun;4(3): 174-5
S.c. Dilsaver"Withdrawal phenomena associated with antidepressant Drug Saf. 1994 Feb;10(2):103-14
RA. Dominguez, P.J. Goodnick"Adverse events after the abrupt discontinuation of paroxetine" Pharmacotherapy. 1995 Nov-Dee; 15(6):778-80
J. Donoghue, P. Haddad"Pharmacists lack knowledge of antidepressant discontinuation symptoms,"J Clin Psychiatry. 1999 Feb;60(2): 124-5
Drug and Therapeutics Bulletin [No authors listed] "Withdrawing patients from antidepressants."Drug Ther Bull. 1999 Jul;37(7):49-52
E. Einbinder"Fluoxetine withdrawal?"Am J Psychiatry. 1995 Aug;152(8):1235
I. Elkin, PhD, M.T. Shea, PhD“National Institute of Mental Health Treatment of Depression Collaborative Research Program”Arch Gen Psychiatry Vol. 46 11/1998
J. M. Ellison, J.E. Milofsky, E. Ely"Fluoxetine-induced bradycardia and syncope in two patients" J Clin Psychiatry. 1990 Sep;51(9):385-6
J.M. Ellison"SSRI Withdrawal Buzz"J Clin Psychiatry. 1994Dec;55(12):544-5
Farah, T.E. Lauer"Possible venlafaxine withdrawal syndrome" Am J Psychiatry. 1996 Apr;153(4):576
M.Fava
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 82 of 246 PageID# 8312

"A comparison of symptoms following treatment interruption: Evidence from arandomized, double-blind trial with fluoxetine, sertraline, and paroxetine."Eur Psychiatry 1998;13(suppI4):204-5
G.A. Fava"Do antidepressant and antianxiety drugs increase chronicity in affective disorders?" Psychother Psychosom. 1994;61(3-4): 125-31
M. Fava, R. Mulroy, J. Alpert, A.A. Nierenberg, J.F. Rosenbaum"Emergence of adverse events following discontinuation of treatment with extended-release venlafaxine"Am J Psychiatry. 1997 Dec;154(12):1760-2
G.A. Fava"Holding on: depression, sensitization by antidepressant drugs, and the prodigal experts"Psychother Psychosom. 1995;64(2):57-61
G.A. Fava, S. Grandi"Withdrawal syndromes after paroxetine and sertraline discontinuation" J Clin Psychopharmacol. 1995 Oct;15(5):374-5
Robert J. FeRubeis, PhD, Steven D. Hollon, PhD, Jay D. Amsterdam, MD “Cognitive Therapy vs. Medications in Treatment of Moderate to Severe Depression”Arch Gen Psychiatry 2005;62;409-416
F. Frost, S. Fal"Shock-like sensations after discontinuation of selective serotonin reuptake inhibitors" Am 1 Psychiatry. 1995 May;152(5):810
B. Geller, T.B. Cooper, F.G. Carr, J.E. Warham, A. Rodriguez"Prospective study of scheduled withdrawal from nortriptyline in children andadolescents"J Clin Psychopharmacol. 1987 Aug;7(4):252-4
Gillespie"SSRIs and withdrawal syndrome."World Congress of Psychiatry, Madrid. Aug 23-28; 1996
J. Glenmullen, MD Prozac BacklashNew York: Simon & Schuster, 2000
R.N. Golden"Selective serotonin reuptake inhibitor elimination half-lives: the long and the short of it"Biol Psychiatry. 1998 JuI15;44(2):75-6
F.Golightly, MB, BS, MRCPsych“Antidepressant discontinuation syndromes: a review of presentation and management”
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 83 of 246 PageID# 8313

Mental Health Practice; 2/2000; Vol. 3 No. 5
A.J. GoudieWhat is the clinical significance of the discontinuation syndrome seen with clozapine? J Psychopharmacol. 2000 Jun;14(2): 188-92
Dr. Ben Green, MRCPsych, ILTM"Persistent adverse neurological effects following SSRI discontinuation (PANES)" http://www.priory.com/psych/panes.htm
P. Grof R. Joffe, S. Kennedy, E. Persad, J. Syrotiuk, D. Bradford"An open study of oral flesinoxan, a 5-HT1A receptor agonist, in treatment-resistantdepression"Int Clin Psychopharmacol. 1993 Fall;8(3): 167-72
P. Haddad, I . Anderson"Antidepressants aren't addictive: clinicians have depended on them for years." I Psychopharmacol. 1999;13(3):291-2; discussion 299
P. Haddad, M. Lejoyeux, A. Young "Antidepressant discontinuation reactions" BMJ. 1998 Apr 11 ;316(7138):1105-6
P.M. Haddad"Antidepressant discontinuation syndromes"Drug Saf. 2001;24(3): 183-97
P.M. Haddad, S. Devarajan, S.M. Dursun"Antidepressant discontinuation (withdrawal) symptoms presenting as 'stroke'"J PsychopharmacoL 2001 Jun;15(2): 139-41
P.M. Haddad"Do antidepressants have any potential to cause addiction?" J Psychopharmacol. 1999;13(3):300-7
P.M. Haddad, M. Qureshi“ Misdagnosis of antidepressants and the discontinuation symptoms”Acta Psychiatr Scand. 2000 Dec;102(6):466-7; discussion 467-8
P.M. Haddad"Newer antidepressants and the discontinuation syndrome"I Clin Psychiatry. 1997;58 SuppI7:17-21; discussion 22
P.M. Haddad, JS. Hellewell"Reply to AJ Goudie - What is the clinical significance of the discontinuation syndrome seen with clozapine?"J Psychopharmacol. 2000 Jun;14(2): 191-92
P.M. Haddad"The SSRI discontinuation syndrome"I Psychopharmacol. 1998; 12(3):305-13
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 84 of 246 PageID# 8314

Harvard Mental Health Letter"Symptoms that start when an antidepressant stops" Harv Ment Health Lett. 2001 Feb;17(8):7-8
D. Healy"Reply to A.J. Goudie - What is the clinical significance of the discontinuation syndrome seen with clozapine?"J Psychopharmacol. 2000 Jun;14(2): 191
V. Hendrick, Z.N. Stowe, L.L. Altshuler, A. Hostetter, A. Fukuchi "Paroxetine use during breast-feeding"J. Clin Psychopharmacol. 2000 Oct;20(5):587-9
V. Hendrick, A. Fukuchi, L. Altshuler, M. Widawski, A. Wertheimer, M.V. Brunhuber "Use of sertraline, paroxetine and fhivoxamine by nursing women" Br J Psychiatry.2001 Aug;179:163-6
P.J. Hilts“Jury Award $6.4 Million in Killings Tied to Drug”N e w Y o r k T im e s 8 June 2001
Hindmarch, S. Kimber, S.M. Cockle"Abrupt and brief discontinuation of antidepressant treatment: effects on cognitive function and psychomotor performance"Int Clin Psychopharmacol. 2000 Nov;15(6):305-18
S.E. Hyman, MD & Eric J. Nestler MD. PhD“Initiation and Adaption: A Paradigm for Understanding Psychotropic Drug Action”Am J Psychiatry 153:2; Feb 1996
Inman"Report number 6: Paroxetine."Pharmacoepidemiology and Drug Safety 1993;2:393-422
S. Ito, G. KorenAntidepressants and breast-feeding" Am J Psychiatry. 1997 Aug; 154(8): 1174
B.L. Jacobs, CA. Fornal"5-HT and motor control: a hypothesis" Trends Neurosci. 1993 Sep;16(9):346-52
R. Judge, M.G. Parry, D. Quail, J.G. Jacobson"Discontinuation symptoms: comparison of brief interruption in fluoxetine and paroxetine treatment"Int Clin Psychopharmacol. 2002 Sep;17(5):217-25
E.M. Kaplan
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 85 of 246 PageID# 8315

"Antidepressant noncompliance as a factor in the discontinuation syndrome" J Clin Psychiatry. 1997;58 Suppl 7:31-5; discussion 36
D. Kasantikul"Reversible delirium after discontinuation of fluoxetine" J Med Assoc Thai. 1995 Jan;78(l):53-4
L.S. Kent, J.D. Laidlaw"Suspected congenital sertraline dependence" Br J Psychiatry. 1995 Sep;167(3):412-3
N.J. Keuthen, P. Cyr, J.A. Ricciardi, W.E. Minichiello, M.L. Buttolph, M.A. [enike "Medication withdrawal symptoms in obsessive-compulsive disorder patients treated with paroxetine"J Clin Psychopharmacol. 1994 Jun;14(3):206-7
C.J. Kilpatrick, K.T. Bunce, M.B. Tyers
"5-HT3 receptors"Med Res Rev. 1990 Oct-Dec;10(4):441-75
L. F. Koopowitz, M. Berk "Paroxetine-induced withdrawal effects"Hum Psychopharmacol. 1995 Vol 10:147-8
M. Kotlyar, M. Golding, E.R. Brewer, S.W. Carson Possible nefazodone withdrawal syndromeAm J Psychiatry. 1999 Jul; 156(7): 1117
M.S. Kreider, W.D. Bushnell, R. Oakes, D.E. Wheadon"A double-blind, randomized study to provide safety information on switching fluoxetine-treated patients to paroxetine without an intervening washout period" J Clin Psychiatry. 1995 Apr;56(4): 142-5
Landry"Hypomania following abrupt discontinuation of paroxetine" Currents in Affective Illness 1997; 16(4)
Landry P, Roy L"Withdrawal hypomania associated with paroxetine" J Clin Psychopharmacol. 1997 Feb;17(l):60-1
Lane"Withdrawal symptoms after discontinuation of selective serotonin reuptake inhibitors (SSRIs)"Journal of Serotonin Research, 1996;3:75-83
K.E. Lasser MD, MPH, Paul D. Allen, MD, MPH“Timing of a New Black Box Warning and Withdrawals for Prescription Medications”AMA, May 1, 2002-Vol 287, No. 17
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 86 of 246 PageID# 8316

A.L. Lazowick, G.M. Levin"Potential withdrawal syndrome associated with SSRI discontinuation" Ann Pharmacother. 1995 Dec;29(12): 1284-85
F.L. Leiter, A.A. Nierenberg, KM. Sanders, T.A. Stern"Discontinuation reactions following sertraline" Biol Psychiatry. 1995 Nov15;38(10):694-5
M. Lejoyeux, J. Ades"Antidepressant discontinuation: a review of the literature" J Clin Psychiatry. 1997;58Suppl 7:11-5; discussion 16
M. Lejoyeux, J. Ades, I . Mourad, J. Solomon, S. Dilsaver“Antidepressant Withdrawal Syndrome: Recognition, Prevention and Management" CNS Drugs 1996;Apr. 5(4): 278-92
M. Lejoyeux, C. Rodiere-Rein, J. Ades"Withdrawal syndrome from antidepressive drugs. Report of 5 c a s e s "Encephale. 1992 May-Jun;18(3):251 [Article in French]
B. Liskin, S.P. Roose, B.T. Walsh, W.K. Jackson"Acute psychosis following phenelzine discontinuation" J Clin Psychopharmacol. 1985 Feb;5(l):46-7
A.K. Fouie, RA. Fannon, F.J. Ajari"Withdrawal reaction after sertraline discontinuation"Am J Psychiatry. 1994 Mar;151(3):450-1
J.B. Fucot, G.H. Crampton1/8-OH-DPAT suppresses vomiting in the cat elicited by motion, cisplatin or xylazine" Pharmacol Biochem Behav. 1989 Jul;33(3):627-31
S. Mace, D. Taylor“Selective serotonin reuptake inhibitors: a review of efficacy and tolerability in depression” Exp. Opin. Pharmacother. (2000) l(5):917-933
F. J. Mackay, N.R Dunn, F.V. Wilton, G.F. Pearce, S.N. Freemantle, RD. Mann1 / A Comparison of Fluvoxamine, Fluoxetine, Setraline and Paroxetine Examined by Observational Cohort Studies"Pharmacoepidemiol Drug Saf 1997 Apr; 6: 235-46
S.M. Maixner, J.F. GredenExtended antidepressant maintenance and discontinuation syndromes Depress Anxiety. 1998;8 Suppll:43-53
G. Mallya, K. White, C. Gunderson"Is there a serotonergic withdrawal syndrome?" Biol Psychiatry. 1993 Jun 1-15 ;33( 11- 12):851-2
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 87 of 246 PageID# 8317

O. Mammen, J.M. Pere!, S. Wheeler Antidepressants and breast-feeding Am J Psychiatry. 1997 Aug;154(8): 1174-5
A.M. Mann, AS. Macpherson"Clinical experience with imipramine in the treatment of depression"
J. Mann, MD“The Medical Management of Depression”N Engl J Med 2005;353:1819-34Can Psychiatr Assoc J. 1959 Jan;4(l):38-47
T.R Mareth, T.M. Brown "SSRI withdrawal"J Clin Psychiatry. 1996 Jul;57(7):310J.S. Markowitz, c.r, DeVane, H.L. Liston, S.A. Montgomery“An assessment of selective serotonin reuptake inhibitor discontinuation symptoms with citalopram"Int Clin Psychopharmacol. 2000 Nov;15(6):329-33
J.S. Markowitz"Re: Nefazodone withdrawal symptoms" Can J Psychiatry. 1999 Apr;44(3):286-7
Janet Maslin“Books of the tines; exploring a dark side of depression remedies”N e w Y o r k T im e s 29 June 2000
T. McMahon"Bipolar affective symptoms associated with use of captopril and abrupt withdrawal ofpargyline and propranolol"Am J Psychiatry. 1985 Jun;142(6):759-60
T.e. McMahon“A clinical overview of syndromes following withdrawal of antidepressants" Hosp Community Psychiatry. 1986 Sep;37(9):883-4
D. Michelson, M. Fava, J. Amsterdam, J. Apter, P. Londborg, R Tamura, RG. Tepner "Interruption of selective serotonin reuptake inhibitor treatment. Double-blind, placebo- controlled trial"Br J Psychiatry. 2000 Apr; 176:363-8
e. Milliken, S.J. Cooper"Withdrawal Symptoms from Paroxetine" Hum PsychopharmacoI1998;13: 217-9
S.M. Mirin, A.F. Schatzberg, D.E. Creasey"Hypomania and mania after withdrawal of tricyclic antidepressants" Am J Psychiatry. 1981 Jan;138(l):87-9
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 88 of 246 PageID# 8318

J. e. Nelson, RS. Schottenfeld, e.D. Conrad "Hypomania after desipramine withdrawal" Am J Psychiatry. 1983 May;140(5):624-5
H. Nordeng, R. Lindemann, KV. Perminov, A. Reikvam"Neonatal withdrawal syndrome after in utero exposure to selective serotoninreuptake inhibitors"Acta Paediatr. 2001 Mar;90(3):288-91
S. Nuss, C.N. Kincaid"Serotonin discontinuation syndrome: does it really exist?" W V Med J. 2000 Mar- Apr;96(2):405-7
S.Nuss, MD, C.R. Kincaid, MD“Serotonin discontinuation syndrome: does it really exist”The West VA Medical Journal; March/April 2000; Vol. 96S. Oehrberg, P.E. Christiansen, K Behnke, A.L. Borup, B. Severin, J. Soegaard, H. Calberg, R. Judge, J.K Ohrstrom, P.M. Manniche"Paroxetine in the treatment of panic disorder. A randomised, double-blind, placebo- controlled study"Br J Psychiatry. 1995 Sep;167(3):374-9
M. Olfson, G.L. Klerman"Trends in the prescription of antidepressants by office-based psychiatrists." Am J Psychiatry. 1993 Apr;150(4):571-7
K. Otani, O. Tanaka, S. Kaneko, M. Ishida, N. Yasui, Y. Fukushima "Mechanisms of the development of trazodone withdrawal symptoms" Int Clin Psychopharmacol. 1994 Summer;9(2):131-3
L. Pacheco, P. Malo, E. Aragues, M. Etxebeste "More cases of paroxetine withdrawal syndrome" Br J Psychiatry. 1996 Sep;169(3):384
G. Parker, J. Blennerhassett"Withdrawal reactions associated with venlafaxine" Aust N Z J Psychiatry. 1998 Apr;32(2):291-4
S.D. Phillips"A possible paroxetine withdrawal syndrome" Am J Psychiatry. 1995 Apr;152(4):645-6
B.G. Pollock"Discontinuation symptoms and SSRIs" J Clin Psychiatry. 1998 Oct;59(10):535-7
B.G. Pollock, B.H. Mulsant, R. Nebes, M.A. Kirshner, A.E. Begley, S. Mazumdar, C.F. Reynolds, III"Serum anticholinergicity in elderly depressed patients treated with paroxetine or nortriptyline"Am JPsychiatry. 1998 Aug;155(8):1110-2
S.H. Preskorn"Pharmacokinetics of antidepressants: why and how they are relevant to treatment" JClin Psychiatry. 1993 Sep;54 Suppl: 14-34; discussion 55-6
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 89 of 246 PageID# 8319

J.S. Price, P.C. Waller, S.M. Wood & A. V.P. MacKay“A comparison of the post-marketing safety of four selective serotonin re-uptake inhibitors including the investigation of symptoms occurring on withdrawal”BR J Clin Pharmacol 1996; 42: 757-763
J.S. Price, P.C. Waller PC, S.M. Wood“SSRI withdrawal syndrome rare and relatively mild”BR J Clin Pharmacol 1993; 42 757
RG. Priest, C. Vize, A. Roberts, M. Roberts, A. Tylee"Lay people's attitudes to treatment of depression: results of opinion poll for Defeat Depression Campaign just before its launch" BMJ. 1996 Oct 5;313(7061):858-9
R. E. Pyke"Paroxetine withdrawal syndrome"Am J Psychiatry. 1995 Jan; 152 (1): 149-50
M. Rajagopalan, J. Little"Discontinuation symptoms with nefazodone"Aust N Z J Psychiatry. 1999 Aug;33(4):594-7
S. L. Rauch, R.L. O'Sullivan, M.A. [enike"Open treatment of obsessive-compulsive disorder with venlafaxine: a series of ten cases"J. Clin Psychopharmacol. 1996 Feb;16(l):81-4
R.R. Reeves, H.B. Pinkofsky"Lhermitte's sign in paroxetine withdrawal"I Clin Psychopharmacol. 1996 Oct;16(5):411-2
E. Richelson"Pharmacology of antidepressants"Psychopathology, 1987;20 Suppl 1:1-12
E. Richelson"The pharmacology of antidepressants at the synapse: focus on newer compounds"J Clin Psychiatry. 1994 Sep;55 Suppl A:34-9; discussion 40-1,98-100
E. Richelson"Serotonin: and what about its side effects?"Depress Anxiety. 1998; 7 Suppll:18-20
E. Richelson"Synaptic effects of antidepressants."J Clin Psychopharmacol. 1996 Jun; 16(3 SuppI2):lS-7S; discussion 7S-9S
E. Richelson“Pharmacology of Antidepressants”Mayo Clin Proc. 2001; 76:511-527
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 90 of 246 PageID# 8320

J.F. Rosenbaum, J. Zajecka"Clinical management of antidepressant discontinuation" J Clin Psychiatry. 1997;58 Suppl 7:37-40
J.F. Rosenbaum, M. Fava, S.L. Hoog, RC. Ascroft, W.B. Krebs"Selective se ro ton in reuptake inhibitor discontinuation syndrome: a randomized clinical trial"Biol Psychiatry. 1998 JuI15; 44(2):77-87
Rosenblatt"Paroxetine withdrawal after slow-dosage taper" Currents in Affective Illness1996;15:8-9Rosenblatt"Toxicology and drug interactions." Currents in Affective Illness 1996;15:3-4
H.A. Rosenstock"Sertraline withdrawal in two brothers: a case report" Int Clin Psychopharmacol. 1996 M ar;ll(l):58-9
A.J. Rothschild"Mania after withdrawal of isocarboxazid"J Clin Psychopharmacol. 1985 Dec;5(6):340-2
A.F. Schatzberg"Antidepressant discontinuation syndrome: an update on serotonin reuptake inhibitors"J. Clin Psychiatry 1997;58 Suppl 7:3-4
A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, l.F. Rosenbaum, A.H. Young, /.Zajecka"Possible biological mechanisms of the serotonin reuptake inhibitor discontinuation syndrome. Discontinuation Consensus Panel"J. Clin Psychiatry. 1997;58 Suppl 7:23-7
A.F. Schatzberg, P. Haddad, E.M. Kaplan, M. Lejoyeux, J.F. Rosenbaum, A.H. Young, J. Zajecka"Serotonin reuptake inhibitor discontinuation syndrome: a hypothetical definition. Discontinuation Consensus panel"J. Clin Psychiatry. 1997;58 Suppl 7:5-10
I. O. Schechter"Treatment of disequilibrium and nausea in the SRI discontinuation syndrome"J. Clin Psychiatry. 1998 Aug;59(8):431-2
CH. Schenck, M.W. Mahowald, S.W. Kim, K.A. O'Connor, T.D. Hurwitz
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 91 of 246 PageID# 8321

"Prominent eye movements during NREM sleep and REM sleep behavior disorder associated with fluoxetine treatment of depression and obsessive-compulsive disorder" Sleep. 1992 Iun;15(3):226-35
K. A. Schulman, MD, D.M. Seils, MA“A national survey o f provisions in clinical-trial agreements between medical schools and industry sponsors”N Engl J Med, 2002, Vol. 347, No. 107
C. Sherman“Long-term side effects surface with SSRIs”Clinical Psychiatry News 26(5): 1, 1998
D. Shoenberger"Discontinuing paroxetine: a personal account" Psychother Psychosom. 2002 Jul- Aug;71 (4):237-8
R. Silvestri, E.F. Pace-Schott, T. Gersh, R. Stickgold, C Salzman, LA. Hobson "Effects of fluvoxamine and paroxetine on sleep structure in normal subjects: a home- based Nightcap evaluation during drug administration and withdrawal"J. Clin Psychiatry. 2001 Aug;62(8):642-52L. G. Sobrinho"The drive to look for insight"Psychother Psychosom. 2003 Mar-Apr;72(2): 112
M.L Spencer"Fluoxetine hydrochloride (Prozac) toxicity in a neonate"Pediatrics. 1993 Nov;92(5):721-2
M.M. Stahl, M. Lindquist, M. Pettersson, I.R Edwards, J.H. Sanderson, N.F. Taylor, A.P. Fletcher, J.S. Schou"Withdrawal reactions with selective serotonin re-uptake inhibitors as reported to the WHO system"Eur J Clin Pharmacol. 1997;53(3-4):163-9
M.B. Stein, M.J. Chartier, A.L. Hazen, CD. Kroft, RA. Chale, D. Cote, J.R Walker "Paroxetine in the treatment of generalized social phobia: open-label treatment and double-blind placebo-controlled discontinuation"J Clin Psychopharmacol. 1996 Jun;16(3):218-22
M.B. Stein, M.R Liebowitz, RB. Lydiard, CD. Pitts, W. Bushnell, I. Gergel "Paroxetine treatment of generalized social phobia (social anxiety disorder): a randomized controlled trial"JAMA. 1998 Aug 26;280(8):708-13
"Extroverted Like Me: How a month and a half on Paxil taught me to love being shy" By Seth StevensonPosted Tuesday, January 2, 2001, at 6:30 PM PT http://slate.msn.com/id/95903
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 92 of 246 PageID# 8322

Stoker and Eric report from the American Psychiatric Association Annual Meeting May22-27, 1993 in San Francisco
J.A. Stoukides, CA. Stoukides"Extrapyramidal symptoms upon discontinuation of fluoxetine"Am J Psychiatry. 1991 Sep;148(9):1263
Z.N. Stowe, L.S. Cohen, A. Hostetter, J.C Ritchie, M.J. Owens, CB. Nemeroff "Paroxetine in human breast milk and nursing infants" Am J Psychiatry. 2000 Feb;157(2):185-9
G.M. Strickland, D.W. Hough"Unilateral facial numbness and visual blurring associated with paroxetine discontinuation"J Clin Psychopharmacol. 2000 Apr;20(2):271-2
E. Szabadi"Fluvoxamine withdrawal syndrome"Br J Psychiatry. 1992 Feb;160:283-4
T. Terao"Misdiagnosis of antidepressant discontinuation symptoms" Acta Psychiatr Scand.2001 Jul;104(l):77-8
Therrien"Selective serotonin reuptake inhibitors and withdrawal symptoms: a review of the literature."Hum Psychopharmacol. 1997;12:309-23
D.R. Thomas, D.R. Nelson, A.M. Johnson"Biochemical effects o f the antidepressant paroxetine, a specific 5-hydroxytryptamine uptake inhibitor"Psychopharmacology (Berl). 1987 ;93(2): 193-200
C. Thompson"Discontinuation of antidepressant therapy: emerging complications and their relevance"J Clin Psychiatry. 1998 Oct;59(10):541-8
T. Trenque, D. Piednoir, C. Frances, H. Millart, M.F. Germain"Reports of withdrawal syndrome with the use of SSRIs: a case/non-case study in the French Pharmacovigilance database" Pharmacoepidemiol Drug Saf. 2002 Jun ;ll(4 ):281- 3
FF. Tulloch, A.M. Johnson."The pharmacologic profile of paroxetine, a new selective serotonin reuptake inhibitor" J Clin Psychiatry. 1992Feb;53 Suppl:7-12
P. Tyrer
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 93 of 246 PageID# 8323

"Clinical effects of abrupt withdrawal from tri-cyclic antidepressants and monoamine oxidase inhibitors after long-term treatment"J Affect Disord. 1984Feb ;6 (l):l-7
M. Walker-Kinnear, S. McNaughton"Paroxetine discontinuation syndrome in association with sertindole therapy" Br J Psychiatry. 1997 Apr;170:389
D.G. Watt, L.J. Bouyer, I.T. Nevo, A.V. Smith, Y. Tiande "What is motion sickness?"Ann NY Acad Sci. 1992 May 22;656:660-7
W HO-GenevaThe IC D -10 Classification of M ental and Behavioral Disorders, 1992 (Section defining 'withdrawal')
K.L. Wisner, J.M. Perel, RL. Findling "Antidepressant treatment during breast-feeding Am J Psychiatry. 1996 Sep;153(9): 1132-7
K.L. Wisner, RL. Findling, J.M. Perel "Paroxetine in breast milk"Am JPsychiatry. 2001 Jan;158(l):144-5
K.L. Wisner, A.J. Gelenberg, H. Leonard, D. Zarin, E. Frank "Pharmacologic treatment of depression during pregnancy" JAMA. 1999 Oct 6;282(13): 1264-9
RM. Wolfe1 / Antidepressant withdrawal reactions"Am Fam Physician. 1997 Aug;56(2):455-62
A.H. Young, A. Currie, C.H. Ashton "Antidepressant withdrawal syndrome" Br J Psychiatry. 1997 Mar;170:288
A.H. Young, A. Currie"Physicians' knowledge of antidepressant withdrawal effects: a survey" J Clin Psychiatry. 1997;58 Suppl7:28-30
J. Zajecka, K.A. Tracy, S. Mitchell"Discontinuation symptoms after treatment with serotonin reuptake inhibitors: a literature review"J Clin Psychiatry. 1997 Jul;58(7):291-7
J. Zajecka, J. Fawcett, J. Amsterdam, F. Quitkin, F. Reimherr, J. Rosenbaum, D. Michelson, C. Beasley
"Safety of abrupt discontinuation of fluoxetine: a randomized, placebo-controlled study J. Clin Psychopharmacol. 1998 Jun;18(3):193-7
Case 1:14-cv-01614-AJT-JFA Document 126-2 Filed 07/10/15 Page 94 of 246 PageID# 8324