Embed Size (px)
Citation preview
Slide 1
Slide 2
Slide 3
Slide 4 Note down areas that they had problems. If not covered in current session or planned sessions then will come back to at the end
Slide 5 Common clinical question: CXR often first examination. Note this is a normal CXRA: Mediastinal wideningQ: WHERE in mediastinum?A: mediastinal bleed causes loss of definition of aortic arch, apical cap, loss of paraaortic line, left pleural effusion. Deviation of NG tube to right.Q: What are some common associated injuries?A: Upper rib fractures, pneumothorax
Slide 6 Q: What signs here suggest aortic injury?A: Widened upper med, loss arch, loss para-aortic line, effusion, deviation NG tube, left apical cap. See if they see the missing rib from prior lung surgery
Slide 7 (Normal on left for comparison with TAI on right to reinforce concept)
Q: How can we be sure we have checked everything in a trauma portable CXR? A: We MUST be systematic to assure we miss no findings on CXR:
Ask learner to talk about what search pattern THEY use for supine trauma chest X-ray. If they don’t have one, emphasize they NEED to develop and consistently use one. Such as…Heart size-Mediastinum-Lungs & Pleura-Soft tissues-Bones-
In this case, Heart size- enlargedMediastinum- Too wideLungs & Pleura- OKSoft tissues- OKBones- OK

Slide 8 A: CT aortic angiogram.Q: How is aortic CTA performed?A: With contrast, large bolus. Thin slices, multiplanar reconstructionsQ: Are CT aortic angiogram images obtained earlier or later after the injection than the images for a CT Pulmonary arteriogram?A: Later (contrast has to enter SVC and pass through the entire Pulmonary circulation before it opacifies aorta. If we instead do a CTPA, we image earlier, catching the contrast while it is still in the pulmonary arteries
Slide 9 Q: What about if you can’t give contrast? What other options do we have?A: CT non contrast – limited, can’t exclude injury but will show if blood in mediastinum.MRI – only if patient stable enough which is rareTEE – talk about requiring anesthesia
Slide 10 (Note to instructor: This short case illustrates the importance of window/level setting in review of trauma cases)
Slide 11 Q: How are we going to review the CT?A: Systematically. Q: What is our approach?A: Consider every organ and decide if normal or not.Q: Is this the proper window and level setting for a trauma exam?A: This is the mediastinal window, one of several that must be reviewed. Failure to look systematically on all three window/level settings (mediastinal, bone, lung) risks missing major abnormalities.
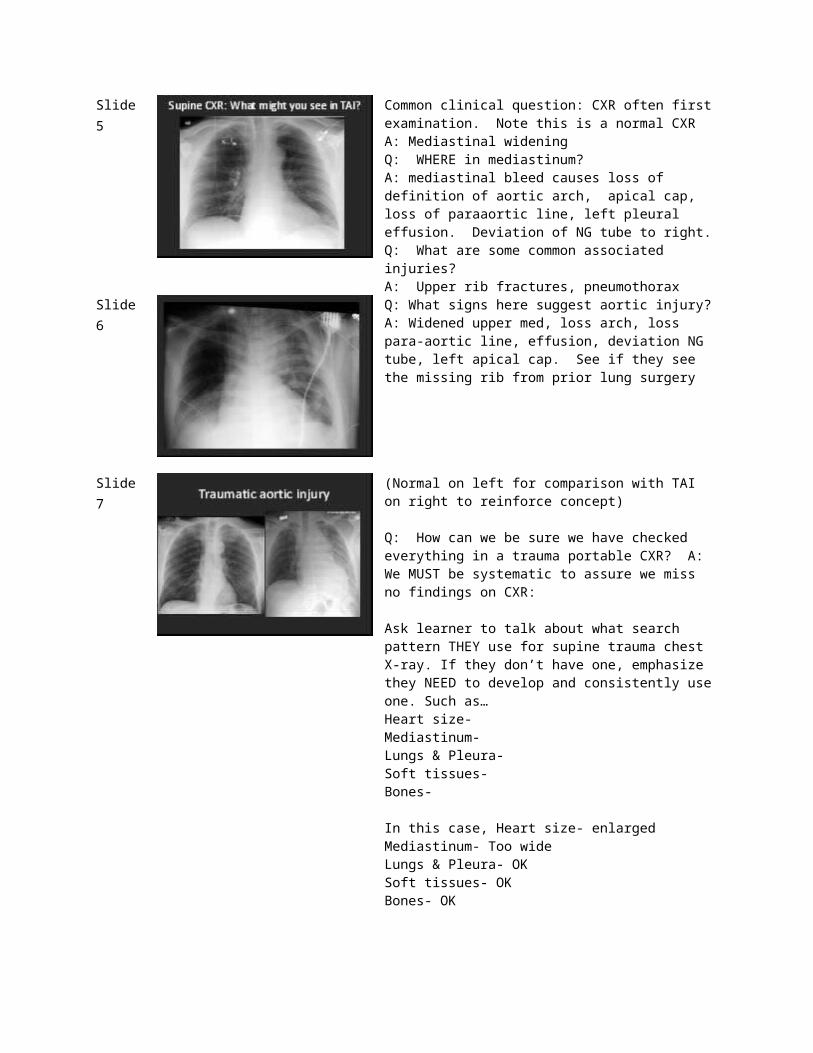
Slide 12 Same images on lung windowQ: What is the black ovoid thing in posterior left lung?A: Traumatic Pneumatocele.Q: What caused it?A: Posterior left rib fractureQ: What is the black stuff just anterior to the heart?A: Small pneumothorax bilaterally surrounds parietal pleural reflection (anterior junction line).Q: What is the increased attenuation in the lung apex?A: Pulmonary contusion injury.
Slide 13 Same images at bone window/level settingQ: What findings do we see here?A: The rib fractures are easier to see (increasing our chance to find them)
Slide 14 Note to instructor:(This case used to illustrate the pitfall of satisfaction of search)
Q: What will be the appropriate imaging for this patient?A: AP portable Chest and Pelvis. Trauma CT chest/abdomen/pelvis with IV contrast, if hemodynamically stable.
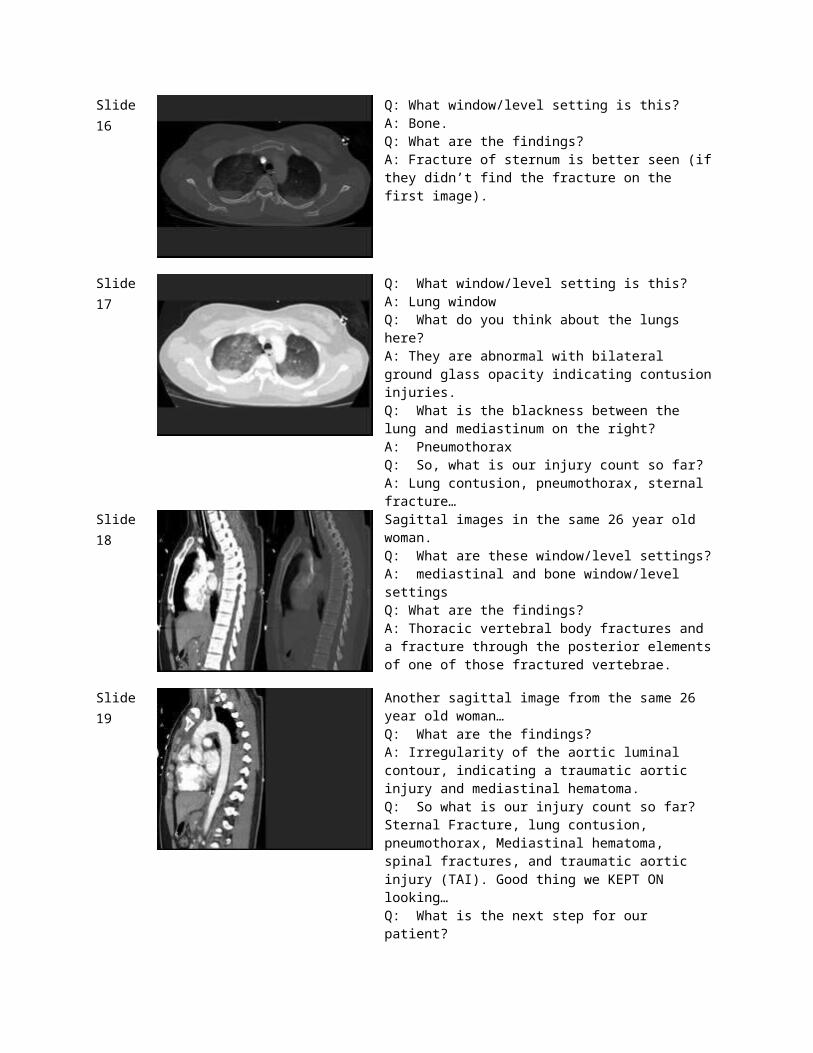
Slide 15 Q: Which window is this?A: MediastinalQ: What is it best for?A: Extravasation of contrast with traumatic aortic injury, infiltration of fat with edema, abnormal fluid collections, etc
Slide 16 Q: What window/level setting is this?A: Bone.Q: What are the findings?A: Fracture of sternum is better seen (if they didn’t find the fracture on the first image).
Slide 17 Q: What window/level setting is this?A: Lung windowQ: What do you think about the lungs here?A: They are abnormal with bilateral ground glass opacity indicating contusion injuries.Q: What is the blackness between the lung and mediastinum on the right?A: PneumothoraxQ: So, what is our injury count so far?A: Lung contusion, pneumothorax, sternal fracture…
Slide 18 Sagittal images in the same 26 year old woman.Q: What are these window/level settings?A: mediastinal and bone window/level settingsQ: What are the findings?A: Thoracic vertebral body fractures and a fracture through the posterior elements of one of those fractured vertebrae.
Slide 19 Another sagittal image from the same 26 year old woman…Q: What are the findings?A: Irregularity of the aortic luminal contour, indicating a traumatic aortic injury and mediastinal hematoma.Q: So what is our injury count so far? Sternal Fracture, lung contusion, pneumothorax, Mediastinal hematoma, spinal fractures, and traumatic aortic injury (TAI). Good thing we KEPT ON looking…Q: What is the next step for our patient?A: (next slide…)
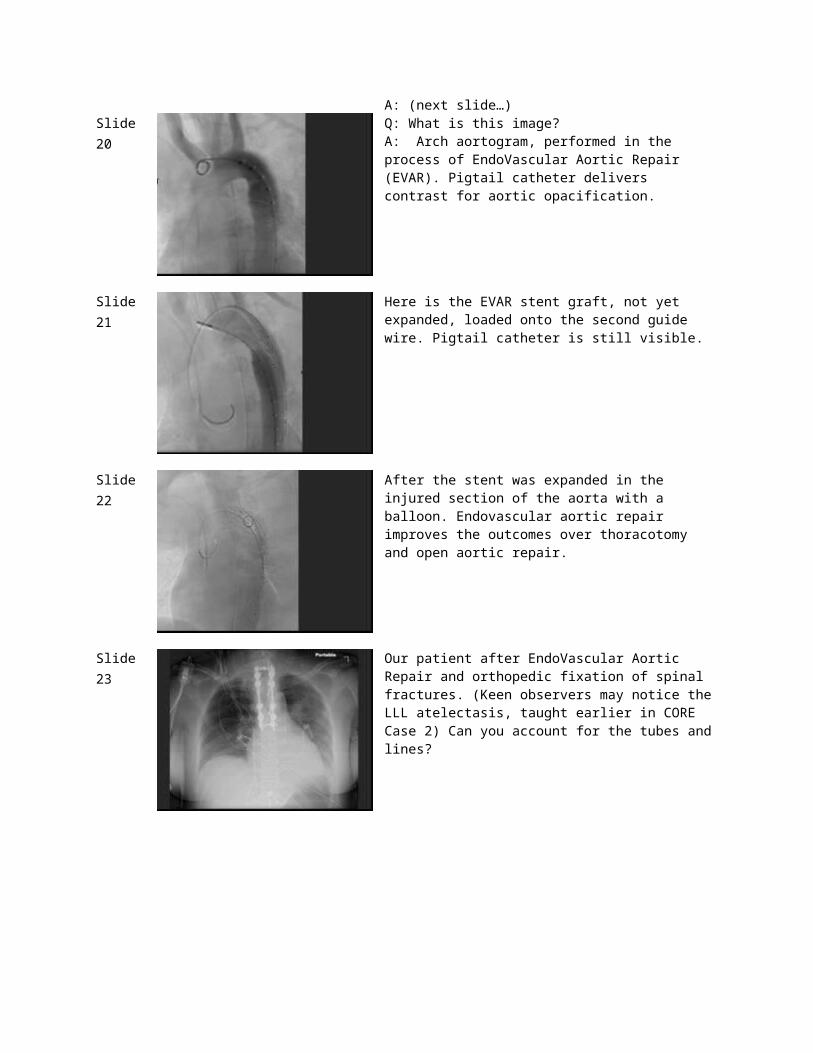
Slide 20 Q: What is this image?A: Arch aortogram, performed in the process of EndoVascular Aortic Repair (EVAR). Pigtail catheter delivers contrast for aortic opacification.
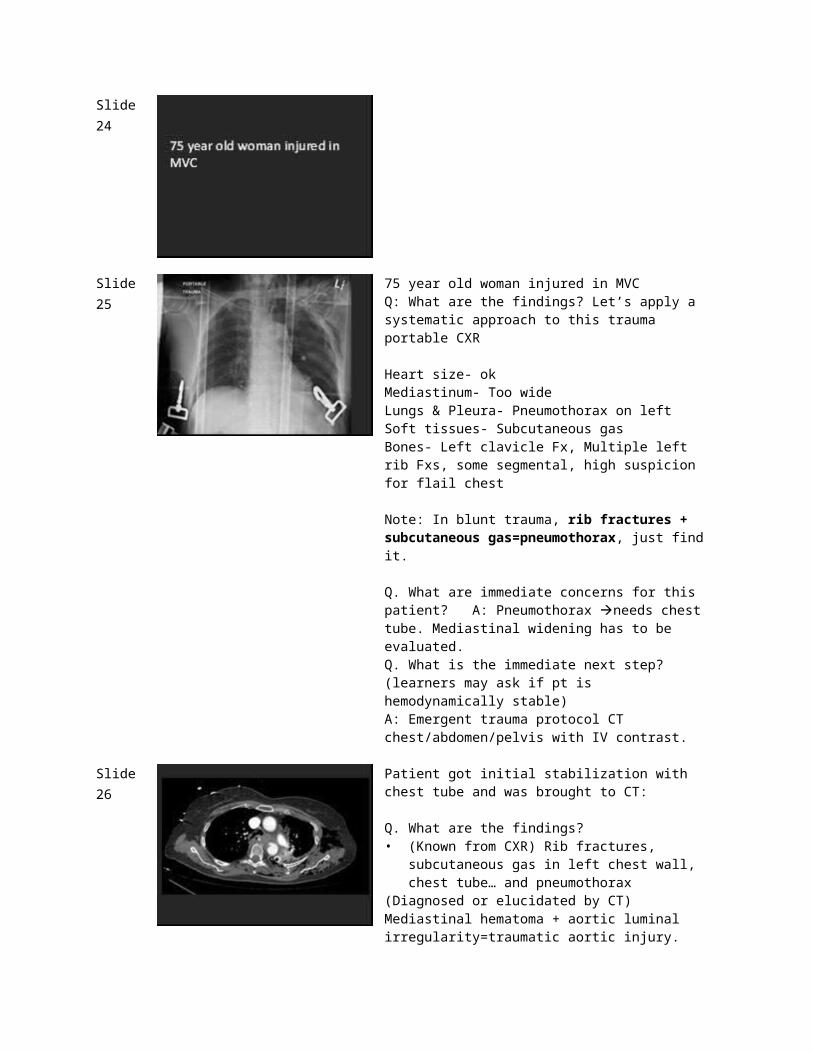
Slide 21 Here is the EVAR stent graft, not yet expanded, loaded onto the second guide wire. Pigtail catheter is still visible.
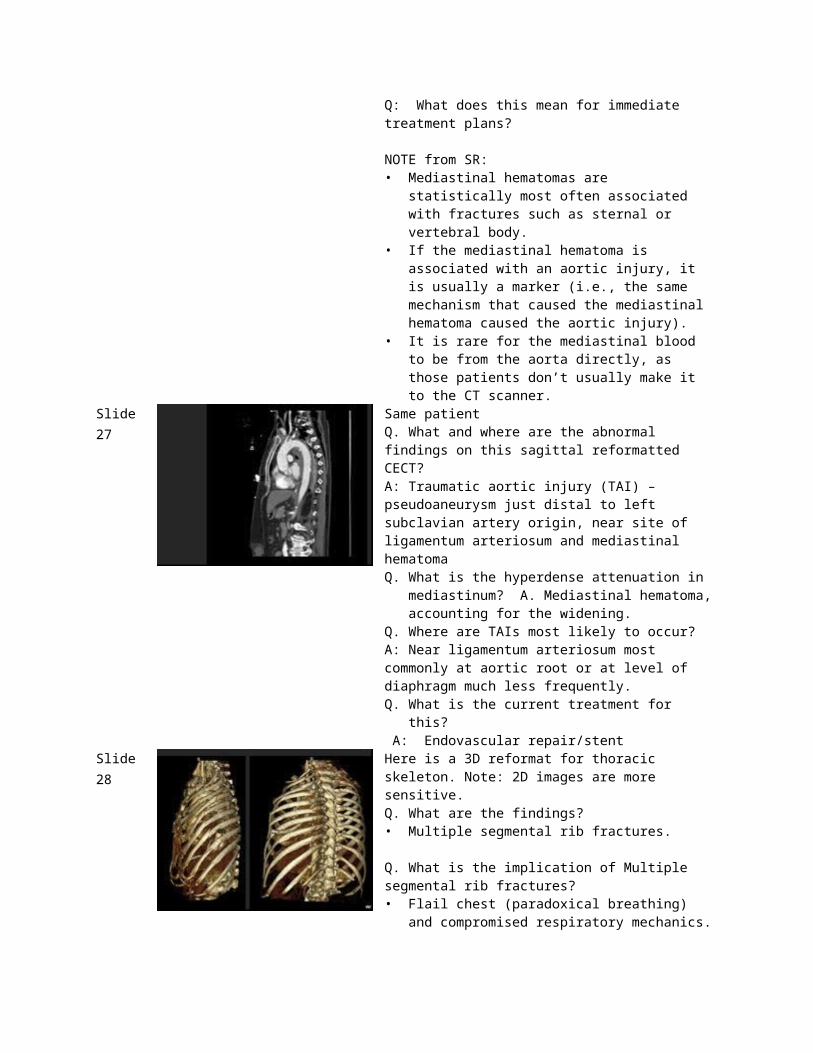
Slide 22 After the stent was expanded in the injured section of the aorta with a balloon. Endovascular aortic repair improves the outcomes over thoracotomy and open aortic repair.
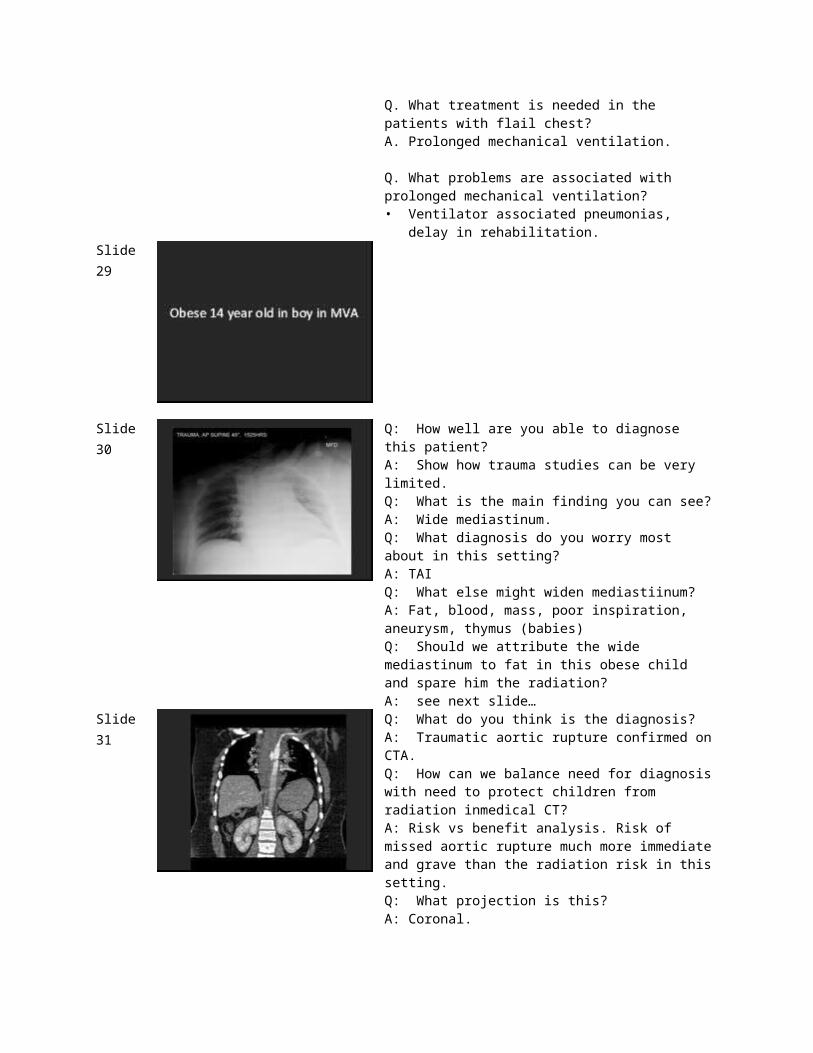
Slide 23 Our patient after EndoVascular Aortic Repair and orthopedic fixation of spinal fractures. (Keen observers may notice the LLL atelectasis, taught earlier in CORE Case 2) Can you account for the tubes and lines?
Slide 24
Slide 25 75 year old woman injured in MVCQ: What are the findings? Let’s apply a systematic approach to this trauma portable CXR
Heart size- okMediastinum- Too wideLungs & Pleura- Pneumothorax on leftSoft tissues- Subcutaneous gasBones- Left clavicle Fx, Multiple left rib Fxs, some segmental, high suspicion for flail chest
Note: In blunt trauma, rib fractures + subcutaneous gas=pneumothorax, just find it.
Q. What are immediate concerns for this patient? A: Pneumothorax needs chest tube. Mediastinal widening has to be evaluated.Q. What is the immediate next step? (learners may ask if pt is hemodynamically stable)A: Emergent trauma protocol CT chest/abdomen/pelvis with IV contrast.
Slide 26 Patient got initial stabilization with chest tube and was brought to CT:
Q. What are the findings?• (Known from CXR) Rib fractures, subcutaneous gas in
left chest wall, chest tube… and pneumothorax(Diagnosed or elucidated by CT) Mediastinal hematoma + aortic luminal irregularity=traumatic aortic injury.Q: What does this mean for immediate treatment plans?
NOTE from SR:• Mediastinal hematomas are statistically most often
associated with fractures such as sternal or vertebral body.
• If the mediastinal hematoma is associated with an aortic injury, it is usually a marker (i.e., the same mechanism that caused the mediastinal hematoma caused the aortic injury).
• It is rare for the mediastinal blood to be from the aorta directly, as those patients don’t usually make it to the CT scanner.
Slide 27 Same patientQ. What and where are the abnormal findings on this sagittal reformatted CECT?A: Traumatic aortic injury (TAI) – pseudoaneurysm just distal to left subclavian artery origin, near site of ligamentum arteriosum and mediastinal hematomaQ. What is the hyperdense attenuation in mediastinum? A.
Mediastinal hematoma, accounting for the widening.Q. Where are TAIs most likely to occur?A: Near ligamentum arteriosum most commonly at aortic root or at level of diaphragm much less frequently.Q. What is the current treatment for this? A: Endovascular repair/stent
Slide 28 Here is a 3D reformat for thoracic skeleton. Note: 2D images are more sensitive.Q. What are the findings?• Multiple segmental rib fractures.
Q. What is the implication of Multiple segmental rib fractures?• Flail chest (paradoxical breathing) and compromised
respiratory mechanics.
Q. What treatment is needed in the patients with flail chest?A. Prolonged mechanical ventilation.
Q. What problems are associated with prolonged mechanical ventilation?• Ventilator associated pneumonias, delay in
rehabilitation.
Slide 29
Slide 30 Q: How well are you able to diagnose this patient?A: Show how trauma studies can be very limited.Q: What is the main finding you can see?A: Wide mediastinum.Q: What diagnosis do you worry most about in this setting?A: TAIQ: What else might widen mediastiinum?A: Fat, blood, mass, poor inspiration, aneurysm, thymus (babies)Q: Should we attribute the wide mediastinum to fat in this
obese child and spare him the radiation?A: see next slide…
Slide 31 Q: What do you think is the diagnosis?A: Traumatic aortic rupture confirmed on CTA.Q: How can we balance need for diagnosis with need to protect children from radiation inmedical CT?A: Risk vs benefit analysis. Risk of missed aortic rupture much more immediate and grave than the radiation risk in this setting.Q: What projection is this?A: Coronal.
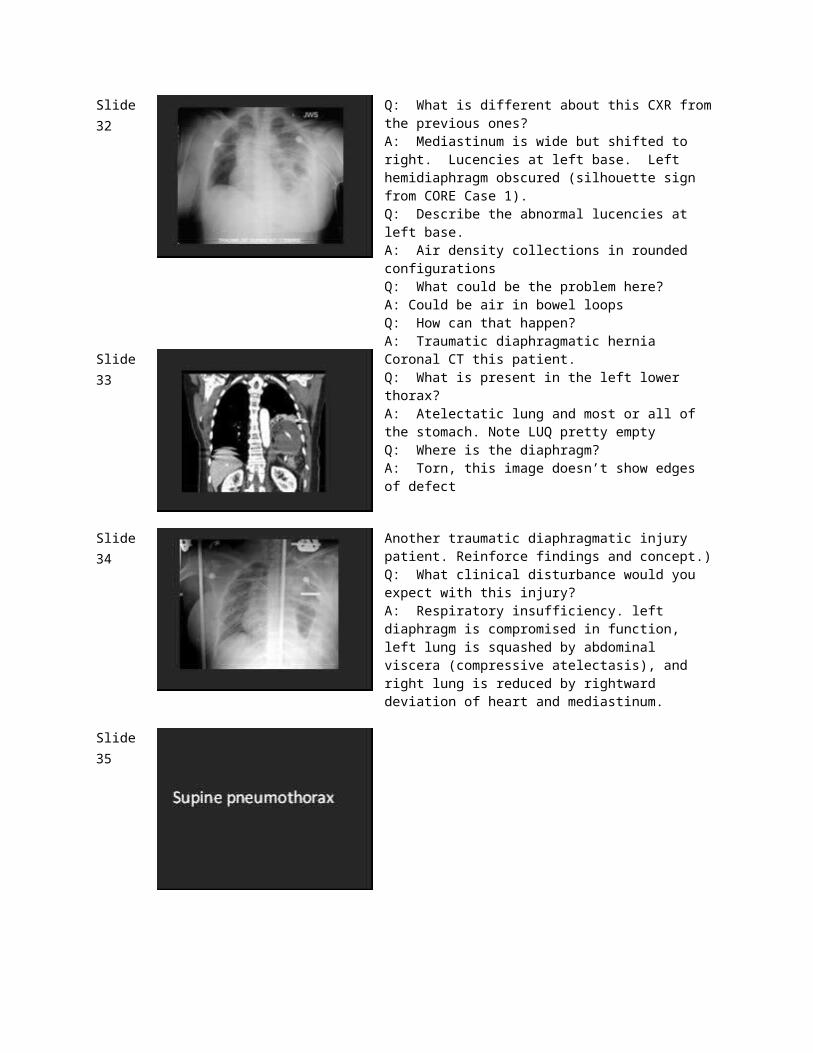
Slide 32 Q: What is different about this CXR from the previous ones?A: Mediastinum is wide but shifted to right. Lucencies at left base. Left hemidiaphragm obscured (silhouette sign from CORE Case 1).Q: Describe the abnormal lucencies at left base.A: Air density collections in rounded configurationsQ: What could be the problem here?A: Could be air in bowel loopsQ: How can that happen?A: Traumatic diaphragmatic hernia
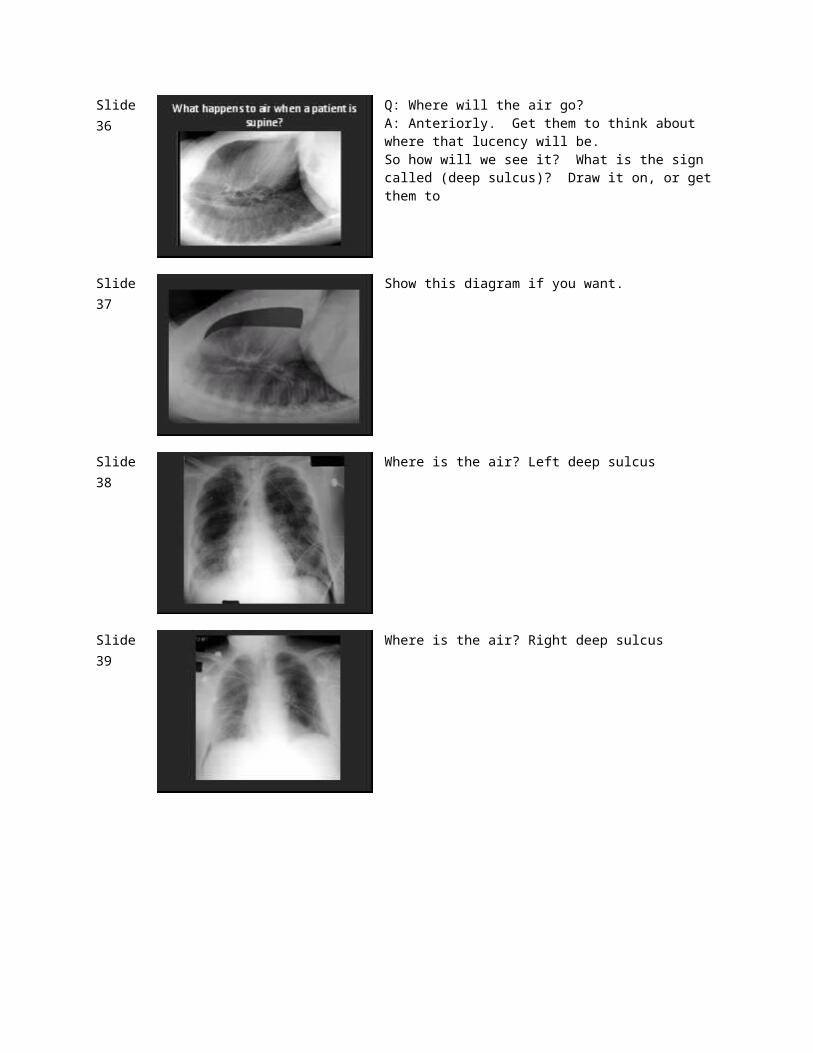
Slide 33 Coronal CT this patient.Q: What is present in the left lower thorax?A: Atelectatic lung and most or all of the stomach. Note LUQ pretty emptyQ: Where is the diaphragm?A: Torn, this image doesn’t show edges of defect
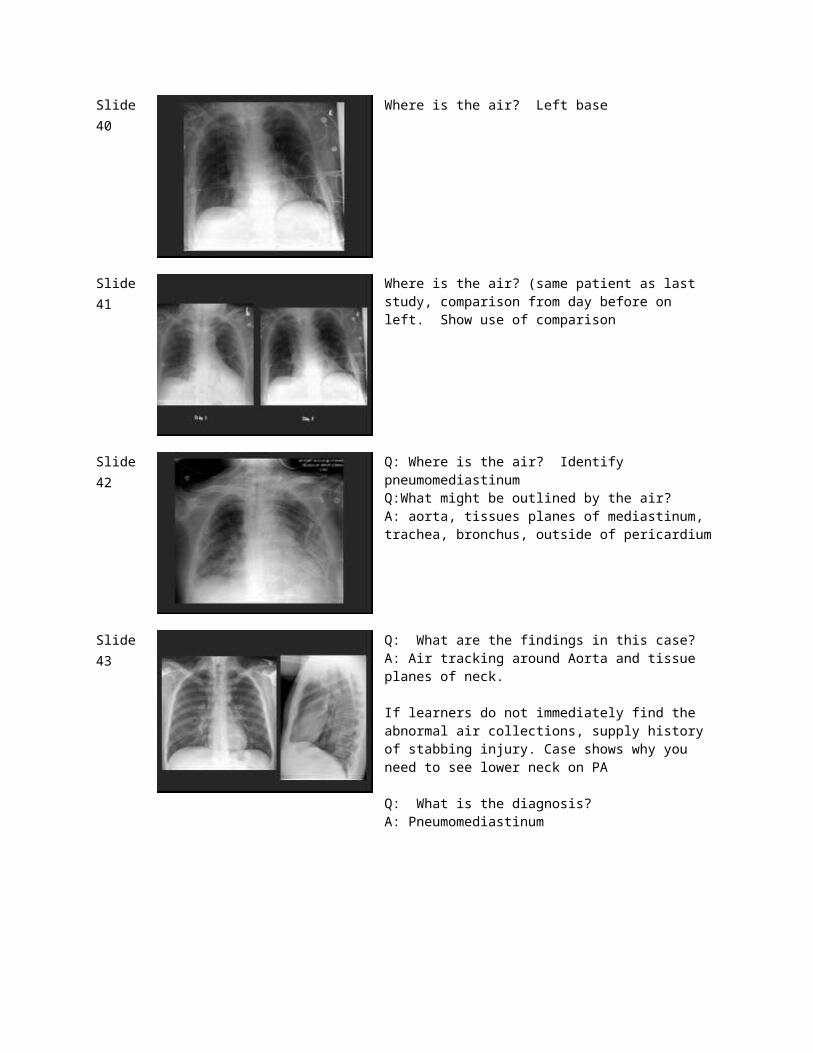
Slide 34 Another traumatic diaphragmatic injury patient. Reinforce findings and concept.)Q: What clinical disturbance would you expect with this injury?A: Respiratory insufficiency. left diaphragm is compromised in function, left lung is squashed by abdominal viscera (compressive atelectasis), and right lung is reduced by rightward deviation of heart and mediastinum.
Slide 35
Slide 36 Q: Where will the air go?A: Anteriorly. Get them to think about where that lucency will be.So how will we see it? What is the sign called (deep sulcus)? Draw it on, or get them to
Slide 37 Show this diagram if you want.
Slide 38 Where is the air? Left deep sulcus
Slide 39 Where is the air? Right deep sulcus
Slide 40 Where is the air? Left base
Slide 41 Where is the air? (same patient as last study, comparison from day before on left. Show use of comparison
Slide 42 Q: Where is the air? Identify pneumomediastinumQ:What might be outlined by the air?A: aorta, tissues planes of mediastinum, trachea, bronchus, outside of pericardium
Slide 43 Q: What are the findings in this case?A: Air tracking around Aorta and tissue planes of neck.
If learners do not immediately find the abnormal air collections, supply history of stabbing injury. Case shows why you need to see lower neck on PA
Q: What is the diagnosis?A: Pneumomediastinum
Slide 44 spontaneous, trauma, iatrogenic, vomiting, tumor, etc
Q: What kind of traumatic injury could cause this? Blunt trauma compressing chest with closed glottis and rupture of an airway, penetrating trauma (i.e., stabbing injury)
Slide 45 Q: What are the lucencies in the skin caused by?A: Extensive subcutaneous air dissects through the tissues.Q: What diagnostic problem may arise with extensive subcutaneous air?A: The subcutaneous air shadows may mask other abnormal air collections.Q: Does this patient have other abnormal air collections?A: Pneumomediastinum and hydropneumothorax (horizontal line on left, as taught in CORE Case 2)
Slide 46 Same patient as the last. Can they find and account for all the air collections?
Slide 47 Same patient as the last. Can they point out all the air collections?A: SubQ emphysema, pneumomedastinum, left hydropneumothorax
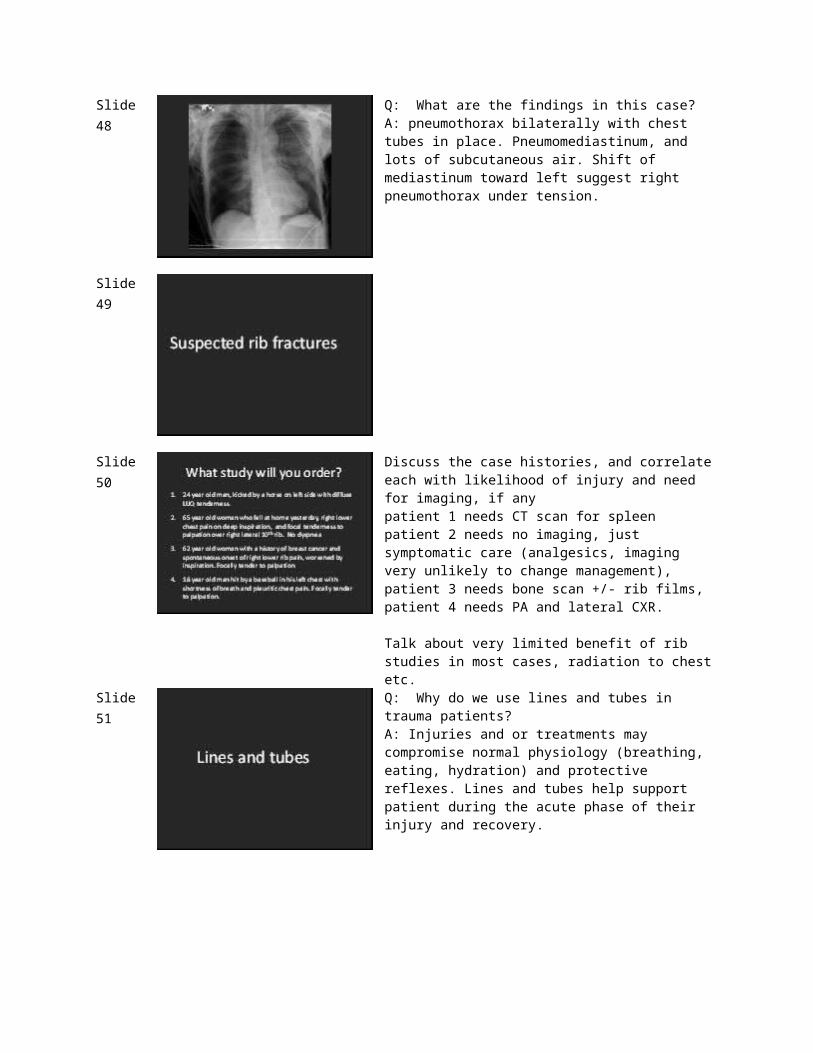
Slide 48 Q: What are the findings in this case?A: pneumothorax bilaterally with chest tubes in place. Pneumomediastinum, and lots of subcutaneous air. Shift of mediastinum toward left suggest right pneumothorax under tension.
Slide 49
Slide 50 Discuss the case histories, and correlate each with likelihood of injury and need for imaging, if anypatient 1 needs CT scan for spleenpatient 2 needs no imaging, just symptomatic care (analgesics, imaging very unlikely to change management),patient 3 needs bone scan +/- rib films,patient 4 needs PA and lateral CXR.
Talk about very limited benefit of rib studies in most cases, radiation to chest etc.
Slide 51 Q: Why do we use lines and tubes in trauma patients?A: Injuries and or treatments may compromise normal physiology (breathing, eating, hydration) and protective reflexes. Lines and tubes help support patient during the acute phase of their injury and recovery.
Slide 52 Normal line positions. Get students to draw or you draw(INCLUDE OR REPLACE BY FOLLOWING SLIDES?)
Slide 53 What is the line? Where is it? (PICC in SVC)
Slide 54 What is the line? Where is it? (PICC in SVC)
Slide 55 What is the line? Where is it? (RIJ in SVC)
Slide 56 What is the line? Where is it? (RIJ in SVC)
Slide 57 Q: What is the line? Where is it?A: ETT mid trachea)Q: What is a good position for an ETT?A: Normal ETT placement w/ tip at ~1/2 b/t carina and medial clavicle.Q: How can we see lines and tubes better? A: adjust evel and window, CLARE or similar filter
Slide 58 Q: What is the line? Where is it?A: ETT mid trachea)Q: What is a good position for an ETT?A: Normal ETT placement w/ tip at ~1/2 b/t carina and medial clavicle.Q: How can we see lines and tubes better?A: adjust level and window, CLAHE (contrast limited adaptive histogram equalization) or similar filter
Slide 59 Q: What are the tubes?A: chest tubesQ: Are these most likely draining air or fluid? Why?A: Air as at apices.
Slide 60 Q: What are the tubes?A: chest tubesQ: Are these most likely draining air or fluid? Why?A: Air as at apices.
Slide 61 Pigtail catheter, (also RIJ, ETT, gastric)
Slide 62 Pigtail catheter, (also RIJ, ETT, gastric)

Slide 63 Q: What is the line?A: Swan Ganz in proximal left PAQ: Where do you want these?A: the tip of the catheter should not extend distal to the main pulmonary artery, except momentarily to measure a pulmonary capillary wedge pressure (LV end diastolic pressure), then pulled back.Q: What if the Swan-Ganz catheter is left too far distal?A: Vascular injury (Pulmonary artery pseudoaneurysm) which can result in fatal hemorrhage.
Slide 64 Q: What is the line?A: Swan Ganz in proximal left PAQ: Where do you want these?A: the tip of the catheter should not extend distal to the main pulmonary artery, except momentarily to measure a pulmonary capillary wedge pressure (LV end diastolic pressure), then pulled back.Q: What if the Swan-Ganz catheter is left too far distal?A: Vascular injury (Pulmonary artery pseudoaneurysm) which can result in fatal hemorrhage.
Slide 65 Normal tube positions. Get students to draw or you draw
Slide 66 Q: What is this tube? How do you recognize it?A: Feeding tube. (Dobhoff) Metallic type – get them to think about why we have that (to help peristalsis transit beyond pylorus)Q: Why past the pylorus?A: reduce reflux

Slide 67 Q: What is this tube? How do you recognize it?A: Feeding tube. (Dobhoff) Metallic type – get them to think about why we have that (to help peristalsis transit beyond pylorus)Q: Why past the pylorus?A: reduce reflux
Slide 68 Q: What is the tube?A: GastricQ: Where should it be?: In body of stomachQ: Where might we see it misplaced?A: pharynx, esophagus, bronchus
Slide 69 Q: What is the tube?A: GastricQ: Where should it be?A: In body of stomachQ: Where might we see it misplaced?A: pharynx, esophagus, bronchus
Slide 70 Q: Are you happy with this radiograph on your patient?A: No !!Q: Why not?A: ETT is misplaced in the Right mainstem bronchus
Slide 71 If malposition of the ETT is allowed to persist, ETT in RMB produces left lung atelectasis, with respiratory compromise
Slide 72 Q: What is this line?A: Dobhoff feeding tubeQ: Where is it?A: in LLL bronchus
Slide 73 Q: What about these lines?A: Normal lines,
Ask learners to identify these, if time permits. Task shows problems of trying to carefully track multiple lines on an ICU patient , working out which are overlying etc.
Slide 74 So, for this patient’s radiograph, the X-ray consult form states “check Dobhoff” (Exercise to emphasize Importance of looking at corners of image.)
Q: So, what will be your report for this image? (Some learners will only find the NGT, the pitfall we hope to highlight)A: Dobhoff feeding tube is misplaced in Right mainstem bronchus, and a nasogastric tube (NGT) terminates in stomach
(This case reinforces the point of getting a ‘low chest’ rather than a KUB for enteric tubes)
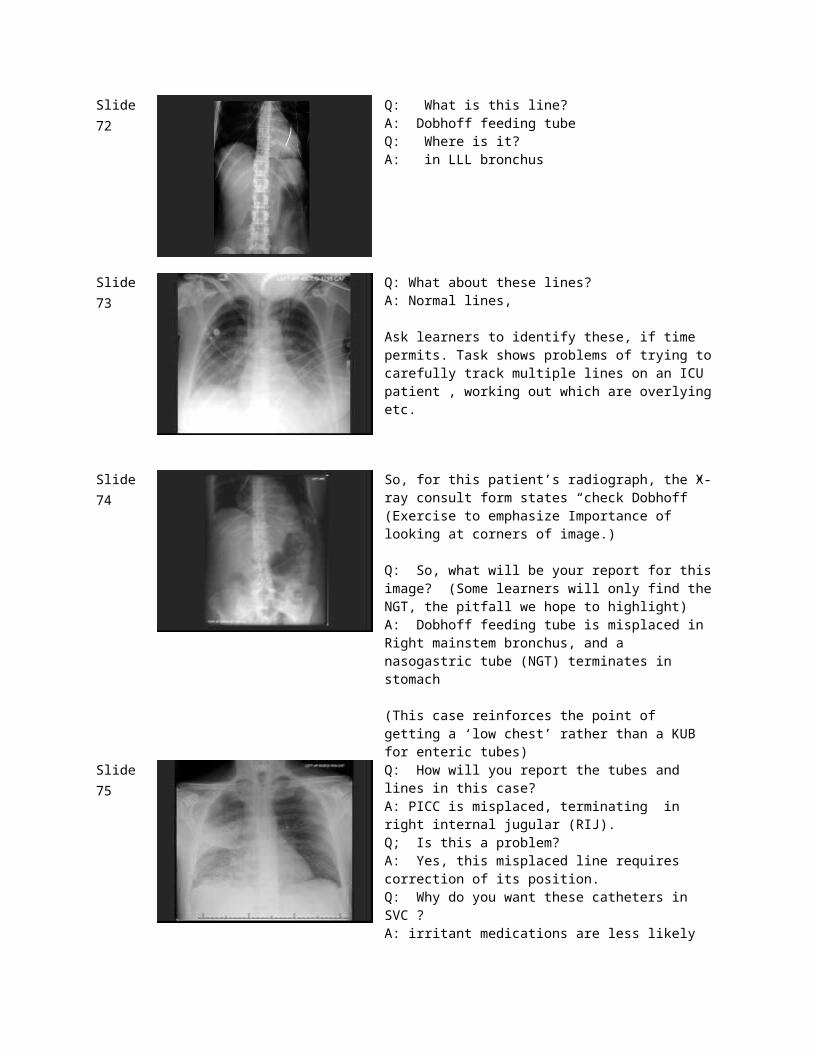
Slide 75 Q: How will you report the tubes and lines in this case?A: PICC is misplaced, terminating in right internal jugular (RIJ).Q; Is this a problem?A: Yes, this misplaced line requires correction of its position.Q: Why do you want these catheters in SVC ?A: irritant medications are less likely to irritate the high flow, high volume SVC, reducing risk of phlebitis relative to small veins. Thrombosis risk is lower in SVC than in a smaller vein.Q: What additional problems?A: Vagal stimulation – this patient fainted every time they flushed the line.
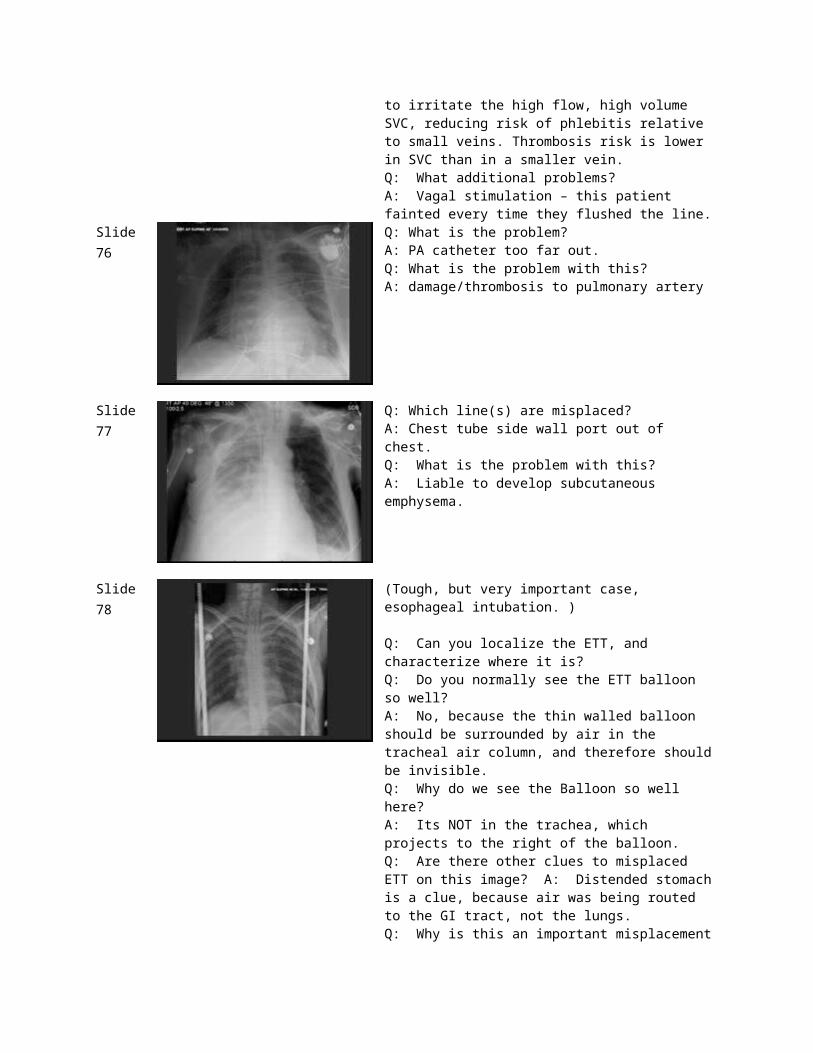
Slide 76 Q: What is the problem?A: PA catheter too far out.Q: What is the problem with this?A: damage/thrombosis to pulmonary artery
Slide 77 Q: Which line(s) are misplaced?A: Chest tube side wall port out of chest.Q: What is the problem with this?A: Liable to develop subcutaneous emphysema.
Slide 78 (Tough, but very important case, esophageal intubation. )
Q: Can you localize the ETT, and characterize where it is?Q: Do you normally see the ETT balloon so well?A: No, because the thin walled balloon should be surrounded by air in the tracheal air column, and therefore should be invisible.Q: Why do we see the Balloon so well here?A: Its NOT in the trachea, which projects to the right of the balloon.Q: Are there other clues to misplaced ETT on this image? A: Distended stomach is a clue, because air was being routed to the GI tract, not the lungs.Q: Why is this an important misplacement to recognize? A: As occurred in this trauma patient intubated in the field, anoxic brain injury and death are the predicatable result
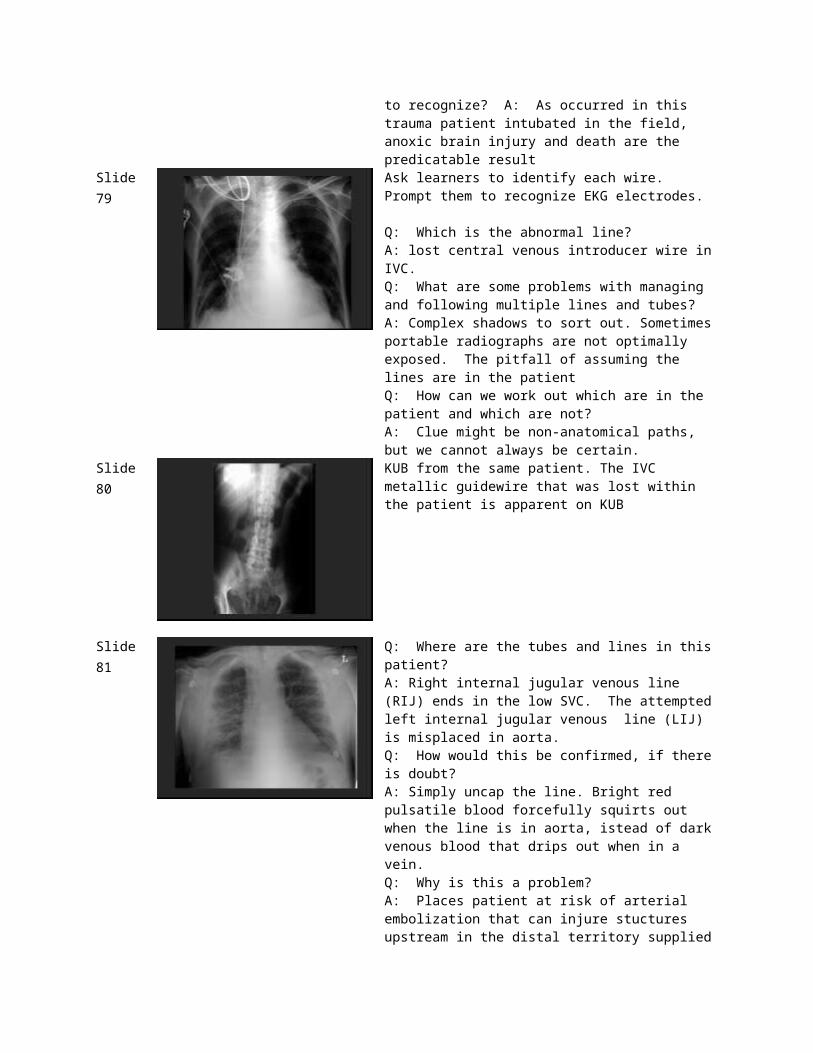
Slide 79 Ask learners to identify each wire. Prompt them to recognize EKG electrodes.
Q: Which is the abnormal line?A: lost central venous introducer wire in IVC.Q: What are some problems with managing and following multiple lines and tubes?A: Complex shadows to sort out. Sometimes portable radiographs are not optimally exposed. The pitfall of assuming the lines are in the patientQ: How can we work out which are in the patient and which are not?A: Clue might be non-anatomical paths, but we cannot always be certain.
Slide 80 KUB from the same patient. The IVC metallic guidewire that was lost within the patient is apparent on KUB
Slide 81 Q: Where are the tubes and lines in this patient?A: Right internal jugular venous line (RIJ) ends in the low SVC. The attempted left internal jugular venous line (LIJ) is misplaced in aorta.Q: How would this be confirmed, if there is doubt?A: Simply uncap the line. Bright red pulsatile blood forcefully squirts out when the line is in aorta, istead of dark venous blood that drips out when in a vein.Q: Why is this a problem?A: Places patient at risk of arterial embolization that can injure stuctures upstream in the distal territory supplied by the artery
Slide 82
Slide 83 This paitent’s CTA. Get them to identify the CT findings and how they produce the CXR findings
Slide 84 Another patient’s CTA,A Which CXR findings might you see in this patient?A: widened mediastinum, effusion, loss of the paraaortic line.
Slide 85 Another example





























