Embed Size (px)
Citation preview

CASE 409: A 48 y/o woman collapses suddenly at home

History• A 48-year-old obese (312 lbs) woman was brought to the
Emergency Room by the Rescue Squad and was pronounced dead after all attempts at resuscitation failed. According to relatives, the decedent was watching TV, munching chips and dip, and drinking beer, when all of a sudden she stood up, gasped, grabbed her chest, and fell to the floor, upsetting the table. She hit her head on the edge of the table as she fell. The patient had had a long history of medical problems and was currently being seen in the Creighton Clinic for a variety of illnesses, including type II diabetes mellitus, hypertension, and chronic obstructive pulmonary disease. Her relatives claimed she drank heavily, but was not particularly "soused" on the day of her collapse. She had complained of swelling of the ankles and pain in the lower legs for the last several days.

• List the causes of sudden death.• Does the coroner need to be contacted? Who will sign
the death certificate?• Postmortem examination revealed an obese woman
appearing older than the stated age of 48. There was a recent laceration on the forehead. The only other significant external finding was an obvious erythema of the right leg below the knee and an obvious increase in circumference of the right calf as compared to the left. Internal examination revealed a massive “saddle” embolus in the pulmonary artery and marked visceral congestion. Calculi were present in the gallbladder and mild fatty change was noted in the liver (liver wt. 2100 g). Blood alcohol level was 120 mg/dL (0.12% v/v). Alcohol, caffeine, nicotine, and propranolol were found in the toxicologic screen of the urine.

What was found!

Cut section of lungThromboembolusbronchus

Micro of a Pulmonary Artery occluded with a thromboembolus- note lines of Zahn

Thrombus in deep leg vein-vein opened up

• What is the cause of death? Describe the mechanism of death and the pathogenesis of this process.
• Why aren't there infarcts in the lung in this case? If there were infarcts, how would they look, grossly and microscopically?
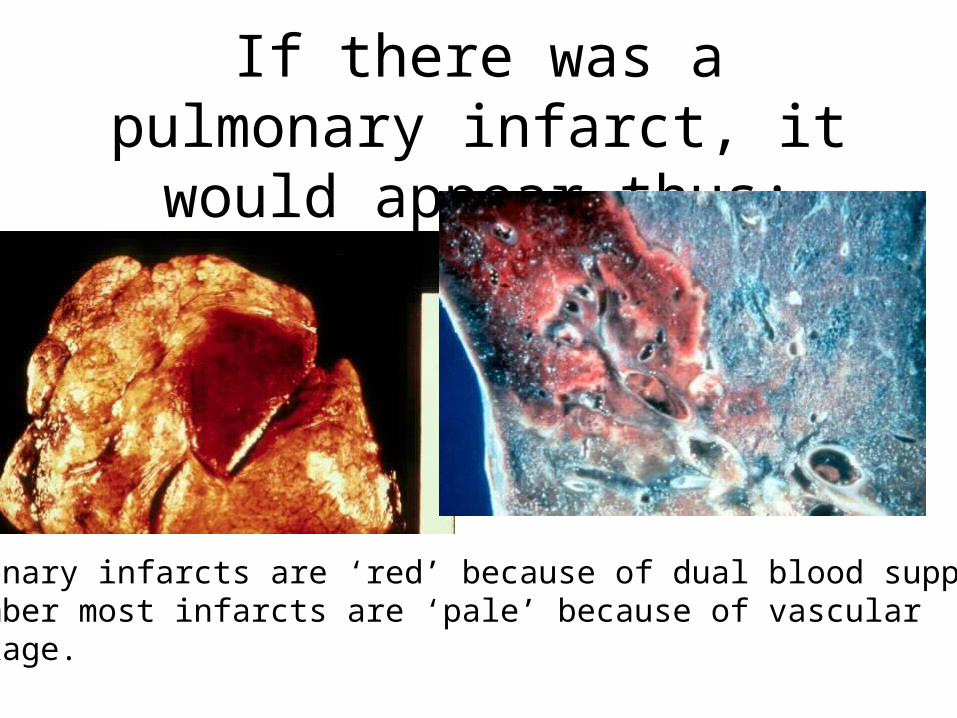
If there was a pulmonary infarct, it would appear thus:
Pulmonary infarcts are ‘red’ because of dual blood supply- Remember most infarcts are ‘pale’ because of vascular Blockage.

Pulmonary infarct

Other findings at autopsy:Chronic cholecystitis with cholelithiasis

Fatty change of the liver (wt 2100gms) (Yellow & pale)

• What are the usual predisposing conditions to pulmonary thromboemboli?
• What are the usual sources of pulmonary thromboemboli? Of systemic thromboemboli?
• What is the usual outcome of massive pulmonary emboli? Of smaller pulmonary emboli? What are the consequences of chronic pulmonary embolism?
• What are the common clinical signs and symptoms of pulmonary thromboemboli (non-saddle type)?
• Are there any characteristic laboratory or ECG findings to help diagnose PE?
• What are some management strategies to help prevent recurrent PE?

Discuss other types of embolism including gas, fat, amniotic fluid, and bone marrow.
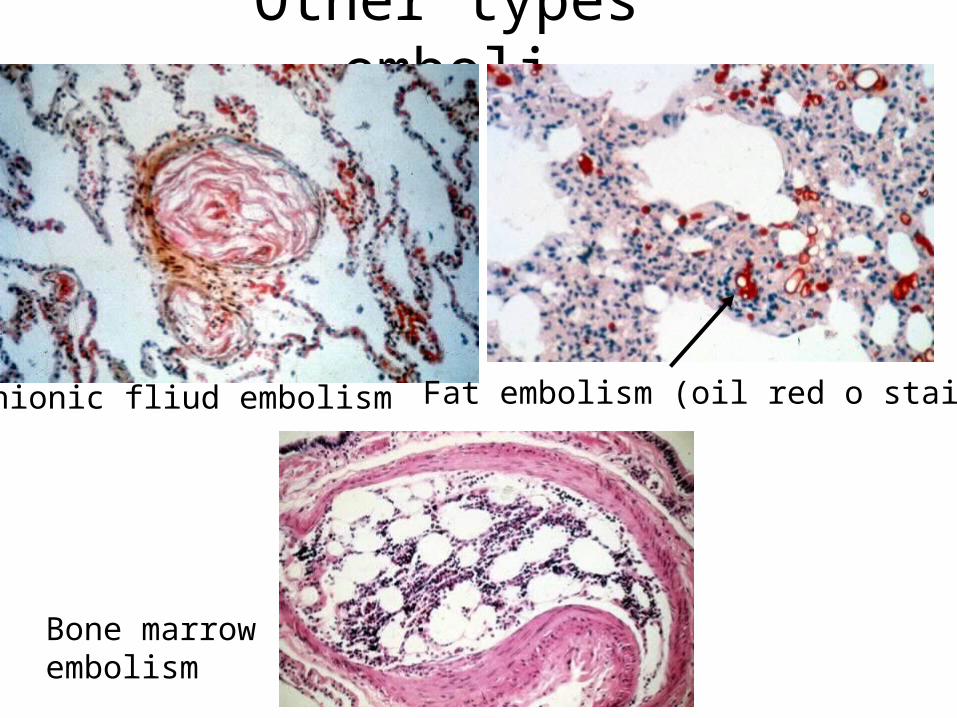
Other types emboli
Amnionic fliud embolism Fat embolism (oil red o stain)
Bone marrowembolism