Embed Size (px)
Citation preview
8 National Institute of Mental Health and Neuro Sciences
Common Infections of the Nervous System
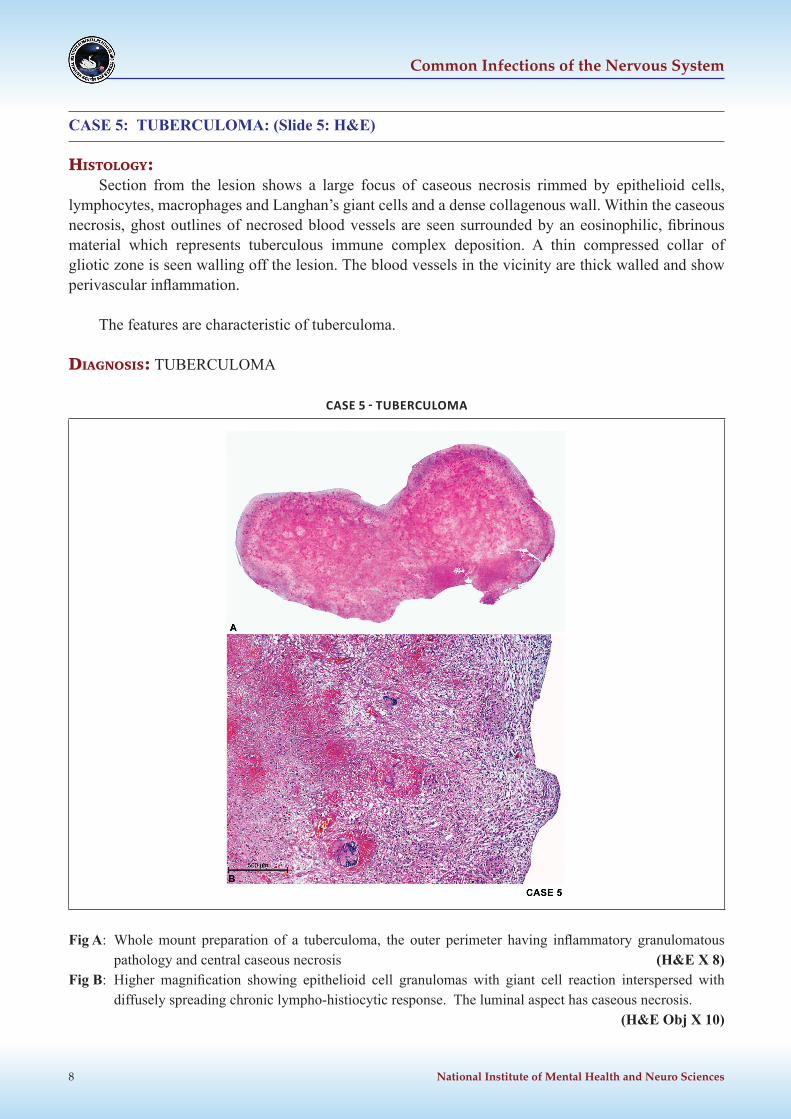
CASE 5: TUBERCULOMA: (Slide 5: H&E)
HIstology:Section from the lesion shows a large focus of caseous necrosis rimmed by epithelioid cells,
lymphocytes, macrophages and Langhan’s giant cells and a dense collagenous wall. Within the caseous necrosis, ghost outlines of necrosed blood vessels are seen surrounded by an eosinophilic, fibrinous material which represents tuberculous immune complex deposition. A thin compressed collar of gliotic zone is seen walling off the lesion. The blood vessels in the vicinity are thick walled and show perivascular inflammation.
The features are characteristic of tuberculoma.
dIagnosIs: TUBERCULOMA
CASE 5 - TUBERCULOMA
Fig A: Whole mount preparation of a tuberculoma, the outer perimeter having inflammatory granulomatous pathology and central caseous necrosis (H&E X 8)
Fig B: Higher magnification showing epithelioid cell granulomas with giant cell reaction interspersed with diffusely spreading chronic lympho-histiocytic response. The luminal aspect has caseous necrosis.
(H&E Obj X 10)

Human Brain Bank, NIMHANS, Bangalore 9
Bacterial Infections
Spectrum of pathology caused by Mycobacterium tuberculosis: Tuberculous Meningitis, Tuberculous Abscess, Tuberculoma)
Mass Lesion : Tuberculoma, with central caseous necrosis similar to lymph node and pulmonary lesions Chronic basal arachnoiditis with or without hydrocephalusTuberculous abscess : Acute disease. The wall contains granulomas and Acid Fast Bacilli (AFB)HIV + TBM : Thin basal exudates, poorly formed granulomas, basal smear positive for Mycobacteria inside macrophages and extracellular space.Diagnosis : CSF examination, culture, Bactec, PCR available (keep limitations in mind while interpreting the diagnosis based on PCR)
The most common mode of presentation of neurotuberculosis is tuberculous meningitis, the other forms being tuberculoma, tuberculous abscess, encephalopathy and radiculomyelitis. The incidence of tuberculous meningitis (TBM) in patients with systemic tuberculosis ranges from 7-12%.
TBM is more correctly characterized as a meningoencephalitis because it affects not only the meninges but also the adjacent parenchyma and vasculature of the brain as well. It results from the discharge of tubercle bacilli directly into the subarachnoid space from a caseous focus (Rich’s focus) located most often in the base of the brain in a subcortical location or in the choroid plexus. Occasionally, the meninges are infected by a direct spread from a neighboring focus of infection in the middle ear or spine.
Meningeal tuberculosis occurs in four forms: as disseminated miliary tubercles, a focal caseous plaque, proliferative organising meningitis or acute caseous inflammatory meningitis which is the commonest form causing significant tissue destruction. The exudate in TBM typically fills the basal and prepontine cisterns and extends anteriorly along the floor of the III ventricle to the chiasmatic cisterns where it envelops the optic nerves to track along the Sylvian fissures. In advanced cases, tiny tubercles develop along the blood vessels. The thick fibrinous exudate in the basal cisterns can block the IV ventricular outlets and cause obstructive hydrocephalus.
Microscopically, in the acute exudative phase, the exudate consists of polymorphs, RBCs, macrophages and lymphocytes within a network of fibrin when it is reminiscent of pyogenic meningitis. As the disease progresses, it enters the proliferative phase when lymphocytes predominate accompanied by fibroblasts which lay down collagen. The macroscopic tubercles correspond to foci of caseation. The gross appearance of the exudate parallels the histologic progression and is accordingly graded as Grade I when the exudate is thin and the cerebral vessels are clearly visible through it, grade II when the exudate is thicker and the vessels are less clearly apparent and grade III when a thick fibrinous exudate totally obscures the vessels at the base of the brain, from the view. The number of Mycobacteria within the exudate is highly variable.
The small and medium sized arteries in the vicinity of the exudate show evidence of vasculitis. The inflammation can involve the veins and capillaries as well and may proceed to fibrinoid necrosis with resultant thrombosis or a reactive subendothelial cellular proliferation completely occluding the lumen leading to endarteritis obliterans. These vessel changes are responsible for the ischemic sequelae of TBM such as infarction, which is seen most often in the territory of the middle cerebral artery (reflecting the presence of the exudate within the Sylvian fissure). Infarction can also involve the basal ganglia and hypothalamus due to involvement of the perforating vessels. One of the common causes for rapid
10 National Institute of Mental Health and Neuro Sciences
Common Infections of the Nervous System
deterioration and death is infarction of the brain stem involving the vital centers. Partial or total blocking of the foramina of Lushka by thick fibrinous exudates in the basal cisterns leads to a communicating or obstructive hydrocephalus. In the brain parenchyma adjacent to zones of thick adherent exudates, a “border zone reaction” of edema, perivasculitis and gliosis can develop.
Tuberculomas are intracranial mass lesions with a predilection for the cerebellum, the pontine tegmentum, and the paracentral lobule of the parietal cortex. They are round to oval masses ranging from 2-12mm and result from fusion of several smaller nodules akin to matting of tuberculous lymph nodes. On sectioning, the center is necrotic but firm with a grey, gelatinous but tough rim and a surrounding narrow zone of gliosis. Perilesional edema is variable and the mass is usually easily separable from the adjoining parenchyma. Microscopically, they are composed of a caseous center surrounded by a granulomatous reaction that includes lymphocytes, giant cells and fibrosis of variable degree. Ziehl-Neelsen stain may demonstrate the acid fast bacilli. Tuberculomas may spontaneously become cystic, fibrous and calcified; lose their bacilli and the inflammatory exudate. With advances in imaging and effective antibiotic therapy, tuberculomas are rarely resected nowadays.
With the AIDS epidemic, tuberculous abscesses are being encountered more often. This term is used when the lesion has a necrotic center surrounded by a capsule like a true abscess, but is devoid of the granulomatous reaction and giant cells, but teaming with acid fast bacilli. The absence of a granulomatous reaction to the tubercle bacilli suggests failure of immune mechanisms. They have to be distinguished from pseudo abscesses formed by liquefaction of the caseous material in tuberculomas. In India, tuberculosis has been the most common opportunistic infection in AIDS patients. But in these patients, it is essential to exclude both Toxoplasma and Cryptococcal infections before labeling the case as one of tuberculous etiology as both are notorious to masquerade as tuberculosis on neuroimaging and clinical features.
Whitener proposed the following diagnostic criteria for tuberculous abscess.(a) Macroscopic evidence of a tuberculous abscess in the brain has a central cavity with pus.(b) Histological evidence of the abscess being composed of inflammatory granulation tissue containing
acute and chronic inflammatory cells, particularly polymorphonuclear leucocytes.(c) Proof of mycobacterial pathology by either positive culture of the pus or demonstration of acid fast
organisms in the abscess wall or the pus.
cHronIc menIngItIs
Common causes of chronic meningitis Infectious Non Infectious Mycobacterium tuberculosis Carcinoma Cryptococcus neoformans Sarcoid Treponema pallidum Granulomatous angiitis Candidiasis SLE Brucellosis Behcet’s disease Toxoplasmosis Subarachnoid haemorrhage Nocardiosis Drug/chemical toxicity Lyme disease Post infections allergic Pheohyphomycosis Encephalomyelitis Cysticercosis Actinomycosis Partially treated bacterial meningitis