Embed Size (px)
Citation preview

ORIGINAL CONTRIBUTION
Case Finding for Cognitive Impairment in Elderly Emergency Department Patients
From the Division of Community Health Sciences* and Department of Internal Medicine, 1 Emergency Medicine, ~ and Family Medicine,~ Northeastern Ohio Universities College of Medicine, Rootstown, Ohio, and the Departments of Medicine," Emergency Medicine, # and Family Practice, ~* Summa Health System, Akron City Hospital, Akron, Ohio.
Received for publication April 28, 1993. Revision received July 21, 1993. Accepted for publication August 3, 1993.
Paper presented at Society for Academic Emergency Medicine Annual Meeting, May 1993.
This study was supported in part by Grant #3205from the Ohio Department of Affmg, Alzheimer's Research and Diagnostic Center.
Lowell W Gerson, PhD*
Steven R Counsell, MD TM
Phil B Fontanarosa, MD, FACEP ~
William D Smucker, MD*§**
See related editorial page 873.
Study objectives: To determine the feasibility of a case- finding program for cognitive impairment in elderly emergency department patients, and to describe the prevalence of cognitive impairment in screened patients and identify factors associated with impairment.
Design: A three-month cross-sectional study. The six-item 0rientation-Memory-Concentration (0MC) Test was admi- nistered to eligible patients.
Setting: Community teaching hospital with annual ED census of 69,000 adults.
Participants: All patients 65 years of age and older physically able to communicate and without a prior diagnosis of dementia were eligible. Five hundred forty-seven of 958 patients (59%) were interviewed; only 95 (10%) refused. Other reasons for exclusion were too ill, 113 (12%); other (sleeping, privacy, repeat visits, incomplete forms), 99 (10%); known dementia, 59 (6%); and communication problems, 45 (5%).
Results: A mean time of 1.9 minutes (+0.91 SD) was required to complete the test. One hundred eighty-three of 547 patients (33.5%) had scores that indicated at least moderate cognitive impairment. Logistic regression analyses identified two factors associated with impairment: age of more than 80 years (odds ratio, 3.68; 95% confidence interval, 2.21-6.14)and residence in a nursing home (odds ratio, 13.8; 95% confidence interval, 3.79-50.2).
Conclusion: Screening for cognitive impairment in elderly ED patients using the 0MC Test is feasible. There is a high preva- lence of cognitive impairment in elderly ED patients, and the prevalence increases with age. Identification of cognitive impair- ment is important in the assessment of elderly ED patients and may affect clinical evaluation, patients' understanding of medi- cal information, and compliance with discharge instructions.
APRIL 1994 23:4 ANNALS OF EMER6ENCY MEDICINE 813
ORIGINAL CONTRIBUTION
Case Finding for Cognitive Impairment in
Elderly Emergency Department Patients
From the Division of CommunityHealth Sciences * and Departmentof Internal Medicine, t EmergencyMedicine, f and Family Medicine, §
Northeastern Ohio UniversitiesCollege of Medicine, Rootstown, Ohio,and the Departments of Medicine, II
Emergency Medicine, # and FamilyPractice, .. Summa Health System,Akron City Hospital, Akron, Ohio.
Received for publicationApril 28, 1993. Revision receivedJuly 21, 1993. Accepted forpublication August 3, 1993.
Paper presented at Society forAcademic Emergency MedicineAnnual Meeting, May 1993.
This study was supported in partby Grant #3205 from the OhioDepartment ofAging, Alzheimer'sResearch and Diagnostic Center.
Lowell W Gerson, PhD*
Steven RCounsell. MOtU
Phil BFontanarosa. MD. FACEP*'William 0 Smucker, MD*§**
See related editorial, page 873.
Study objectives: To determine the feasibility of acasefinding program for cognitive impairment in elderly emergencydepartment patients, and to describe the prevalence of cognitiveimpairment in screened patients and identify factors associatedwith impairment.
Design: Athree-month cross-sectional study. The six-itemOrientation-Memory-Concentration (OMC) Test was administered to eligible patients.
Setting: Community teaching hospital with annual ED census of69,000 adults.
Participants: All patients 65 years of age and older physicallyable to communicate and without aprior diagnosis of dementiawere eligible. Five hundred forty-seven of 958 patients (59%)were interviewed; only 95 (10%) refused. Other reasons forexclusion were too ill, 113 (12%); other (sleeping, privacy, repeatvisits, incomplete forms). 99 (10%); known dementia, 59 (6%);and communication problems, 45 (5%).
Results: A mean time of 1.9 minutes (±0.91 SO) was requiredto complete the test. One hundred eighty-three of 547 patients(33.5%) had scores that indicated at least moderate cognitiveimpairment. Logistic regression analyses identified two factorsassociated with impairment: age of more than 80 years (oddsratio, 3.68; 95% confidence interval, 2.21-6.14) and residencein anursing home (odds ratio, 13.8; 95% confidence interval.3.79-50.2).
Conclusion: Screening for cognitive impairment in elderly EDpatients using the OMC Test is feasible. There is ahigh prevalence of cognitive impairment in elderly ED patients, and theprevalence increases with age. Identification of cognitive impairment is important in the assessment of elderly ED patients andmay affect clinical evaluation, patients' understanding of medical information, and compliance with discharge instructions.
APRIL 1994 23:4 ANNALS OF EMERGENCY MEDICINE 813

CASE FINDING Gerson et al
[Gerson LW, Counsell SR, Fontanarosa PB, Smucker WD: Case finding for cognitive impairment in elderly emergency depart- ment patients. Ann Emerg Med April 1994;23:813-817.]
INTRODUCTION
Cognitive impairment is an important problem that affects 5% to 10% of people older than age 65.1 Age is a consis- tent risk factor, with one-half of those 85 years and older having dementia. 2 The Society for Academic Emergency Medicine Geriatric Emergency Medicine Task Force con- sidered the effect cognitive impairment has on the clinical encounter in the emergency department and on patients' quality of life after discharge. They recommended that emergency physicians consider mental and functional sta- tus of elderly patients as part of the emergency encounter and as a preventive health measure) Although the ED has the potential to become an excellent location for identifying elderly patients with cognitive impairment and linking them to appropriate services for further evaluation and treatment, this role has not been evaluated.
We designed this study with two objectives toward this end. The first was to determine the feasibility of a case- finding program for cognitive impairment in elderly ED patients. The second was to describe the prevalence of cognitive impairment in screened patients and to identify factors associated with impairment.
Figure. Orientation-Memory-Concentration Test
Score of 1 for each incorrect item. 1. What year is it now? 2. What month is it now?
Memory phrase-"Repeat this phrase after me: John Brown, 42 Market Street, Chicago"
3. About what time is it? (with,n one hour) 4. Count backward from 20 to 1 5. Say the months in reverse order
(Oecember, November, October, September, August, July, June, May, April March, February, January)
6. Repeat the memory phrase
1 X 4 = 1 X 3 =
ScoreO-5: No impairment Score 6 -1 O: Minimal impairment Score >10: Implies presence of dementia Score 11-21: Moderate impairment Score_> 22: Severe impairment
1 X 3 = 2 X 2 = 2 X 2 =
5 X 2 =
Total
MATERIALS AND METHODS
The study was performed in a midwestern community teaching hospital with 69,000 adult ED visits a year. The case-finding program was conducted from March 1, 1992, through May 31, 1992. All patients age 65 years and older treated in the ED during shifts as described below were asked to participate in the study. Only the initial visit was included for patients who visited the ED more than once during the study period. Patients were excluded if they refused to participate, their physical condition prevented their participation, they had a known dementia, or they were unable to communicate in English.
The ED social worker interviewed all patients who were evaluated during the day shift (7:00 AM to 3:00 PM) Monday through Friday. The remaining shifts were strati- fied into three blocks: evenings (3:00 eM to 11:00 PM), weekend days (7:00 AM to 3:00 PM), and nights (11:00 eM to 7:00 AM). Medical students trained in administering the screening instrument interviewed patients during these shifts. Five shifts per week were randomly selected in a 3:2:1 ratio to approximate patient flow patterns and cor- respond to student availability.
The screening instrument used was the six-item Orientation-Memory-Concentration (OMC) Test (Figure). 4 This is a shortened version of the original Information- Memory-Cognition Mental Status Test developed by Blessed and coworkers. 5 A weighted score of more than ten on the OMC Test is indicative of at least moderate cognitive impairment#
The interviewers recorded the time it took to complete the test and reviewed medical records to abstract informa- tion that may be associated with dementia, including sex,
Table 1. Characteristics of study patients
Characteristic Proportion %
Women 338/520 650 Age __80 yr* 179/518 34.6 Residing in nursing home 33/410 8.0 Living alone 118/414 28.5 Discharge diagnoses (ICD)
Circulatory {390-459) 130/518 25.1 Symptoms, signs, ill-defined conditions (780-799) 108/518 20.8 Respiratory (460-519) 72/518 13.9 Digestive (570-579) 55/518 10.6 Injury (800-999) 52/518 10.0 Other 101/518 19.5
Admitted to hospital 269/519 51 8 *Mean age, 76.7 4-_ 7.7 SD.
8 1 4 ANNALS OF EMERGENCY MEDICINE 23:4 APRIL 1994
CASE FINDINGGerson et al
[Gerson LW. Counsell SR, Fontanarosa PB, Smucker WO: Casefinding for cognitive impairment in elderly emergency department patients. Ann Emerg Med April 1994;23:813-817.]
INTRODUCTION
Cognitive impairment is an important problem that affects5% to 10% of people older than age 65. 1 Age is a consistent risk factor, with one-half of those 85 years and olderhaving dementia. 2 The Society for Academic EmergencyMedicine Geriatric Emergency Medicine Task Force considered the effect cognitive impairment has on the clinicalencounter in the emergency department and on patients'quality of life after discharge. They recommended thatemergency physicians consider mental and functional status of elderly patients as part of the emergency encounterand as a preventive health measure. 3 Although the EDhas the potential to become an excellent location foridentifying elderly patients with cognitive impairmentand linking them to appropriate services for furtherevaluation and treatment, this role has not beenevaluated.
We designed this study with two objectives toward thisend. The first was to determine the feasibility of a casefinding program for cognitive impairment in elderly EDpatients. The second was to describe the prevalence ofcognitive impairment in screened patients and to identifyfactors associated with impairment.
Figure.Orientation-Memory-Concentration Test
MATERIALS AND METHODS
The study was performed in a midwestern communityteaching hospital with 69,000 adult ED visits a year. Thecase-finding program was conducted from March 1, 1992,through May 31, 1992. All patients age 65 years and oldertreated in the ED during shifts as described below wereasked to participate in the study Only the initial visit wasincluded for patients who visited the ED more than onceduring the study period. Patients were excluded if theyrefused to participate, their phYSical condition preventedtheir participation, they had a known dementia, or theywere unable to communicate in English.
The ED social worker interviewed all patients whowere evaluated during the day shift (7:00 AM to 3:00 PM)
Monday through Friday The remaining shifts were stratified into three blocks: evenings (3:00 PM to 11:00 PM),
weekend days (7:00 AM to 3:00 PM), and nights (11:00 PM to7:00 AM). Medical students trained in administering thescreening instrument interviewed patients during theseshifts. Five shifts per week were randomly selected in a3:2: 1 ratio to approximate patient flow patterns and correspond to student availability
The screening instrument used was the six-itemOrientation-Memory-Concentration (OMe) Test (Figure).4This is a shortened version of the original InformationMemory-Cognition Mental Status Test developed byBlessed and coworkers. 5 A weighted score of more thanten on the OMC Test is indicative of at least moderatecognitive impairment.4
The interviewers recorded the time it took to completethe test and reviewed medical records to abstract information that may be associated with dementia, including sex,
Score of 1for each incorrect item.1. What year is it now?2. What month is it now?
Memory phrase-"Repeat this phrase after me:John Brown, 42 Market Street, Chicago"
3. About what time is it? (within one houri 14. Count backward from 20 to 1 25. Say the months in reverse order 2
(December, November. October,
September, August, July,
June, May, April, March.
February, January)
6. Repeat the memory phrase 5
Score 0-5: No impairmentScore 6 -1 0: Minimal impairmentScore >10: Implies presence of dementiaScore 11-21: Moderate impairmentScore ~ 22: Severe impairment
X 4X 3
X 3X 2X 2
X 2 =
Total
Table 1.Characteristics of study patients
Characteristic
WomenAge ~80 yr*Residing in nursing homeLiving aloneDischarge diagnoses (ICD)
Circulatory (390-459)Symptoms, signs, ill-defined conditions 1780-799)Respiratory (460-5191Digestive (570-579)Injury (800-9991Other
Admitted to hospital
'Mean age, 76.7 ± 7.7 SO.
Proportion
338/520179/51833/410
118/414
130/518108/51872/51855/51852/518
101/518269/519
%
65.034.68.0
28.5
25.120.813.910.610019.5518
8 1 4 ANNALS OF EMERGENCY MEDICINE 234 APRIL 1994
CASE FINDING Gerson et al
age, living arrangement, discharge diagnoses, and hospital admission.
Logistic regression analyses were performed to identify factors associated with possible dementia. The first step in building the model was 2 x 2 comparisons. Significant factors (P < .05) using these unadjusted analyses then were entered in the logistic regression. Odds ratios (OR) with 95% confidence intervals (CI) were calculated for statistically significant factors in the model.
The study was approved by the institutional review boards of Akron City Hospital and the Northeastern Ohio Universities College of Medicine. The approval was for these epidemiologic questions and prohibited revealing results to patients, families, or physicians.
RESULTS
Of 958 potentially eligible patients approached during the study period, only 95 (10%) refused the interview. Also excluded from the analyses were 158 patients (17%) whose physical condition prevented interviews, 59 patients (6%) with known dementia, and 99 patients (10%) for other reasons (sleeping, family present, inter- ruptions, repeat visits, incomplete forms). Five hundred forty-seven patients (57%) met the inclusion criteria and comprised the study group.
A description of the sample is shown in Table 1. Sixty- five percent of patients were women, and 92% of patients resided in the community. The mean age was 76.7 (+7.7 SD) years, and 34.6% of patients were more than 80 years old. The most common discharge diagnoses were diseases of the circulatory system (25%), followed by symptoms, signs, and ill-defined conditions (21%). Fifty-two percent of the interviewed patients were admitted to the hospital. Excluded patients differed (P < .05) from those who were included in that they were slightly older (mean age, 79.5 years; 46% older than 79 years), were more likely to reside in nursing homes (37.9%), and were less likely to live alone (10.3%).
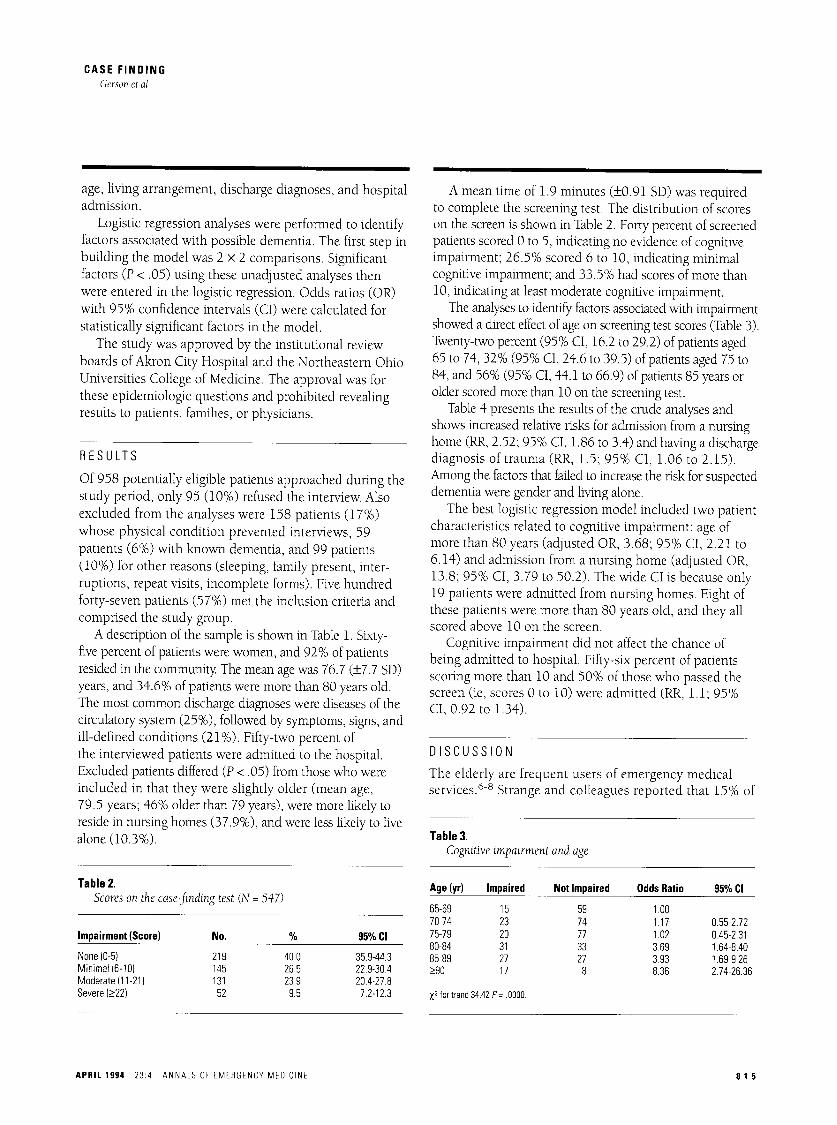
Table 2. Scores on the case-finding test (N = 547)
Impairment (Score) No. % 95% CI
None (0-5) 219 40.0 35.9-44.3 Minimal (6-10) 145 26.5 22.9-30.4 Moderate (11-21 ) 131 23.9 20.4-27.8 Severe (>22) 52 9.5 7.2-12.3
A mean time of 1.9 minutes (_+0.91 SD) was required to complete the screening test. The distribution of scores on the screen is shown in Table 2. Forty percent of screened patients scored 0 to 5, indicating no evidence of cognitive impairment; 26.5% scored 6 to 10, indicating minimal cognitive impairment; and 33.5% had scores of more than 10, indicating at least moderate cognitive impairment.
The analyses to identify factors associated with impairment showed a direct effect of age on screening test scores (Table 3). Twenty-two percent (95% CI, 16.2 to 29.2) of patients aged 65 to 74, 32% (95% CI, 24.6 to 39.5) of patients aged 75 to 84, and 56% (95% CI, 44.1 to 66.9) of patients 85 years or older scored more than 10 on the screening test.
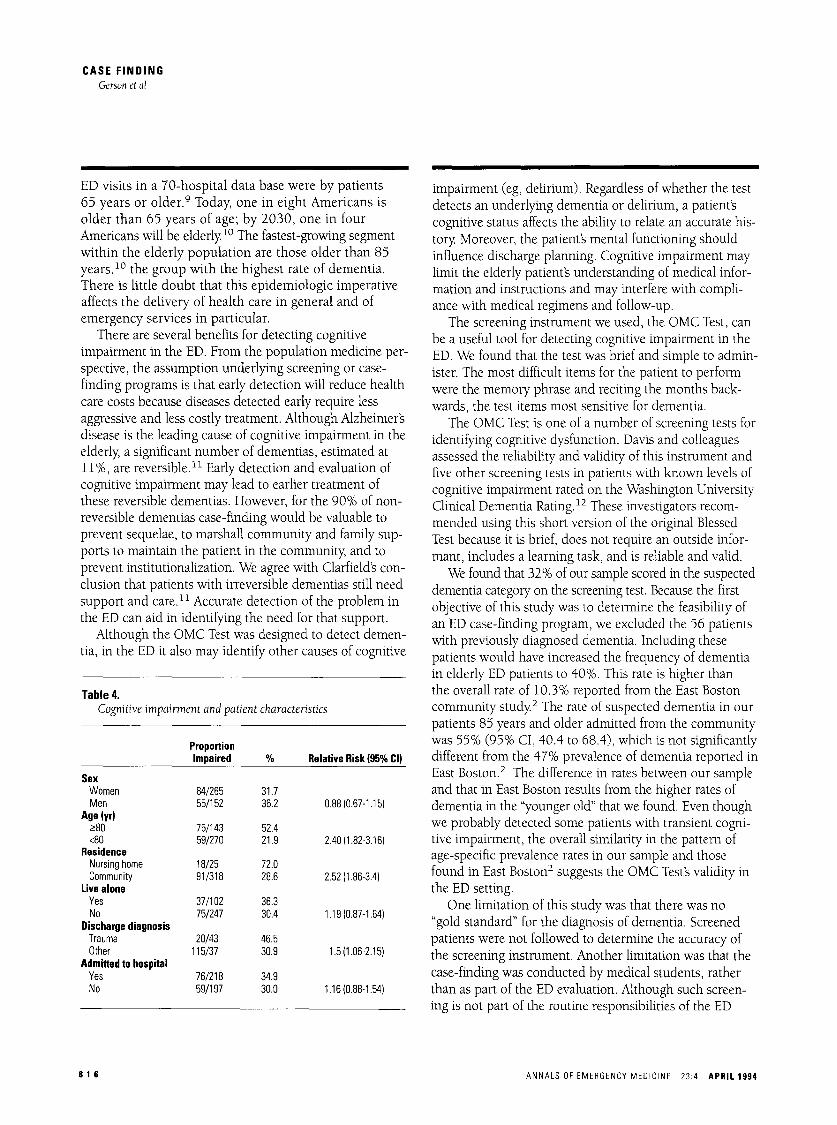
Table 4 presents the results of the crude analyses and shows increased relative risks for admission from a nursing home (RR, 2.52; 95% CI, 1.86 to 3.4) and having a discharge diagnosis of trauma (RR, 1.5; 95% CI, 1.06 to 2.15). Among the factors that failed to increase the risk for suspected dementia were gender and living alone.
The best logistic regression model included two patient characteristics related to cognitive impairment: age of more than 80 years (adjusted OR, 3.68; 95% CI, 2.21 to 6.14) and admission from a nursing home (adjusted OR, 13.8; 95% CI, 3.79 to 50.2). The wide CI is because only 19 patients were admitted from nursing homes. Eight of these patients were more than 80 years old, and they all scored above 10 on the screen.
Cognitive impairment did not affect the chance of being admitted to hospital. Fifty-six percent of patients scoring more than 10 and 50% of those who passed the screen (ie, scores 0 to 10) were admitted (RR, 1.1; 95% CI, 0.92 to 1.34).
DISCUSSION
The elderly are frequent users of emergency medical services. 6-8 Strange and colleagues reported that 15% of
Table 3. Cognitive impairment and age
Age (yr) Impaired Not Impaired Odds Ratio 95% CI
65-69 15 59 1.00 70-74 23 74 1.17 0.55-2.72 75-79 20 77 1.02 0.45-2.31 80-84 31 33 3.69 1.64-8.40 85-89 27 27 3.93 1.69-9.26 >90 17 8 8.36 2.74-26.36
Z 2 fortrend 34.42 P= .0000.
APRIL 1994 23:4 ANNALS OF EMERGENCY MEDICINE 81 5
CASE FINDINGGerson et al
age, living arrangement, discharge diagnoses, and hospitaladmission.
Logistic regression analyses were performed to identifyfactors associated with possible dementia. The first step inbuilding the model was 2 x 2 comparisons. Significantfactors (P < .05) using these unadjusted analyses thenwere entered in the logistic regression. Odds ratios (OR)with 95% confidence intervals (Cl) were calculated forstatistically significant factors in the model.
The study was approved by the institutional reviewboards of Akron City Hospital and the Northeastern OhioUniversities College of Medicine. The approval was forthese epidemiologic questions and prohibited revealingresults to patients, families, or physicians.
RESULTS
Of 958 potentially eligible patients approached during thestudy period, only 95 00%) refused the interview. Alsoexcluded from the analyses were 158 patients 07%)whose phYSical condition prevented interviews, 59patients (6%) with known dementia, and 99 patients00%) for other reasons (sleeping, family present, interruptions, repeat visits, incomplete forms). Five hundredforty-seven patients (57%) met the inclusion criteria andcomprised the study group.
A description of the sample is shown in Table 1. Sixtyfive percent of patients were women, and 92% of patientsresided in the community. The mean age was 76.7 (t7.7 SD)years, and 34.6% of patients were more than 80 years old.The most common discharge diagnoses were diseases of thecirculatory system (25%), followed by symptoms, signs, andill-defined conditions (21 %). Fifty-two percent ofthe interviewed patients were admitted to the hospital.Excluded patients differed (P < .05) from those who wereincluded in that they were slightly older (mean age,79.5 years; 46% older than 79 years), were more likely toreside in nursing homes (37.9%), and were less likely to livealone 00.3%).
A mean time of 1.9 minutes (to.91 SD) was reqUiredto complete the screening test. The distribution of scoreson the screen is shown in Table 2. Forty percent of screenedpatients scored 0 to 5, indicating no evidence of cognitiveimpairment; 26.5% scored 6 to 10, indicating minimalcognitive impairment; and 33.5% had scores of more than10, indicating at least moderate cognitive impairment.
The analyses to identify factors associated with impairmentshowed a direct effect of age on screening test scores (Table 3).Twenty-two percent (95% cr, 16.2 to 29.2) of patients aged65 to 74, 32% (95% CI, 24.6 to 39.5) of patients aged 75 to84, and 56% (95% cr, 44.1 to 66.9) of patients 85 years orolder scored more than 10 on the screening test.
Table 4 presents the results of the crude analyses andshows increased relative risks for admission from a nursinghome (RR, 2.52; 95% cr, 1.86 to 3.4) and having a dischargediagnosis of trauma (RR, 1. 5; 95% CI, 1.06 to 2.15).Among the factors that failed to increase the risk for suspecteddementia were gender and living alone.
The best logistic regression model included two patientcharacteristics related to cognitive impairment: age ofmore than 80 years (adjusted OR, 3.68; 95% CI, 2.21 to6.14) and admission from a nursing home (adjusted OR,13.8; 95% CI, 3.79 to 50.2). The wide cr is because only19 patients were admitted from nursing homes. Eight ofthese patients were more than 80 years old, and they allscored above 10 on the screen.
Cognitive impairment did not affect the chance ofbeing admitted to hospital. Fifty-six percent of patientsscoring more than 10 and 50% of those who passed thescreen (ie, scores 0 to 10) were admitted (RR, 1.1; 95%CI, 0.92 to 1.34).
DISCUSSION
The elderly are frequent users of emergency medicalservices 6 -8 Strange and colleagues reported that 15% of
Table 3.Cognitive impairment and age
x' for trend 34,42 p= .0000.
Table 2.Scores on the case-finding test (N = 547)
Impairment (Score) No. % 95%CI
None (0-5) 219 40.0 35.9-44.3Minimal (6-10) 145 26.5 22.9-304Moderate (11-21) 131 23.9 20.4-27.8Severe (~22) 52 9.5 7.2-12.3
APRIL 1994 234 ANNALS OF EMERGENCY MEDICINE
Age (yr)
65-6970-7475-7980-8485-89~90
Impaired
152320312717
Not Impaired
59747733278
Odds Ratio
1001.171023.693.938.36
95% CI
055-272045-2.311.64-8401.69-9.26274-26.36
81 5
CASE F I N D I N G Gerson et al
ED visits in a 70-hospital data base were by patients 65 years or older. 9 Today, one in eight Americans is older than 65 years of age; by 2030, one in four Americans will be elderly lo The fastest-growing segment within the elderly population are those older than 85 years, 1° the group with the highest rate of dementia. There is little doubt that this epidemiologic imperative affects the delivery of health care in general and of emergency services in particular.
There are several benefits for detecting cognitive impairment in the ED. From the population medicine per- spective, the assumption underlying screening or case- finding programs is that early detection will reduce health care costs because diseases detected early require less aggressive and less costly treatment. Although Alzheimer's disease is the leading cause of cognitive impairment in the elderly, a significant number of dementias, estimated at 11%, are reversible. 11 Early detection and evaluation of cognitive impairment may lead to earlier treatment of these reversible dementias. However, for the 90% of non- reversible dementias case-finding would be valuable to prevent sequelae, to marshall community and family sup- ports to maintain the patient in the community, and to prevent institutionalization. We agree with Clarfield's con- clusion that patients with irreversible dementias still need support and care. t t Accurate detection of the problem in the ED can aid in identifying the need for that support.
Although the OMC Test was designed to detect demen- tia, in the ED it also may identify other causes of cognitive
Table 4. Cognitive impairment and patient characteristics
Proportion Impaired % Relative Risk {95% CI)
Sex Women 84/265 31.7 Men 55/152 36.2 0.88 (0.67-1.15)
Age (yr) >80 75/143 52.4 <88 59/270 21.9 2.40 (1.82-3.18)
Residence Nursing home 18/25 72.0 Community 91/318 28.6 2.52 (1.86-3.4)
Live alone Yes 37/102 36.3 No 75/247 30.4 1.19 (0.87-1.64)
Discharge diagnosis Trauma 20/43 46.5 Other 115/37 30.9 1.5 (1.06-2.15)
Admitted to hospital Yes 76/218 34.9 No 59/197 30.0 1.16 (0.88-1.54)
impairment (eg, delirium). Regardless of whether the test detects an underlying dementia or delirium, a patient's cognitive status affects the ability to relate an accurate his- tory. Moreover, the patient's mental functioning should influence discharge planning. Cognitive impairment may limit the elderly patient's understanding of medical infor- mation and instructions and may interfere with compli- ance with medical regimens and follow-up.
The screening instrument we used, the OMC Test, can be a useful tool for detecting cognitive impairment in the ED. We found that the test was brief and simple to admin- ister. The most difficult items for the patient to perform were the memory phrase and reciting the months back- wards, the test items most sensitive for dementia.
The OMC Test is one of a number of screening tests for identifying cognitive dysfunction. Davis and colleagues assessed the reliability and validity of this instrument and five other screening tests in patients with known levels of cognitive impairment rated on the Washington University Clinical Dementia Rating. 12 These investigators recom- mended using this short version of the original Blessed Test because it is brief, does not require an outside infor- mant, includes a learning task, and is reliable and valid.
We found that 32% of our sample scored in the suspected dementia category on the screening test. Because the first objective of this study was to determine the feasibility of an ED case-finding program, we excluded the 56 patients with previously diagnosed dementia. Including these patients would have increased the frequency of dementia in elderly ED patients to 40%. This rate is higher than the overall rate of 10.3% reported from the East Boston c o m m u n i t y study. 2 The rate of suspected dementia in our patients 85 years and older admitted from the community was 55% (95% CI, 40.4 to 68.4), which is not significantly different from the 47% prevalence of dementia reported in East Boston. 2 The difference in rates between our sample and that in East Boston results from the higher rates of dementia in the "younger old" that we found. Even though we probably detected some patients with transient cogni- tive impairment, the overall similarity in the pattern of age-specific prevalence rates in our sample and those found in East Boston 2 suggests the OMC Test's validity in the ED setting.
One limitation of this study was that there was no "gold standard" for the diagnosis of dementia. Screened patients were not followed to determine the accuracy of the screening instrument. Another limitation was that the case-finding was conducted by medical students, rather than as part of the ED evaluation. Although such screen- ing is not part of the routine responsibilities of the ED
81 6 ANNALS OF EMERGENCY MEDICINE 23:4 APRIL 1994
CASE FINDINGGerson et al
ED visits in a 70-hospital data base were by patients65 years or older.9 Today, one in eight Americans isolder than 65 years of age; by 2030, one in fourAmericans will be elderly. 10 The fastest-growing segmentwithin the elderly population are those older than 85years,10 the group with the highest rate of dementia.There is little doubt that this epidemiologic imperativeaffects the delivery of health care in general and ofemergency services in particular.
There are several benefits for detecting cognitiveimpairment in the ED. From the population medicine perspective, the assumption underlying screening or casefinding programs is that early detection will reduce healthcare costs because diseases detected early require lessaggressive and less costly treatment. Although Alzheimer'sdisease is the leading cause of cognitive impairment in theelderly, a significant number of dementias, estimated at11 %, are reversible. 11 Early detection and evaluation ofcognitive impairment may lead to earlier treatment ofthese reversible dementias. However, for the 90% of nonreversible dementias case-finding would be valuable toprevent sequelae, to marshall community and family supports to maintain the patient in the community, and toprevent institutionalization. We agree with Clarfield's conclusion that patients with irreversible dementias still needsupport and care. 11 Accurate detection of the problem inthe ED can aid in identifying the need for that support.
Although the OMC Test was designed to detect dementia, in the ED it also may identify other causes of cognitive
Table 4.Cognitive impairment and patient characteristics
ProportionRelative Risk (95% CIIImpaired %
SexWomen 84/265 31.7Men 55/152 36.2 0.88 (0.67-1.151
Age (yr)~80 75/143 52A<80 59/270 21.9 2AO (1.82-3.161
ResidenceNursing home 18/25 noCommunity 91/318 28.6 2.52 (1.86-3A)
Live aloneYes 37/102 36.3No 75/247 30A 1.19 (0.87-1.64)
Discharge diagnosisTrauma 20/43 46.5Other 115/37 30.9 1.5 (1.06-2.15)
Admitted to hospitalYes 76/218 34.9No 59/197 30.0 1.16 (0.88-1.54)
816
impairment (eg, delirium). Regardless of whether the testdetects an underlying dementia or delirium, a patient'scognitive status affects the ability to relate an accurate history. Moreover, the patient's mental functioning shouldinfluence discharge planning. Cognitive impairment maylimit the elderly patient's understanding of medical information and instructions and may interfere with compliance with medical regimens and follow-up.
The screening instrument we used, the OMC Test, canbe a useful tool for detecting cognitive impairment in theED. We found that the test was brief and simple to administer. The most difficult items for the patient to performwere the memory phrase and reciting the months backwards, the test items most sensitive for dementia.
The OMC Test is one of a number of screening tests foridentifying cognitive dysfunction. Davis and colleaguesassessed the reliability and validity of this instrument andfive other screening tests in patients with known levels ofcognitive impairment rated on the Washington UniversityClinical Dementia Rating. 12 These investigators recommended using this short version of the original BlessedTest because it is brief, does not require an outside informant, includes a learning task, and is reliable and valid.
We found that 32% of our sample scored in the suspecteddementia category on the screening test. Because the firstobjective of this study was to determine the feaSibility ofan ED case-finding program, we excluded the 56 patientswith previously diagnosed dementia. Including thesepatients would have increased the frequency of dementiain elderly ED patients to 40%. This rate is higher thanthe overall rate of 10.3% reported from the East Bostoncommunity study 2 The rate of suspected dementia in ourpatients 85 years and older admitted from the communitywas 55% (95% CI, 40.4 to 68.4), which is not significantlydifferent from the 47% prevalence of dementia reported inEast Boston.2 The difference in rates between our sampleand that in East Boston results from the higher rates ofdementia in the "younger old" that we found. Even thoughwe probably detected some patients with transient cognitive impairment, the overall similarity in the pattern ofage-specific prevalence rates in our sample and thosefound in East Boston2 suggests the OMC Test's validity inthe ED setting.
One limitation of this study was that there was no"gold standard" for the diagnosis of dementia. Screenedpatients were not followed to determine the accuracy ofthe screening instrument. Another limitation was that thecase-finding was conducted by medical students, ratherthan as part of the ED evaluation. Although such screening is not part of the routine responsibilities of the ED
ANNALS OF EMERGENCY MEDICINE 23:4 APRIL 1994

CASE F I N D I N G Ccrson et al
social worker, she volunteered to participate in this study and interviewed patients evaluated in the ED during day shifts. Nevertheless, given the simplicity and limited time requirements (less than two minutes) to perform the OMC Test, we suggest that this screen could be adminis- tered easily and quickly by physicians or nurses as part of the standard ED evaluation of older patients.
CONCLUSION
Screening for cognitive impairment in elderly ED patients using the OMC Test is feasible based on its brevity, ease of administration, and patient acceptability. There is a high prevalence of cognitive impairment in elderly ED patients, and the prevalence increases with advancing age. Identification of cognitive impairment is an impor- tant element in the assessment of elderly ED patients as impairment may affect clinical evaluation, patients' under- standing of medical information, and compliance with discharge instructions.
Reprint no. 47/1/53847
Address for reprints:
Lowell W Gerson, PhD
Northeastern Ohio Universities College of Medicine
PO Box 95
Rootstown, Ohio 44272-0095
216-325-2511
Fax 216-325-7943
REFERENCES 1. Larson EB, Kukall WA, Katzman RL: Cognitive impairment: Dementia and Alzheimer's disease. Ann Rev Pub Health 1992;13:431-439.
2. Evans BA, Funkenstein NH, Albert MS, et al: Prevalence of Alzheimer's disease in a community population of older persons: Higher than previously reported. JAMA 1989;226:2551-2556.
3. Sanders AB: Care of the elderly in emergency departments: Conclusions and recommendations. Ann Emerg Med 1992;21:830-834.
4. Katzman R, Brown T, Fuld P, et al: Validation of a short orientation-memory-concentration test of cognitive impairment. Am J Psychiatry 1983;140:734-739.
5. Blessed G, Tomlinson BE, Roth M: The association between quantitative measures of dementia and of senile changes in the cerebral grey matter of elderly subjects. BrJ Psychiatry 1968;114:797-811.
6. Baum SD, Rubenstein LZ: Old people in the emergency room: Age related differences in emergency department use and care. JAm GeriatrSoc 1987;35:398-407.
7. Gerson LW, Skvarch L: Emergency medical services utilization by the elderly. Ann Emerg Med 1982;1:610-612.
8. Ettinger WH, Casani JA, Coon P J, et al: Patterns of use of the emergency department by elderly patients. J Gerontol 1987;12:638-642.
9. Strange GR, Chen EH, Sanders AB: Use of emergency departments by elderly patients: Projections from a multicenter data base. Ann Emerg Med 1992;21:819-824.
10. US Senate Special Committee on Aging: Aging America: Trends and Projections. Washington, DC, US Department of Health and Human Services, 1988.
11. Clarfield AM: The reversible dementias: Do they reverse? Ann Intern Med 1988;109:476-486.
12. Davis PB, Morris JC, Grant E: Brief screening tests versus clinical staging in senile dementia of the Alzheimer type. JAm Geriatr Soc 1990;38:129-135,
APRIL 1994 23:4 ANNALS OF EMERGENCY MEDICINE 81 7
CASE FINDINGGerson et al
social worker, she volunteered to participate in this studyand interviewed patients evaluated in the ED during dayshifts. Nevertheless, given the SimpliCity and limited timerequirements (less than two minutes) to perform theOMC Test, we suggest that this screen could be administered easily and quickly by physicians or nurses as part ofthe standard ED evaluation of older patients.
CONCLUSION
Screening for cognitive impairment in elderly ED patientsusing the OMC Test is feasible based on its brevity, ease ofadministration, and patient acceptability. There is a highprevalence of cognitive impairment in elderly EDpatients, and the prevalence increases with advancingage. Identification of cognitive impairment is an important element in the assessment of elderly ED patients asimpairment may affect clinical evaluation, patients' understanding of medical information, and compliance withdischarge instructions,
REFERENCES1. Larson EB, Kukall WA, Katzman RL: Cognitive impairment: Dementia and Alzheimer's disease.Ann Rev Pub Health 1992;13:431-439
2. Evans DA. Funkenstein HH. Albert MS. et al: Prevalence of Alzheimer's disease in a communitypopulation of older persons: Higher than previously reported. JAMA 1989;226:2551-2556.
3. Sanders AB Care of the elderly in emergency departments: Conclusions andrecommendations. Ann Emerg Med 1992;21 :830-834.
4. Katzman R. Brown T, Fuld P. et al: Validation of a short orientation-memory-concentration testof cognitive impairment: Am J Psychiatry 1983;140:734-739
5. Blessed G. Tomlinson BE. Roth M: The association between quantitative measures ofdementia and of senile changes in the cerebral grey matter of elderly subjects. Sr J Psychiatry1968;114:797-811.
6 Baum SD. Rubenstein LZ: Old people in the emergency room Age related differences inemergency department use and care. JAm Geriatr Soc 1987;35:398-407.
7. Gerson LW. Skvarch L: Emergency medical services utilization by the elderly. Ann Emerg Med1982;1:610-612.
8 Ettinger WHo Casani JA. Coon PJ. et al: Patterns of use of the emergency department byelderly patients. J GeranIOl 1987;12:638-642.
9 Strange GR, Chen EH. Sanders AB: Use of emergency departments by elderly patients:Projections from amulticenter data base. Ann Emerg Med 1992;21 :81 9-824.
10. US Senate Special Committee on Aging: Aging America: Trends and Projections. Washington.DC. US Department of Health and Human Services, 1988.
11. Clarfield AM: The reversible dementias: Do they reverse? Ann Intern Med 1988;1 09:476-486.
12. Davis PB. Morris JC. Grant E: Brief screening tests versus clinical staging in senile dementiaof the Alzheimer type. JAm Geriatr Soc 1990;38:129-135.
APRIL 1994 23:4 ANNALS OF EMERGENCY MEDICINE
Reprint no. 47/1/53847
Address for reprints:
Lowell WGerson, PhD
Northeastern Ohio Universities College of Medicine
PO Box 95
Rootstown, Ohio 44272-0095
216-325-2511
Fax 216-325-7943
81 7





























