Embed Size (px)
Citation preview

Case Management Case Management and Diabetes Mellitusand Diabetes Mellitus
Charlton Wilson, Jeff Curtis, Charlton Wilson, Jeff Curtis, Suzanne Lipke, Robin Thompson, Suzanne Lipke, Robin Thompson,
Susan Dethman Susan Dethman

Outline: Case Outline: Case ManagementManagement
Role Role ProcessProcess ExperiencesExperiences

To improve diabetes care, To improve diabetes care, Task Force on Community Preventive Task Force on Community Preventive
ServicesServicessupports the following interventions:supports the following interventions:
Self management Self management Self Management EducationSelf Management Education
Health-care system level Health-care system level interventions interventions Disease ManagementDisease Management Case ManagementCase Management
TThe Task Force on Community Preventive Services he Task Force on Community Preventive Services is a 15-member non-Federal Task force is a 15-member non-Federal Task force supported by the Centers for Disease Control and Prevention (CDC).supported by the Centers for Disease Control and Prevention (CDC).

Diabetes Self-Diabetes Self-Management EducationManagement Education
Structured education programs Structured education programs self-monitoring of blood glucoseself-monitoring of blood glucose education about diet and exerciseeducation about diet and exercise treatment planstreatment plans motivation for patients to use the motivation for patients to use the
skills for self-management of diabetes.skills for self-management of diabetes.

Disease ManagementDisease Management
Organized, proactive, multi-component Organized, proactive, multi-component approach for all members of a approach for all members of a population with a specific diseasepopulation with a specific disease identify the target population in the identify the target population in the
community or organization community or organization implement care plans proven to be effective implement care plans proven to be effective track, measure, and manage health track, measure, and manage health
outcomes outcomes

Case ManagementCase Management
Assignment of a case manager toAssignment of a case manager to PlanPlan CoordinateCoordinate Integrate care for people with a disease Integrate care for people with a disease
or conditionor condition Case Management, Care Case Management, Care
Management, Care CoordinationManagement, Care Coordination

ModelsModels

ModelsModels

Steps For Diabetes Case Steps For Diabetes Case ManagementManagement
AssessmentAssessment Analysis of assessment findingsAnalysis of assessment findings Outcome identificationOutcome identification PlanningPlanning Diabetes Self Management EducationDiabetes Self Management Education EvaluationEvaluation Follow upFollow up Program effectivenessProgram effectiveness

AssessmentAssessment
Determine the priority of Determine the priority of information obtained by the client’s information obtained by the client’s immediate condition or needimmediate condition or need
Include the client’s familyInclude the client’s family Collect the information in a Collect the information in a
systematic mannersystematic manner Document findings in a retrievable Document findings in a retrievable
formatformat

AssessmentAssessment
Integrate the assessment process Integrate the assessment process with data from other members of the with data from other members of the health care team to ensure health care team to ensure continuity and collaborationcontinuity and collaboration
Include information related to Include information related to client’s knowledge of diabetes and client’s knowledge of diabetes and current diabetes self-management current diabetes self-management behaviors.behaviors.

Analysis of AssessmentAnalysis of Assessment Identify actual or potential problems Identify actual or potential problems
and/or challenges and barriersand/or challenges and barriers Identify interpersonal, cultural , Identify interpersonal, cultural ,
psychosocial and environmental psychosocial and environmental conditions that affect the clientconditions that affect the client
Validate findings with the client, family Validate findings with the client, family and health care teamand health care team
Document findings in a manner that Document findings in a manner that identifies outcomes identifies outcomes
Incorporate findings into an Incorporate findings into an individualized care planindividualized care plan

Outcome IdentificationOutcome Identification
Formulate outcomes from Formulate outcomes from assessment findingsassessment findings
Determine that outcomes are Determine that outcomes are realistic, attainable and measurablerealistic, attainable and measurable
Ensure that outcomes reflect Ensure that outcomes reflect scientific knowledge of diabetes carescientific knowledge of diabetes care
Use outcomes to evaluate goal Use outcomes to evaluate goal attainmentattainment

PlanningPlanning
Assist client with developing goals Assist client with developing goals Patient selected plan - Individualize Patient selected plan - Individualize
the plan to meet the client’s needs the plan to meet the client’s needs Identify priorities in relation to Identify priorities in relation to
expected outcomes expected outcomes Document the planDocument the plan Collaborate with other team Collaborate with other team
members about the planmembers about the plan

Diabetes Self-Management Diabetes Self-Management TrainingTraining
Provide diabetes education that is Provide diabetes education that is pertinent to the client’s assessed pertinent to the client’s assessed needs and health valuesneeds and health values
Use appropriate teaching methodsUse appropriate teaching methods Allow opportunities for the client to Allow opportunities for the client to
demonstrate skillsdemonstrate skills Incorporate empowerment strategies Incorporate empowerment strategies Document understanding of educationDocument understanding of education

EvaluationEvaluation
Evaluate outcomes on a systematic Evaluate outcomes on a systematic and on-going basisand on-going basis
Document client’s response to Document client’s response to implementing the care plan implementing the care plan
Evaluate the effectiveness of Evaluate the effectiveness of interventions in relation to outcomesinterventions in relation to outcomes
Revises plan as neededRevises plan as needed Documents revisionsDocuments revisions Collaborates with team on evaluationCollaborates with team on evaluation

Follow - UpFollow - Up
Determine frequency of follow-upDetermine frequency of follow-up Use a systematic approach for each Use a systematic approach for each
follow up visitfollow up visit Provide client with feed backProvide client with feed back Incorporate a tracking system to Incorporate a tracking system to
avoid “lost to follow-up” statusavoid “lost to follow-up” status

Case Management Case Management InterventionsInterventions
Treatment StrategiesTreatment Strategies Medical Nutrition TherapyMedical Nutrition Therapy Exercise prescriptionsExercise prescriptions Coping BehaviorsCoping Behaviors Medication adjustmentMedication adjustment
Diabetes Self Management TrainingDiabetes Self Management Training 10 core content areas10 core content areas ADA National Standards for Diabetes ADA National Standards for Diabetes
Self-Management EducationSelf-Management Education

Case Management Case Management InterventionsInterventions
Supportive CounselingSupportive Counseling Readiness for ChangeReadiness for Change Motivational InterviewingMotivational Interviewing
Problem SolvingProblem Solving Skills buildingSkills building
MonitoringMonitoring Individualized Care PlansIndividualized Care Plans Coordination of ResourcesCoordination of Resources

Things to ConsiderThings to Consider
Age-appropriate, culturally, ethically and Age-appropriate, culturally, ethically and spiritually sensitive care and supportspiritually sensitive care and support
Educate patients, families and support Educate patients, families and support systemssystems
Continuity of careContinuity of care Coordination of care for various settings Coordination of care for various settings Managing informationManaging information Effective communication with diabetes teamEffective communication with diabetes team Non-judgmental approachNon-judgmental approach

ReimbursementReimbursement
Case management at this point in Case management at this point in time is not a reimbursable item, time is not a reimbursable item, however, the professional expertise however, the professional expertise of the individual can be billed for of the individual can be billed for third party. third party.
Case management is generally used Case management is generally used as a patient management tool and a as a patient management tool and a current and future cost containment current and future cost containment utilization.utilization.

SchedulingScheduling
Time slots typically provided to the Time slots typically provided to the case manager normally are 2 to 4 case manager normally are 2 to 4 times greater than time allocation times greater than time allocation for the Primary Care Provider. This for the Primary Care Provider. This allows for a more in-depth interview allows for a more in-depth interview and analysis of the patient and their and analysis of the patient and their understanding of the current care understanding of the current care plan and disease process.plan and disease process.

SchedulingScheduling
Scheduling will also reflect case Scheduling will also reflect case load.load.
A benchmark has not been A benchmark has not been established as to the number of established as to the number of patients a diabetes case manager patients a diabetes case manager can effectively be responsible for. can effectively be responsible for.

Case LoadCase Load
At the Wewoka Service Unit, 75 At the Wewoka Service Unit, 75 patients to be effectively managed by patients to be effectively managed by the case manager utilizing a 32 hour the case manager utilizing a 32 hour work week was initially suggested.work week was initially suggested.
Each individual organization will Each individual organization will have to determine case load for their have to determine case load for their case managers. This will vary with case managers. This will vary with severity of patient and their disease severity of patient and their disease process, including learning barriers.process, including learning barriers.

IssuesIssues
Roles and ResponsibilitiesRoles and Responsibilities Professional relationshipsProfessional relationships AccountabilityAccountability
Space, toolsSpace, tools LocationLocation Registry AccessRegistry Access
Case Load ManagementCase Load Management Continuous healing relationships vs Continuous healing relationships vs
dynamic patient populationsdynamic patient populations Those issues unique to your communityThose issues unique to your community

Case Case Management in Management in Indian Health Indian Health
SettingsSettingsA poll of participants in the A poll of participants in the Diabetes Summer InstitutesDiabetes Summer Institutes
Portland SessionPortland Session

A poll of case management A poll of case management services in Indian Health services in Indian Health
settingssettings Voluntary, self reported poll (written Voluntary, self reported poll (written
survey) of participants in the case survey) of participants in the case management class management class
Returned N= 22 (out of 27)Returned N= 22 (out of 27) Completed on day 1of the instituteCompleted on day 1of the institute

Type of OrganizationType of Organization
0
10
20
30
40
50
60
70
80
%
IHS Tribal Urban
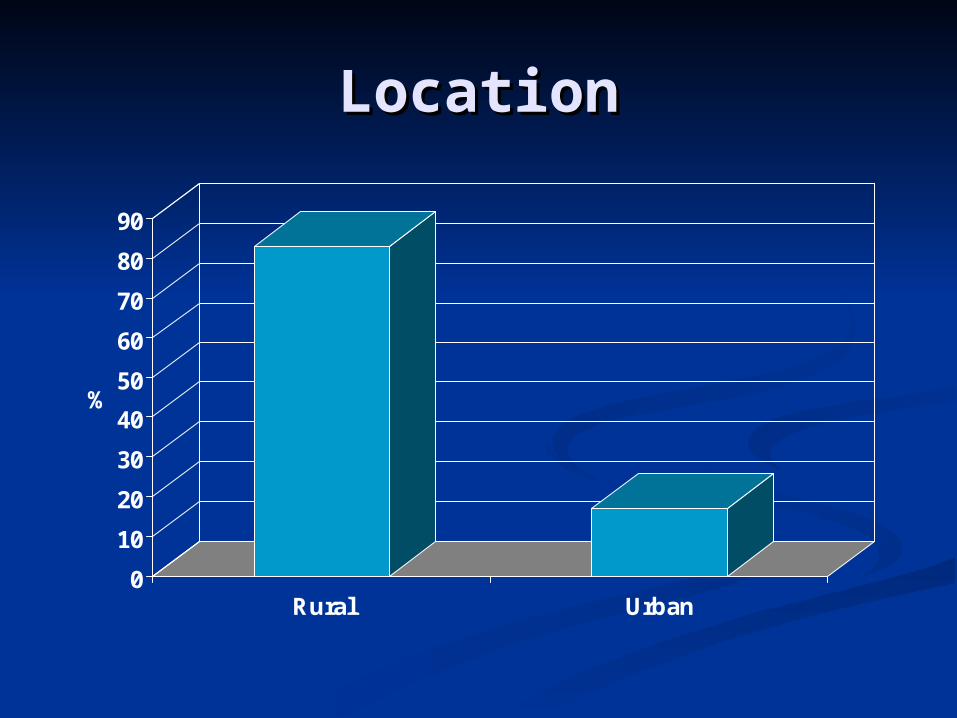
LocationLocation
0
10
20
30
40
50
60
70
80
90
%
Rural Urban

Patient Education Patient Education ProgramProgram
0
20
40
60
80
100
Yes No
Do you have a formal program?
0
10
20
30
40
50
60
70
80
Yes No/Unknown
Is the program recognized
Of those who had a program

Do you currently have a Do you currently have a case management program?case management program?
0
10
20
30
40
50
60
%
Yes No

How many case managers How many case managers in your program?in your program?
0
5
10
15
20
25
30
35
40
45
50
%
1 2 3 4
Of those who had a case management program
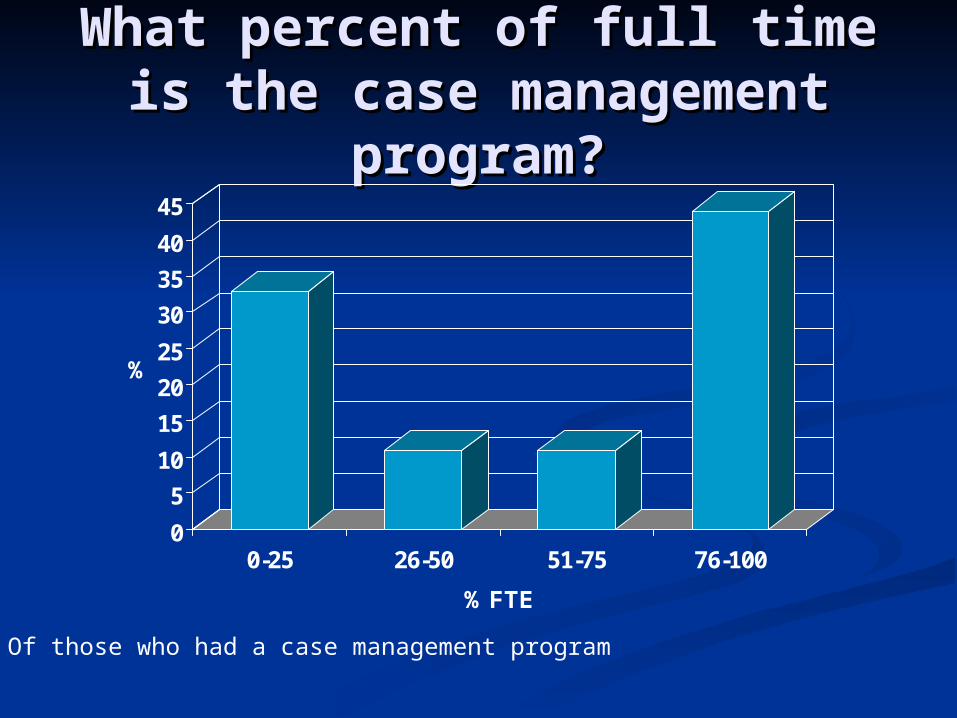
What percent of full time is What percent of full time is the case management the case management
program?program?
0
5
10
15
20
25
30
35
40
45
%
0-25 26-50 51-75 76-100
% FTE
Of those who had a case management program

What additional duties does What additional duties does the case manager have? the case manager have?
0
10
20
30
40
50
60
%
Clinic work Prog Management Nutrition services
Of those who had a case management program

Professions of the case Professions of the case managermanager
0
5
10
15
20
25
30
35
40
45
50
% o
f p
rog
ram
s
RN RD APN LPN/LVN CHR
Of those who had a case management program
How many patients/case How many patients/case manager?manager?
95-10095-100 176176 300300 348348
50% - Unknown50% - Unknown
Of those who had a case management program

Case Manager SupportCase Manager Support
0
20
40
60
80
100
Yes No
Do you have access to a clinical provider?
0
20
40
60
80
100
Yes No
Is the clinic provider specified?
Of those who had a case management program

Pilot Evaluation # 1: Pilot Evaluation # 1: AimAim
To evaluate the effectiveness of a To evaluate the effectiveness of a Nurse Care Coordinator who Nurse Care Coordinator who provided active outreach, education, provided active outreach, education, and care coordination to American and care coordination to American Indian and Alaskan Native people Indian and Alaskan Native people with diabetes in an IHS primary care with diabetes in an IHS primary care system system

Pilot ProjectPilot Project LocationLocation
Phoenix Indian Medical Center Phoenix Indian Medical Center Nurse Care Coordinator (NCC)Nurse Care Coordinator (NCC)
RN, CDERN, CDE 295 people selected by “lottery” from the registry295 people selected by “lottery” from the registry
Outreach Outreach letters, phone calls, opportunistic notification letters, phone calls, opportunistic notification
EducationEducation Individual consultationIndividual consultation
CoordinationCoordination Scheduling, follow up, reinforcementScheduling, follow up, reinforcement

Evaluation MeasuresEvaluation Measures Outreach effectivenessOutreach effectiveness
Quarterly accounting of face-to-face consultationQuarterly accounting of face-to-face consultation VisitsVisits
Education and coordination effectivenessEducation and coordination effectiveness Adherence with IHS standards of careAdherence with IHS standards of care IHS diabetes care and outcomes audit performed IHS diabetes care and outcomes audit performed
at baseline, 4 , 8 and 12 month intervals at baseline, 4 , 8 and 12 month intervals Comparison populationComparison population
290 people from the active diabetes registry who 290 people from the active diabetes registry who did not have a nurse care coordinatordid not have a nurse care coordinator

Outreach EffectivenessOutreach Effectiveness
0
20
40
60
80
100
4 month 8 Month 12 month
Time interval from project start
% o
f p
atie
nts
in
th
e ca
se
load
No response tooutreach/refused
Receiving careelsewhere
Addressunknown
Face-to-face visit
Chi2 for trend 9.6, p = 0.002

Baseline Characteristics
With NCC n=295
Without NCC n=290
Age (years) * 4813 4514
Duration of Diabetes (years)
4.3 4.1
HbA1c (%) 8.82.4 8.62.3
Eye exam done (%)
50 50
DM education (%)
24 23
Self monitoring blood glucose
(%)
47 44
* p< 0.05 by Chi2

4 month follow up
-10
0
10
20
30
40
50
60D
iab
ete
Ed
uca
tion
Die
tin
stru
ctio
n
SM
BG
Fo
ot e
xam
Eye
Exa
m
De
nta
l exa
m
Lip
id te
stin
gchan
ge
fro
m b
asel
ine
aud
it
With NCC Without NCC
**
*
* Difference between groups p < 0.05 by Chi2

8 month follow up
-10
0
10
20
30
40
50
60D
iab
ete
Ed
uca
tion
Die
tin
stru
ctio
n
SM
BG
Fo
ot E
xam
Eye
exa
m
De
nta
l exa
m
Ch
ole
ste
rol
Te
stin
g
chan
ge
fro
m b
asel
ine
aud
it
With NCC Without NCC
*
**
*
* Difference between groups p < 0.05 by Chi2
* **

12 month follow up
-10
0
10
20
30
40
50
60D
iab
ete
Ed
uca
tion
Die
tin
stru
ctio
n
SM
BG
Fo
ot E
xam
Eye
exa
m
De
nta
l exa
m
Ch
ole
ste
rol
Te
stin
g
chan
ge
fro
m b
asel
ine
aud
it
With NCC Without NCC
*
**
*
* Difference between groups p < 0.05 by Chi2
* **

Evaluation # 1: Evaluation # 1: ConclusionsConclusions
For American Indian and Alaskan For American Indian and Alaskan Native people with diabetes the Native people with diabetes the addition of a Nurse Care addition of a Nurse Care Coordinator to the primary care Coordinator to the primary care health system results in:health system results in: Effective outreachEffective outreach An increased adherence with the An increased adherence with the
IHS Diabetes Standards of CareIHS Diabetes Standards of Care

Pilot Evaluation # 2: AimPilot Evaluation # 2: Aim
To evaluate the ability of a nurse To evaluate the ability of a nurse care coordinator to affect utilization care coordinator to affect utilization of ambulatory health care services of ambulatory health care services by American Indian and Alaskan by American Indian and Alaskan Native people with diabetes in an Native people with diabetes in an IHS primary care system IHS primary care system

Pilot ProjectPilot Project LocationLocation
Phoenix Indian Medical CenterPhoenix Indian Medical Center Nurse Care Coordinator (NCC)Nurse Care Coordinator (NCC)
RN, CDERN, CDE 295 people selected by “lottery” from the registry295 people selected by “lottery” from the registry
Outreach Outreach letters, phone calls, opportunistic notification letters, phone calls, opportunistic notification
EducationEducation Individual consultationIndividual consultation
CoordinationCoordination Scheduling, follow up, reinforcementScheduling, follow up, reinforcement

Evaluation MeasuresEvaluation Measures 295 people with a nurse care coordinator 295 people with a nurse care coordinator
(NCC) were compared to 290 people without (NCC) were compared to 290 people without a nurse care coordinatora nurse care coordinator
Visits were classified into 4 categories:Visits were classified into 4 categories: Combined ambulatory health care encountersCombined ambulatory health care encounters Emergency department encounters Emergency department encounters Primary health care encountersPrimary health care encounters Pharmacy encountersPharmacy encounters

Evaluation MeasuresEvaluation Measures• The number of visits during the project year were The number of visits during the project year were
divided by the number of visits during the divided by the number of visits during the preceding year so that each group served as its preceding year so that each group served as its own controlown control
• The attributable difference was calculated as the The attributable difference was calculated as the difference of the % change between the cohort with difference of the % change between the cohort with and the cohort without a nurse care coordinatorand the cohort without a nurse care coordinator
Attributable difference = Attributable difference = %% NCC group - % NCC group - % without NCC group without NCC group
100100

Selected Ambulatory Selected Ambulatory Utilization DataUtilization Data
LocatioLocationn
Visits by people Visits by people with NCC (N)with NCC (N)
Visits by people Visits by people without NCC without NCC
(N)(N)Year priorYear prior Year Year
duringduringYear priorYear prior Year Year
duringduring
Combined Combined visitsvisits
23642364 25052505 25322532 26022602
Primary Primary carecare
11331133 12801280 10351035 10941094
PharmacyPharmacy 476476 549549 525525 591591EmergencEmergenc
y y departmedepartme
ntnt
685685 610610 869869 851851

Ambulatory Health Care Ambulatory Health Care Utilization Differences Utilization Differences
Attributable to Nurse Care Attributable to Nurse Care Coordination for People With Coordination for People With
DiabetesDiabetes
-10-8-6-4-202468
10
Combined Primarycare
Pharmacy Emergencydepartment
Location of ambulatory encounters
%ch
an
ge N
CC
co
ho
rt -
%
ch
an
ge w
ith
ou
t N
CC
co
ho
rt

Evaluation # 2: Evaluation # 2: ConclusionsConclusions
For American Indian and Alaskan Native For American Indian and Alaskan Native people with diabetes the addition of a nurse people with diabetes the addition of a nurse care coordinator to the primary care health care coordinator to the primary care health system results in:system results in: An increased total number of health care An increased total number of health care
encountersencounters But, more use of primary care and But, more use of primary care and
pharmacy services and less use of pharmacy services and less use of emergency department encounters emergency department encounters suggesting a more efficient and effective suggesting a more efficient and effective utilization of ambulatory servicesutilization of ambulatory services

Evaluation of Full Evaluation of Full Project: AimProject: Aim
To evaluate the effectiveness of a To evaluate the effectiveness of a team of four Nurses providing team of four Nurses providing education and case management to education and case management to American Indian and Alaskan Native American Indian and Alaskan Native people with diabetes in an IHS people with diabetes in an IHS primary care system primary care system

Pilot ProjectPilot Project LocationLocation
Phoenix Indian Medical CenterPhoenix Indian Medical Center Registry 4,112 patients seen in the yearRegistry 4,112 patients seen in the year Nurse Care Coordinator (NCC)Nurse Care Coordinator (NCC)
Four RNs, three had CDE at the timeFour RNs, three had CDE at the time 1,461 different patients (1:365)1,461 different patients (1:365) 2,580 in-person encounters (1.8 encounters)2,580 in-person encounters (1.8 encounters)
Evaluation CohortEvaluation Cohort Patients with patient education documentation and 2 HbA1c’s Patients with patient education documentation and 2 HbA1c’s
within a yearwithin a year Compared those with and those without Case Compared those with and those without Case
management encountermanagement encounter

Process measure documentation in past year
Not Case Managed
N=277
Case Managed
N=793
Odds Ratio (95%
confidence interval)
p-value
Percent Percent
Eye examination 60 80 2.9 (2.1,4.0) 0.0001
Diet Instruction by a registered Dietician
12 28 3.0 (2.0,4.5) 0.0001
Self Monitor Blood Glucose 79 89 2.2 (1.5,3.3) 0.0001
Dental Examination 30 43 1.7 (1.2, 2.2) 0.0002
Comprehensive Foot examination 59 68 1.5 (1.1, 2.0) 0.005
Screening for nephropathy 64 73 1.4 (0.9, 2.0) 0.002
Adjusted for age, sex, treatment type, BMI
Selected adjusted* process measure outcomes of interest among patients included in the evaluation cohort at PIMC, IHS, 2001-2002

Selected adjusted treatment pattern differences among patientsincluded in the evaluation cohort at PIMC, IHS, 2001-2002.
Treatment pattern documentation in past year
Not Case Managed
N=277
Case Manage
dN=793
Odds Ratio (95%
confidence interval)
p-value
Percent Percent
Hyperglycemia Treatment Type*
diet 12 7 0.5 (0.3, 0.9) 0.008
oral 59 65 1.0 (0.8, 1.4) 0.94
insulin/insulin +oral 29 28 1.0 (0.7, 1.3) 0.92
Treatment of Hypertension with ACEi or ARB $
88 85 1.2 (0.8, 1.8) 0.28
Treatment of elevated LDLc with Lipid lowering agents &
32 35 0.8 (0.5, 1.3) 0.41
Use of daily Aspirin # 44 24 0.4 (0.3, 0.6) 0.0001
* Adjusted for age, sex$ Analysis restricted to 736 of the patients in the evaluation cohort with a clinical diagnosis of hypertension& Analysis restricted to 594 of the patients in the evaluation cohort with a low density lipoprotein cholesterol of > 2.58 mmol.L (100mg.dL)# Adjusted for age, sex, treatment type

Qualitative ExperiencesQualitative Experiences
Developing inter-personal Developing inter-personal relationships helps to build trustrelationships helps to build trust
Persistence is required and Persistence is required and rewardedrewarded
Individual assessment facilitates the Individual assessment facilitates the development of a care and education development of a care and education planplan

ResourcesResources Norris SL, Nichols PJ, Caspersen CJ, Glasgow Norris SL, Nichols PJ, Caspersen CJ, Glasgow
RE, Engelgau MM, Jack L, Isham G, Snyder RE, Engelgau MM, Jack L, Isham G, Snyder SR, Carande-Kulis VG, Garfield S, Briss P, SR, Carande-Kulis VG, Garfield S, Briss P, McCulloch D: The effectiveness of disease and McCulloch D: The effectiveness of disease and case management for people with diabetes. A case management for people with diabetes. A systematic review. systematic review. Am J Prev Med Am J Prev Med 2002; 22:15-2002; 22:15-38.38.
Wilson, C, Curtis J, Lipke S, Bochenski C, Wilson, C, Curtis J, Lipke S, Bochenski C, Gilliland S, Description of the Case Load and Gilliland S, Description of the Case Load and Apparent Effectiveness of Nurse Case Apparent Effectiveness of Nurse Case Managers in a Large Clinical Practice: Managers in a Large Clinical Practice: Implications for Workforce Development, Implications for Workforce Development, Diabetic MedicineDiabetic Medicine 2005, (in press) 2005, (in press)

ModelsModels





























