Embed Size (px)
Citation preview
Case Presentation
Managing treatment side effects in the correctional environment
Stephen Tabet, MD, MPHUniversity of Washington Division of Infectious Diseases
Harborview Medical CenterNorthwest AETC
Background
48-year-old Caucasian female presents to the prison infimary with yeast vaginitis. A review of her chart reveals this is her fourth episode since her initial incacercation 2 months ago. She had previously been treated with topical miconazole vaginal suppositories.
On examination, she has erythematous vaginal mucosa with few areas of abrasion; no ulcerations.
What would you do next? At this point, would you do a vaginal yeast culture and
do resistance testing?
Background
The patient is treated with oral fluconazole 150 mg/day for 3 days. HIV testing is done.
One week later, the patient presents asymptomatic with minimal vaginal erythema. She is positive for HIV antibodies.
Among other labs, CD4 count and viral load are done. CD4 T-cell count is 32 and HIV bDNA is >500,000
She is given tmp/smx for PCP prophylaxis and azithromycin for MAC prophylaxis
Next Step?
The patient is expected to be incarcerated another 16 months.
Is offering antiretroviral therapy appropriate or should it be addressed when she is released?
Initial Regimen
An initial regimen of d4T (30 mg) BID (weight adjusted), 3TC (150 mg) BID, and SQV (400 mg) / RTV (400 mg) BID is initiated
One month later - HIV bDNA: 60,575 3 months later - HIV RNA: undetectable (<50 copies);
CD4 count: 219 She has no recurrence of yeast vaginitis
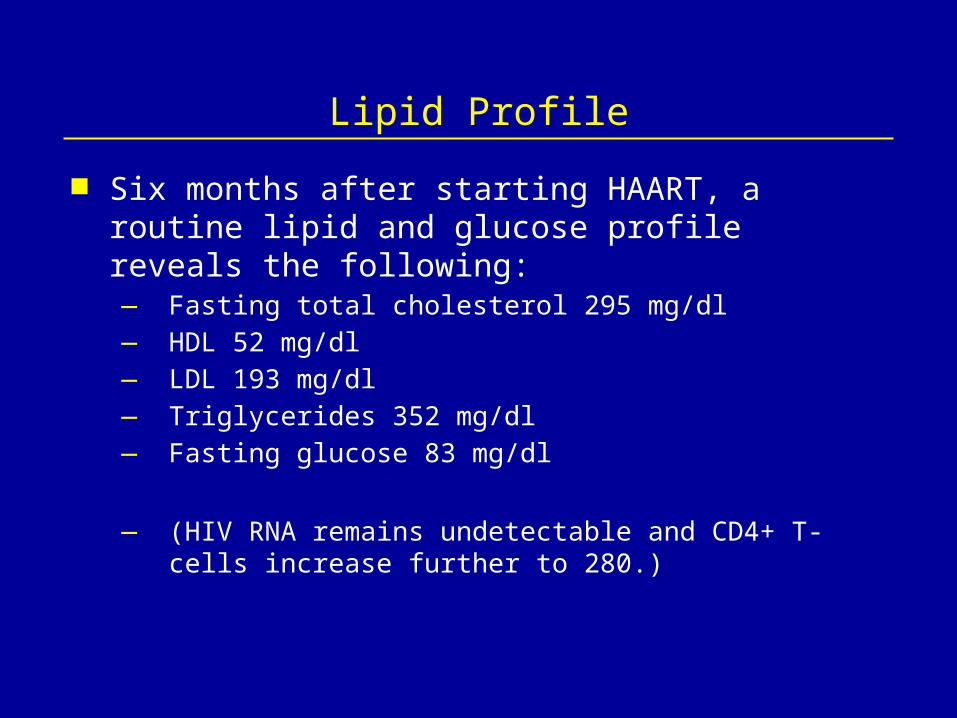
Lipid Profile
Six months after starting HAART, a routine lipid and glucose profile reveals the following:— Fasting total cholesterol 295 mg/dl — HDL 52 mg/dl— LDL 193 mg/dl— Triglycerides 352 mg/dl— Fasting glucose 83 mg/dl
— (HIV RNA remains undetectable and CD4+ T-cells increase further to 280.)
(Carr et al. Lancet. 1999;353:2093-98)
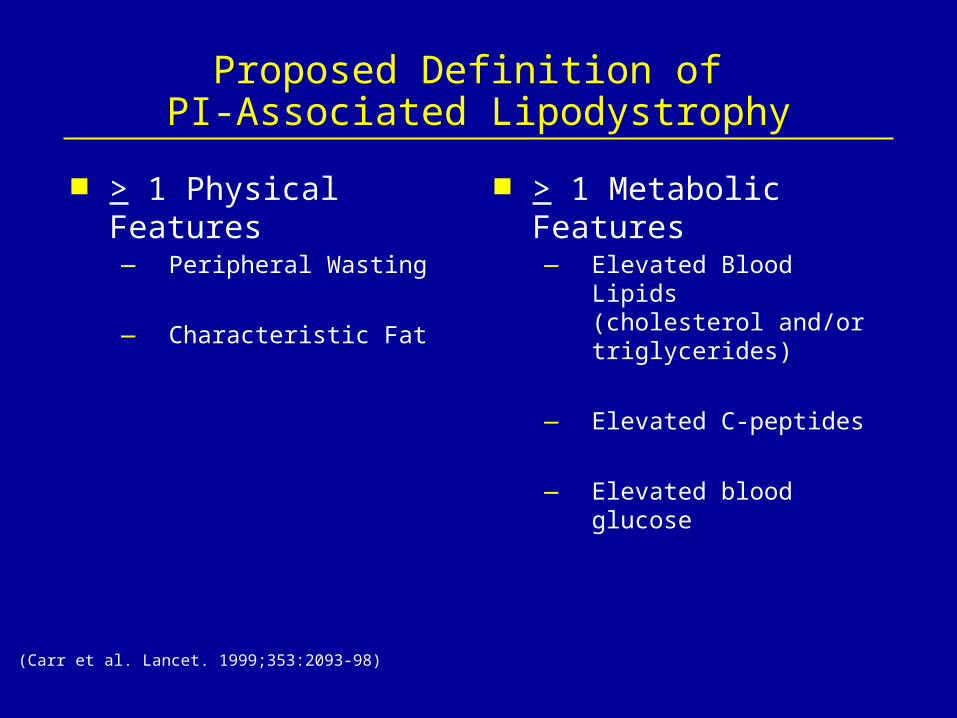
Proposed Definition of PI-Associated Lipodystrophy
> 1 Physical Features— Peripheral Wasting
— Characteristic Fat
> 1 Metabolic Features— Elevated Blood Lipids
(cholesterol and/or triglycerides)
— Elevated C-peptides
— Elevated blood glucose
(Lichtenstein et al. 13th ICOA, 2000)
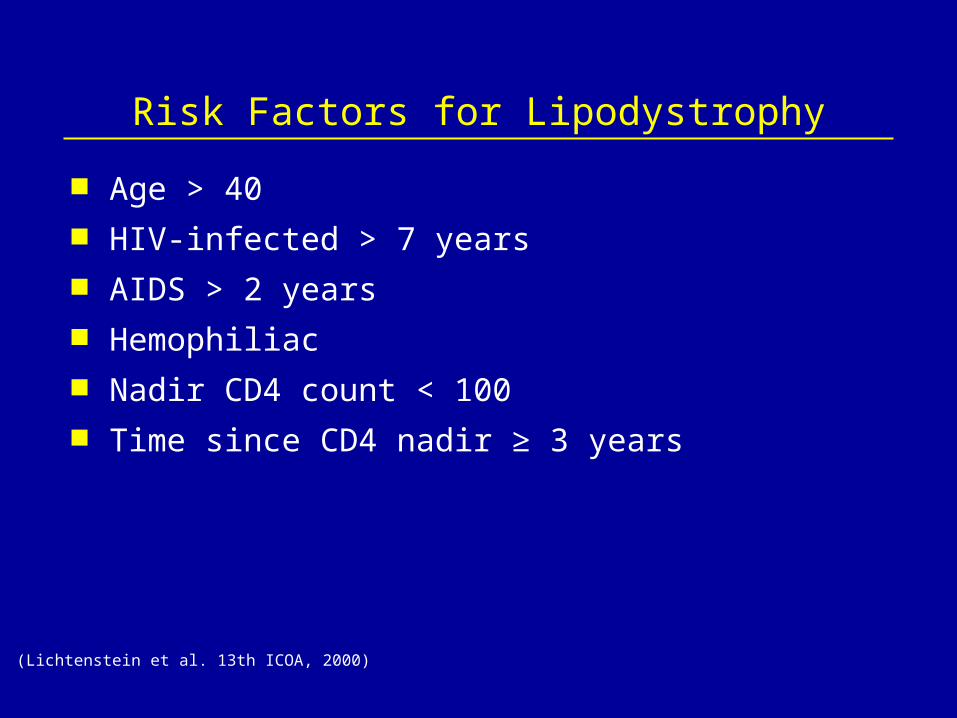
Risk Factors for Lipodystrophy
Age > 40 HIV-infected > 7 years AIDS > 2 years Hemophiliac Nadir CD4 count < 100 Time since CD4 nadir ≥ 3 years
Patient’s Lifestyle
The patient reports eating a regular prison diet consisting of 3800 calories/day. She is placed on a “low-cholesterol diet”.
She doesn’t have hypertension or diabetes mellitus
Discussion
What Would You Do Next? Treat her with a ‘statin’ - HMG-CoA reductase inhibitor Change her regimen to a PI-sparing one Take her off her medications until her lipids
normalize and then restart a different regimen Treat her with gemfibrozil

RTV/SQV, and HMG-CoA Reductase Inhibitors
Pharmacokinetics of Pravastatin, Atorvastatin, and Simvastatin studied in 41 subjects receiving RTV/SQV (400/400 mg) BID
Pravastatin concentrations declined by 50% with RTV/SQV Atorvastatin concentrations increased by 4.5-fold
with RTV/SQV Simvastatin concentrations increased by 31.6-fold
with RTV/SQV Pravastatin may not need dose reduction with RTV/SQV,
but Atorvastatin and Simvastatin should be reduced or avoided for patients taking RTV/SQV
(Fichtenbaum, 7th CROI, 2000)
The Patient is Prescribed Pravastatin
The patient is continued on her current antiretroviral regimen
She is started on Pravastatin (40 mg) QD 3 months later her total cholesterol, LDL, HDL, and
triglycerides have normalized
Patient Presents Visceral Fat Accumulation
One year after starting HAART, the patient reports weight gain in her abdomen and breasts and weight loss in her buttocks, thighs and legs at her follow-up visit for treatment of hypercholesterolemia
The patient’s weight is stable at 119 lbs; her face is normal in appearance with no wasting
Her abdomen is protuberant Her breasts are symmetrically enlarged (since last
examination 7 months prior) with no palpable masses Her thighs and legs are thin but not overtly atrophied
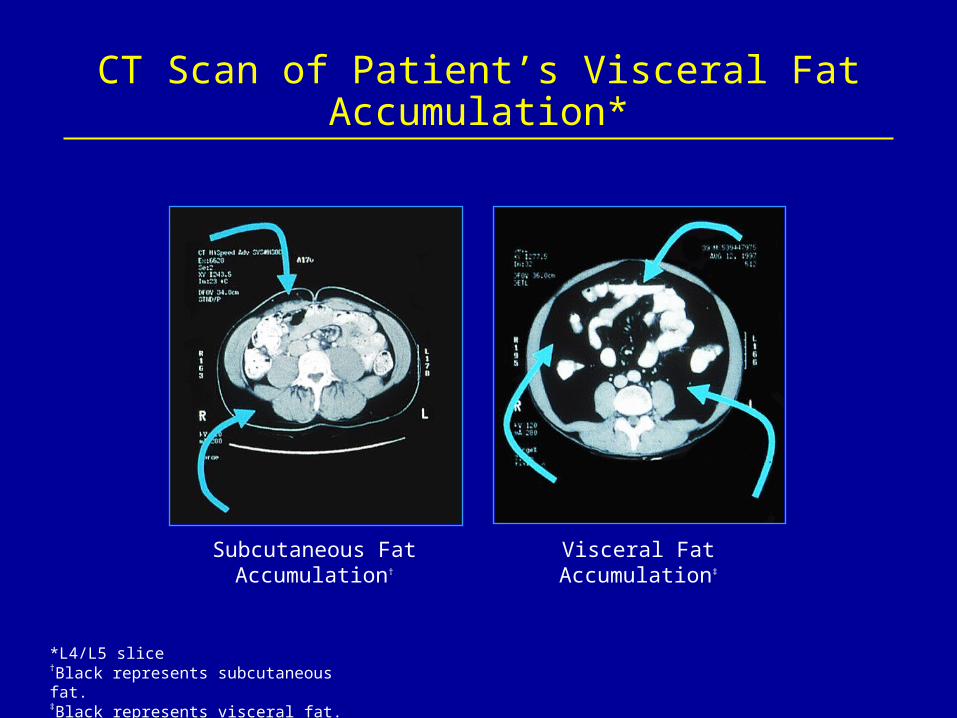
CT Scan of Patient’s Visceral Fat Accumulation*
Subcutaneous FatAccumulation†
Visceral FatAccumulation‡
*L4/L5 slice
†Black represents subcutaneous fat.‡Black represents visceral fat.
(Mulligan. 7th CROI, 2000)
Gender Differences: Lipodystrophy and Metabolic Differences
Women: Greater prevalence of visceral and truncal fat accumulation, insulin resistance and lactic acidosis
Men: Greater prevalence of peripheral fat wasting and hyperlipidemia
Discussion
What would you do? Switch her to a PI-sparing regimen (Studies indicate
that switching to PI sparing regimens rarely resolves lipodystrophy)— Bonnet et al. 7th CROI, 2000— Collier et al. 8th CROI, 2001— Bernasconi 13th Intl AIDS Conference, 2000
The Patient is Continued on Current HAART
The patient is written for a daily exercise regimen She is motivated to continue antiretrovirals

Insulin Resistance
A random blood glucose sample is drawn The patient has a fasting glucose of 187 with a normal
hemoglobin A1c
Discussion
What should you do?
(Hadigan et al. JAMA. 2000;284:472-477)
Metformin Therapy and Insulin Resistance
26 HIV-infected, nondiabetic patients presented fat redistribution and abnormal oral glucose tolerance test (OGTT) results, and they were randomly assigned to receive Metformin (500 mg) BID (n = 14) or identical placebo (n = 12) for 3 months
Main Outcome Measures: Insulin area under the curve (AUC), calculated 120 minutes following a 75-g OGTT at baseline vs a 3-month follow-up
Metformin Therapy andInsulin Resistance
Results: Patients treated with Metformin demonstrated significant reductions in mean (SEM) insulin AUC 120 minutes after OGTT and at 3 months
The study suggests that a relatively low dosage of Metformin reduces insulin resistance and related cardiovascular risk parameters in HIV-infected patients with lipodystrophy
(Hadigan et al. JAMA. 2000;284:472-477)
Patient is Started on Metformin
The patient is started on Metformin (500 mg) BID She is cautioned about the potential for lactic acidemia

Managing Dyslipidemia in HIV: Conclusions
Dyslipidemia is influenced by HAART and host factors
Disease progression is involved in the development of dyslipidemia
Treatment changes should not be made without careful consideration of virologic and immunologic outcomes
Symptoms management and lifestyle changes should be the focus of patients with dyslipidemia