Embed Size (px)
Citation preview

Case Presentation Webinar
Care of a long stay
critically ill child
Heide Kunzmann 4 February 2013
Presented in collaboration with
the Child Nurse Practice
Development Initiative

Introduction
Who is this child? • Name: Jacob (Name changed for confidentiality)
• DOB: 21\01\2011
• Age: 2 years
• Weight: 11.8kg
• Birth weight: 2.8kg
• Admission date:15\01\2013
• Admission reason: Acute flacid paralysis

Genogram
23yr 20yr
Jacob
2011
56yr 56yr
17yr 16yr
PURPLE blocks denote those
people that live together

Some background
• This child lives in a family where his maternal great
grandfather and great grandmother are the
breadwinners.
• His own father does not work, neither does his mom.
They both have grade 10.
• His two uncles dropped out of school and have no
income.
• They stay in a brick home, open plan with an enclosed
bathroom (running water, electricity and a toilet in the
house).
• This house is on the outskirts of George.

The story of Jacob…
• Born at term, NVD, no complications
• A well child till March 2012

March 2012
• He presented with a 8 day history of weakness in his legs
• He had a squint and had ophtalmoplegia
• Initially thought to be TBM because he had a positive TB contact (father)
• CT brain normal
• Deteriorated and required intubation and ventilation on 13\3\2012 in George hospital
• Transferred to Red Cross War Memorial Children’s Hospital (RCWMCH)
• Guillain-Barre Syndrome (GBS) was diagnosed and sucsessfully treated
• Stayed till 11\5\2012 at RCWMCH, then transferred back to George
• Well rehabilitated, walked in August 2012

Growth Chart
• Born on the 10th.
• Grew along the 25th
centile.
• Noted to track above
the 25th centile
during first admission
to hospital.

GBS pathophysiology
Background
• Identified in 2 french soldiers by physicians Guillain and
Barre in 1916.
• Initially thought to be a single disorder, but today there
are several variants.
• Guillian-Barre syndrome is a collection of clinical
symptoms of weakness and diminished reflexes.
• In countries where poliomelitis is under control, GBS is
the most important form of acute flassid paralysis [1]

GBS pathophysiology continued..
• Post infectious immune-mediated disease, usually
respiratory and gastrointestinal.
• During infection the body launches an immune response.
• Some of the antigens of the infectious agents capsules
are the same as those in the nerves.
• This leads to the bodies own immune response to cross
react with the gangliosides and glycolipids that are in the
myelin in the peripheral nervous system.
• This leads to immunologic damage to the peripheral
nervous system
• This leads to delay in conduction causing flaccid
paralysis

Disease pathophysiology
• Miller-Fisher syndrome is a variant of GBS
• 5% of all GBS
• Signs and symptoms include:
• Ataxia
• Areflexia
• Ophthalmoplegia -very important feature
• Limb weakness
• Ptosis
• Facial palsy
• Bulbar palsy

Prognosis
• Good recovery 1-3 months
• Peak weakness 10-14 days
• Average time on ventilator 50 days [1]
• Death in 2-12% [1]
commonly secondary to complications
related to GBS
• Respiratory distress
• Sepsis
• Thromboembolic disease, biggest cause is paralysis and
ventilation
• Persistent motor defect (foot drop, muscle wasting,
sensory ataxia) occurs in a significant percentage of
survivors
• Recurrence of GBS occurs in 2-5% of patients [2]

January 2013 Mom noticed something was not so
well with Jacob…
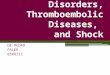
Jacob’s presentation at
George Hospital
8\01 10\01 12\01 13\01 11\01
• Head lag
• Drooling
• Poor
feeding
(mom
complained
about this,
only able to
eat some
jelly) • Dehydrated,
Hypovolemic
• Diplopia and
squinting\eyelids
normal
• Bulbar weakness,
pooling secretion
• Slight cough
• Flaccid arms,
reflexes
• Legs no
reflexes\power
3+, moving
against gravity
• Diaphragm
normal, but
bilateral LL
collapse
• Urine retention
• Investigations
done
Admitted to
George
hospital
Intubated
Referred to
RXH

How was the condition diagnosed
and treated? (George hospital)
• Investigations
• LP-proteine .21 (on admission)
• MRI\CT brain
• CXR done-not suggestive of PTB LL collapse
• Herpes\Enterovirus\Cocksackie
• LP-proteine now .43 (day 5)
• Assessments
• Clinical-differencial diagnosis (TBM,Herpes\bacterial
Meningitis)
• Medications
• Aciclovir
• TB treatment restarted
• Ceftriaxone

Current admission to RCWMCH…
• Came on a fixed wing plane
• At this point – strong suspicion of GBS
• Presentation at admission:
• Ophthalmoplegia - Paralysis of extraocular muscles reponsible for eye movements.
• Strabismus
• Bulbar weakness
• Dysphagia
• Drooling
• Diplopia
• Flaccid arms, reflexes
• Legs no reflexes\power 3+, moving against gravity

• Strong clinical evidence of Guillain-Barre syndrome (Miller
Fisher variant) due to the cranial nerve involvement.
15\01 17\01 25\01 27\01 18\01
• Polygam
• T\A, B\C
and urine
MC&S was
done
• Tracheostomy
• Aciclovir and
Cefotaxime
stopped
• All cultures
came back
negative
• Investigations
done for
mycoplasma,
cocksakie,
enterovirus
• Porphyria test
done
• MRI brain-
consistent
with GBS
• TB treatment
stopped
• Reinsertion of
urinary catheter
for urine
retention
• Picorna virus
came back
positive (Entero
virus)
• Augmentin
started due to
1000000 mixed
growth on urine
Jacob’s investigations and
treatment at RCWMCH
Looking for
cause of GBS

Nursing care 1
Facilitate mother-child interaction • Make sure that the mom understands what is
GBS. Have frequent contact sessions to ensure she understands.
• This will decrease her anxiety so that she can have a calming and reassuring influence on her child.
• Important to get the mom involved in caring for her child, this is going to be a long stay.
• Empowerment of the mom.
• As well as comfort to the child-making the child feel safe during an extreemly distressing time.

Nursing care 2
Non pharmacological Tx • Regular turnings and ROM
exercises, with proper positioning
to prevent shortening of muscles
• Distraction
• Multi-disciplinary team approach
• Eye patches to help with diplopia
• Tears to prevent dying out of eyes
• Full ventilation to comfort, do not
try to wean
Pharmacological Tx
• Morphine (stop after
tracheostomy done)
• Valeron (for stretches)
• Clonidine (taper down after a
week)
• Paracetamol
• Gabapentin (increase with
increments)
Manage pain and provide comfort • Patients with GBS describe the pain as severe and
distressing[1] - aching, throbbing and shock like pain,
particularly over the shoulders, buttocks and thighs,
Reason - immobility.

Nursing care 3
Promote good nutrition
• Ensure the dietician is consulted to work out the
calories needed.
• MVT, Folic and Zinc is added.
• Involve the speech therapist to promote
communication and establish safe swallowing.
Ensure hydration
• Monitor intake and output.
• Pay attention to ensenceable losses, due to
autonomic nerves system involvement they sweat a
lot.

Nursing care 4
Reduce microbial load • Implement the VAP bundle
• Adhere to basic infection control policies
Maintain skin and mucosal integrity • Due to diaphoresis (autonomic changes), ensure
you wash and dry them well.
• Let him lie on cotton.
• Dry his neck often due to the drooling.
• Regular turning due to paralysis-prevent pressure sores
• Ensure splints are applied properly

Nursing care 5
Support regulatory system
• Due to the autonomic nervous system
involvement, it is possible that the patient may
become bradycardic - ensure BP is adequate
and patient is saturating well.
• Urinary retention due to urinary sphincter
involvement - ensure bladder is not distended and
that patient is passing a good amount of urine –
Jacob failed 2 attempts to remove his catheter
• Bowel paresis and gastric dysmotility - ensure
patient does not become constipated (Sorbitol)

Nursing care 6
Promote development
• The groundwork for reading and writing is done
during the next year- reading to Jacob is important,
showing him the pictures.
• Math skills are learnt through solving problems like 8
piece puzzle sets or stacking rings - assist him in
playing these games.
• Creativeness is explored by shaking things to make
a sound, playing with clay - OT and the music man.
• Socialising by playing alongside another child - the
child in the bed space next to him also has GBS[3]

Reflecting back on the care of Jacob
• Essential to have a multi-disciplinary approach to a child diagnosed
with GBS.
• It takes a big team to care for this child (OT, speech therapist, physio,
dietician, music therapist, aromatherapist, nurses and doctors) and
the mom should be actively involved.
• Age appropriate care is important when doing daily activities.
• The biggest risk factors that can lead to complications are mechanical
ventilation and immobilisation.
• Pain control is important.
• Establishing ways of communication is very important.
• There is no way of caring for a child with GBS if you are not willing to
work in a team and actively involving the mother.

References
1. Guillain-Barre Syndrome
http://emedicine.medscape.com/article/315632-
overview [Accessed 1st February 2013]
2. Das. A., Kalita, J. and Misra, U.K. 2004 Recurrent
Guillain Barre’ syndrome. Electromyography Clinical
Neurophysiology.; 44(2): 95-102
3. Child Development Tracker – Your two year old.
http://www.pbs.org/parents/childdevelopmenttracker/tw
o/ [Accessed 3rd February 2013]