Embed Size (px)
Citation preview

257A case of fever of unknown origin: Necrotizing sarcoid granulomatosis
A case of fever of unknown origin: Necrotizing sarcoid granulomatosis G. Ünlü1, T.A. Önyılmaz2, S.A. Barış2, N. Turhan2, Ç. Vural3, İ. Başyiğit2, H. Boyacı2
1Department of Clinical Microbiology and Infectious Diseases. Haseki Training and Research Hospital, İstanbul, Departments of 2Chest Diseases, 3Pathology, Faculty of Medicine, University Kocaeli, Turkey
Case report Clin Ter 2014; 165 (5):257-260. doi: 10.7417/CT.2014.1756
Correspondence: Dr. Serap Argun Barış. Kocaeli University Faculty of Medicine, Department of Chest Diseases, Umuttepe, Kocaeli, Turkey. Tel.: +90.26230.37211. E-mail: [email protected]
Copyright © Società Editrice Universo (SEU)ISSN 0009-9074
Introduction
Necrotizing sarcoid granulomatosis (NSG) was first described by Liebow (1) in 1973 as one of five forms of pulmonary angiitis and granulomatosis (Wegener’s granulo-matosis, limited Wegener’s granulomatosis, lymphomatoid granulomatosis, NSG, and bronchocentric granulomatosis) unrelated to infection or connective tissue disorders. The etiology and pathogenesis of NSG is still not fully clear. Sarcoid-like granulomas, necrosis, and granulomatous vasculitis are the most important indications of the disease. Because of pulmonary involvement, skin lesions, and rarely detected uveitis, NSG is separated from sarcoidosis, and because of its benign clinical course, it is separated from Wegener’s granulamatosis (2).
The main symptoms of NSG are dyspnea, cough, and chest pain. Fever, fatigue, weakness, and weight loss are sometimes observed, or the patient may be asymptomatic. NSG is rarely detected in the etiology of fever of unknown origin (FUO). Here in, we present a case of FUO that persisted for one year, with fatigue and weakness present.
Abstract
Necrotizing sarcoid granulomatosis is a rare type of vasculitis; its etiology and pathogenesis are still unknown. The disease primarily affects the lungs, although extra-pulmonary involvement has been reported. The typical symptoms are cough, chest pain, dyspnea, and weight loss; high temperatures have been reported in rare cases. We present the case of a 65-year-old woman who was diagnosed with lymph node tuberculosis, for which she received treatment for six months. The patient experienced no improvement in her symptoms, which included fever, weakness and dyspnea. A re-evaluation of previ-ously collected thoracoscopic biopsy material revealed compatibility with necrotizing sarcoid granulomatosis. Clin Ter 2014; 165(5):257-260. doi: 10.7417/CT.2014.1756
Key words: dyspnea, fever of unknown origin, necrotizing sarcoid granulomatosis, vasculitis
Despite ongoing treatment for tuberculosis administered due to a diagnosis of granulomatous lymphadenitis, the patient’s clinical and radiological findings did not improve. Therefore, the case was examined as a case of FUO, and because of the NSG finding in its etiology, the case was found to be interesting.
Case report
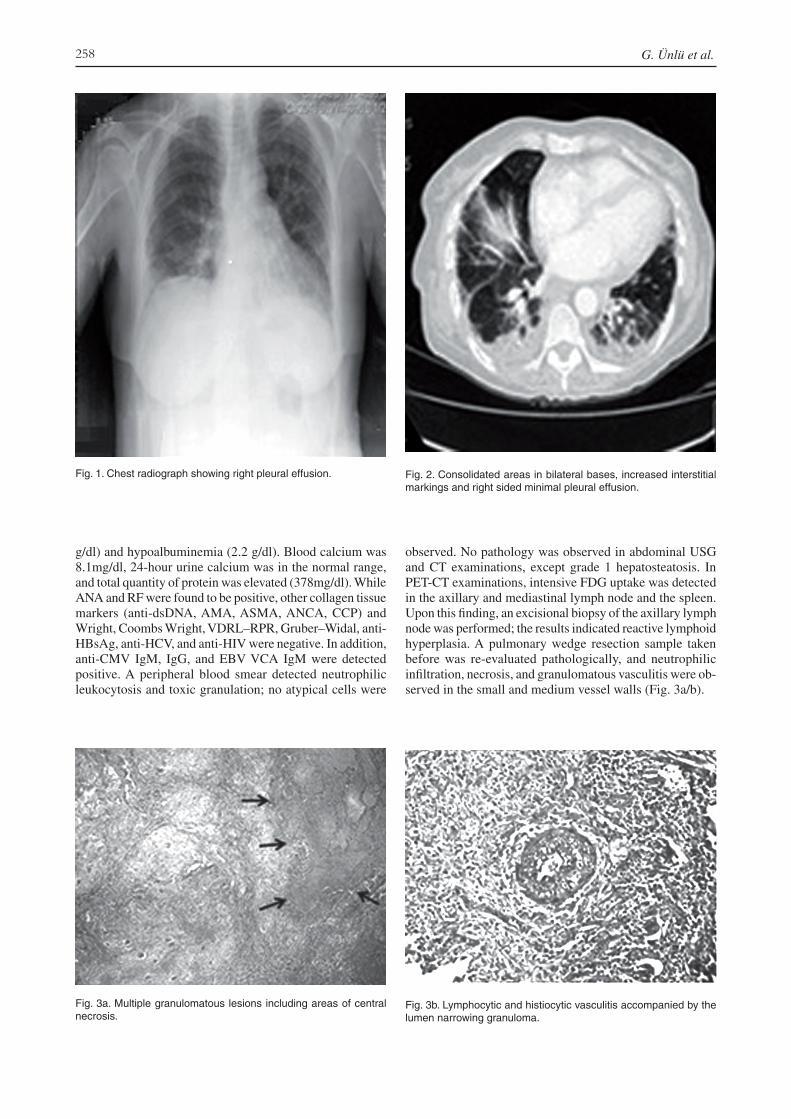
A 65-year-old female patient was admitted with a fever that had persisted for one year, fatigue, weakness, shortness of breath, and intermittent dry cough. On physical examina-tion, the patient was conscious and cooperative; respiratory rate was 16/min, pulse rate was 76/min, and blood pressure was 120/80 mmHg. During a systemic examination, inspira-tory crackles were detected. A computed tomography (CT) scan had been taken six months prior in a health care center, after admittance due to her ongoing complaints; the results showed mediastinal lymphadenopathy and pulmonary nodules. In order to clarify the diagnosis, a surgical wedge biopsy was conducted; the results revealed necrotizing gra-nulomatous inflammation, and anti-tuberculosis treatment was started (INH 300 mg, RFM 600 mg, EMB 1500 mg, PZA 4000 mg). After the six-month INH 300 mg + RFM 600 mg treatment was completed, minimal pleural effusion in the right lung was detected in her control chest radiography, and radiological recovery was observed (Fig. 1).
A control CT revealed right axillary, paratracheal, sub-carinal and right hilar maximum 17 mm LAP, consolidated areas in bilateral bases, increased interstitial markings, and right-sided minimal pleural effusion (Fig. 2).
No significant lymph node size diversity was detected when comparing the current CT with the one scanned six month prior.
The patient, who had a continuous fever and cough, had been admitted as FUO; blood and urine cultures obtained during febrile periods were negative. In order to determine the etiology of the FUO, the patient’s serological tests were studied. Laboratory tests revealed mild anemia (Hb: 11.1
258 G. Ünlü et al.
g/dl) and hypoalbuminemia (2.2 g/dl). Blood calcium was 8.1mg/dl, 24-hour urine calcium was in the normal range, and total quantity of protein was elevated (378mg/dl). While ANA and RF were found to be positive, other collagen tissue markers (anti-dsDNA, AMA, ASMA, ANCA, CCP) and Wright, Coombs Wright, VDRL–RPR, Gruber–Widal, anti-HBsAg, anti-HCV, and anti-HIV were negative. In addition, anti-CMV IgM, IgG, and EBV VCA IgM were detected positive. A peripheral blood smear detected neutrophilic leukocytosis and toxic granulation; no atypical cells were
observed. No pathology was observed in abdominal USG and CT examinations, except grade 1 hepatosteatosis. In PET-CT examinations, intensive FDG uptake was detected in the axillary and mediastinal lymph node and the spleen. Upon this finding, an excisional biopsy of the axillary lymph node was performed; the results indicated reactive lymphoid hyperplasia. A pulmonary wedge resection sample taken before was re-evaluated pathologically, and neutrophilic infiltration, necrosis, and granulomatous vasculitis were ob-served in the small and medium vessel walls (Fig. 3a/b).
Fig. 1. Chest radiograph showing right pleural effusion. Fig. 2. Consolidated areas in bilateral bases, increased interstitial markings and right sided minimal pleural effusion.
Fig. 3a. Multiple granulomatous lesions including areas of central necrosis.
Fig. 3b. Lymphocytic and histiocytic vasculitis accompanied by the lumen narrowing granuloma.

259A case of fever of unknown origin: Necrotizing sarcoid granulomatosis
After evaluating the clinical findings together, the patient was diagnosed with NSG, and treatment with methylpred-nisolone (40mg/day) was started. With the treatment, the patient’s fever, fatigue, and weakness symptoms diminished. A thorax CT taken after three months of treatment showed a decrease in lymph node size, and total regression of the pleural effusion and consolidation areas (Fig. 4).
Discussion
In this article, we present a female patient who was diagnosed with a necrotizing granulomatous etiology of sar-coidosis. The patient suffered continuous fever, despite her ongoing treatment for diagnosed tuberculosis lymphadenitis. NSG, a rarely seen type of granulomatous vasculitis, was first described by Liebow (1) in 1973 as one of five forms of pulmonary angiitis and granulomatosis unrelated to infection or connective tissue disorders. The five forms are defined by their histological structures and other features of natural history: 1. classical Wegener’s granulomatosis (WG); 2. limited angiitis and granulomatosis of the Wegener type; 3. lymphomatoid granulomatosis; 4. NSG; and 5. broncho-centric granulomatosis. The clinical and radiological signs may be confused with sarcoidosis, malignancy, and WG, although NSG has a benign course. Diagnosis is difficult and time consuming, and NSG diagnosis does not have a specific laboratory investigation. Diagnostic histopatholo-gical findings are sarcoid-like granulomas, necrosis, and granulomatous vasculitis.
Although the previously mentioned granulomatous pul-monary diseases are common findings in routine diagnosis, NSG is usually confused with sarcoidosis in practice. Extra-pulmonary uptake is seen more frequently in sarcoidosis than in NSG, and rarely seen pleural involvement and vasculitis are significant in making a differential diagnosis between NSG and sarcoidosis (3-5). In radiological analysis, single or multiple nodular densities are usually seen; therefore,
there are cases in the literature that were initially thought to be metastasis. Because of the histopathological presence of granulomas and the radiological detection of nodules, differential diagnosis with Wegener’s granulomatosis and examination of ANCA levels are recommended (6, 7).
Cough, chest pain, dyspnea, fatigue, and weakness are the main symptoms of NSG. Although subfebrile tempera-tures have been reported, NSG is rarely seen in the etiology of FUO (4).
The clinical and histopathological findings of NSG might cause it to be confused with tuberculosis, especially in regions where tuberculosis is endemic. In our case, the patient was initially considered to have tuberculosis due to an observation of necrosis and granuloma in an open lung biopsy. During the clinical course, the patient did not respond well to the routine tuberculosis treatment, and her fever did not regress. Consequently, after a re-evaluation of the initial pathology results, the patient was diagnosed with NSG.
In conclusion, the pathophysiology of NSG has not yet been fully clarified, and it might be confused with the granulomatous vasculitis of autoimmune diseases such as Wegener’s granulomatosis, sarcoidosis, hypersensitivity pneumonitis, and Sjögren syndrome, as a result of the cli-nical and histopathological findings. In this case, we believe that NSG might be the etiology of the long-lasting fever, and especially in regions where tuberculosis is endemic, a conclusive differential diagnosis with tuberculosis should be made.
References
1. Yeboah J, Afkhami M, Lee C, et al. Necrotizing sarcoid granulomatosis. Curr Opin Pulm Med 2012; 18:493-8
2. Ozcan A, Demirag F, Okten F, et al. Necrotizing Sarcoid Granuloma Mimicking a Metastatic Lung Cancer, A Case Report. Respir Dis 2007; 18:71-4
Fig. 4. Thorax CT taken after three months of treatment showed a total regression of the pleural effusion and consolidation areas.

260 G. Ünlü et al.
3. Panigada S, Ullmann N, Sacco O, et al. Necrotizing sarcoid granulomatosis of the lung in a 12-year-old boy with an at-ypical clinical course. Pediatr Pulmonol 2012; 47(8):831-5
4. Abdelmoula S, Ben Brahim E, Lagha M, et al. Sarcoid-like necrotizing granulomatosis. A case report. Rev Pneumol Clin 2002; 58(6 Pt 1):351-4
5. Chittock DR, Joseph MG, Paterson NA, et al. Necrotizing Sarcoid Granulomatosis with Pleural Involvement: Clinical
and Radiographic Features. Chest 1994; 106:672-66. Quaden C, Tillie-Leblond I, Delobbe A, et al. Necrotising
sarcoid granulomatosis: clinical, functional, endoscopical and radiographical evaluations. Eur Respir J 2005; 26:778-85
7. Strickland-Marmol LB, Fessler RG, Rojiani AM. Necrotizing Sarcoid Granulomatosis Mimicking an Intracranial Neopla-sm: Clinicopathologic Features and Review of the Literature. Mod Pathol 2000; 13(8):909-13





























