Embed Size (px)
Citation preview

Case Report
Acute fibrinous and organizing pneumonia in systemic lupuserythematosus: A case report and review of the literaturepin_2586 755..759
Lida P. Hariri,1 Sebastian Unizony,2 John Stone,2 Mari Mino-Kenudson,1 Amita Sharma,3 Osamu Matsubara4
and Eugene J. Mark1
1Department of Pathology, 2Department of Rheumatology, 3Department of Radiology, Massachusetts GeneralHospital, Boston, Massachusetts, USA and 4Department of Pathology, National Defense Medical College,Tokorozawa, Japan
Pulmonary manifestations of systemic lupus erythemato-sus (SLE) typically include pleuritis, alveolar hemorrhage,and infectious pneumonia due to immunosuppression withless common entities including bronchiolitis, interstitialpneumonia, and pulmonary fibrosis. More rare manifesta-tions include organizing pneumonia (OP) and diffuse alveo-lar damage (DAD). A similar but distinct entity of acutefibrinous and organizing pneumonia (AFOP), characterizedby intra-alveolar fibrin deposition and associated organiz-ing pneumonia, has been reported in association with con-nective tissue disorders, but has not been described inassociation with SLE. Reported herein is a patient with SLEand accompanying antiphospholipid syndrome with recentpulmonary embolism, persistent respiratory symptomology,and persistent radiographic abnormalities who underwentlung biopsy displaying features of AFOP. This case in con-junction with previous literature indicates that AFOP can bea manifestation of connective tissue disease including SLEand may be an underreported variant of medical lungdisease due to overlap in histological characteristics withOP and DAD.
Key words: collagen vascular disease, connective tissuedisease, diffuse alveolar damage, fibrinous organizing pneumo-nia, interstitial pneumonitis
INTRODUCTION
Systemic lupus erythematosus (SLE) is an autoimmune dis-order which may affect virtually any organ system, with
principal manifestations including serositis, arthritis, renal,dermatologic, and pulmonary involvement.1 Pulmonarypathology in SLE is common, including pleuritis, alveolarhemorrhage, and infectious pneumonia with less commonentities including bronchiolitis, interstitial pneumonitis includ-ing usual interstitial pneumonia and non-specific interstitialpneumonitis, interstitial fibrosis, pulmonary hypertension,and pulmonary embolism and infarction associated withantiphospholipid syndrome.1–6 More recently, the occurrenceof organizing pneumonia (OP) and diffuse alveolar damage(DAD) have been documented in patients with SLE andcharacterized by an acute or subacute clinical picture withdyspnea, cough, and/or hemoptysis.3,5,7–10
Acute fibrinous and organizing pneumonia (AFOP)recently has been recognized as an entity with histologicalsimilarities to OP, DAD, and eosinophilic pneumonia (EP).However, it has a distinct overall histological pattern, charac-terized by intra-alveolar fibrin associated with organizingpneumonia, the latter consisting of loose intraluminal connec-tive tissue and lymphohistiocytic infiltrate in a patchy distri-bution. Acute fibrinous and organizing pneumonia lacks thepresence of hyaline membranes classically seen in DAD,intrabronchiolar fibrosis seen in OP, and eosinophilic infiltrateseen in EP.11,12 In the initial study of 17 patients describingAFOP as a distinct entity, one patient had polymyositis, onepatient had ankylosing spondylitis, and one patient had fibro-myalgia. Other associations seen in this study included amio-darone exposure, Haemophilus influenza, Acinetobacter,lymphoma, hairspray use, construction work, coal mining,and zoological work, each in one patient.11 Prior case reportsin the literature have also reported AFOP in association withjuvenile dermatomyositis,13 a patient with collagen vasculardisease symptomology including joint pain, red papular skinlesions, myalgias and anti-nuclear antibody (ANA) positivity,but no documented specific disease,14 stem cell transplantfor acute myelogenous leukemia,15 hypersensitivity to
Correspondence: Lida Hariri, MD, PhD, Massachusetts GeneralHospital, 55 Fruit St., Warren Building Room 219, Boston, MA 02114,USA. Email: [email protected]
Received 22 April 2010. Accepted for publication 24 June 2010.© 2010 The AuthorsPathology International © 2010 Japanese Society of Pathology andBlackwell Publishing Asia Pty Ltd
Pathology International 2010; 60: 755–759 doi:10.1111/j.1440-1827.2010.02586.x
abacavir therapy in an HIV positive patient,16 and in a numberof cases with no known association (Table 1).7,17–21 Acutefibrinous and organizing pneumonia has not been associatedwith SLE to date. We present a case report of AFOP in apatient with SLE.
CLINICAL SUMMARY
A 47 year old man was admitted to Massachusetts GeneralHospital (MGH) with worsening dyspnea on exertion for3–4 weeks and associated cough productive of greenishsputum. He had been diagnosed with SLE at age 39, withmanifestations including oral ulcers, arthritis, pleuropericardi-tis, leukopenia, high anti-nuclear antibody titers, and positiveanti-double stranded DNA and Smith antibodies. His symp-toms had been controlled with prednisone 20 mg daily. At age44, he developed antiphospholipid syndrome with ischemiaof the left 5th finger, with persistently elevated antiphospho-lipid antibodies. Other past medical history included large Bcell lymphoma diagnosed at age 44, in remission after sixcycles of CHOP + rituximab, and latent tuberculosis treatedwith isoniazid at age 39. The patient smoked half a pack ofcigarettes daily for 25 years, but quit smoking 1 month priorto admission.
Before admission to hospital, the patient himself increasedhis glucocorticoid dose from baseline 20 mg to 40 mg dailyfor approximately one week, with a subsequent increase to75 mg daily for several days, and then 100 mg daily for3 days before presenting to MGH, but his dyspnea andcough did not improve despite the increased steroid dosing.On admission, angiographic CT of the chest was performed.It revealed multiple segmental and subsegmental pulmonaryemboli and bilateral air space consolidations with air bron-chograms. He was given levofloxacin and began anticoagu-lation with unfractionated heparin. His prednisone wastapered down to 20 mg daily over 1 week.
Transthoracic echocardiography showed pericardial thick-ening with constrictive physiology. He underwent bronchos-copy on hospital day 3, at which time bronchio-alveolarlavage was performed. Cytologic examination revealed pul-monary macrophages with mixed inflammation and no evi-
dence of malignant cells. Flow cytometry showed noevidence of a monoclonal B or unusual T cell population. Thepatient left the hospital against medical advice on hospitalday 4 on enoxaparin sodium (Lovenox).
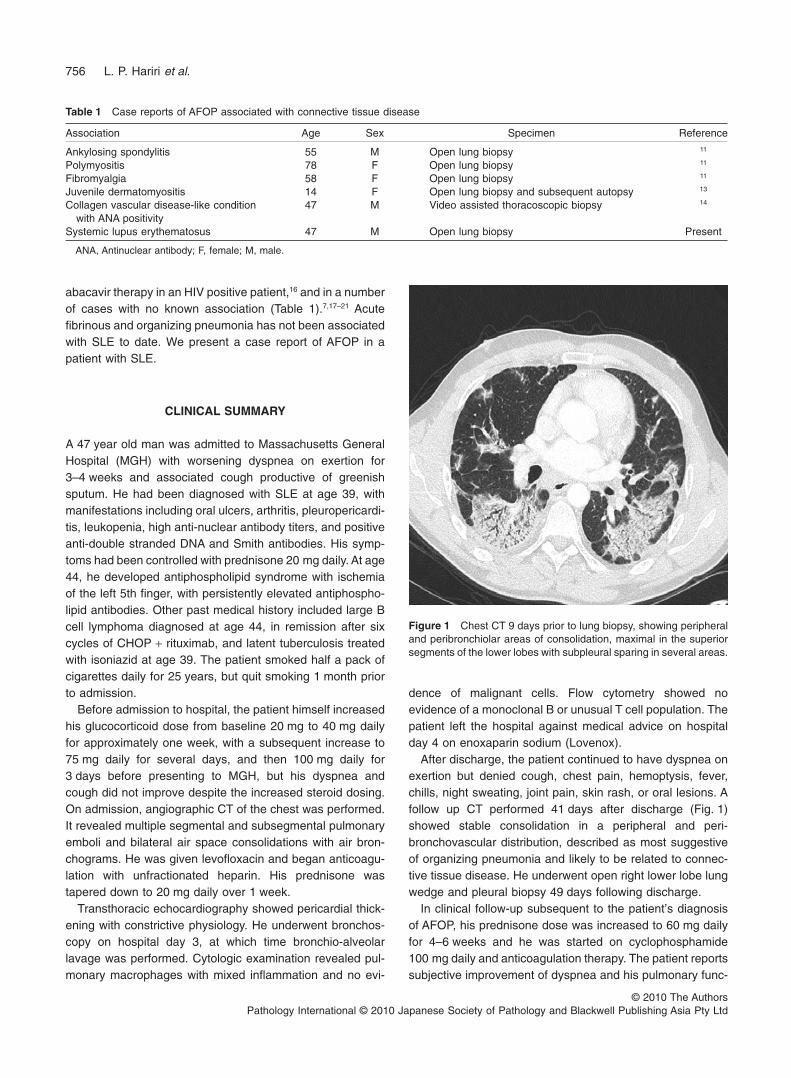
After discharge, the patient continued to have dyspnea onexertion but denied cough, chest pain, hemoptysis, fever,chills, night sweating, joint pain, skin rash, or oral lesions. Afollow up CT performed 41 days after discharge (Fig. 1)showed stable consolidation in a peripheral and peri-bronchovascular distribution, described as most suggestiveof organizing pneumonia and likely to be related to connec-tive tissue disease. He underwent open right lower lobe lungwedge and pleural biopsy 49 days following discharge.
In clinical follow-up subsequent to the patient’s diagnosisof AFOP, his prednisone dose was increased to 60 mg dailyfor 4–6 weeks and he was started on cyclophosphamide100 mg daily and anticoagulation therapy. The patient reportssubjective improvement of dyspnea and his pulmonary func-
Table 1 Case reports of AFOP associated with connective tissue disease
Association Age Sex Specimen Reference
Ankylosing spondylitis 55 M Open lung biopsy 11
Polymyositis 78 F Open lung biopsy 11
Fibromyalgia 58 F Open lung biopsy 11
Juvenile dermatomyositis 14 F Open lung biopsy and subsequent autopsy 13
Collagen vascular disease-like conditionwith ANA positivity
47 M Video assisted thoracoscopic biopsy 14
Systemic lupus erythematosus 47 M Open lung biopsy Present
ANA, Antinuclear antibody; F, female; M, male.
Figure 1 Chest CT 9 days prior to lung biopsy, showing peripheraland peribronchiolar areas of consolidation, maximal in the superiorsegments of the lower lobes with subpleural sparing in several areas.
756 L. P. Hariri et al.
© 2010 The AuthorsPathology International © 2010 Japanese Society of Pathology and Blackwell Publishing Asia Pty Ltd

ba
dc
Figure 2 Patchy distribution of intra-alveolar fibrin in the form of fibrin ballswithout formation of hyaline membranes.Alveolar septa in affected areas havechronic inflammation, but fibrosis isessentially absent in areas of acute fibrin-ous and organizing pneumonia (AFOP).(a) Hematoxylin-eosin 10¥. Scale bar =30 mm. (b) Hematoxylin-eosin 40x. (c)Periodic acid Schiff stain 40x (d)Trichrome stain 40¥. Scale bar = 10 mm.
Figure 3 Background of diffuse intersti-tial pneumonitis and fibrosis in areas unaf-fected by acute fibrinous and organizingpneumonia (AFOP). (a) Hematoxylin-eosin 10x (b) Trichrome 10x. Scalebar = 30 mm.
a b
a b
Figure 4 Mild patchy intra-alveolar hem-orrhage with small amounts of hemosid-erin deposition. (a) Hematoxylin-eosin 20x(b) Iron Stain 20x. Scale bar = 15 mm.
A case report of AFOP in SLE 757
© 2010 The AuthorsPathology International © 2010 Japanese Society of Pathology and Blackwell Publishing Asia Pty Ltd

tion tests have shown 25% improvement, including increasesin full expiratory volume over 1 s, full vital capacity, total lungcapacity, and vital capacity.
PATHOLOGIC FINDINGS
Two right lower lobe lung wedge biopsies and a pleuralbiopsy were performed. The biopsies were fixed in neutralbuffered formalin, embedded into paraffin, and sectioned into5 mm thick sections. Morphological characteristics wereassessed on standard hematoxylin and eosin (H&E) stainedsections.
The dominant diagnostic finding in the lung biopsies wasthe presence of intra-alveolar fibrin in the form of fibrin ‘balls’within the alveolar spaces in a patchy distribution within thelung parenchyma, occupying approximately 25% of thespecimen (Fig. 2). Lung parenchyma associated with areasof intra-alveolar fibrin accumulations also displayed an inter-stitial lymphoplasmacytic infiltrate and organizing pneumoniaconsisting of intraluminal loose connective tissue within thealveolar ducts and bronchioles. No hyaline membranes werepresent. In parenchyma not containing fibrin deposits, therewas a diffuse interstitial pneumonitis and fibrosis (Fig. 3).There was also mild patchy intra-alveolar hemorrhage withsmall amounts of hemosiderin (Fig. 4). There was no vascu-litis, capillaritis, or nuclear debris. There was no infarction orlymphoma. Silver, acid-fast, Brown-Hopps, and Periodicacid-Schiff (PAS) stains showed no organisms. CD138, IgG4,CD34, trichrome, and elastic stains were also examined. Thepleural biopsy consisted of fibrosis.
DISCUSSION
Acute fibrinous and organizing pneumonia is a recentlydescribed entity sharing similar histological features with OP,DAD, and EP, but with distinctive histopathology. Acute fibrin-ous and organizing pneumonia has previously been reportedin associated with connective tissue diseases including poly-myositis, ankylosing spondylitis, juvenile dermatomyositis,fibromyalgia, and a patient with suspected collagen vasculardisease including ANA positivity but no specific diagno-sis,11,13,14 but has not been reported in association with knownSLE. We report the first case of AFOP associated with SLE.
Acute fibrinous and organizing pneumonia is characterizedby the predominant histologic finding of fibrin deposits,forming fibrin balls within alveolar spaces in a patchy distri-bution. Organizing pneumonia is associated with the fibrindeposition, consisting of loose intraluminal connective tissueand a lymphoplasmacytic infiltrate. Whereas other reportsdescribe a lymphohistiocytic infiltrate, the presence of
plasma cells may be an important feature in distinguishingSLE associated AFOP. Hyaline membranes classically seenin DAD are not observed; however, hyaline membranes aretypically seen in the earlier exudative phase of DAD, which isoften followed by proliferative and fibrotic phases, duringwhich there is organization of intra-alveolar exudates, fol-lowed by progressive interstitial fibrosis and loss of hyalinemembranes. These later phases of DAD are distinguishedfrom AFOP by the disease distribution, where DAD is char-acterized by diffuse pathology affecting all aspects of lungparenchyma but AFOP is patchy, typically involving thealveoli and terminal bronchioles. Acute fibrinous and organiz-ing pneumonia is distinguished from OP and EP by the lackof fibrosis typically seen in OP and lack of eosinophilic infil-trate seen in EP.11 Although the overall histological patterns ofthese entities are distinct, the novelty of AFOP and the over-lapping histological features of AFOP with OP and especiallyDAD may be cause for AFOP to be underreported. However,given the similarities in clinical presentation and histologicalfeatures, it is possible that AFOP is part of a spectrum of DADand/or OP.
In this case, the patient also had antiphospholipid syn-drome as a manifestation of his SLE with subsequent pul-monary emboli 1.5 months prior to his lung biopsy. Thisraises the question of whether the patient’s AFOP pre-sented concomitantly with or subsequent to the emboli for-mation. His respiratory symptomology was unchangedbetween his presentation of pulmonary emboli and subse-quent respiratory difficulties following anticoagulationtherapy, thus it cannot be definitively discerned if thepatient’s AFOP is associated with his SLE, antiphospholipidsyndrome, both, or neither syndrome. Similarly, as thepatient has a history of large B cell lymphoma and AFOPhas been found associated with lymphoma, leukemia, andchemotherapy,11,15,16,21 one possibility is that the patient’sAFOP is somehow related to his history of lymphoma.However, we found no evidence of lymphoma and thepatient had been in remission for 2 years. A large scalestudy is required to provide more definitive evidence as tothe association between AFOP, SLE, and/or antiphospho-lipid syndrome, however given the rarity of this entity, astudy of this scale would be difficult to perform. As AFOPhas been associated with a spectrum of connective tissuediseases, the association should be further investigated.
REFERENCES
1 Harvey AM, Shulman LE, Tumulty PA, Conley CL, SchoenrichEH. Systemic lupus erythematosus: Review of the literature andclinical analysis of 138 cases. Medicine (Baltimore) 1954; 33:291–437.
2 Murin S, Wiedemann HP, Matthay RA. Pulmonary manifesta-tions of systemic lupus erythematosus. Clin Chest Med 1998;19: 641–65, viii.
758 L. P. Hariri et al.
© 2010 The AuthorsPathology International © 2010 Japanese Society of Pathology and Blackwell Publishing Asia Pty Ltd

3 Keane MP, Lynch JP 3rd. Pleuropulmonary manifestations ofsystemic lupus erythematosus. Thorax 2000; 55: 159–66.
4 Memet B, Ginzler EM. Pulmonary manifestations of systemiclupus erythematosus. Semin Respir Crit Care Med 2007; 28:441–50.
5 Swigris JJ, Fischer A, Gillis J, Meehan RT, Brown KK. Pulmo-nary and thrombotic manifestations of systemic lupus erythe-matosus. Chest 2008; 133: 271–80.
6 Lynch DA. Lung disease related to collagen vascular disease. JThorac Imaging 2009; 24: 299–309.
7 Gammon RB, Bridges TA, al-Nezir H, Alexander CB, KennedyJI Jr. Bronchiolitis obliterans organizing pneumonia associatedwith systemic lupus erythematosus. Chest 1992; 102: 1171–4.
8 Otsuka F, Amano T, Hashimoto N et al. Bronchiolitis obliteransorganizing pneumonia associated with systemic lupus erythe-matosus with antiphospholipid antibody. Intern Med 1996; 35:341–4.
9 Lamblin C, Bergoin C, Saelens T, Wallaert B. Interstitial lungdiseases in collagen vascular diseases. Eur Respir J Suppl2001; 32: 69s–80s.
10 Takada H, Saito Y, Nomura A et al. Bronchiolitis obliteransorganizing pneumonia as an initial manifestation in systemiclupus erythematosus. Pediatr Pulmonol 2005; 40: 257–60.
11 Beasley MB, Franks TJ, Galvin JR, Gochuico B, Travis WD.Acute fibrinous and organizing pneumonia: A histologicalpattern of lung injury and possible variant of diffuse alveolardamage. Arch Pathol Lab Med 2002; 126: 1064–70.
12 Cordeiro CR. Airway involvement in interstitial lung disease.Curr Opin Pulm Med 2006; 12: 337–41.
13 Prahalad S, Bohnsack JF, Maloney CG, Leslie KO. Fatal acutefibrinous and organizing pneumonia in a child with juveniledermatomyositis. J Pediatr 2005; 146: 289–92.
14 Balduin R, Giacometti C, Saccarola L et al. Acute fibrinous andorganizing pneumonia in a patient with collagen vasculardisease ‘stigma’. Sarcoidosis Vasc Diffuse Lung Dis 2007; 24:78–80.
15 Lee SM, Park JJ, Sung SH et al. Acute fibrinous and organizingpneumonia following hematopoietic stem cell transplantation.Korean J Intern Med 2009; 24: 156–9.
16 Yokogawa N, Alcid DV. Acute fibrinous and organizing pneumo-nia as a rare presentation of abacavir hypersensitivity reaction.Aids 2007; 21: 2116–17.
17 Tzouvelekis A, Koutsopoulos A, Oikonomou A et al. Acutefibrinous and organising pneumonia: A case report and review ofthe literature. J Med Case Reports 2009; 3: 74.
18 Kobayashi H, Sugimoto C, Kanoh S, Motoyoshi K, Aida S. Acutefibrinous and organizing pneumonia: Initial presentation as asolitary nodule. J Thorac Imaging 2005; 20: 291–3.
19 Cincotta DR, Sebire NJ, Lim E, Peters MJ. Fatal acute fibrinousand organizing pneumonia in an infant: The histopathologicvariability of acute respiratory distress syndrome. Pediatr CritCare Med 2007; 8: 378–82.
20 Bhatti S, Hakeem A, Torrealba J, McMahon JP, Meyer KC.Severe acute fibrinous and organizing pneumonia (AFOP)causing ventilatory failure: Successful treatment with mycophe-nolate mofetil and corticosteroids. Respir Med 2009; 103:1764–7.
21 Vasu TS, Cavallazzi R, Hirani A, Marik PE. A 64-year-old malewith fever and persistent lung infiltrate. Respir Care 2009; 54:1263–5.
A case report of AFOP in SLE 759
© 2010 The AuthorsPathology International © 2010 Japanese Society of Pathology and Blackwell Publishing Asia Pty Ltd