Embed Size (px)
Citation preview

Hindawi Publishing CorporationCase Reports in CardiologyVolume 2013, Article ID 609610, 4 pageshttp://dx.doi.org/10.1155/2013/609610
Case ReportAtypical Chest X-Ray Calcification in an Idiopathic ConstrictivePericarditis Case
ULur CoGkun,1 Esmail Polat Canbolat,1 Ümit YaGar Sinan,1
Cem Bostan,1 Kadriye KJlJçkesmez,1 Ahmet YJldJz,1 Murat BaGkurt,1
Fatma Nihan Turhan ÇaLlar,1 Alican Hatemi,2 Cenk Eray YJldJz,2 Sadettin Cöhcen,2
Aziz Tevfik Gürmen,1 and Mehmet Serdar KüçükoLlu1
1 Istanbul University, Institute of Cardiology, Cardiology Department, Haseki Street, Fatih, 34096 Istanbul, Turkey2 Istanbul University, Institute of Cardiology, Cardiovascular Surgery Department, Haseki Street, Fatih, 34096 Istanbul, Turkey
Correspondence should be addressed to Ugur Coskun; [email protected]
Received 7 May 2013; Accepted 11 June 2013
Academic Editors: H. Kataoka, K. P. Letsas, K. Nikus, J. Peteiro, D. Richter, C. S. Snyder, and M. B. Srichai
Copyright © 2013 Ugur Coskun et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Constrictive pericarditis is an uncommon cause of heart failure. It is a clinical entity caused by thickening, fibrosis, and/orcalcification of the pericardium. We present a 50-year-old female patient who was admitted to our institution with a 6-monthhistory of progressive dyspnea on exertion, abdominal swelling, and lower extremity edema. Her chest X-ray revealed an obliquelinear calcification in the cardiac silhouette. Transthoracic echocardiography revealed biatrial enlargement. Left ventricular size andsystolic function were normal. Cardiac computed tomography revealed the pericardial thickening (>5mm) and heavy calcificationin left atrioventricular groove. Simultaneous right and left heart catheterization showed elevation and equalization of right-sidedand left-sided diastolic filling pressures, with characteristic dip, and plateau. Pericardiectomywas performedwhich revealed a thick,fibrous, calcified, and densely adherent pericardium constricting the heart. The postoperative period was uneventful and was inNYHA functional class I after 3 months.
1. Introduction
Constrictive pericarditis (CP) is uncommon cause of heartfailure. It is a clinical entity caused by thickening, fibrosis,and/or calcification of the pericardium.This entity often leadsto impairment of diastolic filling, resulting predominantly insymptoms of right heart failure [1]. Currently, idiopathic orviral pericarditis is the predominant cause in the industrial-ized countries, followed by cardiac surgery and mediastinalirradiation, which are as well the major and increasing causesof CP in the industrialized countries [2–4]. Tuberculosis isstill a common cause of CP in developing and underdevel-oped countries, as well as in the immunosuppressed patients[5]. Modern series from Saudi Arabia, Mexico, Turkey, andIndia document tuberculosis in 38% to 83% of all cases of CP.Pericardial disease rarely presents as the initial manifestationof tuberculosis [6–9]. Although pericardial calcification on
chest X-ray suggests constriction, it is not diagnostic but maylead to more detailed investigations. A pericardial thicknessless than 2mm is normal and greater than 6mm in size isspecific for constriction [10]. Cardiac CT andMRI can detectpericardial thickening and calcification with high accuracy[11]. Echocardiography and new Doppler techniques are veryuseful for differential diagnosis between CP and restrictivecardiomyopathy [12, 13]. The gold standard for diagnosis iscardiac catheterization with analysis of intracavitary pressurecurves, which are high in end diastole and equal in allchambers.The diastolic profile in both ventricles presents thetypical dip-and-plateau pattern and the difference betweenthe diastolic pressures of both ventricles should not exceed3–5mmHg. Early diagnosis remains challenging and mayrequiremultimodal cardiac imaging. Confirming the diagno-sis of constrictive pericarditis is crucial, since surgical inter-ventionmay be the onlymethod for alleviating the symptoms.

2 Case Reports in Cardiology
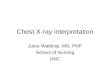
Figure 1: Oblique linear calcification (thick arrow) in chest X-ray.
2. Case Report
A 50-year-old female patient was admitted to our institutionwith 6-month history of progressive dyspnea on exertion,abdominal swelling, and lower extremity edema. Threemonths prior to her visit to our institution, the patient’s treat-ment was initiated in another medical service, with suspicionof liver disease, and she was given furosemide. However,her condition progressively worsened with extreme swellingof the lower limbs and abdomen, significant limitations oneffort, and difficulty to walk and to lie down in the supineposition. She had no past medical history.
On physical examination at admission to the cardiologydepartment, the patient was hemodynamically stable (bloodpressure 100/60mmHg and pulse 100 beat per minute irreg-ular), tachypneic (24 cpm), and not cyanotic (92% oxygensaturation in room air) but pale. Her pulse was strong,irregular and symmetrical. Cardiac and pulmonary ausculta-tion revealed a low intensity arrhythmia, normal S1 and S2sounds, and diminished breath sounds in both lung bases,accompanied by crackles. There was marked jugular venousdistension up to themandibular angle, painless hepatomegaly(liver palpable 5 cm below the right costal margin on themidclavicular line), positive hepatojugular reflux, and lowerlimb edema up to the knee (+++/++++).
Biochemical laboratory tests were in normal limits.Cardiac enzymes were normal, and brain natriuretic pep-tide (BNP) was slightly above normal, at 140 pg/mL (0–125 pg/mL). Chest X-ray showed an oblique linear calcifi-cation in the cardiac silhouette (Figure 1). The electrocar-diography revealed atrial fibrillation with diffuse nonspecificT-wave inversions. Transthoracic echocardiography revealedbiatrial enlargement. Left ventricular size and systolic func-tion were normal. Doppler transmitral inflow velocitiesrevealed a restrictive physiology, however, tissue Dopplervelocities of the mitral annulus were normal (10 cm/sec).Inferior vena cava was dilated (25mm), with reduced res-piratory variation (<50%). Cardiac computed tomography(CT) revealed the pericardial thickening (>5mm) and heavycalcification in left atrioventricular groove (Figure 2). Simul-taneous right and left heart catheterization showed elevation
Figure 2: Pericardial thickening (thin arrows) and heavy calcifica-tion of left atrioventricular groove (thick arrow) in cardiac CT.
Figure 3: Equalization of right sided and left-sided diastolic fillingpressures, with characteristic dip, and plateau in right-left cardiaccatheterization.
and equalization of right sided and left-sided diastolic fillingpressures, with characteristic dip and plateau (Figure 3).Coronary angiography was normal. During fluoroscopy,linear calcifications around the heart were seen, similarto the chest X-ray (Figure 4). All of the findings wereconsistent with constrictive pericarditis. Pericardiectomywas performed, which revealed a thick, fibrous, calcified,and densely adherent pericardium constricting the heart(Figure 5). Pathology revealed a pericardium thickness of0.5 cm, diffused fibrous tissue cells, nonspecific inflammatorycells, acellular hyalinization, and several focal dystrophiccalcifications. The postoperative period was uneventful, andthe patient was discharged from our hospital one monthafter admission with significant improvement, and she wasin NYHA functional class I after 3 months.
3. Discussion
The diagnosis of constrictive pericarditis should be seriouslyconsidered in patients with signs of chronic right side heartfailure with exertional dyspnea, lower limb edema, mild livercongestion, and chest X-ray calcification in the presence ofnormal ventricular contraction. Other cardiac diseases, inparticular right atrial myxoma, tricuspid valve dysfunction,and restrictive cardiomyopathy, must be ruled out [14]. Our

Case Reports in Cardiology 3
Figure 4: In coronary angiography during fluoroscopy linear calcifi-cations (thick arrow) around the heart.
Figure 5: Macroscopic thick pericardial pieces.
patient had right side heart failure symptoms and an atypicalchest X-ray calcification. This led us to consider additionalinvestigations. Therefore, we have performed cardiac CTand cardiac catheterization. The investigations allowed us toconfirm the diagnosis of constrictive pericarditis. Our patienthad no previous medical history of pericarditis, tuberculosis,open-heart surgery, chest trauma, or radiotherapy.Therefore,we ended up with the definitive diagnosis of idiopathicconstrictive pericarditis.
Ling et al. reported roentgenological localization of peri-cardial calcification in 36 out of 135 patients with constrictivepericarditis, who underwent pericardiectomy. They mostlyfound pericardial calcification on the inferior-diaphragmaticborder of the heart, rather than on the right ventricular areaand the end of left atrioventricular groove [15]. We considerthat our patient’s chest X-ray findings were different fromthose usually presented in constrictive pericarditis.
In conclusion, in case there is any calcification in achest X-ray with right-sided heart failure symptoms, weshould consider the diagnosis of constrictive pericarditis andperforming further cardiac investigations.
Conflict of Interests
This paper or part of it has not been published previously.There is no relationship with industry and financial associ-ations that might pose a conflict of interests.
Authors’ Contribution
All authors have contributions in the preparation of the paperand also have read and agreed on the contents of the paper.
References
[1] B. C.McCaughan, H. V. Schaff, and J. M. Piehler, “Early and lateresults of pericardiectomy for constrictive pericarditis,” Journalof Thoracic and Cardiovascular Surgery, vol. 89, no. 3, pp. 340–350, 1985.
[2] L. H. Ling, J. K. Oh, H. V. Schaff et al., “Constrictive pericarditisin the modern era: evolving clinical spectrum and impact onoutcome after pericardiectomy,” Circulation, vol. 100, no. 13, pp.1380–1386, 1999.
[3] J. Cameron, S. N. Oesterle, J. C. Baldwin, and E. W. Hancock,“The etiologic spectrum of constrictive pericarditis,” AmericanHeart Journal, vol. 113, no. 2, pp. 354–360, 1987.
[4] S. C. Bertog, S. K. Thambidorai, K. Parakh et al., “Constrictivepericarditis: etiology and cause-specific survival after peri-cardiectomy,” Journal of the American College of Cardiology, vol.43, no. 8, pp. 1445–1452, 2004.
[5] P. P. Sengupta, M. F. Eleid, and B. K. Khandheria, “Constrictivepericarditis,” Circulation Journal, vol. 72, no. 10, pp. 1555–1562,2008.
[6] V. V. Bashi, S. John, E. Ravikumar, P. S. Jairaj, K. Shyamsunder,and S. Krishnaswami, “Early and late results of pericardiectomyin 118 cases of constrictuve pericarditis,” Thorax, vol. 43, no. 8,pp. 637–641, 1988.
[7] M. Pedreira Perez, A. Virgos Lamela, F. J. CrespoMancebo et al.,“40 years’ experience in the surgical treatment of constrictivepericarditis,” Archivos del Instituto de Cardiologica de Mexico,vol. 57, pp. 363–373, 1987.
[8] H. Raffa and J. Mosieri, “Constrictive pericarditis in SaudiArabia,” East AfricanMedical Journal, vol. 67, no. 9, pp. 609–613,1990.
[9] S. Arsan, S. Mercan, A. Sarigul et al., “Long-term experiencewith pericardiectomy: analysis of 105 consecutive patients,”Thoracic and Cardiovascular Surgeon, vol. 42, no. 6, pp. 340–344, 1994.
[10] D. H. Spodick,The Pericardium: A Comprehensive Textbook, M.Dekker, New York, NY, USA, 1997.
[11] R. Rienmuller, M. Gurgan, E. Erdmann, B. M. Kemkes, E.Kreutzer, and C. Weinhold, “CT and MR evaluation of peri-cardial constriction: a new diagnostic and therapeutic concept,”Journal of Thoracic Imaging, vol. 8, no. 2, pp. 108–121, 1993.
[12] B. Maisch, P. M. Seferovic, A. D. Ristic et al., “Guidelines onthe diagnosis andmanagement of pericardial diseases.The TaskForce on theDiagnosis andManagement of PericardialDiseasesof the European Society of Cardiology,”EuropeanHeart Journal,vol. 25, pp. 587–610, 2004.
[13] J.-W. Ha, S. R. Ommen, A. J. Tajik et al., “Differentiation ofconstrictive pericarditis from restrictive cardiomyopathy usingmitral annular velocity by tissue Doppler echocardiography,”American Journal of Cardiology, vol. 94, no. 3, pp. 316–319, 2004.

4 Case Reports in Cardiology
[14] B. H. Lorell, “Pericardial diseases,” in Heart Disease, E. Braun-wald, Ed., pp. 1496–1505, W.B. Saunders Company, Philadel-phia, Pa, USA, 1997.
[15] L. H. Ling, J. K. Oh, J. F. Breen et al., “Calcific constrictivepericarditis: is it still with us?” Annals of Internal Medicine, vol.132, no. 6, pp. 444–450, 2000.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com