Embed Size (px)
Citation preview

CentralBringing Excellence in Open Access
Journal of Cardiology & Clinical Research
Cite this article: Katugaha SB, Swierzbinski MJ, Kapoor K, Singh R (2017) Candida glabrata Infection on Retained Implantable Cardioverter Defibrillator Lead in Heart Transplant Patient Requiring Redo Upper Mini-Sternotomy Approach. J Cardiol Clin Res 5(2): 1095.
*Corresponding author
Kunal Kapoor, VCU School of Medicine Inova Fairfax Campus, Inova Office of Undergraduate Medical Education, 3300 Gallows Rd, Falls Church, VA, 22042, USA, Tel: 703-776-6699; Email:
Submitted: 30 December 2016
Accepted: 01 February 2017
Published: 02 February 2017
Copyright© 2017 Kapoor et al.
OPEN ACCESS
Keywords•Candidaglabrata• Cardiovascular implantable Electronic Device (CIED)• Mini-sternotomy• Heart transplant
Case Report
Candida glabrata Infection on Retained Implantable Cardioverter Defibrillator Lead in Heart Transplant Patient Requiring Redo Upper Mini-Sternotomy ApproachShalika B. Katugaha1, Matthew J. Swierzbinski2, Kunal Kapoor3*, and Ramesh Singh4
1Infectious Diseases Physicians, Inova Fairfax Hospital Heart and Vascular Institute, USA2Infectious Diseases Physicians Inc., Annandale, USA3Virginia Commonwealth University School of Medicine Inova Campus, USA4Inova Fairfax Hospital Heart and Vascular Institute, USA
Abstract
We present the first documented case of a Candida glabrata infection on the retained lead of a cardiovascular implantable electronic device (CIED) in an immunosuppressed heart transplant recipient. This is the first documented case of a redo upper mini-sternotomy approach for a lead removal and innominate vein reconstruction with bovine patch. The patient is a 55 year-old male with non-ischemic cardiomyopathy with biventricular implantable cardioverter defibrillator (ICD) placement who underwent orthotropic heart transplant. ICD leads were divided at that time. A contralateral pacemaker was inserted post-operatively for complete heart block. The patient presented with four weeks of fever and erythema at the site of previous ICD placement. Transesophageal echo revealed echogenic structures measuring 1.8 cm and 1.1 cm attached to the pacer wire near the junction of the right atrium and inferior vena cava. Pacemaker leads were removed successfully. However, one of the three ICD leads fractured during extraction, leaving a residual coil. Culture of the extracted leads grew C. glabrata. A multi-disciplinary team including cardiothoracic surgery, infectious diseases, and cardiology determined that the most reliable way to eradicate infection would be to combine surgical management with aggressive medical management. Given multiple prior sternotomies, risk of re-entry into the thoracic cavity posed additional risks. An alternative surgical approach was performed to minimize risk.
ABBREVIATIONS CIED: Cardiovascular Implantable Electronic Device; ICD:
Implantable Cardioverter Defibrillator; SVC: Superior Vena Cava; IV: Intravenous
CASE PRESENTATIONThe patient is 55 year old Caucasian gentleman with a history
of non-ischemic cardiomyopathy with biventricular implantable cardioverter defibrillator (ICD) placement seventeen years prior. Eight years before presenting, he underwent an orthotropic heart transplant. In the two months prior to heart transplant, he required implantation of biventricular assist devices. At the time of heart transplant, his ICD was removed. The leads were divided at the superior vena cava (SVC) and in the pocket on the left.
Post-transplant, the patient experienced complete heart block, requiring placement of a dual chamber pacemaker on the right.
The patient presented to the hospital with four weeks of intermittent fevers and swelling, redness and pruritus at his previous ICD site. He also endorsed lethargy and unintentional weight loss. His symptoms persisted despite a two-week course of doxycycline. The patient’s immunosuppression included tacrolimus 2.5mg daily (level: 12.6 ng/mL) and mycophenolate mofetil 3g daily.
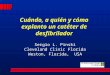
Physical exam was notable for erythema and swelling on the left side of the chest over the previous ICD site (Figure 1). The patient’s CBC revealed: white blood cell count of 3.82 K/cm, absolute neutrophil count of 5.92 K/uL, and absolute lymphocyte
CentralBringing Excellence in Open Access
Kapoor et al. (2017)Email:
2/3J Cardiol Clin Res 5(2): 1095 (2017)
count of 0.42K/uL. Chest x-ray revealed intact pacemaker leads. Three retained ICD leads were identified on the left.
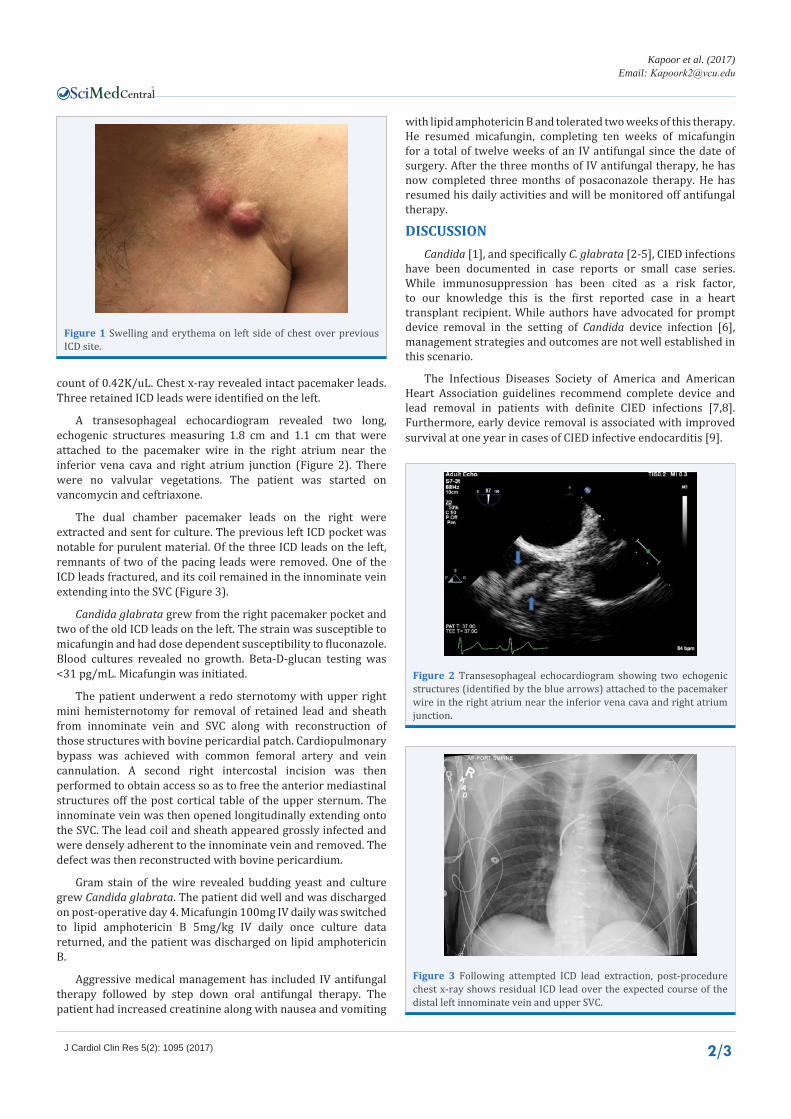
A transesophageal echocardiogram revealed two long, echogenic structures measuring 1.8 cm and 1.1 cm that were attached to the pacemaker wire in the right atrium near the inferior vena cava and right atrium junction (Figure 2). There were no valvular vegetations. The patient was started on vancomycin and ceftriaxone.
The dual chamber pacemaker leads on the right were extracted and sent for culture. The previous left ICD pocket was notable for purulent material. Of the three ICD leads on the left, remnants of two of the pacing leads were removed. One of the ICD leads fractured, and its coil remained in the innominate vein extending into the SVC (Figure 3).
Candida glabrata grew from the right pacemaker pocket and two of the old ICD leads on the left. The strain was susceptible to micafungin and had dose dependent susceptibility to fluconazole. Blood cultures revealed no growth. Beta-D-glucan testing was <31 pg/mL. Micafungin was initiated.
The patient underwent a redo sternotomy with upper right mini hemisternotomy for removal of retained lead and sheath from innominate vein and SVC along with reconstruction of those structures with bovine pericardial patch. Cardiopulmonary bypass was achieved with common femoral artery and vein cannulation. A second right intercostal incision was then performed to obtain access so as to free the anterior mediastinal structures off the post cortical table of the upper sternum. The innominate vein was then opened longitudinally extending onto the SVC. The lead coil and sheath appeared grossly infected and were densely adherent to the innominate vein and removed. The defect was then reconstructed with bovine pericardium.
Gram stain of the wire revealed budding yeast and culture grew Candida glabrata. The patient did well and was discharged on post-operative day 4. Micafungin 100mg IV daily was switched to lipid amphotericin B 5mg/kg IV daily once culture data returned, and the patient was discharged on lipid amphotericin B.
Aggressive medical management has included IV antifungal therapy followed by step down oral antifungal therapy. The patient had increased creatinine along with nausea and vomiting
with lipid amphotericin B and tolerated two weeks of this therapy. He resumed micafungin, completing ten weeks of micafungin for a total of twelve weeks of an IV antifungal since the date of surgery. After the three months of IV antifungal therapy, he has now completed three months of posaconazole therapy. He has resumed his daily activities and will be monitored off antifungal therapy.
DISCUSSIONCandida [1], and specifically C. glabrata [2-5], CIED infections
have been documented in case reports or small case series. While immunosuppression has been cited as a risk factor, to our knowledge this is the first reported case in a heart transplant recipient. While authors have advocated for prompt device removal in the setting of Candida device infection [6], management strategies and outcomes are not well established in this scenario.
The Infectious Diseases Society of America and American Heart Association guidelines recommend complete device and lead removal in patients with definite CIED infections [7,8]. Furthermore, early device removal is associated with improved survival at one year in cases of CIED infective endocarditis [9].
Figure 1 Swelling and erythema on left side of chest over previous ICD site.
Figure 2 Transesophageal echocardiogram showing two echogenic structures (identified by the blue arrows) attached to the pacemaker wire in the right atrium near the inferior vena cava and right atrium junction.
Figure 3 Following attempted ICD lead extraction, post-procedure chest x-ray shows residual ICD lead over the expected course of the distal left innominate vein and upper SVC.

CentralBringing Excellence in Open Access
Kapoor et al. (2017)Email:
3/3J Cardiol Clin Res 5(2): 1095 (2017)
Katugaha SB, Swierzbinski MJ, Kapoor K, Singh R (2017) Candida glabrata Infection on Retained Implantable Cardioverter Defibrillator Lead in Heart Transplant Patient Requiring Redo Upper Mini-Sternotomy Approach. J Cardiol Clin Res 5(2): 1095.
Cite this article
Cardiothoracic surgery, transplant infectious diseases, and transplant cardiology determined that our patient’s best chance for cure was surgical removal of the retained coil despite surgical risk.
Medical management alone would be ineffective because Candida species produce biofilms on synthetic devices, rendering them very difficult to eradicate from infected devices [1]. C. glabrata is known to have emerging resistance to both azoles and echinocandins [10,11]. An immunosuppressed heart transplant recipient would be at highest risk to fail medical therapy. Given that the retained lead had a gross appearance of infection and culture positivity for Candida glabrata while on IV micafungin, our case suggests the importance of device removal, especially in this population.
Surgery and location of the lead also carried a high mortality risk. Given prior thoracic surgeries, there was significant inflammation and the right ventricle was adherent to the sternum. Our surgical approach minimized damage to the right ventricle and other underlying structures.
To our knowledge, this is the first documented approach for a redo upper mini-sternotomy for infected lead removal with innominate vein reconstruction with bovine patch. Reports documenting success of upper mini hemisternotomies in redo cases include aortic valve replacements [12-15], thoracic aortic aneurysms [16], and aortic root and ascending aorta surgeries [17]. Though not a redo case, there is prior evidence that a mini-sternotomy approach has been successful in an innominate vein repair [18]. Our case highlights the utility of this less invasive surgical technique.
CONCLUSIONIn cases of Candida species associated with CIEDs, the
entire device needs to be removed for definitive treatment. This is especially true in solid organ transplant recipients, as immunosuppression renders antifungal therapy alone an ineffective approach. In this case, an alternative surgical approach utilizing an upper mini-sternotomy approach for wire removal and innominate vein reconstruction with bovine patch was undertaken to minimize risks.
REFERENCES1. Kojic EM, Darouiche RO. Candida infections of medical devices. Clin
Microbiol Rev. 2004; 17: 255-267.
2. Roger P-, Boissy C, Gari-Toussaint M, Foucher R, Mondain V, Vandenbos F, et al. Medical Treatment of a Pacemaker Endocarditis due to Candida albicans and to Candida glabrata. J Infect. 2000; 41: 176-178.
3. Glavis-Bloom J, Vasher S, Marmor M, Fine AB, Chan PA, Tashima KT, et al. Candida and cardiovascular implantable electronic devices: a case of lead and native aortic valve endocarditis and literature review. Mycoses. 2015; 58: 637-641.
4. Waheed A, Romano J, Raman AA, Raman A. Candida glabrata: an
unexpected culprit in endocarditis from an ICD lead. (A Case in Point). The Journal of Critical Illness. 2003; 18: 171.
5. Victor F, De Place C, Camus C, Le Breton H, Leclercq C, Pavin D, et al. Pacemaker lead infection: echocardiographic features, management and outcome. Heart. 1999; 81: 82-87.
6. Halawa A, Henry PD, Sarubbi FA. Candida endocarditis associated with cardiac rhythm management devices: review with current treatment guidelines. Mycoses. 2011; 54: e168-74.
7. Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016; 62: e1-50.
8. Baddour LM, Epstein AE, Erickson CC, Knight BP, Levison ME, Lockhart PB, et al. Update on cardiovascular implantable electronic device infections and their management: a scientific statement from the American Heart Association. Circulation. 2010; 121: 458-477.
9. Athan E, Chu VH, Tattevin P, Selton-Suty C, Jones P, Naber C, et al. Clinical characteristics and outcome of infective endocarditis involving implantable cardiac devices. JAMA. 2012; 307:1727-1735.
10. Pfaller MA, Andes DR, Diekema DJ, Horn DL, Reboli AC, Rotstein C, et al. Epidemiology and outcomes of invasive candidiasis due to non-albicans species of Candida in 2,496 patients: data from the Prospective Antifungal Therapy (PATH) registry 2004-2008. PLoS One. 2014; 9: e101510.
11. Alexander BD, Johnson MD, Pfeiffer CD, Jimenez-Ortigosa C, Catania J, Booker R, et al. Increasing echinocandin resistance in Candida glabrata: clinical failure correlates with presence of FKS mutations and elevated minimum inhibitory concentrations. Clin Infect Dis. 2013; 56: 1724-1732.
12. Mikus E, Calvi S, Tripodi A, Lamarra M, Del Giglio M. Upper ‘J’ ministernotomy versus full sternotomy: an easier approach for aortic valve reoperation. J Heart Valve Dis. 2013; 22: 295-300.
13. Gaeta R, Lentini S, Raffa G, Pellegrini C, Zattera G, Vigano M. Aortic valve replacement by ministernotomy in redo patients with previous left internal mammary artery patent grafts. Ann Thorac CardiovascSurg 2010; 16: 181-186.
14. Totaro P, Carlini S, Pozzi M, Pagani F, Zattera G, D’Armini AM, et al. Minimally invasive approach for complex cardiac surgery procedures. Ann Thorac Surg. 2009; 88: 462-466.
15. Dell’A more A, Del Giglio M, Calvi S, Pagliaro M, Fedeli C, Magnano D, et al. Mini re-sternotomy for aortic valve replacement in patients with patent coronary bypass grafts. Interact Cardiovasc Thorac Surg 2009; 9: 94-97.
16. Kamohara K, Furukawa K, Doi K, Itoh M, Furutachi A, Okazaki Y, et al. Staged resternotomy for a retrosternal giant aneurysm of the thoracic aorta using an inferior T-shaped ministernotomy. Ann Thorac Surg. 2011; 92: 1911-1913.
17. Perrotta S, Lentini S. Ministernotomy approach for surgery of the aortic root and ascending aorta. Interact CardiovascThoracSurg. 2009; 9: 849-858.
18. Siordia JA, Ayers GR, Garlish A, Subramanian S. Innominate vein repair after iatrogenic perforation with central venous catheter via mini-sternotomy-Case report. Int J Surg Case Rep. 2015; 11: 98-100.


![2015 S-ICD Coding Guide - Boston Scientific...ICD-9 Procedure Code Procedure Description 37.20 Non-invasive programmed electrical stimulation [NIPS] 37.70 Initial insertion of lead](https://img.pdfslide.net/doc/110x75/60f53dcb016c4641450e6342/2015-s-icd-coding-guide-boston-scientific-icd-9-procedure-code-procedure-description.jpg)