Embed Size (px)
Citation preview

Case ReportCardiac and Pulmonary Ultrasound for Diagnosing TRALI
J I Alonso-Fernaacutendez J R Prieto-Recio C Garciacutea-Bernardo I Garciacutea-SaizJ Rico-Feijoo and C Aldecoa
Anesthesiology and Postoperative Critical Care Department Rıo Hortega Universitary Hospital 47009 Valladolid Spain
Correspondence should be addressed to C Aldecoa caldecoaalsaludcastillayleones
Received 16 August 2015 Accepted 20 October 2015
Academic Editor Zsolt Molnar
Copyright copy 2015 J I Alonso-Fernandez et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
Unexpected acute respiratory failure after anesthesia is a diagnostic challenge residual neuromuscular blockade bronchialhyperresponsiveness laryngospasm atelectasis aspiration pneumonitis and other more uncommon causes should be taken intoaccount at diagnosis Lung ultrasound and echocardiography are diagnostic tools that would provide the differential diagnosis Wereport a suspected case of a transfusion related acute lung injury (TRALI) following administration of platelets The usefulness oflung and cardiac ultrasound is discussed to facilitate the challenging diagnosis of the acute early postoperative respiratory failure
1 Introduction
Respiratory failure which happens unexpectedly after anes-thesia is a diagnostic challenge Several concurrent causesin emergent surgery could explain respiratory distress andpostoperative hypoxemia residual neuromuscular blockadebronchial hyperresponsiveness laryngospasm atelectasischemical pneumonitis and other rarer causes such as heartfailure by volume overload ARDS due to a septic processpulmonary embolism or acute respiratory distress due totransfusion reactions
2 Case Report
We report the case of a 56-year-old woman with personalhistory of smoking dyslipidemia hypertension overweight(BMI 28) and amaurosis fugax episode whereby continuedantiplatelet therapy with clopidogrel The patient came to theemergency room for severe abdominal pain in the right lowerquadrant with nausea and vomiting of 24-hour durationThe examination revealed abdominal distension painfulpalpation in the right iliac fossa and decreased bowel sounds
The woman underwent abdominal ultrasound whichreported appendage of increased caliber with thickened walldata compatible with uncomplicated acute appendicitis She
entered the surgery department beginning antibiotic treat-ment with amoxicillinclavulanic and deciding urgent openinterventionThe preintervention clinical situationwas stablefrom both respiratory and hemodynamic points of view Thelaboratory exams and X-ray exams were also normal beforethe surgery
It was decided to administer a pool of platelets obtainedby apheresis with a volume of 250 cc in 30 minutes half anhour before intervention due to platelet dysfunction by clopi-dogrel Pharmacological induction of anesthesia with propo-fol fentanyl and rocuroniumwas performed Standardmon-itorization included SpO
2 ECG and noninvasive arterial
pressure and neuromuscular block monitoring was appliedIntubation was performed without any problems includingvomiting or aspiration After induction elevated airwaypressures were evident without bronchospasm signs in theauscultation improving after lung recruitment maneuversSubsequently she remained stable from both respiratory andhemodynamic points of view during the whole interventionThe surgery lasted 60 minutes No general peritonitis wasobserved Extubation was performed when the Train of Fourratio was higher than 09 and the conscious was recoveredAfter extubation while staying at the postanesthesia care unitfifteen minutes after the extubation she presented with pro-gressive dyspnea cyanosis and severe agitation which may
Hindawi Publishing CorporationCase Reports in Critical CareVolume 2015 Article ID 362506 4 pageshttpdxdoiorg1011552015362506
2 Case Reports in Critical Care
(a) (b)
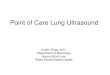
Figure 1 (a) Top Doppler tissue of the lateral mitral annulus showing the value of 1198901015840 Bottom Doppler mitral filling Together both imagesshow a pattern of normal mitral filling estimate normal filling pressure (value 1198641198901015840 lt 8) (b) The picture shows lung ultrasound realized witha sectorial probe in the patientrsquos right chest between fourth and fifth ribs in midclavicular line Figure shows presence of vertical B lines gt3mm (yellow arrows) indicative of pulmonary edema Blue arrows show rib shadows
be related to the hypoxia and necessitated the administrationof high-flow oxygen A lung auscultation showed no ralesrhonchi or wheezing She was moved to the ResuscitationUnit where she persisted in need of high concentrationsof oxygen The patient remained hemodynamically stablewithout tachycardia and in sinus rhythm No hypothermiaand shivering were observed
She underwent an urgent echocardiogram by an expertoperator showing cardiac chambers of normal size preservedsystolic function and normal pattern of relaxation fillingmitral 1198641198901015840 = 62 (lateral measures) and the tissue Dopplershows 1198861015840 minor compared to 1198901015840 (see Figure 1) Also thepresence of significant valvular and pericardial effusion wasdiscarded In the thoracic ultrasound the presence of B linesand areas of subpleural condensation in both hemithoraceswere shown (see Figure 1) An urgent chest radiographwas requested showing the presence of bilateral pulmonaryinfiltrates not present previously on admission Noninvasivemechanical ventilation was established after the TEE and theresults were observed Arterial blood and gas analysis wererepeated confirming the existence of moderate respiratoryfailure (PaO
2FiO2= 8406 = 140)
Faced with the possibility of having platelet transfusionreaction it was reported to the Hematology Departmentthat dismissed the remaining blood components from thesame donor Procalcitonin and lactate were also requestedshowing values within normal ranges Diuretic therapy wasinitiatedwithout improvement of pulmonary infiltrates in thefollowing hours In serial radiographs in 48 hours the pul-monary infiltrates persisted She remained hemodynamicallystable during the next three days The antibiotic treatmentwas discontinued on the third day of admission due to lackof fever and leukocytosis From a respiratory point of viewshe needed noninvasive ventilation with pressure support of15 cmH
2O The patient was discharged with supplemental
oxygen by nasal cannula on the fifth day of admission in
the Resuscitation Unit X-ray and lung ultrasound at dis-charging were normal
3 Discussion
TRALI is a clinical syndrome presented as acute hypoxemiaand noncardiogenic pulmonary edema during or after atransfusion of blood products There is no single definitionof this process but in 2004 the Canadian Blood Service andHema-Quebec proposed in its consensus conference somecriteria [1] that have been widely accepted Its incidence isnot well established Thus Silliman et al [2] establish theexistence of TRALI in 1 over 1323 blood product transfusionsPredisposition also seems to be different depending onthe type of blood product infused from highest to lowestrisk platelet transfusion of whole blood apheresis plateletspacked red cells and fresh frozen plasma Its pathophysiologyis not completely enlightened [3] and could be explained bya dual mechanism with the presence of leukocyte immuneantibodies or a cytokine liberation due to a preexisting lungdamage and subsequent migration of neutrophils causingthat pulmonary capillary injury
The clinical presentation includes dyspnea tachypneaand hypoxemia as cardinal symptoms Fever tachycardiahypotension and even hypertension may also be presentThere is no laboratory test to confirm the diagnosis of TRALI
The differential diagnosis of a patient who suddenlydevelops respiratory failure after a transfusion of bloodproducts should include hemodynamic overload anaphy-lactic reaction bacterial contamination of blood productstransfused and hemolytic transfusion reaction
In the reported case the differential diagnosis of hemo-dynamic overload was performed using echocardiographicassessment including both systolic function as noninvasiveestimation of filling pressure by 1198641198901015840
Case Reports in Critical Care 3
Transthoracic two-dimensional echocardiography hasbecome an essential tool for the confirmation of ARDSafter following the redefinition of Berlin The morphologicalstudy will allow us to analyze the size morphology andglobal and segmental contraction It allows discarding dilatedcardiomyopathy hypertrophic cardiomyopathy ventriculardysfunction or acute stress cardiomyopathy Application ofDoppler will allow us to assess valvular dysfunction and amore detailed assessment of the hemodynamic status anddiastolic function [4] The ldquoearly mitral flow peak velocity toearly diastolic mitral annulus displacement velocityrdquo (1198641198901015840)ratio correlates closely with left ventricular end-diastolicpressures (LVEDP) The mitral filling pattern with 1198641198901015840 isa method to estimate the right ventricular filling Valuesabove 15 have been correlated with high pulmonary wedgepressure and values below 9 have been correlatedwith normalone [5] Adding pulmonary venous flow to 1198641198901015840 ratio mayfacilitate LVEDP assessment To improve the accuracy of1198641198901015840 to assess the left ventricular pressure and discard a
pseudonormal pattern the use of the values of tissue Dopplerhas been proposed When the relationship in 11989010158401198861015840 is higherthan 1 a normal pattern is present However the assessmentof pulmonary venous flow using a transthoracic approach isdifficult
The morphology and function of the right ventriclecan also rule out the presence of acute or chronic corpulmonale Overall the information provided by echocardio-graphy allowed excluding cardiogenic pulmonary edema asthe primary cause of respiratory failure
Lung ultrasound is a supplement to the informationprovided by echocardiography The pulmonary ultrasound isable to define numerous causes that alter pulmonary function[6] In the ultrasound technique lung ribs spine and lung airact as barriers to ultrasounds causing artifacts that we recog-nize and interpret for a correct diagnosis The altered lungpresents a change in the airintrathoracic liquid ratio withthis liquid being either alveolar or interstitial edema or alsoblood mucus pus or increased cellularity The explorationis done in the supine position allowing easy anterolateralapproach and according to the BLUE protocol [7] 3 points ineach hemithorax are enough to draw conclusions Firstly thepresence of pleural sliding sign rules out pneumothorax as acause of respiratory failure The presence of B lines verticallines starting from the pleural line and extending in depthwith variations in size synchronized with the respiratorycycle is suggestive of an alveolar interstitial syndrome whichmeans cardiogenic or noncardiogenic pulmonary edemaMultiple B lines 7mm apart are caused by thickened interlob-ular septa characterizing interstitial edema [8] In contrast Blines 3mm or less apart are caused by ldquoground-glassrdquo areascharacterizing alveolar edema [9]The presence of subpleuralparenchyma with patchy consolidations and lines B is moresuggestive of ARDS heart failure as what happened in ourcase [10] The learning curve for B line assessment is short[11] and this method is reproducible without any variability[12]Thus the information that has been given by pulmonaryultrasound outdoes chest X-ray [13] The data supplied byechocardiography on systolic and diastolic function help todefine better the origin of pulmonary disorders
However although this approach is useful in most casesan area of uncertainty exists when 1198641198901015840 values are between9 and 15 and lung ultrasound does not show any dataof parenchymal damage In such cases advanced echocar-diographic methods [14] for estimating pulmonary wedgepressure further evaluations or invasive measurements maybe needed
The absence of rash urticaria or angioedema duringadministration of platelets and the absence of clinical andlaboratory data (procalcitonin) in severe sepsis and pre-postintervention also strengthens the diagnosis of acute lunginjury associated with transfusion (TRALI)
In conclusion whilemanaging a patient who has receivedsome type of blood product the presence of respiratory fail-ure requires a differential diagnosis with TRALIThe reversalof antiplatelet effect through platelet transfusion should beindividualized on urgent interventions Echocardiographytogether with thoracic ultrasound facilitates the differentialdiagnosis of respiratory failure in the surgical critical patient
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
The authors acknowledge James H Taylor MD as collabora-tor
References
[1] S Kleinman T Caulfield P Chan et al ldquoToward an under-standing of transfusion-related acute lung injury statement ofa consensus panelrdquo Transfusion vol 44 no 12 pp 1774ndash17892004
[2] C C Silliman L K Boshkov Z Mehdizadehkashi et alldquoTransfusion-related acute lung injury epidemiology and aprospective analysis of etiologic factorsrdquo Blood vol 101 no 2pp 454ndash462 2003
[3] A P J Vlaar and N P Juffermans ldquoTransfusion-related acutelung injury a clinical reviewrdquoThe Lancet vol 382 no 9896 pp984ndash994 2013
[4] S F Nagueh C P Appleton T C Gillebert et al ldquoRec-ommendations for the evaluation of left ventricular diastolicfunction by echocardiographyrdquo Journal of the American Societyof Echocardiography vol 22 no 2 pp 107ndash133 2009
[5] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressuresa comparative simultaneous Doppler-catheterization studyrdquoCirculation vol 102 no 15 pp 1788ndash1794 2000
[6] D Lichtenstein ldquoLung ultrasound in acute respiratory failure anintroduction to the BLUE-protocolrdquo Minerva Anestesiologicavol 75 no 5 pp 313ndash317 2009
[7] D A Lichtenstein and G A Meziere ldquoRelevance of lungultrasound in the diagnosis of acute respiratory failure theBLUE protocolrdquo Chest vol 134 no 1 pp 117ndash125 2008
4 Case Reports in Critical Care
[8] D Lichtenstein ldquoShould lung ultrasonography be more widelyused in the assessment of acute respiratory diseaserdquo ExpertReview of Respiratory Medicine vol 4 no 5 pp 533ndash538 2010
[9] G Volpicelli M Elbarbary M Blaivas et al ldquoInternationalevidence-based recommendations for point-of-care lung ultra-soundrdquo Intensive CareMedicine vol 38 no 4 pp 577ndash591 2012
[10] F Corradi C Brusasco and P Pelosi ldquoChest ultrasound in acuterespiratory distress syndromerdquo Current Opinion in CriticalCare vol 20 no 1 pp 98ndash103 2014
[11] V E Noble L Lamhaut R Capp et al ldquoEvaluation of a thoracicultrasound training module for the detection of pneumothoraxand pulmonary edema by prehospital physician care providersrdquoBMCMedical Education vol 9 article 3 2009
[12] D Lichtenstein I Goldstein E Mourgeon P Cluzel P Grenierand J-J Rouby ldquoComparative diagnostic performances ofauscultation chest radiography and lung ultrasonography inacute respiratory distress syndromerdquo Anesthesiology vol 100no 1 pp 9ndash15 2004
[13] P Van der Linden M Lambermont A Dierick et al ldquoRecom-mendations in the event of a suspected transfusion-related acutelung injury (TRALI)rdquoActaClinica Belgica vol 67 no 3 pp 201ndash208 2012
[14] F Gonzalez-Vilchez M Ares J Ayuela and L Alonso ldquoCom-bined use of pulsed and colorM-mode Doppler echocardiogra-phy for the estimation of pulmonary capillary wedge pressurean empirical approach based on an analytical relationrdquo Journalof the American College of Cardiology vol 34 no 2 pp 515ndash5231999
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Case Reports in Critical Care
(a) (b)
Figure 1 (a) Top Doppler tissue of the lateral mitral annulus showing the value of 1198901015840 Bottom Doppler mitral filling Together both imagesshow a pattern of normal mitral filling estimate normal filling pressure (value 1198641198901015840 lt 8) (b) The picture shows lung ultrasound realized witha sectorial probe in the patientrsquos right chest between fourth and fifth ribs in midclavicular line Figure shows presence of vertical B lines gt3mm (yellow arrows) indicative of pulmonary edema Blue arrows show rib shadows
be related to the hypoxia and necessitated the administrationof high-flow oxygen A lung auscultation showed no ralesrhonchi or wheezing She was moved to the ResuscitationUnit where she persisted in need of high concentrationsof oxygen The patient remained hemodynamically stablewithout tachycardia and in sinus rhythm No hypothermiaand shivering were observed
She underwent an urgent echocardiogram by an expertoperator showing cardiac chambers of normal size preservedsystolic function and normal pattern of relaxation fillingmitral 1198641198901015840 = 62 (lateral measures) and the tissue Dopplershows 1198861015840 minor compared to 1198901015840 (see Figure 1) Also thepresence of significant valvular and pericardial effusion wasdiscarded In the thoracic ultrasound the presence of B linesand areas of subpleural condensation in both hemithoraceswere shown (see Figure 1) An urgent chest radiographwas requested showing the presence of bilateral pulmonaryinfiltrates not present previously on admission Noninvasivemechanical ventilation was established after the TEE and theresults were observed Arterial blood and gas analysis wererepeated confirming the existence of moderate respiratoryfailure (PaO
2FiO2= 8406 = 140)
Faced with the possibility of having platelet transfusionreaction it was reported to the Hematology Departmentthat dismissed the remaining blood components from thesame donor Procalcitonin and lactate were also requestedshowing values within normal ranges Diuretic therapy wasinitiatedwithout improvement of pulmonary infiltrates in thefollowing hours In serial radiographs in 48 hours the pul-monary infiltrates persisted She remained hemodynamicallystable during the next three days The antibiotic treatmentwas discontinued on the third day of admission due to lackof fever and leukocytosis From a respiratory point of viewshe needed noninvasive ventilation with pressure support of15 cmH
2O The patient was discharged with supplemental
oxygen by nasal cannula on the fifth day of admission in
the Resuscitation Unit X-ray and lung ultrasound at dis-charging were normal
3 Discussion
TRALI is a clinical syndrome presented as acute hypoxemiaand noncardiogenic pulmonary edema during or after atransfusion of blood products There is no single definitionof this process but in 2004 the Canadian Blood Service andHema-Quebec proposed in its consensus conference somecriteria [1] that have been widely accepted Its incidence isnot well established Thus Silliman et al [2] establish theexistence of TRALI in 1 over 1323 blood product transfusionsPredisposition also seems to be different depending onthe type of blood product infused from highest to lowestrisk platelet transfusion of whole blood apheresis plateletspacked red cells and fresh frozen plasma Its pathophysiologyis not completely enlightened [3] and could be explained bya dual mechanism with the presence of leukocyte immuneantibodies or a cytokine liberation due to a preexisting lungdamage and subsequent migration of neutrophils causingthat pulmonary capillary injury
The clinical presentation includes dyspnea tachypneaand hypoxemia as cardinal symptoms Fever tachycardiahypotension and even hypertension may also be presentThere is no laboratory test to confirm the diagnosis of TRALI
The differential diagnosis of a patient who suddenlydevelops respiratory failure after a transfusion of bloodproducts should include hemodynamic overload anaphy-lactic reaction bacterial contamination of blood productstransfused and hemolytic transfusion reaction
In the reported case the differential diagnosis of hemo-dynamic overload was performed using echocardiographicassessment including both systolic function as noninvasiveestimation of filling pressure by 1198641198901015840
Case Reports in Critical Care 3
Transthoracic two-dimensional echocardiography hasbecome an essential tool for the confirmation of ARDSafter following the redefinition of Berlin The morphologicalstudy will allow us to analyze the size morphology andglobal and segmental contraction It allows discarding dilatedcardiomyopathy hypertrophic cardiomyopathy ventriculardysfunction or acute stress cardiomyopathy Application ofDoppler will allow us to assess valvular dysfunction and amore detailed assessment of the hemodynamic status anddiastolic function [4] The ldquoearly mitral flow peak velocity toearly diastolic mitral annulus displacement velocityrdquo (1198641198901015840)ratio correlates closely with left ventricular end-diastolicpressures (LVEDP) The mitral filling pattern with 1198641198901015840 isa method to estimate the right ventricular filling Valuesabove 15 have been correlated with high pulmonary wedgepressure and values below 9 have been correlatedwith normalone [5] Adding pulmonary venous flow to 1198641198901015840 ratio mayfacilitate LVEDP assessment To improve the accuracy of1198641198901015840 to assess the left ventricular pressure and discard a
pseudonormal pattern the use of the values of tissue Dopplerhas been proposed When the relationship in 11989010158401198861015840 is higherthan 1 a normal pattern is present However the assessmentof pulmonary venous flow using a transthoracic approach isdifficult
The morphology and function of the right ventriclecan also rule out the presence of acute or chronic corpulmonale Overall the information provided by echocardio-graphy allowed excluding cardiogenic pulmonary edema asthe primary cause of respiratory failure
Lung ultrasound is a supplement to the informationprovided by echocardiography The pulmonary ultrasound isable to define numerous causes that alter pulmonary function[6] In the ultrasound technique lung ribs spine and lung airact as barriers to ultrasounds causing artifacts that we recog-nize and interpret for a correct diagnosis The altered lungpresents a change in the airintrathoracic liquid ratio withthis liquid being either alveolar or interstitial edema or alsoblood mucus pus or increased cellularity The explorationis done in the supine position allowing easy anterolateralapproach and according to the BLUE protocol [7] 3 points ineach hemithorax are enough to draw conclusions Firstly thepresence of pleural sliding sign rules out pneumothorax as acause of respiratory failure The presence of B lines verticallines starting from the pleural line and extending in depthwith variations in size synchronized with the respiratorycycle is suggestive of an alveolar interstitial syndrome whichmeans cardiogenic or noncardiogenic pulmonary edemaMultiple B lines 7mm apart are caused by thickened interlob-ular septa characterizing interstitial edema [8] In contrast Blines 3mm or less apart are caused by ldquoground-glassrdquo areascharacterizing alveolar edema [9]The presence of subpleuralparenchyma with patchy consolidations and lines B is moresuggestive of ARDS heart failure as what happened in ourcase [10] The learning curve for B line assessment is short[11] and this method is reproducible without any variability[12]Thus the information that has been given by pulmonaryultrasound outdoes chest X-ray [13] The data supplied byechocardiography on systolic and diastolic function help todefine better the origin of pulmonary disorders
However although this approach is useful in most casesan area of uncertainty exists when 1198641198901015840 values are between9 and 15 and lung ultrasound does not show any dataof parenchymal damage In such cases advanced echocar-diographic methods [14] for estimating pulmonary wedgepressure further evaluations or invasive measurements maybe needed
The absence of rash urticaria or angioedema duringadministration of platelets and the absence of clinical andlaboratory data (procalcitonin) in severe sepsis and pre-postintervention also strengthens the diagnosis of acute lunginjury associated with transfusion (TRALI)
In conclusion whilemanaging a patient who has receivedsome type of blood product the presence of respiratory fail-ure requires a differential diagnosis with TRALIThe reversalof antiplatelet effect through platelet transfusion should beindividualized on urgent interventions Echocardiographytogether with thoracic ultrasound facilitates the differentialdiagnosis of respiratory failure in the surgical critical patient
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
The authors acknowledge James H Taylor MD as collabora-tor
References
[1] S Kleinman T Caulfield P Chan et al ldquoToward an under-standing of transfusion-related acute lung injury statement ofa consensus panelrdquo Transfusion vol 44 no 12 pp 1774ndash17892004
[2] C C Silliman L K Boshkov Z Mehdizadehkashi et alldquoTransfusion-related acute lung injury epidemiology and aprospective analysis of etiologic factorsrdquo Blood vol 101 no 2pp 454ndash462 2003
[3] A P J Vlaar and N P Juffermans ldquoTransfusion-related acutelung injury a clinical reviewrdquoThe Lancet vol 382 no 9896 pp984ndash994 2013
[4] S F Nagueh C P Appleton T C Gillebert et al ldquoRec-ommendations for the evaluation of left ventricular diastolicfunction by echocardiographyrdquo Journal of the American Societyof Echocardiography vol 22 no 2 pp 107ndash133 2009
[5] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressuresa comparative simultaneous Doppler-catheterization studyrdquoCirculation vol 102 no 15 pp 1788ndash1794 2000
[6] D Lichtenstein ldquoLung ultrasound in acute respiratory failure anintroduction to the BLUE-protocolrdquo Minerva Anestesiologicavol 75 no 5 pp 313ndash317 2009
[7] D A Lichtenstein and G A Meziere ldquoRelevance of lungultrasound in the diagnosis of acute respiratory failure theBLUE protocolrdquo Chest vol 134 no 1 pp 117ndash125 2008
4 Case Reports in Critical Care
[8] D Lichtenstein ldquoShould lung ultrasonography be more widelyused in the assessment of acute respiratory diseaserdquo ExpertReview of Respiratory Medicine vol 4 no 5 pp 533ndash538 2010
[9] G Volpicelli M Elbarbary M Blaivas et al ldquoInternationalevidence-based recommendations for point-of-care lung ultra-soundrdquo Intensive CareMedicine vol 38 no 4 pp 577ndash591 2012
[10] F Corradi C Brusasco and P Pelosi ldquoChest ultrasound in acuterespiratory distress syndromerdquo Current Opinion in CriticalCare vol 20 no 1 pp 98ndash103 2014
[11] V E Noble L Lamhaut R Capp et al ldquoEvaluation of a thoracicultrasound training module for the detection of pneumothoraxand pulmonary edema by prehospital physician care providersrdquoBMCMedical Education vol 9 article 3 2009
[12] D Lichtenstein I Goldstein E Mourgeon P Cluzel P Grenierand J-J Rouby ldquoComparative diagnostic performances ofauscultation chest radiography and lung ultrasonography inacute respiratory distress syndromerdquo Anesthesiology vol 100no 1 pp 9ndash15 2004
[13] P Van der Linden M Lambermont A Dierick et al ldquoRecom-mendations in the event of a suspected transfusion-related acutelung injury (TRALI)rdquoActaClinica Belgica vol 67 no 3 pp 201ndash208 2012
[14] F Gonzalez-Vilchez M Ares J Ayuela and L Alonso ldquoCom-bined use of pulsed and colorM-mode Doppler echocardiogra-phy for the estimation of pulmonary capillary wedge pressurean empirical approach based on an analytical relationrdquo Journalof the American College of Cardiology vol 34 no 2 pp 515ndash5231999
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Critical Care 3
Transthoracic two-dimensional echocardiography hasbecome an essential tool for the confirmation of ARDSafter following the redefinition of Berlin The morphologicalstudy will allow us to analyze the size morphology andglobal and segmental contraction It allows discarding dilatedcardiomyopathy hypertrophic cardiomyopathy ventriculardysfunction or acute stress cardiomyopathy Application ofDoppler will allow us to assess valvular dysfunction and amore detailed assessment of the hemodynamic status anddiastolic function [4] The ldquoearly mitral flow peak velocity toearly diastolic mitral annulus displacement velocityrdquo (1198641198901015840)ratio correlates closely with left ventricular end-diastolicpressures (LVEDP) The mitral filling pattern with 1198641198901015840 isa method to estimate the right ventricular filling Valuesabove 15 have been correlated with high pulmonary wedgepressure and values below 9 have been correlatedwith normalone [5] Adding pulmonary venous flow to 1198641198901015840 ratio mayfacilitate LVEDP assessment To improve the accuracy of1198641198901015840 to assess the left ventricular pressure and discard a
pseudonormal pattern the use of the values of tissue Dopplerhas been proposed When the relationship in 11989010158401198861015840 is higherthan 1 a normal pattern is present However the assessmentof pulmonary venous flow using a transthoracic approach isdifficult
The morphology and function of the right ventriclecan also rule out the presence of acute or chronic corpulmonale Overall the information provided by echocardio-graphy allowed excluding cardiogenic pulmonary edema asthe primary cause of respiratory failure
Lung ultrasound is a supplement to the informationprovided by echocardiography The pulmonary ultrasound isable to define numerous causes that alter pulmonary function[6] In the ultrasound technique lung ribs spine and lung airact as barriers to ultrasounds causing artifacts that we recog-nize and interpret for a correct diagnosis The altered lungpresents a change in the airintrathoracic liquid ratio withthis liquid being either alveolar or interstitial edema or alsoblood mucus pus or increased cellularity The explorationis done in the supine position allowing easy anterolateralapproach and according to the BLUE protocol [7] 3 points ineach hemithorax are enough to draw conclusions Firstly thepresence of pleural sliding sign rules out pneumothorax as acause of respiratory failure The presence of B lines verticallines starting from the pleural line and extending in depthwith variations in size synchronized with the respiratorycycle is suggestive of an alveolar interstitial syndrome whichmeans cardiogenic or noncardiogenic pulmonary edemaMultiple B lines 7mm apart are caused by thickened interlob-ular septa characterizing interstitial edema [8] In contrast Blines 3mm or less apart are caused by ldquoground-glassrdquo areascharacterizing alveolar edema [9]The presence of subpleuralparenchyma with patchy consolidations and lines B is moresuggestive of ARDS heart failure as what happened in ourcase [10] The learning curve for B line assessment is short[11] and this method is reproducible without any variability[12]Thus the information that has been given by pulmonaryultrasound outdoes chest X-ray [13] The data supplied byechocardiography on systolic and diastolic function help todefine better the origin of pulmonary disorders
However although this approach is useful in most casesan area of uncertainty exists when 1198641198901015840 values are between9 and 15 and lung ultrasound does not show any dataof parenchymal damage In such cases advanced echocar-diographic methods [14] for estimating pulmonary wedgepressure further evaluations or invasive measurements maybe needed
The absence of rash urticaria or angioedema duringadministration of platelets and the absence of clinical andlaboratory data (procalcitonin) in severe sepsis and pre-postintervention also strengthens the diagnosis of acute lunginjury associated with transfusion (TRALI)
In conclusion whilemanaging a patient who has receivedsome type of blood product the presence of respiratory fail-ure requires a differential diagnosis with TRALIThe reversalof antiplatelet effect through platelet transfusion should beindividualized on urgent interventions Echocardiographytogether with thoracic ultrasound facilitates the differentialdiagnosis of respiratory failure in the surgical critical patient
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
The authors acknowledge James H Taylor MD as collabora-tor
References
[1] S Kleinman T Caulfield P Chan et al ldquoToward an under-standing of transfusion-related acute lung injury statement ofa consensus panelrdquo Transfusion vol 44 no 12 pp 1774ndash17892004
[2] C C Silliman L K Boshkov Z Mehdizadehkashi et alldquoTransfusion-related acute lung injury epidemiology and aprospective analysis of etiologic factorsrdquo Blood vol 101 no 2pp 454ndash462 2003
[3] A P J Vlaar and N P Juffermans ldquoTransfusion-related acutelung injury a clinical reviewrdquoThe Lancet vol 382 no 9896 pp984ndash994 2013
[4] S F Nagueh C P Appleton T C Gillebert et al ldquoRec-ommendations for the evaluation of left ventricular diastolicfunction by echocardiographyrdquo Journal of the American Societyof Echocardiography vol 22 no 2 pp 107ndash133 2009
[5] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressuresa comparative simultaneous Doppler-catheterization studyrdquoCirculation vol 102 no 15 pp 1788ndash1794 2000
[6] D Lichtenstein ldquoLung ultrasound in acute respiratory failure anintroduction to the BLUE-protocolrdquo Minerva Anestesiologicavol 75 no 5 pp 313ndash317 2009
[7] D A Lichtenstein and G A Meziere ldquoRelevance of lungultrasound in the diagnosis of acute respiratory failure theBLUE protocolrdquo Chest vol 134 no 1 pp 117ndash125 2008
4 Case Reports in Critical Care
[8] D Lichtenstein ldquoShould lung ultrasonography be more widelyused in the assessment of acute respiratory diseaserdquo ExpertReview of Respiratory Medicine vol 4 no 5 pp 533ndash538 2010
[9] G Volpicelli M Elbarbary M Blaivas et al ldquoInternationalevidence-based recommendations for point-of-care lung ultra-soundrdquo Intensive CareMedicine vol 38 no 4 pp 577ndash591 2012
[10] F Corradi C Brusasco and P Pelosi ldquoChest ultrasound in acuterespiratory distress syndromerdquo Current Opinion in CriticalCare vol 20 no 1 pp 98ndash103 2014
[11] V E Noble L Lamhaut R Capp et al ldquoEvaluation of a thoracicultrasound training module for the detection of pneumothoraxand pulmonary edema by prehospital physician care providersrdquoBMCMedical Education vol 9 article 3 2009
[12] D Lichtenstein I Goldstein E Mourgeon P Cluzel P Grenierand J-J Rouby ldquoComparative diagnostic performances ofauscultation chest radiography and lung ultrasonography inacute respiratory distress syndromerdquo Anesthesiology vol 100no 1 pp 9ndash15 2004
[13] P Van der Linden M Lambermont A Dierick et al ldquoRecom-mendations in the event of a suspected transfusion-related acutelung injury (TRALI)rdquoActaClinica Belgica vol 67 no 3 pp 201ndash208 2012
[14] F Gonzalez-Vilchez M Ares J Ayuela and L Alonso ldquoCom-bined use of pulsed and colorM-mode Doppler echocardiogra-phy for the estimation of pulmonary capillary wedge pressurean empirical approach based on an analytical relationrdquo Journalof the American College of Cardiology vol 34 no 2 pp 515ndash5231999
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Case Reports in Critical Care
[8] D Lichtenstein ldquoShould lung ultrasonography be more widelyused in the assessment of acute respiratory diseaserdquo ExpertReview of Respiratory Medicine vol 4 no 5 pp 533ndash538 2010
[9] G Volpicelli M Elbarbary M Blaivas et al ldquoInternationalevidence-based recommendations for point-of-care lung ultra-soundrdquo Intensive CareMedicine vol 38 no 4 pp 577ndash591 2012
[10] F Corradi C Brusasco and P Pelosi ldquoChest ultrasound in acuterespiratory distress syndromerdquo Current Opinion in CriticalCare vol 20 no 1 pp 98ndash103 2014
[11] V E Noble L Lamhaut R Capp et al ldquoEvaluation of a thoracicultrasound training module for the detection of pneumothoraxand pulmonary edema by prehospital physician care providersrdquoBMCMedical Education vol 9 article 3 2009
[12] D Lichtenstein I Goldstein E Mourgeon P Cluzel P Grenierand J-J Rouby ldquoComparative diagnostic performances ofauscultation chest radiography and lung ultrasonography inacute respiratory distress syndromerdquo Anesthesiology vol 100no 1 pp 9ndash15 2004
[13] P Van der Linden M Lambermont A Dierick et al ldquoRecom-mendations in the event of a suspected transfusion-related acutelung injury (TRALI)rdquoActaClinica Belgica vol 67 no 3 pp 201ndash208 2012
[14] F Gonzalez-Vilchez M Ares J Ayuela and L Alonso ldquoCom-bined use of pulsed and colorM-mode Doppler echocardiogra-phy for the estimation of pulmonary capillary wedge pressurean empirical approach based on an analytical relationrdquo Journalof the American College of Cardiology vol 34 no 2 pp 515ndash5231999
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom





















![TotalAnomalousPulmonaryVenousConnectionwithLethal ......Diagnosing PVO at the foetal stage is challenging be-cause there is lower pulmonary blood flow in the foetal circulation [1]](https://img.pdfslide.net/doc/110x75/6131d9d91ecc51586944fe7e/totalanomalouspulmonaryvenousconnectionwithlethal-diagnosing-pvo-at-the.jpg)






